
Abstract
Recurrence of pectus excavatum deformities occurs after both open and MIRPE. Recurrence risks are also based on multiple factors and differ based on the initial repair procedure. Identifying the contributing factors to a previous procedure’s failure is critical to proper repair and prevention of another recurrence. Each case must be taken on an individual basis and is contingent on the patient’s anatomy and previous repair technique. A combination of surgical techniques may be necessary in to successful repair some patients.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Background
Surgical repair of pectus excavatum (PE) has evolved significantly over the past 50 years. There are a variety of techniques that have been successfully used on patients of all ages but the two most common methods used today include modifications of the open Ravitch approach and the minimally invasive repair (MIRPE) or “Nuss”. Recurrence rates after repair of PE using both techniques have been reported in 2–37 % of patients [1–17]. No high-quality reports comparing long-term recurrences of MIRPE to open repair have been published. The cause of recurrence varies based on the technique of initial repair utilized. For patients presenting after failed or recurrent primary MIRPE repair; the placement, number of bars, bar migration, and too early of support removal can all be associated with failure (Figs. 15.1a, b and 15.2a, b) [2, 4, 12–14, 18–28]. Connective tissue disorders can complicate and increase recurrence risk in both previous Nuss and open PE repairs [1, 4, 29, 30]. Recurrence risks for the open repair are also based on multiple factors which include incomplete previous repair, repair at a young age, dissection either too extensive or too little, early removal or lack of support structures, and incomplete healing of the chest wall with pseudoarthrosis and necrosis (Fig. 15.3a, b) [1, 3, 5, 8, 13–15, 16, 21, 31–34, 35, 36].

(a, b) Failure of the Nuss procedure can be due to bar rotation or migration as is seen in these two patient’s lateral chest roentgenogram (a) rotation of a long bar with single stabilizers is seen, (b) Rotation of the lower bar is seen on this patient with 2 support bars and stabilizers

Too lateral entrance of the support bars positions the support bars intrathoracic and fails to elevate the defect anteriorly. (a) posteriorly displaced bar is seen on in this patient’s lateral chest roentgenogram. Arrow point to pectus excavatum defect still seen below the level of the bar. (b) computerized tomography shows intrathoracic portion of support bar with failure to support and elevate the pectus excavatum defect. Arrow points to the space between the chest wall and the bar

Malunion and recurrence of pectus excavatum defect after previous Ravitch repair are seen in these patient’s photographs, computerized tomography and 3-D reconstruction images (a) A 46 year-old female with significant recurrence after open Ravitch procedure. CT scan shows failed union between the rib (thin arrow) and Sternum (thick arrow) (b) A 44 year old male with significant recurrence after open Ravitch procedure. 3D reconstruction shows recurrence and failure of the chest wall to reconstitute
Regardless of which initial procedure was used, some patients will experience recurrence. There are only a few publications devoted exclusively to repair of recurrent pectus deformities, and most studies include children with only a few adults [1–5, 9, 11, 13, 14, 31, 37]. Several of these publications are reviewed in Table 15.1. Most of these reports describe experience with a single operative technique in the repair of recurrent pectus excavatum. The reports by Redlinger and Croitoru et al. advocated a modified Nuss technique for both open and Nuss recurrent PE [13, 14]. Multiple bars were required and they reported slightly higher complication and bar displacement rates with revision versus primary repairs. Others have advocated the use of a modified open Ravitch repair in all patients with recurrent PE, reporting excellent results in a small group of patients, with only a marginally longer length of stay compared to patients undergoing primary repair (6 days versus 5 days) [9]. Studies have shown that repairs in adults may be more difficult and have increased risks of complications due to increased rigidity of the chest wall [3, 7, 10, 18, 30, 31, 38–48]. Complex open repairs were required in many adult patients after prior open repair when compared to other studies [9, 32, 33]. Luu et al., reported on 13 recurrent patients in ages 16–54 years [9]. Eight of these were previous MIRPE and 5 had been a modified Ravitch repair. All of the failed MIRPE procedure patients in this series underwent a modified Ravitch repair for correction, while the recurrent open repair patients required complex reconstructions. Results are reported as good or excellent in many patients undergoing reoperation [5, 9, 11, 31, 49]. Follow up is limited and the long-term durability of repairs unknown. Many publications do not report their length of follow up. Those studies that do provide a longer length of follow up have shown good efficacy in preventing further recurrence of PE during the follow-up periods [2, 5, 11, 31, 49].
Surgery for Recurrent Pectus Excavatum
In general, reoperative repair should avoid or repair the issues that contributed to the first surgical approach recurring. Assessment of why a patient’s repair was unsuccessful or recurred is necessary for treating recurrence adequately. Both open and minimally invasive techniques have been described for repair of recurrent PE. Both approaches can offer advantages in the repair of recurrent defects, however, some recurrent defects may require an application of both open and minimally invasive repair techniques to achieve optimal outcomes. Regardless of the approach advocated, reports describing experience with repair of recurrent PE all mention the increased technical difficulties, higher complication rates and longer hospital stays [9, 11, 13, 14].
Recurrent Pectus Excavatum after MIRPE or Nuss Procedure
Recurrences following the Nuss repair are reported at a similar rate as that seen after Ravitch however many aspects of the presentation differ. Technical issues constitute a large proportion of the cases reported as “failed” versus “recurrent” in patients repaired with MIRPE. Some of the more common technical failures and causes reported for recurrent PE after Nuss procedure are listed in Table 15.2.
The majority of experienced centers reporting on revision of prior failed or recurrent MIRPE patients found that malpositioned or displaced bars were a large portion of the issue [2, 5, 13, 14, 31] (Fig. 15.4a–c). Bar displacement is the most common complication following Nuss repair, with displacement rates greater than 10 % in some studies [6–8, 12, 19, 23, 25–27, 42, 43, 50–54]. Adult patients have also been noted to have a greater incidence of bar rotation and complications [4, 5]. This can lead to recurrence of the pectus deformity as well as need for subsequent reoperation. There are a variety of different issues that can lead to bar rotation and migration. The majority of revisions reported on noted bars that were too long (Fig. 15.5) [13, 14]. These bars were replaced with bars that were 1–4 in. shorter on average. Bars that were placed too lateral or intercostal stripping and lateral displacement occurring after placement was another common technical issue noted (Fig. 15.6a, b). When lateral displacement occurs, the bar will fail to contact the sternum and support it anteriorly (Fig. 15.7). The entry and exit sites into the chest should not be too lateral or muscle stripping can occur [13, 14, 20, 26, 53]. Use of a different interspace was recommended should intercostal stripping and lateral displacement occur [13]. Figure of eight suture reinforcement of the ribs bordering the stripped intercostal space can also be performed. The utilization of forced sternal elevation may also help facilitate bar placement and rotation and minimize intercostal stripping [55].

