
Abstract
There are many different types of spinal schwannomas including single and multiple (associated or not to neurofibromatosis), cystic, hemorrhagic, melanotic, and malignant. Their location is usually intradural and extramedullary, but some can be found intramedullary, extradural, intra-/extradural, and even intraosseous.
Considering cervical schwannomas, they are most often strictly intradural, but may also be totally or partially extradural (dumbbell tumors) either intraspinal or foraminal or extraspinal. These dumbbell forms are as frequent as 18 % when considering the whole spine, but at the cervical level, they account for 50 % of all schwannomas.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
There are many different types of spinal schwannomas including single and multiple (associated or not to neurofibromatosis), cystic, hemorrhagic, melanotic, and malignant [1–3]. Their location is usually intradural and extramedullary, but some can be found intramedullary, extradural, intra-/extradural, and even intraosseous [1, 4, 5].
Considering cervical schwannomas, they are most often strictly intradural, but may also be totally or partially extradural (dumbbell tumors) either intraspinal or foraminal or extraspinal [6, 7] (Fig. 42.1). These dumbbell forms are as frequent as 18 % when considering the whole spine, but at the cervical level, they account for 50 % of all schwannomas [8, 9].

Classification and appropriate surgical approach to cervical schwannomas. Best treated by a posterior approach: (a) intradural. (b) intra-/extradural. (c) intradural intramedullary. Best treated by a lateral approach: (d) extraspinal. (e) extraspinal-foraminal. (f) extra-/intraspinal extradural. (g) extra-/intraspinal intradural (Modified from Bruneau and George [31])
Schwannomas are the second most frequent extramedullary tumors after meningiomas, but the most common type of nerve sheath tumor before neurofibromas (66 % vs. 11 % for Seppala et al. [10]). The cervical level accounts for 15–30 % of all spinal schwannomas [4, 11, 12]. Strictly intradural schwannomas increase from 8 % at the upper cervical level to 80 % at the thoracolumbar level [13].
At the cervical level, schwannomas predominate on the two first cervical nerve roots, which account for 18–36 % [10, 11, 14]. Worthy of mention, the C1 and C2 schwannomas very often have an extradural component (85 %), while intradural forms are observed in only 15 % [15].
2 Diagnosis
Pain is the most common presenting symptom being either local (50 %) or radicular (30 %). Very rarely patients present with symptoms due to raised intracranial pressure associated with papilledema [16] or hydrocephalus [17, 18].
At the time of diagnosis, motor deficit is rare and usually moderate including 30 % and 15 % of radicular and medullary deficits, respectively [10, 11]. Sphincter disturbances are exceptionally observed.
MRI is the best imaging tool as it offers all the relevant information for diagnosis, localization, and surgical strategy. Schwannomas are generally hypointense in T1 sequences and hyperintense in T2. They can be differentiated from meningiomas, which are isointense or less hypointense in T1. Moreover schwannomas are markedly and heterogeneously enhanced after contrast injection, sometimes in a ring-like manner, while meningiomas show moderate and homogeneous enhancement. Then the oval shape of schwannomas extending obliquely along the axis of the nerve root is very suggestive. The shape is still more suggestive in case of dumbbell forms [19, 20].
MRI permits to define any type of extension (intradural, extradural, foraminal, and extraspinal). It shows very well the cystic and hemorrhagic forms [21]. Conversely it is generally difficult to differentiate schwannomas from solitary neurofibromas. MRI is also quite sufficient to demonstrate the relationship between the schwannoma and the vertebral artery (VA). In case of foraminal extension, the VA is most of the time displaced anteriorly and medially. It is also important to evaluate the size of both VAs.
A computerized tomography (CT) scan may still be useful to appreciate the bony erosion in foraminal and extraspinal types. It varies from a limited widening of the intervertebral foramen to a large defect in one or several vertebral bodies and/or facet joints.
3 Surgical Treatment
Any intraspinal schwannoma has to be resected surgically since it will lead more or less rapidly to a spinal cord or cauda equina compression. Only a limited life expectancy of the patient or a very bad general condition may suggest the option of radiosurgery [5, 22].
