
Abstract
Although there is no single standard protocol for breast MRI acquisition, high quality breast MRI generally requires use of a dedicated breast MRI coil and adequate (≥ 1.5 T) magnetic field strength. Currently, breast MRI requires gadolinium contrast agent administration for cancer detection and a dynamic acquisition (dynamic contrast enhanced, or DCE, MRI) using a method that allows for homogenous fat suppression. In order to maximize sensitivity and sensitivity, MRI protocols must balance spatial and temporal resolution so that important morphologic and kinetic enhancement features can be readily identified. In addition, it is important to develop an approach that attains consistency, addresses technical challenges, and minimizes artifacts. Finally, advanced approaches, such as use of higher magnetic field strength (e.g. 3 T) scanners, diffusion weighted imaging, and MR spectroscopy present unique opportunities and challenges that must be considered and addressed prior to adoption in routine clinical practice.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Breast MRI
- Technique
- Acquisition
- Protocol
- Spatial resolution
- Temporal resolution
- Artifacts
- 3 T
- Dynamic contrast enhanced
- Fat suppression
1 Introduction
Breast MRI was initially proposed for breast cancer detection in the 1970s [1] using pre-contrast intrinsic signal properties related to differences in longitudinal (T1) and transverse (T2) relaxation times exhibited by abnormal breast tissue when compared to normal tissue in vitro [2]. However, MRI use did not gain wide clinical acceptance until it was demonstrated that breast cancers exhibit higher signal on T1-weighted images after the administration of intravenous gadolinium-based contrast [3]. Breast MRI is now commonly used for a variety of clinical indications, which are covered in greater detail in Section II of clinical indications for breast MRI. In order to maximize the clinical utility of breast MRI, one must carefully balance patient and equipment factors in order to develop a breast MRI program that provides consistent, high quality images with superior sensitivity for breast cancer detection. This chapter discusses the technical considerations that are central to the performance of quality breast MRI for a variety of clinical indications.
2 General Breast MRI Technique Considerations
Despite the increasing utilization of breast MRI for a variety of clinical indications, there is currently no single standard protocol for image acquisition. Both the American College of Radiology (ACR) and the European Society of Breast Imaging (EUSOBI) have set minimum standards for acquisition of breast MRI. However, each of these guidelines allow for much flexibility in how images are acquired and what equipment is used. As reflected in these guidelines, there is consensus that high quality breast MRI acquisition should employ a high spatial resolution dynamic contrast-enhanced (DCE) protocol with bilateral acquisition that provides complete coverage of the breasts and axillae using a dedicated breast MRI coil. The clinical images should include key pulse sequences with appropriate spatial and temporal resolution for assessment of lesion morphologic and kinetic information and be free of significant artifacts. Such an approach allows for effective morphologic and semi-quantitative enhancement kinetic feature assessment of breast lesions, as described in the standardized American College of Radiology (ACR) Breast Imaging-Reporting and Data System (BI-RADS) MRI lexicon [4].
2.1 Patient Positioning and Comfort
Breast MRI should be performed with the patient positioned prone in the MRI scanner with the breasts pendant in the dedicated breast coils. This allows the breast tissue to be optimally imaged and findings to be accurately localized by stretching out the normal fibroglandular tissue elements away from the chest wall. This approach also has the advantage of increasing the distance of breast tissue from the heart and lungs, which helps to minimize cardiac and respiratory motion artifacts. Most commonly, the patient’s arms are raised above her head in order to avoid wrap artifact; however, some coil designs allow the arms to remain at the patient’s side yet posterior to the breasts.
Proper positioning with attention to patient comfort and clear communication allows breast MRI to be performed efficiently and without the aid of cardiac or respiratory gating. Maximizing patient comfort can decrease the likelihood of significant intra- and inter-scan motion. Common points of discomfort are the face, ribs, elbows, and sternum, which can be relieved with appropriate placement of vendor-supplied pads to support the sternum, head, and outer edge of the chest and cushions and/or pillows to support the hips, and elbows. It may be preferable to image patients feet first (in the bore of the magnet) rather than head first to decrease claustrophobia. Patients who have limited range of motion at the shoulder joint may require imaging with their arms at their sides (along the torso). In such cases, it may be useful to wrap the arms so that they are fixed in position and increase the field of view to include the arms to minimize the potential for wrap-around artifacts. Finally, specific yet concise instructions and communication allows patients to anticipate what they will experience while in the scanner, which improves compliance.
2.2 Magnetic Field Strength
Breast MRI should not be performed at low magnetic field (B0) strength and ideally should be performed with a 1.5 tesla (T) or greater magnet. Higher field strength allows for increased signal to noise ratio (SNR), which can facilitate acquisition of MR images that meet general spatial and temporal resolution standards. Over the past decade, breast MRI is increasingly being acquired clinically at higher field strength (e.g. 3 and 7 T), which can allow acquisition of high spatiotemporal resolution images with improved contrast resolution that simply cannot be achieved at 1.5 T. Higher field strength imaging also can decrease scan times; however, there are technical, physical, and safety challenges posed by 3 T and higher field strength imaging that need to be addressed. These challenges are discussed further at the end of the chapter (Imaging at Higher Field Strengths).
2.3 Coils
In order to maximize signal, breast MRI should be performed using only dedicated breast surface coils, and preferably using coils with a high number of coil elements. Having a high number of coil elements allows for parallel imaging, which is particularly efficient for breast imaging because it can facilitate high spatial resolution acquisitions in less scan time [5]. Newer MRI systems typically support 32 or more simultaneous radiofrequency (RF) channels, with 16-channel phased-array breast coils commercially available [6]. The breasts should be stabilized within the coil in the lateral-to-medial direction (for axial acquisitions) to minimize the effects of motion, such as ghosting artifacts, and degradation of the subtraction images [7].
