
Abstract
Chronic obstructive pulmonary disease (COPD) is a lung disease that is often associated with chronic bronchitis, bronchiolitis and emphysema. The disease pathology is heterogeneous in nature and usually results from several environmental factors including cigarette smoke, biomass smoke particle, diesel and automobile exhausts that can potentially expose lung tissues into severe oxidative stress condition. Some individuals, with genetic predisposition, are worse affected. The disease pathology becomes complicated and deadly when environmental and genetic factors both work in a concerted manner. In recent years, transient receptor potential (TRP) channels have been identified as key factors in COPD initiation and progression. TRP channels have been widely implicated as potential targets for genetic manipulation and pharmacological intervention to control the disease. The present chapter briefly discusses expression pattern of different TRP channel members in the lungs and airway epithelium, their physiological role in developing COPD disease pathology with special attention to oxidative stress and the pharmacological intervention and possible genetic manipulation to tackle the disease in near future.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Chronic obstructive pulmonary disease (COPD) is usually caused by multiple factors, and it is the fourth leading cause of death worldwide [1]. COPD disease pathology is heterogeneous in nature, and it includes chronic bronchitis, bronchiolitis and emphysema. The condition is presented by chronic airway inflammation [2], and the disease pathology is associated with obstruction of airflow into the lung [3,4,5]. The condition is not fully reversible at the onset of the disease and is usually progressive in nature, causing debilitating disability and finally death.
Asthmatic condition is often treated with glucocorticoids, but it is unsuccessful in treating COPD-related inflammation. Until now, no effective therapeutic and pharmacological intervention is available to reduce COPD-associated mortality [6, 7]. Extensive research performed in this specific subject area has identified oxidative damage to lung epithelial cells is directly linked to the COPD disease pathology [8,9,10]. Several factors, including smoking, domestic smoke exposure, outdoor pollution, socio-economic status, and ethnicity, have been identified as major contributors towards developing COPD [11].
Reactive oxygen species (ROS) are known causative agents for cellular oxidative stress and tissue damages. Oxidative stress in pathological condition causes oxidant burden. Free dioxygen radical (O2−.) in oxidative stress condition may function as signal transduction molecule in initiation and progression of the COPD disease state. Transient receptor potential (TRP) channels have been widely implicated in relation to COPD initiation and progression [12,13,14,15]. TRP channels are polymodal cation selective ion channels that sense and respond to environmental changes and stimuli such as pH, temperature, osmolarity and exposure to chemical agents. TRP channels also play a significant role in several cellular processes, including apoptosis and neural functions. The mechanism of calcium influx through ROS-sensitive channel and subsequent cellular signaling mechanisms are still largely unknown.
In recent past, scientists put significant effort in order to inhibit ROS-activated TRP channels by antioxidant treatment. TRPM2, one subgroup of the TRP channels, have been reported to be ROS-sensor [16]. Recent development in this specific area has identified TRPM2 channel as a potential candidate in order to modulate the antioxidant enzyme glutathione peroxidase activity [17].
TRPA1, expressed in the chemosensory C-fibers, has been reported to be activated by most of the oxidizing and electrophilic chemicals including but not limited to chlorine, acrolein, isocyanates and tear gas. The chemical stimuli exert their toxic effects by activating TRPA1 through covalent protein modification [18].
COPD disease pathology is not only restricted to lungs, but it has been established as a systemic disease that significantly affects multiple organ systems. Smoking cigarette is directly linked to developing COPD-associated morbidities, and the beneficial effect of quitting smoking has been emphasized as a first line of correcting measure to treat the disease [19].
Human body is constantly exposed not only to oxidants from exogenous sources but also to the reactive oxidant species (ROS) produced endogenously. Glutathione-S-transferase (GST) and superoxide dismutase (SOD) are two main antioxidant enzymes responsible for scavenging ROS activity and play pivotal roles in maintaining redox homeostasis. Cigarette smoke and other environmental pollutants irritate various immune cells located in the lung and cause oxidative stress. Epithelial cells being first line of defense is usually worse affected. This phenomenon ultimately leads to a disruption in redox homeostasis and cause severe damage, which in turn contributes toward developing COPD [20].
Different experimental approaches have identified TRP channels respond to several exogenous stimuli to the airway sensory neurons. The stimuli include harmful chemicals, stimuli causing pain, glandular secretion, depression, cough and other protective responses.
Till date, about 30 TRP channels have been identified. These are further subdivided into seven main subfamilies on the basis of sequence homology. These are TRPC (canonical), TRPV (vanniloid), TRPM (melastatin), TRPP (polycystein), TRPML (mucolipin), TRPA (ankyrin) and TRPN (NOMPC-like). TRPN channels are found only in invertebrates and fish, and the expression of other six subfamilies has been confirmed in human. The subsequent effect of TRP channel activation leads to either neurogenic inflammatory and/or brain-mediated responses of the airways. If undiagnosed and left untreated, these responses mature into severe breathing problem, and eventually COPD disease pathology sets in. The exact and specific roles of individual TRP channels in specific disease conditions are still largely unknown.
2 TRP Channel-Mediated Chemosensation and Associated Responses
Trigeminal chemosensory nerve endings located in the nasal mucosa is the first line of defense in combating exposure of toxic chemical-induced pathological events in the airway [21]. Release of calcitonin gene-related peptide (CGRP), neurokinin A (NKA) and tachykinins substance P (SP) occurs from the nerve ending because of chemical stimulation. The associated downstream signaling events include neurogenic inflammatory vasodilation and leakage, leading to constriction and obstruction of the nasal passage [22, 23].
Oxidative stress and other noxious chemical compounds activate unmyelinated bronchopulmonary C-fibers and initiate action potentials that conduct centrally to evoke unpleasant sensations (e.g. coughing, dyspnea and chest tightness) and to stimulate/modulate reflexes (e.g. cough, bronchoconstriction, respiratory rate and inspiratory drive) [24].
Key components of this pathological event are highly sensitive to regulation of intracellular calcium concentration ([Ca2+]i) and play a significant role in nociception and other exogenous stimuli-induced responses. This finding actually emphasizes the importance of cellular calcium mobilization and calcium-mediated signal transduction. As COPD pathology is usually associated with cellular signaling mechanisms initiated by an increase of [Ca2+]i as a result of cellular calcium influx, TRP channels draw wide attention due to its cation selective gating properties with a focused interest of calcium influx, specifically through these channels [25].
Localization of different subtypes of TRP channels was confirmed in the epithelium and smooth muscle of the lung tissue. Cigarette smoke, industrial pollutants, aldehyde, chlorine and fragrances are the known activators of TRP channels in the human lung epithelium and in the airways. During signal transduction event, calcium is released into the cytoplasm from endoplasmic reticulum (ER), and the immediate effect is store-operated calcium entry through store-operated calcium influx channels, including TRP channels [18]. TRP channels are mostly plasma membrane (PM)-bound (except nuclear membrane and mitochondrial membrane) and selectively allow influx of cations including of Ca2+, Mg2+ and trace metal ions [26].
One of the important mechanisms of cellular calcium influx happens through Store-Operated Calcium Entry (SOCE) [27]. ER calcium store is usually replenished by such a mechanism in a faster way after store depletion. Stromal Interaction Molecule 1 (STIM1) with PM localization has been discovered as critical communicating protein that controls SOCE [28] when the store becomes empty. Immediately after STIM1 discovery, ER Ca2+ sensor Orai1 has been identified as the pore-forming subunit of the Ca2+ release-activated Ca2+ (CRAC) channels [29,30,31]. STIM1 mediated activation of SOC channels require Orai and TRPC1 interaction [32,33,34,35,36,37,38,39,40]. The role of STIM1 and Orai1 variants in SOCE has been reviewed extensively in Ref. [41].
