
Abstract
Lead is the most potent and persistent toxic metal found naturally in the earth’s crust. Humans are exposed to lead particles through inhalation, ingestion, or skin contact, through several sources that influence food, drinking water, soil, and air. If this heavy metal enters the body, interferes with the organ systems. US Centers for Disease Control and Prevention (CDC) recently declared that no level of lead can be considered “safe”. The outcomes associated with lead exposure have become more apparent and are an ever-increasing concern across the globe, as a plethora of disorders are caused by its contact. Not only adults but young children and fetuses are also vulnerable to its toxic effects leading to neurodevelopment and kidney-related disorders. This chapter provides insight into the clinical manifestation of lead exposure especially the impact on the mental health (neurodevelopment) of the fetus, children, and adults, the mechanism of lead-induced neurotoxicity, available biomarkers, challenges, mitigation, preventive measures, and therapy for lead exposure. Future recommendations to undertake necessary steps to protect the population from environmental toxicity have also conversed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Lead (Pb) is the most potent and persistent toxic metal naturally occurring element in the earth’s crust. Lead in the environment in present its inorganic form. A level of 0.016 mg/dl of blood lead levels has been observed in pre-industrial humans, indicating the minimum contribution of natural sources for adding lead to the environment (Ezzati et al. 2004). Most lead exposure occurs through anthropogenic activities. Known sources of lead exposure are cigarette smoke, combustion exhaust, sewage sludge, fertilizers, mining, Pb-bearing sulfide deposits, Pb additives in petrol, Pb water pipes, Pb in paints, toys, etc. (Meyer et al. 2008). These sources influence food, drinking water, soil, and air. Drinking water is the major pathway of accumulation of Pb in humans which arises mostly due to the use of lead piping, which is still being used in some places (Neeti and Prakash 2013). Other sources of the increased level of Pb in water are landfills, electroplating, Au–Ag-Pb–Zn mining, etc. (Obeng-Gyasi 2019b). Lead exposure has also been associated positively with socio-economic status and smoking (Remy et al. 2019). Humans are exposed to lead particles through inhalation, ingestion, or via skin contact. Human fetuses are exposed to lead through the placenta (Iwai-Shimada et al. 2019; Rísová 2019; Singh et al. 2020). Ingested inorganic Pb is mainly excreted through urine or feces. It has been observed that children have a higher tendency of lead exposure than adults, which can be explained on a body weight basis (Carrington et al. 2019).
In adult blood, more than 90% of lead is absorbed by the erythrocytes with a half-life ranging from 28 to 36 days. However, some lead from the serum enters the soft tissues and is accumulated in the brain, kidney, liver, muscles, bones, and teeth over some time. In addition, as the age increases, the reserved pool of lead in the bones during calcium deficiency, pregnancy, or menopause is released back into the blood. This acts as an endogenous source of lead poisoning to various organs and is a major risk (ATSDR 2010; Klotz and Göen 2017; Organization 2019).
Lead, being a heavy metal, interferes with the organ systems of the body (Mansouri et al. 2020). Nowadays, it is very uncommon to find acute cases of lead toxicity which usually occurs through occupational exposure or accidental exposure to lead-containing agents. However, chronic cases of lead poisoning have been seen, as determined by elevated levels of blood lead concentration. The six countries Algeria, Yemen, Myanmar, North Korea, Iraq, and Afghanistan pose a higher risk of exposure because these countries did not follow the international standard of low-lead levels in the gasoline till 2013 (Cassleman et al. 2020). However, the developed nations took the initiative and banned the lead-containing gasoline and paint which drastically decreased chronic lead exposure but, low-level exposure remains a matter of concern (Flora et al. 2012).
Neurotoxicants may be defined as any substance or chemical that alters the regular operation and/or compromise adaptability in the central and/or peripheral nervous system, either during development or at maturity (Cardenas-Iniguez et al. 2022). Approximately, 200 substances can fall under neurotoxicants.
In the last two decades, lead neurotoxicity has been well recognized. Previous norms related to safe levels of lead was restricted to blood lead level < 10ug/dL, however, more recently, the US Centers for Disease Control and Prevention (CDC) updated and recommended that no level of lead can be considered “safe” (Bellinger 2018; Betts 2012). In the recent estimation of the global disease burden, lead has been ranked 17th to 30th most important contributor to the disability-adjusted life years (DALY) (Lim et al. 2012). The outcomes associated with lead exposure have become more apparent and are an ever-increasing concern across the globe. Not only adults but also young children are vulnerable to its toxic effects leading to neurodevelopment and kidney-related disorders (Murata et al. 2009). A plethora of disorders are caused by lead exposure. The adverse effects include behavioral alterations in children and neuronal developmental disorders in infants, a deficit in motor coordination, and cardiovascular disorders. In addition, its chronic exposure reduces fertility and causes renal dysfunction, convulsion, or even coma (Lustberg and Silbergeld 2002; Weaver et al. 2005).
A report by WHO (2004) states that in the year 2000, ~ 120 million people had blood lead levels between 5 and 10 mg/dl and nearly the same number had values > 10 mg/dl. This report further revealed that 90% of these children belong to underdeveloped countries. 40% of these children had blood lead concentrations of > 5 mg/dl and 50% had blood lead concentrations of > 10 mg/dl (Ezzati et al. 2004). A shocking figure of 9.8 million disability-adjusted life years (DALYs) was caused by the disease burden from mild mental retardation associated with lead exposure (Ezzati et al. 2004). Furthermore, the report of the Global Burden of disease dataset 2019 confirmed that ~ 800 million children have hazardous levels of lead in their bodies. The majority of the cases belong to Southeast Asia and India is the highest contributor to it. In India, nearly 275 million children are reported with raised lead levels and out of total deaths due to lead poisoning, 26% of deaths are reported in India GBD Compare (Metrics IFH Evaluation 2017).