(a–c) Lateral chest and A/P roentgenograms show bar rotation and migration in three patients after Nuss pectus excavatum repair

Lateral roentgenogram of patient with recurrent pectus defect less than 1 month after Nuss repair and placement of single bar. Note a longer than recommended length of bar and curvature beyond the mid-axillary line with rotation and displacement

(a, b) Lateral chest roentgenograms showing single pectus bar with failed elevation of the pectus excavatum defect secondary to lateral displacement (a) and intrathoracic migration (b). Arrows note pectus excavatum deformity still present despite support bar indwelling

Thoracoscopic view of intrathoracic pectus support bar which fails to contact the anterior chest wall due to lateral intercostal placement. Arrow notes space between chest wall and support bar
Adequate stability is also impacted by the number of bars and balance of the chest wall on support structures. For heavier, stiffer chests, several bars may be necessary to support the weight and elevate the defect. The pressure required to elevate the chest is significant and an inadequate number of bars to support the chest anterior can lead to lateral stripping of the intercostals and increased risk of bar rotation [22, 27, 55–58]. Recommendations as to what the adequate number of bars are varies [6, 18, 20, 25, 53, 59]. Initial reports of the Nuss procedure encompassed young patients with only one bar advocated however the majority recommend increased number of bars with more significant defects and advanced ages [53]. Older patients have also been reported by others to require more bars for PE repair and two or more bars may give better and more stable results [18, 25, 58, 60, 61]. For some patients presenting with reported recurrence, there may have been an incomplete repair of their defect following the initial Nuss with a portion of their defect remaining postsurgical due to an inadequate number of support bars (Fig. 15.8a–c) [3].

(a–c) Photographs (a) and radiographic imaging (b, c) are shown of a 26 year-old male with pectus excavatum deformity 2 years after placement of single support bar with residual defect of Haller Index 4.6 and chronic postoperative pain. The single bar fails to elevate and support the defect inferiorly
Recurrence has also been attributed to premature removal of the pectus bars before adequate remodeling has occurred and the chest wall secured into a corrected position. The optimal length of time recommended to leave support bars in place varies however, several experienced centers have increased their recommended time to 2–3 years [6, 7, 25, 40, 57, 62]. Patients with Marfan’s and other connective tissue disorders have been shown to have a higher risk for recurrence and recommendations are for leaving the bars in place for up to 4 years [1, 4, 29].
A significant problem encountered after a failed Nuss can be extensive intrathoracic adhesions [5]. These can require several hours of extensive adhesiolysis before dissection across the chest and mediastinum is achieved for bar placement. Use of sternal elevation may be helpful and others have described a subxiphoid incision to manually elevate the sternum during dissection across the chest, especially with extensive adhesions [5, 9, 13, 14, 63, 64].
Recurrent Pectus Excavatum after Ravitch and Open Procedures
The original open procedure for PE repair was described and accredited to Ravitch in the 1940s [65, 66]. Modifications of this technique have been used successfully for several decades [2, 15, 42, 67–69]. The open repair involves resection of the deformed costal cartilage with or without sternal osteotomy. Recurrence risks are based on multiple factors as listed in Table 15.3. Once recurrence occurs, subsequent repair becomes more complex. The challenges encountered with re-operative repair can vary based on the extent of initial operative repair. There is limited literature published on repair of recurrent open PE, however, most reported higher complication rates, longer hospital stays, and higher rates of bar displacement when repaired with MIRPE [5, 13, 14].
Surgical repair of patients having undergone a previous Ravitch or other open PE repair technique may have unique problems when recurrence occurs. Repair can be quite challenging due to rigidity of the bony chest wall and scar tissue from the prior surgical intervention. Extensive calcification, ossification and fusion of the previously excised cartilage may prevent adequate elevation of the chest wall without reexcision [9, 32, 33, 35, 70]. Osteotomies of the sternum, sterno-costal junctions and more laterally along the ribs may be necessary to mobilize the anterior chest wall. Recurrences following open PE repair can also arise from osteonecrosis, malunion due to pseudomembranous attachments, instability and/or chest wall hernia (Fig. 15.9a, b) [1, 3, 4, 9, 17, 31, 33]. When non-union occurs bilaterally, this can also lead to an entity known as “floating sternum”, which requires revision to reattach and stabilize the sternum (Fig. 15.10) [34, 36, 71].