2.4 Contrast Agent
Although non-contrast MRI techniques, such as diffusion weighted imaging and MR spectroscopy, have shown early promise for breast cancer detection and characterization, all clinical breast MRIs performed for cancer detection or characterization currently require the administration of a gadolinium contrast agent. Chelated gadolinium has paramagnetic properties that result in decreased T1, T2, and T2* relaxation times [8]. Thus, fluid-sensitive imaging, such as T2-weighted series, should be acquired prior to the administration of contrast. Since the decrease in relaxation from injection of the gadolinium chelate is greatest for T1-weighted sequences, DCE MRI is performed with T1-weighting. For breast imaging, the gadolinium chelate should be injected intravenously at a dose of 0.1 mmol/kg body weight followed by a 20 mL saline flush at a rate of approximately 2 mL/s using a power injector. This method both ensures contrast quickly reaches the intravascular space and allows for consistency in contrast enhancement timing across examinations.
2.5 Primary Imaging Acquisition Plane and Bilateral Imaging
One of the first decisions when building a breast MRI protocol is to decide on the primary acquisition plane, which may be the only image orientation acquired during the exam. Coronal, sagittal, and axial acquisition planes are all acceptable, particularly because high-quality multi-planar reformats can be reconstructed from imaging at or near isotropic resolution. Primary sagittal and axial acquisitions offer more intuitive orientations of the breast when compared to primary coronal acquisitions. Because the breast is organized anatomically into segments that extend anteroposteriorly from the nipple, both sagittal and axial acquisitions allow optimal visualization of these segments since the full anteroposterior span of the breast is presented on each image. Furthermore, the full plane of the sagittal images closely correlates with standard mediolateral oblique (MLO) and medial-lateral (ML) views obtained on x-ray mammography, whereas the full plane of axial images closely correlates with standard craniocaudal (CC) views. An additional benefit of a primary axial acquisition plane when compared to sagittal is that it allows for more natural side-by-side comparison of the breasts on each image. The authors’ practices perform a primary axial acquisition plane for this reason, with multi-planar reformats generated in coronal and sagittal planes. Primary coronal acquisition is rarely performed because it provides the least intuitive orientation and thus is not considered further in this chapter.
Regardless of plane of acquisition, bilateral imaging is favored over unilateral imaging for several reasons. First, bilateral imaging is clinically desirable because it allows for evaluation of both breasts at an identical post-contrast injection time point. Bilateral scanning also allows for assessment of symmetry of enhancement, which is useful for discriminating unique foci and non-mass enhancement lesions from normal background parenchymal enhancement (BPE). There are also technical reasons to perform bilateral imaging rather than unilateral imaging for breast MRI. Because the phase-encoding gradient is typically applied in the left—right direction to minimize the effects of cardiac motion, images acquired in the axial plane with unilateral acquisition are more prone to wrap-around artifacts from the non-imaged contralateral breast [7].
2.6 Field-of-View
The appropriate field-of-view (FOV) used for breast MRI depends on the primary acquisition plane. In general, the smallest FOV necessary to include the entire breast and both axillae is recommended in order to maximize in-plane spatial resolution for the same matrix size. For a bilateral axial acquisition plane, the FOV must be large enough to cover both breasts and axilla in the right—left direction. The appropriate FOV for a sagittal primary acquisition plane must account for the entire breast and axilla in the superior—inferior direction.
3 Key Breast MRI Pulse Sequences
A standard breast MRI examination includes multiple acquired sequences, which typically comprise the following (Fig. 1.1):
-
(i)
Scout or localizer obtained in all three perpendicular planes.
-
(ii)
T2-weighted (bright fluid) sequence, most commonly with fat suppression.
-
(iii)
Non-fat suppressed T1-weighted sequence.
-
(iv)
Multi-phase T1-weighted sequences performed before and multiple times after contrast administration.
-
(v)
Silicone sensitive sequence (if silicone implants are present).

Key breast MRI pulse sequences. Thirty-nine year old woman presents for breast MRI to evaluate extent of disease for known invasive ductal carcinoma of the left breast (arrow). Basic sequences include three-plane localizer sequence (a), fluid-sensitive sequence (in this case, fast spin echo T2-weighted image with fat saturation) (b), non-fat suppressed T1- weighted sequence (c), multiphase dynamic contrast-enhanced T1-weighted series with representative pre-contrast (d) and first post-contrast (e) images presented. Note the enhancing mass (arrow), which represents the biopsy-proven invasive ductal carcinoma, with susceptibility artifact within, representing a biopsy marker clip. A silicone-weighted series (f) was also obtained in this woman with pre-pectoral silicone implants
Of the above sequences, the 3-plane localizer, T2-weighted sequence, and T1-weighted multi-phase (DCE) sequences (including a pre-contrast and an early and delayed post-contrast series) are required by the ACR Breast MRI Accreditation Program [9]. Although optional from an ACR accreditation standpoint, most complete breast MR examinations also include a non-fat suppressed T1-weighted sequence. Furthermore, a silicone sensitive sequence should also be obtained in women with silicone breast implants. The role and optimization of each individual sequence is discussed in detail below.
For all sequences except the three-plane localizer, the frequency encoding gradient is applied in the anterior-posterior (AP) direction to minimize artifacts due to cardiac motion that would project into the breasts and simulate or obscure suspicious enhancement if the phase encoding direction was AP [10]. Thus, for sagittal acquisition the preferred phase encoding direction is superior—inferior and for axial acquisition the preferred phase encoding direction is left–right.
3.1 Three-Plane Localizer
A scout or three-plane localizer is required on all systems to localize the breasts. This allows the technologist to select the appropriate FOV for the patient’s anatomy and scan acquisition plane (FOV considerations are discussed in more detail above).
