
Abstract
Vitamin D has been shown to be essential for various cellular functions. Apart from the role of vitamin D in calcium and bone homeostasis, it plays a crucial role in immune system. The main source of vitamin D is skin synthesis. Patients with inflammatory bowel disease (IBD) are prone to vitamin D deficiency due to a combination of environmental factors and malabsorption from inflamed or partially resected bowel. Consequently, the prevalence of osteopenia and osteoporosis in IBD patients is high. Vitamin D has a proven role in innate and adaptive immunity. It regulates the function of immune system cells, including macrophages, monocytes, dendritic cells, T and B cells. It supports a favorable immune response, mucosa integrity, and a balanced microbiome. Epidemiological data and experimental models support the hypothesis of vitamin D deficiency as a pathogenic mechanism of IBD. Interestingly, a north–south gradient of Crohn’s and ulcerative colitis has been observed, which is linked to decreased skin production of vitamin D in northern latitudes. Clinical and basic studies have demonstrated a correlation between vitamin D status and severity of IBD. Those studies underline the significance of an optimal vitamin D level for patients with IBD, and pose a question for the possibility of vitamin D as therapeutic modality for IBD. This idea has been explored with mixed results. Due to its antibacterial and immunomodulating actions, vitamin D acts prophylactically against Clostridium difficile infection. Furthermore, vitamin D is postulated to potentially lower the risk of colon cancer in IBD patients with its anti-inflammatory properties. Due to its multiple beneficial actions, sufficient level of serum of vitamin D is recommended. More studies are needed to clarify the suspected causative association between vitamin D and IBD pathogenesis, and its use as potential therapeutic modality.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Vitamin D
- Inflammatory bowel disease
- Ulcerative colitis
- Crohn’s disease
- Vitamin D deficiency
- Colon cancer
- Clostridium difficile colitis
- IBD flare
- Metabolic bone disease
- Dysbiosis
Introduction
Vitamin D Synthesis and Metabolism
Vitamin D is an essential vitamin for humans. It plays a crucial role in calcium homeostasis and bone metabolism. Furthermore, vitamin D has key effects on the immune system, muscle function, and brain development [1]. It consists of a group of fat-soluble molecules with a four-ringed cholesterol backbone. The main circulating molecule is the 25-hydroxyvitamin D [25(OH)D] (calcidiol). The active form of vitamin D is 1,25-dihydroxyvitamin D [1,25(OH)2D] (calcitriol). 1,25(OH)2D acts intracellularly, through the vitamin D receptor (VDR), and regulates gene transcription. VDR is a nuclear hormone receptor, can be found in all nucleated cells, and belongs to class II steroid hormone receptor [2].
Vitamin D can be found in a limited number of foods. Its main natural source is the dermal synthesis. Vitamin D in the skin is formed as vitamin D3 (cholecalciferol). 7-dehydrocholesterol in skin cells under exposure to solar ultraviolet B radiation converted to pre-vitamin D3, which is transformed to vitamin D3 after a thermal induction. Skin production is very efficient and minimal exposure of arms and face can produce vitamin D equivalent of 200 international units (IU) from food consumption [3]. Nevertheless, the specific amount of vitamin D produced by sun exposure cannot be estimated with accuracy as it is dependent on the season, latitude, time of the day, the presence of sunscreen and skin type [4]. Of note, melanin lessens the dermal production of vitamin D3. People with limited exposure to sunlight such as disabled persons and older people with less effective cutaneous production are prone to vitamin D deficiency. Vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol) can be found in very few foods, including salmon, tuna, and mushrooms. Human-made ergocalciferol and cholecalciferol supplements have been developed, and fortified food with ergocalciferol and cholecalciferol is common in many countries including the United States [1]. Vitamin D3 and D2 are of similar potency. The absorption of the vitamin D contained in food is performed by enterocytes. Micelles are formed in the gut, absorbed by the enterocytes, and incorporated into chylomicrons. Various diseases affecting the fat absorption distress the vitamin D absorption, examples include Crohn’s disease (CD), pancreatic insufficiency, celiac disease, cholestatic liver disease, and cystic fibrosis [1, 5]. Dermal produced and diet delivered inactive vitamin D is metabolized to the liver and kidneys to its active forms, by two enzymatic hydroxylation reactions, which form 25(OH)D and 1,25(OH)2D, respectively (Fig. 3.1). Synthesis of the active form of vitamin D, calcitriol, is performed by the kidneys, and is regulated by two hormones, the parathyroid hormone (PTH) which increases the production, and fibroblast-like growth factor-23 (FGF23), which decreases it [1]. The half-life of 25(OH)D is 2–3 weeks, while for 1,25 (OH)2D it is between 4 and 6 h.

Vitamin D metabolism
IBD and Vitamin D Deficiency
Vitamin D Requirement s and Deficiency
The ideal level of vitamin D is an area of controversy and under research. Levels of 25(OH)D are used as an estimation of vitamin D adequacy, as this is the best indicator of vitamin D status. Levels lower than 20 ng/mL (50 nmol/L) are generally considered deficient, levels between 21 and 29 ng/mL (52.5 and 72.5 nmol/L) are insufficient and levels between 30 and 100 ng/mL (75 and 250 nmol/L) are considered normal [1, 5–7]. Interestingly, these numbers are based on observations that do not take into account extra-skeletal health. Those observations include sufficient production by the kidneys of 1,25(OH)2D for optimal calcium absorption from the gut, maximum level of suppression of PTH, and a protective level against a clinical end point, such as a fracture. Racial differences in vitamin D levels have been observed. African Americans have lower total serum 25(OH)D concentrations than other races without the consequences of vitamin D deficiency as the bioavailable 25(OH)D is similar between the different ethnic groups. The phenomenon is explained by lower levels of vitamin D-binding protein in this ethnic group as well [8].
Deficiency to vitamin D among people of all ages is very common and has multiple pathogenetic mechanisms [1, 5, 6, 9–11]. Impaired cutaneous production, insufficient dietary intake, and fat malabsorption decrease the availability of the vitamin. Residents of northern latitudes, dark skinned, hospitalized, or institutionalized individuals, and older adults have suboptimal dermal production of vitamin D. Furthermore, older adults minimize the vitamin D containing food intake. Disorders in the metabolism of the vitamin D, like hydroxylation by the liver or kidney, affect the active forms of the vitamin. Finally, in hereditary diseases, such as hereditary vitamin D-resistant rickets, where the VDR is defective and resistant to vitamin D, patients develop rickets within the first 2 years of life. Moreover, obese people, and patients taking medications that increase the metabolism of vitamin D, like phenytoin, are prone to low levels of the vitamin [1, 5, 6, 9–11]. Research data underline the correlation between obesity and vitamin D deficiency, and causative mechanisms include preferred deposition of vitamin D in fatty tissue, making it unavailable, or volumetric dilution, as higher body mass can cause a dilution eff ect [12–15].
