
Abstract
Pancreatic endocrine neoplasms (PanNENs) are epithelial tumors affecting adults between the ages of 40 and 60 [1]. They are usually solitary and sporadic but may be part of hereditary syndromes, including multiple endocrine neoplasia type 1 (MEN1), von Hippel Lindau (VHL), neurofibromatosis type 1 (NF1) and tuberous sclerosis complex (TSC).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Tuberous Sclerosis Complex
- Allelic Imbalance
- Pancreatic Endocrine Neoplasm
- Tumor Suppressor Pathway
- TSC2 Gene
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Pancreatic endocrine neoplasms (PanNENs) are epithelial tumors affecting adults between the ages of 40 and 60 [1]. They are usually solitary and sporadic but may be part of hereditary syndromes, including multiple endocrine neoplasia type 1 (MEN1), von Hippel Lindau (VHL), neurofibromatosis type 1 (NF1) and tuberous sclerosis complex (TSC).
PanNENs are clinically defined as functioning (F-) or non-functioning (NF-). Patients with F-PanNEN present with a syndrome related to inappropriate hormone secretion. These tumors include insulinomas, gastrinomas, glucagonomas, VIPomas, and somatostatinomas [2–7]. The majority of patients harbor NF-PanNENs and usually present with mass-related symptoms of abdominal pain, nausea, or weight loss. With the exception of insulinomas, most PanNENs, either functional or non-functional, are diagnosed when they have developed into extensive malignant disease, and liver metastases are common. Patients with well-differentiated NF-PanNENs have a 5-year survival rate of approximately 65% and a 10-year survival rate of 45% [3, 8, 9].
2 Classification
The 2010 classification of the World Health Organization (WHO) (Table 8.1) identifies two categories based on tumor morphology: well-differentiated neuroendocrine neoplasms (PanNENs) and poorly differentiated neuroendocrine carcinomas (NECs) [10]. The latter are invariably high-grade malignancies while the former include more than 90% PanNENs with a clinical behavior varying from indolent to malignant, which cannot be predicted based on either tissue architecture or cytological features.
3 Pathology
Macroscopically, PanNENs are usually solitary, solid masses, from 1 to 5 cm in diameter, with rounded borders. The expansive pattern of growth determines compression and deviation of the main pancreatic and biliary ducts and of adjacent structures when extending outside the pancreas. The usual PanNEN is rich in small vessels and has scant fibrotic stroma. Necrotic yellowish foci can be observed in larger masses. Features of malignancy evident at macroscopic examination include involvement of the perivisceral fat and invasion of the duodenal wall or adjacent organs. PanNENs may have unusual features, including cystic aspects, and may lead to be misinterpreted as cystic neoplasia; more rarely, they show considerable fibrosis, mimicking ductal adenocarcinoma.
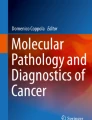
Microscopically, the majority of PanNENs are well-differentiated tumors that grow as solid nests or with trabecular patterns (Fig. 8.1), although glandular, acinar, and cribriform features are observed as well. A rich vascularization is typical. Necrosis can be present as either confluent areas ("infarct-like") in large tumors, or as punctate foci. Cytologically, PanNENs are composed of small to medium-sized cells with a finely granular cytoplasm and round or oval nuclei with salt-and-pepper chromatin. Tumoral infiltration of the duodenum and/or the biliary duct wall together with lymph node metastases identify the malignant forms, as does the involvement of the peripancreatic fat.

A typical well-differentiated neuroendocrine neoplasm. b A typical poorly differentiated neuroendocrine carcinoma (H&E staining)
Immunohistochemistry serves to confirm the endocrine nature of the neoplasia and thus to differentiate PanNENs from other neoplasms, based on the use of antibodies to at least one general endocrine marker, either synaptophysin [11] or chromogranin A (CgA) [12]. The cytosolic neuron-specific enolase (NSE) [13] and protein gene product 9.5 (PGP 9.5) [14] are less specific and their diagnostic utility is limited. PanNENs may express the normally produced pancreatic hormones (insulin, glucagon, somatostatin, and pancreatic polypeptide), or hormones of ectopic origin (gastrin, vasoactive intestinal polypeptide, adrenocorticotrophic hormone), or bioamines (serotonin). While any of these may be demonstrated by immunohistochemistry, the information has no clinical application.
Proliferative activity has a recognized prognostic value [10, 15], and its assessment by Ki67 immunostaining is a routine practice in several institutions, including ours (Fig. 8.2).