This chapter provides insight into clinical manifestation of lead exposure especially the impact on the mental health (neurodevelopment) of the fetus, children, and adults, the mechanism of lead-induced neurotoxicity, available biomarkers, challenges, mitigation, preventive measures, and therapy for lead exposure. There is a need to undertake necessary steps to protect the population from environmental toxicity, future recommendations for the same have been discussed in the concluding part of the chapter.
2 Material and Methodology
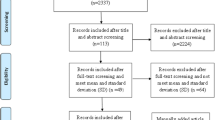
This review paper includes a systematic search in Google scholar, PubMed, and MEDLINE. The search was conducted using different keyword strings as ((“Lead exposure” OR “Lead toxicity” OR “Lead effects”) AND “Mental health”) on Google Scholar, and ((“Lead exposure” OR “Lead toxicity” OR “Lead effects”) AND (“Human brain” OR “cognitive” OR “Behavioral problems”)) on PubMed and Medline. The keywords were searched in the title and abstracts of the research papers. No criteria was set to select population-based studies. The screening of literature was done from 2013 to 2023. The search was confined to English language and included data on humans only. Besides the database search, a manual search including the reference lists of original articles and previous reviews was also performed. The studies based on association or effects of lead exposure, toxicity on humans were included for the present paper (Fig. 4.1 PRISMA flow diagram). Out of these, only those studies which complied with the inclusion criteria were included. Blogs, private websites, and newspaper articles were excluded. A total of 29 studies were screened for the review.

Source Page et al. (2021)
PRISMA flow chart illustrating the selection process of the included studies.
3 Lead and Mental Health
Environmental and occupational lead exposure is a serious public health concern. The individuals at high exposure are prone to encephalopathy, anemia, and kidney damage. Even the lower doses of exposure can alter the cognitive development in children as well as in adults (Fenga et al. 2016). It is well documented that blood lead levels are inversely associated with neuropsychological development. It can also affect the mental conditions like anger, mood, general distress, schizophrenia, and violence (Cassleman et al. 2020). Because of its health risks even at low exposure, it has been suggested that there is no safe level of lead exposure.
3.1 Effects on the Fetus
Human embryonic and fetal growth are the foundation for healthiness and illness across the lifespan. The exposure of fetus to lead can have a deep impact on its growth, as it can cross the placental barrier and accrues in the tissues of the developing fetus (Gundacker and Hengstschläger 2012). BPb level of 10–15 μg/dL in the women of reproduction age affects the growing fetus. The exposure events of lead happening before the child birth are correlated to various long-term health and behavioral issues (Brubaker et al. 2009; Canfield et al. 2005; Cecil et al. 2011). It is assumed that intrauterine contact to lead disrupts the development of brain networks before birth. Interrupted connectivity in utero may lead to reduction in the integrity of network structure, which in turn may result in cognitive deficits linked with neurotoxic insults from lead exposure. The fetus exposed to lead deviate from characteristic patterns of neurodevelopment as per fetal resting-state functional connectivity (RSFC) MRI study. The relatively lesser age-linked rise in cross-hemispheric connections and increased connectivity of the superior frontal gyrus and the posterior cingulate cortex has been reported in prenatal lead-exposed fetuses (Thomason et al. 2019).
3.2 Cognitive and Behavioral Effects in Children
There are numerous studies citing the potency of lead to affect the cognition and behavior of children. Moreover, different blood lead levels show different types of cognitive and behavioral problems. Earlier it was known that blood lead levels at 10 μg/dL and above can cause cognitive and behavioral problems among children. Blood concentrations at or below 10 g/dL resulted in neurophysiological and neurobehavioral deficits. It may have an impact on academic performance (Liu et al. 2013) distractibility, memory problems, decreased verbal and quantitative scores, impaired visual-motor coordination, and longer reaction times (Bellinger 2008; Canfield et al. 2003a, b; 2004; 2005; Chiodo et al. 2004; Dietrich et al. 1993; Lanphear et al. 2005; Rocha and Trujillo 2019). However, recent studies found concrete evidence of significant damage to the brain at levels below 5 μg/dL. Studies conducted by various researchers (Canfield et al. 2003a, b; Chiodo et al. 2004; Lanphear et al. 2005) showed that children with blood lead levels of below 5 μg/dL are linked to impulsivity, deficiencies in verbal processing, non-verbal thinking, reading, and arithmetic, reaction time, attention, as well as low scores on a variety of achievement tests. Simple reaction time, teacher report cards, and neuropsychological tests have all shown that children's attention is interrupted at levels below 3 g/dL (Chiodo et al. 2004; Després et al. 2005; Min et al. 2009). Moreover, it has been proved that continuous low-level lead exposure leads to cognitive and psychological impairment instead high-level exposure results in seizures, commas, and death.
Generally, lead toxicity is asymptomatic in children. However, children below the age of 5 years may show symptoms like poor appetite, lethargy, weight loss, abdominal pain, vomiting, constipation, headache, irritability, tiredness, and nervousness (Collin et al. 2022). Anemia is one of the symptoms of lead toxicity and thus, the pale color (a result of anemia) of children may signify lead exposure. Children who have been exposed to lead may also have learning issues. Lead encephalopathy exhibits symptoms like seizures, vomiting, clumsiness, agitation, etc. The symptomatic cases of lead poisoning must be treated immediately.
