
Abstract
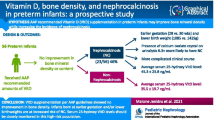
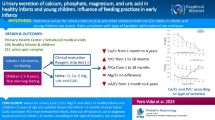
The incidence of urolithiasis in infants is unknown. The aim of this study was to investigate clinical characteristics, nutrition, calcium, phosphate, 25-hydroxyvitamin D (25(OH)D), alkaline phosphate, and parathyroid hormone in infants with urolithiasis. There were 32 infants (23 boys and 9 girls) of the mean age of 6.4 ± 3.7 months (range 2–12 months), with diagnosis of urolithiasis enrolled into the study. Boys were younger than girls (5.3 vs. 9.1 months, respectively; p < 0.05). The infants were receiving prophylactic vitamin D3. Twenty-one of them were fed with milk formula, 9 were breastfed, and 2 were on a mixed diet. The major clinical symptoms consisted of irritability in 19 (59%) and urinary tract infection in 6 (19%) infants. Hypercalcemia and hyperphosphatemia were detected in the serum in 30 (94%) and 19 (60%) infants, respectively. The serum calcium level was higher in boys than girls (10.8 vs. 9.8 mg/dL, respectively; p < 0.05). Four (12.5%) infants had increased activity of alkaline phosphatase. The serum level of 25(OH)D was high in 3 (9%), low in 2 (6%), and normal in 27 (85%) infants. Parathyroid hormone was low in eight (25%) infants. Hypercalciuria and hyperphosphaturia were found in 11 (34%) boys and 8 (25%) girls. Family history of urolithiasis was positive in eight (25%) infants. We conclude that urolithiasis occurs in infancy more often in boys fed with milk formula and in those who received vitamin D supplementation. Hypercalcemia, hyperphosphatemia, and hypercalciuria are the most common changes present in clinical metabolic tests.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
The incidence of pediatric urolithiasis depends on the geographic, genetic, and socioeconomic factors and is on the rise worldwide (Weigert and Hoppe 2018; Jobs et al. 2014; López and Hoppe 2010). Approximately 10% of all cases of urinary stones are diagnosed in infants (Hesse 2005). Urolithiasis appears at any age in pediatric population. In the youngest infants, predisposing causes can be recognized in 75–80% of patients (Walther et al. 1980). The most common risk factors of urinary stone formation are metabolic changes such as hypercalciuria, hyperoxaluria, and hypocitraturia (Milliner and Murphy 1993).
25-Hydroxyvitamin D (25(OH)D) has pleiotropic effects in human body, since vitamin D receptors are expressed in the majority of cells (Unal et al. 2014). The all-presence of vitamin D3 receptors has clinical implications in that it may have to do with a reduction of risk of cancer, autoimmune and infectious diseases, depression, diabetes, and cardiovascular incidents (Pludowski et al. 2018). Vitamin D3 in a dose of 400 IU a day for infants, who are exclusively breastfed, is recommended by the Institute of Medicine of the US National Academy of Sciences, the American Endocrine Society, the European Society for Pediatric Gastroenterology Hepatology and Nutrition, and the American Academy of Pediatrics to prevent rickets (Holick et al. 2011; IOM 2011). The serum concentration of 25(OH)D between 20 and 50 ng/mL is established as the normal range. A routine measurement of 25(OH)D is not recommended for healthy infants, but those with chronic diseases can benefit from monitoring. In some patients, however, vitamin D3 supplementation may have significant adverse effects such as hypercalcemia, hypercalciuria, constipation, hypertension, nephrocalcinosis, or urolithiasis. Therefore, this study seeks to define the relationship between the content of 25(OH)D and calcium and urolithiasis in infants aged under 12 months.