In case of foraminal and/or extraspinal location, observation may be chosen, but often pain and/or neurological deficit (motor weakness) makes the patient ask for its relief.
3.1 Surgical Technique
The surgical technique differs according to the tumor location and its level.
-
1.
Pure intradural schwannomas
-
In the vast majority of cases with an intradural location, there is a common agreement to use the midline posterior approach through a laminectomy, hemilaminectomy, or laminoplasty [23] (Figs. 42.1a–c and 42.2).
Fig. 42.2 
Large intradural schwannoma resected through a posterior approach. (a–e) Preoperative MRI (a, sagittal T2, b sagittal T1, c sagittal T1 with gadolinium, d axial T1 with gadolinium, and e axial T2 images showing a left-sided C2–C4 intradural tumor (T) (d) severely compressing the spinal cord (SC). (f–h) Intraoperative images. (f) View of the tumor after opening of the dura mater. (g) After partial debulking, the inferior tumoral pole and the spinal cord are visible. (h) The pathological nerve root bearing the tumor is identified and sacrificed. (i) Postoperative image confirming complete resection and spinal cord decompression (Courtesy of M. Bruneau, Erasme hospital)
-
In the usual cases, the opening on two vertebral levels is sufficient for an adequate exposure and resection.
-
A vertical paramedian incision of the dura, curved laterally at both extremities, is realized. Then in schwannomas posterior to the spinal cord (origin from the posterior rootlets), an en bloc excision can be achieved; in anterolateral and large tumors, debulking of the tumoral mass is first realized. It permits to mobilize the tumor and to look for the proximal and distal rootlets.
-
Generally a limited number of rootlets (one or two) gives origin to the schwannoma. They are identified and separated from the others; they are coagulated and cut before taking out the remaining part of the tumor. In contrast to some meningiomas, there is usually no difficulty to separate the tumor from the spinal cord except in case of intramedullary extension, which is rare.
-
-
2.
Intra-/extradural components
In case of extradural and intradural components (dumbbell form), some modifications must be added (Figs. 42.1b and 42.3).
Fig. 42.3 
Intra-/extradural C2–C3 schwannoma resected through a posterior approach. (a–d) Preoperative workup. The tumor (T) severely compresses the spinal cord. (e) Postoperative control after complete resection. (f–i) Intraoperative images. (f) The tumor is visible immediately following opening of the dura mater. The spinal cord (white arrows) is significantly shifted. (g) The nerve root bearing the tumor is identified (black arrow). (h) The tumor extends extradurally through the dural sheath of the nerve root. (i) Normal anterior rootlets (black arrow) have been preserved (Courtesy of M. Bruneau, Erasme hospital)
-
The laminectomy is extended laterally toward the facets [24].
-
A dural contraincision perpendicular to the paramedian incision directed to the foramen is performed. The dura always adheres to the tumor capsule and has to be cut around the tumor at the level of intra-/extradural communication. This results in a defect, which needs to be closed with a patch (aponeurosis or synthetic) after tumor removal.
-
The extradural component is resected until the distal root is reached. It may be necessary to resect some more bone toward the neuroforamen or to bite some more bone on the medial aspect of the facet joint. In a limited number of cases, when the nerve root appears still functional after electrostimulation distal to the lesion, the extradural tumor can be debulked while leaving the peripheral normal nerve rootlets intact. It exposes nevertheless to the risk of tumor recurrence. The patient must be kept aware of the possibility of postoperative deficit in this condition, but in practice, it rarely happens, thanks to compensating mechanisms that developed over time.
-
-
3.
Extradural and foraminal and/or extraspinal component
There are two options in this case. Some authors advise a posterior approach with facetectomy [7, 25]. It always needs an additional fixation procedure and sometimes a complementary anterior approach if the extraspinal component is large. Moreover at the cervical level, it does not permit a proper control of the VA, which may be hazardous. In case of very large tumor, the posterior approach may need to be completed with an additional anterior approach [6, 7].
The other option is to use the anterolateral approach which in our experience is more advisable since any component from extraspinal to intradural can be resected with a perfect control of the VA and no need for additional fixation [14, 15, 26] (Figs. 42.1d–g, 42.4, and 42.5).