3 Oxidative Damage and COPD
COPD pathogenesis mainly happens due to oxidative stress in the lung tissue. Exposure of lung to inhaled exogenous oxidants along with endogenously produced oxidative stress in the lung due to ageing and various metabolic processes creates significant oxidative damage. Oxidant and COPD-associated pathology includes but not limited to cell membrane damage due to destruction of membrane lipid bilayer, proteins and nucleic acids [42].
Cigarette smoke (CS) has long been identified as a major cause of COPD due to oxidative stress produced in the lower airways [43]. CS-induced damage to the lung tissue and the development of COPD depends on the extent of inhaled cigarette smoke exposure. Hydroxyl radical (OH−.) in the inhaled CS causes lipid peroxidation of the cell membrane proteins. OH−., upon reacting with unsaturated fatty acids of the membrane phospholipid, generates organic acid free radicals and causes membrane damage [44]. The secondary metabolite formed due to rapid degradation of the unstable intermediate oxidant molecules causes further lipid peroxidation. The intermediate oxidants molecules include alkanes (e.g. ethane/pentane) and aldehydes (e.g. malondialdehyde). The concentration of thiobarbituric acid reactive substance (TBARS) has been found in higher quantities in smoker lungs with COPD [45].
Non smoking-associated COPD development and progression of the disease has been linked to several factors. Deficiency of α1 antitrypsin, presence of chronic asthma, ROS-exposure due to polluted air, biomass smoke (BS) exposure, etc. has been found to be the major cause of nonsmoking-associated COPD [45].
Smoker lungs have been shown to have elevated high granular density alveolar macrophages, which has been identified as a major contributor for increased ROS production [46, 47]. The deadly association among H2O2, O2−. and OH−. radicals results in bronchial hyper responsiveness in COPD patients [48].
Endogenous cell-derived ROS produced in metabolically active cells is a result of enzymatic reactions involving a group of oxidant enzymes. Three main members of such an oxidant enzymes are NADPH oxidase, eosinophil peroxidase (EPO) and myeloperoxidase (MPO) [49]. Mitochondria are the source of reactive nitrogen species (RNS), O2−. and H2O2 production [50, 51]. Sources of exogenously produced ROS are CS [52] and the lipid peroxidation in inflammation of airway epithelium due to environmental ozone exposure [53].
4 TRP Channels and COPD
Increased TRPC6 mRNA expression in human alveolar and lung tissue macrophages has been reported in COPD patients [54]. The pathophysiological roles of non-neuronal TRPV1/TRPA1 channels have been widely studied in infection, inflammation and immunity. The sensory input of non-neuronal TRP channel mediated signal transduction mechanisms ultimately results indirect neurogenic pain or inflammation.
TRPV1/TRPA1 activation has been positively correlated with airway neurogenic inflammation. Non-neurogenic inflammatory responses produced by non-neuronal TRPA1 results inflammatory airway diseases. Thus TRPA1 has been identified as a prominent target to treat inflammatory respiratory diseases [55]. TRP channels are also involved as active removal mechanisms of foreign toxic substances in the cell. TRPV1/TRPA1 isoforms are widely expressed in lung sensory neurons, and those specific TRP channel activation causes alteration in vagal output associated with change in respiratory pattern, blood flow and coughing behavior.
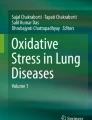
TRPV2/TRPV4 expressed in the alveolar macrophages play critical roles in immune response initiation [56]. Contribution of different TRP channel family members in relation to COPD development is summarized in Fig. 10.1.

Summary of different TRP channels expressed in lung tissues and the exogenous toxic agents they sense and respond. Respective membrane topology, functional domain and proposed binding sites with respect to the modulators of individual TRP channels are depicted in this figure. 4α-PDD 4α -Phorbol 12,13-didecanoate, 5,6 EET 5,6-Epoxy-eicosatrienoic acid, AA arachidonic acid, A Ankyrin repeat, AITC allyl isothiocyanate, ADPR ADP-ribose, cADPr cyclic ADP-ribose, CaM calmodulin binding site, CIRB calmodulin-IP3-receptor-binding site, CIRPIB calmodulin-IP3-receptor-phospho-inositide-bindingsite, RTX Resinferatoxine, TRP TRP box, Nudix nudix box, P pore, S1–6 transmembrane segment 1–6, TRP box, PDZ, PSD95/SAP90-Discs-large-Zonula-occludentes-1 domain. (Taken from Ref. [151] with permission)
4.1 TRPC6
TRPC6 and TRPC7 both gene expression has been detected in lung tissue [57]. TRPC6 being predominantly expressed in macrophages, lymphocytes and neutrophils [12] and also in the airway epithelium became a target gene for inflammation-induced lung diseases.
Increased TRPC6 gene expression has been reported in macrophages isolated from COPD patients [54]. In COPD patients phospholipase C (PLC), one of the important modulators of TRPC channels including TRPC6, has been found to be activated [58] as a result of CXC chemokine receptor activation. Thus TRPC6 activation and CXC chemokine receptor activation-mediated inflammation in COPD has been emerging as an interesting area of research.
4.2 TRPC4
Expression of TRPC proteins has been reported in endothelial cells, vascular smooth muscle cells and mast cells [59]. Discovery of TRPC4 knock out (KO) mouse model [60] opened up the possibility of detailed study for the role of TRPC4 in lung diseases and in COPD. Vascular endothelial cells of lungs in TRPC4 KO mice have a defective Ca2+ influx mechanism which has been found to be induced by thrombin [61]. Investing future research effort on TRPC4 in context to COPD and respiratory diseases certainly has potential to shed lights on COPD disease pathology.
4.3 TRPM2
Recently TRPM2 channel has been described as an oxidant sensor [62]. TNF-α and lipopolysaccharides (LPS) are two known potent activators of TRPM2 channels [63]. TRPM2 channel is largely expressed in inflammatory cells, including endogenous ROS-producing cells. Primary human monocytes have been shown to cause TRPM2 mRNA upregulation upon LPS or TNFα challenge [63]. Targeted gene knockdown studies of TRPM2 employing specific siRNA have been shown to reduce TNF-α, IL-6, IL-10 and [Ca2+]i rise upon LPS exposure [63].
Direct activation of TRPM2 and IL-8 production by H2O2 and subsequent cellular calcium influx have been shown in human monocyte cell line [64]. TRPM2 has been identified as an important target in oxidative damage-induced cellular inflammatory processes. The involvement of TRPM2 channel-mediated oxidative stress-induced cellular inflammatory processes has been tested in TRPM2−/− mice compared to WT counterparts [65, 66]. Further research on monocytes isolated from TRPM2−/− mice has shown reduced Ca2+ influx and reduced macrophage inflammatory protein-2α (MIP-2α or CXCL-2α) production in response to oxidative stress compared to WT mice [67].
Research from Heiner group [68] has shown involvement of TRPM2 in the neutrophil chemotaxis in human. Yamammoto group [64] also has provided the evidence for the existence of similar TRPM2-mediated mechanisms in experimental mice model. All those immune cell-induced cellular inflammatory pathways have been so far characterized in the COPD disease state.
4.4 TRPM8
Expression of TRP channels has been confirmed in vagal afferent neurons. Cold and menthol, a TRPM8 ligand, both have been reported as TRPM8 activators [69]. So-called thermoreceptor sensory function of TRPM8 channels operating at non-physiological low temperature zone has not proved to be of beyond doubt. Cold air is known to cause airway constriction, mucus secretion, cough and plasma protein infiltration which is characteristic to processes associated with inflammatory airway diseases [70, 71]. COPD being one of the well-characterized inflammatory airway diseases certainly draws attention with a possible linkage between TRPM8 pathology and the disease presentation. Presence of a functional variant of TRPM8 protein in human epithelial cell has recently been reported that promotes ER calcium release and subsequent increase in inflammatory cytokine transcription [72, 73].