(a, b) Computerized tomography (a) of the chest and intraoperative photograph (b) showing fibrous malunion and recurrence due to improper healing after prior Ravitch pectus repair. The instrument is place under the lower cartilage attachments which are completely separate from the sternum. Arrows

Intraoperative photograph showing “sternal floating” after prior open Ravitch pectus repair with bilateral non-union of costocartilages and sternum
Successful repair of areas of malunion, pseudo-arthrosis and sternal floating requires repeat open repair. Open repair and stabilization has also been recommended by other authors for these complicated recurrences [3, 9]. Rib/sternal reattachment and sites of repeated osteotomies prone to malunion or non-union can be approximated with titanium plating or FiberwireTM (Arthrex, Inc, Naples, FL).
Rigidity of the chest wall following Ravitch is the main component that must be overcome to achieve an adequate repair. MIRPE is more difficult as a result, and bar displacement more likely. Additionally, a study by Redlinger et. al. also mentions findings of significant intrathoracic adhesions following Ravitch repair, despite this being considered an extra-pleural repair, making placement of pectus bars difficult [13]. The use of forced sternal elevation to move the sternum anterior has been reported to be helpful for safe dissection and repair with MIRPE [55, 57, 72–74].
Despite these challenges, MIRPE following previous open repair can be quite successful [5, 11, 14, 31]. Redlinger et al. reported on 100 patients they successfully repaired with the Nuss procedure after recurrences (45 prior open and 51 prior Nuss) [13]. Repair of patients with previous Ravitch procedures required multiple bars. Opening the previous Ravitch incision for manual lifting of the sternum during the dissection under the pectus defect was felt to significantly improve the safety of the dissection and success of the procedure [13].
Rarely following Ravitch repair at too young and age, patients can have impairment of the normal chest wall growth, or acquired asphyxiating thoracic dystrophy, which was first described by Haller in 1996 [35]. Haller speculated that this “acquired Jeune’s syndrome” was related to disruption of the normal growth centers of the affected ribs. These patients typically had repair of their defect at a very young age (<4 years), which had been common in the 1970s and 1980s. This is a complicated disorder with high risks for reconstruction to improve the chest defects presents. These patients required complex reconstructions of which discussion is beyond the context of this report and limited reports are published [21, 32, 35].
Indications for Surgical Revision Repair
Indications for repair of recurrent pectus excavatum are similar to those for primary repair and reviewed in Table 15.4 [1, 3–5, 9, 11, 14, 37, 64, 75–82]. Those patients with a recurrent, significant defect and those with symptomatology correlating with the return of their defect, including dyspnea, palpitations, and inability to keep up with their peers, all factor into the decision to repair a recurrent defect. Additionally, patients that have undergone previous open repair may have areas of non-union, chest wall hernias and other conditions that lead to chronic pain and chest wall instability [3, 33–35, 37, 71, 76]. Resultant symptoms from this type of defect can be severe and may be an indication for surgery despite not meeting criteria based on the measurements of their defect. Reoperation should be individualized to the patient with great consideration given to the increased operative complexity and risk of complications. Extensive patient education about the surgical complications, recovery period, and final results are necessary to create realistic expectations for the patient.
In general, we have approached all our revision cases from a stepwise evaluation including:
-
1.
Physical exam to identify areas of pseudoarthrosis and malunion between the sternum and ribs, or serial instability of the costal joints “floating sternum” [36, 71]. Assessment of compliance and residual flexibility of anterior chest wall.
-
2.
CT or MRI studies of the chest are necessary to allow for measurements of the defect, but also for visualization of areas of malunion or non-union that are not appreciated on physical exam. Identification of chest wall hernia, irregular cartilage regeneration at the retrosternal level and incomplete reunion of previous resection sites can be performed [70, 81, 83–85].
-
3.
Evaluation of prior operative notes, chest roentgenograms and films relative to patient’s prior procedures.
-
4.
Evaluation of physiologic abnormalities which may include echocardiogram, pulmonary functions and cardiopulmonary V02 and exercise parameters [7, 23, 75, 80, 81, 86–92].
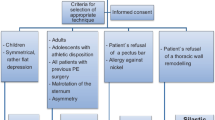
For the majority of reoperative patients, we plan MIRPE utilizing forced elevation (Johnson, ATS publication pending) (Fig. 15.11a, b). shows an algorithm for our approach to revision patients. Open resection with osteotomy and partial modified revision Ravitch are performed when necessary if the chest wall will not elevate adequately. Patients with pseudoarthrosis or “floating sternum” are planned for a combined procedure with elevation of the chest wall and stabilization of sternocostal instability [36, 71]. Patients with acquired thoracic dystrophy require more complex open reconstructions [32, 35] Table 15.5 outlines the operative steps:

(a, b) Algorithm for surgical approach to recurrent patients (a) previous Nuss/Minimally invasive pectus excavatum repair (b) open repair
Procedure Detailed Description
All patients are administered intravenous antibiotic prophylaxis prior to initiation of procedure. General anesthesia with double-lumen intubation is performed. A transesophageal echocardiogram probe is placed and cardiac compression, function, and absence of pericardial effusion documented throughout the case. The patient is placed in supine position with arms secured at the sides. Two longitudinal 5-in. rolls are placed under the back parallel to the spine and the arms padded and tucked at the sides. Groins are left exposed and prepped into the surgical field should emergent access and cardiopulmonary bypass be necessary (Fig. 15.12). This positioning facilitates access to both anterior and lateral aspects of the chest wall for placing and affixing bars.

