
Abstract
In the last century, advances in biomedical sciences led to improvements in quality of human life mainly by decreasing the disease burden and providing various healthcare innovations. Effective medications were developed for most infectious diseases, lifestyle disorders, and other diseases. For once, we all believed that we can create a disease-free world; however, the excessive use of medications generated drug-resistant human pathogens leading to untreatable forms of many diseases. In the last few decades, the focus has been to understand the evolution of drug resistance, tackle the current drug-resistant disease agents, and develop new drugs that are potent and reliable for long-term usage. In this chapter, we will discuss the emerging themes in drug resistance research. As biologists are gaining deeper understanding of cellular complexity and disease agents, numerous modern themes have been pursued. The focus is to identify novel drug targets and develop specific drug molecules detrimental for the disease causing pathogens, and to harness host immunity. For the scope of this chapter, we will primarily discuss pharmacogenomics, therapeutic antibodies, cell-to-cell communication, exosomes, structuromics, and posttranslational modifications.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Pharmacogenomics
1.1 Introduction
The completion of human genome project in 2003 followed by emergence of high-throughput sequencing and genotyping technologies has led to the initiation of a new era in the research field with central focus on genomics. This has changed the way of looking at conventional study approaches leading to merging of different domains, which resulted in the opening of new research frontiers such as pharmacogenomics, network medicine, and systems pharmacology to name a few. In this section, we aim to provide a broad overview of the pharmacogenomics, including major developments that have occurred in this field and finally highlighting the significant achievements and future perspective.
Pharmacogenomics (PGx) and pharmacogenetics (PGt) involve individual’s genetic signatures to study drug response and/or drug toxicity behavior often referred to as phenotype. PGx differs from PGt in terms of the involvement of entire genome instead of few selected genes with no prior hypothesis. Genetic signature refers to the markers such as single-nucleotide polymorphisms (SNPs) and copy number variations (CNVs). Drug response phenotype implies to individual who responds well to the treatment (the good responder) and to one who doesn’t (the poor responder) based on drug metabolism profile categorized into extensive metabolizer, intermediate metabolizer, and poor metabolizer. Individuals with extensive-metabolizer phenotype excrete the drug from the body completely earlier than expected, failing to achieve its desired therapeutic effect. These individuals require higher doses than the normal individuals which are basically intermediate metabolizers. Poor metabolizers accumulate the drug in the body and may experience adverse drug reactions (ADR). Some people also show drug toxicity due to hypersensitivity reactions that may also be due to the individual specific genetic signatures such as genes in the human leukocyte antigen (HLA) system. So, these individuals may require a lower dose or switch to another drug.
Several factors affect the outcome of a PGx/PGt study including ethnicity, disease (brain disorders-serum drug levels are not useful), genetics (host susceptibility genes) and environment (diet, smoking, alcohol); and therefore these are considered an important part of study design based on the study hypothesis. The steps involved in a PGx/PGt study are depicted in Fig. 1.

Steps toward personalized medicine: To date around 136 FDA-approved drugs are available with pharmacogenetics information in their labeling
1.2 Role of Pharmacogenomics in Drug Resistance
The ultimate goal of pharmacogenomics is the development of optimized drug therapy based on the genetic makeup of an individual with maximum efficacy. The drug effects are determined by number of drug-metabolizing genes categorized into three groups—phase I (functionalization by cytochrome P450 superfamily), phase II (conjugation by conjugating enzymes such as sulfotransferases and UDP-glucuronosyltransferases), and phase III (excretion by drug transporters). The genetic variation in these genes may lead to differential response to drug treatment which can have important clinical implications. Drug transporters (phase III) have pivotal role in regulating the absorption, distribution, and excretion of many medications. There are number of studies where inherited variation in these transporters has been associated with differential response in different diseases and development of drug resistance in many diseases. Few such studies are discussed below.
1.2.1 Tuberculosis
Rifampicin is a first-line drug used to treat tuberculosis. Weiner et al. conducted a pharmacokinetics study in pulmonary tuberculosis patients from Africa, North America, and Spain compared with North American healthy controls to investigate the reasons for the interindividual variations in rifampicin levels. The study found that polymorphisms in the SLCO1B1 gene (encodes drug transporter OATP1B1—organic anion transporter peptide) had a significant influence on rifampicin exposure. Approximately 36 % lower exposure of rifampicin was found in patients with SLCO1B1 463 CA genotypes than CC genotypes (Weiner et al. 2010).
1.2.2 Epilepsy
There are number of studies in epilepsy where poor or no response to antiepileptic drugs (AEDs) is associated with variation in drug transporters. Siddiqui et al. investigated the role of genetic variation in ABCB1 (ATP-binding cassette subfamily, B1), encoding P-glycoprotein (P-gp) for multidrug resistance in epilepsy (Siddiqui et al. 2003). ABCB1 can efflux AEDs out of the cells. They studied ABCB1 C3435T variant (rs1045642) in 200 patients with drug-resistant epilepsy, 115 patients with drug-responsive epilepsy, and 200 controls, all of European ancestry. It was found that multidrug-resistant epilepsy patients were more likely to have the CC genotype than the TT genotype (Siddiqui et al. 2003).
1.2.3 HIV
The pharmacokinetics profile of antiretroviral drugs used in HIV therapy is also dependent on genetic differences in drug transporters. Anderson et al. conducted a study to understand the relationship of antiretroviral drug pharmacokinetics and pharmacodynamics with polymorphisms in drug-metabolizing genes. They observed that “indinavir” oral clearance was 24 % faster in individuals having multidrug resistance-associated protein 2 (MRP2)-24C/T variant which can interfere with drug efficacy as indinavir is a substrate of MRP2 and thus can limit drug absorption and accelerate drug clearance (Anderson et al. 2006).
1.3 Role of Pharmacogenomics in Drug Discovery
The information from PGx can help in drug discovery and development. The example of Herceptin (trastuzumab), a humanized monoclonal antibody against ErbB2 receptor used in breast cancer treatment (Vogel and Franco 2003; Noble et al. 2004), explains how well PGt tests can help in progressing drug discovery and development. It has been observed that more positive response was observed in patients with tumors overexpressing ErbB2. With PGt testing, individuals having overexpression of ErB2 and appropriate for Herceptin treatment can be identified (McCarthy et al. 2005). Similar approach can be used with drug transporters. One approach can be the use of specific inhibitors against transporters to stop efflux of drugs to overcome drug resistance in subgroup where overexpression of specific transporter is observed. The other approach can be identifying the molecular players like nuclear receptors regulating expression of transporters as their genetic variability is responsible for nonresponsiveness to drugs and drugs can be designed against those molecular players to achieve therapeutic efficacy. More research in PGx and development of specific technologies can really help in progress of medicinal sciences.
2 Therapeutic Antibodies for Bacterial Diseases
2.1 The Growing Problem of Antimicrobial Resistance
Antibiotics are the most commonly prescribed class of therapeutic agents both prophylactically and therapeutically. However, the use of antibiotics is not just limited to clinical settings. In an attempt to make food safer to eat, antibiotics have been introduced in poultry and dairy farms. In addition, several antibiotics are also being exploited in water sources for irrigation to prevent crop from diseases. This indiscriminate use of antibiotics has contributed heavily to the spread of antimicrobial resistance. Resistance to most antibiotics has been observed within 4–7 years of their introduction (Clatworthy et al. 2007). This has led to reemergence of infectious diseases, which had previously been effectively controlled by chemotherapy. This has in turn prompted surveillance programs by the World Health Organization (WHO) and Centers of Disease Control and Prevention (CDC) and European Center for Disease Prevention and Control (ECDC) to monitor the rise and spread of antibiotic resistance (http://www.who.int/drugresistance/global_action_plan/en/, http://www.cdc.gov/drugresistance/cdc_role.html, http://ecdc.europa.eu/en/healthtopics/antimicrobial_resistance/database/Pages/database.aspx).
According to current estimates by the CDC, there were two million cases of infections with 23,000 deaths from antibiotic-resistant organisms every year in the United States alone (2013 Threat Report, CDC http://www.cdc.gov/drugresistance/threat-report-2013/index.html). Several bacterial and fungal pathogens have made a comeback and have once again become an unmet clinical need of infectious disease (Fauci and Morens 2012). The ESKAPE pathogens, namely, Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species, are posing a serious challenge in the nosocomial environment and are rapidly becoming pan resistant to all known classes of antibiotics used against them (Rice 2008).