2 Methods
Thirty-two infants aged 2–12 months (23 boys and 9 girls), who had been referred to the Department of Pediatrics and Nephrology of Warsaw Medical University in Warsaw, Poland, due to newly diagnosed urolithiasis, were investigated. The exclusion criteria were chronic liver or kidney diseases, history of prematurity or low birth weight (< 2,500 g), and a failure to growth. The survey was conducted on nutrition, vitamin D3 supplementation, clinical symptoms, and family history of urolithiasis. The serum levels of calcium (Ca), phosphate (P), alkaline phosphatase (ALP), parathyroid hormone (PTH), 25(OH)D, and capillary blood gas and acid-base content were investigated. In addition, urinary calcium, phosphate, magnesium, and creatinine were investigated in random urine samples. These measurements were conducted with a dry-chemistry method (VITROS 5600, Ortho Clinical Diagnostics, Raritan, NJ 08869). The PTH content was measured with an immunoenzymatic method using the Immulite 2000xPi system (Siemens Medical Solutions Diagnostics, NJ) with a reference range of 10–65 pg/mL. The serum content of vitamin D3 was measured with the chemiluminescence method using the ARCHITECT i1000SR system (Abbott Diagnostics; Chicago, IL), with a reference range of 20–50 ng/mL. The urine calcium/creatinine (Ca/Cr), magnesium/creatinine, and phosphate/creatinine (P/Cr) ratios were calculated. The reference range for Ca/Cr was taken as less than 0.81 (Habbig et al. 2011; Hoppe and Kemper 2010). The infants were divided into the female and male groups. Metabolic indicators were compared between the two groups.
Data were presented as means ±SD and 95 confidence intervals (95%CI). Differences between the female and male groups were evaluated with a two-tailed unpaired t-test. A p-value <0.05 defined statistically significant differences. The analysis was performed using a commercial Statistica package v11.0 for Windows (StatSoft; Tulsa, OK).
3 Results
Table 1 shows the baseline characteristics of infants with urolithiasis. Urinary stones were diagnosed by means of abdominal ultrasonography. The calculi were seen in the left kidney in 25 (78%) infants, in 17 (53%) in the right kidney, and in 9 (28%) bilaterally. Ultrasonography was ordered in infants due to unexplained irritability in 19 (59%), urinary tract infection in 6 (19%), or a dilation of the urinary collecting system in 7 (22%) cases. The urinary tract infection was caused by Pseudomonas aeruginosa in one, Klebsiella spp. in four, and Enterobacter spp. in one infant. All of the infants received oral vitamin D3 in a total dose of 400–500 IU a day since the neonatal period. Twenty-one infants received only milk formula, supplemented with 40–56 IU of vitamin D3 per 100 ml of milk, 9 were breastfed, and 2 were both breastfed and also received milk formula. A family history of urolithiasis was negative in 24 (75%) infants (Table 1).
Hypercalcemia was detected in 30 (95%) and hyperphosphatemia in 19 (60%) infants with urolithiasis. The serum PTH content was below 10 pg/mL in 8 (25%) infants, and there was no single case of increased PTH. An increased level of ALP was noticed in only 4 (12%) infants, with the remaining 28 infants having a normal ALP level. Blood gas and acid-base content was within the norm in all infants. The serum 25(OH)D content was elevated in three (9%) and was below the lower cutoff value in two (6%) infants with urolithiasis. The remaining 27 infants had the level of 25(OH)D within the normal range (Fig. 1).

Serum 25(OH)D content in infants with urolithiasis
All of the infants had a fresh urine sample examined under light microscopy to exclude cystinuria. Hypercalciuria was found in 11 (34.4%) patients with urolithiasis; the excretion of calcium was within the norm in 21 (65.6%) infants. Hyperphosphaturia was found in eight (25%) infants. Eighteen (56.2%) infants had the Mg/Cr ratio > 0.2 (Table 2).
The results also were stratified into the female (mean age 9.1 ± 3.3 months) and male (mean age 5.3 ± 2.4 months) groups. The only significant gender difference found was a higher calcium level in the male infants (Table 3). In addition, we found a significant inverse correlation between calcium and both 25(OH)D and ALP (Table 4).
