
Abstract
This study investigated whether manipulation of motor cortex excitability by transcranial direct current stimulation (tDCS) modulates neuromuscular fatigue and functional near-infrared spectroscopy (fNIRS)-derived prefrontal cortex (PFC) activation. Fifteen healthy men (27.7 ± 8.4 years) underwent anodal (2 mA, 10 min) and sham (2 mA, first 30 s only) tDCS delivered to the scalp over the right motor cortex. Subjects initially performed a baseline sustained submaximal (30 % maximal voluntary isometric contraction, MVC) isometric contraction task (SSIT) of the left elbow flexors until task failure, which was followed 50 min later by either an anodal or sham treatment condition, then a subsequent posttreatment SSIT. Endurance time (ET), torque integral (TI), and fNIRS-derived contralateral PFC oxygenated (O2Hb) and deoxygenated (HHb) hemoglobin concentration changes were determined at task failure. Results indicated that during the baseline and posttreatment SSIT, there were no significant differences in TI and ET, and increases in fNIRS-derived PFC activation at task failure were observed similarly regardless of the tDCS conditions. This suggests that the PFC neuronal activation to maintain muscle force production was not modulated by anodal tDCS.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others
Keywords
- Maximal Voluntary Contraction
- Endurance Time
- Cortical Excitability
- Elbow Flexor
- Corticospinal Excitability
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Transcranial direct current stimulation (tDCS) is a noninvasive and minimally discomforting electrical brain stimulation technique that is used to modulate cortical excitability and behavioral responses [1, 2]. tDCS has been used for the treatment of a variety of neurological or neuropsychiatric disorders. tDCS applies low-intensity (1 ~ 2 mA) controlled direct currents to the scalp overlying a target region of the brain via surface electrodes. The tDCS effects on cortical excitability are dependent on current polarity, intensity, and duration of the stimulation, such that anodal stimulation over the motor cortex increases corticospinal excitability, whereas cathodal stimulation decreases corticospinal excitability [2].
Neuromuscular fatigue is represented by a decrease in the ability of muscle fibers to generate force, which can be attributed to both central and peripheral mechanisms. Peripheral fatigue is characterized by changes at or distal to the neuromuscular junction, whereas central fatigue refers to a progressive reduction in voluntary neuronal activation of muscle during exercise. Central fatigue can be further differentiated into changes in the activity of spinal motoneurons (spinal fatigue) due to intrinsic cellular properties (e.g., discharge rates) and to reduced motor cortical neuronal drive (supraspinal fatigue), and both these central fatigue levels can be modulated by afferent inputs [3].
Cogiamanian et al. [4] were the first to investigate whether manipulation of motor cortex excitability by anodal tDCS (1.5 mA, 10 min) modulates neuromuscular fatigue in healthy subjects during a subsequent sustained submaximal isometric contraction task (SSIT) at 35 % of maximal voluntary contraction (MVC) of the elbow flexors until task failure. Their results indicated that anodal tDCS improved endurance time (ET) during posttreatment SSIT by ~ 20 % compared to sham tDCS (i.e., baseline SSIT compared to posttreatment SSIT), suggesting a decrease in residual neuromuscular fatigue that was modulated by anodal tDCS via central (supraspinal) neuroplastic mechanisms.
Previous neuroimaging studies have reported that, during neuromuscular fatigue of unilateral small muscle group exercise, the prefrontal cortex (PFC) increases neuronal activation to reinforce muscle force for the continuation of the performance [5–9]. This increase in cortical neuronal activation during neuromuscular fatigue is implied by an enhanced cortical oxygenation and blood flow by means of a neurovascular coupling mechanism [10]. Noninvasive functional near-infrared spectroscopy (fNIRS) neuroimaging measures several physiological parameters related to cortical oxygenation and blood flow and includes measurements of concentration changes in oxygenated (O2Hb) and deoxygenated (HHb) hemoglobin. Therefore, the aim of this study was to investigate the fNIRS-derived PFC activation responses of anodal tDCS modulation of motor cortex excitability during a subsequent SSIT of the elbow flexors until task failure.