Table 4.1 illustrating the few works conducted on infants and children for showing a positive association of lead exposure and mental health. It is well documented that different biomarkers including blood, urine, bone can successfully estimate the lead exposure in children. However, most of the studies used blood (venous, umbilical) as a choice of biomarker. It is clear from the table that blood lead levels even at 2.9 μg/L can affect the mental health of children. Rodríguez-Carrillo et al. (2022) did not find any association between urine lead concentration (median: 0.42 μg/L) and behavioral functions (Rodríguez-Carrillo et al. 2022).
3.3 Lead Exposure and Mental Health in Adults
Around the globe, usage of leaded gasoline was at its peak from 1940 to the early 1900s. Therefore, it is expected that millions of adults must have lead exposure during their childhood phase. Adult lead poisoning in adults is usually brought on by the usage of traditional medicine and occupational exposure (Kumar 2009). There is an agreement that children exposed to lead suffer from low IQ levels, inattention, hyperactivity, and tend to indulge in violence, antisocial behavior, etc., but research focused on neurobehavioral functioning in adults gives mixed opinions. However, most of the studies found a positive association between lead exposure and psychiatric problems in adults (Cassleman et al. 2020). Occupational exposure to lead can affect general intellectual performance, processing, attention, visuospatial abilities, and motor functions (Fenga et al. 2016).
Lead encephalopathy is rarely seen in adults but individuals using traditional medicines or having occupational exposure to lead may suffer from it (Kumar 2009). Generally, high level of lead exposure (occupational) in adults shows symptoms like limb and abdominal pain, headache, numbness, tingling in hands and feet, memory loss, and mood swings. Abnormal and low sperm count can be a reason for lead exposure in men. Women exposed to lead during pregnancy may experience miscarriage or deliver a premature baby. Sustained low-level exposure leads to anemia. Adults exposed to lead may show aggression (more than normal), hyperactivity, and insomnia. Delirium, coma, seizures, numbness, and motor deficits are some other symptoms.
Table 4.2 describes that individuals having blood lead levels even at a level of 0.6 μg/L can show symptoms of ill mental health in adults. Bone is also used as a biomarker for the estimation of long-term exposure of lead in adults. The adults having elevated levels of lead may experience psychiatric problems including anxiety, fatigue. They may suffer from Alzheimer’s disease schizophrenia and Parkinson’s disease.
4 Mechanism of Lead-Induced Neurotoxicity
Of all the organ affected, lead accumulation primarily affects the brain and elicits excito-toxicity of the brain, the release of various neurotransmitters, the second messenger system, as well as apoptosis. One of the major effects is its function to substitute for calcium which results in mitochondrial dysfunction and apoptosis cascade leading to neuronal death. Mitochondrial dysfunction results in increased reactive oxygen species and activation of programmed cell death (Simons 1986). Since various enzymes such as acetylcholine, dopamine, and neurotransmitters are dependent on calcium signaling, the substitution with lead alters their activity (Goldstein 1993). In addition, lead delays the differentiation of glial progenitors that can cause demyelination and hypomyelination. Indirectly, lead also dysregulates chemosynthesis with increased production of aminolevulinic acid (ALA) further inhibiting the gamma aminobutyric acid receptors (GABA). As a result of this cascade, anemia occurs along with a deficit in neurocognitive ability. These symptoms might appear immediately or may be delayed with common symptoms including reduced intellectual ability, vision loss, and behavioral issues (Hwang 2007; Lidsky and Schneider 2006).
4.1 Effects of Lead on Neurodevelopment
The brain is extremely sensitive to Pb during the developmental period and especially during the gestational period which is marked by neuronal proliferation, migration, and differentiation. Lead exposure adversely affects the developing brain even at minute levels (Bellinger 2008; Liu et al. 2014). During early development, hippocampal-dependent spatial learning and memory are affected as lead exposure alters the NR1 and NR2 subunits and signaling of N-methyl-D-aspartate (NMDA) receptors (Guilarte and McGlothan 1998). Additionally, Pb exposure alters brain-derived neurotrophic factors (BDNF) (Neal et al. 2010) as well as impairs hippocampal LTP via epigenetic modulation through DNA methyltransferases and methyl cytosine binding proteins (Schneider et al. 2013). From the animal studies on neonatal rats, it is clear that alterations of long-term potentiation (LTP) and paired-pulse facilitation (PPF) of hippocampal dentate gyrus occurred (Ruan et al. 1998). This hippocampal long-term potentiation is an important component of learning as well as memory. With lead exposure, the dendritic spines, the crucial structure of pyramidal neurons are severely affected. Such changes can cause a reduction or loss of learning and memory function. Any deviation in synaptic formation, maturation, or structural alterations is detrimental to the development of the brain. Post-synaptic neuroligins (NLGNs) are integral proteins that are required for synaptogenesis, dendritic spine maturation, and its stability. Upon lead exposure, NLGN proteins are disrupted and causes altered dendritic spine formation in hippocampus (Zhao et al. 2018). In addition, exposure to lead might result in abnormal alteration of the synaptic transmission that is often associated with memory impairment. This was predicted from a study, where it was observed that PB-exposed rats had decreased expression of NR2A and phosphorylated GluR1 causing synoptical morphological and functional alterations in the hippocampal CA1 pyramidal neurons that ultimately leads to behavioral changes (Wang et al. 2016). From previous studies, it has already been established that children with the blood lead concentration of 10 µg/dL are also susceptible to intellectual impairment exhibiting low intelligent quotient. Accordingly, each increase of 10 µg per deciliter in the blood results in a significant decline in the IQ by 4.6 points which is considered to be a tremendous decline (Canfield et al. 2003a, 2003b; Heidari et al. 2022; Lanphear et al. 2005). During fetal development, lead can cross the placental membrane. In an assessment of prenatal exposure to lead, it has been observed that levels of lead in the cord blood were 1.23 μg/dl indicating that during development, lead can effortlessly pass the placental barrier and accrue in the blood of the fetus (Jedrychowski et al. 2009; Vigeh et al. 2014). A study observed that levels of lead in the first-trimester maternal plasma and whole blood can be a predictor of neurodevelopmental disorders in the early stage of life (Hu et al. 2006). Interestingly, epigenetic modifications such as DNA methylation are known to play a part in hampered neurodevelopment. This was estimated by a study wherein trimester-specific maternal blood lead concentrations, DNA methylations in umbilical cord blood, and infant neurodevelopmental outcomes were measured (Rygiel et al. 2021).