Consistent with this notion of the presence of oxidant and TRM8-mediated mechanisms in COPD has been further supported by the fact that menthol cigarette smokers in COPD patients had shown severe airway inflammation compared to non-menthol smokers with COPD individuals [74]. In the same study employing in vitro model, the degree of ROS production has been compared between non-menthol cigarette smoke extract (Non-M-CSE) and menthol cigarette smoke extract (M-CSE) groups. Initially similar degree of increased extracellular ROS production has been reported in both groups. However, M-CSE group eventually produced a robust cytoplasmic calcium elevation, MAP Kinase (MAPK) activation, NF-κB signaling and release of IL-8. N-acetyl-cysteine (NAC), a ROS scavenger, was able to block the ROS-induced responses in both CSE treatment groups.
Additionally EGTA (an extracellular Ca2+ chelator) and AMTB (a TRPM8 antagonist), or both were able to completely inhibit both CSE-induced responses. Those findings strongly indicate a functional role of TRPM8 channel in oxidant-induced airway inflammation and possibility of TRPM8 being a therapeutic target to treat COPD. When menthol has been introduced into the Non-M-CSE groups, the rise in cytoplasmic calcium and release of IL-8 had been significantly increased compared to the Non-M-CSE only group. The involvement of TRPM8 in oxidative stress-induced inflammatory responses in smokers has been supported by employing either TRPM8 knocked down cells or TRPM8 knock out animal models [75].
4.5 TRPA1
Involvement of TRPA1 channel has been proved beyond doubt as major signaling mechanisms in COPD disease pathology [76]. Cigarette smoke extract (CSE), acrolein and crotonaldehyde have been shown to produce contraction of bronchial rings in guinea pigs which has been shown to be prevented by pretreatment with HC-030031, a specific TRPA1 antagonist and not by capsazepine, a TRPV1 antagonist or reactive oxygen scavengers [77].
Covalent modification of the N-terminus cysteine residues of TRPA1 by prostaglandins is one of the well-studied mechanisms of the channel activation [78, 79]. Another important activation mechanism is the lipid peroxidation, a mediator of cigarette smoke-induced inflammation [80, 81]. TRPA1 agonist-induced tussive responses in preclinical guinea pig model were found to be inhibited by HC-030031 [82]. Considering COPD disease etiology, the involvement of TRPA1s role in neurogenic inflammation is not well established. Recent evidence also suggests the involvement of TRPA1 in the non-neurogenic inflammatory pathways in experimental mice model [55].
TRPA1-induced neurogenic inflammation is usually associated with COPD [77]. Studies on preclinical animal models have provided evidence that TRPA1 channels play a significant role in cigarette smoke-induced bronchial inflammation [77]. Cigarette smoke is a complex mixture of several irritants known for potentially activating TRPA1 channel. Acrolein and crotonaldehyde [77, 83,84,85,86], along with nicotine [87] present in cigarette smoke, have been identified as direct TRPA1 activators. Biomass smoke (BM), mainly produced by burning wood, has been recently identified as activator of TRPA1-induced chemosensation in cultured jugular ganglia isolated from guinea pig [88]. Primary cultures of human airway fibroblasts, smooth muscle cells and epithelial cells have been reported to release IL-8 upon cigarette smoke-induced TRPA1 stimulation [55].
4.6 TRPV1
Neuronal TRPV1 channels are mostly expressed in C- and Aδ- fibers of primary sensory neurons. This channel has been widely described as nociceptors. TRPV1 channels are major intra and intercellular communication channels of the respiratory tract covering nose, alveoli, smooth muscle and blood vessel [13, 89].
Present TRPV1 research in relation to COPD is revolving in the areas of TRPV1’s role in sensory nerves and, especially, in tussive response associated with COPD [90, 91]. Involvement of neuronal TRPV1 responses in COPD pathology in human is still questionable while the role of non-neuronal TRPV1-response is becoming more evident in recent years [92].
Heat, protons, voltage, endogenous chemicals (including lipoxygenase products) and exogenous chemicals (including capsaicin and resiniferatoxin) are the known activators of TRPV1 [57]. Protein kinase A (PKA), protein kinase C (PKC) and other kinase-induced direct phosphorylation also activate TRPV1 channel [93, 94]. Phospholipase C (PLC) also has been shown as a TRPV1 mediator [95]. TRPV1-induced release of TNF-α and downstream proinflammatory response in sensory neurons has been reported [96]. Elevated levels of endogenous TRPV1 activators such as arachidonic acid metabolites involved in PKA, PKC and PLC pathways have been found in the lungs of COPD patients.
Low pH, a known TRPV1 activator, has been found in the exhaled breath condensate of COPD sufferers [97]. Hypersensitive tussive response upon capsaicin inhalation has been noted in COPD patients, an indicator of TRPV1 signaling mechanisms [98]. In experimental rat model, hypersensitivity of capsaicin-induced airway inflammation responses in pulmonary myelinated primary afferents was reported [99]. A systematic meta-analysis also suggests a strong correlation of TRPV1 in COPD disease pathology [100].
Apoptosis caused by inhaled airborne particulate material has been found to be completely inhibited by capsazepine in human airway epithelial cells and in TRPV1−/− mice [101]. Parallel studies also reported TRPV1 agonist-induced ER stress and loss of cell viability in BEAS-2B and A549 airway epithelial cell lines [102]. TRPV1 stimulation also caused release of IL-6, a proinflammatory cytokine from airway bronchial epithelial cells [103]. These evidences strongly support the role of non-neurogenic TRPV1 responses in COPD. Back in 1984, it has been reported that capsaicin treatment-induced ablation of TRPV1 in neonatal rats were resistant to cigarette smoke (CS)-induced increase in vascular permeability in the airways. In recent years, TRPV1 homozygous KO (TRPV1−/−) mice were found to be resistant to LPS-induced inflammation and bronchial hyperactivity, and that pretreatment with TRPV1 agonist SA13353 failed to produce both neutrophil influx and increase in cytokines TNFα and CXCL1 [104].
Tiotropium, a widely prescribed drug for COPD treatment as bronchodilator opened up the initial idea about possible linkage of TRPV1 in COPD disease pathology [105]. Tiotropium was found to inhibit capsaicin, a potent TRPV1 agonist-induced cough (Tussive stimulation) and single C-fiber firing in the guinea pig model [105] and in other preclinical studies [106].
Both TRPV1 and TRPV4 mRNA have been found to be upregulated in patients with COPD and were shown to be involved in CS-induced elevated ATP release in the COPD airways [107].
4.7 TRPV4
Known functions of TRPV4 channels include epithelial cell volume control, epithelial and endothelial permeability, bronchial smooth muscle contraction and participation in autoregulation of mucociliary transport. Those functions of TRPV4 appear important for the regulation of COPD pathogenesis, and thus TRPV4 emerges as a candidate gene for COPD. TRPV4 is widely expressed in heart, lung, kidney, CNS and skin [108]. In the lungs the highest levels of TRPV4 expression have been found in the epithelial linings of the trachea, bronchi and lower airways and the alveolar septal walls [109, 110].
TRPV1 and TRPV4 both channels are thermo- and osmo-sensitive [111]. TRPV1 has been emerging as a hyperosmotic sensor and TRPV4 as hypoosmotic [112] and mechanical sensor [113]. TRPV4 also senses and responds to chemical stimuli including, 4α-phorbol 12, 13-didecanoate (4α PDD) [111], GSK1016790A [110] and 5′, 6′-epoxyeicosatrienoic acid (EET) [114]. TRPV4 is important in controlling epithelial and endothelial barrier function, especially in response to increased vascular pressure and stretch. TRPV4 channel activation has been implicated in cellular ATP release mechanisms and subsequent downstream purinergic signaling pathways. It is important to note that increased levels of ATP have been found in bronchoalveolar lavage fluid (BALF) from COPD patients [115]. Recently association of small nuclear polymorphisms (SNPs) in TRPV4 in relation to COPD disease pathology has been confirmed [25].