Immunohistochemical staining for Ki67 shows 1% positive cells (a) and 15% positive cells (b)
Poorly differentiated NECs are solid masses with extensive necrosis. Histologically, they resemble small-cell carcinomas or large-cell endocrine carcinomas of others organs, with a high mitotic rate, a proliferative activity of > 20%, and abnormal immunostaining for p53 that correlates with intragenic mutations in the TP53 gene [8, 10, 16]. NECs are usually negative for CgA while synaptophysin persists in the neoplastic cells.
4 Staging and Grading
The European Neuroendocrine Tumor Society (ENETS) has proposed a tumornode-metastasis (TNM)-based staging system for PanNEN [17] to which subsequent modifications have been proposed [18]. The TNM system is based on the evaluation of the following parameters: size, extrapancreatic invasion, and lymph node and liver metastasis. The clinical need to differentiate between carcinomas at the same stage is facilitated by the use of a grading system based on the measurement of the proliferative activity, by counting mitosis or assessing the immunohistochemical Ki-67 index. Both the TNM staging and the tumor grading systems have been shown to be valid tools for prognostic stratification of PanNENs in clinical practice [19, 20].
5 Genetics
Most PanNENs occur sporadically (90%), but they may be part of four hereditary cancer syndromes [9]: Multiple endocrine neoplasia type 1 (MEN1), von Hippel-Lindau disease (VHL), neurofibromatosis type 1 (NF1), and tuberous sclerosis complex (TSC). Of note, studies concerning these familial syndromes have furnished clues as to the molecular mechanisms involved in sporadic PanNEN tumorigenesis. The genetic aberrations associated with PanNENs include chromosomal alterations, epigenetic changes such as methylation, and mutations in single genes. The functional genomic alterations are found at the RNA level and include protein-coding mRNAs and regulatory small RNAs known as “non-coding RNAs” [21].
Accumulating evidence points towards a tumor suppressor pathway and chromatin remodeling as the most important mechanisms associated with PanNENs. Genome-wide analyses by comparative genomic hybridization have shown that virtually all PanNENs display chromosomal alterations [22–24]. Chromosomal losses are slightly more frequent than gains, whereas amplification events are uncommon. The presence of numerous regions of chromosomal losses and gains suggests the existence of two molecular subgroups: one showing frequent allelic imbalances (AI) and another showing low AI [25, 26]. These two subgroups have been shown to correspond to aneuploid and near-diploid tumors, respectively, and their identification was suggested to have prognostic value [26]. The total number of genomic changes per tumor appears to be associated with both tumor burden and disease stage, suggesting the accumulation of genetic alterations during tumor progression. A strong correlation has been found between sex-chromosome loss and an aggressive behavior of PanNENs, namely, the presence of local invasion or metastasis [27]. Retinoblastoma and TP53 gene defects have never been observed in PanNENs but are consistently present in NECs [16]. DNA methylation of the RASSF1A gene has been suggested as a major event in PanNENs [28, 29], possibly leading to gene inactivation. However, a very recent study demonstrated RASSF1A expression in the presence of promoter methylation [30]. Mutations in oncogenes are never or rarely observed in PanNENs [31, 32]. Instead, mutations in tumor suppressor genes represent the major genetic anomaly encountered in this type of tumor. Indeed, mutations in the tumor suppressor gene MEN1 are the most common anomaly associated with PanNENs [33, 34]. MEN1 encodes for the scaffold protein menin, which is known to interact with several proteins involved in, for example, transcription regulation, maintaince of genome stability, and histone modification.
A recent systematic whole-exome analysis exploiting next-generation sequencing technologies confirmed that MEN1 gene mutations are the most relevant anomalies in PanNEN [32]. More interestingly, mutually exclusive mutations were found in genes involved in chromatin remodeling (ATRX and DAXX). The majority of the mutations in these genes were associated with the loss of corresponding proteins that normally associate to form a macromolecular complex. This complex is involved in the deposition of histone H3 family member H3.3 at transcriptionally silent regions of the genome, including telomeres, and therefore is responsible for correct nucleosome assembly, the dysfunction of which likely leads to increased DNA damage and genome instability. Furthermore, the loss of ATRX/DAXX seems to be associated with ALT (alternative telomere lengthening), a crucial mechanism by which PanNENs maintain telomere length [35].
In addition to alterations in chromatin-associated genes, other tumor suppressor genes that have been found mutated in PanNENs are PTEN and TSC2, which are negative regulators of the mTOR pathway. Activation of mTOR pathways in primitive PanNENs was already demonstrated in analyses of expression profiles, which revealed the down-regulation of the TSC2 gene and alteration of TSC2 and PTEN protein expression in the vast majority of tumors analyzed [36].