Moreover, exposure to Pb makes modification in nitric oxide synthase which alters the brain vasculature, consequently affecting the serotonergic system and may intensify aggressive behavior (Martínez-Lazcano et al. 2018). So, the neurobehavioral dysfunctions and deficits in cognition can be linked to environmental Pb exposure (Santa Maria et al. 2019).
5 Available Biomarkers of Lead Exposure
Biological monitoring measures are important for the evaluation of the toxicological agents that might be detrimental to human health and the environment (Berlin et al. 1982). Biomarker monitors and measures the interaction with the biological system and the physical, chemical, or biological agents. Biomarkers give an index of the contamination of the biological system and identify the risk factors associated with it. A variety of biomarkers exists to determine the toxicity of an element such as biological fluids like blood, and urine, and biological tissues such as hair, bone, and nail are being tested for lead exposure. Despite this, the difficulty in assessment exists due to the complex toxico-kinetics of lead within the tissue. Blood is the most common biomarker to assess the levels of ingested/inhaled lead. In humans, more than 50% of lead is transferred to the bloodstream upon exposure (DeSilva 1981). Other biomarkers include bone, teeth, hair, and nail (Barbosa et al. 2005). Bone lead levels have been correlated with serum lead levels in adults that confers its use as a potential biomarker (Hernández-Avila et al. 1998; Hu et al. 1998). Hair is an attractive biomarker for monitoring lead exposure, as it is readily available and obtained via non-invasive procedures and is of low cost (Schuhmacher et al. 1991). Nails have been also used for the detection of chronic exposure of lead due to its several advantages. Lead in nail is considered to remain uneffected from the metabolic activities of the body and reflects the long-term exposure of lead. In this regard, toenails are considered to be superior than fingernails because toenail remains less exposed to the other environmental contaminations (Nowak and Chmielnicka 2000; Takagi et al. 1988).
6 Treatment to Reduce Lead Levels in Human Body
The most effective treatment available to quickly reduce the blood lead level is chelation therapy (Collin et al. 2022). In 1950, the early chelating agent, EDTA, was fetched into clinical use as an antidote for lead toxicity. In chelation therapy, which is a clinical intervention, chelating agents like calcium disodium ethylene diamine tetraacetic acid (CaNa 2 EDTA), Succimer (2,3 meso-dimercaptosuccinic acid or DMSA, oral chelating agent, for mild and asymptomatic cases), are administered, which in turn binds to Pb and removes it from the different tissues of the body (Hao et al. 2013). DMSA being an antioxidant significantly diminishes Pb-induced oxidative stress and apoptosis (Obeng-Gyasi 2019a). Though chelation therapy considerably removes the Pb ions from the body, however, because of the side effects of the chelating agents, their use is limited to severe cases of overexposure to heavy metals (Aaseth et al. 2015; Kushwaha et al. 2018). Another medical treatment for individuals with overt lead intoxication involves decontamination and supportive care (Kosnett et al. 2007).
7 Prevention Therapy
Lead poisoning affects many organs in adults as well as in children. The prevention of exposure to lead through the environment is the primary therapy. The most common sources of lead exposure in children and adults are air, soil, water, paint chips, candies, and toys; some of which can be easily avoided (Collin et al. 2022). Secondary prevention includes regular screening through different biomarkers. Depending upon the levels of lead found medical therapies and dietary supplements may help to lower the level of lead in the body but cannot remove it completely. The early detection of lead poisoning and monitoring of blood lead levels may avoid significant consequences. Preventing direct exposure and taking a proper diet rich in natural antioxidants, vitamins (Flavonoids), iron may prevent lead build-up in the tissues (Collin et al. 2022; Wang et al. 2021).
8 Suggestions and Recommendations
It has become increasingly evident from the previous data that even a low level of environment toxicity to lead can be significantly hazardous to young adolescents leading to various mental disorders and intellectual deficits. In addition, it is also responsible for various cancers, cardiovascular diseases, kidney disorders, and gastrointestinal problems.
-
To prevent the lead toxicity in air, policymakers need to design/ update the laws to protect the environment effectively.
-
Efforts have to be made at global levels via formation of administrative policies, promoting research in the field, and making stringent laws for monitoring pollution levels.
-
Association of lead toxicity and its effects on developing brain resulting in behavior and intellectual deficits has been clearly reported. Still, the efforts to control its exposure are inadequate both at the national and international levels. To prevent various health-related issues due to potential toxins, it is important to identify these and restrict their usage before they enter the environment.
-
Various programs could be created at government level to aware public about the health hazards to these toxins via distributing pamphlets, pasting posters in public places, and by advertisements on television and social media.
