
Abstract
Autoimmunity, infections and immune-mediated mechanisms associated with pathogens, vaccinations and systemic diseases can damage the spinal cord and its adjacent structures. Multiple sclerosis is the most common cause of autoimmune myelitis, preferably affects young women and takes a relapsing–remitting or progressive course. In children, acute disseminated encephalomyelitis frequently accounts for acute myelitis. The clinical hallmarks of neuromyelitis optica spectrum disorder are recurrent episodes of optic neuritis and longitudinally extensive transverse myelitis. Further immune-mediated causes of myelitis include sarcoidosis, Sjögren’s disease, spinal manifestations of systemic autoimmune and inflammatory diseases as well as paraneoplastic, para-/postinfectious and para-/post-vaccinal aetiologies. Diagnostic criteria rely on clinical and magnetic resonance imaging features together with serum and cerebrospinal fluid examination.
Infections with viruses, bacteria, spirochaetales, fungi, protozoa or helminths can affect the spinal cord, nerve roots and adjacent structures, frequently resulting in severe long-term sequelae. Herpes virus transverse myelitis and the tick-transmitted diseases neuroborreliosis and tick-borne encephalitis are the most common causes of infectious myelitis in Central Europe, whereas on a worldwide scale, myelitis caused by enteroviridae (e.g. poliomyelitis or enterovirus) and spinal neurocysticercosis are more frequent. The diagnosis of infectious spinal cord disease is made by cerebrospinal fluid analysis with elevated cell counts and detection of pathogens by microscopy or polymerase chain reaction or a specific intrathecal antibody reaction. Since infectious and autoimmune myelitis are associated with significant morbidity and mortality and often account for severe neurological deficits as well as long-term sequelae, early and specialised multidisciplinary care are recommended.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Immune-Mediated Myelitis
1.1 Introduction
Autoimmune and other immune-mediated causes of myelitis are common and often occur in the context of a more widespread inflammation involving the brain or other organs. Isolated spinal manifestations, particularly idiopathic transverse myelitis and longitudinally extensive transverse myelitis, may occur. The worldwide incidence of acute transverse myelitis is projected to be between 1.35 and 4.6 per million per year [10].
Multiple sclerosis is the most common cause of autoimmune myelitis in adults, whereas acute disseminated encephalomyelitis frequently accounts for acute myelitis in children. Further immune-mediated causes of myelitis include neuromyelitis optica spectrum disorder, sarcoidosis, Sjögren’s disease, spinal manifestations of systemic autoimmune and inflammatory diseases as well as paraneoplastic, para-/postinfectious and para-/post-vaccinal aetiologies (Table 6.1).
The clinical features of autoimmune and immune-mediated myelitis are mainly defined by the anatomic location and extent of injury to the spinal cord in its craniocaudal and transverse axes, to a lesser degree by the immune mechanisms involved. Apart from Sjögren’s syndrome and para-/postinfectious, paraneoplastic and para-/post-vaccinal aetiologies, which can all present with concomitant radiculitis and cause flaccid paresis, weakness is usually of the upper motor neuron type with associated spasticity, exaggerated reflexes and extensor plantar reflexes.
1.2 Multiple Sclerosis
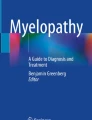
Multiple sclerosis (MS) is the most common autoimmune demyelinating disease of the central nervous system (CNS), showing a female preponderance [35]. MS can take a relapsing–remitting or a primary or secondary progressive disease course, the latter with or without active inflammation [111]. A primary manifestation or relapses of MS as myelitis is common and is the most frequent cause of autoimmune myelitis. In individuals with known MS, a new spinal manifestation should therefore primarily be diagnosed and treated as an MS relapse. Spinal cord lesions in MS are typically short, spanning over one or two segments, and localised laterally in the spinal cord (Fig. 6.1). Contrast enhancement is seen regularly in acute lesions. A longitudinal myelitis is not typical for MS and should trigger alternative diagnoses such as neuromyelitis optica spectrum disorder (NMOSD, see below). Patients presenting with a monofocal myelitis and asymptomatic brain lesions without contrast enhancement have a high risk of developing a clinically definite MS in the future [138]. With at least two additional lesions in cranial MRI, one with contrast enhancement, the current diagnostic criteria allow the definite diagnosis of MS [141] and underline the importance of a cranial MRI in patients initially presenting with a clinically isolated myelitis. CSF examination reveals a mild pleocytosis, normally below 50 cells/μL with a predominance for activated lymphocytes. Oligoclonal bands and signs for a polyspecific intrathecal antibody production are found in the majority of MS patients and support the diagnosis. A thorough differential diagnosis should exclude other causes. Treatment of spinal manifestation of MS follows the general recommendations of relapse treatment including high-dose steroids and in the case of steroid-refractory functional deficits the use of apheresis therapies (see Sect. 6.1.11). Long-term treatment of MS is based on the use of immunomodulatory and immunosuppressive strategies.

Multiple sclerosis (MS). Spinal MRI of a 23-year-old male presenting with subacute onset of right-sided hypaesthesia of the trunk. The patient was subsequently diagnosed with a relapsing–remitting MS. (a, b) Sagittal and (c, d) axial T2- and T1-weighted images show a monosegmental laterally located myelitis. (b, d) Gadolinium enhancement is shown. Arrows indicate the anterior spinal artery (Images courtesy of Dr. Peter Raab, Neuroradiology, Hannover Medical School)
1.3 Neuromyelitis Optica Spectrum Disorder
Neuromyelitis optica spectrum disorder (NMOSD) is a disabling autoimmune condition of the CNS characterised by inflammation predominantly of the optic nerves and the spinal cord. Neuromyelitis optica (NMO), also known as Devic’s disease, was long considered a variant of MS. However, the discovery of highly specific serum autoantibodies against aquaporin 4 (AQP4) in a subset (60–80 %) of patients with NMO has identified NMO as a distinct disease entity completely separate from MS [12, 22, 108, 196]. With characterisation of patients with AQP4 antibodies but not the full clinical picture of NMO, the spectrum of the disease entity has been expanded, and the term NMO spectrum disorder (NMOSD) was introduced [197]. In 2015, the diagnostic criteria of NMOSD were revised and underline the importance of the presence of AQP4 antibodies with stratifying NMOSD in those with and without AQP4 antibodies [198]. The core clinical characteristics required for patients with NMOSD with AQP4 antibodies include clinical syndromes or MRI findings related to optic nerve, spinal cord, area postrema and other brainstem, diencephalic or cerebral presentations. More stringent clinical criteria, with additional neuroimaging findings, are required for diagnosis of NMOSD without AQP4 antibodies or when serologic testing is unavailable.
Spinal cord affection in NMOSD patients shows typically an LETM, which is defined as spanning over at least three vertebral segments (Fig. 6.2). Lesions are often found centrally in the spinal cord. Contrast enhancement is patchy and long lasting. Recently, anti-MOG antibodies were detected in some AQP4 antibody-negative NMOSD patients, constituting approximately 5 % of all NMOSD patients [102, 112, 155]. NMOSD has a strong female preponderance (up to 10:1 depending on geographical region). The occurrence and frequency of myelitis in the first year predicts the long-term course of NMOSD [86]. Contrary to MS, myelitis in NMOSD often leaves residual deficits with complete remissions in only 20 % of cases. Since the outcome of NMOSD attacks is decisive for long-term disability, early escalation of attack treatment is recommended [103]. Apheresis therapies might be superior to high-dose corticosteroids for the first-line treatment of NMOSD myelitis [103]. Concomitant autoimmune or rheumatologic diseases occur in up to 40 % of patients with NMOSD [82]. LETM can also be found of other origin than in NMOSD; therefore, a thorough differential work-up is essential [186]. Long-term treatment of NMOSD is immunosuppressive; first-line therapies are azathioprine or rituximab [187].

Neuromyelitis optica spectrum disorder (NMOSD). Spinal MRI of a 61-year-old woman with acute painful tetraparesis and aquaporin-4 antibody-positive NMOSD. (a) Sagittal T2-weighted and (b) axial T2-weighted images show a longitudinally extensive transverse myelitis (LETM) spanning five vertebral segments and the whole axial plane. Notice spinal oedema with swelling of the myelon. (c) Patchy, “cloud-like” gadolinium enhancement on T1-weighted sagittal image (Images courtesy of Prof. Carsten Lukas, Radiology, St. Josef Hospital Bochum)
1.4 Acute Disseminated Encephalomyelitis
Acute disseminated encephalomyelitis (ADEM) is a monophasic (multiphasic possible) inflammatory multifocal disease of the CNS [180]. ADEM typically affects children and young adults. An association with previous infections and vaccination has repeatedly been reported [149]. Clinical presentation ranges from a prodromal phase with fever, headache and nausea to the rapid appearance of multifocal neurological deficits, often accompanied by reduced consciousness and a psychosyndrome. Cranial MRI typically exhibits large lesions in the white and grey matter with perifocal oedema, often of the same age and gadolinium enhancing [203]. The involvement of the spinal cord is frequently observed, showing lesions of longitudinal extent [9]. ADEM is associated with occurrence of anti-MOG antibodies, particularly in children [11, 112].
Diagnosis is based on the combination of clinical presentation, cranial MRI with multifocal lesions of the same age, spinal MRI with longitudinal myelitis and CSF examination revealing mild to moderate pleocytosis and absence of oligoclonal bands. Therapy comprises of high-dose methylprednisolone but can also include therapeutic plasma exchange, intravenous immunoglobulins and immunosuppressants.
1.5 Idiopathic Transverse Myelitis
The diagnosis of an idiopathic transverse myelitis (ITM) is based on exclusion of other diseases. About 40 % of acute transverse myelopathies remain unexplained [163]. The “Transverse Myelitis Consortium Working Group” (TMCWG) has proposed diagnostic criteria for an idiopathic transverse myelitis [184]. Besides a typical clinical presentation for a spinal cord lesion, the diagnosis requires signs of an inflammatory aetiology either by MRI (hyperintensities in T2-weighted images, contrast enhancement) or in the CSF with a pleocytosis or intrathecal immunoglobulin production (elevated IgG index). Other aetiologies, particularly infectious or autoimmune disease, vascular or metabolic disease and hypovitaminosis, have to be excluded by a thorough differential diagnostic work-up.
ITM usually is monophasic and has a good outcome in the majority of patients [184]. About one third of patients initially diagnosed with an ITM and normal cranial MRI will develop a clinically definite MS within 5 years [138]. Recurring transverse myelitis without other CNS manifestation can occur in about 8 % of patients with an acute isolated ITM [166].
1.6 Myelitis with Systemic Autoimmune Diseases
Spinal cord affliction can occur as a complication of multisystem autoimmune or inflammatory disorders, for example, sarcoidosis, Sjögren’s disease, systemic lupus erythematosus (SLE), Behçet’s disease, mixed connective tissue disease, vasculitis and others.
1.6.1 Sarcoidosis
Sarcoidosis is a granulomatous disease of unknown aetiology which typically involves various organs with a predilection of the lungs (in about 90 % of patients) and lymph nodes [38, 89]. Clinical involvement of the CNS usually occurs early in the disease and is reported in approximately 5–15 % of cases [175]. Cranial neuropathy, papilloedema, aseptic meningitis, hydrocephalus, seizures, psychiatric symptoms, cerebral and also spinal lesions as well as peripheral neuropathy and skeletal muscle involvement have been described as neurological complications. Spinal lesions are typically longitudinally and centrally located in the cord (Fig. 6.3). Primary manifestation of a sarcoidosis as an LETM in the nervous system is possible [19]. Diagnostic work-up includes CSF analysis showing mild to moderate pleocytosis and mild disruption of the blood–brain barrier, serum soluble IL-2 receptor, chest imaging and whole body FDG-PET scan to identify hypermetabolic lymph nodes. Definite diagnosis of sarcoidosis still has to be inferred from biopsy. Therapy comprises of corticosteroids and immunosuppressants; in rapid progressive cases, successful treatment with infliximab has been reported [30, 88, 192].