All reoperative recurrent pectus excavatum patients are positioned supine with arms tucked at the sides and groins exposed should emergent cardiopulmonary bypass be necessary. This positioning facilitates access to both anterior and lateral aspects of the chest wall for placing and affixing bars
Single 3-cm incisions are made bilateral following the rib contour at the inferolateral pectoral borders. Incisions are positioned to allow access to the intercostal spaces adjacent to the defect. Sub-muscular pockets are developed utilizing electrocautery to elevate the pectoralis muscles off the chest wall along the anterior and lateral chest wall. Initially a 5 mm port is placed through the right incision and carbon dioxide insufflation to 5–8 mmHg pressure is utilized. A 5-mm flexible endoscope (Olympus 5-mm Endoeye Flex 5, Central Valley, PA) is placed and allows safe placement of a second 5 mm port inferiorly in the right chest for visualization of intrathoracic procedures. Careful takedown of intrathoracic adhesions is performed under direct visualization. No attempt to cross the mediastinum occurs until sternal elevation is achieved.
Elevation with the RulTract Retractor (Ruletract Inc., Cleveland, OH) is then attempted (Fig. 15.13) [55, 57].Two-mm incisions are placed on either side of the sternal defect and the perforating tips of a bone clamp (Lewin Spinal Perforating Forceps, V. Mueller NL6960; CareFusion, Inc, San Diego, CA) are inserted into the sternum. The clamp is then fully closed. The RuleTract Retractor is attached to the table at the level of the mid-sternum on the left side. The sternum is then attempted for elevation.

Elevation with the RulTract Retractor (Ruletract Inc., Cleveland, OH) attached to the table at the level of the mid-sternum on the left side is attempted. A perforating tips bone clamp (Lewin Spinal Perforating Forceps, V. Mueller NL6960; CareFusion, Inc, San Diego, Calif) and attached to the retractor
If Elevation Is Achieved, a Modified Nuss Will Be Performed for the Revision Case
Procedure for Modified Nuss for Revision
The first bar is positioned in the interspace at the superior aspect of the defect. A second bar is then placed 1–2 inner spaces below this one. If there is residual lower defect, a third bar will be placed (Fig. 15.14a, b). Bars are sized and shaped to best correct the patient’s defect. We use shorter bar lengths and try to minimize the lateral extension of the bar around the chest. Bars are custom bent and shaped for individual patients. Bars are flipped into place with the sternum still held elevated to minimize stress lateralized to the intercostal space. Bilateral circumferential fixation of the bars around the rib using FiberWire® (Arthrex Inc, Naples, FL) is performed. The technique for this has been previously published [93]. Two or three sites of fixation are performed bilaterally for each bar. Fixation should incorporate the islet of the bar bilateral and incorporate a rib either directly below or on either side of the bar. A second and sometimes 3rd site of fixation should be placed more medial on each side closer to the rotational fulcrum depending on the pressure and stability of the bar placement. A small right angle is used to pass the FiberWire® suture through the intercostal space just above a rib and directed towards the apex. The suture is again grasped by passing the right angle inferior to rib. The suture is then securely tied over the bar lying partly in the grooves.

(a, b) Intraoperative photograph and chest roentgenograms showing the placement of 2 and 3 Nuss support bars for repair of pectus excavatum deformity
If Forced Sternal Elevation Cannot Elevate the Chest Anteriorly or Malunion and Sternal Floating Evident
Procedure for Combined Open and Modified Nuss for Revision
If forced sternal elevation cannot elevate the chest anteriorly or malunion and sternal floating evident, the midline incision from patient’s previous open procedure is excised and dissection taken down to the bony chest wall. Sites of calcified restriction or malunion are identified. If cartilage and perichondrium remains, a limited cartilage resection is performed. These techniques are similar to those used in the modified Ravitch repairs, but are limited to areas that will not elevate and in sites with persistent malformation following elevation. For many patients, osteotomy of the sternum and improperly positioned, fused ribs may be required due to extensive scar tissue and calcification. In these scenarios, multiple osteotomies may be required at fixed sites and the sternochondral junctions using bone chisels or a powered bone saw.
Once chest mobility is obtained and anterior elevation is obtained with the RuleTract, exploration and takedown of the mediastinum is thoracoscopically performed. A combination of electrocautery and blunt dissection of pleural and mediastinal adhesions is performed. In cases with significant pericardial adhesions to the sternum, a subxiphoid approach is additionally used for direct takedown of scar tissue by pulling the sternum upward and looking directly. Others have also reported using this approach to safely dissect thru the adherent mediastinal structures [5, 13, 31]. Once the dissection is complete, the Lorentz dissector (Biomet MicroFixation, Jacksonville, FL) is passed across from the right interspace to the contralateral side for guided placement of the support bars (Fig. 15.15). The procedure as previously described is performed for placement of 2–3 support bars and FiberWire securing.