Finally, global microRNA expression analysis revealed that the overexpression of a specific microRNA (miR-21) is strongly associated with an aggressive clinical behavior of PanNENs [37]. MicroRNAs are small non-coding RNAs that regulate gene expression by targeting specific mRNAs for degradation or translation inhibition. MiR-21 has several targets, including PTEN, whose expression is therefore reduced following up-regulation of the microRNA, leading to mTOR activation as well.
6 Conclusions
In patients with PanNENs, the pathology report must include information permitting disease classification, staging, and grading in order to obtain a prognostic evaluation. Genes involved in sporadic PanNEN tumorigenesis mainly belong to tumor suppressor pathways that are responsible for chromatin remodeling and the maintenance of genome stability. The direct consequences of these defective pathways are consistent chromosomal alterations that are a hallmark of PanNENs. Finally, global expression profiling analysis has furnished a strong rationale for the use of targeted therapy in the treatment of advanced-stage disease.
References
Klimstra D, Arnold R, Capella C et al (2010) Neuroendocrine neoplasms of the pancreas. In:Bosman F, Carneiro F, Hruban R, et al (eds) World Health Organization classification of tumors of the digestive system. IARC, Lyon
O’Toole D, Salazar R, Falconi M et al (2006) Rare functioning pancreatic endocrine tumors. Neuroendocrinology 84:189–195
Kloppel G, Rindi G, Anlauf M et al (2007) Site-specific biology and pathology of gastroenteropancreatic neuroendocrine tumors. Virchows Arch 451 Suppl 1:S9-27
Jensen RT, Niederle B, Mitry E et al (2006) Gastrinoma (duodenal and pancreatic). Neuroendocrinology 84:173–182
de Herder WW, Niederle B, Scoazec JY et al (2006) Well-differentiated pancreatic tumor/carcinoma: insulinoma. Neuroendocrinology 84:183–188
Anlauf M, Garbrecht N, Henopp T et al (2006) Sporadic versus hereditary gastrinomas of the duodenum and pancreas: distinct clinico-pathological and epidemiological features. World J Gastroenterol 12:5440–5446
Alexakis N, Neoptolemos JP (2008) Pancreatic neuroendocrine tumours. Best Pract Res Clin Gastroenterol 22:183–205
Hruban RU, Bishop Pitman M, Klimstra DL (2007) Endocrine Neoplasms, in Silverberg SG, Sobin LH (eds): Tumors of the pancreas. Washington, Armed Forces Institute of Pathology
Capelli P, Martignoni G, Pedica F et al (2009) Endocrine neoplasms of the pancreas: pathologic and genetic features. Arch Pathol Lab Med 133:350–364
Heitz PU, Komminoth P, Perren A et al (2004) Pancreatic endocrine tumours, in DeLellis RA, Lloyd RV, Heitz PU, et al (eds): World Health Organization Classification of Tumors. Pathology and Genetics of Tumors of Endocrine Organs. IARC Press, Lyon
Wiedenmann B, Franke WW, Kuhn C, et al (1986) Synaptophysin: a marker protein for neuroendocrine cells and neoplasms. Proc Natl Acad Sci U S A 83:3500–3504
Lloyd RV, Mervak T, Schmidt K et al (1984) Immunohistochemical detection of chromogranin and neuron-specific enolase in pancreatic endocrine neoplasms. Am J Surg Pathol 8:607–14
Bishop AE, Polak JM, Facer P et al (1982) Neuron specific enolase: a common marker for the endocrine cells and innervation of the gut and pancreas. Gastroenterology 83:902–15
Rode J, Dhillon AP, Doran JF et al (1985) PGP 9.5, a new marker for human neuroendocrine tumours. Histopathology 9:147–158
Pelosi G, Bresaola E, Bogina G et al (1996) Endocrine tumors of the pancreas: Ki-67 immunoreactivity on paraffin sections is an independent predictor for malignancy: a comparative study with proliferating-cell nuclear antigen and progesterone receptor protein immunostaining, mitotic index, and other clinicopathologic variables. Hum Pathol 27:1124–1134
Yachida S, Vakiani E, White CM et al (2012) Small cell and large cell neuroendocrine carcinomas of the pancreas are genetically similar and distinct from well-differentiated pancreatic neuroendocrine tumors. Am J Surg Pathol 36:173–184
Rindi G, Kloppel G, Alhman H et al (2006) TNM staging of foregut (neuro)endocrine tumors: a consensus proposal including a grading system. Virchows Arch 449:395–401