Prevalence of Vitamin D Deficiency in IBD
A particularly at risk population for vitamin D deficiency are patients with inflammatory bowel disease (IBD). In addition to environmental and genetic factors mentioned above, IBD-specific factors include an inflamed bowel causing losses through the gastrointestinal tract, resected bowel causing reduced absorption, medication use that affects vitamin D absorption from the intestine, and anorexia from severely active disease. A recent study in pediatric patients with IBD showed an abnormal metabolism of vitamin D, where the PTH is not rationally elevated in the setting of a low vitamin D, compared with healthy controls. Furthermore, conversion of 25(OH)D to 1,25(OH)2D appeared impaired. In the study elevated tumor necrosis factor α (TNF-α) levels were statistically associated with lower 1,25(OH)2D levels. PTH and renal 1-α-hydroxylase suppression from inflammatory cytokines, like TNF-α, may be the cause for abnormal metabolism of vitamin D in IBD patients [16]. Multiple studies have assessed the prevalence of vitamin D deficiency among individuals with IBD, ranging from 22 to 70 % for CD, and as high as 45 % for ulcerative colitis (UC) [17]. In a study of 242 patients with CD from Canada, 8 % of the patients were found to be vitamin D deficient and 22 % of the patients were vitamin D insufficient, defined as 25(OH)D less than 25 nmol/L, and less than 40 nmol/L, respectively. In this patient cohort, predictors of vitamin D deficiency were smoking status, nutrition, and sunlight exposure of the patient [18]. A Norwegian study of 120 IBD adult patients found vitamin D deficiency in 27 % of subjects with CD, and 15 % with UC. The difference was statistically significant between the two groups, P < 0.05. Of note, 37 % of the individuals with CD, who had small bowel resection, were found to have secondary hyperparathyroidism [19].
Metabolic Bone Disease in IBD Patients
Vitamin D and Metabolic Bone Disease
Among the main reasons for the clinically significant metabolic bone disease in IBD patients, vitamin D deficiency plays a crucial role. As a critical risk factor for bone disease, a severe and prolonged vitamin D deficiency can cause hypocalcemia by a decreased intestinal absorption of calcium. Low levels of calcium cause upregulation of the production of PTH, and secondary hyperparathyroidism. This can lead to demineralization of bones and eventually, osteomalacia in adults and rickets and osteomalacia in children. Osteomalacia can be asymptomatic or produce various symptoms like bone pain and muscle weakness, difficulty walking, and fracture [1, 5]. Typical levels of vitamin D (25-hydroxyvitamin D) in the setting of osteomalacia are less than 10 ng/mL.
The prevalence of osteopenia and osteoporosis among patients with IBD appears high. In a study of 63 patients with CD and 41 with UC, 42 % of the patients had osteopenia of the femoral neck [−2.5 Standard Deviation (SD) < bone mineral density (BMD) T score < −1 SD] and 41 % had osteoporosis (BMD T score < −2.5) [20]. In another study of 44 patients with CD and 35 with UC, a high prevalence of osteopenia and osteoporosis were also found, T scores < −1.0 from 51 to 77 %; T scores < −2.5 from 17 to 28 % [21]. A recent study of 143 patients, determined that 48.07 %, and 18.26 % of UC patients had osteopenia and osteoporosis, respectively. For CD patients, 56.41 % had osteopenia, and 15.38 % had osteoporosis [22]. These observations underline the crucial role of adequate vitamin D intake for optimal bone that in turn can improve the overall quality of life for individuals with IBD.
Clinical Consequences of Metabolic Bone Disease in IBD Patients
The clinical significance of osteopenia and osteoporosis of patients with IBD, and the associated risk of fracture have been studied extensively over the past 10 years. The results are conflicting, however, overall an increased risk for fracture among people of IBD has been observed. Several studies highlight the risk of fracture. A large study from the University of Manitoba using an extensive IBD database with 6027 patients, found an increased incidence of fractures, 40 % higher compared with the general population, especially among people older than 60 years of age. More specifically, fractures of the spine, hip, wrist, forearm, and rib were all increased, with incidence ratios 1.74, 1.59, 1.33, 1.25, respectively. Notably, there was no difference between CD and UC, and similar fracture rates were calculated in each age stratum [23]. An analysis of 434 patients with UC, 383 with CD, and 635 controls showed an increased risk of fracture among females with CD, with a relative risk of 2.5. The difference was not statistically significant for male patients with CD or patients with UC [24]. Furthermore, a cohort of CD patients, showed an elevated prevalence of vertebral fractures. Notably, the incidence was similar among patients with normal BMD, and patients with osteopenia and osteoporosis. In the study, the inflammatory process expressed by the C-reactive protein (CRP) positively correlated with height reductions of vertebrae [25]. Subsequent studies have not been able to validate the increased risk of fracture. For example, in a population based study in Olmsted County Minnesota of 238 CD patients were compared with controls matched by sex and age, and the risk of fracture was not increased, compared with the matched controls [26].
The importance of screening for osteoporosis in IBD patients was underlined by the American Gastroenterological Association (AGA). Based on their recommendations, patients with IBD should be screened with dual energy X-ray absorptiometry (DXA) if they have one or more risk factors for osteoporosis, which include postmenopausal women, male older than 50, history of vertebral fractures, hypogonadism, or chronic corticosteroid therapy. Furthermore, they recommend repeat of the test after 2–3 years if the initial test was normal. For patients found with osteoporosis or low trauma fracture, workup for secondary causes of osteoporosis should be initiated, including complete blood count, serum calcium, 25(OH)D, creatinine, alkaline phosphatase, testosterone in males, and serum protein electrophoresis [27]. In the setting of an increased risk of fracture, the impact of osteoporosis and osteopenia on the general health and quality of life of IBD individuals is significant, especially for older a dults.
Vitamin D and Immune Response
Vitamin D plays an important role in innate and adaptive immunity [28–30]. VDR is expressed in the majority of immune system cells like macrophages, monocytes, dendritic cells, T and B cells. Immune cells have the necessary enzymes to convert 25(OH)D to its active form of 1,25(OH)2D. Locally produced active vitamin D has autocrine and paracrine effects, direct and indirect effect on B and T activated cells, modulating effect on the adaptive immune response and on antigen-presenting cells, like dendritic and macrophages, all of which regulate the innate immunity [31]. Largely, this effect facilitates mucosa integrity, supports a balanced microbiome, and promotes an immunosuppressive state by switching from a helper T cell (Th) 1 and 17 profile to Th 2 cell and T regul ator (Treg) cell profile.