5 ROS and RNS: Potential Activators for the TRP Channels
Infiltrating neutrophils, eosinophils and macrophages into the lung alveolar space significantly increases the pulmonary oxidant burden by generating ROS including O2−., H2O2 and hypochlorite. The NO produced by the inflamed tissue occasionally reacts with ROS and results in more damaging reactive nitrogen species (RNS) including peroxynitrite (ONOO−) and nitrogen dioxide (NO2). RNS cause additional nitrative stress in airway diseases [116].
TRPV1 and TRPA1 both have been identified as a potential target for ROS/RNS-mediated cellular calcium signaling processes in both chronic and acute responses to oxidative stress into the lung. ROS-mediated activation of different TRP channels expressed in airway epithelial cells and in sensory nerves towards neurogenic inflammation is schematically shown in Fig. 10.2.

Schematic diagram showing the ROS-induced activation and signal transduction events of TRP channels expressed in sensory nerves and in airway epithelial cells. ROS-induced TRP channel activation following release of proinflammatory mediators leads to the neurogenic inflammation. PGE2 Prostaglandin E2, NGF nerve growth factor, and TNF-α tumor necrosis factor-α. (Taken from Ref. [152])
RNS damages the membrane integrity by directly attacking the unsaturated fatty acids (e.g. oleic acid) of the cell membrane and generates highly reactive nitro-oleic acid [117]. Oxidative stress can directly activate TRPA1 channels by oxidizing cysteine residue of the cytoplasmic N Terminal [118]. TRPA1 channels are found to respond to both the electrophiles and the oxidizing agents entering in the airways. 3-Niro-tyrosine (3-NT), with high biological activity, is one of the several RNS generated by the reaction between RNS and NO and has potential to be used as a marker for NOO−-mediated cellular damages in vivo. Reactive lipid aldehydes are usually formed by an autocatalytic pathway in lipid peroxidation of the cell membrane.
6 Biomass Smoke and TRP Channel Activation
The correlation between COPD and biomass smoke (BS) exposure is now well established. At present there is around 3 billion COPD sufferer worldwide. Burning biomass fuel such as wood and coke is common in developing countries as a cheap alternative to the conventional source of energies including electricity and gas. Burning of these materials releases several air pollutants in large quantities that includes nitrogen oxides, sulphur oxides, hydrogen chloride, polyaromatic hydrocarbons, volatile organic compounds, methane, furans, dioxins and aerosol particulates of both organic and inorganic origin [119]. In COPD patients, inhaled BS has been identified as a major contributing factor towards developing inflammatory responses. The late responses of such inflammatory processes result in tissue proliferation in small airways and severe tissue damage in lung parenchyma. Additionally, the disease state contains recruitment of immune cells to the airway compartments [120].
7 Diesel Exhausts Particle and TRP Channel Activation
Diesel exhausts particle (DEP) is a very common component in the city environment generated by the automobiles. DEP inhalation has been widely implicated in developing COPD and chronic asthma worldwide. The role of DEP as a direct activator of lung-specific afferent sensory nerves in relation to initiation of respiratory symptoms has been studied. The study on the effect of organic extract of diesel exhaust (DEP-OE) on human and in vitro studies and in vivo electrophysiological studies has identified a list of compounds causing TRPA1 activation. DEPs contain high amount of polyaromatic hydrocarbons (PAHs) on their surface and exert toxic and carcinogenic effects. Phenanthrene, a common PAH found in DEP has been found to cause depolarization of vagus nerve [121]. DEP exposure in human primary airway epithelia has been reported to reduce ciliary beat frequency and results in increased oxidative damage, NF-κB pathway activation and increased secretion of proinflammatory cytokines. Some of the secreted immune-responsive biomolecules also act as mediators and sensitize airway sensory neurons [122,123,124,125,126,127,128,129,130]. Signal transduction pathways specifically responsible for such a DEP-evoked events are not fully understood.
Electrophiles activate TRPA1 channels and involve covalent modification of the cysteine residues on the N-terminus (Cytoplasmic domain) [131, 132]. This finding possibly provides clues why endogenously produced oxidative stress causes TRPA1 activation as an integral event in intracellular oxidative stress [118, 133]. Robinson et al. [121] have shown that H2O2 or DEP-OE depolarizes the vagus nerve in a TRPA1-dependent manner [134, 135], and this response was inhibited by the antioxidant N-acetyl cysteine (NAC).
8 Genetic Contributors of COPD
Finding key genetic contributor for the chronic diseases has been a challenge for the investigators and COPD is no exception. Earlier studies [136, 137] have shown evidence that genetic factors are linked to pulmonary function and COPD. Existence of familial aggregation of COPD strongly suggests this notion [136]. Till date, it is not very clear how genetic factors are associated for COPD development and progression. Environmental pollutants have been shown to produce adverse reactions to the bronchial epithelium and recruit inflammatory cells causing pulmonary disease pathology [138]. Association of COPD with polymorphisms of genes like α1-antitrypsin, TNFα and surfactant protein B genes has been suggested in case control studies [139,140,141]. A study on Indian population exposed to industrial pollutants has shown evidence that microsatellite (MSI) instability is weakly associated with smoker’s age and the extent of exposure to exogenous toxins, which are the known cause for developing COPD [142].
α1-antitrypsin deficiency has been previously positively correlated with COPD development in young adults [143]. Phosphorylated serine 19 residue in TRPV4 protein, a human genetic polymorphism, has been previously documented as COPD susceptibility locus. This specific polymorphism has been directly linked to matrix metalloproteinase (MMP1) activation associated with increased calcium influx and downstream signaling pathways [25, 144, 145].
9 Modulators of TRP Channel Expression and Function
Significant development took place in recent years in order to find both competitive and non-competitive inhibitors for the TRP channels in order to control disease states including asthma, COPD and several other airway diseases. The development of TRP antagonists happened slowly, but in recent years, there has been a wide interest in developing TRPV1 and TRPA1 antagonists because of their potential therapeutic role in targeting neuropathic pain. Ruthenium red (RR), a non-selective calcium channel blocker, blocks several TRP channels including TRPV1. Unfavorable cytotoxicity prevented this potent molecule to be considered as potential candidate for further drug development perspective. In recent years (±) camphor has been identified as week TRPA1 antagonist [146, 147]. SB-705498, a potent TRPV1 antagonist developed by GSK cleared its Phase 1 clinical trial in 2007. SB-705498 has shown promise for further clinical trials as it has been shown to be well tolerated in Phase 1 clinical trial with no serious adverse effects. Topical applications of SB-705498 have also been tested in two Phase 2 clinical trials in relation to chronic cough and non-allergic rhinitis [148].
Competitive TRP channel antagonists are therapeutically attractive because of their direct mode of action without upregulating or activating the receptors for the respective channels and usually do not associate with unwanted drug use-related side effects [149]. So far TRPA1 and TRPV1 both appear to be potential target of therapeutic intervention in order to treat respiratory airway diseases including COPD [150].
10 Conclusions and Future Directions
TRP channels have now gained wide interest because they have been documented as sensors for environmental stimuli that can sense and respond to exogenous stimuli. The multifunctional roles played by different TRP channels are important in terms of understanding how the cellular sensors work to respond to exogenous stimuli in normal and pathophysiological conditions and how these channels are linked to the mechanisms of disease progression.