Fig. 42.4 
Extraspinal-foraminal-extradural C5 neurofibroma resected through a lateral approach. (a–c) Preoperative workup. (a) Sagittal T2-weighted MRI showing the intradural extension of the tumor. (b) Angio-CT shows a smaller vertebral artery on the pathological side compared to the right side and an anteromedial displacement by the tumor of the left vertebral artery (arrow) toward the transverse process. The intervertebral foramen is enlarged (*). (c) Axial T1-weighted MRI after gadolinium administration allows the analysis of the anatomical relations of the tumor with the vertebral artery (VA) just in front, the dilated internal jugular vein (IJV), and the internal carotid artery (ICA). Arrowheads delimit the extraspinal extension of the tumor (T). The intradural component severely compresses the spinal cord. (d) Postoperative control after complete resection. The spinal cord (SC) is decompressed. (e–v) Intraoperative images. (e) After lateral retraction of the sternocleidomastoid muscle with a self-retaining retractor, the lateral border of the internal jugular vein is dissected away from the lateral fat. Note the unusual internal jugular vein dilatation. (f) The cervical extension of the tumor is found under the vein after its medial retraction. (The tumor is delimited with arrowheads.) The sympathetic chain (arrow) runs in front of it. (g) The tumor capsule has been opened. (h) The distal aspect of the tumor is controlled after debulking. (i) The longus colli muscle is divided in front of the transverse process. This resection must be done at the level of the transverse processes above and below the tumor. (j) Subperiosteal dissection up to the superior aspect of the C4 transverse process. (k) After resection of the anterior branch of the C4 transverse process, the vertebral artery (arrow) becomes visible. (l) The anterior branch of the C5 transverse process is then resected using a Kerrison rongeur. Obtaining a vertebral artery control at the level of the transverse foramina above and below the tumor is important to subsequently work confidently. (m) The periosteal sheath surrounding the vertebral artery (arrow) is clearly visible and dissected progressively in the cranio-caudal direction. (n) The course of the vertebral artery (arrows) is now identified between C4 and C5 and confirmed on indocyanine green videoangiography (o) which highlights this vessel. (p) The posterior aspect of the vertebral artery is separated from the tumor. This can be done much easier, after tumor debulking. (q) Tumor aspiration is subsequently done with a cavitron ultrasonic aspirator under the vertebral artery. (r) The previously stretched vertebral artery is now decompressed. The intervertebral disk at the C4–C5 level is incised at the level of the uncus (arrow) and a partial oblique corpectomy completed (s). Note the position of the sucker between the drill and the vertebral artery to provide protection of the latter. (t) The posterior longitudinal ligament is incised allowing opening of the dura mater and arachnoid (u) to ensure the absence of any intradural extension. (v) Final view after dural closure and packing the surgical corridor with small pieces of muscle, fat, and biological glue to prevent any cerebrospinal fluid leakage. The vertebral artery runs free in the middle of the field (Reprinted from Bruneau and George [31])
Fig. 42.5 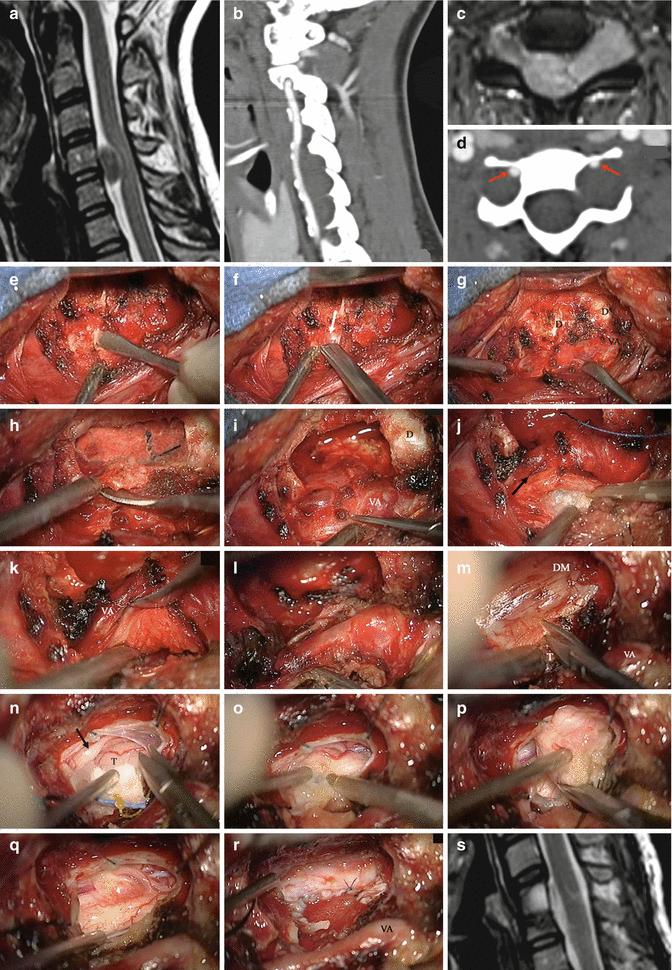