3.2 T2-Weighted (Fluid-Sensitive) Sequence
A fluid-sensitive, typically T2-weighted, sequence is important for improved characterization of lesions and benign findings in the breast. For example, simple cysts, lymph nodes, and some fibroadenomas have high signal on the T2-weighted images. There are multiple acceptable sequence types for fluid-sensitive imaging. The most common are spin echo (SE), fast spin echo (FSE), and short tau inversion recovery (STIR) with an inversion time selected to null fat. These sequences are typically acquired as multi-slice 2D acquisitions because of the long repetition times required for T2-weighting and resulting longer acquisition times, which are more prohibitive for three dimensional (3D) imaging [10]. Thus, the T2-weighted images are typically unable to achieve spatial resolution equivalent to the T1-weighted sequences in a reasonable scan time with adequate SNR. Most protocols utilizing SE or FSE technique for T2-weighted imaging also perform fat suppression in order to readily differentiate bright fluid signal from fat. However, others choose to perform T2-weighted images without fat suppression because it can allow for acquisition of higher spatial resolution images and/or decreased scan times.
3.3 Non-fat Suppressed T1-Weighted Sequence
If active fat suppression is used for the DCE sequences (discussed below), it is recommended to perform an additional T1-weighted sequence without fat suppression prior to the multi-phase T1-weighted sequences. The sequence is fast, provides an overview of breast anatomy, can aid in assessing the amount of fibroglandular tissue in the breast, and is helpful in distinguishing fat from water-based tissues (such as fibroglandular tissue, breast lesions, etc.). Additionally, this sequence can aid in the identification of fat containing lesions, which is important because lesions containing fat (e.g. fat necrosis) are typically benign. This sequence should be performed with similar parameters and spatial resolution as the multi-phase T1-weighted sequences (as described below), but without active fat suppression, which allows for comparison of lesion characteristics across all the T1-weighted sequences.
3.4 Multi-phase T1-Weighted Sequences
The pre-and post-contrast multi-phase T1-weighted MRI images sequences are the most important images for identifying and characterizing lesions. It is imperative that identical scan parameters be used for the multi-phase T1-weighted images so that image registration can be performed, the pre-contrast images can be subtracted from the post-contrast images, and signal differences between sequences can be directly compared. Subtraction images are particularly useful for identifying signal from gadolinium contrast agents and are mandatory if active fat suppression is not utilized so that contrast-enhancement can be readily differentiated from the bright signal of fat (described further below).
The multi-phase T1-weighted images are used for lesion detection, assessment of lesion morphology, and evaluation of lesion contrast enhancement over time. Characterizing lesion morphology, such as shape, margin, and internal enhancement pattern, requires high spatial resolution images with in-plane resolution of ≤1 mm to depict fine features, such as lesion margins. Through-plane slice thickness should be ≤3 mm; however, thinner slices that approach in plane resolution size (i.e. closer to isotropic) decrease volume averaging in the through-plane direction, which can increase the contrast of small lesions compared with background tissue. Additionally, thin slices facilitate higher quality image reformats, eliminating the need to acquire additional images in different planes (discussed further below). Conversely, voxel size should not be so small that SNR suffers.
A 3D GRE pulse sequence is preferred for multi-phase T1-weighted imaging with a short TR. The GRE pulse sequence should be spoiled to avoid any confounding T2 contrast [11]. There are no consensus guidelines for the number of post-contrast acquisitions or total acquisition time for the multi-phase T1-weighted sequences, although at least two post-contrast sequences should be performed in order to allow for the most basic assessment of contrast enhancement kinetic features. Invasive cancers typically enhance early, peaking in enhancement approximately one to two minutes after contrast injection. Although breast cancers more frequently exhibit initial fast enhancement (increase in signal from pre-contrast to first post-contrast series of >100 %) and delayed washout (decrease in signal from first post-contrast to final post-contrast series of >10 %) than benign findings, there remains substantial overlap in the kinetics of malignant and non-malignant lesions of the breast [12]. The multi-phase T1-weighted MRI protocol should be constructed so that one of the early-phase post-contrast sequences will sample the high frequency data at the center of k-space (which defines image contrast) between one and two minutes. This is important to potentially capture the peak enhancement of invasive cancers, but also to differentiate lesions from benign BPE, which typically increases over time (Fig. 1.2). For the majority of Cartesian sequences with rectilinear k-space sampling, the center of the sequence captures the high frequency data. However, Cartesian sequences with elliptical centric k-space sampling and other k-space sampling trajectories, such as radial, may acquire the center of k-space near the beginning of the sequence. Knowledge of the sampling pattern is thus important to properly time the post-contrast sequences.

Lesion conspicuity based on dynamic contrast enhanced (DCE) imaging timing. Early-phase 3D subtraction MIP images obtained in the early-phase post-contrast between 60–120 s (s) (a) demonstrates the patient’s outer posterior right breast cancer (red arrow), easily differentiated from the moderate benign background breast parenchymal enhancement (BPE, blue arrow). Delayed-phase 3D subtraction MIP image obtained between 420–480 s demonstrates that the cancer (red arrow) is less conspicuous because it has begun to washout while BPE (blue arrows) has increased in both breasts (b). Since in general, cancers tend to washout over time while BPE tends to increase (c), it is recommended that early phase DCE images be utilized for breast cancer detection
3.5 Silicone Implants
Silicone, like water, has a longer T2 relaxation time than fat. Thus, on a standard T2-weighted sequence without fat suppression, water will be brighter than silicone, which is brighter than fat [13]. For evaluation of silicone implant rupture, it is often ideal to have a sequence that suppresses both the water and fat, leaving silicone as the only material remaining bright on imaging. This is possible using a T2-weighted FSE pulse sequence with water suppression and an inversion pulse with an inversion time to null fat [13].
4 Balancing Spatial and Temporal Resolution
High spatial resolution and high temporal resolution are typically competing demands of MR acquisition. High spatial resolution imaging results in longer scan times, decreasing the temporal resolution. High spatial resolution is critical for accurate assessment of lesion morphologic features, but high temporal resolution is necessary for accurate depiction of lesion enhancement curves over time. Studies have shown that when forced to compromise, spatial resolution and accurate depiction of lesion morphology is more important to diagnostic accuracy than characterization of the signal enhancement curve. Thus, when creating a breast MRI protocol, spatial resolution is often prioritized over temporal resolution [14].