A wide variety of exogenous and endogenous stimuli-induced activations of different TRP channels play a significant role in COPD development and progression. Targeting TRP channels has enormous potential in treating pulmonary diseases including COPD. TRP channels appear to be a family of endogenous defense system to combat noxious stimuli-induced cellular damages and play critical immunological roles in many lung diseases including COPD. Rise in cytoplasmic calcium through TRP channel and subsequent cellular signaling pathways that lead to hyperactivated proinflammatory and immunological responses including activation of different transcription factors, chromatin remodeling and altered gene expression have potential to shed lights on the mechanisms of the COPD for future drug development to combat the disease. Identification of specific TRP genes responsible for COPD will provide further knowledge about how a specific population of chronic COPD is predisposed to the disease and what genetic manipulation and pharmacological intervention could be done in order to prevent or slow down the disease progression.
Abbreviations
- [Ca2+]i:
-
Intracellular calcium
- 4αPDD:
-
4α-phorbol 12, 13-didecanoate
- BS:
-
Biomass smoke
- CGRP:
-
Calcitonin gene-related peptide
- CNS:
-
Central nervous system
- COPD:
-
Chronic obstructive pulmonary diseases
- CRAC:
-
Ca2+ release-activated Ca2+ (CRAC) channels
- CS:
-
Cigarette smoke
- EET:
-
5′, 6′-epoxyeicosatrienoic acid (EET)
- EGTA:
-
Ethylene gycol-bis (β-aminoethyl ether)-N,N,N′,N′-tetraacetic acid
- ER:
-
Endoplasmic reticulum
- GST:
-
Glutathione-S-transferase
- NKA:
-
Neurokonin A
- PM:
-
Plasma membrane
- SNPs:
-
Small nuclear polymorphisms
- SOD:
-
Superoxide dismutase
- SP:
-
Tachykinins substance P
- STIM:
-
Stromal Interaction Molecule
- TRP channels:
-
Transient receptor potential channels
References
Decramer M, Janssens W, Miravitlles M (2012) Chronic obstructive pulmonary disease. Lancet 379:1341–1351
Bateman ED, Hurd SS, Barnes PJ et al (2008) Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J 31:143
Cosio Piqueras MG, Cosio MG (2001) Disease of the airways in chronic obstructive pulmonary disease. Eur Respir J 18:41s–49s
Culver B (2015) Defining airflow limitation and chronic obstructive pulmonary disease: the role of outcome studies. Eur Respir J 46:8–10
William LE (2016) Defining airflow obstruction. Chron Obstruct Pulmon Dis 3:515–518
Barnes PJ (2013) Corticosteroid resistance in patients with asthma and chronic obstructive pulmonary disease. J Allergy Clin Immunol 131:636–645
Calverley PMA, Anderson JA, Celli B et al (2007) Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 356:775–789
Barnes PJ (2017) Cellular and molecular mechanisms of asthma and COPD. Clin Sci 131:1541–1558
Eapen MS, Myers S, Walters EH et al (2017) Airway inflammation in chronic obstructive pulmonary disease (COPD): a true paradox. Expert Rev Respir Med 11:827–839
Bose P, Bathri R, Kumar L et al (2015) Role of oxidative stress & transient receptor potential in chronic obstructive pulmonary disease. Indian J Med Res 142:245–260
Vijayan V (2013) Chronic obstructive pulmonary disease. Indian J Med Res 137:251–269
Banner KH, Igney F, Poll C (2011) TRP channels: emerging targets for respiratory disease. Pharmacol Ther 130:371–384
Grace MS, Baxter M, Dubuis E et al (2014) Transient receptor potential (TRP) channels in the airway: role in airway disease. Br J Pharmacol 171:2593–2607
Preti D, Szallasi A, Patacchini R (2012) TRP channels as therapeutic targets in airway disorders: a patent review. Expert Opin Ther Pat 22:663–695
Katharine A-B, Christopher P, Verkuyl JM (2013) Targeting TRP channels in airway disorders. Curr Top Med Chem 13:310–321
Ru X, Yao X (2014) TRPM2: a multifunctional ion channel for oxidative stress sensing. Acta Phys Sin 66:7–15
Nazıroğlu M, Zgülbilal CÖ, Doğan Ç et al (2011) Glutathione modulates Ca2+ influx and oxidative toxicity through TRPM2 channel in rat dorsal root ganglion neurons. J Membr Biol 242:109
Bessac BF, Jordt S-E (2010) Sensory detection and responses to toxic gases: mechanisms, health effects, and countermeasures. Proc Am Thorac Soc 7:269–277
Jindal S, Aggarwal A, Chaudhry K et al (2006) Tobacco smoking in India: prevalence, quit-rates and respiratory morbidity. Indian J Chest Dis Allied Sci 48:37–42
Mach WJ, Thimmesch AR, Pierce JT et al (2011) Consequences of hyperoxia and the toxicity of oxygen in the lung. Nurs Res Pract 2011:260482
Baraniuk JN, Kim D (2007) Nasonasal reflexes, the nasal cycle, and sneeze. Curr Allergy Asthma Rep 7:105–111
Baraniuk JN, Lundgren JD, Goff J et al (1990) Calcitonin gene-related peptide in human nasal mucosa. Am J Phys Lung Cell Mol Phys 258:L81–L88
Petersson G, Malm L, Ekman R et al (1989) Capsaicin evokes secretion of nasal fluid and depletes substance P and calcitonin gene-related peptide from the nasal mucosa in the rat. Br J Pharmacol 98:930–936
Taylor-Clark TE, Undem BJ (2011) Sensing pulmonary oxidative stress by lung vagal afferents. Respir Physiol Neurobiol 178:406–413
Zhu G, Investigators I, Gulsvik A et al (2009) Association of TRPV4 gene polymorphisms with chronic obstructive pulmonary disease. Hum Mol Genet 18:2053–2062
Alarie Y, Ferguson JS, Stock MF et al (1987) Sensory and pulmonary irritation of methyl isocyanate in mice and pulmonary irritation and possible cyanide like effects of methyl isocyanate in guinea pigs. Environ Health Perspect 72:159–167
Putney JW (1986) A model for receptor-regulated calcium entry. Cell Calcium 7:1–12
Oritani K, Kincade PW (1996) Identification of stromal cell products that interact with pre-B cells. J Cell Biol 134:771
Feske S, Prakriya M, Rao A et al (2005) A severe defect in CRAC Ca2+ channel activation and altered K+ channel gating in T cells from immunodeficient patients. J Exp Med 202:651
Mercer JC, DeHaven WI, Smyth JT et al (2006) Large store-operated calcium selective currents due to co-expression of Orai1 or Orai2 with the intracellular calcium sensor, Stim1. J Biol Chem 281:24979–24990
Prakriya M, Lewis RS (2015) Store-operated calcium channels. Physiol Rev 95:1383–1436
Cheng KT, Ong HL, Liu X et al (2011) Contribution of TRPC1 and Orai1 to Ca2+ entry activated by store depletion. In: Islam MS (ed) Transient receptor potential channels. Springer, Dordrecht, pp 435–449
Cheng KT, Ong HL, Liu X et al (2013) Chapter seven – contribution and regulation of TRPC channels in store-operated Ca2+ entry. In: Prakriya M (ed) Current topics in membranes. Academic, San Diego, pp 149–179
Desai PN, Zhang X, Wu S et al (2015) Multiple types of calcium channels arising from alternative translation initiation of the Orai1 message. Sci Signal 8:ra74
Huang GN, Zeng W, Kim JY et al (2006) STIM1 carboxyl-terminus activates native SOC, Icrac and TRPC1 channels. Nat Cell Biol 8:1003