Antibacterial Activity of Vitamin D
Vitamin D upregulates the innate immune system and coordinates the immune response to bacterial infections. Therefore, vitamin D antibacterial properties regulate a balanced microbiome. Intracellular bacteria, like Mycobacterium tuberculosis activate Toll-like receptors (TLRs), which institute a direct antimicrobial action against those pathogens. Activation of TLRs of macrophages, by M. tuberculosis derived lipopeptide, upregulates VDR gene and vitamin D-1α-hydroxylase (CYP27b1 in humans) gene, which converts the 25(OH)D to the active 1,25(OH)2D. A cascade of reactions occurs which produce an immune response of the host towards the pathogen, including cathelicidin, an antimicrobial peptide [32]. Vitamin D directly influences cathelicidin production [33]. Moreover, vitamin D stimulates the upregulation of pattern recognition receptor NOD2. Muramyl dipeptide is a product of Gram-negative and Gram-positive bacteria and activates the NOD2 receptor. As a consequence, the nuclear transcription factor kappa-light-chain-enhancer of activated B cells (NF-κB) is stimulated, which causes expression of the gene DEFB2, encoding antimicrobial peptide defensin β2. Importantly, the pathogenesis of CD has been linked with the impaired function of NOD2 and DEFB2 [34].
Autophagy and Vitamin D
Autophagy is an important part of immune innate system. Vitamin D plays a crucial role as it induces and regulates this catabolic process [35]. By affecting different pathways which induce autophagy, vitamin D regulates immune and inflammatory responses. More specifically, 1,25(OH)2D via cathelicidin helps the co-localization of mycobacterial phagosomes with a utophagosomes in human macrophages [36].
Vitamin D and Dendritic Cells
Vitamin D has significant effects on adaptive immunity, as it acts as an immune modulator. VDR can be found in activated B and T cells, and dendritic cells [37]. Dendritic cells, as antigen-presenting cells, act as a messenger between innate and adaptive immune system and play a significant role in the regulation of adaptive immunity. Vitamin D decreases the proliferation, differentiation, and maturation of dendritic cells. Dendritic cells are stimulated by lipopolysaccharide, part of the Gram-negative bacteria cell wall, and are able to produce more 1,25(OH)2D after an increased expression of vitamin D 1α-hydroxylase [38]. Monocytic differentiation to dendritic cells is suppressed by vitamin D action, and in this way the ability of dendritic cells to stimulate T-cell proliferation is reduced. Vitamin D decreases the production of interleukin (IL) 12, and the upregulation of the co-stimulatory molecules cluster of differentiation 40 (CD40), CD80, CD86, and class II major histocompatibility complex (MHC) molecules. Vitamin D also increases the production of IL-10 by the dendritic cells. Overall, the effect is immunosuppressive, as IL-12 induces Th 1 cells, and upregulation of CD40, CD80, and CD86 in antigen-presenting cells activates Th 1 cells. Moreover, vitamin D increases the production of Treg, by an upregulation of Fox2 and IL-10 [39]. In this way, vitamin D supports a nonspecific antigen response and drives a possible over response of the immune system that could lead to pathologic conditions [40, 41].
Vitamin D and Macrophages
Vitamin D upregulates the differentiation of monocytes to macrophages, increases the production of prostaglandin E2, which has immunosuppressant properties, and decreases the granulocyte macrophage colony stimulating factor (GM-CSF). Furthermore, it reduces proinflammatory cytokines like interferon (IFN) γ, lysosomal acid phosphatase, hydrogen peroxide, and macrophage-specific membrane antigens production from macrophages. Of note, decreased production of INF-γ causes impaired activation of macrophages [42]. Also, vitamin D can reduce the antigen-presenting ability of macrophages by blocking the expression of MHC-2 antigens. In addition, 1,25(OH)2D impairs the expression of TLR2, TLR4, and TLR9, and as an effect less IL-6 is produced after a TLR9 challenge [43]. In antigen-presenting cells like macrophages, vitamin D impairs the IL-6 and IL-23 production, thus blocking the Th 17 cells response [39].
Vitamin D and T Cells Differentiation
Vitamin D key targets are the Th 1, 2, and 17 cells, follicular helper T cells (TFH) and Treg cells, and their differentiation. Type 1 Th cells act on cell-mediated immune responses and produce pro-inflammatory cytokines like IFN-γ and lymphotoxin. In IBD, Th1 cells are directed against self-proteins. Type 2 Th cells play a role on antibody-mediated immunity and produce anti-inflammatory cytokines, IL-4, IL-5, and IL-13. Examples of diseases influenced by type 2 Th cells are asthma and food allergies [28]. 1,25(OH)2D suppresses Th1 cells activity, and in this way decreases their production of pro-inflammatory cytokines like IFN-γ, IL-2, and TNF-α. Also, it inhibits the Th 17 and TFH cells pro-inflammatory cytokine production, IL-17 and IL-21, respectively [44]. Vitamin D controls the overproduction of these cytokines, and appears to have a potential role in controlling IBD [30]. Vitamin D acts on the differential of T cells in favor of Th 2, and Treg cells over Th 1 and Th 17 cells. Thus, a balance is achieved between an inflammatory and immunosuppressive response of the immune system. In parallel, vitamin D acts directly on B cells, inhibiting the proliferation and increasing the apoptosis of activated B cells. Also, cytotoxic activity of CD+ T cells is reduced by the action of vitamin D [44–46]. Moreover, 1,25(OH)2D limits the production of plasma cells, immunoglobulin production, and post-switch m emory B cells [47].
Vitamin D and IBD Pathogenesis
Vitamin D deficiency has been proposed as a pathogenetic mechanism of IBD (Table 3.1). Multiple studies and observations underline the significance of vitamin D deficiency in the development of IBD, and possible mechanisms have been suggested. However, only one clinical study has examined the vitamin D level in relation to risk of IBD. A large prospective cohort study of more than 70,000 women found that sufficient levels of vitamin D were linked with sta tistically significant lower incidence of CD, P < 0.02 [48].
North–South Gradient of IBD
Studies in Europe and United States have observed a geographical distribution and variation of UC and CD. The incidence of IBD is higher in northern latitudes [49–52]. The putative explanation for this north–south gradient is the exposure to UVB radiation, which is lower in northern latitudes. Dermal vitamin D production depends on the sunlight exposure, and populations of southern latitudes have lower risk of developing IBD, and low sun exposure has been proven as risk factor for IBD [53, 54].