-
Also, it is important to educate people on various sources of exposure and routes of inhalation.
-
Few suggestions and recommendations for preventing environmental toxicity include
-
− Industries need to certify that that the raw material used and the final product as well as factory emissions are not environment hazardous.
-
− It is important to assess the effect of potential toxins on the developing brain by various relevant bodies including pollution control boards and agencies
-
− The prevalence of mental disorders, intelligence deficits, and learning disabilities should be recorded in a national database which needs to regularly updated.
-
-
Longitudinal studies need to be designed to study the effect of different toxins on brain at multiple exposure timings as majority of intellect issues are a cumulative effect of chemical and social exposure from fetal life to childhood. Therefore, neuroimaging at starting from the fetal period to adulthood may help to monitor the different stages of brain development and maturation, under various environmental conditions.
-
It is important to assess neuropsychological and behavioral aspects of children at early ages through standardized instruments.
9 Conclusions
Previous studies and data’s suggest that lead neurotoxicity may be a contributing factor for adverse mental health outcomes, even at levels generally considered to pose low or no risk. Thus, no blood concentration of lead is safe; its neurological and behavioral effects are thought to be irreversible. WHO has also identified lead as one of 10 chemicals of major public health concern needing immediate action by Member States to protect the health of workers, children and women. Efforts has to be made at the national and international levels to control the lead exposure. Adverse behavioral outcomes observed in children with similarly low blood lead levels emphasizes the need for considering ways to further reduce environmental lead exposures. Therefore, it is important to state the awareness and advocacy surrounding the issue of such neurotoxicant exposures in order to influence policy makers that can enact legislation to largely mitigate and eliminate these toxic environmental exposures.
References
Aaseth J, Skaug MA, Cao Y, Andersen O (2015) Chelation in metal intoxication—principles and paradigms. J Trace Elements Med Biol 31:260–266
Abd-Wahil MS, Jaafar MH, Md-Isa Z (2022) Assessment of urinary lead (Pb) and essential trace elements in autism spectrum disorder: a case-control study among preschool children in Malaysia. Biol Trace Element Res 200(1):97–121. https://doi.org/10.1007/s12011-021-02654-w
ATSDR (2010) Case studies in environmental medicine (CSEM) lead toxicity
Barbosa F, Tanus-Santos JE, Gerlach RF, Parsons PJ (2005) A critical review of biomarkers used for monitoring human exposure to lead: advantages, limitations, and future needs. Environ Health Perspect 113(12):1669–1674
Bellinger DC (2008) Very low lead exposures and children’s neurodevelopment. Curr Opin Pediat 20(2):172–177
Bellinger D (2018) Tetraethyl lead, paints, pipes, and other lead exposure routes: the impact on human health
Berlin A, Yodaiken R, Logan D (1982) International seminar on the assessment of toxic agents at the workplace roles of ambient and biological monitoring, Luxembourg, 8–12 December, 1980. Int Arch Occup Environ Health 50(2):1258
Betts KS (2012) CDC updates guidelines for children’s lead exposure. Environ Health Perspect 120(7):a268. https://doi.org/10.1289/ehp.120-a268
Brubaker CJ, Schmithorst VJ, Haynes EN, Dietrich KN, Egelhoff JC, Lindquist DM et al (2009) Altered myelination and axonal integrity in adults with childhood lead exposure: a diffusion tensor imaging study. Neurotoxicology 30(6):867–875
Canfield RL, Henderson CR Jr, Cory-Slechta DA, Cox C, Jusko TA, Lanphear BP (2003a) Intellectual impairment in children with blood lead concentrations below 10 μg per deciliter. N Engl J Med 348(16):1517–1526
Canfield RL, Kreher DA, Cornwell C, Henderson CR (2003b) Low-level lead exposure, executive functioning, and learning in early childhood. Child Neuropsychol 9(1):35–53
Canfield RL, Gendle MH, Cory-Slechta DA (2004) Impaired neuropsychological functioning in lead-exposed children. Develop Neuropsychol 26(1):513–540
Canfield R, Jusko T, Kordas K (2005) Environmental lead exposure and children’s cognitive function. Rivista Italiana Di Pediatria Ital J Pediat 31(6):293
Cardenas-Iniguez C, Burnor E, Herting MM (2022) Neurotoxicants, the developing brain, and mental health. Biol Psych Global Open Sci 2:223–232
Carrington C, Devleesschauwer B, Gibb HJ, Bolger PM (2019) Global burden of intellectual disability resulting from dietary exposure to lead, 2015. Environ Res 172:420–429
Cassleman KL, Dorrance KA, Todd AC (2020) Neuropsychiatric implications of chronic lead exposure. Milit Med 185(5–6):e914–e918
Cecil KM, Dietrich KN, Altaye M, Egelhoff JC, Lindquist DM, Brubaker CJ, Lanphear BP (2011) Proton magnetic resonance spectroscopy in adults with childhood lead exposure. Environ Health Perspect 119(3):403–408