Neurosarcoidosis. MRI of the thoracic spinal cord of a 52-year-old woman with acute paraparesis and biopsy-proven pulmonary sarcoidosis. (a) Sagittal T2- and (b) fat-suppressed T1-weighted images after gadolinium injection show a longitudinally extensive lesion with enhancement of the dorsal column (Images courtesy of Prof. Carsten Lukas, Radiology, St. Josef Hospital Bochum)
1.6.2 Sjögren’s Syndrome
Sjögren’s syndrome is a systemic autoimmune disease that affects primarily the exocrine glands and is associated with anti-SSA (anti-Ro) and anti-SSB (anti-La) antibodies [194]. Typical symptoms are dry eyes and reduced production of saliva. Vasculitis and CNS involvement can be observed as typical and frequent extraglandular manifestations of primary Sjögren’s syndrome [48, 60]. A painful, mostly sensory polyneuropathy and sensory ganglionopathy are the most frequent neurological complications. CNS involvement shows a wide spectrum, occurs far less often and includes asymptomatic white matter lesions on MRI but also severe focal neurological symptoms including optic neuritis and transverse myelitis [48]. Myelitis often is longitudinal in extent and can affect all parts of the cord [14]. Overlap syndromes with NMOSD are frequently encountered; hence, testing for AQP4 antibodies is recommended [14, 85].
1.6.3 Systemic Lupus Erythematosus (SLE)
Neurological involvement in patients with SLE is frequent and ranges from mild neurocognitive dysfunction and mood changes to severe psychiatric and neurological manifestations such as seizures, stroke and psychosis [15]. Spinal cord involvement is less common (about 1–2 %) and mostly presents as transverse myelitis [105]. Myelitis with longitudinal extent has also been reported [76, 125]. Diagnostic work-up should include serological tests in search for anti-nuclear antibodies (ANA), anti-double-stranded DNA (anti-dsDNA) antibodies and antiphospholipid antibodies. CSF analysis shows mild to moderate pleocytosis and mild disruption of the blood–brain barrier. Severity of neurological impairment during myelitis is a prognostic marker for long-term outcome [154]. Overlap syndromes with NMOSD are reported [154] and testing for AQP4 antibodies is recommended [85].
1.6.4 Behçet’s Disease
Behçet’s disease as another chronic, multisystem, inflammatory disorder is characterised by a small vessel vasculitis [24]. The clinical picture is dominated by recurring aphthous stomatitis, genital ulceration, uveitis and arthropathy [40]. Neurological manifestations commonly involve the basal ganglia and brainstem and occur in up to a third of the patients [2]. In approximately 10 % of Behçet cases with neurological manifestation, spinal cord involvement is reported. LETM can also be the sole presentation of neuro-Behçet’s disease [39]. Myelitis associated with Behçet’s disease often presents as longitudinally extensive [58, 190, 201]. Outcome of Behçet-associated myelitis is often poor. Early and aggressive immunosuppressive treatment is critical [98].
1.6.5 Mixed Connective Tissue Disease
Spinal cord affection in conjunction with mixed connective tissue (MCTD) disease is extremely rare, has only been reported in single case studies and often presents as transverse myelitis in the thoracic cord [16]. Neurological complications occur in about 10 % of patients with MCTD and are most commonly peripheral neuropathies, meningitis, psychosis and convulsions [126].
1.6.6 Systemic Sclerosis
Only few cases of myelitis associated with systemic sclerosis have been reported [110, 182]. Neurological complications of systemic sclerosis are uncommon and usually present as myopathy or neuropathy of cranial or peripheral nerves. Rarely, the CNS or spinal cord is afflicted, the latter as compressive (secondary to osteolysis, calcific deposits or facet arthropathy) or non-compressive transverse myelopathy [6, 110]. MRI, CSF and clinical evaluation support the diagnosis of myelitis, and immunosuppressive therapies are used for remission induction.
1.6.7 Vasculitis
The clinical presentation of spinal cord disease associated with vasculitis can range from mild myelitis to severe necrotising myelopathy. Most common causes are SLE, Behçet’s disease and Sjögren’s syndrome (see above). Single cases of myelitis in patients with pANCA-associated vasculitis [71], urticarial vasculitis [20] and immune-complex allergic vasculitis [129] have been described. In one 65-year-old man with systemic pANCA-associated vasculitis, MRI showed patchy cord enhancement from T10 to the conus, remitting after steroid therapy [71]. Usually pANCA-positive Wegener’s granulomatosis only affects the brain, meninges and cranial nerves.
1.6.8 Antiphospholipid Syndrome
The antiphospholipid syndrome (APS) is a systemic autoimmune disorder characterised by presence of antiphospholipid antibodies, recurrent thrombosis and obstetrical morbidity. Neurological manifestations of APS are mainly thrombotic and include stroke, transient ischaemic attack, Sneddon’s syndrome, neuropsychological deficits and peripheral neuropathy [146]. In a systemic review covering the literature from 1966 to 2010, 14 cases of APS and simultaneous transverse myelitis were identified [147]. The causal relationship is unclear, particularly since a comorbidity of APS and NMOSD was reported [82, 121] and the presented cases remained untested for AQP4 antibodies.
1.7 Paraneoplastic Myelopathies
Myelopathies occurring in association with cancer are rare. Spinal cord paraneoplastic syndromes include inflammatory, necrotising or demyelinating myelitis, which may have a focal, transverse or longitudinally extensive dissemination [42]. Myelitis can be accompanied by motor neuron disease, subacute motor neuronopathy or stiff-person syndrome.
The diagnosis of a paraneoplastic myelitis is made by exclusion of other autoimmune or infectious causes of myelitis and CSF or imaging findings supporting acute inflammation, i.e. CSF pleocytosis and IgG index elevation, as well as gadolinium enhancement. Cancers and paraneoplastic antibodies commonly associated with myelitis include small cell lung carcinoma (anti-Hu, anti-Ri, anti-amphiphysin, anti-CRMP5/CV2, anti-GAD, P/Q and N type calcium channel antibodies), breast carcinoma (anti-PCA1, anti-amphiphysin) and ovarian cancer (anti-Ri) [84, 120]. Additionally, AQP4 antibodies are sometimes found positive, particularly in patients with breast carcinoma and in the elderly [130, 140]. Hence, LETM in the context of NMOSD can also represent a cancer-associated aetiology. Other cancers associated with AQP4 antibodies include lung, thymic and cervical carcinomas, leiomyosarcoma and lymphomas. Apart from cancers, demyelinating myelopathy was also described as a rare manifestation of graft-versus-host disease [63]. The paraneoplastic form of stiff-person syndrome occurs in 5–10 % of patients; is characterised by rapidly evolving pain, rigidity and stiffness; and is frequently associated with anti-amphiphysin, anti-GAD65 or anti-glycine receptor antibodies.
Paraneoplastic myelitis is often progressive and may lead to wheelchair dependency and death [57]. Acute paraneoplastic myelitis is treated with high-dose corticosteroids, intravenous immunoglobulins and therapeutic plasma exchange and stiff-person syndrome additionally with antispasticity drugs. Therapy of the underlying tumour is the most important long-term treatment; however, since relapses and progressive courses occur, additional immunosuppressive treatment is often needed.
1.8 Para-/Postinfectious Myelitis
Myelitis can be associated with concomitant or antecedent viral, rarely bacterial, infections [149]. Patients typically report an upper respiratory tract infection or a nonspecific febrile illness. Para-/postinfectious myelitis may present as isolated, mostly transverse myelitis, or together with a more widespread encephalomyelitis and can range from mild urinary symptoms from a conus/epiconus lesion [143] to severe ADEM and even involvement of the whole peripheral and central nervous system (“encephalomyeloradiculopathy”) [114]. An immune-mediated mechanism, i.e. bystander activation or molecular mimicry, is thought to be the pathogenic mechanism. Specific causes of para-/postinfectious myelitis are discussed under the individual pathogens involved. Typical are herpes viruses, orthomyxo- and paramyxoviruses (influenza, measles, mumps) and rubella virus. As with idiopathic transverse myelitis, diagnosis depends on spinal MRI, typically showing gadolinium enhancement and an inflammatory CSF with pleocytosis, abnormal IgG index and sometimes oligoclonal bands but absent pathogen or specific antibody index. Steroid pulse therapy and plasma exchange are used for remission induction, intravenous immunoglobulins in cases with contraindications for these therapies [172]. Since para-/postinfectious myelitis usually is monophasic, long-term immunosuppressive therapy is rarely needed.
1.9 Myelitis After Vaccination and as Complication of Immunotherapy
Neurological complications of vaccinations are rare [123]. LETM with local oedema and axonal motor neuropathy was described in a 77-year-old Japanese woman after vaccination against A/H1N1 influenza [156]. In a systematic review of PubMed, EMBASE and DynaMed, 37 cases of transverse myelitis associated with previous vaccinations were found for a period from 1970 to 2009 [1]. Cases were associated with vaccines against hepatitis B, measles–mumps–rubella, diphtheria–tetanus, rabies, poliovirus, influenza, typhus, pertussis and Japanese B encephalitis in decreasing order and typically occurred in the first month after vaccination.
Therapeutic inhibition of the tumour necrosis factor (TNF)-α is associated with CNS demyelination [46, 202]. In a review of 33 patients with neurological complaints which occurred within a median of 10 months after initiation of anti-TNFα agents, 22 had CNS involvement, 16 with encephalitic lesions, 5 with optic neuritis and 8 with transverse myelitis [169]. CSF and evoked potentials frequently are abnormal in patients with CNS involvement. Myelitis associated with anti-TNFα agents usually is monophasic, but relapsing episodes with final diagnosis of multiple sclerosis have been described. Consequently, anti-TNFα therapy should be discontinued when demyelinating myelitis occurs.
Both myelitis after vaccination and as complication of immunotherapy lack specific clinical and ancillary findings. It is discussed controversially whether the temporal association of vaccinations and anti-TNFα therapies with myelitis indicates a causal relationship, triggering of an underlying disease process, or occurs merely by chance.
1.10 Diagnostic Work-Up
Patients presenting with signs and symptoms of acute autoimmune or immune-mediated spinal cord affection should be immediately subjected to MRI of the complete spinal axis. First priority is to rule out a compressive aetiology [184]. The appearance and longitudinal extension of intramedullary lesions can guide diagnosis (Table 6.2). Further diagnostic testing (Table 6.3) should include CSF analysis, blood testing and cranial MRI, since most of these diseases can affect the brain as well [162]. A CSF pleocytosis with a cell count over 50 cells/μl should prompt the consideration of an infectious cause (see below), even though a high CSF cell count does not exclude an autoimmune inflammatory aetiology, particularly NMOSD, or even a neoplastic disorder. Additional blood testing aims to find systemic disorders such as SLE, Sjögren’s syndrome or sarcoidosis. A neurological involvement of these disorders should be considered in the setting of a positive serology and typical clinical presentation. The presence of a paraneoplastic antibody should prompt the search for the primary tumour using appropriate imaging techniques and a whole body FDG-PET scan where available. FDG-PET scanning can also be helpful to detect inflammatory lymph nodes in the setting of systemic sarcoidosis.
1.11 Therapeutic Strategies
With the exception of MS where additionally immunomodulatory therapies are used, treatment of spinal cord manifestations of autoimmune disorders is immunosuppressive. For acute attacks, high-dose methylprednisolone pulses are first line, sometimes to be followed by therapeutic plasma exchange, immunoadsorption or intravenous immunoglobulins (Table 6.4). When no complete recovery is achieved, immunosuppressive therapy, e.g. with rituximab, cyclophosphamide or mitoxantrone may be used for further remission induction. In the majority of autoimmune spinal cord diseases, the risk of a relapsing course is given; therefore, long-term treatment is required.