Distorted Immunity in Vitamin D Deficiency
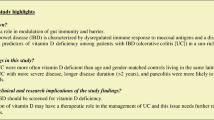
Experimental models have been developed to assess the relation of vitamin D status with the pathogenesis of IBD. An experimental IBD animal model was developed using IL-10 knockout mice, who displayed diarrhea, enterocolitis, and weight loss. The researchers showed that vitamin D deficient mice had more severe symptoms than vitamin D sufficient mice, and the difference was statistically significant [55, 56]. Interestingly, in a similar experimental model with VDR and IL-10 double knockout mice, high expression of inflammatory cytokines, such as IFN-γ, IL-1β, IL-2, IL-12, and TNF-α, was observed in the experimental colitis, and VDR was essential in the model to control the inflammation in the knockout mice [57]. Furthermore, vitamin D appears vital for the preservation of an intact intestinal barrier in the intestine, as it supports the integrity of junction complexes of the mucosa. This was shown in a colitis model using dextran sulfate sodium as stressor for the mucosa of the intestine. Mice deficient of VDR developed severe colitis, characterized by diarrhea, rectal bleeding, and death. These mice were shown to have severe disruption in epithelial junctions and reduction in the junction proteins like claudins, ZO-1, and occludins [58–60]. Interestingly, a disrupted and malfunctioning intestinal epithelial barrier, with distorted tight junctions, has been found in CD, in parallel with impaired expression and distribution of claudin 2, 5, and 8 [60]. Further research with the model of dextran sodium sulfate-induced colitis in mice showed that 1,25(OH)2D produced locally in the colon, and distally in the kidneys affect the severity of the colitis, and mice with normal vitamin D levels demonstrate less histological evidence of colitis, symptom of weight loss, and expression of inflammatory cytokines [61]. In the same animal model, vitamin D has been shown to ameliorate the symptoms of colitis and reduce secretion of TNF-α. The reduction of TNF-α was performed by downregulating a number of genes, which are associated with TNF-α production, a crucial factor of inflammation in IBD [62].
Vitamin D, Dysbiosis, and IBD
Low vitamin D levels can alter the enteric flora and distort the microbiome. Recent studies have proposed an interesting link between vitamin D status, dysbiosis, and IBD. Using the VDR and IL-10 double knockout model, vitamin D deficient mice showed 50-fold bacteria increase in the colon and in parallel, angiogenin-4, an antibacterial protein associated with enteric bacteria control, was reduced. It was hypothesized that vitamin D deficiency influenced a colitis, which was driven by a distorted antibacterial activity and a change in the gut microbiota [63]. In addition, autophagy, as we mentioned earlier, is regulated by vitamin D, and insufficient vitamin D can affect autophagy. This can change the microbiome, the intestinal homeostasis, and contribute to the pathophysiology of IBD. A correlation between vitamin D, dysbiosis, autophagy, and genetic susceptibility for IBD has been observed. Another study demonstrated that vitamin D regulates autophagy gene ATG16L1. This is a susceptibility gene for IBD, which affects the antimicrobial action of Paneth cells and autophagy by decreased lysozyme activity. At the same time, the bacterial product butyrate positively influences VDR and expression of ATG16L1 and reduces inflammation in an experimental colitis model. Vitamin D deficiency could affect intestinal homeostasis by decreased autophagy and lead to development of states of chronic mucosal inflammation, and potentially IBD [64].
Intestinal Inflammation and Vitamin D
The research findings highlight the vital role of VDR for the homeostasis of the mucosal barrier of the intestine and inflammation of the epithelium. A correlation between intestinal inflammation markers, like calprotectin, and vitamin D status has been noted, and underlines the link between vitamin D and gut inflammation. In a study of patients with UC and CD, the serum 25(OH)D was inversely correlated with fecal calprotectin, but not with other systemic inflammation markers like CRP. This correlation was statistical significant [65]. In addition, NF-κB has a critical role in inflammation. VDR negatively regulates the NF-κB by positively modulating the inhibitor of κBα, an endogenous inhibitor of NF-κB, and in this way regulates the inflammation level in the intestine [66]. Moreover, a study showed the anticolitic potential of epithelial VDR, which reduces apoptosis by acting on a crucial pre-apoptotic modulator PUMA, which downregulates and hence decreases the colonic inflammation a nd protects the intestinal mucosa [67].
Vitamin D Receptor Gene Polymorphism
IBD susceptibility appears to have a strong genetic component. Examples of genetic components are VDR and vitamin D-binding protein (DBP) gene polymorphism. VDR gene is located in a region on chromosome 12, and genome screening techniques have found a linkage between the polymorphism of VDR gene with the pathogenesis of IBD [68–70]. A recent meta-analysis evaluated the relation between IBD and four genetic polymorphisms in VDR gene, ApaI, BsmI, FokI, and TaqI. Based on their subgroup analysis, a significant link found between VDR ApaI polymorphism and an increased risk for CD, as well as the TaqI polymorphism and a decreased risk for UC. Furthermore, the study highlights the varying genetic fingerprinting of different ethnic groups [71]. Moreover, DBP gene polymorphism has been associated with IBD. A statistical analysis of 884 individuals, including 636 IBD individuals showed that DBP 420 variant Lys found more frequently in non-IBD controls than in IBD patients [72].
Vitamin D Status and IBD Severity
Multiple clinical studies have been conducted to assess a possible correlation between vitamin D level and severity of IBD. The results of the studies are conflicting, but overall highlight the significance of sufficient vitamin D level for optimal control of IBD. A recent multi-institution IBD cohort with 3217 patients demonstrated that vitamin D deficiency is an independent risk factor for IBD-related surgery. A dose–response correlation was found in the CD cohort, and restoration of normal levels of vitamin D was associated with reduced risk for subsequent surgery [73]. A retrospective cohort study of 101 IBD patients from a single academic tertiary referral center examining the vitamin D status in patients with IBD on anti-TNF-α therapy found vitamin D insufficiency in the cohort of both primary nonresponders and those with a loss of response [74]. Severity of disease activity was found to negatively correlate with 25(OH)D levels in a cohort study of 34 patients with CD [75]. A cross-sectional study of 182 patients with CD found disease activity, assessed by the CD activity index and CRP levels, correlated with lower vitamin D levels [76]. Moreover, in a cohort of 220 IBD patients, 141 with CD and 79 with UC, serum concentration of vitamin D correlates with health-related quality of life in UC and CD during the winter and spring period [77].
Fewer studies explored the significance of optimum vitamin D level for the severity of UC. Vitamin D status and clinical disease activity using the six-point partial Mayo index were assessed in a cross-sectional study with 34 patients with UC, and individuals with low levels of 25(OH)D were statistically more likely to have elevated severity of UC [78]. Recently, preliminary results of a 5-year prospective study of over 1000 patients with IBD found that lower vitamin D levels correlated with poor quality of life, increased utilization of health care system by 44 %, and increased use of medications like steroids, biologics, and narcotics [79]. Although these studies show positive correlations, many studies have found no association between vitamin D status and dise ase severity, even though a large portion of patients were vitamin D deficient [80, 81].