In general, the compromises between spatial and temporal resolution have decreased with state-of-the art MR systems and breast coils. The ACR Breast MRI Accreditation Program [9] requires that the early-phase post-contrast sequence be completed by four minutes after contrast injection; however, three minutes or less is most desirable [14, 15] and should be achievable without difficulty on modern scanners. Parallel imaging is now standard on modern MRI systems and also helps to shorten scan times [16–19]. There has been much research in recent years to develop novel accelerated MRI acquisition techniques to provide simultaneously high spatial and high temporal resolution scans. These include techniques such as novel k-space sampling schemes and reconstruction using high spatial frequency k-space data from adjacent time frames (view-sharing) [20–23]. Some of these methods are being used to obtain hybrid high spatiotemporal resolution imaging protocols [24, 25], although their exact benefit in the routine clinical setting is not known.
5 Methods of Fat Suppression
Either passive (image subtraction) or active removal of fat from the DCE MR images is necessary to ensure detection of contrast-enhancement separate from the bright signal of fat. The benefit of utilizing subtraction for fat suppression is that it allows for higher temporal resolution as well as potentially more complete fat suppression since it does not rely on B0 homogeneity and shimming. Relying only on image subtraction for detection and characterization of enhancing lesions also has drawbacks—misregistration resulting from interscan motion can result in “pseudoenhancement” and lead to diagnostic errors. Furthermore, subtracted images are prone to degradation of image quality [26]. Thus, it is the authors’ preference to perform active fat suppression for the T1-weighted DCE MRI images and additionally perform image subtraction. Using this approach allows an examination to be interpreted solely from the acquired T1-weighted fat suppressed images if the subtraction images are degraded by motion artifact.
Multiple methods exist for active fat suppression, exploiting the small differences in resonant frequency between lipid and water protons and/or the difference in T1 relaxation times between adipose tissue and water to suppress the fat signal. Intermittent fat suppression with a frequency selective fat saturation pulse to eliminate fat signal is commonly employed for T2-weighted SE and FSE sequences and T1-weighted GRE sequences. Inversion pulses and water only excitation pulses are also possibilities. More recently, fat-water separation techniques such as two-point Dixon based methods [27], including Iterative Decomposition of water and fat with Echo Asymmetry and Least squares estimation (IDEAL) [28], have become more common. These methods acquire multiple echo times (two or more) allowing separation of water and fat and result in water-only and fat-only images. A longer minimum TR is required to acquire the multiple echo times, thus acquisition time is longer. However, uniform suppression of fat signal is challenging in breast MRI due to B0 inhomogeneity given the complex anatomy and variation in tissue types across the FOV. Dixon methods improve the robustness of fat removal in the presence of B0 inhomogeneity [29]. Additionally, Dixon methods also provide fat-only images, eliminating the separate non-fat suppressed T1-weighted MRI acquisition and saving overall scan time.
6 Image Reformats
Subtraction of post-contrast images from the pre-contrast T1-weighted images is required to remove bright signal from fat (if active fat suppression is not used) so that contrast-enhancing lesions can more easily be seen. However, regardless of the use of active fat suppression for the DCE MR images, the use of image subtraction can be helpful since it removes non-enhancing fibroglandular tissue and other non-enhancing anatomy (besides adipose tissue), enabling easier visualization of potential suspicious areas of contrast enhancement. Subtraction images are most valuable for accentuating enhancing lesions that are evident on the early-phase (for the same reasons described above) DCE images, but can be performed for any of the post-contrast sequences by simply subtracting the pre-contrast images’ signal from the desired post-contrast images. One of the most commonly used subtraction reformats is a 3D subtraction maximum intensity projection (MIP) that is created from an individual subtraction series (most frequently the first post-contrast DCE series). The MIP is valuable clinically as an “overview” image that allows for quick assessment of symmetry, BPE, and the presence of suspicious findings.
If the acquired images have sufficient spatial resolution and thin slices, multi-planar reformats (MPRs) can be performed (Fig. 1.3). MPRs allow suspicious findings to be evaluated in multiple planes, aiding detection and characterization, as some lesion types such as non-mass enhancement can be at times easier to detect in a second plane. Also, creation of MPRs eliminates the need to acquire additional sequences in perpendicular planes, saving overall scan time.

Subtracted maximum intensity projection (MIP) and multi-planar reformats (MPRs) in a 39 year old patient with biopsy proven left invasive ductal carcinoma (arrows, same patient as in Fig. 1.1). Patient with biopsy-proven invasive ductal carcinoma (arrow) with evidence of multifocal malignancy on MIP (a). Known malignancy is evident as a mass (arrow) on the source first post-contrast T1-weighted dynamic contrast enhanced (DCE), which was acquired in the axial plane (b). Multi-planar coronal (c) and sagittal (d) reformats from the source first post-contrast DCE image (a) provide improved characterization and localization of the known malignancy
7 Attaining Consistency and Addressing Challenges
There are inherent challenges to performing breast MRI that must be addressed to obtain consistent high quality breast MR examinations. First and foremost, a quality breast MRI program includes highly trained technologists who regularly perform breast MRI and are comfortable with appropriate patient positioning and communication. Protocol sequences and sequence timings should be as consistent as possible from patient to patient, regardless of breast size or body habitus. However, the FOV can be adjusted for body habitus for image optimization and reduction of artifact as needed. Finally, there are technical and physical challenges to obtaining high quality breast MRI, some of which are accentuated at higher magnetic field strength, which require attention and are discussed in greater detail below.
8 Artifacts
Imaging artifacts can occur in breast MRI scans from a variety of sources. Such artifacts are important to recognize as they can cause misinterpretation by obscuring and/or mimicking pathology. Several of the most common artifacts affecting clinical breast MRI are summarized here.