Scarpa A, Mantovani W, Capelli P et al (2010) Pancreatic endocrine tumors: improved TNM staging and histopathological grading permit a clinically efficient prognostic stratification of patients. Mod Pathol 23:824–833
Fischer L, Kleeff J, Esposito I et al (2008) Clinical outcome and long-term survival in 118 consecutive patients with neuroendocrine tumours of the pancreas. Br J Surg 95:627–635
Pape UF, Jann H, Muller-Nordhorn J et al (2008) Prognostic relevance of a novel TNM classification system for upper gastroenteropancreatic neuroendocrine tumors. Cancer 113:256–265
Barbarotto E, Schmittgen TD, Calin GA (2008): MicroRNAs and cancer: profile, profile, profile. Int J Cancer 122:969–977
Stumpf E, Aalto Y, Hoog A et al (2000) Chromosomal alterations in human pancreatic endocrine tumors. Genes Chromosomes Cancer 29:83–87
Speel EJ, Richter J, Moch H et al (1999) Genetic differences in endocrine pancreatic tumor subtypes detected by comparative genomic hybridization. Am J Pathol 155:1787–1794
Hu W, Feng Z, Modica I et al (2010) Gene Amplifications in Well-Differentiated Pancreatic Neuroendocrine Tumors Inactivate the p53 Pathway. Genes Cancer 1:360–368
Nagano Y, Kim do H, Zhang L et al (2007) Allelic alterations in pancreatic endocrine tumors identified by genome-wide single nucleotide polymorphism analysis. Endocr Relat Cancer 14:483–492
Rigaud G, Missiaglia E, Moore PS et al (2001) High resolution allelotype of nonfunctional pancreatic endocrine tumors: identification of two molecular subgroups with clinical implications. Cancer Res 61:285–292
Missiaglia E, Moore PS, Williamson J et al (2002) Sex chromosome anomalies in pancreatic endocrine tumors. Int J Cancer 98:532–538
Arnold CN, Sosnowski A, Schmitt-Graff A et al (2007) Analysis of molecular pathways in sporadic neuroendocrine tumors of the gastro-entero-pancreatic system. Int J Cancer 120:2157–2164
House MG, Herman JG, Guo MZ et al (2003) Aberrant hypermethylation of tumor suppressor genes in pancreatic endocrine neoplasms. Ann Surg 238:423–431; discussion 431-432
Malpeli G, Amato E, Dandrea M et al (2011) Methylation-associated down-regulation of RASSF1A and up-regulation of RASSF1C in pancreatic endocrine tumors. BMC Cancer 11:351
Corbo V, Beghelli S, Bersani S et al (2012) Pancreatic endocrine tumours: mutational and immunohistochemical survey of protein kinases reveals alterations in targetable kinases in cancer cell lines and rare primaries. Ann Oncol 23:127–134
Jiao Y, Shi C, Edil BH et al (2011) DAXX/ATRX, MEN1, and mTOR pathway genes are frequently altered in pancreatic neuroendocrine tumors. Science 331:1199–1203
Moore PS, Missiaglia E, Antonello D et al (2001) Role of disease-causing genes in sporadic pancreatic endocrine tumors: MEN1 and VHL. Genes Chromosomes Cancer 32:177–181
Corbo V, Dalai I, Scardoni M et al (2010) MEN1 in pancreatic endocrine tumors: analysis of gene and protein status in 169 sporadic neoplasms reveals alterations in the vast majority of cases. Endocr Relat Cancer 17:771–783
Heaphy CM, de Wilde RF, Jiao Y et al (2011) Altered telomeres in tumors with ATRX and DAXX mutations. Science 333:425
Missiaglia E, Dalai I, Barbi S et al (2010) Pancreatic endocrine tumors: expression profiling evidences a role for AKT-mTOR pathway. J Clin Oncol 28:245–255
Roldo C, Missiaglia E, Hagan JP et al (2006) MicroRNA expression abnormalities in pancreatic endocrine and acinar tumors are associated with distinctive pathologic features and clinical behavior. J Clin Oncol 24:4677–4684
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Italia
About this chapter
Cite this chapter
Scarpa, A., Corbo, V. (2013). Pathology and Genetics. In: Pederzoli, P., Bassi, C. (eds) Uncommon Pancreatic Neoplasms. Updates in Surgery. Springer, Milano. https://doi.org/10.1007/978-88-470-2673-5_8
Download citation
DOI: https://doi.org/10.1007/978-88-470-2673-5_8
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-2672-8
Online ISBN: 978-88-470-2673-5
eBook Packages: MedicineMedicine (R0)