2.2 The Need for New Therapeutic Interventions
Owing to the growing problem of antimicrobial resistance, there is an urgent need for development of new therapeutic agents against infectious pathogens. Antimicrobial resistance has surfaced against all known classes of drugs including colistin which has been considered the last-resort antibiotic against several multidrug-resistant pathogens (Liu et al. 2016). With the exhaustion of the clinically useful antibiotic repertoire, attention is now being focused on other biologics that can serve to incapacitate pathogens. The post-antibiotic era has begun, and with that drug discovery programs are shifting focus toward large-molecule therapies which are based on an understanding of the host’s own immune defenses. Antibodies are one such class of agents that have historic precedence for use in successful treatment of certain infections. In the pre-antibiotic era, as early as the 1890s, antibodies were being used for the treatment of select infections, but with the discovery of antibiotics, antibody therapies took a backseat. As a result, their potential was neither fully realized nor exploited.
2.3 The Foundations of Antibody Therapy
The discovery of passive antibody immunotherapy for infectious diseases is credited to Emil von Behring and Shibasaburo Kitasato. They were the first to show that serum from guinea pigs infected with a sublethal dose of Corynebacterium diphtheriae could be used to protect healthy guinea pigs from a lethal challenge of the organism. Similar protection was also shown by them against another bacterial pathogen, Clostridium tetani (Von Behring and Kitasato 1965, 1991). For this discovery in 1901, von Behring secured the first physiology/medicine Nobel Prize. As is evident, the protection was afforded by antibodies directed against the diphtheria or tetanus toxins. At the same time, Paul Ehrlich made his contribution to the field by standardizing the therapeutic dose by titrating the antiserum in infected animals and establishing methods for generation of high-titer antiserum using large animals such as horses (Bosch and Rosich 2008). This was an important advancement in dose determination for immune-based therapies for which he was awarded the Nobel Prize in 1908 (along with Élie Metchnikoff for his discovery of phagocytosis). In the United States, the mass production of diphtheria antiserum for therapeutic use began in 1895 by the H. K. Mulford Company in Glenolden, Philadelphia (later Merck Sharp & Dohme Corp. in 1929). Subsequently, antiserum was successfully used in the treatment of some bacterial diseases such as diphtheria, tetanus, pneumococcal pneumonia, and meningitis (Casadevall 1996). These early advances not only helped lay the foundations of vaccinology but also established the therapeutic potential of antibodies. However, despite these early achievements, interest in serum-based therapies rapidly declined in the 1930s. The reasons for this decline included the problem of serum sickness (due to the presence of foreign animal proteins), unpredictable therapeutic outcomes (which was due to instability of preparations, differences in batches, and a lack of understanding of disease stage at the time of administration), and most importantly perhaps the rise of antibiotics. While antibodies continued to be exploited for vaccine discovery, their application to treatment of infections quickly decreased. After the discovery of penicillin by Alexander Fleming in 1928, antibiotics quickly became the magic bullets for treatment of life-threatening and nonlife-threatening microbial infections.
2.4 Antibody Structure
The typical immunoglobulin G (IgG) molecule is a Y-shaped molecule which has two longer heavy chains each of which is in turn linked to two shorter light chains by disulfide bonds. The heavy chains are also linked to each other by disulfide bonds. The light chains and their associated heavy-chain regions which form the fork of the “Y,” known as the Fab fragment, are involved in antigen binding. The stem of the “Y” which is composed of the two heavy chains is known as the Fc portion and is involved in binding to receptors on the surface of phagocytic cells. The Fab and Fc fragments are separated from each other by a hinge region which allows flexibility of movement to the Fab fragment. Further, the heavy and light chains are divided into distinct domains known as the variable and constant regions. Each heavy chain has three constant regions (CH1, CH2, and CH3) and one variable (VH) region. Each light chain has one constant (CL) and one variable (VL) region. Each Fab fragment is therefore composed of the VH and VL regions (which form the V region) and the CH1 and CL regions (which form the C region). The amino acid residues in the variable region define the specificity of the Ab. The V region of the Fab fragment which makes contact with the antigen is known as the paratope, and it is complementary to the residues on the antigen which form the antigen’s epitope (Putnam et al. 1979; Litman et al. 1993; Mattu et al. 1998; Maverakis et al. 2015).
2.5 Types of Therapeutic Antibody Molecules
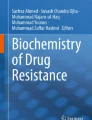
Therapeutic antibodies come in many flavors (Chames et al. 2009). From the conventional polyclonal sera to antibodies with multiple specificities and unconventional structure, all forms are currently being explored in therapy (Fig. 2).

Therapeutic antibody structural representation: (a) basic antibody structure, (b) single-chain variable fragment, (c) dimer of single-chain variable fragment, (d) toxin/therapeutic compound bound to single-chain variable fragment, (e) bispecific T-cell engager, (f) bispecific antibody, (g) bispecific F(ab)2 region, (h) bispecific Fab region, (i) diabody, and (j) heavy-chain only antibody
-
1.
While polyclonal antibodies are not as common in development anymore, monoclonal antibodies are still at the forefront of antibody therapies.
-
2.
Chimeric antibodies combine the portions of mouse and human antibodies where the human portion makes up to 70 %, allowing better specificity of the Fc region and reduced toxicity.
-
3.
Further advancement of technology has made possible the generation of humanized antibodies which are 85–50 % human, and these therefore have even better safety profiles.
-
4.
Antibody fragments comprising solely of the VL and VH domains, termed scFv (single-chain variable fragment), are used to provide specificity in the absence of Fc receptor-mediated opsonophagocytosis.
-
5.
Two scFv linked together with a very short linker make a structure known as the diabody.
2.6 Clinical Pipeline
The first monoclonal antibody to be approved for clinical use against an infectious agent was Palivizumab/Synagis for respiratory syncytial virus (RSV) in 1998. Palivizumab has been developed by MedImmune against the F protein of RSV (Johnson et al. 1997), for treatment of severe respiratory infection in high-risk infants. In recent years, antibody therapies have been in development against many infectious pathogens. Antibody therapies are being developed to enable pathogen clearance by diverse approaches.
2.6.1 Neutralization of Viruses and Toxins
Direct neutralization by formation of antigen-antibody complexes which can be cleared by the immune system.
2.6.2 Opsonophagocytic Killing
Antibodies specific for proteins on the pathogen’s surface. The Fc region is in turn able to bind the Fc receptors on surface of phagocytic cells. This allows the phagocyte to directly engulf and mediate killing of the pathogen.
2.6.3 Complement Activation
Binding of antibodies can also lead to complement activation which in turn can lead to pathogen lysis by formation of the membrane attack complex (particularly in Gram-negative bacteria and fungi).
2.6.4 Antibody-Drug Conjugates
Antibody-drug conjugate is a novel class of biologics where an antibody provides a means of delivery of a small-molecule chemotherapeutic agent.
There are several candidates currently in clinical development that are based on one or more of the abovementioned approaches (ter Meulen 2007, 2011; Bebbington and Yarranton 2008; Nagy et al. 2008; Saylor et al. 2009). These therapies are frequently directed against surface structures of the pathogens which are often critical for attachment, toxin injection, and immune evasion. Also, many candidates in development are directed against bacterial toxins which continue to cause injury to the host even after elimination of the pathogen. Some of them are discussed below:
Bacillus
One such target is the protective antigen (PA) of Bacillus anthracis. PA is a pore-forming protein of B. anthracis which heptamerizes, forming a pore in the endosomal membrane through which it delivers lethal factor (LF) and edema factor (EF) into the cell cytosol of host. All the antibodies in development against B. anthracis PA act by blocking the binding of PA to its receptor. Raxibacumab (Human Genome Sciences, NCT02016963), AVP-21D9 (Emergent BioSolutions, NCT01202695), Anthim (Elusys Therapeutics, NCT01453907), and Valortim (PharmAthene, NCT00964561) are antibodies in development for anthrax. Raxibacumab has recently been approved for treatment of inhalation anthrax in combination with antibiotics (Tsai and Morris 2015).
Clostridium
Toxin neutralization is also an effective strategy for Clostridium botulinum. There are seven toxins elaborated by C. botulinum BoNT/A-G. Of these BoNT/A is the most devastating toxin causing paralysis. A mixture of three IgG monoclonal antibodies with humanized regions, XOMA 3AB, is currently under development against BoNT/A (Nayak et al. 2014) (NCT01357213). The antibody targets different regions of the BoNT/A toxin. Clostridium difficile, which causes pseudomembranous colitis or diarrhea associated with antibiotics, exerts its effects by production of toxins A (TcdA) and B (TcdB), which mediate damage to epithelial cells (Voth and Ballard 2005). A combination of human monoclonal antibodies to TcdA (GS-CDA1) and TcdB (MDX-1388) is currently in development by Medarex (NCT00350298). Similarly, Merck Sharp & Dohme Corp. is also developing actoxumab-bezlotoxumab (a mixture of monoclonal antibodies to TcdA and TcdB which has completed phase III clinical trial (NCT01513239, Yang et al. 2015)).