Jardin I, Lopez JJ, Salido GM et al (2008) Orai1 mediates the interaction between STIM1 and hTRPC1 and regulates the mode of activation of hTRPC1-forming Ca2+ channels. J Biol Chem 283:25296–25304
Rosado JA, Sage SO (2000) Coupling between inositol 1,4,5-trisphosphate receptors and human transient receptor potential channel 1 when intracellular Ca2+ stores are depleted. Biochem J 350:631–635
Singh BB, Liu X, Ambudkar IS (2000) Expression of truncated transient receptor potential protein 1α (Trp1α): evidence that the Trp1 C terminus modulates store-operated Ca2+ entry. J Biol Chem 275:36483–36486
Yuan JP, Zeng W, Huang GN et al (2007) STIM1 heteromultimerizes TRPC channels to determine their function as store-operated channels. Nat Cell Biol 9:636
Choi S, Maleth J, Jha A et al (2014) The TRPCs–STIM1–Orai interaction. In: Nilius B, Flockerzi V (eds) Mammalian transient receptor potential (TRP) cation channels: volume II. Springer, Cham, pp 1035–1054
Rosado JA, Diez R, Smani T et al (2015) STIM and Orai1 variants in store-operated calcium entry. Front Pharmacol 6:325
Valko M, Leibfritz D, Moncol J et al (2007) Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol 39:44–84
Kumar R, Vijayan VK (2012) Smoking cessation programs and other preventive strategies for chronic obstructive pulmonary disease. J Assoc Physicians Indian Suppl 60:54–56
Rahman I, Morrison D, Donaldson K et al (1996) Systemic oxidative stress in asthma, COPD, and smokers. Am J Respir Crit Care Med 154:1055–1060
Premanand R, Kumar S, Mohan A (2007) Study of thiobarbituric reactive substances and total reduced glutathione as indices of oxidative stress in chronic smokers with and without chronic obstructive pulmonary disease. Indian J Chest Dis Allied Sci 49:9–12
Schaberg T, Klein U, Rau M et al (1995) Subpopulations of alveolar macrophages in smokers and nonsmokers: relation to the expression of CD11/CD18 molecules and superoxide anion production. Am J Respir Crit Care Med 151:1551–1558
Drath DB, Karnovsky ML, Huber GL (1979) The effects of experimental exposure to tobacco smoke on the oxidative metabolism of alveolar macrophages. J Reticuloendothel Soc 25:597–604
Rahman I, Adcock IM (2006) Oxidative stress and redox regulation of lung inflammation in COPD. Eur Respir J 28:219
Hayashi Y, Sawa Y, Nishimura M et al (2004) Peroxynitrite, a product between nitric oxide and superoxide anion, plays a cytotoxic role in the development of post-bypass systemic inflammatory response. Eur J Cardiothorac Surg 26:276–280
Church DF, Pryor WA (1985) Free-radical chemistry of cigarette smoke and its toxicological implications. Environ Health Perspect 64:111–126
Hiltermann JTN, Lapperre TS, van Bree L et al (1999) Ozone-induced inflammation assessed in sputum and bronchial lavage fluid from asthmatics: a new noninvasive tool in epidemiologic studies on air pollution and asthma. Free Radic Biol Med 27:1448–1454
Nightingale JA, Rogers DF, Barnes PJ (1999) Effect of inhaled ozone on exhaled nitric oxide, pulmonary function, and induced sputum in normal and asthmatic subjects. Thorax 54:1061
Comhair SAA, Thomassen MJ, Erzurum SC (2000) Differential induction of extracellular glutathione peroxidase and nitric oxide synthase 2 in airways of healthy individuals exposed to 100% O2 or cigarette smoke. Am J Respir Cell Mol Biol 23:350–354
Finney-Hayward TK, Popa MO et al (2010) Expression of transient receptor potential C6 channels in human lung macrophages. Am J Respir Cell Mol Biol 43:296–304
Nassini R, Pedretti P, Moretto N et al (2012) Transient receptor potential Ankyrin 1 channel localized to non-neuronal airway cells promotes non-neurogenic inflammation. PLoS One 7:e42454
Earley S, Gonzales AL, Crnich R (2009) Endothelium-dependent cerebral artery dilation mediated by TRPA1 and Ca2+-activated K+ channels. Circ Res 104:987–994
Venkatachalam K, Montell C (2007) TRP channels. Annu Rev Biochem 76:387–417
Baggiolini M (2001) Chemokines in pathology and medicine. J Intern Med 250:91–104
Freichel M, Tsvilovskyy, Camacho-Londoño JE (2014) TRPC4- and TRPC4-containing channels. In: Nilius B, Flockerzi V (eds) Mammalian transient receptor potential (TRP) cation channels: volume I. Springer Berlin Heidelberg, Berlin/Heidelberg, pp 85–128
Freichel M, Suh SH, Pfeifer et al (2001) Lack of an endothelial store-operated Ca2+ current impairs agonist-dependent vasorelaxation in TRP4−/− mice. Nat Cell Biol 3:121
Tiruppathi C, Freichel M, Vogel SM et al (2002) Impairment of store-operated Ca2+ entry in TRPC4 (−/−) mice interferes with increase in lung microvascular permeability. Circ Res 91:70–76
Hara Y, Wakamori M, Ishii M, Maeno E, Nishida M, Yoshida T, Yamada H, Shimizu S, Mori E, Kudoh J, Shimizu N, Kurose H et al (2002) LTRPC2 Ca2+-permeable channel activated by changes in redox status confers susceptibility to cell death. Mol Cell 9:163–173
Wehrhahn J, Kraft R, Harteneck C et al (2010) Transient receptor potential melastatin 2 is required for lipopolysaccharide-induced cytokine production in human monocytes. J Immunol 184:2386
Yamamoto S, Shimizu S, Kiyonaka S et al (2008) TRPM2-mediated Ca2+ influx induces chemokine production in monocytes that aggravates inflammatory neutrophil infiltration. Nat Med 14:738
Araki Y, Sugihara H, Hattori T (2006) The free radical scavengers edaravone and tempol suppress experimental dextran sulfate sodium-induced colitis in mice. Int J Mol Med 17:331–334
Blackburn AC, Doe WF, Buffinton GD (1998) Salicylate hydroxylation as an indicator of hydroxyl radical generation in dextran sulfate-induced colitis. Free Radic Biol Med 25:305–313
Tsutsui M, Hirase R, Miyamura S et al (2018) TRPM2 exacerbates central nervous system inflammation in experimental autoimmune encephalomyelitis by increasing production of CXCL2 chemokines. J Neurosci 38:2203–2217
Heiner I, Radukina N, Eisfeld J et al (2005) Regulation of TRPM2 channels in neutrophil granulocytes by ADP-ribose: a promising pharmacological target. Naunyn Schmiedeberg’s Arch Pharmacol 371:325–333
Xing H, Ling JX, Chen M et al (2008) TRPM8 mechanism of autonomic nerve response to cold in respiratory airway. Mol Pain 4:1744-8069-4-22
Yoshihara S, Geppetti P, Hara M et al (1996) Cold air-induced bronchoconstriction is mediated by tachykinin and kinin release in guinea pigs. Eur J Pharmacol 296:291–296
Carlsen K-H, Carlsen KCL (2002) Exercise-induced asthma. Paediatr Respir Rev 3:154–160
Sabnis AS, Reilly CA, Veranth JM et al (2008) Increased transcription of cytokine genes in human lung epithelial cells through activation of a TRPM8 variant by cold temperatures. Am J Phys Lung Cell Mol Phys 295:L194–L200
Sabnis AS, Shadid M, Yost GS et al (2008) Human lung epithelial cells express a functional cold-sensing TRPM8 variant. Am J Respir Cell Mol Biol 39:466–474
Lin A-H, Liu M-H, Ko H-KB et al (2017) Inflammatory effects of menthol vs. non-menthol cigarette smoke extract on human lung epithelial cells: a double-hit on TRPM8 by reactive oxygen species and menthol. Front Physiol 8:263