2 Methods
2.1 Subjects
Fifteen healthy men (mean ± SD age, height, and weight: 27.7 ± 8.4 years, 176.4 ± 7.4 cm, 72.7 ± 8.7 kg, respectively) participated in the study. All subjects had no known health problems (e.g., metabolic or neuromuscular disorders) or any upper extremity muscle or joint injuries. The study conformed to the recommendations of the local Human Research Ethics Committee in accordance with the Declaration of Helsinki.
2.2 Experimental Setup
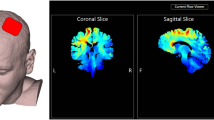
An Eldith tDCS system (Neuroconn, Ilmenau, Germany) was used to deliver constant direct currents (2 mA) through a pair of 0.3-cm-thick square (24 cm2) sponge electrodes soaked in saline solution (140 mM NaCL). The anode electrode was placed on the scalp overlying the right motor cortical representation of the left arm, and the cathode was placed over the right shoulder based on the electrode setup method described by Cogiamanian et al. [4].
Subjects were seated on a preacher arm curl bench, securing the shoulder angle at 45 ° flexion with a supinated forearm position and an elbow joint angle of 90 °. The elbow joint was aligned with the axis of rotation of an isokinetic dynamometer (Cybex6000, Lumex Inc., Ronkonkoma, USA). Torque signals were collected onto a data acquisition system (PowerLab, ADInstruments, Bella Vista, Australia) at a sampling rate of 200 Hz, and real-time visual feedback of torque signals was displayed on the computer monitor.
A NIRO-200 oximeter (Hamamatsu Photonics K.K., Hamamatsu, Japan) was used to measure PFC O2Hb and HHb concentration changes using the modified Beer-Lambert Law. The probe unit has two silicon photodiodes as photodetectors on one side and three laser-emitting diodes (775, 810, and 850 nm) on the other side separated from each other by a distance of 4 cm. A probe unit was firmly attached over the skin of the forehead (in a region corresponding to Fp2 according to the 10–20 International EEG system) contralateral to the left exercising arm with a double-sided adhesive tape. The probe unit, in turn, was covered with a black band. The NIRO-200 provides estimates of concentration changes (from an arbitrary baseline of zero) in O2Hb and HHb at a sampling rate of 6 Hz. The quantification of O2Hb and HHb concentration changes, expressed in ΔμM, was obtained by including an age-dependent constant differential path length factor (5.13 + 0.07 × age0.81) [11].
2.3 Protocol
Subjects underwent anodal or sham tDCS treatment conditions separated by 1–2 weeks and the order of intervention was randomized among the participants. Subjects initially performed three 3-s MVCs with a 45-s rest between contractions, and MVC was determined by taking the mean peak torque of the three MVC trials. Following a 3-min rest, subjects performed a baseline SSIT of the left elbow flexors at 30%MVC until task failure, which was followed 50 min later by either anodal or sham treatment conditions. The sham intervention was identical to the tDCS intervention, except that the current was programmed to return to zero for the remaining time period after 30 s of stimulation. A posttreatment SSIT was performed ~ 10 min following the treatment conditions.
2.4 Statistical Analysis
ET at task failure was determined by the time point in which participants were unable to maintain greater than 90 % of the target torque output for more than 2 s, in spite of continual verbal encouragement. Torque integral (TI) was determined as the area under the torque curves until task failure. PFC O2Hb and HHb concentration changes were determined at task failure (average of 5 s around this time point). ET, TI, and PFC O2Hb and HHb changes during the baseline and posttreatment SSIT were compared between the anodal and sham tDCS sessions by a two-way repeated measures ANOVA. An individual paired Student’s t-test was used to determine if PFC O2Hb and HHb changes were different from pre-exercise levels for both anodal and sham tDCS conditions. Significance was set at P ≤ 0.05. Data are presented as mean ± SD.