Staphylococcus
Staphylococcus aureus produces many surface-associated as well as secreted virulence factors and toxins (such as proteases, adhesins, superantigens, leukocidins, autolysins) that serve as good targets for antibody therapy (Sause et al. 2016). Altastaph is a polyclonal IgG preparation directed against capsular polysaccharides 5 and 8 which has completed phase II trial (NCT00063089). Another polyclonal antibody in development (from Bristol-Myers Squibb) is Veronate which is directed against fibrinogen-binding protein, clumping factor A (ClfA) (DeJonge et al. 2007), but it failed to show any significant protection in the phase III trial (NCT00113191). Similarly a monoclonal Ab, Aurexis/tefibazumab (also developed by Bristol-Myers Squibb) directed against ClfA and aimed to be used in combination with antibiotic therapy has also completed phase IIa dose-escalation study (NCT00198289). Pagibaximab (Biosynexus Inc.) is a monoclonal antibody directed against lipoteichoic acids of staphylococcal cell wall and is in development for sepsis in neonates (NCT00646399). Aurograb (NeuTec Pharma.) has completed phase III trial for use in combination with vancomycin for treatment of methicillin-resistant S. aureus infections. Sanofi is developing SAR279356 (NCT01389700) a monoclonal antibody against the surface polysaccharide poly-N-acetylated glucosamine (PNAG) (Kelly-Quintos et al. 2006).
Escherichia coli
Chimeric monoclonal antibodies to Shiga toxins 1 and 2 (Stx 1 and 2) are in development by Thallion Pharmaceuticals (NCT01252199) against bacteria that produce Shiga toxin such as “Shiga toxin-producing E. coli (STEC).” This organism can cause hemolytic uremic syndrome and acute renal failure.
Pseudomonas
Pseudomonas aeruginosa is one of the most recalcitrant nosocomial pathogens. Pseudomonas pathogenesis relies on production of cytotoxins, surface adhesion molecules, and biofilms. Panobacumab (also known as KBPA-101 and Aerumab11) is a pentameric IgM monoclonal antibody targeting the O11 lipopolysaccharide of P. aeruginosa which is being developed by Kenta Biotech Ltd. and has completed phase IIa safety and pharmacokinetics trial (NCT00851435, Lazar et al. 2009; Que et al. 2014). Pseudomonas infections are particularly problematic in cystic fibrosis patients. KB001-A is a humanized monoclonal antibody targeting the pcrV structural component of the Pseudomonas type III secretion system, essential for translocation of Pseudomonas cytotoxins, and is being developed by KaloBios Pharmaceuticals (NCT01695343) for treatment of cystic fibrosis patients. MedImmune is developing MEDI3902 which is a bispecific antibody against P. aeruginosa. The antibody simultaneously targets the PcrV protein as well as Psl (a capsular lipopolysaccharide) and has shown promise for use independently as well as an adjunct to existing chemotherapeutic regimens (DiGiandomenico et al. 2014). It has recently completed a phase I clinical trial (NCT02255760).
2.7 Advantages and Disadvantages of Antibody Therapy
Antibody therapeutics offer several advantages over antibiotic therapy. First and foremost, antibodies have a good safety profile (especially monoclonals) and hence are better tolerated. Owing to their specificity, they suffer less from off-target and nonspecific effects. Also due to their specificity, antibodies do not have adverse effects on normal microflora of the body. However, the extreme specificity of antibodies makes them very narrow-spectrum therapeutics which in turn makes them less attractive for pharmaceutical companies. Nevertheless, antibodies have multifunctional capabilities. They don’t just exert their effects by directly blocking epitopes but also enhance immune function by mediating opsonization, agglutination, complement activation, and engagement of toxic cells by antibody-dependent cellular cytotoxicity (ADCC). Thus, they not only block pathogen attack but also aid in pathogen clearance from tissue spaces and bloodstream. When used in combination with antibiotics, they can work in conjunction with curtail pathogens and in some instances have even been shown to work synergistically to enhance the efficiency of antibiotics to which resistance has developed (DiGiandomenico et al. 2014). Another important advantage of antibodies is that they can be used not only therapeutically but also prophylactically.
Antibody therapies do suffer from several challenges as well. Besides being extremely narrow in their spectrum, they also pose the risk of being rendered ineffective if epitopes that they are directed against undergo a change. Bacterial and viral pathogens are known to show antigenic variation which can make antibodies ineffective. However in such a case, the paratope on the antibody may be modified to allow targeting of the new epitope. Further, since these antibodies are proteins, there is a chance that the immune system could mount a response against the antibody itself. Such anti-idiotypic antibodies can neutralize the therapeutic molecule, and they have been documented in treatment with therapeutic antibodies at least in case of rheumatoid arthritis (Isaacs et al. 1992). Additionally, certain types of antigens are only elaborated by select strains of the pathogen making such antigens less attractive for clinical development. Knowledge of the antigenic epitope is also crucial for developing an antibody therapeutic.
3 Development of Drug Resistance Through Inter- and Intracellular Communication
Cell-to-cell communication is the key to cellular adaptation and survival. Different types of cells have developed ways to communicate with each other. Initially, the intercellular communication was believed to be maintained by soluble paracrine and endocrine factors and by physical cell-to-cell contacts. The first of such contacts discovered were cell-cell synapses, gap junctions, plasmodesmata, and cellular projections (Abounit and Zurzolo 2012). In eukaryotes, one of these ways is through formation of nanotubular networks that provide valuable communicative means. Tunneling nanotubes, the long extensions of membrane between two cells placed distantly, and their networks were first discovered in plant and animal cells (Tarakanov and Goncharova 2009). In 2011, Dubey et al. showed how bacteria communicate with each other by nanotubes (Dubey and Ben-Yehuda 2011). Interestingly, bacteria can form nanotubes not only between same species but between different species as well (Dubey and Ben-Yehuda 2011; Pande et al. 2015). These nanotubes have been shown to be involved in cargo transport and antibiotic resistance (Dubey and Ben-Yehuda 2011; Pande et al. 2015). It is not clear if these bacterial nanotubes are just a communication mechanism or a survival strategy to counteract drug pressure.
Further, the molecular mechanisms of nanotube formation are still unknown. The study by Pande et al. has shown that bacteria form nanotubes during stress conditions such as nutrient starvation (Pande et al. 2015). These bacterial nanotubes reflect complex social behavior as bacteria from different species can form nanotubes to communicate (Dubey and Ben-Yehuda 2011; Pande et al. 2015). Hence, such nanotube formation may be a mechanism to exchange nutrients and other metabolites in bacterial communities such as biofilms. Biofilm-forming bacteria are known to survive drug pressure, and it is possible that in community some bacteria transfer metabolites to protect others from drug-induced pressure. The fitness advantage can answer how some bacteria survive drug pressure and acquire antibiotic resistance by staying metabolically quiescent for very long time. Further, mechanism of this vectorial transport also needs to be elaborated. One of the ways to maintain directionality is quorum sensing, the other could be electrical coupling. Also, concentration-dependent gradient between the two bacteria may help in determining the direction of flow.
Structurally, bacterial nanotubes resemble vectorial structure. Temperature may affect membrane motility, permeability, and membrane potential that in turn may affect nanotube composition, structure, and number. Another mode of intracellular communication is synapse, a link between nerve cells that are separated by a small gap across which neurotransmitters can be diffused through to generate an impulse. Synapse has also been proposed in plants and between immune and target cells, long after the corresponding notion of neuronal synapse in animals. Tunneling nanotubes have been shown to regulate neuronal synapses. These F-actin-based structures are involved in organelle transfer and electrical coupling between cells (Wang and Gerdes 2015). These nanotubes may help drug-sensitive cancer cell to connect with drug-resistant mutant cells and survive drug pressure (Wang and Gerdes 2015). Although tunneling nanotubes are absent in bacteria, similar structural forms are involved in antibiotic resistance indicating divergent evolution.
Nanotubes have been shown to transport proteins, plasmids, and other macromolecules between the cells. This mechanism may confer high levels of resistance markers being transferred between the cells. Consequently, nanotubular structures will be an important target for designing new drugs to overcome development of drug resistance. These drugs can be given in addition to other drugs that kill the target cells. Thus, combination therapies can be developed targeting bacterial physiology as well as nanotube formation. These therapies would be sensitive as well as specific for a given disease, considering the fact that nanotubular structures are specific for a given cell type.