Vitamin D as Therapeutic Modality for IBD
Published data from experimental models of colitis, and observational studies, have shown that vitamin D could be used as a potential therapeutic agent for IBD [39, 58, 82]. Two main treatment studies have examined the effect of vitamin D supplementation on CD and UC, and the potential of its use as a therapeutic modality. A multicenter, randomized, double-blind, placebo-controlled study in Denmark was performed in 180 patients with CD in remission. In the two treatment groups, 1200 IU of 1,25(OH)2D with 1200 mg of calcium or 1200 mg of calcium (placebo group) were administered daily for 1 year. Twenty nine percent of the individuals on calcium alone had a relapse, compared with 13 % for the group of vitamin D, which was not statistically significant (P = 0.06) [83]. A second prospective study in patients with CD compared the efficacy of 1,25(OH)2D and 25(OH)D as a therapeutic intervention for disease activity and bone health [84]. In the short term, after 6 weeks CD activity index, CRP protein, and markers of bone turnover were significantly decreased (P < 0.05) in the 1,25(OH)2D treatment arm. Of note, no significant differences were noted for the 25(OH)D treat ment group at 6 weeks, and for either group at 12 months [84].
Vitamin D and Risk of Clostridium difficile Infection in IBD Patients
Patients with IBD are at increased risk for Clostridium difficile infection (CDI) [85, 86]. Vitamin D influences the antibacterial properties of the intestine, and production of antimicrobial compounds like cathelicidins. It acts prophylactically against infections and as modulator of the microbiome [32, 33, 87]. A recent multi-institutional IBD cohort study found that sufficient plasma 25(OH)D level was associated with lower risk of CDI in IBD patients [88]. Vitamin D could potentially be used to aid in the prevention of CDI.
Vitamin D and Risk of Colon Cancer in IBD Patients
Individuals with IBD are in increased risk for colorectal cancer (CRC). CRC is one of the main causes for mortality among patients with IBD [89]. Inflammation is a risk factor for the development of CRC and frequent relapses of IBD add significantly to that risk [90, 91]. Vitamin D through its anti-inflammatory properties may act as potential protective agent against CRC in IBD. In vitro studies have shown 1,25(OH)2D reduces the growth and promotes differentiation of colon cancer cell lines [92–94]. A study using the human colon cancer line, HT-29, found an impaired growth of HT-29 cells treated with vitamin D. The study proposes a putative target of vitamin D, via the TLR4 pathway, against CRC in populations with IBD [95]. UC patients have lower expression of VDR, and have been shown to have a higher risk of CRC, and thus, a low VDR expression has been proposed as marker of dysplasia and cancer in individuals with UC [96]. A meta-analysis of case–control studies found that daily vitamin D supplementation could decrease the CRC incidence, as patients with sufficient vitamin D serum levels had a 50 % lower risk of CRC compared with patients with low vitamin D levels [97]. Furthermore, daily intake of 1000 IU of vitamin D could reduce the risk for CRC by 50 % [98]. Conversely, a randomized, double-blind, placebo-controlled clinical study of 36,282 postmenopausal women didn’t demonstrate a significance reduction of the risk of CRC among postmenopausal women receiving 400 IU/day of vitamin D for 7 years [99]. Notably, the study has significant limitations as the dose of vitamin D, 400 IU/day, appears lower than the current recommendations, and the serum level of vitamin D was not assessed during the study.
Clinical Recommendations
The significance of optimal vitamin D status for intestinal health and homeostasis is well known and accepted among clinical experts. Even though more research is needed to prove the link between vitamin D deficiency and gut inflammation, it is appropriate to ensure that every patient with IBD has an optimal serum 25(OH)D level (Table 3.2). At this point, no gastroenterology guidelines have been proposed for the assessment of vitamin D status in subjects with IBD. The Clinical Guidelines Subcommittee of The Endocrine Society recommends testing serum 25(OH)D level for every patient with IBD on steroid therapy [6]. We believe that a reasonable approach consists of screening for vitamin D deficiency yearly. More frequent testing is needed in deficient patients with or without metabolic bone disease, and in those with active IBD on steroids. The ideal timing to screen patients is the late winter or early spring when the level of vitamin D is the lowest, especially in patients living in northern latitudes [100]. The U.S. Preventive Services Task Force recently released its recommendations where screening for vitamin D deficiency for asymptomatic adults is not recommended as the current evidence is insufficient to assess the balance of benefit and harm.
The ideal daily vitamin D intake for patients with IBD depends on age and level of serum 25(OH)D. For patients with normal vitamin D levels, infants should receive 400 IU of vitamin D per day, children 1 year and older and adults should receive 600 IU, and the elderly over 70 years 800 IU, based on the recommendations from the Institute of Medicine and the Endocrine Practice Guidelines [101]. For patients at risk for vitamin D deficiency, the recommendation is for at least 1000 IU/day. For adults with documented low levels of 25(OH)D 6000 IU/day for 6 weeks, or 50,000 IU/week for 8 weeks is recommended [6]. The most appropriate vitamin D regimen for patients with IBD was tested in a randomized, controlled, non-blinded, clinical trial. Three different oral regimens were used for 6 weeks, including 2000 IU of vitamin D2 daily, 2000 IU of vitamin D3 daily, and 50,000 IU of vitamin D2 weekly. All 3 regimens were well tolerated, but two oral regimens of 2000 IU of vitamin D3 daily and 50,000 IU of vitamin D2 we ekly were superior in raising the 25(OH)D serum levels [102].
Future Areas of Research
Future research is needed to expand our understanding on various aspects of the interaction between vitamin D status and IBD pathogenesis and its effect on the natural course of IBD (Table 3.3). It is still unclear if low vitamin D is a risk factor for the development of CD and UC. Experimental models have shown a possible relationship but very few clinical studies have been performed and demonstrate a causative association [48]. Most of those studies are cross-sectional and underpowered. More prospective, well-designed studies are needed to clarify the consequences of vitamin D deficiency and answer if vitamin D can prevent the development of the disease. Additional studies are needed to investigate if vitamin D deficiency promotes IBD relapses, or if low vitamin D level is just the result of an inflamed gut with impaired absorption. Data from published research works suggest this association but larger, high quality studies are required to prove the theoretical risk of a more severe disease in the setting of vitamin D deficiency [73–76, 78, 103]. Moreover, the optimal dosing of vitamin D and appropriate vitamin D serum level for ideal intestinal health are additional research areas. The use of vitamin D as a potential therapeutic modality for the treatment of IBD comes with advantages, as it is cheap, easily tolerated and has a safe pharmaceutical profile. Fortunately, research efforts are underway to improve our knowledge of vitamin D deficiency and its effects, and new progress will be made in the prevention and treatment of IBD.
References
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–81.
Lowe KE, Maiyar AC, Norman AW. Vitamin D-mediated gene expression. Crit Rev Eukaryot Gene Expr. 1992;2(1):65–109.
Haddad JG. Vitamin D—solar rays, the Milky Way, or both? N Engl J Med. 1992;326(18):1213–5.