2 Myelitis Caused by Pathogens
2.1 Introduction
Infections with viruses, bacteria, spirochaetales, fungi, protozoa or helminths can affect the spinal cord, nerve roots and adjacent structures, frequently resulting in severe long-term sequelae [13]. Herpes virus transverse myelitis and the tick-transmitted diseases neuroborreliosis and tick-borne encephalitis are the most common causes of infectious myelitis in Central Europe, whereas worldwide myelitis caused by enteroviridae (e.g. poliomyelitis or enterovirus) and spinal neurocysticercosis are more frequent. While most pathogens can cause acute myelitis, which represents a medical emergency, chronic myelitis or myelopathy with symptoms evolving over weeks or months is mostly restricted to retroviruses. Table 6.5 summarises the most common pathogens causing myelitis and their endemic regions.
2.2 Herpes Family Viruses
Members of the herpes family viruses are capable of invading the CNS and infect particularly neurons. They establish a latent and life-long persisting infection in the dorsal root ganglia (review in [174]). These viruses can cause myelitis by primary infection and/or reactivation and probable spread to the spinal cord [81].
2.2.1 Herpes Simplex Virus
Herpes simplex virus (HSV) type 1 is the most common cause of infectious myelitis. HSV-1 myelitis can be subacute or chronic and mostly presents as monosegmental myelitis. Predisposing factors are diabetes mellitus, malignancies and conditions compromising the immune system, for example, immunosuppressive therapy or HIV infection. Nevertheless, not always an underlying condition can be found in individuals with herpes myelitis. Diagnostic work-up should particularly involve analysis of cerebrospinal fluid, normally exhibiting a mild pleocytosis (between 10 and 200 cells/μL) and mild disruption of the blood–brain barrier. Detection of viral DNA by polymerase chain reaction (PCR) in the CSF is the most important diagnostic step and helps to identify the causative agent. Importantly, PCR analysis can be negative for the first days after reactivation/infection. Therefore, the repeated analysis of the humoral immune response in the CSF can be helpful. The appearance of a positive CSF/serum antigen-specific index (ASI) is projected after 7 days of infection. Therapy includes high-dose aciclovir (10 mg/kg body weight IV, three times a day) for at least 14 days. Outcomes are variable; complete recovery is possible. Reoccurrence has been reported in up to 20 % of cases [31].
2.2.2 Varicella Zoster Virus
Reactivation of varicella zoster virus (VZV) normally involves a single or more dermatomes and can be accompanied or followed by myelitis (Fig. 6.4). Myelitis can also occur during primary infection. Diagnosis is supported by PCR and antibody analysis in the CSF. Therapy is the same as for HSV myelitis.

VZV myelitis. (a, b) Herpes zoster skin lesion in a 70-year-old man presenting with paraparesis, urinary incontinence and sensory level Th7. T1-weighted (c) sagittal and (d) axial images of the thoracic spinal cord showing a well-demarked focal intramedullary lesion with gadolinium enhancement (Images courtesy of Prof. Erich Schmutzhard, Neurology, and Prof. Elke Gizewski, Neuroradiology, Innsbruck Medical University)
2.2.3 Cytomegalovirus
Cytomegalovirus (CMV) infection/reactivation is particularly observed in immunocompromised individuals. CMV can cause a lumbosacral polyradiculomyelitis and also an LETM [167]. CSF examination reveals a mild to moderate pleocytosis and mild disruption of the blood–brain barrier. Diagnosis is assured by positive PCR amplification of CMV-DNA in the CSF. CMV infection/reactivation can also be monitored by analysis of pp65 antigen levels in peripheral blood samples, particularly in bone marrow transplant recipients [65, 178]. Therapy involves ganciclovir and foscarnet. Prognosis is poor.
2.2.4 Epstein–Barr Virus
Epstein–Barr virus (EBV) is the causative agent of mononucleosis and therefore mostly found in children and young adults. Initial infection can be followed after weeks with signs of a polyradiculomyelopathy. This is most often a postinfectious immune-mediated syndrome, and patients respond well to steroid therapy, which is often given in combination with aciclovir.
2.2.5 Human Herpes Virus
Very rarely, human herpes virus (HHV)-6 and HHV-7 may be the causative agent of myelitis, in particular, as a complication after bone marrow transplantation [4, 195].
2.3 Flaviviruses
Flaviviruses are transmitted by arthropods (ticks, mosquitoes) and have either no (dengue viruses) or well-defined mammalian (tick-borne encephalitis viruses, Japanese encephalitis virus) and/or avian (West Nile virus) hosts. They are subsumed under the term arboviruses, i.e. arthropod-borne viruses. They cause either meningitis, encephalitis with special predilection for basal ganglia, or myelitis in which case they clearly show a predilection of the grey matter, i.e. of the anterior horns, causing a syndrome similar to poliomyelitis [75, 148].
2.3.1 Dengue Viruses
Dengue fever is a common arboviral infection in tropical and subtropical areas. Manifestations are increasingly recognised, but the exact incidence is still unknown [99, 193].
Dengue viruses are transmitted to humans by the bites of infective female Aedes mosquitoes (A. aegypti, A. albopictus, A. scutellaris, A. polynesiensis) with distinct peculiarities in ecology, behaviour and geographical distribution [49]. Infected humans are the primary reservoir, thus serving as the principal source of the virus for uninfected mosquitoes. However, although uncommon, vertical transmission from mother to foetus, transfusion-related transmission, transplantation-related transmission and needle stick-related transmission have been reported.
The clinical manifestations of dengue fever ranges from an asymptomatic state to severe dengue and dengue haemorrhagic shock syndrome, caused by inflammation, capillary leakage and multiorgan impairment. Encephalitis and meningitis are the most frequent CNS manifestations [77]; rarely dengue viruses may cause myelitis, mainly poliomyelitis [5].
Dengue virus-related myelitis presents in MRI as diffuse signal intensity alterations in the spinal cord. Since – as other flaviviridae – dengue viruses mainly affect the grey matter of the spinal cord, particularly anterior horn cells, the acute clinical presentation is flaccid para- or tetraparesis, eventually evolving into spastic para- or tetraparesis [44]. In these cases, myelitis is probably caused by direct viral invasion, as indicated by intrathecal synthesis of dengue IgG antibodies [122, 144]. Diagnosis is confirmed by detection of the virus, viral nucleic acid, antigen or antibodies in the CSF. The level of suspicion is increased by the presence of other laboratory abnormalities as thrombocytopenia, progressive leucopenia and clinical signs of capillary leakage syndrome.
Dengue viral infections of the CNS are managed symptomatically; careful monitoring and maintenance of fluid and electrolyte balance is essential, aggressive management of fever may contribute to success as a neuroprotective measure. Non-steroidal anti-inflammatory agents should not be prescribed since they may aggravate the bleeding diathesis [69].
2.3.2 Tick-Borne Encephalitis Viruses
Up to 30,000 cases of tick-borne encephalitis (TBE) are estimated to occur annually in the European and Asian northern hemisphere [79], thus rendering TBE to the most important and most frequent zoonotic arboviral infection in this region [3]. In nature, TBE virus (TBEV) cycles between infected ticks and small mammals, mainly rodents. Transstadial and transovarial transmission of the virus occur. Beside tick bites, alimentary routes of TBEV transmission – by consuming raw milk or milk products, mainly of goats – are seen.
There are three viral subtypes, the Central European TBEV, the Eastern European subtype and the Siberian/Eastern subtype, the latter two are usually transmitted by Ixodes persulcatus, whereas Ixodes ricinus is the major vector of the Central European TBEV subtype. After the infective tick bite, the virus multiplies at the site of inoculation; dendritic cells of the skin transmit the virus to local lymph nodes from where infected lymphocytes initiate the systemic spread of the infection. Infection of the CNS can occur everywhere, however, most frequently and most intensely involving brainstem, cerebellum, basal ganglia, thalami and spinal cord, where mainly anterior horn cells are infected [18]. Typically, the disease runs a biphasic course; the majority of TBEV infections, however, remain asymptomatic. After an incubation period of 2–28 days, the first stage, i.e. viraemic phase, presents with fever, muscle pains and fatigue. After an afebrile period of several days, the second phase starts mainly with meningitis, encephalitis (in older patients) and in up to 5–15 % with myelitis, most frequently presenting as poliomyelitis with flaccid paresis of the upper limbs [157].
No specific antiviral therapy exists; supportive measurements are most important to assure initial survival in patients with brainstem and encephalomyelitic involvement. CSF and MRI show unspecific changes; the diagnosis is confirmed by specific intrathecal antibody production [177]. Case fatality rate in tick-borne encephalitis depends on the initial clinical presentation being worst in the encephalitic and myelitic form. In Central European TBE, fatality rates are low (<2 %) [92], whereas in Siberian and far Eastern subtypes, fatality rates of >10 % have been reported.
In addition, long-term sequelae after TBE have been reported in 40–50 % in Western [92] and >60 % of patients in far Eastern and Siberian subtypes of disease [92, 177], and only 20 % of patients with TBE myelitis fully recover [91]. Active vaccination is recommended for TBEV-exposed persons in endemic regions.
2.3.3 West Nile Virus
West Nile virus (WNV) has first been described in Eastern Africa (West Nile province in Uganda) from where it has spread throughout the Eastern sub-Saharan African countries, towards Middle East countries, Balkan and, since around 15 years, towards the United States and Canada [68, 133, 164, 165]. Within the past 5 years, South European countries, in particular, Greece and Italy, and most recently even Central European Countries (e.g. Hungary, Italy, Austria) have reported autochthonous cases; [33]. The specific peculiarity of WNV infection is the transmission by mosquitoes, thus rendering WNV to the single most important mosquito-borne disease in temperate climates, e.g. the United States and Central Europe. The course of disease is very similar to TBE; however, in elderly and older subjects, a severe course of WNV neuroinvasive disease, i.e. encephalitis and myelitis, is seen more frequently. As in TBE, the myelitic course of WNV infection is predominated by affection of the anterior horn cells, thereby causing the clinical entity of a poliomyelitis type of disease [107, 113]. The presence of an intrathecal specific antibody production confirms the diagnosis of WNV neuroinvasive disease [45]. Management is supportive and includes all intensive care measures, when necessary [142]. In contrast to TBE, there is no protective vaccine available yet.
2.3.4 Japanese Encephalitis
Japanese encephalitis (JE) occurs in Asian countries ranging from Southeast China towards the Southeast and South Asian countries, including Nepal, India and small pouches in Pakistan. JE virus is transmitted by anopheles mosquitoes; the course is biphasic and frequently leads to encephalitis and also myelitis, where – similar to the other above-mentioned arboviral infections – the anterior horn cells are predominantly affected, thus causing a poliomyelitic course of disease. If the CNS is affected in JE, which occurs in <10 % of cases, the course of disease is much more severe than in TBE or even in WNV encephalitis/myelitis. Case fatality rates of >30 % have been reported [179]. Diagnostic and supportive management strategies are similar to other viral encephalitis and myelitis [90]. A highly efficacious active vaccine exists; travellers to endemic areas, mainly during rainy season, when the mosquito activity is highest, are advised to get this protective vaccination, in particular, if they plan to stay for more than 4 weeks in this endemic area.