4 Exosome-Mediated Drug Resistance
4.1 Extracellular Vesicles as Carriers of Drug-Resistant Traits Across Pathologies
Drugs impart an evolutionary selection pressure on the target cells. The phenomenon of transmission of drug resistance across population involves multiple mechanisms and helps in selecting for resistant cells from heterogeneous population. One recently discovered mechanism that has garnered much attention is the transfer of these traits by means of secreted vesicles, also termed as extracellular vesicles (EVs) (Yanez-Mo et al. 2015). These vesicles are further subclassified depending upon their size and density as either large oncosomes derived from cancerous cells (ranging in size from 1 μm to 10 μm), microvesicles (100 nm to 1 μm), and exosomes (30–100 nm) (Minciacchi et al. 2015). While large oncosomes and microvesicles are the recent focus of attention, exosomes have long been studied, and sufficient evidence exist that implicate their role in pathologies (Robbins and Morelli 2014; Braun and Moeller 2015; Campos et al. 2015; Coleman and Hill 2015; Fujita et al. 2015; Mahmoudi et al. 2015; Schorey et al. 2015).
4.2 Vesicle-Mediated Drug Resistance in Noncommunicable Disorders
A major impediment in managing the epidemic of noncommunicable disorders (NCDs) is the emergence of resistance to the existing line of drugs. Drug resistance is a phenomenon that comes across disease boundaries including emergence of steroid-resistant asthma (Luhadia 2014), insulin resistance leading to non-insulin-dependent diabetes mellitus, obesity, hypertension, dyslipidemia, atherosclerosis (DeFronzo 1997), and most importantly chemoresistance in cancers (Singh and Settleman 2010). While the direct role for exosomes has not been established for other conditions, their role in cancer drug resistance has been documented in several studies. Acquired and de novo resistance to existing therapies including chemotherapy, radiation therapy, and other targeted therapies has become a huge concern in the treatment of cancer (Meads et al. 2009), and exosomes have been implicated in several of these mechanisms (Azmi et al. 2013).
Radiation therapy employs high-energy waves, such as X-rays, electron beams, gamma rays, or protons for eliminating cancer cells, and theoretically this presents an attractive therapeutic choice; however, few cancerous cells were found to survive these high-energy radiations, the detailed cause for which is still being investigated. It has emerged recently that one of the mechanisms by which cancerous cells counters radiations is by secreting “survivin” which is a member of the inhibitor of apoptosis protein (IAP) family in exosomes (Khan et al. 2009). This creates a microenvironment that promotes further metastasis and drug resistance. Cancer cells have been shown to use exosomal pathway to physically efflux drugs, cisplatin, and doxorubicin that are one of the most widely used drugs (Shedden et al. 2003; Safaei et al. 2005). Similarly, in a breast cancer cell line that expresses Her2, the resistance to trastuzumab (monoclonal antibody-targeting Her2 receptor) arises due to exosomes that overexpress and secrete Her2. These exosomes are released by cancer-associated fibroblasts that increase cancer stem cells and induce several anti-apoptotic pathways (Ciravolo et al. 2012). Exosomes transferred from stroma to breast cancer cells lead to resistance against chemotherapy and radiation through antiviral and NOTCH3 pathways (Boelens et al. 2014). Tumor microenvironment has classically been associated with chronic hypoxia that can affect the DNA damage repair pathways and thereby induce DNA replication errors. This leads to genetic instability contributing to radiation resistance (Bristow and Hill 2008). Horizontal transfer of miRNAs and phosphorylated glycoproteins by drug-resistant breast cancer cell lines has also been suggested to be a novel mechanism of transmission of chemoresistance (Chen et al. 2014). Substantiating this principle, it was found that exosomes from docetaxel (DOC ⁄exo)-resistant MCF-7 breast cancer cells can confer drug resistance in drug-sensitive variant MCF-7 cell line (MCF-7/S).
Exosomes also play a role in thwarting body’s own defense mechanisms against cancerous cells as was demonstrated in several studies. It was reported that cancerous cells avoid complement-mediated lysis by exosomal secretion of protein mortalin (Pilzer and Fishelson 2005; Pilzer et al. 2005). Another study reported that TNF-α, which is secreted in association with exosomes, prevents cell death induced by activation of cytotoxic T cells (Zhang et al. 2006). Separately, lymphoma exosomes were found to protect target cells from attack of antibodies by releasing CD20 (Aung et al. 2011).
Exosomes carry several proteins that are unique to cancer cells. While some promote drug resistance, others have been used for cancer detection as biomarkers; for instance, exosome-associated glypican-1 (GPC-1) has been shown to sensitively differentiate between healthy individuals and patients with pancreatic cancer (Melo et al. 2015). Apart from this exosome, encapsulated DNA has also been used for cancer detection as well as to determine mutational status of parental tumor cells (Skog et al. 2008; Guescini et al. 2010; Thakur et al. 2014). Thus, exosomes play multifaceted roles in several noncommunicable disorders.
4.3 Vesicle-Mediated Drug Resistance in Pathogenic Disorders
Most human pathogens are bacterial species that lack typical machinery required for exosome production; however, they are known to produce outer membrane vesicles (OMVs) that bud from their plasma membranes and are known to carry proteins, phospholipids, lipopolysaccharides, and nucleic acids. OMVs of bacteria play a variety of roles on extracellular activities within intra- and interspecies microbes. Experimental data suggests that these vesicles often act as bacterial virulence factor and play significant role in pathogenesis. They’ve also been implicated in transmission of drug resistance by bacterial species such as S. aureus and P. aeruginosa to entire polymicrobial community by transfer of vesicle enclosed β-lactamase enzyme that allows recipient gram-positive and gram-negative bacteria to survive in the presence of antibiotic penicillin (Ciofu et al. 2000; Lee et al. 2013).
Transfer of plasmid containing genes for antibiotic resistance has been a classic route by which drug resistance can rapidly spread across population. Several of the gram-negative, but not gram-positive, eubacteria-derived vesicles were shown to carry nuclease-protected linear or supercoiled DNAs (Dorward and Garon 1990). In a laboratory demonstration of similar phenomenon in malaria parasite Plasmodium falciparum, Neta Regev-Rudzki et al. demonstrated that strains that were separately transfected with plasmids conferring resistance to WR99210 or blasticidin S upon co-culture allowed parasite to grow in the presence of both the drugs, while culturing them separately didn’t allowed growth of parasite (Regev-Rudzki et al. 2013).
Though much is known about the role of extracellular vesicles from bacteria and fungi in pathogenesis, the details of the role played by them in drug resistance is still an active area of research. Future research in extracellular vesicles is expected to shed new lights on the mechanisms of emergence and transmission of drug resistance across various physiological and pathological processes.
5 Structuromics
Transcription is one of the most important and basic steps for a cellular system. During transcription, RNA is formed using DNA as a template along with RNA polymerase and different kinds of modulator proteins. After transcription, primary transcript forms and additional modifications make mature RNAs, which are subsequently used for their respective functions. Mature RNA molecules retain some conserved sequences responsible for the formation of signature secondary structures for the interaction with different set of proteins. These secondary structures remain the same at a given time in the cell. But, these structures may change when RNA interacts with different set of proteins to maintain the physiology of the cell. Level of a given protein varies with time and requirement. It is intriguing to understand how the protein concentration varies for a given protein with time, keeping the sequence and hence the signature secondary structures the same. It suggests that RNA sequence or secondary structure is being modulated in response to specific signal. Thus, variations in different protein concentrations keep the cells alive and healthy in temporal environment (biotic and abiotic stress).
A highly informative concept came as “structuromics” by Howard Y. Chang’s group, which gave the comprehensive analysis of in vivo RNA secondary structure. The approach which they named “in vivo click selective 2′-hydroxyl acylation and profiling experiment (icSHAPE)” utilizes biochemical modifications of unpaired RNA bases and determines the structural dynamics of whole-cell RNA modules (Spitale et al. 2015). Understanding of this machinery will provide information such as protein-binding sites within specific secondary structures.
5.1 Role of Structuromics in Deciphering the Drug Resistance Mechanism
Exploring the structure of RNAs and analyzing their interaction with protein molecules in vivo will shed light on intracellular regulatory networks. These mechanisms resemble hidden weapons of bacteria and they are activated by the cell when needed. If we know the way and time of their activation, we can target those modules by making them nonfunctional. For example, RNAIII of S. aureus, which is 514 nucleotides long RNA molecule, regulates many genes encoding exportins and cell wall-associated proteins (Waters and Storz 2009). RNAIII interacts with different sets of proteins with its 5′ and 3′ domains and regulate their expression. It also controls expression of many virulence factors; these factors keep them viable and give strength to fight against host (Morfeldt et al. 1995; Boisset et al. 2007; Novick and Geisinger 2008; Chevalier et al. 2010; Liu et al. 2011). Targeting the modules formed by RNAIII under specific conditions will help in reducing the virulence of S. aureus. Though most of these structures arise during infection of the host and, hence, are difficult to target technically. In such cases, RNA structuromics might play a significant role, giving the vision of RNAIII complexes.