Binkley N, Novotny R, Krueger D, et al. Low vitamin D status despite abundant sun exposure. J Clin Endocrinol Metab. 2007;92(6):2130–5.
Rosen CJ. Clinical practice. Vitamin D insufficiency. N Engl J Med. 2011;364(3):248–54.
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–30.
Institute Of Medicine, Taylor CL, Ross AC, Yaktine AL, Del Valle HB, editors. Dietary reference intakes calcium vitamin D. Washington, DC: National Academies Press; 2011.
Powe CE, Evans MK, Wenger J, et al. Vitamin D-binding protein and vitamin D status of black Americans and white Americans. N Engl J Med. 2013;369(21):1991–2000.
Holick MF, Siris ES, Binkley N, et al. Prevalence of Vitamin D inadequacy among postmenopausal North American women receiving osteoporosis therapy. J Clin Endocrinol Metab. 2005;90(6):3215–24.
Lips P, Hosking D, Lippuner K, et al. The prevalence of vitamin D inadequacy amongst women with osteoporosis: an international epidemiological investigation. J Intern Med. 2006;260(3):245–54.
Holick MF. High prevalence of vitamin D inadequacy and implications for health. Mayo Clin Proc. 2006;81(3):353–73.
Peterson CA, Tosh AK, Belenchia AM. Vitamin D insufficiency and insulin resistance in obese adolescents. Ther Adv Endocrinol Metab. 2014;5(6):166–89.
Drincic AT, Armas LA, Van Diest EE, et al. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity (Silver Spring). 2012;20(7):1444–8.
Mawer EB, Backhouse J, Holman CA, et al. The distribution and storage of vitamin D and its metabolites in human tissues. Clin Sci. 1972;43(3):413–31.
Blum M, Dolnikowski G, Seyoum E, et al. Vitamin D(3) in fat tissue. Endocrine. 2008;33(1):90–4.
Prosnitz AR, Leonard MB, Shults J, et al. Changes in vitamin D and parathyroid hormone metabolism in incident pediatric Crohn’s disease. Inflamm Bowel Dis. 2012;19(1):45–53.
Pappa HM, Grand RJ, Gordon CM. Report on the vitamin D status of adult and pediatric patients with inflammatory bowel disease and its significance for bone health and disease. Inflamm Bowel Dis. 2006;12(12):1162–74.
Siffledeen JS, Siminoski K, Steinhart H, et al. The frequency of vitamin D deficiency in adults with Crohn’s disease. Can J Gastroenterol. 2003;17(8):473–8.
Jahnsen J, Falch JA, Mowinckel P, et al. Vitamin D status, parathyroid hormone and bone mineral density in patients with inflammatory bowel disease. Scand J Gastroenterol. 2002;37(2):192–9.
Pollak RD, Karmeli F, Eliakim R, et al. Femoral neck osteopenia in patients with inflammatory bowel disease. Am J Gastroenterol. 1998;93(9):1483–90.
Bjarnason I, Macpherson A, Mackintosh C, et al. Reduced bone density in patients with inflammatory bowel disease. Gut. 1997;40(2):228–33.
Dumitrescu G, Mihai C, Dranga M, et al. Bone mineral density in patients with inflammatory bowel disease from north-eastern Romania. Rev Med Chir Soc Med Nat Iasi. 2014;117(1):23–8.
Bernstein CN, Blanchard JF, Leslie W, et al. The incidence of fracture among patients with inflammatory bowel disease. A population-based cohort study. Ann Intern Med. 2000;133(10):795–9.
Vestergaard P, Krogh K, Rejnmark L, et al. Fracture risk is increased in Crohn’s disease, but not in ulcerative colitis. Gut. 2000;46(2):176–81.
Siffledeen JS, Siminoski K, Jen H, et al. Vertebral fractures and role of low bone mineral density in Crohn’s disease. Clin Gastroenterol Hepatol. 2007;5(6):721–8.
Loftus Jr EV, Crowson CS, Sandborn WJ, et al. Long-term fracture risk in patients with Crohn’s disease: a population-based study in Olmsted County, Minnesota. Gastroenterology. 2002;123(2):468–75.
Bernstein CN, Leslie WD, Leboff MS. AGA technical review on osteoporosis in gastrointestinal diseases. Gastroenterology. 2003;124(3):795–841.
Cantorna MT, Zhu Y, Froicu M, et al. Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system. Am J Clin Nutr. 2004;80(6 Suppl):1717S–20.
Cantorna MT, Mahon BD. D-hormone and the immune system. J Rheumatol Suppl. 2005;76:11–20.
Reich KM, Fedorak RN, Madsen K, et al. Vitamin D improves inflammatory bowel disease outcomes: basic science and clinical review. World J Gastroenterol. 2014;20(17):4934–47.
Guillot X, Semerano L, Saidenberg-Kermanac’h N, et al. Vitamin D and inflammation. Joint Bone Spine. 2010;77(6):552–7.
Liu PT, Stenger S, Li H, et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science. 2006;311(5768):1770–3.
Adams JS, Ren S, Liu PT, et al. Vitamin d-directed rheostatic regulation of monocyte antibacterial responses. J Immunol. 2009;182(7):4289–95.
Wang TT, Dabbas B, Laperriere D, et al. Direct and indirect induction by 1,25-dihydroxyvitamin D3 of the NOD2/CARD15-defensin beta2 innate immune pathway defective in Crohn disease. J Biol Chem. 2010;285(4):2227–31.
Wu S, Sun J. Vitamin D, vitamin D receptor, and macroautophagy in inflammation and infection. Discov Med. 2011;11(59):325–35.
Yuk JM, Shin DM, Lee HM, et al. Vitamin D3 induces autophagy in human monocytes/macrophages via cathelicidin. Cell Host Microbe. 2009;6(3):231–43.
Provvedini DM, Tsoukas CD, Deftos LJ, et al. 1,25-dihydroxyvitamin D3 receptors in human leukocytes. Science. 1983;221(4616):1181–3.
Fritsche J, Mondal K, Ehrnsperger A, et al. Regulation of 25-hydroxyvitamin D3-1 alpha-hydroxylase and production of 1 alpha,25-dihydroxyvitamin D3 by human dendritic cells. Blood. 2003;102(9):3314–6.
Daniel C, Sartory NA, Zahn N, et al. Immune modulatory treatment of trinitrobenzene sulfonic acid colitis with calcitriol is associated with a change of a T helper (Th) 1/Th17 to a Th2 and regulatory T cell profile. J Pharmacol Exp Ther. 2008;324(1):23–33.
Canning MO, Grotenhuis K, de Wit H, et al. 1-alpha,25-Dihydroxyvitamin D3 (1,25(OH)(2)D(3)) hampers the maturation of fully active immature dendritic cells from monocytes. Eur J Endocrinol. 2001;145(3):351–7.