2.4 Retroviruses
2.4.1 Human Immunodeficiency Virus
The human immunodeficiency virus (HIV) is a ubiquitously occurring retrovirus accounting for a total of about 37 million infected individuals worldwide (http://www.who.int/gho/hiv/en/ of October 10th, 2016). Already during early infection, HIV can find its way into the CNS and cause an acute transverse myelitis. This is often categorised as an immune-mediated phenomenon and shows a good response to high-dose steroids and the start of antiretroviral therapy [70]. During further course of the disease, more chronic changes in the CNS are observed, particularly as encephalopathies but also as myelopathies. These are often characterised as slowly progressing gait disturbances and have to be distinguished from HIV- or antiretroviral therapy-associated neuropathies. Spinal MRI not always shows abnormalities, sometime only subtle changes of a beginning spinal atrophy or diffuse hyperintensities in the FLAIR and T2-weighted images with longitudinal extent and often restriction to the lateral and posterior thoracic cord [32] (Fig. 6.5). Diagnostic work-up should include exclusion of other infectious causes. Besides antiretroviral therapy regimes, no specific therapy applies for HIV myelopathy.

HIV myelopathy. T2-weighted (a) cervical and (b) thoracic spinal MRI of a 43-year-old woman with a known HIV infection and a progressive paraparesis and gait ataxia are shown. (c, d) Note the longitudinal hyperintensities along the complete spinal cord with a restriction to the lateral and posterior cord. Lines indicate the sectional plane position of the axial images. Gadolinium enhancement was not found (images not shown) (Images courtesy of Dr. Peter Raab, Neuroradiology, Hannover Medical School)
2.4.2 Human T-Cell Lymphotropic Virus Type 1
Human T-cell lymphotropic virus type 1 (HTLV-1) is endemic in Japan, sub-Saharan Africa, the Middle East, the Caribbean and Central and South America. Rarely sporadic cases are also observed in Europe and North America. HTLV-1 can cause a chronic meningomyelopathy. Diagnosis is based on MRI findings showing T2 longitudinal hyperintensities in the posterior and lateral columns of the cervical and thoracic cord as well as cord atrophy [101] and on CSF findings with mild pleocytosis, mild blood–brain barrier disruption and detection of HTLV-1 intrathecal antibody production. Treatment can only be symptomatic as a specific antiretroviral treatment does not exist.
2.5 Other Viruses
2.5.1 Poliomyelitis Viruses and Enteroviruses
Poliomyelitis viruses – being the aim of a global eradication campaign initiated in the early 1990s by the WHO – and a wide range of enteroviruses are small RNA viruses which are transmitted via the feco-oral route. It is mainly the fecal contamination of the environment [17] and the water supplies which constitute the major transmission pathways, rendering the envisaged global eradication of wild-type poliovirus so difficult and a major technical and political challenge [62, 124].
Poliomyelitis still exists in Afghanistan, Pakistan, parts of India, Nigeria, Somalia and parts of northern Kenya; most recently wild-type virus has been detected in Israel [93, 104] and a small epidemic has also been reported from war-stricken Syria. Three serotypes of wild-type polioviruses exist in nature, all of them similarly transmissible and potentially causing disease in man.
The course of disease in case of poliomyelitis virus infection may be rather diverse, ranging from unspecific flu-like signs and symptoms being associated with gastrointestinal discomfort – in the majority of cases – to most severe courses with encephalitis and poliomyelitis, i.e. anterior horn cell myelitis. Such patients develop acute flaccid mono-, para- or tetraparesis, frequently associated with painful radiculitis. In the initial phase, the flaccid paresis may be associated with loss of deep tendon reflexes, leading to rapid atrophy of muscles, being associated with joint contractures, shortening of tendons and inability to normal development of the limbs. In areas where the disease has been almost eradicated, newly developing epidemics might affect not only children but also younger adults.
In an Australian cohort, out of more than 1300 isolates from patients suffering from acute poliomyelitis, 53 % were confirmed as Sabin vaccine like poliomyelitis virus, 41 % were non-polio enteroviruses and 6 % other enteroviruses. This finding indicates that outside the known geographical foci in Afghanistan, Pakistan, Nigeria, Somalia and Kenya, the occurrence of poliomyelitis is very rarely due to a wild-type poliovirus (serotypes 1, 2, 3) but mostly due to Sabin vaccine like poliovirus or non-polio enterovirus (mainly enterovirus 68,69,70). In rare cases, also Coxsackie viruses and other enteroviruses may cause a poliomyelitis-type disease [117]. Enteroviruses 69, 70 and 71 caused epidemics of viral haemorrhagic conjunctivitis; in such an epidemiologic and clinical setting, polio-like signs can be usually attributed to these enteroviruses [33, 116, 134, 135].
Poliomyelitis due to wild-type polioviruses can easily be prevented by vaccines, both oral and parenteral (Sabin and Salk vaccines, respectively). Rarely, the oral polio vaccine (Sabin) may cause a wild-type polio-like disease in immunocompromised patients (e.g. pregnant women) if these patients get infected via the feco-oral route or contact (feco-oral contact) with newly vaccinated children. However, this oral polio vaccine strategy has contributed and still contributes to a very high level of herd immunity; therefore, it is still widely used in the global polio eradication campaign.
2.5.2 Rabies Virus
Rabies is a fatal infectious disease of the nervous system, mainly transmitted to humans and animals through bites of rabid animals, in particular dogs, foxes and bats. In up to 20 %, rabies runs an atypical paralytic form, difficult to distinguish from Guillain–Barré syndrome (GBS) or myelitis. The diagnosis of this course of disease is particularly difficult when the history is concealed or not remembered anymore. The latter fact can easily be understood since the incubation period of rabies may be months or even years. Imaging of rabies myelitis has been shown to involve mainly the grey matter of the spinal cord, very similar to poliomyelitis. The white matter is relatively spared [51, 191]. Nevertheless, a clear-cut neuroimaging clue does not exist; therefore, the appropriate history and a high level of suspicion are necessary to timely diagnose the flaccid (=silent) form of rabies. This is of utmost importance since rabid humans are equally infective as are rabid animals. The prognosis of any type of rabies is bleak, i.e. invariably fatal.
2.5.3 Mumps, Measles, Rubella and Influenza Viruses
All these viral diseases have been shown to cause in rare cases involvement of the spinal cord by direct viral invasion [171]. However, more frequently postinfectious/parainfectious diseases are seen [7, 23, 36]. The diagnosis is made easily if the clinical entity of the respective viral disease (mumps, measles, etc.) is clearly associated with the myelitic signs and symptoms and within the epidemiologic setting of a measles, mumps [8] or influenza outbreak [199].
2.5.4 Hepatitis Viruses
Single cases of myelitis have been reported in or after infection with hepatitis A, B and C virus [170]. Detection of viral DNA or RNA in the CSF [80, 176] or of a specific intrathecal antibody production [56, 97] is diagnostic.
2.6 Neuroborreliosis
Borrelia burgdorferi is the causative agent of neuroborreliosis or Lyme disease. It is transmitted by the Ixodes tick species and endemic in the northern hemisphere (Europe, North America) and Asia. Early infection usually shows dermatological changes at the site of the tick bite with an erythema chronicum migrans. In the next stage (stage II), mainly cranial nerve palsies (typically N. VII) and painful meningoradiculitis (Bannwarth’s syndrome) are observed. Transverse myelitis can be a rare manifestation in this stage (Fig. 6.6). It represents less than 5 % of all cases of neuroborreliosis in larger series [72, 131]. A more chronic and progressive myelopathy in late neuroborrelioses has also been described [31]. Neuroborreliosis has no specific MRI abnormalities, with multiple sclerosis being a common differential diagnosis. Diagnosis is based on CSF analysis showing a mild to moderate pleocytosis, often with mixed cytology, and high amounts of plasma cells and elevated levels of CXCL13 in the CSF [127, 151, 168]. Calculation of specific intrathecal antibody synthesis against Borrelia burgdorferi using ELISA screening tests and Western Blot validation is pertinent for the diagnosis of neuroborreliosis. Serum/blood testing alone is not sufficient. A missing pleocytosis but signs of intrathecal antibody synthesis should be interpreted with caution and are most often evidence for a history of infection. Therapy of choice is IV ceftriaxone for at least 14–21 days, in stage II oral doxycycline (100 mg twice daily) for 14 days can also be chosen [50]. With adequate antibiotic therapy, there is often a full recovery of myelitis.

Neuroborreliosis. This 37-year-old man had a yearlong history of a progressive gait disturbance when presenting for diagnostic work-up. The spinal MRI disclosed a multisegmental myelitis and meningoradiculitis with gadolinium enhancement of the meninges and anterior and posterior horn roots (arrows). (a, c) T2w-TSE images, (b, d) T1w-SE images with gadolinium. CSF revealed a pleocytosis and signs of an intrathecal antibody synthesis against Borrelia burgdorferi. After 3 weeks of IV ceftriaxone, the patient made a full clinical and radiological recovery (Images courtesy of Dr. Peter Raab, Neuroradiology, Hannover Medical School)
2.7 Neurosyphilis
Clinical picture and manifestation of an infection of the CNS with Treponema pallidum are manifold. The most frequently reported clinical manifestation in a Dutch survey was tabes dorsalis [41]. Individuals with tabes dorsalis show sensory gait ataxia and lancing pains. MRI reveals cord atrophy and often hyperintensities in the dorsal roots and posterior columns of the lower thoracic cord [136]. Diagnosis is based on serological and CSF findings demonstrating an intrathecal antibody production. Particularly, the diagnosis is certain with a positive CSF VDRL testing [74]. If the VDRL is negative, a positive FTA-ABS associated with raised CSF cell count, protein or IgG index is a useful method of identifying neurosyphilis [181]. Therapy is long-term and high-dose IV penicillin.
2.8 Bacterial Infections of the Spinal Cord
2.8.1 Mycobacteria
Infection with Mycobacterium tuberculosis is second only to HIV/AIDS as the greatest killer worldwide due to a single infectious agent. In 2014, 9.6 million people fell ill with tuberculosis, and 1.5 million died from it. Over 95 % of the deaths occurred in low- and middle-income countries, but tuberculosis has increasingly been diagnosed also in the developed countries and is becoming a major disease burden (http://www.who.int/gho/tb/en/ of October 10th, 2016). Infection of the CNS with Mycobacterium tuberculosis or Mycobacterium avium is most commonly meningitis, but intramedullary or intradural extramedullary tuberculomas have been observed [185]. CSF examination typically reveals mild to moderate pleocytosis and severe disruption of the blood–brain barrier. Specific pathogen diagnostics are possible with culture and PCR amplification techniques. Treatment has to be long term starting with a quadruple tuberculostatic therapy (for up to 6 months) and then continuing with a triple therapy for a total of up to 2 years. A rarely described and poorly understood clinical entity is the mycobacterial myelopathy, most likely direct intramedullary infection playing the major part of pathogenicity. Steroid therapy has been shown to be not more effective than long duration of mycobacterial chemotherapy, most likely being necessary for a minimum of 2 years [53].
2.8.2 Mycoplasma, Chlamydophila and Bartonella
Mycoplasma pneumoniae and Chlamydophila spp. (e.g. Chlamydophila pneumoniae, Chlamydophila psittaci) may cause parainfectious myelopathies. In rare cases, direct invasion of the endothelial cells of arteries and arterioles serving the spinal cord has been described [66, 200]. Only few cases of myelitis presenting as Brown-Sequard syndrome have been described after cat scratch disease due to Bartonella henselae [25]. Long-term antibiotic therapy with doxycycline, macrolide antibiotics or gyrase inhibitors is needed; however, the evidence on efficacy, duration of therapy and long-term sequelae is scarce [188].