C4–C5 extraspinal-foraminal intra-/extradural neurofibroma compressing the spinal cord. (a–d) Preoperative images. (a) Sagittal T2-weighted MRI. The spinal cord is severely compressed. (b) Angio-CT sagittal reconstruction showing tumoral-induced vertebral artery displacement. Tumor can be seen on three levels. (c) Axial T2-weighted MRI shows the intradural extension. An asymptomatic lesion also exists on the right side. (d) Axial angio-CT scan. The vertebral arteries (arrows) are displaced anteromedially against the bone of the anterior branch of the transverse process. The intervertebral foramen is widely enlarged. (e–r) Intraoperative images. (e) Subperiosteal dissection at the superior border of the C5 transverse process. (f) The vertebral artery appears after resection of the anterior branch of the transverse process (arrow). (g) The vertebral artery (VA) has been exposed on both sides of the tumor. The intervertebral disks (d) are visible. (h) A partial oblique corpectomy has been tailored depending on tumor extension, removing the superior aspect of C5 and C4, but leaving the C3–C4 intervertebral disk intact. The spatula separates the vertebral artery from the uncus. (i) The uncus and lateral border of the vertebrae have been resected by a high speed drill. (j) The extraspinal part of the tumor is removed by ultrasonic aspiration. The black arrow shows the interface between the nerve root sheath and the vertebral artery. (k) This interface is dissected with a spatula for separating the tumor from the vertebral artery. (l) Working laterally and medially toward the vertebral artery allows to resect, respectively, the extraspinal and foraminal-intraspinal components of the tumor. (m) The intradural portion is reached by opening the dura mater (DM). (n) The arachnoid is incised and the intradural portion of the tumor (T) is exposed. The black arrow indicates the tumor-bearing nerve root. (o) The tumor is debulked by ultrasonic aspiration. (p) When its size is reduced, the lesion becomes mobile and can be safely separated from the spinal cord. (q) At the completion of surgery, the spinal cord is completely decompressed. The pathological nerve rootlets have been divided. (r) Closure of the dura mater is obtained with a dural patch. The vertebral artery is well observed. (s) Postoperative sagittal T2-weighted MRI showing the spinal cord decompression (Reprinted from Bruneau and George [31])




-
This anterolateral approach of the cervical spine is performed on a patient in supine position.
-
The skin incision is vertical along the medial border of the sternocleidomastoid (SM) muscle at the corresponding level and extended over 6–7 cm.
-
The field is opened by first exposing the medial aspect of the sternocleidomastoid muscle (SM) which is then retracted laterally until the internal jugular vein (IJV) is reached. The lateral aspect of the IJV is separated from the SM and retracted medially. The retractors are progressively moved down into the field. In contrast to a classical anterior cervical approach, all the vasculo-nervous elements are kept undissected in their sheath and retracted medially together with the trachea and esophagus using a malleable blade.
-
The anterolateral aspect of the vertebral bodies becomes apparent. In the depth of the field, there is a fatty and lymphatic sheath, which is retracted laterally to expose the prevertebral muscles (longus colli and longus capitis).
-
The sympathetic trunk running over these muscles is retracted laterally. This trunk is in close relationship with the fascia. As such, it is safe to dissect the fascia away from the underlying muscles and to fix this fascia with several points laterally.