5.2 Role of Structuromics in Drug Designing
Till now, siRNA-mediated drugs have been used for some of the diseases like age-related macular degeneration (AMD), pachyonychia congenita (PC, a rare form of hereditary keratoderma that can affect the skin, mouth, hair, and eyes), and coronary artery disease and are also being used in HIV (Rossi 2006; Kleinman et al. 2008; Smith et al. 2008). Deciphering the structure of RNA-protein complexes (for some specific cases) either by structuromics or by cryo-electron microscopy will explore the mechanism of action of specific targets of siRNA molecules. This may play a crucial role in understanding the possible mechanisms of cells becoming resistant to an siRNA-based drug molecule. Subsequently, with the available information, chemical modifications within an siRNA molecule might provide additional information in its target inhibition. For example, addition of a drug (e.g., cross-linker which will inhibit the dissociation of protein and RNA molecule at its specific time of action) with siRNA will improve its stability as well as its action. Thus, RNA structuromics is a revolutionary aspect of RNA-based drug discovery.
6 Posttranslationally Modified Protein Networks as Drug Targets
In cellular information transfer, the most important transducers are proteins that define vital nature of the cell. For long, the central dogma of molecular information was thought to be DNA to RNA to protein. However, the translated proteins are often only the preprocessed forms which need further modifications to make them the elegant biological devices. The most common post-transnational modifications are phosphorylation, acetylation, glycosylation, and ubiquitinylation. Interestingly, these conserved modifications modify the protein activity, localization, and stability in both prokaryotes and eukaryotes. Therefore, these modifications and the enzymes responsible for carrying out these modifications are considered one of the most promising drug targets against many diseases such as cancer, malaria, and tuberculosis, among others. Specific posttranslationally modified (PTM) events are crucial in clinical manifestations and successful infections in most infectious disease. Therefore, targeting these modifications can be more effective than aiming a single drug target.
In M. tuberculosis, there are 11 Ser/Thr protein kinases, 2 Tyr phosphatases, and 1 Ser/Thr phosphatase. The genome also encodes at least one protein lysine acetyl transferase and one deacetylase (Nambi et al. 2010, 2013; Singhal et al. 2015). These enzymes together modify at least 400 important proteins reversibly to help the bacteria handle the stress and adapt by physiological changes (Prisic et al. 2010; Singhal et al. 2015). Another related pathogen M. ulcerans that causes Buruli ulcer has a kinase present in pathogenicity-related plasmid pMUM001 (Arora et al. 2014). This kinase phosphorylates some other structural proteins, also coded by virulence-associated plasmid, and helps the pathogen in successful infection (Arora et al. 2014). Interestingly, while proteins such as PrkC or PknB are conserved in most gram positive and actinomycetes, there are some other kinases that are exclusive and possess dual specificity (Arora et al. 2012, 2013). Two such kinases present in B. anthracis: one is the first DYRK-like kinase of prokaryotes PrkD and another is Ser-/Thr-/Tyr-specific enzyme PrkG (Arora et al. 2012). B. anthracis has evolved for its pathogenic lifestyle needs, lost tyrosine kinases, and expressed dual specificity protein kinases that are important for growth and possibly pathogenicity of the organism (Arora et al. 2012). Interestingly, all Ser/Thr protein kinases, dual specificity protein kinases, Tyr kinases, and acetyltransferases are shown to modify and regulate key physiological pathway proteins such as glycolysis, protein translation, and one-carbon metabolism (Arora et al. 2010, 2012, 2013; Singhal et al. 2013, 2015; Maji et al. 2015; Pereira et al. 2015; Prisic et al. 2015; Sajid et al. 2015). Several of these modifications regulated the key metabolic events in overlapping manner. The network of such signaling events forms nodes that fine-tune cellular response and help in adaptation and thriving under different stress conditions. Therefore, identification and targeting such nodes will be key to novel drug discovery.
7 Conclusions
The human genome has 46 chromosomes and around 20,000–25,000 protein-coding genes. Interestingly, the total number of human diseases known is estimated to be 10,000–30,000. In the years before the discovery of antibiotics, the general perception was humankind will never be able to successfully combat the pathogens such as tuberculosis, malaria, and cholera. In the next hundred years, we have achieved an unparallel understanding of life at the molecular level. Medical science has provided limited but effective solutions to combat major diseases. However, drug-resistant disease forms have constantly challenged our success. The emergence of drug-resistant forms has resulted in prolonged illness and increased rate of death even for common infections. According to WHO estimate, people infected with drug-resistant form of MRSA are 64 % more likely to die than compared to nonresistant forms. To end our misery from palpable drug-resistant diseases, in the future we will have to adapt cooperative drug discovery strategies and benefit from emerging themes such as immunotherapy, pharmacogenomics, and structuromics to annihilate these enemies of mankind. It is a necessity to use new and powerful beacons that target different disease forms. To achieve this, discovery of effective therapeutic agents that can provide protection against both acute and chronic forms along with better disease management is urgently required. With the experience of combating these diseases in last century, we must not rely on conserved drug target strategies and may have to develop multiple subordinate strategies each potent enough to strike pestilence effectively.
References
Abounit S, Zurzolo C (2012) Wiring through tunneling nanotubes–from electrical signals to organelle transfer. J Cell Sci 125:1089–1098. doi:10.1242/jcs.083279
Anderson PL, Lamba J, Aquilante CL, Schuetz E, Fletcher CV (2006) Pharmacogenetic characteristics of indinavir, zidovudine, and lamivudine therapy in HIV-infected adults: a pilot study. J Acquir Immune Defic Syndr 42:441–449. doi:10.1097/01.qai.0000225013.53568.69
Arora G, Sajid A, Gupta M, Bhaduri A, Kumar P, Basu-Modak S, Singh Y (2010) Understanding the role of PknJ in Mycobacterium tuberculosis: biochemical characterization and identification of novel substrate pyruvate kinase A. PLoS One 5, e10772. doi:10.1371/journal.pone.0010772
Arora G, Sajid A, Arulanandh MD, Singhal A, Mattoo AR, Pomerantsev AP, Leppla SH, Maiti S, Singh Y (2012) Unveiling the novel dual specificity protein kinases in Bacillus anthracis: identification of the first prokaryotic dual specificity tyrosine phosphorylation-regulated kinase (DYRK)-like kinase. J Biol Chem 287:26749–26763. doi:10.1074/jbc.M112.351304
Arora G, Sajid A, Arulanandh MD, Misra R, Singhal A, Kumar S, Singh LK, Mattoo AR, Raj R, Maiti S, Basu-Modak S, Singh Y (2013) Zinc regulates the activity of kinase-phosphatase pair (BasPrkC/BasPrpC) in Bacillus anthracis. Biometals 26:715–730. doi:10.1007/s10534-013-9646-y