2.8.3 Brucella
Infection by one of the four main subtypes of Brucella spp. causes the zoonotic brucellosis. Brucella melitensis, Brucella abortus Bang and Brucella suis (in recent years also Brucella ovis) cause a systemic infectious disease; the bacteria are transmitted to humans from infected animals, e.g. goats, sheep, pigs, cows or camels. High-risk areas include mainly the Middle East/Mediterranean region but also Central and South America and sub-Saharan Africa. Infection occurs usually by consumption of unpasteurised milk or milk products, but also veterinarians, butchers, hunters or laboratory workers are at risk. After a prolonged generalised disease with anorexia, headache, myalgia and intermittent undulating fever, organ malfunction and involvement of the CNS may occur [37]. One of the most frequent and most serious complications of Brucella spp. infection is spondylitis which may occur in up to 50 % of cases with systemic infection [95]. Lesions may affect all levels of the vertebral spine, most commonly however, the lumbar spine at the level L4–L5 [61]. Adjacent granuloma and abscess formation causes epidural space-occupying lesions and compression of the spinal cord and nerve roots. Granuloma may also develop within the spinal cord. The diagnosis is based upon clinical history, history of exposure and a long-standing preceding generalised disease, local pains and focal neurological findings. Diagnosis is supported by serology, blood culture and culture from biopsies. Isolation of bacteria from tissue and blood is successful in up to 70 % of cases. Beside neurosurgical decompression, treatment of neurobrucellosis comprises of an antimicrobial chemotherapeutic combination of rifampicin and doxycyclin, minimum 6 weeks. To avoid common relapses, intramuscular streptomycin has been recommended to be added in myelitis, spondylitis or endocarditis [106]. Seroconversion, negative blood cultures and improvement in neuroimaging and of clinical signs and symptoms indicate resolution of the disease, supporting the decision to stop the combination antimicrobial chemotherapy.
2.8.4 Listeria Monocytogenes, Staphylococci and Streptococci
Listeria monocytogenes, staphylococci and streptococci have been described to cause – in rare cases – intramedullary infection, including abscess formation. The direct visualisation of the pathogenic agent by computed tomography-guided biopsy allows the diagnosis, including microbiological work-up of the material, and appropriate therapy [26, 128].
2.9 Schistosomiasis
Parasitic or fungal causes of myelitis are rare but should be considered when myelitis occurs in habitants or travellers in endemic regions [161]. Schistosoma are endemic in Central and South America (Schistosoma mansoni) and sub-Saharan Africa (Schistosoma mansoni and Schistosoma haematobium). Myelopathy of the lumbosacral region is the most common neurological complication of Schistosoma mansoni and Schistosoma haematobium infection [54]. MRI shows longitudinal extensive myelitis and cord swelling and heterogeneous contrast enhancement [55] (Fig. 6.7). Specific diagnosis can be based on serological testing, evidence of Schistosoma infection and identification of parasite antigens in blood or CSF [64]. Therapy consists of praziquantel and steroids. Complete or partial recovery is observed in most of the patients. Early diagnosis and prompt treatment are essential [150].

Schistosomiasis. A 24-year-old male Brazilian student was visiting Germany when developing a conus/cauda syndrome. The spinal MRI shows a longitudinal myelitis with predominant involvement of the conus medullaris with patchy gadolinium enhancement. Diagnosis of schistosomiasis was based on positive Schistosomiasis mansoni antibody testing. A full recovery was achieved by treatment with praziquantel. (a, c) T2w-TSE images, (c, d) T1w-SE images with gadolinium (Images courtesy of Dr. Peter Raab, Neuroradiology, Hannover Medical School)
2.10 Eosinophilic Radiculomyelitis Caused by Nematode Larvae Migrantes
Third-stage larvae of Gnathostoma spinigerum (Southeast Asia), Angiostrongylus cantonensis (Southeast Asia), Angiostrongylus costaricensis (Central America), Toxocara canis (worldwide) and Baylisascaris procyonis (North America) have the capacity to cause the clinical entity of a larva migrans syndrome [115, 159]. Potentially, the larvae invade the subarachnoid space, radices and myelon [52, 83, 96, 152, 158]. The disease is characterised by usually acute, rarely subacute, onset of radicular or intramedullary signs and symptoms [78]. Human infection by the nematode larva of Gnathostoma spinigerum results from eating raw fish, snails, shrimps, frogs or insufficiently cooked chicken or duck meat contaminated with larvae of this parasite [148, 158]. Dogs, cats and pigs are the definitive hosts. After ingestion, the highly motile larvae migrate through all deep and subcutaneous tissues with specific neurotropism. Whereas Gnathostoma spinigerum frequently causes long haemorrhagic tracts from nerve roots to the myelon and even brainstem, all the other larvae migrantes only rarely invade the brainstem or myelon [108, 189]. If they do, the onset and course of disease is less fulminant, frequently also accentuated by granuloma formation [132]. This might create difficulties in differentiating such a granuloma from a tumour, tuberculoma, etc. Typically, eosinophilia is found to be more pronounced in gnathostomiasis but may also be present in the other nematode larval meningitis or myelitis manifestations [94]. Albendazole may be used to kill these larvae migrantes; however, concomitant steroid therapy might be necessary to alleviate toxic or allergic reactions with clinical deterioration.
2.11 Neurocysticercosis
Involvement of the spinal cord by the larvae of Taenia solium (pig tapeworm) is very rare, even in endemic areas, such as Latin America, sub-Saharan Africa or South and Southeast Asia. If humans ingest Taenia eggs (due to fecal contamination of food, water or autoinfection in case of intestinal taeniasis), they become intermediate hosts, thus being prone to develop the clinical entity of cysticercosis. In tropical areas, up to 50,000 deaths are attributed to neurocysticercosis, mainly due to intracranial cyst formation, leading to severe encephalitic brain oedema, space-occupying lesions and epilepsy, even intractable status epilepticus [47]. In less than 0.2 % of infections, the spinal canal or the spinal cord is involved; usually the space-occupying effect of the cysticercal cysts is responsible for spinal neurocysticercosis. Spinal neurocysticercosis may be associated with cauda equina or Brown-Sequard syndrome, and CSF findings might be similar as in eosinophilic meningitis [183]; however, in pure cyst formation, eosinophilia may also be absent. The diagnosis is confirmed by neuroimaging and serology, which should include ELISA for cysticercus cellulosae antigen thereby confirming an active neurocysticercosis [59]. Anthelmintic therapy is – at least in cerebral neurocysticercosis – a combination therapy with praziquantel and albendazole. Concomitant dexamethasone administration should begin prior to the anthelmintic therapy and should be prolonged for up to a week beyond the termination of anthelmintic drugs. In specified cases, neurosurgical intervention might be necessary.
2.12 Fungal Myelopathies
Involvement of the spinal cord with fungal pathogens is exceedingly rare [100]. Both compressive myelopathy due to vertebral osteomyelitis and granulomatous meningitis and spinal cord infarction due to meningovascular infiltration [139] have been described in patients with Blastomyces, Histoplasma, Coccidioides immitis, Aspergillus spp., Candida spp. and Cryptococcus spp. infection [21, 28, 43, 67, 87, 118, 137, 145, 153]. Direct visualisation of the pathogenic agent is essential to allow for the best possible specific antimycotic chemotherapy [73, 160]. No evidence is available as to dosage and duration of antimycotic chemotherapy. Recently, in the United States, direct inoculation of an otherwise non-pathogenic fungus into the subarachnoid space by contaminated steroid injections has caused an epidemic of Exserohilum rostratum CNS infections [27, 29].
2.13 Diagnostic Work-Up
The diagnostic work-up of pathogen-caused myelitis is following the same routines as for immune-mediated myelitis. Besides early gadolinium-enhanced MRI of the spinal cord to rule out a compressive aetiology, the analysis of the CSF is the cornerstone of the diagnostic work-up. A pathogen-driven myelitis should be suspected in cell counts >50 cells/μL. Pleocytosis and a disruption of the blood–brain barrier are often observed. PCR amplification of viral DNA or RNA allows specific identification of the causative agent [173]. The additional analysis of the humoral response and the calculation of an antigen-specific antibody index as sign for a specific intrathecal immunoglobulin production are helpful, particularly in PCR-negative settings. Bacterial pathogens are mostly identified by culture of the CSF or when bacteraemia is present in blood cultures. In addition, PCR amplification is helpful in identifying infections with mycobacteria. Analysis of the humoral response and calculation of an antigen-specific antibody index are essential for the diagnosis of neuroborreliosis and neurosyphilis (see above).
2.14 Therapeutic Strategies
Therapeutic strategies are first of all anti-infective. Depending on the identified pathogens, antiviral, antibiotic, antiparasitic or antifungal treatment regimens have to be chosen (details listed above). Concomitant steroids can be given in most of the pathogen-caused myelitis cases [119].
Conclusions
Myelitis can be caused by infections, autoimmunity and other immune-mediated mechanisms including para-/postinfectious and paraneoplastic aetiologies. Differential diagnosis is guided by clinical history, neurological examination, CSF analysis and spinal MRI. Due to advances in imaging and laboratory techniques, particularly identification of new autoantibodies and methods for humoral and nucleic acid detection of pathogens, these diseases are increasingly diagnosed in clinical practice. Infectious and autoimmune myelitis are associated with significant morbidity and mortality and often account for severe neurological deficits and long-term sequelae; therefore, early and specialised multidisciplinary care are recommended.