-
The longus colli muscle is cut transversally above the transverse processes and then longitudinally along the vertebral bodies so that the transverse processes come onto view with the tumor in between the two of them.
-
The VA is controlled above and below the tumor after resection of the transverse processes.
-
The resection of the longus capitis muscle permits the exposure laterally of the distal root. Very often the root is no more functional as demonstrated by the absence of response to its stimulation. In that case, the distal root is cut after coagulation and the tumor can then be debulked progressing from lateral to medial, underneath the VA.
-
Then the VA is mobilized laterally and the tumor remnants, medial to it, are removed.
-
Sometimes a little amount of the bone on the posterolateral aspect of the vertebral bodies needs to be drilled away; this realizes an enlargement of the intervertebral foramen whenever it has not been sufficiently done by the tumor itself.
-
After having resected the extradural part of the tumor, the dura is cut around the tumor where it goes intradurally. The intradural component can then be pulled out and removed progressively until the proximal root becomes visible.
-
The root is cut and the last intradural piece of tumor is removed.
-
The dural defect is closed using some aponeurosis, packed with a piece of fat taken from the fatty sheath, and stuck with fibrin glue [27].
In case there is a response to the stimulation of the root, the tumoral capsule is incised and the tumor debulked with preservation of the intact rootlets following the same progression from lateral to medial: lateral, under, and finally medial to the VA inside the foramen.
-
Closure of the wound is done in three layers: platysma, subcutaneous tissue and skin without drainage.
3.2 Schwannomas of the C1 and C2 Roots
At the C0–C1 and C1–C2 levels, the respective C1 and C2 roots are running behind the joints, which are more anteriorly located than at the lower levels of the cervical spine. Therefore it is possible to enlarge the posterior approach very laterally toward the VA (posterolateral approach) without any drilling of the joint (Fig. 42.6). This enlargement needs to expose the lamina of C2 and the posterior arch of the atlas very far laterally with control of the VA in its groove [28]. In the exceptional case of tumoral extension beyond the VA, the anterolateral approach is necessary in order to achieve a safe control of the VA. The surgical technique of this specific approach has been described elsewhere in this book (Chap. 43).

C1–C2 intra-/extradural neurofibroma. This patient is known for a neurofibromatosis type I. He suffered from a progressive myelopathy due to a C1–C2 neurofibroma. Symptoms resolved after complete tumor removal through a posterolateral approach. (a–c) Preoperative workup. (a) Sagittal T2-weighted MRI. The spinal cord is displaced dorsally by the tumor (arrow). (b) Axial T1-weighted MRI with gadolinium. The tumor (T) extends from the extradural compartment (white arrow) to the intradural one in front of the spinal cord (black arrow). (c) Axial T2-weighted MRI. (d-i). Intraoperative views. (d) The C2 nerve sheath is dissected extradurally. (dm dura mater, occ occipital bone). (e) The dura mater has been incised longitudinally with a contraincision to reach the level of the exiting nerve root. Gentle traction is applied on the extradural tumor remnant. An arrow indicates a C2 posterior rootlet. (f) Pathological rootlets (tumor bearing) are coagulated and will be sectioned. (g) The tumor is progressively debulked by ultrasonic aspiration. An arrow indicates the anterior extension of the tumor, in front of the spinal cord. (h) The lesion can then be progressively mobilized laterally. (i) Final view of the C1–C2 interspace at the completion of the tumor resection (Reprinted from Bruneau and George [27])
4 Complications
In the vast majority of schwannomas located intradurally, mortality and morbidity should be very low. The plane of separation between the tumor and spinal cord is easy to open and manipulations of the cord should be minimal. A complete resection can be achieved in more than 90 %. However, it may happen that a little piece of tumor adherent to the spinal cord has to be left in place with a very low risk of recurrence [29].
Extradural extension into the foramen necessitates a more or less important resection of the facet joints. This raises the question of spinal stability and the need of additional fixation.
The extraspinal extension of those tumors, displacing the VA, can better be resected with adequate exposure of the VA using the anterolateral approach. The VA must be controlled above and below so that any (exceptional) injury can be easily repaired. In this view, evaluation of the size of the VA on preoperative MRI is useful. There is a potential complication (never observed in our experience), related to the injury of a radiculomedullary artery arising at the tumoral level, without supply of the medulla by a collateral network, causing medullary ischemia.