Intraoperative photograph of patient with recurrent severe pectus excavatum after open Ravitch. Extensive malunion is seen. Areas of pseudoarthrosis and fibrous malunion are debrided back to healthy tissue. Stainless steel pectus bars are placed to elevate and support the chest anterior. Bone graft and plating will then be utilized to further stabilize and repair these sites
Extensive calcification of the chest wall following repair can be equally debilitating following open repair. Correction of this condition is extremely difficult, with the concern that any subsequent repair may result in a similar result as scarring occurs following operative intervention. Osteotomies of the sterno-costal junctions, as well as osteotomies more laterally along the ribs may be necessary to mobilize the anterior chest wall. Repeated osteotomies in similar locations are prone to malunion or non-union, which has led to our use of titanium plating or Fiberwire to stabilize these areas. Open repair can also lead to disruption of the blood supply to portions of the bony portions of the chest wall, which can lead to sections of the chest wall that are absent. These areas are difficult to stabilize, and titanium plating is at times necessary to restore chest wall stability [34, 37]. Titanium sternal plating (Biomet Microfixation, Jacksonville, FL and DePuy Synthes) and FiberWire fixation is then utilized to approximate the sites of costocartilage/rib to the sternum following elevation. Plates are chosen based on length and shape to best accommodate the fixation (Figs. 15.16 and 15.17). Multiple plates are utilized for all unstable areas and FiberWire for attachment to the sternum at other sites. For more extensive deformities with osteonecrosis and extensive chest wall hernia, use of cadaveric bone graft, methylmethacrylate and biologic mesh can be utilized for repair. These more extensive techniques are covered in previous publications [32, 33].

Intraoperative photograph of titanium plating utilized to secure a site of malunion after failed Ravitch procedure