Chiodo LM, Jacobson SW, Jacobson JL (2004) Neurodevelopmental effects of postnatal lead exposure at very low levels. Neurotoxicol Teratol 26(3):359–371
Chouhdari A, Farnaghi F, Hassanian-Moghaddam H, Zamani N, Sabeti S, Shahrabi-Farahani H (2020) Blood lead levels in opium-poisoned children: one cross-sectional study in Iran. Addict Health 12(3):159–166
Collin MS, Kumar Venkataraman S, Vijayakumar N, Kanimozhi V, Arbaaz SM, Stacey RS et al (2022) Bioaccumulation of lead (Pb) and its effects on human: a review. J Hazard Mater Adv 7:100094
Coon S, Stark A, Peterson E, Gloi A, Kortsha G, Pounds J et al (2006) Whole-body lifetime occupational lead exposure and risk of Parkinson’s disease. Environ Health Perspect 114(12):1872–1876
DeSilva P (1981) Determination of lead in plasma and studies on its relationship to lead in erythrocytes. Occup Environ Med 38(3):209–217
Després C, Beuter A, Richer F, Poitras K, Veilleux A, Ayotte P et al (2005) Neuromotor functions in Inuit preschool children exposed to Pb, PCBs, and Hg. Neurotoxicol Teratol 27(2):245–257
Dietrich KN, Berger OG, Succop PA, Hammond PB, Bornschein RL (1993) The developmental consequences of low to moderate prenatal and postnatal lead exposure: intellectual attainment in the Cincinnati Lead Study Cohort following school entry. Neurotoxicol Teratol 15(1):37–44
Ezzati M, Lopez AD, Rodgers AA, Murray CJ (2004) Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. World Health Organization, New York
Fenga C, Gangemi S, Alibrandi A, Costa C, Micali E (2016) Relationship between lead exposure and mild cognitive impairment. J Prevent Med Hyg 57(4):E205
Flora G, Gupta D, Tiwari A (2012) Toxicity of lead: a review with recent updates. Interdiscip Toxicol 5(2):47–58
Garí M, Grzesiak M, Krekora M, Kaczmarek P, Jankowska A, Król A et al (2022) Prenatal exposure to neurotoxic metals and micronutrients and neurodevelopmental outcomes in early school age children from Poland. Environ Res 204:112049. https://doi.org/10.1016/j.envres.2021.112049
Goldstein G (1993) Evidence that lead acts as a calcium substitute in second messenger metabolism. Neurotoxicology 14(2–3):97–101
Guilarte TR, McGlothan JL (1998) Hippocampal NMDA receptor mRNA undergoes subunit specific changes during developmental lead exposure. Brain Res 790(1–2):98–107
Gundacker C, Hengstschläger M (2012) The role of the placenta in fetal exposure to heavy metals. Wien Med Wochenschr 162(9–10):201–206
Hao P, Han SH, Liu HY, Chandni V, Cai XQ, Zhang YH (2013) Relationship of inflammation and endothelial dysfunction with risks to cardiovascular disease among people in Inner Mongolia of China. Biomed Environ Sci 26(10):792–800
Heidari S, Mostafaei S, Razazian N, Rajati M, Saeedi A, Rajati F (2022) The effect of lead exposure on IQ test scores in children under 12 years: a systematic review and meta-analysis of case-control studies. Syst Rev 11(1):106. https://doi.org/10.1186/s13643-022-01963-y
Hernández-Avila M, Smith D, Meneses F, Sanin LH, Hu H (1998) The influence of bone and blood lead on plasma lead levels in environmentally exposed adults. Environ Health Perspect 106(8):473–477
Hu H, Rabinowitz M, Smith D (1998) Bone lead as a biological marker in epidemiologic studies of chronic toxicity: conceptual paradigms. Environ Health Perspect 106(1):1–8
Hu H, Téllez-Rojo MM, Bellinger D, Smith D, Ettinger AS, Lamadrid-Figueroa H et al (2006) Fetal lead exposure at each stage of pregnancy as a predictor of infant mental development. Environ Health Perspect 114(11):1730–1735. https://doi.org/10.1289/ehp.9067
Hwang L (2007) Environmental stressors and violence: lead and polychlorinated biphenyls. Rev Environ Health 22(4):313–328
Ishitsuka K, Yamamoto-Hanada K, Yang L, Mezawa H, Konishi M, Saito-Abe M et al (2020) Association between blood lead exposure and mental health in pregnant women: results from the Japan environment and children’s study. Neurotoxicology 79:191–199. https://doi.org/10.1016/j.neuro.2020.06.003
Iwai-Shimada M, Kameo S, Nakai K, Yaginuma-Sakurai K, Tatsuta N, Kurokawa N et al (2019) Exposure profile of mercury, lead, cadmium, arsenic, antimony, copper, selenium and zinc in maternal blood, cord blood and placenta: the Tohoku Study of Child Development in Japan. Environ Health Prevent Med 24:1–11
Jedrychowski W, Perera FP, Jankowski J, Mrozek-Budzyn D, Mroz E, Flak E et al (2009) Very low prenatal exposure to lead and mental development of children in infancy and early childhood. Neuroepidemiology 32(4):270–278
Kadawathagedara M, Muckle G, Quénel P, Michineau L, Le Bot B, Hoen B et al (2023) Infant neurodevelopment and behavior in Guadeloupe after lead exposure and Zika maternal infection during pregnancy. Neurotoxicology 94:135–146. https://doi.org/10.1016/j.neuro.2022.11.007
Klotz K, Göen T (2017) Human biomonitoring of lead exposure. Met Ions Life Sci 17:99–121
Kosnett MJ, Wedeen RP, Rothenberg SJ, Hipkins KL, Materna BL, Schwartz BS et al (2007) Recommendations for medical management of adult lead exposure. Environ Health Perspect 115(3):463–471
Kumar A (2009) Lead loadings in household dust in Delhi, India. Indoor Air 19(5):414–420