Lamb JG, Romero EG, Lu Z et al (2017) Activation of human transient receptor potential melastatin-8 (TRPM8) by calcium-rich particulate materials and effects on human lung cells. Mol Pharmacol 92:653–664
Mukhopadhyay I, Kulkarni A, Khairatkar-Joshi N (2016) Blocking TRPA1 in respiratory disorders: does it hold a promise? Pharmaceuticals 9:70
Andrè E, Campi B, Materazzi S et al (2008) Cigarette smoke–induced neurogenic inflammation is mediated by α,β-unsaturated aldehydes and the TRPA1 receptor in rodents. J Clin Invest 118:2574–2582
Grace M, Birrell MA, Dubuis E et al (2012) Transient receptor potential channels mediate the tussive response to prostaglandin E2 and bradykinin. Thorax 67:891
Takahashi N, Mizuno Y, Kozai D et al (2008) Molecular characterization of TRPA1 channel activation by cysteine-reactive inflammatory mediators. Channels 2:287–298
Macpherson LJ, Dubin AE, Evans MJ et al (2007) Noxious compounds activate TRPA1 ion channels through covalent modification of cysteines. Nature 445:541–545
Trevisani M, Siemens J, Materazzi S (2007) 4-Hydroxynonenal, an endogenous aldehyde, causes pain and neurogenic inflammation through activation of the irritant receptor TRPA1. Proc Natl Acad Sci 104:13519
Birrell MA, Belvisi MG, Grace M et al (2009) TRPA1 agonists evoke coughing in guinea pig and human volunteers. Am J Respir Crit Care Med 180:1042–1047
Bautista DM, Jordt S-E, Nikai T et al (2006) TRPA1 mediates the inflammatory actions of environmental irritants and proalgesic agents. Cell 124:1269–1282
Facchinetti F, Amadei F, Geppetti P et al (2007) α,β-unsaturated aldehydes in cigarette smoke release inflammatory mediators from human macrophages. Am J Respir Cell Mol Biol 37:617–623
Andrè E, Gatti R, Trevisani M et al (2009) Transient receptor potential ankyrin receptor 1 is a novel target for pro-tussive agents. Br J Pharmacol 158:1621–1628
Lin YS, Hsu C-C, Bien M-Y et al (2010) Activations of TRPA1 and P2X receptors are important in ROS-mediated stimulation of capsaicin-sensitive lung vagal afferents by cigarette smoke in rats. J Appl Physiol 108:1293–1303
Talavera K, Gees M, Karashima Y et al (2009) Nicotine activates the chemosensory cation channel TRPA1. Nat Neurosci 12:1293–1299
Shapiro D, Deering-Rice CE, Romero EG et al (2013) Activation of transient receptor potential ankyrin-1 (TRPA1) in lung cells by wood smoke particulate material. Chem Res Toxicol 26:750–758
Watanabe N, Horie S, Michael GJ et al (2006) Immunohistochemical co-localization of transient receptor potential vanilloid (TRPV)1 and sensory neuropeptides in the guinea-pig respiratory system. Neuroscience 141:1533–1543
Grace MS, Belvisi MG (2011) TRPA1 receptors in cough. Pulm Pharmacol Ther 24:286–288
Maher SA, Dubuis ED, Belvisi MG (2011) G-protein coupled receptors regulating cough. Curr Opin Pharmacol 11:248–253
Agopyan N, Bhatti T, Yu S et al (2003) Vanilloid receptor activation by 2- and 10-μm particles induces responses leading to apoptosis in human airway epithelial cells. Toxicol Appl Pharmacol 192:21–35
Premkumar LS, Ahern GP (2000) Induction of vanilloid receptor channel activity by protein kinase C. Nature 408:985
De Petrocellis L, Harrison S, Bisogno T et al (2001) The vanilloid receptor (VR1)-mediated effects of anandamide are potently enhanced by the cAMP-dependent protein kinase. J Neurochem 77:1660–1663
Rohacs T, Thyagarajan B, Lukacs V (2008) Phospholipase C mediated modulation of TRPV1 channels. Mol Neurobiol 37:153
Hu Y, Gu Q, Lin R-L et al (2010) Calcium transient evoked by TRPV1 activators is enhanced by tumor necrosis factor-α in rat pulmonary sensory neurons. Am J Phys Lung Cell Mol Phys 299:L483–L492
MacNee W, Rennard SI, Hunt JF et al (2011) Evaluation of exhaled breath condensate pH as a biomarker for COPD. Respir Med 105:1037–1045
Doherty MJ, Mister R, Pearson MG et al (2000) Capsaicin responsiveness and cough in asthma and chronic obstructive pulmonary disease. Thorax 55:643
Zhang G, Lin R-L, Wiggers M et al (2008) Altered expression of TRPV1 and sensitivity to capsaicin in pulmonary myelinated afferents following chronic airway inflammation in the rat. J Physiol 586:5771–5786
Zhang L, Chang WW, Ding H et al (2011) Transforming growth factor-β1 polymorphisms and chronic obstructive pulmonary disease: a meta-analysis. Int J Tuberc Lung Dis 15:1301–1307
Agopyan N, Head J, Yu S, Simon SA (2004) TRPV1 receptors mediate particulate matter-induced apoptosis. Am J Phys Lung Cell Mol Phys 286:L563–L572
Reilly CA, Taylor JL, Lanza DL et al (2003) Capsaicinoids cause inflammation and epithelial cell death through activation of vanilloid receptors. Toxicol Sci 73:170–181
Seki N, Shirasaki H, Kikuchi M et al (2007) Capsaicin induces the production of IL-6 in human upper respiratory epithelial cells. Life Sci 80:1592–1597
Tsuji F, Murai M, Oki K et al (2010) Effects of SA13353, a transient receptor potential vanilloid 1 agonist, on leukocyte infiltration in lipopolysaccharide-induced acute lung injury and ovalbumin-induced allergic airway inflammation. J Pharmacol Sci 112:487–490
Birrell MA, Bonvini SJ, Dubuis E et al (2014) Tiotropium modulates transient receptor potential V1 (TRPV1) in airway sensory nerves: a beneficial off-target effect. J Allergy Clin Immunol 133:679–687
Bateman ED, Rennard S, Barnes PJ et al (2009) Alternative mechanisms for tiotropium. Pulm Pharmacol Ther 22:533–542
Baxter M, Eltom S, Dekkak B et al (2014) Role of transient receptor potential and pannexin channels in cigarette smoke-triggered ATP release in the lung. Thorax 69:1080–1089
Yin J, Kuebler WM (2009) Mechanotransduction by TRP channels: general concepts and specific role in the vasculature. Cell Biochem Biophys 56:1–18
Alvarez DF, King JA, Weber D et al (2006) Transient receptor potential vanilloid 4-mediated disruption of the alveolar septal barrier. Circ Res 99:988–995
Willette RN, Bao W, Nerurkar S et al (2008) Systemic activation of the transient receptor potential vanilloid subtype 4 channel causes endothelial failure and circulatory collapse: part 2. J Pharmacol Exp Ther 326:443–452
Watanabe H, Vriens J, Suh SH et al (2002) Heat-evoked activation of TRPV4 channels in a HEK293 cell expression system and in native mouse aorta endothelial cells. J Biol Chem 277:47044–47051
Strotmann R, Harteneck C, Nunnenmacher K et al (2000) OTRPC4, a nonselective cation channel that confers sensitivity to extracellular osmolarity. Nat Cell Biol 2:695–702
Liedtke W, Choe Y, Martí-Renom MA et al (2000) Vanilloid receptor–related osmotically activated channel (VR-OAC), a candidate vertebrate osmoreceptor. Cell 103:525–535
Watanabe H, Vriens J, Prenen J et al (2003) Anandamide and arachidonic acid use epoxyeicosatrienoic acids to activate TRPV4 channels. Nature 424:434
Mortaz E, Braber S, Nazary M et al (2009) ATP in the pathogenesis of lung emphysema. Eur J Pharmacol 619:92–96