8.1 Motion Artifacts
Both physiologic and non-physiologic movement during image acquisition can cause artifacts. Sources of physiologic motion commonly impacting breast MRI are blood flow and vessel pulsation, respiration, and cardiac motion. Motion artifacts propagate in the phase-encoding direction; therefore, the direction of the phase-encoding gradient must be selected to minimize detrimental effects of such motion on the diagnostic quality of the images. In order to minimize physiologic motion artifacts across the breasts, the phase-encoding gradient should be left—right for axial imaging and superior—inferior for coronal or sagittal imaging (Fig. 1.4).

Cardiac motion artifact evident in the phase encoding direction on 1.5 T MR images in a 38 year old woman with a newly diagnosed invasive cancer in the left breast. Pre-contrast (a) and initial phase (b) post-contrast T1-weighted MR images (axial primary acquisition) demonstrate cardiac motion artifact in the phase encoding (right—left, vertical blue arrows) direction in a 44 year old patient with known invasive ductal carcinoma (angled white arrow) in the left breast. Note that due to gadolinium concentrating in the heart and great vessels, this effect is accentuated on the post-contrast images (b). Alternate selection of anterior-posterior as the phase encoding direction could cause the cardiac motion artifact to overlay and obscure much of the lesion and surrounding area. As a result, it is recommended that the phase encoding direction be left—right for primary axial acquisitions and superior—inferior for primary sagittal or coronal acquisitions
8.2 Misregistration Artifacts
Even slight patient motion during the multi-phase T1-weighted imaging sequences can significantly compromise image subtraction and associated MIP images, reformats, and temporal kinetic evaluation. Resulting image misregistration can create artifacts in subtraction images that simulate suspicious enhancement (i.e. “pseudoenhancement,” Fig. 1.5). This issue becomes even more pronounced in protocols with higher spatial resolution. In addition to proper patient positioning and communication, minimizing overall scan time (e.g. by performing multi-planar reformats instead of acquiring alternate scan planes) is important to minimize patient discomfort and motion. Motion correction software may also be helpful to reduce misregistration [26], but cannot be relied upon alone.

“Pseudoenhancement” on subtraction MR images resulting from interscan patient motion in a 49 year old woman presenting for high risk screening due to personal history of treated breast cancer and BRCA mutation. Subtraction image (a) created by subtracting the pre-contrast (b) from the initial post-contrast (c) 3D T1-weighted fast gradient echo 3 T images demonstrates an apparent rim-enhancing mass in the central right breast (arrow). Direct comparison of the anatomic landmarks at the same slice number on the source pre-contrast (b) and initial post-contrast (d) images demonstrates the apparent enhancement is artifactually created by misregistration of normal non-enhancing signal (arrows) on T1-weighted images due to mild inter-scan patient motion
8.3 Inhomogeneous Fat Suppression
Uniform fat suppression is important for the detection of breast cancer, as the high signal of fat can hinder detection of enhancing lesions. Inhomogeneous fat suppression is a common problem in breast MRI and can be due to a variety of factors, primarily related to inadequate shimming causing B0 inhomogeneity or to incorrectly selected water center frequency (Fig. 1.6). At higher magnetic field strength (e.g. 3 T), B1 inhomogeneity (discussed more below) can also lead to inhomogeneous fat suppression. Fat suppression also can be more challenging in women with fatty breasts (due to high fat signal relative to water) or pendulous breasts (due to shimming difficulties for bilateral imaging). Review by the MRI technologist of the location of water and fat peaks and adjustment, if necessary, of the water center frequency automatically selected by the system software may improve frequency-selective fat saturation. Alternate shimming approaches, through manual adjustment of the shim volume or use of advanced higher order shimming techniques, may improve magnetic field homogeneity and resulting uniformity of fat suppression.

Inhomogeneous fat suppression due to B0 inhomogeneity secondary to suboptimal shimming. Poor fat suppression (arrows) is evident in a 76 year old woman, presenting for breast MRI to evaluate extent of disease, in the cleavage on the T1-weighted first post contrast series obtained at 3 T (a). Incomplete fat suppression is noted in the mastectomy bed (arrow) in a 57-year-old woman presenting for high risk screening on the T1-weighted first post contrast series obtained at 1.5 T (b). In both cases, unique anatomic considerations (pendulous breasts in (a), asymmetry due to mastectomy in (b)) contributed to pronounced B0 inhomogeneity. Patient adaptive shimming techniques can help decrease these effects
8.4 Metallic/Susceptibility Artifacts
Metallic objects, including biopsy marker clips, chemotherapy ports, jewelry, etc. can cause disturbances in the main magnetic field, resulting in metallic/susceptibility artifacts in images (Fig. 1.7). Such artifacts can be helpful (e.g. for confirming biopsy clip placement) or a hindrance if they are large and may obscure cancer [30]. The degree of magnetic field distortion is determined by the size, shape, and composition of the metallic object [31]. Metallic artifacts typically appear as signal voids, sometimes also accompanied by signal flares in some types of sequences (e.g. spin echo). Metallic biopsy markers are available in non-ferromagnetic titanium, which cause less distortion than markers made of stainless steel. Use of titanium markers may be preferable for 3 T imaging, as magnet susceptibility is greater at higher field strengths. Susceptibility artifacts can be further reduced in size by using fast spin echo rather than gradient echo sequences, reducing TE, and increasing readout gradient strength (increasing bandwidth).