Chest roentgenogram is shown of patient postoperative from revision procedure after recurrent Ravitch. Sites of malunion were stabilized with titanium plates. Two support Nuss bars were utilized
Support bars are securely affixed to the chest wall and then the sternum is released and the bone clamp removed. The pectoralis muscles are reattached to the chest wall covering the bars and incisions closed with layered absorbable suture. A single approximating stitch is placed on the sites of the clamp insertion.
Once the chest wall defect is completely corrected, the pectoralis muscle and fascia, as well as the rectus abdominus muscle and fascia are reattached to the chest wall. The incisions are closed with layered absorbable suture. Chest tubes are placed through the lower port site on the right and left if deemed necessary.
Conclusion
Recurrence of pectus excavatum deformities occurs after both open and MIRPE. Recurrence risks are based on multiple factors and differ based on the initial repair procedure. Identifying the sources of a previous procedure’s failure is critical to preventing the recurrence. Surgeon experience with the type of procedure is also important as reoperative cases can be difficult and are prone to increased complications. Complete correction of the pectus defect may not possible with MIRPE alone, and a combination of surgical techniques may be necessary in many patients. Each case must be taken on an individual basis based on that patient’s anatomy and previous repair technique.
References
Ellis DG, Snyder CL, Mann CM. The ‘re-do’ chest wall deformity correction. J Pediatr Surg. 1997;32(9):1267–71.
Antonoff MB, Erickson AE, Hess DJ, et al. When patients choose: comparison of Nuss, Ravitch, and Leonard procedures for primary repair of pectus excavatum. J Pediatr Surg. 2009;44(6):1113–8; discussion 118–9.
Colombani PM. Recurrent chest wall anomalies. Semin Pediatr Surg. 2003;12(2):94–9.
De Ugarte DA, Choi E, Fonkalsrud EW. Repair of recurrent pectus deformities. Am Surg. 2002;68(12):1075–9.
Guo L, Mei J, Ding F, et al. Modified Nuss procedure in the treatment of recurrent pectus excavatum after open repair. Interact Cardiovasc Thorac Surg. 2013;17(2):258–62.
Kelly RE, Goretsky MJ, Obermeyer R, et al. Twenty-one years of experience with minimally invasive repair of pectus excavatum by the Nuss procedure in 1215 patients. Ann Surg. 2010;252(6):1072–81.
Kelly Jr RE, Mellins RB, Shamberger RC, et al. Multicenter study of pectus excavatum, final report: complications, static/exercise pulmonary function, and anatomic outcomes. J Am Coll Surg. 2013;217(6):1080–9.
Liu T, Liu H, Li Y. Comparison of the Nuss and sternal turnover procedures for primary repair of pectus excavatum. Asian J Surg. 2014;37(1):30–4.
Luu TD, Kogon BE, Force SD, et al. Surgery for recurrent pectus deformities. Ann Thorac Surg. 2009;88(5):1627–31.
Mansour KA, Thourani VH, Odessey EA, et al. Thirty-year experience with repair of pectus deformities in adults. Ann Thorac Surg. 2003;76(2):391–5; discussion 395.
Miller KA, Ostlie DJ, Wade K, et al. Minimally invasive bar repair for ‘redo’ correction of pectus excavatum. J Pediatr Surg. 2002;37(7):1090–2.
Nasr A, Fecteau A, Wales PW. Comparison of the Nuss and the Ravitch procedure for pectus excavatum repair: a meta-analysis. J Pediatr Surg. 2010;45(5):880–6.
Redlinger Jr RE, Kelly Jr RE, Nuss D, et al. One hundred patients with recurrent pectus excavatum repaired via the minimally invasive Nuss technique--effective in most regardless of initial operative approach. J Pediatr Surg. 2011;46(6):1177–81.
Croitoru DP, Kelly Jr RE, Goretsky MJ, et al. The minimally invasive Nuss technique for recurrent or failed pectus excavatum repair in 50 patients. J Pediatr Surg. 2005;40(1):181–6; discussion 186–7.
Fonkalsrud EW. 912 open pectus excavatum repairs: changing trends, lessons learned: one surgeon’s experience. World J Surg. 2009;33(2):180–90.
Willital GH, Meier H. Cause of funnel chest recurrences---operative treatment and long-term results. Prog Pediatr Surg. 1977;10:253–6.
Kasagi Y, Wada J, Nakajima H, et al. Re-operation of pectus excavatum. Nihon Kyobu Geka Gakkai Zasshi. 1989;37(3):540–5.
Aronson DC, Bosgraaf RP, van der Horst C, et al. Nuss procedure: pediatric surgical solution for adults with pectus excavatum. World J Surg. 2007;31(1):26–9; discussion 30.
Castellani C, Schalamon J, Saxena AK, et al. Early complications of the Nuss procedure for pectus excavatum: a prospective study. Pediatr Surg Int. 2008;24(6):659–66.
Croitoru DP, Kelly Jr RE, Goretsky MJ, et al. Experience and modification update for the minimally invasive Nuss technique for pectus excavatum repair in 303 patients. J Pediatr Surg. 2002;37(3):437–45.
Haller Jr JA. Complications of surgery for pectus excavatum. Chest Surg Clin N Am. 2000;10(2):415–26, ix.
Fonkalsrud EW, Reemstsen B. Force required to elevate the sternum of pectus excavatum patients. J Am Coll Surg. 2002;195:575–7.
Kelly Jr RE, Shamberger RC, Mellins RB, et al. Prospective multicenter study of surgical correction of pectus excavatum: design, perioperative complications, pain, and baseline pulmonary function facilitated by internet-based data collection. J Am Coll Surg. 2007;205(2):205–16.
Leonhardt J, Kubler JF, Feiter J, et al. Complications of the minimally invasive repair of pectus excavatum. J Pediatr Surg. 2005;40(11):e7–9.
Nuss D. Minimally invasive surgical repair of pectus excavatum. Semin Pediatr Surg. 2008;17(3):209–17.
Nuss D, Croitoru DP, Kelly Jr RE, et al. Review and discussion of the complications of minimally invasive pectus excavatum repair. Eur J Pediatr Surg. 2002;12(4):230–4.