Jain K, Siddam A, Marathi A et al (2008) The mechanism of oleic acid nitration by NO2. Free Radic Biol Med 45:269–283
Andersson DA, Gentry C, Moss S et al (2008) Transient receptor potential A1 is a sensory receptor for multiple products of oxidative stress. J Neurosci 28:2485–2494
Bessac BF, Jordt S-E (2008) Breathtaking TRP channels: TRPA1 and TRPV1 in airway chemosensation and reflex control. Physiology 23:360–370
Williams A, Jones JM, Ma L, Pourkashanian M (2012) Pollutants from the combustion of solid biomass fuels. Prog Energy Combust Sci 38:113–137
Olloquequi J, Valero JG, Rodríguez E et al (2012) Lung CD57+ cell density is increased in very severe COPD. Histol Histopathol 27:39–47
Robinson RK, Birrell MA, Adcock JJ et al (2018) Mechanistic link between diesel exhaust particles and respiratory reflexes. J Allergy Clin Immunol 141:1074–1084
Bayram H, Devalia JL, Sapsford RJ et al (1998) The effect of diesel exhaust particles on cell function and release of inflammatory mediators from human bronchial epithelial cells in vitro. Am J Respir Cell Mol Biol 18:441–448
Bayram H, Ito K, Issa R et al (2006) Regulation of human lung epithelial cell numbers by diesel exhaust particles. Eur Respir J 27:705–713
Bonvallot V, Baeza-Squiban A, Baulig A et al (2001) Organic compounds from diesel exhaust particles elicit a proinflammatory response in human airway epithelial cells and induce cytochrome p450 1A1 expression. Am J Respir Cell Mol Biol 25:515–521
Daniel EE, O’byrne P (1991) Effect of inflammatory mediators on airway nerves and muscle. Am Rev Respir Dis 143:S3–S5
Li J, Ghio AJ, Cho S-H et al (2009) Diesel exhaust particles activate the matrix-metalloproteinase-1 gene in human bronchial epithelia in a β-arrestin–dependent manner via activation of RAS. Environ Health Perspect 117:400–409
Takizawa H, Abe S, Okazaki H et al (2003) Diesel exhaust particles upregulate eotaxin gene expression in human bronchial epithelial cells via nuclear factor-κB-dependent pathway. Am J Phys Lung Cell Mol Phys 284:L1055–L1062
Takizawa H, Ohtoshi T, Kawasaki S et al (1999) Diesel exhaust particles induce NF-κB activation in human bronchial epithelial cells in vitro: importance in cytokine transcription. J Immunol 162:4705–4711
Totlandsdal AI, Cassee FR, Schwarze P et al (2010) Diesel exhaust particles induce CYP1A1 and pro-inflammatory responses via differential pathways in human bronchial epithelial cells. Part Fibre Toxicol 7:41
Teles AM, Kumagai Y, Brain SD et al (2010) Involvement of sensory nerves and TRPV1 receptors in the rat airway inflammatory response to two environment pollutants: diesel exhaust particles (DEP) and 1,2-naphthoquinone (1,2-NQ). Arch Toxicol 84:109–117
Bessac BF, Sivula M, von Hehn CA et al (2008) TRPA1 is a major oxidant sensor in murine airway sensory neurons. J Clin Invest 118:1899–1910
Cvetkov TL, Huynh KW, Cohen MR et al (2011) Molecular architecture and subunit organization of TRPA1 ion channel revealed by electron microscopy. J Biol Chem 286:38168–38176
Liu T, Ji R-R (2012) Oxidative stress induces itch via activation of transient receptor potential subtype ankyrin 1 in mice. Neurosci Bull 28:145–154
Hadley SH, Bahia PK, Taylor-Clark TE (2014) Sensory nerve terminal mitochondrial dysfunction induces hyperexcitability in airway nociceptors via protein kinase C. Mol Pharmacol 85:839–848
Taylor-Clark TE (2015) Oxidative stress as activators of sensory nerves for cough. Pulm Pharmacol Ther 35:94–99
Li J, Kanju P, Patterson M et al (2011) TRPV4-mediated calcium influx into human bronchial epithelia upon exposure to diesel exhaust particles. Environ Health Perspect 119:784–793
Givelber RJ, Couropmitree NN, Gottlieb DJ et al (1998) Segregation analysis of pulmonary function among families in the Framingham study. Am J Respir Crit Care Med 157:1445–1451
Sanford AJ, Chagani T, Weir TD et al (2001) Susceptibility genes for rapid decline of lung function in the lung health study. Am J Respir Crit Care Med 163:469–473
Bose P, Bathri R (2012) Association of microsatellite instability and chronic obstructive pulmonary disorder in isocyanate-exposed population of Bhopal. Indian J Hum Genet 18:172–176
Guo X, Lin H-M, Lin Z et al (2000) Polymorphisms of surfactant protein gene A, B, D, and of SP-B-linked microsatellite markers in COPD of a Mexican population. Chest 117:249S–250S
Keatings VM, Cave SJ, Henry MJ et al (2000) A polymorphism in the tumor necrosis factor-α gene promoter region may predispose to a poor prognosis in COPD. Chest 118:971–975
Berndt A, Leme AS, Shapiro SD (2012) Emerging genetics of COPD. EMBO Mol Med 4:1144
Brode SK, Ling SC, Chapman KR (2012) Alpha-1 antitrypsin deficiency: a commonly overlooked cause of lung disease. Can Med Assoc J 184:1365–1371
Tian W, Fu Y, Garcia-Elias A et al (2009) A loss-of-function nonsynonymous polymorphism in the osmoregulatory TRPV4 gene is associated with human hyponatremia. Proc Natl Acad Sci 106:14034–14039
Tsushima H, Mori M (2006) Antidipsogenic effects of a TRPV4 agonist, 4α-phorbol 12,13-didecanoate, injected into the cerebroventricle. Am J Phys Regul Integr Comp Phys 290:R1736–R1741
Belvisi MG, Dubuis E, Birrell MA (2011) Transient receptor potential A1 channels: insights into cough and airway inflammatory disease. Chest 140:1040–1047
Rami HK, Gunthorpe MJ (2004) The therapeutic potential of TRPV1 (VR1) antagonists: clinical answers await. Drug Discov Today: Ther Strateg 1:97–104
Bareille P, Murdoch RD, Denyer J et al (2012) The effects of a TRPV1 antagonist, SB-705498, in the treatment of seasonal allergic rhinitis. Int J Clin Pharmacol Ther 51:576–584
Messeguer A, Planells-Cases R, Ferrer-Montiel A (2006) Physiology and pharmacology of the vanilloid receptor. Curr Neuropharmacol 4:1–15
Vriens J, Appendino G, Nilius B (2009) Pharmacology of vanilloid transient receptor potential cation channels. Mol Pharmacol 75:1262
Dietrich A, Steinritz D, Gudermann T (2017) Transient receptor potential (TRP) channels as molecular targets in lung toxicology and associated diseases. Cell Calcium 67:123–137
Zholos AV (2015) TRP channels in respiratory pathophysiology: the role of oxidative, chemical irritant and temperature stimuli. Curr Neuropharmacol 13:279–291
Funding
This work was supported by Council of Scientific and Industrial Research (CSIR), India.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Mandal, A., Srivastava, A., Chakraborti, T., Chakraborti, S. (2020). TRP Channels, Oxidative Stress and Chronic Obstructive Pulmonary Disease. In: Chakraborti, S., Parinandi, N., Ghosh, R., Ganguly, N., Chakraborti, T. (eds) Oxidative Stress in Lung Diseases. Springer, Singapore. https://doi.org/10.1007/978-981-32-9366-3_10
Download citation
DOI: https://doi.org/10.1007/978-981-32-9366-3_10
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-32-9365-6
Online ISBN: 978-981-32-9366-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)