Magnetic susceptibility artifacts. Signal void and surrounding incomplete fat suppression (arrow) due to magnetic susceptibility related to the presence of a port catheter in the superior right breast on first post-contrast T1-weighted DCE image with fat suppression in a 64-year old woman during mid-therapy monitoring (a). Signal void in the subareolar right breast (arrow) due to magnetic susceptibility related to the presence of a titanium metallic biopsy marker clip from a prior needle biopsy on first post-contrast T1-weighted DCE image with fat suppression in a 43-year old woman presenting for breast MRI to evaluate extent of disease (b)
8.5 Aliasing/Phase Wrap Artifacts
Tissue outside of the prescribed field-of-view can alias and overlay on the opposite side of the image. This phenomenon is observed in the phase-encoding direction as MR manufacturers have implemented techniques to automatically suppress image wrap in the frequency-encoding directions. Because the phase-encoding gradient is typically applied in the left—right direction to minimize the effects of cardiac motion, axial images can suffer wrap artifacts of the patient’s arms (Fig. 1.8) if they are positioned at the patient’s sides, or wrap artifacts from the non-imaged contralateral breast in the case of unilateral acquisitions [7]. 3D acquisitions utilize two phase-encoding directions and therefore also exhibit phase wrap in the slice-select direction. Means to mitigate phase wrap include appropriate selection of phase-encoding direction, widening the imaging FOV to include all tissue in the phase-encoding direction, applying saturation bands to suppress the signal from outside the FOV, or phase oversampling (also known as ‘no phase wrap’) techniques.

Phase wrap artifact in a 57-year old woman presenting for high-risk screening MRI. Selected image from a T1-weighted fast gradient recalled echo sequence obtained at 1.5 T demonstrates phase wrap artifact of the left arm (which was positioned along the patient’s torso for comfort in this woman status post left mastectomy with lymphedema) in the region of the right axilla (arrow). Note also incomplete fat suppression in the left axilla due to B0 inhomogeneity
Other general MRI artifacts that may affect breast MR examinations include chemical shift artifacts resulting from differences in the resonant frequencies of hydrogen in fat and water, which causes spatial misregistration between the “fat image” and the “water image” in the frequency-encoding direction and manifests as bright or dark bands at fat-tissue interfaces. RF noise artifacts can also occur due to interference from external RF sources, potentially resulting from inadequate shielding of the scan room during image acquisition.
9 3 T Breast MR Considerations
Imaging at higher magnetic field strength holds potential advantages, primarily related to increased spatial and temporal resolution. As a result, clinical use of MRI scanners with field strength greater than 1.5 T has increased substantially in recent years. While clinical scanning has been reported in up to 7 T magnetic field strengths [32, 33], 3 T is much more readily available [34] and thus merits further discussion.
Scanning at 3 T provides a near doubling of the SNR when compared with 1.5 T, and this increased SNR can be used to obtain higher spatial resolution images at comparable imaging times or to shorten imaging times. Breast MR examinations can also benefit from improved fat suppression because of the greater spectral separation of fat and water at 3 T. Studies have reported significant improvement in accuracy at 3 T compared with 1.5 T in the same patients for differential diagnosis of enhancing breast lesions [35] and for assessing extent of disease in ductal carcinoma in situ [36]. However, specific refinement of breast imaging protocols is required to address the technical and safety challenges of imaging at higher field strength. Such challenges include increased RF energy deposition, increased spatial inhomogeneities of the main magnetic field (B0) and applied radiofrequency field (B1), and increased susceptibility effects [34].
9.1 Specific Absorption Rate (SAR)
SAR is a measure of radiofrequency (RF) energy deposition that causes tissue heating. When compared to 1.5 T, SAR for breast MRI increases approximately four fold at 3 T when imaging parameters are held constant. Parallel imaging is a primary means to reduce MR imaging times and resulting RF power deposition. Use of reduced flip angles also directly reduces SAR, but with resulting effects on contrast. Additional strategies to mitigate SAR effects require tradeoffs in image acquisition rates, resolution, and slice coverage. Multi-source parallel RF transmission techniques (e.g. dual-source [37, 38]) may also help to reduce SAR by enabling greater control of the distribution of magnetic and electric fields produced in tissue, as well as shortening RF pulse durations.
9.2 B0 Inhomogeneity
Variations of the main magnetic field can cause magnetic susceptibility effects and incomplete fat suppression (Fig. 1.6), particularly at the interfaces between soft tissue (breast) and air. Uniform B0 throughout the entire field of view is especially important for T1-weighted gradient echo imaging with fat saturation. B0 inhomogeneities are more problematic at 3 T than 1.5 T due to increased magnetic susceptibility at higher magnetic field strengths [39]. Higher order image-based shimming methods can substantially improve B0 uniformity for breast imaging.
9.3 B1 Inhomogeneity
Variations in the applied magnetic field are also more pronounced at 3 T vs. 1.5 T due to the higher RF transmit frequency causing standing wave and/or dielectric effects. B1 inhomogeneities cause the applied flip angle and signal measured to be nonuniform across the field of view, resulting in shading and variations in tissue contrast depending on location [40]. B1 inhomogeneities can be particularly problematic in breast imaging due to the large field of view required for bilateral imaging and the off-center positioning of the breasts within the transmitting whole-body RF birdcage coil [41]. Use of 3D imaging and increased flip angles can minimize such effects and newer dual source parallel RF excitation techniques substantially improve B1 homogeneity for breast imaging [42].
10 Advanced MRI Techniques
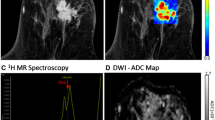
Emerging advanced functional MRI sequences such as diffusion-weighted imaging (DWI) and MR spectroscopy (MRS) can provide potentially useful in vivo measurements of tissue microstructure and metabolism to complement the anatomic and vascular information provided by conventional breast MRI examinations [43]. These techniques are under investigation to improve disease detection and characterization, but have not yet been widely incorporated into clinical breast MRI protocols and interpretations. There are specific challenges and considerations to successfully implementing such advanced sequences. Generally, higher field strength and high performance gradients are advantageous to maximize signal strength and data quality for advanced MRI techniques. In particular, excellent shimming and fat suppression are essential to reduce artifacts in both DWI and MRS. These advanced approaches are described in more detail in a later chapter on multiparametric imaging.