Arora G, Sajid A, Singhal A, Joshi J, Virmani R, Gupta M, Verma N, Maji A, Misra R, Baronian G, Pandey AK, Molle V, Singh Y (2014) Identification of Ser/Thr kinase and forkhead associated domains in Mycobacterium ulcerans: characterization of novel association between protein kinase Q and MupFHA. PLoS Negl Trop Dis 8, e3315. doi:10.1371/journal.pntd.0003315
Aung T, Chapuy B, Vogel D, Wenzel D, Oppermann M, Lahmann M, Weinhage T, Menck K, Hupfeld T, Koch R, Trumper L, Wulf GG (2011) Exosomal evasion of humoral immunotherapy in aggressive B-cell lymphoma modulated by ATP-binding cassette transporter A3. Proc Natl Acad Sci U S A 108:15336–15341. doi:10.1073/pnas.1102855108
Azmi AS, Bao B, Sarkar FH (2013) Exosomes in cancer development, metastasis, and drug resistance: a comprehensive review. Cancer Metastasis Rev 32:623–642. doi:10.1007/s10555-013-9441-9
Bebbington C, Yarranton G (2008) Antibodies for the treatment of bacterial infections: current experience and future prospects. Curr Opin Biotechnol 19:613–619. doi:10.1016/j.copbio.2008.10.002
Boelens MC, Wu TJ, Nabet BY, Xu B, Qiu Y, Yoon T, Azzam DJ, Twyman-Saint VC, Wiemann BZ, Ishwaran H, Ter Brugge PJ, Jonkers J, Slingerland J, Minn AJ (2014) Exosome transfer from stromal to breast cancer cells regulates therapy resistance pathways. Cell 159:499–513. doi:10.1016/j.cell.2014.09.051
Boisset S, Geissmann T, Huntzinger E, Fechter P, Bendridi N, Possedko M, Chevalier C, Helfer AC, Benito Y, Jacquier A, Gaspin C, Vandenesch F, Romby P (2007) Staphylococcus aureus RNAIII coordinately represses the synthesis of virulence factors and the transcription regulator Rot by an antisense mechanism. Genes Dev 21:1353–1366. doi:10.1101/gad.423507
Bosch F, Rosich L (2008) The contributions of Paul Ehrlich to pharmacology: a tribute on the occasion of the centenary of his Nobel Prize. Pharmacology 82:171–179. doi:10.1159/000149583
Braun GS, Moeller MJ (2015) Progenitor cell-derived extracellular vesicles: an emerging diagnostic and therapeutic tool for renal disease. Nephrol Dial Transplant 30:339–341. doi:10.1093/ndt/gfv027
Bristow RG, Hill RP (2008) Hypoxia and metabolism. Hypoxia, DNA repair and genetic instability. Nat Rev Cancer 8:180–192. doi:10.1038/nrc2344
Campos JH, Soares RP, Ribeiro K, Andrade AC, Batista WL, Torrecilhas AC (2015) Extracellular vesicles: role in inflammatory responses and potential uses in vaccination in cancer and infectious diseases. J Immunol Res 2015:832057. doi:10.1155/2015/832057
Casadevall A (1996) Antibody-based therapies for emerging infectious diseases. Emerg Infect Dis 2:200–208. doi:10.3201/eid0203.960306
Chames P, Van RM, Weiss E, Baty D (2009) Therapeutic antibodies: successes, limitations and hopes for the future. Br J Pharmacol 157:220–233. doi:10.1111/j.1476-5381.2009.00190.x
Chen WX, Liu XM, Lv MM, Chen L, Zhao JH, Zhong SL, Ji MH, Hu Q, Luo Z, Wu JZ, Tang JH (2014) Exosomes from drug-resistant breast cancer cells transmit chemoresistance by a horizontal transfer of microRNAs. PLoS One 9, e95240. doi:10.1371/journal.pone.0095240
Chevalier C, Boisset S, Romilly C, Masquida B, Fechter P, Geissmann T, Vandenesch F, Romby P (2010) Staphylococcus aureus RNAIII binds to two distant regions of coa mRNA to arrest translation and promote mRNA degradation. PLoS Pathog 6, e1000809. doi:10.1371/journal.ppat.1000809
Ciofu O, Beveridge TJ, Kadurugamuwa J, Walther-Rasmussen J, Hoiby N (2000) Chromosomal beta-lactamase is packaged into membrane vesicles and secreted from Pseudomonas aeruginosa. J Antimicrob Chemother 45:9–13. doi:10.1093/jac/45.1.9
Ciravolo V, Huber V, Ghedini GC, Venturelli E, Bianchi F, Campiglio M, Morelli D, Villa A, Della MP, Menard S, Filipazzi P, Rivoltini L, Tagliabue E, Pupa SM (2012) Potential role of HER2-overexpressing exosomes in countering trastuzumab-based therapy. J Cell Physiol 227:658–667. doi:10.1002/jcp.22773
Clatworthy AE, Pierson E, Hung DT (2007) Targeting virulence: a new paradigm for antimicrobial therapy. Nat Chem Biol 3:541–548. doi:10.1038/nchembio.2007.24
Coleman BM, Hill AF (2015) Extracellular vesicles–their role in the packaging and spread of misfolded proteins associated with neurodegenerative diseases. Semin Cell Dev Biol 40:89–96. doi:10.1016/j.semcdb.2015.02.007
DeFronzo RA (1997) Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidaemia and atherosclerosis. Neth J Med 50:191–197
DeJonge M, Burchfield D, Bloom B, Duenas M, Walker W, Polak M, Jung E, Millard D, Schelonka R, Eyal F, Morris A, Kapik B, Roberson D, Kesler K, Patti J, Hetherington S (2007) Clinical trial of safety and efficacy of INH-A21 for the prevention of nosocomial staphylococcal bloodstream infection in premature infants. J Pediatr 151:260–265. doi:10.1016/j.jpeds.2007.04.060
DiGiandomenico A, Keller AE, Gao C, Rainey GJ, Warrener P, Camara MM, Bonnell J, Fleming R, Bezabeh B, Dimasi N, Sellman BR, Hilliard J, Guenther CM, Datta V, Zhao W, Gao C, Yu XQ, Suzich JA, Stover CK (2014) A multifunctional bispecific antibody protects against Pseudomonas aeruginosa. Sci Transl Med 6:262ra155. doi:10.1126/scitranslmed.3009655
Dorward DW, Garon CF (1990) DNA is packaged within membrane-derived vesicles of gram-negative but not gram-positive bacteria. Appl Environ Microbiol 56:1960–1962
Dubey GP, Ben-Yehuda S (2011) Intercellular nanotubes mediate bacterial communication. Cell 144:590–600. doi:10.1016/j.cell.2011.01.015
Fauci AS, Morens DM (2012) The perpetual challenge of infectious diseases. N Engl J Med 366:454–461. doi:10.1056/NEJMra1108296
Fujita Y, Kosaka N, Araya J, Kuwano K, Ochiya T (2015) Extracellular vesicles in lung microenvironment and pathogenesis. Trends Mol Med 21:533–542. doi:10.1016/j.molmed.2015.07.004
Guescini M, Genedani S, Stocchi V, Agnati LF (2010) Astrocytes and Glioblastoma cells release exosomes carrying mtDNA. J Neural Transm (Vienna) 117:1–4. doi:10.1007/s00702-009-0288-8
Isaacs JD, Watts RA, Hazleman BL, Hale G, Keogan MT, Cobbold SP, Waldmann H (1992) Humanised monoclonal antibody therapy for rheumatoid arthritis. Lancet 340:748–752. doi:10.1016/0140-6736(92)92294-P
Johnson S, Oliver C, Prince GA, Hemming VG, Pfarr DS, Wang SC, Dormitzer M, O’Grady J, Koenig S, Tamura JK, Woods R, Bansal G, Couchenour D, Tsao E, Hall WC, Young JF (1997) Development of a humanized monoclonal antibody (MEDI-493) with potent in vitro and in vivo activity against respiratory syncytial virus. J Infect Dis 176:1215–1224. doi:10.1086/514115
Kelly-Quintos C, Cavacini LA, Posner MR, Goldmann D, Pier GB (2006) Characterization of the opsonic and protective activity against Staphylococcus aureus of fully human monoclonal antibodies specific for the bacterial surface polysaccharide poly-N-acetylglucosamine. Infect Immun 74:2742–2750. doi:10.1128/IAI.74.5.2742-2750.2006
Khan S, Aspe JR, Asumen MG, Almaguel F, Odumosu O, Acevedo-Martinez S, De Leon M, Langridge WH, Wall NR (2009) Extracellular, cell-permeable survivin inhibits apoptosis while promoting proliferative and metastatic potential. Br J Cancer 100:1073–1086. doi:10.1038/sj.bjc.6604978