References
Agmon-Levin N, Kivity S, Szyper-Kravitz M, Shoenfeld Y (2009) Transverse myelitis and vaccines: a multi-analysis. Lupus 18(13):1198–1204
Akman-Demir G, Serdaroglu P, Tasci B (1999) Clinical patterns of neurological involvement in Behcet’s disease: evaluation of 200 patients. The Neuro-Behcet Study Group. Brain 122:2171–2182
Amato-Gauci A, Zeller H (2012) Tick-borne encephalitis joins the diseases under surveillance in the European Union. Euro Surveill 17(42):1–2
Aoki K, Arima H, Kato A et al (2012) Human herpes virus 6-associated myelitis following allogeneic bone marrow transplantation. Ann Hematol 91:1663–1665
Araújo FM, Araújo MS, Nogueira RM et al (2012) Central nervous system involvement in dengue: a study in fatal cases from a dengue endemic area. Neurology 78:736–742
Averbuch-Heller L, Steiner I, Abramsky O (1992) Neurologic manifestations of progressive systemic sclerosis. Arch Neurol 49(12):1292–1295
Bale JF (2014) Measles, mumps, rubella, and human parvovirus B19 infections and neurologic disease. Handb Clin Neurology Vol 121 (3rd series). In: Jose B, Ferro JM (eds) Neurologic aspects of systemic dis part II. Elsevier, Amsterdam, Netherlands, 1345–1413
Bansal R, Kalita J, Mirsra UK, Kishore J (1998) Myelitis: a rare presentation of mumps. Pediatr Neursurg 28:204–206
Banwell B et al (2008) Neuromyelitis optica-IgG in childhood inflammatory demyelinating CNS disorders. Neurology 70:344–352
Bhat A, Naguwa S, Cheema G, Gershwin ME (2010) The epidemiology of transverse myelitis. Autoimmun Rev 9(5):A395–A399
Baumann M, Sahin K, Lechner C, Hennes EM, Schanda K, Mader S et al (2015) Clinical and neuroradiological differences of paediatric acute disseminating encephalomyelitis with and without antibodies to the myelin oligodendrocyte glycoprotein. J Neurol Neurosurg Psychiatry 86(3):265–272
Bennett JL, Lam C, Kalluri SR et al (2009) Intrathecal pathogenic anti-aquaporin-4 antibodies in early neuromyelitis optica. Ann Neurol 66:617–629
Berger JR, Sabet A (2002) Infectious myelopathies. Semin Neurol 22:133–141
Berkowitz AL, Samuels MA (2014) The neurology of Sjogren’s syndrome and the rheumatology of peripheral neuropathy and myelitis. Pract Neurol 14(1):14–22
Bertsias GK et al (2010) EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs. Ann Rheum Dis 69:2074–2082
Bhinder S, Harbour K, Majithia V (2007) Transverse myelitis, a rare neurological manifestation of mixed connective tissue disease-a case report and a review of literature. Clin Rheumatol 26(3):445–447
Blake IM, Martin R, Goel A, Khetsuriani N et al (2014) The role of older children and adults in wild poliovirus transmission. Proc Natl Acad Sci U S A 111:10604–10609
Bogovic P, Lotric-Furlan S, Strle F (2010) What tick-borne encephalitis may look like: clinical signs and symptoms. Travel Med Infect Dis 8:246–250
Bolat S, Berding G, Dengler R, Stangel M, Trebst C (2009) Fluorodeoxyglucose positron emission tomography (FDG-PET) is useful in the diagnosis of neurosarcoidosis. J Neurol Sci 287(1–2):257–259
Bolla G, Disdier P, Verrot D, Swiader L, Andrac L, Harle JR et al (1998) Acute transverse myelitis and primary urticarial vasculitis. Clin Rheumatol 17(3):250–252
Bollyky PL, Czartoski TJ, Limaye A (2006) Histoplasmosis presenting as an isolated spinal cord lesion. Arch Neurol 63:1802–1803
Bradl M, Misu T, Takahashi T et al (2009) Neuromyelitis optica: pathogenicity of patient immunoglobulin in vivo. Ann Neurol 66:630–643
Buchanan R, Bonthius DJ (2012) Measles virus and associated central nervous system sequelae. Semin Pediatr Neurol 19:107–114
Calamia KT, Kaklamanis PG (2008) Behcet’s disease: recent advances in early diagnosis and effective treatment. Curr Rheumatol Rep 10:349–355
Carman KB, Yimenicioglu S, Ekici A, Yakut A, Dinleyici EC (2013) Co-existence of acute transverse myelitis and Guillain-Barré syndrome associated with Bartonella henselae infection. Paediatr Int Child Health 33(3):190–192
Castro A, Hernández OH, Uribe CS, Guerra A, Urueña P (2013) Brainstem encephalitis and myelitis due to Listeria monocytogenes: a case report and literature review. Biomedica 33:343–349
Centers for Disease Control and Prevention (CDC) (2013) Spinal and paraspinal infections associated with contaminated methylprednisolone acetate injections – Michigan, 2012–2013. MMWR Morb Mortal Wkly Rep 62:377–381
Chen SC, Slavin MA, Heath CH et al (2012) Clinical manifestations of Cryptococcus gattii infection: determinants of neurological sequelae and death. Clin Infect Dis 55:789–798
Chiller TM, Roy M, Nguyen D et al (2013) Clinical findings for fungal infections caused by methylprednisolone injections. N Engl J Med 369:1610–1619
Chintamaneni S, Patel AM, Pegram SB, Patel H, Roppelt H (2010) Dramatic response to infliximab in refractory neurosarcoidosis. Ann Indian Acad Neurol 13:207–210
Cho TA, Vaitkevicius H (2012) Infectious myelopathies. Continuum (Minneap Minn) 18(6 Infectious Disease):1351–1373
Chong J et al (1999) MR findings in AIDS-associated myelopathy. Am J Neuroradiol 20:1412–1416
Communicable Diseases Threats Report; ECDC (2014) Outbreak of enterovirus D68 – USA and Canada (Europe) – monitoring season 43:19–25
Communicable Diseases Threats Report; ECDC (2014). West Nile virus-multistate (Europe) – monitoring season 43:19–25
Compston A, Coles A (2002) Multiple sclerosis. Lancet 359(9313):1221–1231
Connolly JH, Hutchinson WM, Allen IV et al (1975) Carotid artery thrombosis, encephalitis, myelitis and optic neuritis associated with rubella virus infections. Brain 98:583–594
Corbel MJ (1997) Brucellosis: an overview. Emerg Infect Dis 3:213–221
Costabel U (2001) Sarcoidosis: clinical update. Eur Respir J Suppl 32:56s–68s
Coulter I, Huda S, Baborie A, Jacob A (2012) Longitudinally extensive transverse myelitis as the sole presentation of neuro-Behcet’s disease responding to infliximab. J Spinal Cord Med 35(2):122–124
Criteria for diagnosis of Behcet’s disease. International Study Group for Behcet’s Disease (1990) Lancet 335:1078–1080
Daey Ouwens IM, Koedijk FD, Fiolet AT, van Veen MG, van den Wijngaard KC, Verhoeven WM, Egger JI, van der Sande MA (2014) Neurosyphilis in the mixed urban–rural community of the Netherlands. Acta Neuropsychiatr 26(3):186–192
Darnell RB, Posner JB (2011) Spinal cord syndromes. In: Darnell RB, Posner JB (eds) Paraneoplastic syndromes. Oxford University Press, New York, pp 149–182
de Morais SS, Mafra Mde O, Canterle EM, de Lima LL, Ribeiro SL (2008) Histoplasmosis mimicking tuberculosis spondylodiscitis in a patient with rheumatoid arthritis. Acta Reumatol Port 33:360–363
de Sousa AM, Alvarenga MP, Alvarenga RM (2014) A cluster of transverse myelitis following dengue virus infection in the brazilian Amazon region. Trop Med Health 42:115–120
Debiasi RL (2011) West nile virus neuroinasive disease. Curr Infect Dis Rep 13:350–359
Defty H, Sames E, Doherty T, Hughes R (2013) Case report of transverse myelitis in a patient receiving etanercept for rheumatoid arthritis. Case Rep Rheumatol 2013:728371
Del Brutto OH, Rajshekhar V, White ACT et al (2001) Proposed diagnostic criteria for neurocysticercosis. Neurology 57:177–183
Delalande S et al (2004) Neurologic manifestations in primary Sjogren syndrome: a study of 82 patients. Medicine (Baltimore) 83:280–291
Dengue and severe dengue: fact sheet N°117 (2014) World Health Organization (WHO), Geneva. (Webpage on the internet (cited 10 July 2014). Available from: http://www.ncbi.nim.nih.gov/pmc/articles/PMC3753061/#!po=64.5833
Dersch R, Freitag M, Schmidt S, Sommer H, Rauer S, Meerpohl J (2015) Efficacy and safety of pharmacological treatments for acute Lyme neuroborreliosis – a systematic review. Eur J Neurol 22:1249–1259
Desai RV, Jain V, Singh P, Singhi S, Radotra BD (2002) Radiculomyelitic rabies: can MR imaging help? AJNR Am J Neuroradiol 23:632–634
Diao Z, Jin E, Yin C (2010) Angiostrongylus cantonensis: lesions in brain and spinal cord. Am J Trop Med Hyg 82(4):519
Feng Y, Guo N, Liu J, Chen XI et al (2011) Mycobacteria infection in incomplete transverse myelitis is refractory to steroids: a pilot study. Clin Dev Immunol 2011:Art ID 501369, 8. doi:10.1155/2011/501369
Ferrari TC, Moreira PR (2011) Neuroschistosomiasis: clinical symptoms and pathogenesis. Lancet Neurol 10(9):853–864
Ferrari TC (2004) Involvement of central nervous system in the schistosomiasis. Mem Inst Oswaldo Cruz 99:59–62
Ficko C, Imbert P, Mechaï F, Barruet R, Nicand E, Rapp C (2010) Acute myelitis related to hepatitis a after travel to Senegal. Med Trop (Mars) 70(1):7–8, French
Flanagan EP, McKeon A, Lennon VA, Kearns J, Weinshenker BG, Krecke KN et al (2011) Paraneoplastic isolated myelopathy: clinical course and neuroimaging clues. Neurology 76(24):2089–2095
Fukae J et al (2010) Subacute longitudinal myelitis associated with Behcet’s disease. Intern Med 49:343–347
Gabriël S, Blocher J, Dorny P, Abatih EN, Schmutzhard E, Ombay M, Mathias B, Winkler AS (2012) Added value of antigen ELISA in the diagnosis of neurocysticercosis in resource poor settings. PLoS Negl Trop Dis 6(10):e1851
Gono T, Kawaguchi Y, Katsumata Y, Takagi K, Tochimoto A, Baba S et al (2011) Clinical manifestations of neurological involvement in primary Sjogren’s syndrome. Clin Rheumatol 30(4):485–490
Görgülü A, Albayrak BS, Görgülü E et al (2006) Spinal epidural abscess due to Brucella. Surg Neurol 66:141–146
Grassly NC (2013) The final stages of the global eradication of poliomyelitis. Philos Trans R Soc Lond B Biol Sci 368(1623):20120140
Grauer O, Wolff D, Bertz H, Greinix H, Kuhl JS, Lawitschka A et al (2010) Neurological manifestations of chronic graft-versus-host disease after allogeneic haematopoietic stem cell transplantation: report from the Consensus Conference on Clinical Practice in chronic graft-versus-host disease. Brain 133(10):2852–2865
Gray DJ, Ross AG, Li YS, McManus DP (2011) Diagnosis and management of schistosomiasis. BMJ 342:d2651. doi:10.1136/bmj.d2651
Greanya ED, Partovi N, Yoshida EM, Shapiro RJ, Levy RD, Sherlock CH, Stephens GM (2005) The role of the cytomegalovirus antigenemia assay in the detection and prevention of cytomegalovirus syndrome and disease in solid organ transplant recipients: A review of the British Columbia experience. Can J Infect Dis Med Microbiol 16(6):335–341
Guleria R, Nisar N, Chawla TC, Biswas NR (2005) Mycoplasma pneumoniae and central nervous system complications: a review. J Lab Clin Med 146:55–63
Gupta R, Kushwaha S, Behera S, Jaiswal A, Thakur R (2012) Vertebro-cerebral cryptococcosis mimicking tuberculosis: a diagnostic dilemma in countries with high burden of tuberculosis. Indian J Med Microbiol 30:245–248
Gyure KA (2009) West Nile virus infections. J Neuropathol Exp Neurol 68:1053–1060
Halstead SB (2007) Dengue. Lancet 370:1644–1652
Hamada Y, Watanabe K, Aoki T et al (2011) Primary HIV infection with acute transverse myelitis. Intern Med 50:1615–1617