4 Discussion
Urolithiasis affects infants of all ages. In a large study done by Zafar et al. (2018), boys are more frequently affected, during the first 2 years of life. The current study provided similar results as we noticed that there were 72% of males and 28% of females in the investigated population of infants with urolithiasis. However, symptoms of urolithiasis in infants are non-specific and can remain asymptomatic for a long time. Therefore, the exact incidence of urinary tract stones is largely unknown. In a study of Marzuillo et al. (2017), about half or more infants with urolithiasis presented abdominal or flank pain without specific urinary symptoms. In the current study, the most common symptom of urolithiasis was unexplained irritability detected in 59.4% of infants. In fact, colicky pain, hematuria, sterile pyuria, flank tenderness, and urinary retention are rather atypical symptoms for the age of few months. A routine ultrasonography in a patient with urinary tract infection is helpful in the diagnosis of the underlying urinary tract stones. In the current study, the etiology of urinary tract infections in infants with urolithiasis was atypical, consisting mostly of Pseudomonas aeruginosa, Klebsiella spp., and Enterobacter spp.
In the clinical setting, a reliable medical history is extremely important for the appropriate diagnosis and treatment of urolithiasis in infants. Approximately 40% of infants with urinary tract stones have a positive family history (Van’t Hoff 2004). In the infants of the present, 25% of them had a family history of urolithiasis. We observed that the most important information from medical history is that on nutrition and fluid intake. Although breastfeeding in the first year of life is commonly recommended, most of the infants studied (66%) received milk formula, which is fortified with vitamin D3. Yet aside from that, each infant was supplemented with an additional dose of 400–500 IU vitamin D daily.
It ought to be recognized that urolithiasis is only a symptom of other underlying diseases. Infants with urinary tract stones are more likely to have metabolic disorders, especially hypercalciuria and hypocitraturia. The prevalence of hypercalciuria in healthy infants has been reported at 3–7% (Skalova and Lutilek 2006). However, the incidence of hypercalciuria in patients with urolithiasis is much higher. In the current study, hypercalciuria was found in 34.4% of patients. Similar observation has been done in a study of Ergon et al. (2017) in which hypercalciuria is observed in 38% of infants with urolithiasis. Fallahzadeh et al. (2012) have evaluated 36 infants with urolithiasis and found the presence of hypercalciuria in 27.8% of them.
Hypercalciuria can be primary or secondary. Primary idiopathic hypercalciuria is the most common cause of calcium-containing stones in infants. Hypercalciuria and metabolic alkalosis also are observed in a number of genetic diseases such as Bartter’s syndrome type 1, type 2, or infantile type with sensorineural deafness. Other genetic causes of hypercalciuria with urolithiasis are autosomal dominant hypocalcemic hypercalciuria (ADHH) (OMIM Entry – *601199) due to mutations in the calcium-sensing receptor (CASR) gene, familial hypomagnesemia 3 (HOMG3) (OMIM Entry – *248250) due to a defect in renal tubular transport of magnesium, Claudins such as CLDN19 (OMIM Entry *603959) due to transmembrane proteins interacting with the function of tight junctions, or different types of Dent disease (OMIM Entries *300008, *300009, *310468) due to misfunction of voltage-gated chloride ion channel (CLC-5). Another reason of hypercalciuria is a distal renal tubular acidosis. In the autosomal dominant renal tubular acidosis syndromes (OMIM Entry *179800, *109270), hypocitric aciduria, hypokalemia, and osteomalacia are present. Other types of renal tubular acidosis are the autosomal recessive forms (OMIM Entry *602722, *605239) or those with the accompanying hearing loss (OMIM Entry *267300, *192132). In case of a suspected genetic disease, molecular genetic testing should be performed (Ammenti et al. 2006).
Secondary hypercalciuria in young infants is mainly caused by vitamin D toxicity or hyperparathyroidism. It can develop as a result of parenteral nutrition, high protein diet, or treatment with furosemide. Hypervitaminosis D, caused by excessive exogenous supplementation, can also induce hypercalcemia and hypercalciuria. However, most studies do not support the presence of a significant association between a higher serum level of 25(OH)D and increased risk of urinary stone formation. Tang and Chonchol (2013) have demonstrated that a short-term nutritional vitamin D3 supplementation in patients with 25(OH)D deficiency does not increase urinary calcium excretion.