Radicular deficit related to the damage of the nerve root is rare even in the case of a still functional root [30]. However, if there is a response to the stimulation of the distal root, it seems advisable to preserve as much as possible the intact part of the root.
Horner’s syndrome due to damage of the sympathetic trunk (anterolateral approach) may be transiently observed after excessive manipulations but should recover, except if the sympathetic trunk has been cut.
5 Tips and Tricks
-
In case of intradural schwannomas, there is no shame to debulk the tumor if it is safer for the spinal cord and there is no benefit of performing an en bloc removal.
-
In case of extradural extension of the tumor, the anterolateral approach with control of the VA is generally a better choice than a posterior approach with facetectomy and fixation or than a posterior approach combined with an anterior one.
-
A perfect MRI analysis of the different components of the tumor is mandatory before choosing the most suitable approach.
-
Some extradural schwannomas, invaginating the dura, often look as an intra- and extradural type.
-
Evaluation of the size and shift of the VA on the MRI or angio-CT is useful as it helps to anticipate problems.
References
Altas M, Cerci A, Silav G, Sari R, Coskun K, Balak N, Isik N, Elmaci I (2013) Microsurgical management of non-neurofibromatosis spinal schwannoma. Neurocirugia 24:244–249
Celli P, Cervoni L, Tarantino R, Fortuna A (1995) Primary spinal malignant schwannomas: clinical and prognostic remarks. Acta Neurochir 135:52–55
Er U, Kazanci A, Eyriparmak T, Yigitkanli K, Senveli E (2007) Melanotic schwannoma. J Clin Neurosci: Off J Neurosurg Soc Australas 14:676–678
Conti P, Pansini G, Mouchaty H, Capuano C, Conti R (2004) Spinal neurinomas: retrospective analysis and long-term outcome of 179 consecutively operated cases and review of the literature. Surg Neurol 61:34–43; discussion 44
Sachdev S, Dodd RL, Chang SD, Soltys SG, Adler JR, Luxton G, Choi CY, Tupper L, Gibbs IC (2011) Stereotactic radiosurgery yields long-term control for benign intradural, extramedullary spinal tumors. Neurosurgery 69:533–539; discussion 539
Asazuma T, Toyama Y, Maruiwa H, Fujimura Y, Hirabayashi K (2004) Surgical strategy for cervical dumbbell tumors based on a three-dimensional classification. Spine (Phila Pa 1976) 29:E10–E14
Tomii M, Itoh Y, Numazawa S, Watanabe K (2013) Surgical consideration of cervical dumbbell tumors. Acta Neurochir 155:1907–1910
el-Mahdy W, Kane PJ, Powell MP, Crockard HA (1999) Spinal intradural tumours: part I – extramedullary. Br J Neurosurg 13:550–557
Ozawa H, Kokubun S, Aizawa T, Hoshikawa T, Kawahara C (2007) Spinal dumbbell tumors: an analysis of a series of 118 cases. J Neurosurg Spine 7:587–593
Seppala MT, Haltia MJ, Sankila RJ, Jaaskelainen JE, Heiskanen O (1995) Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg 83:621–626
Safavi-Abbasi S, Senoglu M, Theodore N, Workman RK, Gharabaghi A, Feiz-Erfan I, Spetzler RF, Sonntag VK (2008) Microsurgical management of spinal schwannomas: evaluation of 128 cases. J Neurosurg Spine 9:40–47
Gelabert-Gonzalez M, Castro-Bouzas D, Serramito-Garcia R, Santin-Amo JM, Aran-Echabe E, Prieto-Gonzalez A, Allut AG (2011) Tumours of the nerve root sheath in the spine. Rev Neurol 53:390–396
Jinnai T, Koyama T (2005) Clinical characteristics of spinal nerve sheath tumors: analysis of 149 cases. Neurosurgery 56:510–515; discussion 510–515