3 Results
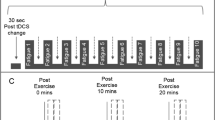
Figure 11.1 shows typical changes in torque and fNIRS-derived PFC activation (i.e., increase in O2Hb and decrease in HHb) during an SSIT until task failure. Group results indicated that during the baseline SSIT, there were no significant differences between anodal or sham tDCS conditions for ET, TI, or PFC O2Hb and HHb changes. Similarly, during the posttreatment SSIT, there was no significant difference between the anodal and sham tDCS conditions for ET (333 ± 119 s vs. 353 ± 146 s, respectively) and TI (5,907 ± 2,557 vs. 6,020 ± 2,597 Nm · s−1, respectively). Although right PFC O2Hb increased and HHb decreased significantly (P < 0.05) relative to pre-exercise levels during the posttreatment SSIT for both anodal (11.3 ± 4.0 and −0.9 ± 2.2 μM, respectively) and sham (10.1 ± 4.2 and −1.1 ± 1.8 μM, respectively) tDCS conditions, there was no significant difference between the conditions.


Typical single-subject recordings of the changes in torque and fNIRS-derived PFC activation (i.e., increase in O2Hb and decrease in HHb) during a 30 % MVC SSIT of the elbow flexors until task failure (second dashed line) following 10-min anodal tDCS condition. Endurance time at task failure was determined by the time point in which participants were unable to maintain greater than 90 % of the target torque output for more than 2 s
4 Discussion
To the best of our knowledge, this is the first study to determine PFC activation during a tDCS-modulated neuromuscular fatigue task. The present study found no significant effects of anodal tDCS on ET, TI, and fNIRS-derived PFC activation during a subsequent SSIT of the elbow flexors. It is important to note that there was no significant difference in ET results within and between anodal and sham tDCS conditions (i.e., baseline and posttreatment SSIT), which is in contrast to Cogiamanian et al. [4] who reported an ~ 40 % reduction in ET in sham tDCS and a smaller reduction of ~ 20 % with anodal tDCS during posttreatment SSIT compared to baseline SSIT. Thus, in the present study, it can be suggested that no residual neuromuscular fatigue was induced by the baseline SSIT on the subsequent posttreatment SSIT.
One reason for the lack of difference between anodal and sham tDCS conditions for the dependent variables could be due to a nonsignificant effect of our tDCS electrode setup to induce changes in cortical excitability. In the present study, no assessment of corticospinal excitability changes was included such as motor-evoked potential (MEP) changes upon transcranial magnetic stimulation (TMS). However, in a subsequent study that utilized TMS (unpublished), no significant changes in MEP were observed after a similar tDCS electrode setup and protocol to that of the present study. Thus, in the present study, it appears that no significant differences in PFC activation during the posttreatment SSIT between anodal and sham tDCS conditions could indicate no modulation of cortical excitability by anodal tDCS and no effect on central (supraspinal) fatigue mechanisms and PFC activation. In future studies, it would be important to use a tDCS electrode setup that has consistently been shown to increase motor cortex excitability (e.g., anode over the motor cortex and cathode over the contralateral frontopolar cortex) [2].
Another possibility for our findings could be that our relatively strict determination of task failure during the 30 % MVC SSIT protocol (i.e., > 90 % of target torque for > 2 s) may not have allowed fatigue to develop to a level that necessitated tDCS modulation. tDCS is known to alter firing rates of motor cortical neurons due to a shift of resting membrane potentials, such that it is assumed that anodal tDCS can increase motor unit recruitment due to the depolarization of resting membrane potentials of motor cortex neurons and corticospinal excitability [2]. Rupp and Perrey [9] reported that fNIRS-derived PFC activation increased (i.e., O2Hb increase and HHb decrease) from pre-exercise levels to exhaustion (ET = ~ 460 s) during a unilateral SSIT at 40 % MVC of the ankle extensors. They concluded that centrally mediated decrease in neuronal activation, as reflected by fNIRS-derived PFC activation measurements, was likely not implicated in neuromuscular fatigue during an SSIT of a small muscle group. In the present study, it could be suggested that maximal voluntary neuronal activation was possible at task failure during our SSIT protocol, such that anodal tDCS was unlikely to further increase voluntary activation, suggesting a ceiling effect at corticospinal levels. This then would also explain the similar fNIRS-derived PFC activation levels at task failure between anodal and sham tDCS conditions.