Park HJ, Chung WJ, Lee IS, et al. Mechanism of bar displacement and corresponding bar fixation techniques in minimally invasive repair of pectus excavatum. J Pediatr Surg. 2008;43(1):74–8.
Park HJ, Kim KS, Lee S, et al. A next-generation pectus excavatum repair technique: new devices make a difference. Ann Thorac Surg. 2015;99:455–61.
Arn PH, Scherer LR, Haller Jr JA, et al. Outcome of pectus excavatum in patients with Marfan syndrome and in the general population. J Pediatr. 1989;115(6):954–8.
Vegunta RK, Pacheco PE, Wallace LJ, et al. Complications associated with the Nuss procedure: continued evolution of the learning curve. Am J Surg. 2008;195(3):313–6; discussion 316–7.
Liu JF, Zhu SH, Xu B. Early results of 18 adults, following a modified Nuss operation for recurrent pectus excavatum. Eur J Cardiothorac Surg. 2013;43(2):279–82.
Jaroszewski DE, Notrica DM, McMahon LE, et al. Operative management of acquired thoracic dystrophy in adults after open pectus excavatum repair. Ann Thorac Surg. 2014;97(5):1764–70.
Jaroszewski D, Johnson K, Lackey J, et al. Complex repair of pectus excavatum recurrence and massive chest wall defect and lung herniation after prior open repair. Ann Thorac Surg. 2013;96(2):e29–31.
Schulz-Drost S, Syed J, Besendoerfer M, et al. Elastic stable chest repair as a means of stabilizing the anterior chest wall in recurrent pectus excavatum with sternocostal pseudarthrosis: an innovative fixation device. Thorac Cardiovasc Surg. 2015;63:419–26.
Haller Jr JA, Colombani PM, Humphries CT, et al. Chest wall constriction after too extensive and too early operations for pectus excavatum. Ann Thorac Surg. 1996;61(6):1618–24; discussion 1625.
Prabhakaran K, Paidas CN, Haller JA, et al. Management of a floating sternum after repair of pectus excavatum. J Pediatr Surg. 2001;36(1):159–64.
Pasrija C, Wehman B, Singh DP, et al. Recurrent pectus excavatum repair via Ravitch technique with rib locking plates. Eplasty. 2014;14:ic46.
Cheng YL, Lee SC, Huang TW, et al. Efficacy and safety of modified bilateral thoracoscopy-assisted Nuss procedure in adult patients with pectus excavatum. Eur J Cardiothorac Surg. 2008;34(5):1057–61.
Coln D, Gunning T, Ramsay M, et al. Early experience with the Nuss minimally invasive correction of pectus excavatum in adults. World J Surg. 2002;26(10):1217–21.
Hebra A, Jacobs JP, Feliz A, et al. Minimally invasive repair of pectus excavatum in adult patients. Am Surg. 2006;72(9):837–42.
Jaroszewski DE, Fonkalsrud EW. Repair of pectus chest deformities in 320 adult patients: 21 year experience. Ann Thorac Surg. 2007;84(2):429–33.
Johnson WR, Fedor D, Singhal S. Systematic review of surgical treatment techniques for adult and pediatric patients with pectus excavatum. J Cardiothorac Surg. 2014;9:25.
Park HJ, Sung SW, Park JK, et al. How early can we repair pectus excavatum: the earlier the better? Eur J Cardiothorac Surg. 2012;42(4):667–72.
Pilegaard HK, Licht PB. Routine use of minimally invasive surgery for pectus excavatum in adults. Ann Thorac Surg. 2008;86(3):952–6.
Ravenni G, Actis Dato GM, Zingarelli E, et al. Nuss procedure in adult pectus excavatum: a simple artifice to reduce sternal tension. Interact Cardiovasc Thorac Surg. 2013;17(1):23–5.
Schalamon J, Pokall S, Windhaber J, et al. Minimally invasive correction of pectus excavatum in adult patients. J Thorac Cardiovasc Surg. 2006;132(3):524–9.
Teh SH, Hanna AM, Pham TH, et al. Minimally invasive repair for pectus excavatum in adults. Ann Thorac Surg. 2008;85(6):1914–8.
Yoon YS, Kim HK, Choi YS, et al. A modified Nuss procedure for late adolescent and adult pectus excavatum. World J Surg. 2010;34(7):1475–80.
Wang L, Zhong H, Zhang FX, et al. Minimally invasive Nuss technique allows for repair of recurrent pectus excavatum following the Ravitch procedure: report of 12 cases. Surg Today. 2011;41(8):1156–60.
Hebra A, Swoveland B, Egbert M, et al. Outcome analysis of minimally invasive repair of pectus excavatum: review of 251 cases. J Pediatr Surg. 2000;35(2):252–7; discussion 257–8.
Huang PM, Wu ET, Tseng YT, et al. Modified Nuss operation for pectus excavatum: design for decreasing cardiopulmonary complications. Thorac Cardiovasc Surg. 2006;54(2):134–7.
Moss RL, Albanese CT, Reynolds M. Major complications after minimally invasive repair of pectus excavatum: case reports. J Pediatr Surg. 2001;36(1):155–8.
Nuss D, Kelly Jr RE, Croitoru DP, et al. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg. 1998;33(4):545–52.
Park HJ. Technical innovations in the minimally invasive approach for treating pectus excavatum: a paradigm shift through six years’ experience with 630 patients. Innovations (Phila). 2007;2(1):25–8.
Jaroszewski DE, Johnson K, McMahon L, et al. Sternal elevation before passing bars: a technique for improving visualization and facilitating minimally invasive pectus excavatum repair in adult patients. J Thorac Cardiovasc Surg. 2014;147(3):1093–5.
Weber PG, Huemmer HP, Reingruber B. Forces to be overcome in correction of pectus excavatum. J Thorac Cardiovasc Surg. 2006;132(6):1369–73.
Park HJ, Jeong JY, Jo WM, et al. Minimally invasive repair of pectus excavatum: a novel morphology-tailored, patient-specific approach. J Thorac Cardiovasc Surg. 2010;139(2):379–86.
Nagasao T, Miyamoto J, Tamaki T, et al. Stress distribution on the thorax after the Nuss procedure for pectus excavatum results in different patterns between adult and child patients. J Thorac Cardiovasc Surg. 2007;134(6):1502–7.
Pilegaard HK, Licht PB. Early results following the Nuss operation for pectus excavatum--a single-institution experience of 383 patients. Interact Cardiovasc Thorac Surg. 2008;7(1):54–7.
Papandria D, Arlikar J, Sacco Casamassima MG, et al. Increasing age at time of pectus excavatum repair in children: emerging consensus? J Pediatr Surg. 2013;48(1):191–6.