11 Summary
Breast MRI is a widely utilized imaging tool for a variety of clinical indications. There are multiple ways to achieve high quality breast MR images, and each approach must be tailored to the specific equipment available. When performed consistently using a DCE technique that balances spatial and temporal resolution, achieves homogeneous fat suppression, and minimizes artifacts, breast MRI offers unparalleled anatomic detail combined with useful physiologic information. The resulting high quality MR images, paired with interpretations by experienced radiologists, provide the most sensitive imaging test for detection and characterization of breast cancer.
References
Damadian R. Tumor detection by nuclear magnetic resonance. Science (New York, NY). 1971;171(3976):1151–3. PubMed PMID: 5544870. Epub 1971/03/19. eng
Bovee WM, Getreuer KW, Smidt J, Lindeman J. Nuclear magnetic resonance and detection of human breast tumor. J Natl Cancer Inst. 1978;61(1):53–5. PubMed PMID: 276638. Epub 1978/07/01. eng
Kaiser WA, Zeitler E. MR imaging of the breast: fast imaging sequences with and without Gd-DTPA. Preliminary observations. Radiology. 1989;170(3 Pt 1):681–6. PubMed PMID: 2916021. Epub 1989/03/01. eng
D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA, et al. ACR BI-RADS® Atlas, breast imaging reporting and data system. Reston, VA, American College of Radiology; 2013.
Nnewihe AN, Grafendorfer T, Daniel BL, Calderon P, Alley MT, Robb F, et al. Custom-fitted 16-channel bilateral breast coil for bidirectional parallel imaging. Magn Reson Med. 2011;66(1):281–9. PubMed PMID: 21287593. Pubmed Central PMCID: 3128917. Epub 2011/02/03. eng
Ladd ME. High-field-strength magnetic resonance: potential and limits. Top Magn Reson Imaging. 2007;18(2):139–52. PubMed PMID: 17621228
Rausch DR, Hendrick RE. How to optimize clinical breast MR imaging practices and techniques on Your 1.5-T system. Radiographics. 2006;26(5):1469–84. PubMed PMID: 16973776. Epub 2006/09/16. eng
Hendrick RE, Haacke EM. Basic physics of MR contrast agents and maximization of image contrast. J Magn Reson Imaging. 1993;3(1):137–48. PubMed PMID: 8428081. Epub 1993/01/01. eng
The American College of Radiology Breast Magnetic Resonance Imaging (MRI) Accreditation Program Requirements [updated 07/31/2015; cited 2015 12/14/2015] Available from: http://www.acr.org/~/media/ACR/Documents/Accreditation/BreastMRI/Requirements.pdf.
Hendrick RE. Breast MRI: fundamentals and technical aspects. Springer Science + Business Media, New York, LLC.; 2008.
Kuhl CK. Current status of breast MR imaging. Part 2. Clinical applications. Radiology. 2007;244(3):672–91. PubMed PMID: 17709824
Wang LC, DeMartini WB, Partridge SC, Peacock S, Lehman CD. MRI-detected suspicious breast lesions: predictive values of kinetic features measured by computer-aided evaluation. AJR Am J Roentgenol. 2009;193(3):826–31. PubMed PMID: 19696298. Epub 2009/08/22. eng
Middleton MS. MR evaluation of breast implants. Radiol Clin North Am. 2014;52(3):591–608. PubMed PMID: 24792659
Kuhl CK, Schild HH, Morakkabati N. Dynamic bilateral contrast-enhanced MR imaging of the breast: trade-off between spatial and temporal resolution. Radiology. 2005;236(3):789–800. PubMed PMID: 16118161
Gutierrez RL, Strigel RM, Partridge SC, DeMartini WB, Eby PR, Stone KM, et al. Dynamic breast MRI: does lower temporal resolution negatively affect clinical kinetic analysis? AJR Am J Roentgenol. 2012;199(3):703–8. PubMed PMID: 22915415
Friedman PD, Swaminathan SV, Smith R. SENSE imaging of the breast. AJR Am J Roentgenol. 2005;184(2):448–51. PubMed PMID: 15671362
Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med. 2002;47(6):1202–10. PubMed PMID: 12111967
Griswold MA, Jakob PM, Nittka M, Goldfarb JW, Haase A. Partially parallel imaging with localized sensitivities (PILS). Magn Reson Med. 2000;44(4):602–9. PubMed PMID: 11025516
Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952–62. PubMed PMID: 10542355
Herrmann KH, Baltzer PA, Dietzel M, Krumbein I, Geppert C, Kaiser WA, et al. Resolving arterial phase and temporal enhancement characteristics in DCE MRM at high spatial resolution with TWIST acquisition. J Magn Reson Imaging. 2011;34(4):973–82. PubMed PMID: 21769981
Le Y, Kipfer H, Majidi S, Holz S, Dale B, Geppert C, et al. Application of time-resolved angiography with stochastic trajectories (TWIST)-Dixon in dynamic contrast-enhanced (DCE) breast MRI. J Magn Reson Imaging. 2013;38(5):1033–42. PubMed PMID: 24038452
Saranathan M, Rettmann DW, Hargreaves BA, Clarke SE, Vasanawala SS. DIfferential Subsampling with Cartesian Ordering (DISCO): a high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging. 2012;35(6):1484–92. PubMed PMID: 22334505. Pubmed Central PMCID: 3354015
Saranathan M, Rettmann DW, BA H, JA L, BL D. Variable spatiotemporal resolution three-dimensional dixon sequence for rapid dynamic contrast-enhanced breast MRI. J Magn Reson Imaging. 2013;40(6):1392–9. PubMed PMID: 24227703
Tudorica LA, Oh KY, Roy N, Kettler MD, Chen Y, Hemmingson SL, et al. A feasible high spatiotemporal resolution breast DCE-MRI protocol for clinical settings. Magn Reson Imaging. 2012;30(9):1257–67. PubMed PMID: 22770687. Pubmed Central PMCID: 3466402
Pinker K, Grabner G, Bogner W, Gruber S, Szomolanyi P, Trattnig S, et al. A combined high temporal and high spatial resolution 3 Tesla MR imaging protocol for the assessment of breast lesions: initial results. Invest Radiol. 2009;44(9):553–8. PubMed PMID: 19652611
American College of Radiology Practice Parameter for the Performance of Contrast-Enhanced MRI of the Breast [updated 10/01/2014, cited 12/14/2015]. Available from: http://www.acr.org/~/media/2a0eb28eb59041e2825179afb72ef624.pdf.