Hamilton AJ, Whitehead DJ, Bull MD, D’Souza RJ (2010) Systemic panca-associated vasculitis with central nervous involvement causing recurrent myelitis: case report. BMC Neurol 10:118
Hansen K, Lebech AM (1992) The clinical and epidemiological profile of Lyme neuroborreliosis in Denmark 1985–1990. Brain 115:399–423
Hardjasudarma M, Willis B, Black-Payne C, Edwards R (1995) Pediatric spinal blastomycosis: case report. Neurosurgery 37:534–536
Hart G (1986) Syphilis tests in diagnostic and therapeutic decision making. Ann Intern Med 104:368–376
Hatanpaa KJ, Kim JH (2014) Neuropathology of viral infections. Handb Clin Neurol 123:193–214
Heinlein AC, Gertner E (2007) Marked inflammation in catastrophic longitudinal myelitis associated with systemic lupus erythematosus. Lupus 16:823–826
Hendarto SK, Hadinegoro SR (1992) Dengue encephalopathy. Acta Paediat Jap 34:250–257
Hsu JJ, Chuang SH, Chen CH, Huang MH (2009) Sacral myeloradiculitis (Elsberg syndrome) secondary to eosinophilic meningitis caused by Angiostrongylus cantonensis. BMJ Case Rep 2009. pii: bcr10.2008.1075
Hubálek Z, Rudolf I (2012) Tick-borne viruses in Europe. Parasitol Res 111:9–36
Inoue J, Ueno Y, Kogure T, Nagasaki F, Kimura O, Obara N, Kido O, Nakagome Y, Kakazu E, Matsuda Y, Fukushima K, Segawa H, Nakajima I, Itoyama Y, Takahashi M, Okamoto H, Shimosegawa T (2008) Analysis of the full-length genome of hepatitis B virus in the serum and cerebrospinal fluid of a patient with acute hepatitis B and transverse myelitis. J Clin Virol 41(4):301–304
Irani DN (2008) Aseptic meningitis and viral myelitis. Neurol Clin 26:635–655
Iyer A, Elsone L, Appleton R, Jacob A (2014) A review of the current literature and a guide to the early diagnosis of autoimmune disorders associated with neuromyelitis optica. Autoimmunity 47(3):154–161
Jabbour RA, Kanj SS, Sawaya RA, Awar GN, Hourani MH, Atweh SF (2011) Toxocara canis myelitis: clinical features, magnetic resonance imaging (MRI) findings, and treatment outcome in 17 patients. Medicine (Baltimore) 90:337–343
Jacob A, Weinshenker BG (2008) An approach to the diagnosis of acute transverse myelitis. Semin Neurol 28(1):105–120
Jarius S, Jacobi C, de Seze J, Zephir H, Paul F, Franciotta D et al (2011) Frequency and syndrome specificity of antibodies to aquaporin-4 in neurological patients with rheumatic disorders. Mult Scler 17(9):1067–1073
Jarius S, Ruprecht K, Wildemann B, Kuempfel T, Ringelstein M, Geis C et al (2012) Contrasting disease patterns in seropositive and seronegative neuromyelitis optica: a multicentre study of 175 patients. J Neuroinflammation 9:14
Joshi TN (2012) Candida albicans spondylodiscitis in an immunocompetent patient. J Neurosci Rural Pract 3:221–222
Jounieaux F, Chapelon C, Valeyre D, Israel Biet D, Cottin V, Tazi A, Fournier E, Wallaert B (2010) [Infliximab treatment for chronic sarcoidosis-a case series]. Rev Mal Respir 27:685–692, French
Judson MA (2015) The clinical features of sarcoidosis: a comprehensive review. Clin Rev Allergy Immunol 49:63–78
Kaiser R, Dobler G (2010) Japanese encephalitis and tick-borne encephalitis: similarities and varieties. MMW Fortschr Med 152:44–45
Kaiser R (2011) Long-term prognosis of patients with primary myelitic manifestation of tick-borne encephalitis: a trend analysis covering 10 years. Nervenarzt 82(8):1020–1025
Kaiser R (2012) Tick-borne encephalitis: clinical findings and prognosis in adults. Wien Med Wochenschr 162:239–243
Kaliner E, Moran-Gilad J, Grotto I et al (2014) Silent reintroduction of wild-type poliovirus to Israel, 2013 – risk communication challenges in an argumentative atmosphere. Euro Surveill 19(7):20703
Kanpittaya J, Sawanyawisuth K, Intapan PM, Khotsri P, Chotmongkol V, Maleewong W (2012) A comparative study of neuroimaging features between human neuro-gnathostomiasis and angiostrongyliasis. Neurol Sci 33:893–898
Karaoglan I, Namiduru M, Akcali A, Cansel N (2008) Different manifestations of nervous system involvement by neurobrucellosis. Neurosciences (Riyadh) 13:283–287
Kelly TG, Madhavan VL, Peters JM, Kazacos KR, Silvera VM (2012) Spinal cord involvement in a child with raccoon roundworm (Baylisascaris procyonis) meningoencephalitis. Pediatr Radiol 42:369–373
Khemiri M, Ouederni M, Barsaoui S (2007) A new case of acute transverse myelitis following hepatitis a virus infection. Med Mal Infect 37(4):237–239, French
Kikuchi H, Aramaki K, Hirohata S (2008) Effect of infliximab in progressive neuro-Behcet’s syndrome. J Neurol Sci 272:99–105
Kilpatrick AM, Randolph SE (2012) Drivers, dynamics, and control of emerging vector-borne zoonotic diseases. Lancet 380:1946–1955
Kim CW, Perry A, Currier B, Yaszemski M, Garfin SR (2006) Fungal infections of the spine. Clin Orthop Relat Res 444:92–99
Kira J et al (1991) Leukoencephalopathy in HTLV-1-associated myelopathy/tropical spastic paraparesis: MRI analysis and a two-year follow-up study after corticosteroid therapy. J Neurol Sci 106:41–49
Kitley J, Woodhall M, Waters P, Leite MI, Devenney E, Craig J et al (2012) Myelin-oligodendrocyte glycoprotein antibodies in adults with a neuromyelitis optica phenotype. Neurology 79(12):1273–1277
Kleiter I, Gahlen A, Borisow N, Fischer K, Wernecke KD, Wegner B et al (2016) Neuromyelitis optica: evaluation of 871 attacks and 1153 treatment courses. Ann Neurol 79(2):206–216
Kopel E, Kaliner E, Grotto I (2014) Lessons from a public health emergency-importation of wild poliovirus to Israel. N Engl J Med 371:981–983
Kovacs B, Lafferty TL, Brent LH, DeHoratius RJ (2000) Transverse myelopathy in systemic lupus erythematosus: an analysis of 14 cases and review of the literature. Ann Rheum Dis 59(2):120–124
Krishnan C, Kaplin AI, Graber JS, Darman JS, Kerr DA (2005) Recurrent transverse myelitis following neurobrucellosis: immunologic features and beneficial response to immunosuppression. J Neurovirol 11:225–231
Kropman E, Bakker LJ, de Sonnaville JJ, Koopmans MP, Raaphorst J, Carpay JA (2012) West Nile virus poliomyelitis after a holiday in Egypt. Ned Tijdschr Geneeskd 155(35):A4333
Lee IH, Kim ST, Oh DK, Kim HJ, Kim KH, Jeon P, Byun HS (2010) MRI findings of spinal visceral larva migrans of Toxocara canis. Eur J Radiol 75:236–240
Lennon VA, Kryzer TJ, Pittock SJ, Verkman AS, Hinson SR (2005) IgG marker of optic-spinal multiple sclerosis binds to the aquaporin-4 water channel. J Exp Med 202:473–477
Littman BH (1989) Linear scleroderma: a response to neurologic injury? Report and literature review. J Rheumatol 16(8):1135–1140
Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sorensen PS, Thompson AJ et al (2014) Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology 83(3):278–286
Mader S, Gredler V, Schanda K, Rostasy K, Dujmovic I, Pfaller K et al (2011) Complement activating antibodies to myelin oligodendrocyte glycoprotein in neuromyelitis optica and related disorders. J Neuroinflammation 8:184
Maramattom BV, Philips G, Sudheesh N, Arunkumar G (2014) Acute flaccid paralysis due to West nile virus infection in adults: a paradigm shift entity. Ann Indian Acad Neurol 17:85–88
Marrie TJ, Purdy RA, Johnston BL, McCormick CW, Benstead T, Ansell J et al (1995) Encephalomyeloradiculopathy of infectious or parainfectious etiology-a new entity? Clin Infect Dis 20(4):945–953
Marx C, Lin J, Masruha MR, Rodrigues MG, da Rocha AJ, Vilanova LC, Gabbai AA (2007) Toxocariasis of the CNS simulating acute disseminated encephalomyelitis. Neurology 69:806–807
Mateen FJ, Black RE (2013) Expansion of acute flaccid paralysis surveillance: beyond poliomyelitis. Trop Med Int Health 18:1421–1432
McCarthy M (2014) Outbreak of polio-like illness is reported in California. BMJ 348:g1780
McCaslin AF, Lall RR, Wong AP, Lall RR, Sugrue PA, Koski TR (2015) Thoracic spinal cord intramedullary aspergillus invasion and abscess. J Clin Neurosci 22(2):404–406
McGee S, Hirschmann J (2008) Use of corticosteroids in treating infectious diseases. Arch Intern Med 168(10):1034–1046
McKeon A (2013) Paraneoplastic and other autoimmune disorders of the central nervous system. Neurohospitalist 3(2):53–64
Mehta LR, Samuelsson MK, Kleiner AK, Goodman AD, Anolik JH, Looney RJ et al (2008) Neuromyelitis optica spectrum disorder in a patient with systemic lupus erythematosus and anti-phospholipid antibody syndrome. Mult Scler 14(3):425–427
Miranda de Sousa A, Puccioni-Sohler M, Dias-Borges A et al (2007) Post-Dengue neuromyelitis optica: a case report of a Japanese descendent Brazilian child. J Infect Chemther 19:396–398
Miravalle AA, Schreiner T (2014) Neurologic complications of vaccinations. Handb Clin Neurol 121:1549–1557
Mohammadi D (2014) Polio-like disease in the news: much ado about nothing? Lancet Neurol 13:650–651
Mornas AR, Thomas T, Pallot PB, Chopin F, Raoux D (2010) Longitudinal myelitis in a patient with systemic lupus erythematosus. Joint Bone Spine 77:181–183
Nadeau SE (2002) Neurologic manifestations of connective tissue disease. Neurol Clin 20(1):151–178
Narayan K, Dail D, Li L, Cadavid D, Amrute S, Fitzgerald-Bocarsly P et al (2005) The nervous system as ectopic germinal center: CXCL13 and IgG in lyme neuroborreliosis. Ann Neurol 57(6):813–823
Nguyen-Huu BK, Thümler A, Weisner B et al (2005) Neurolisteriosis with acute myelitis. Nervenarzt 76:1255–1258
Nikol S, Huehns TY, Pilz G, von Scheidt W (1996) Immune-complex allergic vasculitis in association with the development of transverse myelitis. A case report. Angiology 47(11):1107–1110
Ontaneda D, Fox RJ (2014) Is neuromyelitis optica with advanced age of onset a paraneoplastic disorder? Int J Neurosci 124(7):509–511
Oschmann P, Dorndorf W, Hornig C, Schäfer C, Wellensiek HJ, Pflughaupt KW (1998) Stages and syndromes of neuroborreliosis. J Neurol 245:262–272
Ota KV, Dimaras H, Héon E et al (2009) Toxocariasis mimicking liver, lung, and spinal cord metastases from retinoblastoma. Pediatr Infect Dis J 28:252–254
Oyer RJ, David Beckham J, Tyler KL (2014) West Nile and St. Louis encephalitis viruses. Handb Clin Neurol 123:433–447
Pal SR, Dastur DK, Kaiwar R, Prasad SR (1986) Enterovirus-70 antigen in spinal cord cells of patients with poliomyelitis-like illness. Indian J Med Res 83:108–110
Palacios G, Oberste MS (2005) Enteroviruses as agents of emerging infectious diseases. J Neurovirol 11:424–433
Pandey S (2011) Magnetic resonance imaging of the spinal cord in a man with tabes dorsalis. J Spinal Cord Med 34:609–611
Parr AM, Fewer D (2004) Intramedullary blastomycosis in a child: case report. Can J Neurol Sci 31:282–285
Perumal J, Zabad R, Caon C, MacKenzie M, Tselis A, Bao F et al (2008) Acute transverse myelitis with normal brain MRI: long-term risk of MS. J Neurol 255(1):89–93
Pfausler B, Kampfl A, Berek K, Maier H, Aichner F, Schmutzhard E (1995) Syndrome of the anterior spinal artery as the primary manifestation of aspergillosis. Infection 23:240–242