Olbrecht VA, Arnold MA, Nabaweesi R, et al. Lorenz bar repair of pectus excavatum in the adult population: should it be done? Ann Thorac Surg. 2008;86(2):402–8; discussion 408–9.
Pilegaard HK. Extending the use of Nuss procedure in patients older than 30 years. Eur J Cardiothorac Surg. 2011;40(2):334–7.
Lodge AJ, Wells WJ, Backer CL, et al. A novel bioresorbable film reduces postoperative adhesions after infant cardiac surgery. Ann Thorac Surg. 2008;86(2):614–21.
Pison CJ, Gonzalez AG, Perez MA, et al. Correction of recurrent pectus excavatum post-Ravitch with the Nuss technique. Cir Pediatr. 2009;22(2):77–80.
Ravitch MM. The operative treatment of pectus excavatum. Ann Surg. 1949;129(4):429–44.
Ravitch MM. New trends in pediatric surgery; pectus excavatum, esophageal atresia, intussusception, Hirschsprung’s disease. Surg Clin North Am. 1949;29(4):1535–50.
Fonkalsrud EW, Anselmo DM. Less extensive techniques for repair of pectus carinatum: the undertreated chest deformity. J Am Coll Surg. 2004;198(6):898–905.
Davis JT, Weinstein S. Repair of the pectus deformity: results of the Ravitch approach in the current era. Ann Thorac Surg. 2004;78(2):421–6.
Robicsek F, Watts LT, Fokin AA. Surgical repair of pectus excavatum and carinatum. Semin Thorac Cardiovasc Surg. 2009;21(1):64–75.
Chang PY, Lai JY, Chen JC, et al. Quantitative evaluation of bone and cartilage changes after the Ravitch thoracoplasty by multislice computed tomography with 3-dimensional reconstruction. J Thorac Cardiovasc Surg. 2007;134(5):1279–83.
Renz J, Reyes C. Repair of a floating sternum with autologous rib grafts and polylactide bioabsorbable struts in an 18-year-old male. J Pediatr Surg. 2012;47(12):e27–30.
Johnson WR, Fedor D, Singhal S. A novel approach to eliminate cardiac perforation in the nuss procedure. Ann Thorac Surg. 2013;95(3):1109–11.
Takagi S, Oyama T, Tomokazu N, et al. A new sternum elevator reduces severe complications during minimally invasive repair of the pectus excavatum. Pediatr Surg Int. 2012;28(6):623–6.
Belcher E, Arora S, Samancilar O, et al. Reducing cardiac injury during minimally invasive repair of pectus excavatum. Eur J Cardiothorac Surg. 2008;33(5):931–3.
Colombani PM. Preoperative assessment of chest wall deformities. Semin Thorac Cardiovasc Surg. 2009;21(1):58–63.
Kelly Jr RE. Pectus excavatum: historical background, clinical picture, preoperative evaluation and criteria for operation. Semin Pediatr Surg. 2008;17(3):181–93.
Kragten HA, Siebenga J, Hoppener PF, et al. Symptomatic pectus excavatum in seniors (SPES): a cardiovascular problem? : A prospective cardiological study of 42 senior patients with a symptomatic pectus excavatum. Neth Heart J. 2011;19(2):73–8.
Krasopoulos G, Dusmet M, Ladas G, et al. Nuss procedure improves the quality of life in young male adults with pectus excavatum deformity. Eur J Cardiothorac Surg. 2006;29(1):1–5.
Lester CW. The surgical treatment of funnel chest. Ann Surg. 1946;123(6):1003–22.
Maagaard M, Tang M, Ringgaard S, et al. Normalized cardiopulmonary exercise function in patients with pectus excavatum three years after operation. Ann Thorac Surg. 2013;96(1):272–8.
Swanson JW, Avansino JR, Phillips GS, et al. Correlating Haller Index and cardiopulmonary disease in pectus excavatum. Am J Surg. 2012;203(5):660–4.
Jaroszewski D, Notrica D, McMahon L, et al. Current management of pectus excavatum: a review and update of therapy and treatment recommendations. J Am Board Fam Med. 2010;23(2):230–9.
Coln E, Carrasco J, Coln D. Demonstrating relief of cardiac compression with the Nuss minimally invasive repair for pectus excavatum. J Pediatr Surg. 2006;41(4):683–6; discussion 683–6.
Goretsky MJ, Kelly Jr RE, Croitoru D, et al. Chest wall anomalies: pectus excavatum and pectus carinatum. Adolesc Med Clin. 2004;15(3):455–71.
Haller Jr JA, Kramer SS, Lietman SA. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg. 1987;22(10):904–6.
Gahrton G. ECG changes in pectus excavatum (funnel chest). A pre- and postoperative study. Acta Med Scand. 1961;170:431–8.
Krueger T, Chassot PG, Christodoulou M, et al. Cardiac function assessed by transesophageal echocardiography during pectus excavatum repair. Ann Thorac Surg. 2010;89(1):240–3.
Maagaard M, Udholm S, Hjortdal VE, et al. Right ventricular outflow tract obstruction caused by a displaced pectus bar 30 months following the Nuss procedure. Eur J Cardiothorac Surg. 2015;47:e42–3.
Malek MH, Berger DE, Housh TJ, et al. Cardiovascular function following surgical repair of pectus excavatum: a metaanalysis. Chest. 2006;130(2):506–16.
Malek MH, Coburn JW. Strategies for cardiopulmonary exercise testing of pectus excavatum patients. Clinics (Sao Paulo). 2008;63(2):245–54.
Neviere R, Wurtz A. Longer term effects of closed repair of pectus excavatum on cardiopulmonary status. J Pediatr Surg. 2013;48(9):1988–9.
Tang M, Nielsen HH, Lesbo M, et al. Improved cardiopulmonary exercise function after modified Nuss operation for pectus excavatum. Eur J Cardiothorac Surg. 2012;41(5):1063–7.
McMahon LE, Johnson KN, Jaroszewski DE, et al. Experience with FiberWire for pectus bar attachment. J Pediatr Surg. 2014;49(8):1259–63.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Jaroszewski, D.E., Johnson, K.J. (2016). Revision of Prior Failed/Recurrent Pectus Excavatum Surgery. In: Kolvekar, S., Pilegaard, H. (eds) Chest Wall Deformities and Corrective Procedures. Springer, Cham. https://doi.org/10.1007/978-3-319-23968-2_15
Download citation
DOI: https://doi.org/10.1007/978-3-319-23968-2_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23966-8
Online ISBN: 978-3-319-23968-2
eBook Packages: MedicineMedicine (R0)