Kleinman ME, Yamada K, Takeda A, Chandrasekaran V, Nozaki M, Baffi JZ, Albuquerque RJ, Yamasaki S, Itaya M, Pan Y, Appukuttan B, Gibbs D, Yang Z, Kariko K, Ambati BK, Wilgus TA, DiPietro LA, Sakurai E, Zhang K, Smith JR, Taylor EW, Ambati J (2008) Sequence- and target-independent angiogenesis suppression by siRNA via TLR3. Nature 452:591–597. doi:10.1038/nature06765
Lazar H, Horn MP, Zuercher AW, Imboden MA, Durrer P, Seiberling M, Pokorny R, Hammer C, Lang AB (2009) Pharmacokinetics and safety profile of the human anti-Pseudomonas aeruginosa serotype O11 immunoglobulin M monoclonal antibody KBPA-101 in healthy volunteers. Antimicrob Agents Chemother 53:3442–3446. doi:10.1128/AAC.01699-08
Lee J, Lee EY, Kim SH, Kim DK, Park KS, Kim KP, Kim YK, Roh TY, Gho YS (2013) Staphylococcus aureus extracellular vesicles carry biologically active beta-lactamase. Antimicrob Agents Chemother 57:2589–2595. doi:10.1128/AAC.00522-12
Litman GW, Rast JP, Shamblott MJ, Haire RN, Hulst M, Roess W, Litman RT, Hinds-Frey KR, Zilch A, Amemiya CT (1993) Phylogenetic diversification of immunoglobulin genes and the antibody repertoire. Mol Biol Evol 10:60–72
Liu Y, Mu C, Ying X, Li W, Wu N, Dong J, Gao Y, Shao N, Fan M, Yang G (2011) RNAIII activates map expression by forming an RNA-RNA complex in Staphylococcus aureus. FEBS Lett 585:899–905. doi:10.1128/AAC.00522-12
Liu YY, Wang Y, Walsh TR, Yi LX, Zhang R, Spencer J, Doi Y, Tian G, Dong B, Huang X, Yu LF, Gu D, Ren H, Chen X, Lv L, He D, Zhou H, Liang Z, Liu JH, Shen J (2016) Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis 16:161–168. doi:10.1016/S1473-3099(15)00424-7
Luhadia SK (2014) Steroid resistant asthma. J Assoc Physicians India 62:38–40
Mahmoudi K, Ezrin A, Hadjipanayis C (2015) Small extracellular vesicles as tumor biomarkers for glioblastoma. Mol Aspects Med 45:97–102. doi:10.1016/j.mam.2015.06.008
Maji A, Misra R, Kumar MA, Kumar D, Bajaj D, Singhal A, Arora G, Bhaduri A, Sajid A, Bhatia S, Singh S, Singh H, Rao V, Dash D, Baby SE, Sarojini MJ, Chaudhary A, Gokhale RS, Singh Y (2015) Expression profiling of lymph nodes in tuberculosis patients reveal inflammatory milieu at site of infection. Sci Rep 5:15214. doi:10.1038/srep15214
Mattu TS, Pleass RJ, Willis AC, Kilian M, Wormald MR, Lellouch AC, Rudd PM, Woof JM, Dwek RA (1998) The glycosylation and structure of human serum IgA1, Fab, and Fc regions and the role of N-glycosylation on Fc alpha receptor interactions. J Biol Chem 273:2260–2272. doi:10.1074/jbc.273.4.2260
Maverakis E, Kim K, Shimoda M, Gershwin ME, Patel F, Wilken R, Raychaudhuri S, Ruhaak LR, Lebrilla CB (2015) Glycans in the immune system and The Altered Glycan Theory of Autoimmunity: a critical review. J Autoimmun 57:1–13. doi:10.1016/j.jaut.2014.12.002
McCarthy AD, Kennedy JL, Middleton LT (2005) Pharmacogenetics in drug development. Philos Trans R Soc Lond B Biol Sci 360:1579–1588. doi:10.1098/rstb.2005.1688
Meads MB, Gatenby RA, Dalton WS (2009) Environment-mediated drug resistance: a major contributor to minimal residual disease. Nat Rev Cancer 9:665–674. doi:10.1038/nrc2714
Melo SA, Luecke LB, Kahlert C, Fernandez AF, Gammon ST, Kaye J, LeBleu VS, Mittendorf EA, Weitz J, Rahbari N, Reissfelder C, Pilarsky C, Fraga MF, Piwnica-Worms D, Kalluri R (2015) Glypican-1 identifies cancer exosomes and detects early pancreatic cancer. Nature 523:177–182. doi:10.1038/nature14581
Minciacchi VR, Freeman MR, Di VD (2015) Extracellular vesicles in cancer: exosomes, microvesicles and the emerging role of large oncosomes. Semin Cell Dev Biol 40:41–51. doi:10.1016/j.semcdb.2015.02.010
Morfeldt E, Taylor D, von Gabain A, Arvidson S (1995) Activation of alpha-toxin translation in Staphylococcus aureus by the trans-encoded antisense RNA, RNAIII. EMBO J 14:4569–4577
Nagy E, Giefing C, von Gabain A (2008) Anti-infective antibodies: a novel tool to prevent and treat nosocomial diseases. Expert Rev Anti Infect Ther 6:21–30. doi:10.1586/14787210.6.1.21
Nambi S, Basu N, Visweswariah SS (2010) cAMP-regulated protein lysine acetylases in mycobacteria. J Biol Chem 285:24313–24323. doi:10.1074/jbc.M110.118398
Nambi S, Gupta K, Bhattacharyya M, Ramakrishnan P, Ravikumar V, Siddiqui N, Thomas AT, Visweswariah SS (2013) Cyclic AMP-dependent protein lysine acylation in mycobacteria regulates fatty acid and propionate metabolism. J Biol Chem 288:14114–14124. doi:10.1074/jbc.M113.463992
Nayak SU, Griffiss JM, McKenzie R, Fuchs EJ, Jurao RA, An AT, Ahene A, Tomic M, Hendrix CW, Zenilman JM (2014) Safety and pharmacokinetics of XOMA 3AB, a novel mixture of three monoclonal antibodies against botulinum toxin A. Antimicrob Agents Chemother 58:5047–5053. doi:10.1128/AAC.02830-14
Noble ME, Endicott JA, Johnson LN (2004) Protein kinase inhibitors: insights into drug design from structure. Science 303:1800–1805. doi:10.1126/science.1095920
Novick RP, Geisinger E (2008) Quorum sensing in staphylococci. Annu Rev Genet 42:541–564. doi:10.1146/annurev.genet.42.110807.091640
Pande S, Shitut S, Freund L, Westermann M, Bertels F, Colesie C, Bischofs IB, Kost C (2015) Metabolic cross-feeding via intercellular nanotubes among bacteria. Nat Commun 6:6238. doi:10.1038/ncomms7238
Pereira SF, Gonzalez RL Jr, Dworkin J (2015) Protein synthesis during cellular quiescence is inhibited by phosphorylation of a translational elongation factor. Proc Natl Acad Sci U S A 112:E3274–E3281. doi:10.1073/pnas.1505297112
Pilzer D, Fishelson Z (2005) Mortalin/GRP75 promotes release of membrane vesicles from immune attacked cells and protection from complement-mediated lysis. Int Immunol 17:1239–1248. doi:10.1093/intimm/dxh300
Pilzer D, Gasser O, Moskovich O, Schifferli JA, Fishelson Z (2005) Emission of membrane vesicles: roles in complement resistance, immunity and cancer. Springer Semin Immunopathol 27:375–387. doi:10.1007/s00281-005-0004-1
Prisic S, Dankwa S, Schwartz D, Chou MF, Locasale JW, Kang CM, Bemis G, Church GM, Steen H, Husson RN (2010) Extensive phosphorylation with overlapping specificity by Mycobacterium tuberculosis serine/threonine protein kinases. Proc Natl Acad Sci U S A 107:7521–7526. doi:10.1073/pnas.0913482107
Prisic S, Hwang H, Dow A, Barnaby O, Pan TS, Lonzanida JA, Chazin WJ, Steen H, Husson RN (2015) Zinc regulates a switch between primary and alternative S18 ribosomal proteins in Mycobacterium tuberculosis. Mol Microbiol 97:263–280. doi:10.1111/mmi.13022
Putnam FW, Liu YS, Low TL (1979) Primary structure of a human IgA1 immunoglobulin. IV. Streptococcal IgA1 protease, digestion, Fab and Fc fragments, and the complete amino acid sequence of the alpha 1 heavy chain. J Biol Chem 254:2865–2874
Que YA, Lazar H, Wolff M, Francois B, Laterre PF, Mercier E, Garbino J, Pagani JL, Revelly JP, Mus E, Perez A, Tamm M, Rouby JJ, Lu Q, Chastre J, Eggimann P (2014) Assessment of panobacumab as adjunctive immunotherapy for the treatment of nosocomial Pseudomonas aeruginosa pneumonia. Eur J Clin Microbiol Infect Dis 33:1861–1867. doi:10.1007/s10096-014-2156-1
Regev-Rudzki N, Wilson DW, Carvalho TG, Sisquella X, Coleman BM, Rug M, Bursac D, Angrisano F, Gee M, Hill AF, Baum J, Cowman AF (2013) Cell-cell communication between malaria-infected red blood cells via exosome-like vesicles. Cell 153:1120–1133. doi:10.1016/j.cell.2013.04.029
Rice LB (2008) Federal funding for the study of antimicrobial resistance in nosocomial pathogens: no ESKAPE. J Infect Dis 197:1079–1081. doi:10.1086/533452