5 Conclusion
In conclusion, this study showed that the 10-min anodal tDCS treatment at 2 mA did not affect neuromuscular fatigue and fNIRS-derived PFC activation compared to a sham tDCS treatment. This could be due in part to our tDCS electrode setup to induce an increase in motor cortex excitability, a ceiling effect of tDCS to modulate motor cortex excitability and/or to an absence of supraspinal fatigue mechanisms during the SSIT.
References
Nitsche MA, Liebetanz D, Lang N, Antal A, Tergau F, Paulus W (2003) Safety criteria for transcranial direct current stimulation (tDCS) in humans. Clin Neurophysiol 114(11):2220–2222
Nitsche MA, Paulus W (2000) Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J Physiol 527(Pt 3):633–639
Gandevia SC (2001) Spinal and supraspinal factors in human muscle fatigue. Physiol Rev 81(4):1725–1789
Cogiamanian F, Marceglia S, Ardolino G, Barbieri S, Priori A (2007) Improved isometric force endurance after transcranial direct current stimulation over the human motor cortical areas. Eur J Neurosci 26(1):242–249
Mottola L, Crisostomi S, Ferrari M, Quaresima V (2007) Relationship between handgrip sustained submaximal exercise and prefrontal cortex oxygenation. Adv Exp Med Biol 578:305–309
Muthalib M, Ferrari M, Quaresima V, Nosaka K (2012) Frontal cortex activation during electrical muscle stimulation as revealed by functional near-infrared spectroscopy. Adv Exp Med Biol 737:45–49
Liu JZ, Shan ZY, Zhang LD, Sahgal V, Brown RW, Yue GH (2003) Human brain activation during sustained and intermittent submaximal fatigue muscle contractions: an FMRI study. J Neurophysiol 90(1):300–312
Millet GY, Muthalib M, Jubeau M, Laursen PB, Nosaka K (2012) Severe hypoxia affects exercise performance independently of afferent feedback and peripheral fatigue. J Appl Physiol 112(8):1335–1344
Rupp T, Perrey S (2009) Effect of severe hypoxia on prefrontal cortex and muscle oxygenation responses at rest and during exhaustive exercise. Adv Exp Med Biol 645:329–334
Perrey S (2008) Non-invasive NIR, spectroscopy of human brain function during exercise. Methods 45(5):289–299
Duncan A, Meek JH, Clemence M et al (1995) Optical pathlength measurements on adult head, calf and forearm and the head of the newborn infant using phase resolved optical spectroscopy. Phys Med Biol 40(2):295–304
Acknowledgments
The authors would like to thank Prof. Marco Ferrari and Prof. Samuele Marcora for their valuable comments on the manuscript.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this paper
Cite this paper
Muthalib, M., Kan, B., Nosaka, K., Perrey, S. (2013). Effects of Transcranial Direct Current Stimulation of the Motor Cortex on Prefrontal Cortex Activation During a Neuromuscular Fatigue Task: An fNIRS Study. In: Van Huffel, S., Naulaers, G., Caicedo, A., Bruley, D.F., Harrison, D.K. (eds) Oxygen Transport to Tissue XXXV. Advances in Experimental Medicine and Biology, vol 789. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-7411-1_11
Download citation
DOI: https://doi.org/10.1007/978-1-4614-7411-1_11
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-7256-8
Online ISBN: 978-1-4614-7411-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)