In the current study, we found that most of the infants with urolithiasis had hypercalcemia. The serum level of calcium was higher in boys than in girls, but it failed to associate with the serum 25(OH)D level. We excluded the possibility of hypercalcemia due to the presence of the Williams-Beuren syndrome (OMIM Entry *194050) in any of the infants. This study also demonstrates that most of the infants with urolithiasis had the 25(OH)D content within the normal range and also normal activity of PTH. The serum content of 25(OH)D was increased in only three (9.4%) infants. Hypercalcemia and hypercalciuria in these infants could be ascribed to the overdosing of vitamin D3. Infants with hypercalcemia and a normal level of 25(OH)D have, in all likelihood, idiopathic hypercalcemia (Nesterova et al. 2013). The potential reason for idiopathic infantile hypercalcemia is mutations in the CYP24A1 gene that encodes for the enzyme converting the active forms of vitamin D to inactive metabolites (Ketha et al. 2015). Idiopathic hypercalcemia manifests during infancy with acute episodes of hypercalcemia, hypercalciuria, and nephrocalcinosis (Dinour et al. 2013; Gigante et al. 2016).
A limitation of the current study was a small group of patients from a single clinical center. We also encountered some difficulties in the assessment of calcium excretion. The most important tool in the diagnosis of hypercalciuria is a 24-h urine collection, which is usually difficult in infants, particularly that bladder catheterization is not recommended in this case. In the clinical setting, calcium excretion is most often assessed from random urine samples, and it may somehow vary depending on the diet, medication, and fluid intake.
Despite these limitations we believe we have demonstrated that the most important risk factor for urolithiasis in infants is hypercalcemia. Particular attention should be paid to infants with hypercalcemia who receive milk formula and additional vitamin D3 supplementation. This study also demonstrates that hypercalciuria was a dominant, but not ubiquitous, metabolic abnormality in urine of infants with urolithiasis. The incidence of hypercalciuria was lower than that hypercalcemia. Interestingly, majority of infants with urolithiasis had a normal serum level of 25(OH)D. A low incidence of hypercalciuria detected in infants could be secondary to stone formation in the urinary tract. We believe that the possibility of CYP24A1 gene mutations should be taken into consideration in the diagnostics of infants with urolithiasis, which may have relevance to foreseeing the risk of urolithiasis in adulthood.
References
Ammenti A, Neri E, Agistri R, Beseghi U, Bacchini E (2006) Idiopathic hypercalciuria in infants with renal stones. Pediatr Nephrol 21(12):1901–1903
Dinour D, Beckerman P, Ganon L, Tordjaman K, Eisenstein Z, Holtzman EJ (2013) Loss-of–function mutations of CYP24A1, the vitamin D 24–hydroxylase gene, cause long–standing hypercalciuric nephrolitiasis and nephrocalcinosis. J Urol 190(2):552–557
Ergon EY, Akil İO, Taneli F, Oran A, Ozyurt BC (2017) Etiologic risk factors and vitamin D receptor gene polymorphisms in under one–year–old infants with urolithiasis. Urolithiasis 46(4):349–356
Fallahzadeh MH, Zare J, GH A–H, Derakhshan A, Basiratnia M, Arasteh MM, Fallahzadeh MA, Fallahzadeh MK (2012) Elevated serum levels of Vitamin D in infants with urolithiasis. Iran J Kidney Dis 6(3):186–191
Gigante M, Santangelo L, Diella S, Caridi G, Argentiero L, D’Alessandro MM, Martino M, Stea ED, Ardissino G, Carbone V, Pepe S, Scrutinio D, Maringhini S, Ghiggeri GM, Grandaliano G, Giordano M, Gesualdo L (2016) Mutational spectrum of CYP21A1 gene in a cohort of Italian patients with idiopathic infantile hypercalcemia. Nephron 133(3):193–204
Habbig S, Beck BB, Hoppe B (2011) Nephrocalcinosis and urolithiasis in infants. Kidney Int 80(12):1278–1291