Penna G, Adorini L. 1 Alpha,25-dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J Immunol. 2000;164(5):2405–11.
Helming L, Bose J, Ehrchen J, et al. 1alpha,25-Dihydroxyvitamin D3 is a potent suppressor of interferon gamma-mediated macrophage activation. Blood. 2005;106(13):4351–8.
Dickie LJ, Church LD, Coulthard LR, et al. Vitamin D3 down-regulates intracellular Toll-like receptor 9 expression and Toll-like receptor 9-induced IL-6 production in human monocytes. Rheumatology (Oxford). 2010;49(8):1466–71.
Jeffery LE, Burke F, Mura M, et al. 1,25-Dihydroxyvitamin D3 and IL-2 combine to inhibit T cell production of inflammatory cytokines and promote development of regulatory T cells expressing CTLA-4 and FoxP3. J Immunol. 2009;183(9):5458–67.
Meehan MA, Kerman RH, Lemire JM. 1,25-Dihydroxyvitamin D3 enhances the generation of nonspecific suppressor cells while inhibiting the induction of cytotoxic cells in a human MLR. Cell Immunol. 1992;140(2):400–9.
Barrat FJ, Cua DJ, Boonstra A, et al. In vitro generation of interleukin 10-producing regulatory CD4(+) T cells is induced by immunosuppressive drugs and inhibited by T helper type 1 (Th1)- and Th2-inducing cytokines. J Exp Med. 2002;195(5):603–16.
Chen S, Sims GP, Chen XX, et al. Modulatory effects of 1,25-dihydroxyvitamin D3 on human B cell differentiation. J Immunol. 2007;179(3):1634–47.
Ananthakrishnan AN, Khalili H, Higuchi LM, et al. Higher predicted vitamin D status is associated with reduced risk of Crohn’s disease. Gastroenterology. 2012;142(3):482–9.
Shivananda S, Lennard-Jones J, Logan R, et al. Incidence of inflammatory bowel disease across Europe: is there a difference between north and south? Results of the European collaborative study on inflammatory bowel disease (EC-IBD). Gut. 1996;39(5):690–7.
Armitage EL, Aldhous MC, Anderson N, et al. Incidence of juvenile-onset Crohn’s disease in Scotland: association with northern latitude and affluence. Gastroenterology. 2004;127(4):1051–7.
Khalili H, Huang ES, Ananthakrishnan AN, et al. Geographical variation and incidence of inflammatory bowel disease among US women. Gut. 2012;61(12):1686–92.
Nerich V, Monnet E, Etienne A, et al. Geographical variations of inflammatory bowel disease in France: a study based on national health insurance data. Inflamm Bowel Dis. 2006;12(3):218–26.
Jantchou P, Clavel-Chapelon F, Racine A, et al. High residential sun exposure is associated with a low risk of incident Crohn’s disease in the prospective E3N cohort. Inflamm Bowel Dis. 2014;20(1):75–81.
Nerich V, Jantchou P, Boutron-Ruault MC, et al. Low exposure to sunlight is a risk factor for Crohn’s disease. Aliment Pharmacol Ther. 2011;33(8):940–5.
Kuhn R, Lohler J, Rennick D, et al. Interleukin-10-deficient mice develop chronic enterocolitis. Cell. 1993;75(2):263–74.
Cantorna MT, Munsick C, Bemiss C, et al. 1,25-Dihydroxycholecalciferol prevents and ameliorates symptoms of experimental murine inflammatory bowel disease. J Nutr. 2000;130(11):2648–52.
Froicu M, Zhu Y, Cantorna MT. Vitamin D receptor is required to control gastrointestinal immunity in IL-10 knockout mice. Immunology. 2006;117(3):310–8.
Kong J, Zhang Z, Musch MW, et al. Novel role of the vitamin D receptor in maintaining the integrity of the intestinal mucosal barrier. Am J Physiol Gastrointest Liver Physiol. 2008;294(1):G208–16.
Henderson P, van Limbergen JE, Schwarze J, et al. Function of the intestinal epithelium and its dysregulation in inflammatory bowel disease. Inflamm Bowel Dis. 2011;17(1):382–95.
Zeissig S, Burgel N, Gunzel D, et al. Changes in expression and distribution of claudin 2, 5 and 8 lead to discontinuous tight junctions and barrier dysfunction in active Crohn’s disease. Gut. 2007;56(1):61–72.
Liu N, Nguyen L, Chun RF, et al. Altered endocrine and autocrine metabolism of vitamin D in a mouse model of gastrointestinal inflammation. Endocrinology. 2008;149(10):4799–808.
Zhu Y, Mahon BD, Froicu M, et al. Calcium and 1 alpha,25-dihydroxyvitamin D3 target the TNF-alpha pathway to suppress experimental inflammatory bowel disease. Eur J Immunol. 2005;35(1):217–24.
Lagishetty V, Misharin AV, Liu NQ, et al. Vitamin D deficiency in mice impairs colonic antibacterial activity and predisposes to colitis. Endocrinology. 2010;151(6):2423–32.
Wu S, Zhang YG, Lu R, et al. Intestinal epithelial vitamin D receptor deletion leads to defective autophagy in colitis. Gut. 2015;64(7):1082–94.
Garg M, Rosella O, Lubel JS, et al. Association of circulating vitamin D concentrations with intestinal but not systemic inflammation in inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(12):2634–43.
Wu S, Xia Y, Liu X, et al. Vitamin D receptor deletion leads to reduced level of IkappaBalpha protein through protein translation, protein-protein interaction, and post-translational modification. Int J Biochem Cell Biol. 2010;42(2):329–36.
Liu W, Chen Y, Golan MA, et al. Intestinal epithelial vitamin D receptor signaling inhibits experimental colitis. J Clin Invest. 2013;123(9):3983–96.
Simmons JD, Mullighan C, Welsh KI, et al. Vitamin D receptor gene polymorphism: association with Crohn’s disease susceptibility. Gut. 2000;47(2):211–4.
Dresner-Pollak R, Ackerman Z, Eliakim R, et al. The BsmI vitamin D receptor gene polymorphism is associated with ulcerative colitis in Jewish Ashkenazi patients. Genet Test. 2004;8(4):417–20.
Naderi N, Farnood A, Habibi M, et al. Association of vitamin D receptor gene polymorphisms in Iranian patients with inflammatory bowel disease. J Gastroenterol Hepatol. 2008;23(12):1816–22.
Wang L, Wang ZT, Hu JJ, et al. Polymorphisms of the vitamin D receptor gene and the risk of inflammatory bowel disease: a meta-analysis. Genet Mol Res. 2014;13(2):2598–610.
Eloranta JJ, Wenger C, Mwinyi J, et al. Association of a common vitamin D-binding protein polymorphism with inflammatory bowel disease. Pharmacogenet Genomics. 2011;21(9):559–64.