Robbins PD, Morelli AE (2014) Regulation of immune responses by extracellular vesicles. Nat Rev Immunol 14:195–208. doi:10.1038/nri3622
Rossi JJ (2006) RNAi as a treatment for HIV-1 infection. Biotechniques Suppl:25–29
Safaei R, Larson BJ, Cheng TC, Gibson MA, Otani S, Naerdemann W, Howell SB (2005) Abnormal lysosomal trafficking and enhanced exosomal export of cisplatin in drug-resistant human ovarian carcinoma cells. Mol Cancer Ther 4:1595–1604. doi:10.1158/1535-7163.MCT-05-0102
Sajid A, Arora G, Singhal A, Kalia VC, Singh Y (2015) Protein phosphatases of pathogenic bacteria: role in physiology and virulence. Annu Rev Microbiol 69:527–547. doi:10.1146/annurev-micro-020415-111342
Sause WE, Buckley PT, Strohl WR, Lynch AS, Torres VJ (2016) Antibody-based biologics and their promise to combat Staphylococcus aureus infections. Trends Pharmacol Sci 37:231–241. doi:10.1016/j.tips.2015.11.008
Saylor C, Dadachova E, Casadevall A (2009) Monoclonal antibody-based therapies for microbial diseases. Vaccine 27(Suppl 6):G38–G46. doi:10.1016/j.vaccine.2009.09.105
Schorey JS, Cheng Y, Singh PP, Smith VL (2015) Exosomes and other extracellular vesicles in host-pathogen interactions. EMBO Rep 16:24–43. doi:10.15252/embr.201439363
Shedden K, Xie XT, Chandaroy P, Chang YT, Rosania GR (2003) Expulsion of small molecules in vesicles shed by cancer cells: association with gene expression and chemosensitivity profiles. Cancer Res 63:4331–4337
Siddiqui A, Kerb R, Weale ME, Brinkmann U, Smith A, Goldstein DB, Wood NW, Sisodiya SM (2003) Association of multidrug resistance in epilepsy with a polymorphism in the drug-transporter gene ABCB1. N Engl J Med 348:1442–1448. doi:10.1056/NEJMoa021986
Singh A, Settleman J (2010) EMT, cancer stem cells and drug resistance: an emerging axis of evil in the war on cancer. Oncogene 29:4741–4751. doi:10.1038/onc.2010.215
Singhal A, Arora G, Sajid A, Maji A, Bhat A, Virmani R, Upadhyay S, Nandicoori VK, Sengupta S, Singh Y (2013) Regulation of homocysteine metabolism by Mycobacterium tuberculosis S-adenosylhomocysteine hydrolase. Sci Rep 3:2264. doi:10.1038/srep02264
Singhal A, Arora G, Virmani R, Kundu P, Khanna T, Sajid A, Misra R, Joshi J, Yadav V, Samanta S, Saini N, Pandey AK, Visweswariah SS, Hentschker C, Becher D, Gerth U, Singh Y (2015) Systematic analysis of mycobacterial acylation reveals first example of acylation-mediated regulation of enzyme activity of a bacterial phosphatase. J Biol Chem 290:26218–26234. doi:10.1074/jbc.M115.687269
Skog J, Wurdinger T, van Rijn S, Meijer DH, Gainche L, Sena-Esteves M, Curry WT Jr, Carter BS, Krichevsky AM, Breakefield XO (2008) Glioblastoma microvesicles transport RNA and proteins that promote tumour growth and provide diagnostic biomarkers. Nat Cell Biol 10:1470–1476. doi:10.1038/ncb1800
Smith FJ, Hickerson RP, Sayers JM, Reeves RE, Contag CH, Leake D, Kaspar RL, McLean WH (2008) Development of therapeutic siRNAs for pachyonychia congenita. J Invest Dermatol 128:50–58. doi:10.1038/sj.jid.5701040
Spitale RC, Flynn RA, Zhang QC, Crisalli P, Lee B, Jung JW, Kuchelmeister HY, Batista PJ, Torre EA, Kool ET, Chang HY (2015) Structural imprints in vivo decode RNA regulatory mechanisms. Nature 519:486–490. doi:10.1038/nature14263
Tarakanov AO, Goncharova LB (2009) Cell-cell nanotubes: tunneling through several types of synapses. Commun Integr Biol 2:359–361
ter Meulen J (2007) Monoclonal antibodies for prophylaxis and therapy of infectious diseases. Expert Opin Emerg Drugs 12:525–540. doi:10.1517/14728214.12.4.525
ter Meulen J (2011) Monoclonal antibodies in infectious diseases: clinical pipeline in 2011. Infect Dis Clin North Am 25:789–802. doi:10.1016/j.idc.2011.07.006
Thakur BK, Zhang H, Becker A, Matei I, Huang Y, Costa-Silva B, Zheng Y, Hoshino A, Brazier H, Xiang J, Williams C, Rodriguez-Barrueco R, Silva JM, Zhang W, Hearn S, Elemento O, Paknejad N, Manova-Todorova K, Welte K, Bromberg J, Peinado H, Lyden D (2014) Double-stranded DNA in exosomes: a novel biomarker in cancer detection. Cell Res 24:766–769. doi:10.1038/cr.2014.44
Tsai CW, Morris S (2015) Approval of raxibacumab for the treatment of inhalation anthrax under the US food and drug administration “Animal Rule”. Front Microbiol 6:1320. doi:10.3389/fmicb.2015.01320
Vogel CL, Franco SX (2003) Clinical experience with trastuzumab (herceptin). Breast J 9:452–462. doi:10.1046/j.1524-4741.2003.09602.x
Von Behring E, Kitasato S (1965) On the development of immunity to diphtheria and tetanus in animals. Dtsch Med Wochenschr 90:2183
Von Behring E, Kitasato S (1991) The mechanism of diphtheria immunity and tetanus immunity in animals. 1890. Mol Immunol 28:1317, 1319–1320
Voth DE, Ballard JD (2005) Clostridium difficile toxins: mechanism of action and role in disease. Clin Microbiol Rev 18:247–263. doi:10.1128/CMR.18.2.247-263.2005
Wang X, Gerdes HH (2015) Transfer of mitochondria via tunneling nanotubes rescues apoptotic PC12 cells. Cell Death Differ 22:1181–1191. doi:10.1038/cdd.2014.211
Waters LS, Storz G (2009) Regulatory RNAs in bacteria. Cell 136:615–628. doi:10.1016/j.cell.2009.01.043
Weiner M, Peloquin C, Burman W, Luo CC, Engle M, Prihoda TJ, Mac Kenzie WR, Bliven-Sizemore E, Johnson JL, Vernon A (2010) Effects of tuberculosis, race, and human gene SLCO1B1 polymorphisms on rifampin concentrations. Antimicrob Agents Chemother 54:4192–4200. doi:10.1128/AAC.00353-10
Yanez-Mo M, Siljander PR, Andreu Z, Zavec AB, Borras FE, Buzas EI, Buzas K, Casal E, Cappello F, Carvalho J, Colas E, Cordeiro-da SA, Fais S, Falcon-Perez JM, Ghobrial IM, Giebel B, Gimona M, Graner M, Gursel I, Gursel M, Heegaard NH, Hendrix A, Kierulf P, Kokubun K, Kosanovic M, Kralj-Iglic V, Kramer-Albers EM, Laitinen S, Lasser C, Lener T, Ligeti E, Line A, Lipps G, Llorente A, Lotvall J, Mancek-Keber M, Marcilla A, Mittelbrunn M, Nazarenko I, Nolte-‘t Hoen EN, Nyman TA, O’Driscoll L, Olivan M, Oliveira C, Pallinger E, Del Portillo HA, Reventos J, Rigau M, Rohde E, Sammar M, Sanchez-Madrid F, Santarem N, Schallmoser K, Ostenfeld MS, Stoorvogel W, Stukelj R, Van der Grein SG, Vasconcelos MH, Wauben MH, De Wever O (2015) Biological properties of extracellular vesicles and their physiological functions. J Extracell Vesicles 4:27066. doi:10.3402/jev.v4.27066
Yang Z, Ramsey J, Hamza T, Zhang Y, Li S, Yfantis HG, Lee D, Hernandez LD, Seghezzi W, Furneisen JM, Davis NM, Therien AG, Feng H (2015) Mechanisms of protection against Clostridium difficile infection by the monoclonal antitoxin antibodies actoxumab and bezlotoxumab. Infect Immun 83:822–831. doi:10.1128/IAI.02897-14
Zhang HG, Liu C, Su K, Yu S, Zhang L, Zhang S, Wang J, Cao X, Grizzle W, Kimberly RP (2006) A membrane form of TNF-alpha presented by exosomes delays T cell activation-induced cell death. J Immunol 176:7385–7393. doi:10.4049/jimmunol.176.12.7385
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Arora, G. et al. (2017). Emerging Themes in Drug Resistance. In: Arora, G., Sajid, A., Kalia, V. (eds) Drug Resistance in Bacteria, Fungi, Malaria, and Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-48683-3_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-48683-3_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-48682-6
Online ISBN: 978-3-319-48683-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)