Hesse A (2005) Reliable data from diverse regions of the world exist to show that there has been a steady increase in the prevalence of urolithiasis. World J Urol 23:302–303
Holick MF, Binkley NC, Bischoff–Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH, Weaver CM, Endocrine Society (2011) Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96:1911–1930
Hoppe B, Kemper MJ (2010) Diagnostic examination of the child with urolithiasis or nephrocalcinosis. Pediatr Nephrol 25:403–413
IOM (2011) Dietary reference intakes for calcium and vitamin D. Institute of Medicine of the US National Academy of Sciences. The National Academic Press, Washington, DC
Jobs K, Straż-Żebrowska E, Placzyńska M, Zdanowski R, Kalicki B, Lewicki S, Jung A (2014) Interleukin–18 and NGAL in assessment of ESWL treatment safety in infants with urolithiasis. Cent Eur J Immunol 39(3):384–391
Ketha H, Wadams H, Lteif A, Singh RJ (2015) Iatrogenic vitamin D toxicity in an infant – a case report and review of literature. J Steroid Biochem Mol Biol 148:14–18
López M, Hoppe B (2010) History, epidemiology and regional diversities of urolithiasis. Pediatr Nephrol 25(1):49–59
Marzuillo P, Guarino S, Apicella A, La Manna A, Polito C (2017) Why we need a higher suspicion index of urolithiasis in infants. J Pediatr Urol 13(2):164–171
Milliner DS, Murphy ME (1993) Urolithiasis in pediatric patients. Mayo Clin Proc 68:241–248
Nesterova G, Malicdan MC, Yasuda K, Sakaki T, Vilboux T, Ciccone C, Horst R, Huang Y, Golas G, Introne W, Huizing M, Adams D, Boerkoel CF, Collins MT, Gahl WA (2013) 1,25–(OH)2D–24 hydroxylase (CYP24A1) deficiency as a cause of nephrolithiasis. Clin J Am Soc Nephrol 8(4):649–657
Pludowski P, Holick MF, Grant WB, Konstantynowicz J, Mascarenhas MR, Haq A, Povoroznyuk V, Balatska N, Barbosa AP, Karonova T, Rudenka E, Misiorowski W, Zakharova I, Rudenka A, Łukaszkiewicz J, Marcinowska–Suchowierska E, Łaszcz N, Abramowicz P, Bhattoa HP, Wimalawansa SJ (2018) Vitamin D supplementation guidelines. J Steroid Biochem Mol Biol 175:125–135
Skalova S, Lutilek S (2006) High urinary N–Acetyl–beta–d–glokosaminidase activity and normal calciuria in infants with nocturnal enuresis. Indian Pediatr 43:655–656
Tang J, Chonchol MB (2013) Vitamin D and kidney stone disease. Curr Opin Nephrol Hypertens 22(4):383–389
Unal AD, Tarcin O, Parildar H, Cigerli O, Eroglu H, Nilgun Guvener Demirag NG (2014) Vitamin D deficiency is related to thyroid antibodies in autoimmune thyroiditis. Cent Eur J Immunol 39(4):493–497
Van’t Hoff WG (2004) Aetiological factors in paediatric urolithiasis. Nephron Ciln Pract 98:c45–c48
Walther PC, Lamm D, Kaplan GW (1980) Pediatric urolithiasis: a ten–year review. Pediatrics 65:1068–1072
Weigert A, Hoppe B (2018) Nephrolithiasis and nephrocalcinosis in childhood–risk factor–related current and future treatment options. Front Pediatr 6:98
Zafar MN, Ayub S, Tanwri H, Naqvi SAA, Rizvi SAH (2018) Composition of urinary calculi in infants: a report from an endemic country. Urolithiasis 46(5):445–452
Conflicts of Interest
The authors declare that they have no conflicts of interest in relation to this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all parents/guardians of all the individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Szmigielska, A., Pańczyk-Tomaszewska, M., Borowiec, M., Demkow, U., Krzemień, G. (2019). Vitamin D and Calcium Homeostasis in Infants with Urolithiasis. In: Pokorski, M. (eds) Advances in Medicine and Medical Research. Advances in Experimental Medicine and Biology(), vol 1133. Springer, Cham. https://doi.org/10.1007/5584_2018_310
Download citation
DOI: https://doi.org/10.1007/5584_2018_310
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-12922-4
Online ISBN: 978-3-030-12923-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)