Ananthakrishnan AN, Cagan A, Gainer VS, et al. Normalization of plasma 25-hydroxy vitamin D is associated with reduced risk of surgery in Crohn’s disease. Inflamm Bowel Dis. 2013;19(9):1921–7.
Zator ZA, Cantu SM, Konijeti GG, et al. Pretreatment 25-hydroxyvitamin D levels and durability of anti-tumor necrosis factor-alpha therapy in inflammatory bowel diseases. JPEN J Parenter Enteral Nutr. 2014;38(3):385–91.
Joseph AJ, George B, Pulimood AB, et al. 25 (OH) vitamin D level in Crohn’s disease: association with sun exposure & disease activity. Indian J Med Res. 2009;130(2):133–7.
Jorgensen SP, Hvas CL, Agnholt J, et al. Active Crohn’s disease is associated with low vitamin D levels. J Crohns Colitis. 2013;7(10):e407–13.
Hlavaty T, Krajcovicova A, Koller T, et al. Higher vitamin D serum concentration increases health related quality of life in patients with inflammatory bowel diseases. World J Gastroenterol. 2014;20(42):15787–96.
Blanck S, Aberra F. Vitamin D deficiency is associated with ulcerative colitis disease activity. Dig Dis Sci. 2013;58(6):1698–702.
Kabbani TA, Rivers C, Swoger J, et al. Association of mean vitamin D level with clinical status in inflammatory bowel disease: a 5-year prospective study. In: 79th Annual scientific meeting of the American College of Gastroenterology; 2014.
El-Matary W, Sikora S, Spady D. Bone mineral density, vitamin D, and disease activity in children newly diagnosed with inflammatory bowel disease. Dig Dis Sci. 2011;56(3):825–9.
Levin AD, Wadhera V, Leach ST, et al. Vitamin D deficiency in children with inflammatory bowel disease. Dig Dis Sci. 2011;56(3):830–6.
Narula N, Marshall JK. Management of inflammatory bowel disease with vitamin D: beyond bone health. J Crohns Colitis. 2012;6(4):397–404.
Jorgensen SP, Agnholt J, Glerup H, et al. Clinical trial: vitamin D3 treatment in Crohn’s disease—a randomized double-blind placebo-controlled study. Aliment Pharmacol Ther. 2010;32(3):377–83.
Miheller P, Muzes G, Hritz I, et al. Comparison of the effects of 1,25 dihydroxyvitamin D and 25 hydroxyvitamin D on bone pathology and disease activity in Crohn’s disease patients. Inflamm Bowel Dis. 2009;15(11):1656–62.
Trifan A, Stanciu C, Stoica O, et al. Impact of Clostridium difficile infection on inflammatory bowel disease outcome: a review. World J Gastroenterol. 2014;20(33):11736–42.
Regnault H, Bourrier A, Lalande V, et al. Prevalence and risk factors of Clostridium difficile infection in patients hospitalized for flare of inflammatory bowel disease: a retrospective assessment. Dig Liver Dis. 2014;46(12):1086–92.
Guo C, Gombart AF. The antibiotic effects of vitamin D. Endocr Metab Immune Disord Drug Targets. 2014;14(4):255–66.
Ananthakrishnan AN, Cagan A, Gainer VS, et al. Higher plasma vitamin D is associated with reduced risk of Clostridium difficile infection in patients with inflammatory bowel diseases. Aliment Pharmacol Ther. 2014;39(10):1136–42.
Triantafillidis JK, Nasioulas G, Kosmidis PA. Colorectal cancer and inflammatory bowel disease: epidemiology, risk factors, mechanisms of carcinogenesis and prevention strategies. Anticancer Res. 2009;29(7):2727–37.
Federico A, Morgillo F, Tuccillo C, et al. Chronic inflammation and oxidative stress in human carcinogenesis. Int J Cancer. 2007;121(11):2381–6.
Ahmadi A, Polyak S, Draganov PV. Colorectal cancer surveillance in inflammatory bowel disease: the search continues. World J Gastroenterol. 2009;15(1):61–6.
Cross HS, Pavelka M, Slavik J, et al. Growth control of human colon cancer cells by vitamin D and calcium in vitro. J Natl Cancer Inst. 1992;84(17):1355–7.
Hofer H, Ho G, Peterlik M, et al. Biological effects of 1alpha-hydroxy- and 1beta-(hydroxymethyl)-vitamin D compounds relevant for potential colorectal cancer therapy. J Pharmacol Exp Ther. 1999;291(2):450–5.
Bischof MG, Redlich K, Schiller C, et al. Growth inhibitory effects on human colon adenocarcinoma-derived Caco-2 cells and calcemic potential of 1 alpha,25-dihydroxyvitamin D3 analogs: structure-function relationships. J Pharmacol Exp Ther. 1995;275(3):1254–60.
Murillo G, Nagpal V, Tiwari N, et al. Actions of vitamin D are mediated by the TLR4 pathway in inflammation-induced colon cancer. J Steroid Biochem Mol Biol. 2010;121(1–2):403–7.
Wada K, Tanaka H, Maeda K, et al. Vitamin D receptor expression is associated with colon cancer in ulcerative colitis. Oncol Rep. 2009;22(5):1021–5.
Gorham ED, Garland CF, Garland FC, et al. Optimal vitamin D status for colorectal cancer prevention: a quantitative meta analysis. Am J Prev Med. 2007;32(3):210–6.
Gorham ED, Garland CF, Garland FC, et al. Vitamin D and prevention of colorectal cancer. J Steroid Biochem Mol Biol. 2005;97(1–2):179–94.
Wactawski-Wende J, Kotchen JM, Anderson GL, et al. Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Engl J Med. 2006;354(7):684–96.
Pappa H. Vitamin D deficiency and supplementation in patients with IBD. Gastroenterol Hepatol (N Y). 2014;10(2):127–9.
Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53–8.
Pappa HM, Mitchell PD, Jiang H, et al. Treatment of vitamin D insufficiency in children and adolescents with inflammatory bowel disease: a randomized clinical trial comparing three regimens. J Clin Endocrinol Metab. 2012;97(6):2134–42.
Ulitsky A, Ananthakrishnan AN, Naik A, et al. Vitamin D deficiency in patients with inflammatory bowel disease: association with disease activity and quality of life. JPEN J Parenter Enteral Nutr. 2011;35(3):308–16.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Desalermos, A.P., Farraye, F.A., Miller, H.L. (2016). Vitamin D and Inflammatory Bowel Disease. In: Ananthakrishnan, A. (eds) Nutritional Management of Inflammatory Bowel Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-26890-3_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-26890-3_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-26888-0
Online ISBN: 978-3-319-26890-3
eBook Packages: MedicineMedicine (R0)