Hakuba A, Komiyama M, Tsujimoto T, Ahn MS, Nishimura S, Ohta T, Kitano H (1984) Transuncodiscal approach to dumbbell tumors of the cervical spinal canal. J Neurosurg 61:1100–1106
George B, Laurian C, Keravel Y, Cophignon J (1985) Extradural and hourglass cervical neurinomas: the vertebral artery problem. Neurosurgery 16:591–594
Costello F, Kardon RH, Wall M, Kirby P, Ryken T, Lee AG (2002) Papilledema as the presenting manifestation of spinal schwannoma. J Neuroophthalmol: Off J N Am Neuroophthalmol Soc 22:199–203
Kudo H, Tamaki N, Kim S, Shirataki K, Matsumoto S (1987) Intraspinal tumors associated with hydrocephalus. Neurosurgery 21:726–731
Sun H, Tian H (2011) Intraspinal tumors accompanied by hydrocephalus: case report, systematic review, and discussion of treatment strategy. Neurologist 17:342–345
Matsumoto S, Hasuo K, Uchino A, Mizushima A, Furukawa T, Matsuura Y, Fukui M, Masuda K (1993) MRI of intradural-extramedullary spinal neurinomas and meningiomas. Clin Imaging 17:46–52
De Verdelhan O, Haegelen C, Carsin-Nicol B, Riffaud L, Amlashi SF, Brassier G, Carsin M, Morandi X (2005) MR imaging features of spinal schwannomas and meningiomas. J Neuroradiol 32:42–49
Parmar HA, Ibrahim M, Castillo M, Mukherji SK (2007) Pictorial essay: diverse imaging features of spinal schwannomas. J Comput Assist Tomogr 31:329–334
Kufeld M, Wowra B, Muacevic A, Zausinger S, Tonn JC (2012) Radiosurgery of spinal meningiomas and schwannomas. Technol Cancer Res Treat 11:27–34
Raysi Dehcordi S, Marzi S, Ricci A, Di Cola F, Galzio RJ (2012) Less invasive approaches for the treatment of cervical schwannomas: our experience. Eur Spine J 21:887–896
Uede T, Kurokawa Y, Wanibuchi M, Ze PH, Ohtaki M, Hashi K (1996) Surgical approach for cervical dumbbell type neurinoma: posterior approach by partial hemilaminectomy with preservation of a facet joint. No Shinkei Geka Neurol Surg 24:675–679
McCormick PC (1996) Surgical management of dumbbell tumors of the cervical spine. Neurosurgery 38:294–300
Lot G, George B (1997) Cervical neuromas with extradural components: surgical management in a series of 57 patients. Neurosurgery 41:813–820; discussion 820–812
Bruneau M, George B (2011) Surgical technique for the resection of tumors in relation with the V3 and V4 segments of the vertebral artery. In: George B, Bruneau M, Spetzler R (eds) Pathology and surgery around the vertebral artery. Springer, Paris, pp 361–404
George B, Lot G (1995) Neurinomas of the first two cervical nerve roots: a series of 42 cases. J Neurosurg 82:917–923
Nakamura M, Iwanami A, Tsuji O, Hosogane N, Watanabe K, Tsuji T, Ishii K, Toyama Y, Chiba K, Matsumoto M (2013) Long-term surgical outcomes of cervical dumbbell neurinomas. J Orthop Sci: Off J Jpn Orthop Assoc 18:8–13
Celli P (2002) Treatment of relevant nerve roots involved in nerve sheath tumors: removal or preservation? Neurosurgery 51:684–692; discussion 692
Bruneau M, George B (2011) Surgical technique for the resection of tumors in relation with the V1 and V2 segments of the vertebral artery. In: George B, Bruneau M, Spetzler RF (eds) Pathology and surgery around the vertebral artery. Springer, Paris, pp. 165–200
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
George, B., Bruneau, M. (2016). Schwannomas of the Cervical Spine. In: van de Kelft, E. (eds) Surgery of the Spine and Spinal Cord. Springer, Cham. https://doi.org/10.1007/978-3-319-27613-7_42
Download citation
DOI: https://doi.org/10.1007/978-3-319-27613-7_42
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27611-3
Online ISBN: 978-3-319-27613-7
eBook Packages: MedicineMedicine (R0)