Dixon WT. Simple proton spectroscopic imaging. Radiology 1984;153(1):189–194. PubMed PMID: 6089263.
Reeder SB, Pineda AR, Wen Z, Shimakawa A, Yu H, Brittain JH, et al. Iterative decomposition of water and fat with echo asymmetry and least-squares estimation (IDEAL): application with fast spin-echo imaging. Magn Reson Med. 2005;54(3):636–44. PubMed PMID: 16092103
Glover GH, Schneider E. Three-point Dixon technique for true water/fat decomposition with B0 inhomogeneity correction. Magn Reson Med. 1991;18(2):371–83. PubMed PMID: 2046518
Yitta S, Joe BN, Wisner DJ, Price ER, Hylton NM. Recognizing artifacts and optimizing breast MRI at 1.5 and 3 T. AJR Am J Roentgenol. 2013;200(6):W673–82. PubMed PMID: 23701101
Harvey JA, Hendrick RE, Coll JM, Nicholson BT, Burkholder BT, Cohen MA. Breast MR imaging artifacts: how to recognize and fix them. Radiographics. 2007;27(Suppl 1):S131–45. PubMed PMID: 18180223
van der Velden TA, Schmitz AM, Gilhuijs KG, Veldhuis WB, Luijten PR, Boer VO, et al. Fat suppression techniques for obtaining high resolution dynamic contrast enhanced bilateral breast MR images at 7 tesla. Magn Reson Imaging. 2016;34(4):462–8. doi:10.1016/j.mri.2015.12.012. Epub 2015/12/ 17.
Schmitz AM, Veldhuis WB, Menke-Pluijmers MB, van der Kemp WJ, van der Velden TA, Kock MC, et al. Multiparametric MRI with dynamic contrast enhancement, diffusion-weighted imaging, and 31-phosphorus spectroscopy at 7 T for characterization of breast cancer. Invest Radiol. 2015;50(11):766–71. PubMed PMID: 26135017
Rahbar H, Partridge SC, DeMartini WB, Thursten B, Lehman CD. Clinical and technical considerations for high quality breast MRI at 3 Tesla. J Magn Reson Imaging. 2013;37(4):778–90. PubMed PMID: 23526757
Kuhl CK, Jost P, Morakkabati N, Zivanovic O, Schild HH, Gieseke J. Contrast-enhanced MR imaging of the breast at 3.0 and 1.5 T in the same patients: initial experience. Radiology. 2006;239(3):666–76. PubMed PMID: 16549623
Rahbar H, DeMartini WB, Lee AY, Partridge SC, Peacock S, Lehman CD. Accuracy of 3 T versus 1.5 T breast MRI for pre-operative assessment of extent of disease in newly diagnosed DCIS. Eur J Radiol. 2015;84(4):611–6. PubMed PMID: 25604909. Pubmed Central PMCID: 4348176
Nelles M, Konig RS, Gieseke J, Guerand-van Battum MM, Kukuk GM, Schild HH, et al. Dual-source parallel RF transmission for clinical MR imaging of the spine at 3.0 T: intraindividual comparison with conventional single-source transmission. Radiology. 2010;257(3):743–53. PubMed PMID: 20858848. Epub 2010/09/23. eng
Willinek WA, Gieseke J, Kukuk GM, Nelles M, Konig R, Morakkabati-Spitz N, et al. Dual-source parallel radiofrequency excitation body MR imaging compared with standard MR imaging at 3.0 T: initial clinical experience. Radiology. 2010;256(3):966–75. PubMed PMID: 20720078. Epub 2010/08/20. eng
Rakow-Penner R, Hargreaves B, Glover GH, Daniel B. Breast MRI at 3 T. Appl Radiol. 2009;March:6–13.
Kuhl CK, Kooijman H, Gieseke J, Schild HH. Effect of B1 inhomogeneity on breast MR imaging at 3.0 T. Radiology. 2007;244(3):929–30. PubMed PMID: 17709843
Azlan CA, Di Giovanni P, Ahearn TS, Semple SI, Gilbert FJ, Redpath TW. B1 transmission-field inhomogeneity and enhancement ratio errors in dynamic contrast-enhanced MRI (DCE-MRI) of the breast at 3 T. J Magn Reson Imaging. 2010;31(1):234–9. PubMed PMID: 20027594. Epub 2009/12/23. eng
Rahbar H, Partridge SC, Demartini WB, Gutierrez RL, Parsian S, Lehman CD. Improved B(1) homogeneity of 3 tesla breast MRI using dual-source parallel radiofrequency excitation. J Magn Reson Imaging. 2012;35(5):1222–6. PubMed PMID: 22282269. Epub 2012/01/28. Eng
Rahbar H, Partridge SC. Multiparametric MR imaging of breast cancer. Magn Reson Imaging Clin N Am. 2016;24(1):223–38. PubMed PMID: 26613883. Pubmed Central PMCID: 4672390
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Rahbar, H., Strigel, R.M., Partridge, S.C. (2017). Breast MRI Technique. In: Heller, S., Moy, L. (eds) Breast Oncology: Techniques, Indications, and Interpretation. Springer, Cham. https://doi.org/10.1007/978-3-319-42563-4_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-42563-4_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-42561-0
Online ISBN: 978-3-319-42563-4
eBook Packages: MedicineMedicine (R0)