Kushwaha A, Hans N, Kumar S, Rani R (2018) A critical review on speciation, mobilization and toxicity of lead in soil-microbe-plant system and bioremediation strategies. Ecotoxicol Environ Saf 147:1035–1045
Lanphear BP, Hornung R, Khoury J, Yolton K, Baghurst P, Bellinger DC et al (2005) Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Perspect 113(7):894–899
Lidsky T, Schneider J (2006) Adverse effects of childhood lead poisoning: the clinical neuropsychological perspective. Environ Res 100(2):284–293
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H et al (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2224–2260
Liu J, Li L, Wang Y, Yan C, Liu X (2013) Impact of low blood lead concentrations on IQ and school performance in Chinese children. PLoS ONE 8(5):e65230
Liu JA, Chen Y, Gao D, Jing J, Hu Q (2014) Prenatal and postnatal lead exposure and cognitive development of infants followed over the first three years of life: a prospective birth study in the Pearl River Delta region, China. Neurotoxicology 44:326–334
Lu A-X, Wang S-S, Xu X, Wu M-Q, Liu J-X, Xu M et al (2023) Sex-specific associations between cord blood lead and neurodevelopment in early life: the mother-child cohort (Shanghai, China). Ecotoxicol Environ Saf 249:114337. https://doi.org/10.1016/j.ecoenv.2022.114337
Lustberg M, Silbergeld E (2002) Blood lead levels and mortality. Arch Intern Med 162(21):2443–2449
Ma J, Yan L, Guo T, Yang S, Guo C, Liu Y et al (2019) Association of typical toxic heavy metals with Schizophrenia. Int J Environ Res Public Health 16(21):4200
Malavika L, Goyal T, Mitra P, Saikiran G, Sharma S, Sharma P (2022) Risk factors for lead toxicity and its effect on neurobehavior in Indian children. Indian J Clin Biochem 37(3):294–302. https://doi.org/10.1007/s12291-021-00995-w
Mansouri B, Błaszczyk M, Binkowski LJ, Sayadi MH, Azadi NA, Amirabadizadeh AR, Mehrpour O (2020) Urinary metal levels with relation to age, occupation, and smoking habits of male inhabitants of eastern Iran. Biol Trace Element Res 195(1):63–70. https://doi.org/10.1007/s12011-019-01848-7
Martínez-Lazcano JC, López-Quiroz A, Alcantar-Almaraz R, Montes S, Sánchez-Mendoza A, Alcaraz-Zubeldia M et al (2018) A hypothesis of the interaction of the nitrergic and serotonergic systems in aggressive behavior induced by exposure to lead. Front Behav Neurosci 12:202
McFarlane AC, Searle AK, Van Hooff M, Baghurst PA, Sawyer MG, Galletly C et al (2013) Prospective associations between childhood low-level lead exposure and adult mental health problems: the Port Pirie cohort study. Neurotoxicology 39:11–17
Metrics IFH Evaluation (2017) GBD compare data visualization. In: IHME. University of Washington, Seattle, WA
Meyer PA, Brown MJ, Falk H (2008) Global approach to reducing lead exposure and poisoning. Mutat Res Rev Mutat Res 659(1–2):166–175
Min MO, Singer LT, Kirchner HL, Minnes S, Short E, Hussain Z, Nelson S (2009) Cognitive development and low-level lead exposure in poly-drug exposed children. Neurotoxicol Teratol 31(4):225–231
Murata K, Iwata T, Dakeishi M, Karita K (2009) Lead toxicity: does the critical level of lead resulting in adverse effects differ between adults and children? J Occup Health 51(1):1–12
Neal AP, Stansfield KH, Worley PF, Thompson RE, Guilarte TR (2010) Lead exposure during synaptogenesis alters vesicular proteins and impairs vesicular release: potential role of NMDA receptor–dependent BDNF signaling. Toxicol Sci 116(1):249–263
Neeti K, Prakash T (2013) Effects of heavy metal poisoning during pregnancy. Int Res J Environ Sci 2(1):88–92
Nowak B, Chmielnicka J (2000) Relationship of lead and cadmium to essential elements in hair, teeth, and nails of environmentally exposed people. Ecotoxicol Environ Saf 46(3):265–274
Obeng-Gyasi E (2019a) Lead exposure and cardiovascular disease among young and middle-aged adults. Med Sci 7(11):103
Obeng-Gyasi E (2019b) Sources of lead exposure in various countries. Rev Environ Health 34(1):25–34
Organization WH (2019) Preventing disease through healthy environments: exposure to lead—a major public health concern (9240037632)
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Remy S, Hambach R, Van Sprundel M, Teughels C, Nawrot TS, Buekers J et al (2019) Intelligence gain and social cost savings attributable to environmental lead exposure reduction strategies since the year 2000 in Flanders, Belgium. Environ Health 18:1–9
Reuben A, Schaefer JD, Moffitt TE, Broadbent J, Harrington H, Houts RM et al (2019) Association of childhood lead exposure with adult personality traits and lifelong mental health. JAMA Psych 76(4):418–425. https://doi.org/10.1001/jamapsychiatry.2018.4192
Rísová V (2019) The pathway of lead through the mother’s body to the child. Interdiscip Toxicol 12(1):1–6
Rocha A, Trujillo KA (2019) Neurotoxicity of low-level lead exposure: history, mechanisms of action, and behavioral effects in humans and preclinical models. Neurotoxicology 73:58–80