Pittock SJ, Lennon VA (2008) Aquaporin-4 autoantibodies in a paraneoplastic context. Arch Neurol 65(5):629–632
Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, Fujihara K, Havrdova E, Hutchinson M, Kappos L, Lublin FD, Montalban X, O’Connor P, Sandberg-Wollheim M, Thompson AJ, Waubant E, Weinshenker B, Wolinsky JS (2011) Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol 69:292–302
Popovic N, Milosevic B, Urosevic A et al (2014) Clinical characteristics and functional outcome of patients with West Nile neuroinvasive disease in Serbia. J Neurol 261:1104–1111
Pradhan S, Gupta RK, Kapoor R, Shashank S, Kathuria MK (1998) Parainfectious conus myelitis. J Neurol Sci 161(2):156–162
Puccioni-Sohler M, Soares CN, Papaiz-Alvarenga A et al (2009) Neurological manifectations of Dengue associated with intrathecal specific immune-response. Neurology 73:1413–1417
Reach P, Paugam A, Kahan A, Allanore Y, Wipff J (2010) Coccidioidomycosis of the spine in an immunocompetent patient. Joint Bone Spine 77:611–613
Rodrigues CE, Carvalho JF, Shoenfeld Y (2010) Neurological manifestations of antiphospholipid syndrome. Eur J Clin Invest 40(4):350–359
Rodrigues CE, de Carvalho JF (2011) Clinical, radiologic, and therapeutic analysis of 14 patients with transverse myelitis associated with antiphospholipid syndrome: report of 4 cases and review of the literature. Semin Arthritis Rheum 40(4):349–357
Roman GC (2014) Tropical myelopathies. Handb Clin Neurol 121 (3rd series); Jose B, Ferro JM (eds) Neurologic aspects of systemic diseases part III. Elsevier, Amsterdam, Netherlands B.V, p 1525–1548
Roos KL, Miravalle A (2014) Postinfectious encephalomyelitis. In: Scheld WM, Whitley RJ, Marra CM (eds) Infections of the central nervous system. Wolters Kluwer Health, Philadelphia, pp 331–339
Ross AG et al (2012) Neuroschistosomiasis. J Neurol 259:22–32
Rupprecht TA, Lechner C, Tumani H, Fingerle V (2014) CXCL13: a biomarker for acute Lyme neuroborreliosis: investigation of the predictive value in the clinical routine. Nervenarzt 85(4):459–464
Russeggger L, Schmutzhard E (1989) Spinal toxocaral abscess. Lancet 2(8659):398
Saccente M (2008) Central nervous system histoplasmosis. Curr Treat Options Neurol 10:161–167
Saison J, Costedoat-Chalumeau N, Maucort-Boulch D, Iwaz J, Marignier R, Cacoub P et al (2015) Systemic lupus erythematosus-associated acute transverse myelitis: manifestations, treatments, outcomes, and prognostic factors in 20 patients. Lupus 24(1):74–81
Sato DK, Callegaro D, Lana-Peixoto MA, Waters PJ, de Haidar Jorge FM, Takahashi T et al (2014) Distinction between MOG antibody-positive and AQP4 antibody-positive NMO spectrum disorders. Neurology 82(6):474–481
Sato N, Watanabe K, Ohta K, Tanaka H (2011) Acute transverse myelitis and acute motor axonal neuropathy developed after vaccinations against seasonal and 2009 A/H1N1 influenza. Intern Med 50(5):503–507
Schellinger PD, Schmutzhard E, Fiebach JB, Pfausler B, Maier H, Schwab S (2000) Poliomyelitic-like illness in central European encephalitis. Neurology 55:299–302
Schmutzhard E, Boongird P, Vejjajiva A (1988) Eosinophilic meningitis and radiculomyelitis in Thailand, caused by CNS invasion of Gnathostoma spinigerum and Angiostrongylus cantonensis. J Neurol Neurosurg Psychiatry 51:80–87
Schmutzhard E, Helbok R (2014) Rickettsiae, protozoa, and opisthokonta/metazoa. Handb Clin Neurol 121:1403–1443
Schmutzhard E (2007) Eosinophilic myelitis, a souvenir from South East Asia. Pract Neurol 7:48–51
Schmutzhard E (2010) Parasitic diseases of the central nervous system. Nervenarzt 81:162–171
Scott TF, Frohman EM, De Seze J, Gronseth GS, Weinshenker BG (2011) Therapeutics and Technology Assessment Subcommittee of American Academy of Neurology. Evidence-based guideline: clinical evaluation and treatment of transverse myelitis: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 77(24):2128–2134
Scotti G, Gerevini S (2001) Diagnosis and differential diagnosis of acute transverse myelopathy. The role of neuroradiological investigations and review of the literature. Neurol Sci 22 Suppl 2:S69–S73
Sejvar JJ, Davis LE, Szabados E, Jackson AC (2010) Delayed-onset and recurrent limb weakness associated with West Nile virus infection. J Neurovirol 16:93–100
Sejvar JJ (2014) Clinical manifestations and outcomes of West Nile virus infection. Viruses 6:606–623
Sellner J, Luthi N, Buhler R, Gebhardt A, Findling O, Greeve I et al (2008) Acute partial transverse myelitis: risk factors for conversion to multiple sclerosis. Eur J Neurol 15(4):398–405
Sellner J, Hemmer B, Mühlau M (2010) The clinical spectrum and immunobiology of parainfectious neuromyelitis optica (Devic) syndromes. J Autoimmun 34:371–379
Senel M, Rupprecht TA, Tumani H, Pfister HW, Ludolph AC, Brettschneider J (2010) The chemokine CXCL13 in acute neuroborreliosis. J Neurol Neurosurg Psychiatry 81(8):929–933
Seror R, Richez C, Sordet C, Rist S, Gossec L, Direz G et al (2013) Pattern of demyelination occurring during anti-TNF-alpha therapy: a French national survey. Rheumatology 52(5):868–874
Stübgen JP (2011) Immune-mediated myelitis associated with hepatitis virus infections. J Neuroimmunol 239(1–2):21–27
Sonmez FM, Odemis E, Ahmetoglu A, Ayvaz A (2004) Brainstem encephalitis and acute disseminated encephalomyelitis following mumps. Pediatr Neurol 30:132–134
Sonneville R, Klein IF, Wolff M (2010) Update on investigation and management of postinfectious encephalitis. Curr Opin Neurol 23(3):300–304
Steiner I, Schmutzhard E, Sellner J, Chaudhuri A, Kennedy PG (2012) EFNS-ENS guidelines for the use of PCR technology for the diagnosis of infections of the nervous system. Eur J Neurol 19:1278–1291
Steiner I, Kennedy PG, Pachner AR (2007) The neurotropic herpes viruses. Herpes simplex and varicella zoster. Lancet Neurol 6:1015–1028
Stern BJ, Krumholz A, Johns C, Scott P, Nissim J (1985) Sarcoidosis and its neurological manifestations. Arch Neurol 42:909–917
Suzuki K, Takao M, Katayama Y, Mihara B (2013) Acute myelitis associated with HCV infection. BMJ Case Rep 2013. pii: bcr2013008934. doi: 10.1136/bcr-2013-008934
Taba P, Schmutzhard E, Forsberg P et al (2017) EFNS-ENS guidelines on diagnosis and management of tick borne encephalitis. Eur J Neurol (In press)
Tan BH, Chlebicka NL, Low JG, Chong TY, Chan KP, Goh YT (2008) Use of the cytomegalovirus pp 65 antigenemia assay for preemptive therapy in allogeneic hematopoietic stem cell transplantation: a real-world review. Transpl Infect Dis 10(5):325–332
Tan V, ThaiH Phu NH et al (2014) Viral aetiology of central nervous system infections in adults admitted to a tertiary referral hospital in southern Vietnam over 12 years. PLoS Negl Trop Dis 8(8):e312
Tenembaum S, Chitnis T, Ness J, Hahn JS (2007) Acute disseminated encephalomyelitis. Neurology 68(16 Suppl 2):S23–S36
Timmermans M, Carr J (2004) Neurosyphilis in the modern era. J Neurol Neurosurg Psychiatry 75:1727–1730
Torabi AM, Patel RK, Wolfe GI, Hughes CS, Mendelsohn DB, Trivedi JR (2004) Transverse myelitis in systemic sclerosis. Arch Neurol 61(1):126–128
Torabi AM, Quiceno M, Mendelsohn DEB et al (2004) Multilevel intramedullary spinal neurocysticercosis with eosinophilic meningitis. Arch Neurol 61:770–772
Transverse Myelitis Consortium Working Group (2002) Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurology 59(4):499–505
Trebst C, Raab P, Voss EV, Rommer P, Abu-Mugheisib M, Zettl UK, Stangel M (2011) Longitudinal extensive transverse myelitis-it’s not all neuromyelitis optica. Nat Rev Neurol 7(12):688–698
Trebst C, Raab, Stangel: Myelitis. Eine umfassende Differenzialdiagnose ist entscheidend. DNP 2013; 14:47–53
Trebst C, Jarius S, Berthele A, Paul F, Schippling S, Wildemann B, Borisow N, Kleiter I, Aktas O, Kümpfel T, Neuromyelitis Optica Study Group (NEMOS) (2014) Update on the diagnosis and treatment of neuromyelitis optica: recommendations of the Neuromyelitis Optica Study Group (NEMOS). J Neurol 261:1–16
Tsiodras S, Kelesidis T, Kelesidis I, Voumbourakis K, Giamarellou H (2006) Mycoplasma pneumoniae-associated myelitis: a comprehensive review. Eur J Neurol 13:112–124
Umehara F, Ookatsu H, Hayashi D (2006) MRI studies of spinal visceral larva migrans syndrome. J Neurol Sci 249:7–12
Uygunoğlu U, Pasha M, Saip S, Siva A (2015) Recurrent longitudinal extensive transverse myelitis in a neuro-Behçet syndrome treated with infliximab. J Spinal Cord Med 38(1):111–114
Vaish AK, Jain N, Gupta LK, Verma SK (2011) Atypical rabies with MRI findings: clue to the diagnosis. BMJ Case Rep 2011. pii: bcr0520114234
Vargas DL, Stern BJ (2010) Neurosarcoidosis: diagnosis and management. Semin Respir Crit Care Med 31:419–427
Verma R, Sahu R, Holla V (2014) Neurological manifestations of dengue infection: a review. J Neurol Sci 346:26–34
Vitali C et al (2002) Classification criteria for Sjogren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis 61:554–558
Ward KN, White RP, Mackinnon S, Hanna M (2002) Human herpesvirus-7 infection of the CNS with acute myelitis in an adult bone marrow recipient. Bone Marrow Transplant 30:983–985
Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG (2006) Revised diagnostic criteria for neuromyelitis optica. Neurology 66:1485–1489
Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG (2007) The spectrum of neuromyelitis optica. Lancet Neurol 6(9):805–815
Wingerchuk DM, Banwell B, Bennett JL, Cabre P, Carroll W, Chitnis T et al (2015) International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 85:177–189
Xia JB, Zhu J, Hu J, Wang LM, Zhang H (2014) H7N9 influenza A-induced pneumonia associated with acute myelitis in an adult. Intern Med 53:1093–1095
Yagi K, Kano G, Shibata M, Sakamoto I, Matsui H, Imashuku S (2011) Chlamydia pneumoniae infection-related hemophagocytic lymphohistiocytosis and acute encephalitis and poliomyelitis-like flaccid paralysis. Pediatr Blood Cancer 56:853–855
Yesilot N et al (2007) Clinical characteristics and course of spinal cord involvement in Behcet’s disease. Eur J Neurol 14:729–737
Yokoyama W, Takada K, Miyasaka N, Kohsaka H (2014) Myelitis and optic neuritis induced by a long course of etanercept in a patient with rheumatoid arthritis. BMJ Case Rep 1:2014
Young NP, Weinshenker BG, Lucchinetti CF (2008) Acute disseminated encephalomyelitis: current understanding and controversies. Semin Neurol 28:84–94
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Kleiter, I., Schmutzhard, E., Trebst, C. (2017). Infectious, Autoimmune and Other Immune-Mediated Causes of Myelitis. In: Weidner, N., Rupp, R., Tansey, K. (eds) Neurological Aspects of Spinal Cord Injury. Springer, Cham. https://doi.org/10.1007/978-3-319-46293-6_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-46293-6_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-46291-2
Online ISBN: 978-3-319-46293-6
eBook Packages: MedicineMedicine (R0)