Rodríguez-Carrillo A, Mustieles V, D’Cruz SC, Legoff L, Gil F, Olmedo P et al (2022) Exploring the relationship between metal exposure, BDNF, and behavior in adolescent males. Int J Hyg Environ Health 239:113877. https://doi.org/10.1016/j.ijheh.2021.113877
Roy A, Bellinger D, Hu H, Schwartz J, Ettinger AS, Wright RO et al (2009) Lead exposure and behavior among young children in Chennai, India. Environ Health Perspect 117(10):1607–1611. https://doi.org/10.1289/ehp.0900625
Ruan D-Y, Chen J-T, Zhao C, Xu Y-Z, Wang M, Zhao W-F (1998) Impairment of long-term potentiation and paired-pulse facilitation in rat hippocampal dentate gyrus following developmental lead exposure in vivo. Brain Res 806(2):196–201
Rygiel CA, Dolinoy DC, Bakulski KM, Aung MT, Perng W, Jones TR et al (2021) DNA methylation at birth potentially mediates the association between prenatal lead (Pb) exposure and infant neurodevelopmental outcomes. Environ Epigenet 7(1):5. https://doi.org/10.1093/eep/dvab005
Santa Maria MP, Hill BD, Kline J (2019) Lead (Pb) neurotoxicology and cognition. Appl Neuropsychol Child 8(3):272–293
Schneider J, Kidd S, Anderson D (2013) Influence of developmental lead exposure on expression of DNA methyltransferases and methyl cytosine-binding proteins in hippocampus. Toxicol Lett 217(1):75–81
Schuhmacher M, Domingo J, Llobet J, Corbella J (1991) Lead in children’s hair, as related to exposure in Tarragona Province, Spain. Sci Total Environ 104(3):167–173
Simons T (1986) Cellular interactions between lead and calcium. Br Med Bull 42(4):431–434
Singh L, Anand M, Singh S, Taneja A (2020) Environmental toxic metals in placenta and their effects on preterm delivery-current opinion. Drug Chem Toxicol 43(5):531–538
Takagi Y, Matsuda S, Imai S, Ohmori Y, Masuda T, Vinson J et al (1988) Survey of trace elements in human nails: an international comparison. Bull Environ Contam Toxicol 41(5):1258
Takeuchi H, Taki Y, Nouchi R, Yokoyama R, Kotozaki Y, Nakagawa S et al (2021) Lead exposure is associated with functional and microstructural changes in the healthy human brain. Commun Biol 4(1):912. https://doi.org/10.1038/s42003-021-02435-0
Thomason ME, Hect JL, Rauh VA, Trentacosta C, Wheelock MD, Eggebrecht AT et al (2019) Prenatal lead exposure impacts cross-hemispheric and long-range connectivity in the human fetal brain. Neuroimage 191:186–192
Tlotleng N, Naicker N, Mathee A, Todd AC, Nkomo P, Norris SA (2022) Association between bone lead concentration and aggression in youth from a sub-cohort of the Birth to Twenty Cohort. Int J Environ Res Public Health 19(4):2200
Vigeh M, Yokoyama K, Matsukawa T, Shinohara A, Ohtani K (2014) Low level prenatal blood lead adversely affects early childhood mental development. J Child Neurol 29(10):1305–1311
Wang T, Guan R-L, Liu M-C, Shen X-F, Chen JY, Zhao M-G, Luo W-J (2016) Lead exposure impairs hippocampus related learning and memory by altering synaptic plasticity and morphology during juvenile period. Mol Neurobiol 53:3740–3752
Wang Z, Bao J, Wang T, Moryani HT, Kang W, Zheng J et al (2021) Hazardous heavy metals accumulation and health risk assessment of different vegetable species in contaminated soils from a typical mining city, central China. Int J Environ Res Public Health 18(5):2617
Weaver VM, Jaar BG, Schwartz BS, Todd AC, Ahn K-D, Lee S-S et al (2005) Associations among lead dose biomarkers, uric acid, and renal function in Korean lead workers. Environ Health Perspect 113(1):36–42
Weisskopf MG, Weuve J, Nie H, Saint-Hilaire M-H, Sudarsky L, Simon DK et al (2010) Association of cumulative lead exposure with Parkinson’s disease. Environ Health Perspect 118(11):1609–1613
Wen Q, Verheijen M, Wittens MMJ, Czuryło J, Engelborghs S, Hauser D et al (2022) Lead-exposure associated miRNAs in humans and Alzheimer’s disease as potential biomarkers of the disease and disease processes. Sci Rep 12(1):15966. https://doi.org/10.1038/s41598-022-20305-5
Winter AS, Sampson RJ (2017) From lead exposure in early childhood to adolescent health: a chicago birth cohort. Am J Public Health 107(9):1496–1501. https://doi.org/10.2105/AJPH.2017.303903
Yıldız S, Pirinççioğlu AG, Arıca E (2023) Evaluation of heavy metal (lead, mercury, cadmium, and manganese) levels in blood, plasma, and urine of adolescents with aggressive behavior. Cureus 15(1):157
Zhao Z-H, Zheng G, Wang T, Du K-J, Han X, Luo W-J et al (2018) Low-level gestational lead exposure alters dendritic spine plasticity in the hippocampus and reduces learning and memory in rats. Sci Rep 8(1):3533. https://doi.org/10.1038/s41598-018-21521-8
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2024 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Arora, J., Singal, A., Jacob, J., Garg, S., Aeri, R. (2024). A Systematic Review of Lead Exposure on Mental Health. In: Kumar, N., Jha, A.K. (eds) Lead Toxicity Mitigation: Sustainable Nexus Approaches. Environmental Contamination Remediation and Management. Springer, Cham. https://doi.org/10.1007/978-3-031-46146-0_4
Download citation
DOI: https://doi.org/10.1007/978-3-031-46146-0_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-46145-3
Online ISBN: 978-3-031-46146-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)