
Abstract
The appearance of new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants with increased infectivity and immune escape capabilities has allowed continuation of the COVID-19 pandemic for the foreseeable future. This review describes the worldwide efforts aimed at developing new vaccination and treatment strategies to keep pace with these variants as they emerge. In the case of vaccines and monoclonal antibody-based therapeutics, we describe the development of variant-specific, multivalent, and universal coronavirus directed approaches. Existing treatment approaches consist of repurposed medicines, such as antiviral compounds and anti-inflammatory agents, although efforts are underway to develop new ways of preventing or minimizing the effects of infection with the use of small molecules that disrupt binding the SARS-CoV-2 virus to host cells. Finally, we discuss the preclinical and clinical testing of natural products from medicinal herbs and spices, which have demonstrated anti-inflammatory and antiviral properties and therefore show potential as novel and safe COVID-19 treatment approaches.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
As of June 23, 2022, 66.4% of the world population had received one or more doses of a World Health Organization (WHO)-approved COVID-19 vaccine, and over 12 billion doses have been administered in total [1]. However, the unequal distribution of vaccines has led to considerable moral outrage and could lead to epidemiological and economic disasters, as less than 20% of people in some low countries have received only one dose [2]. To compound the problem, the existing vaccines created to combat the original severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) strain which originated in Wuhan, China, may not work as effectively, if at all, against some of the newer SARS-CoV-2 versions, such as the Omicron subvariants [3]. Despite the devastating effects the COVID-19 pandemic has had on our world, the imbalance in vaccination has still not been corrected, and there is still a significant proportion of the population in many countries and territories that show vaccine hesitancy [4]. Thus, more studies are needed to understand and effectively correct this nonacceptance trend, which may threaten further efforts aimed at controlling the ongoing pandemic. Addressing the problem of how vaccines keep pace with new variants may be an even more difficult prospect. In terms of keeping pace with the emerging variants, it is still not clear whether the best strategy is to develop vaccines against each variant as these emerge in a continuous game of catch-up, or if the construction of vaccines targeting multiple variants simultaneously is the best approach [5].
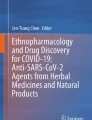
In the meantime, effective therapeutics may be needed for those individuals who are not fully protected by vaccination, or those who are immunocompromised or have a high risk of experiencing a severe COVID-19 disease outcome [6]. Various monoclonal antibodies have been developed which target the SARS-CoV-2 spike protein, and some of these have demonstrated efficacy against the virus [7]. However, as with the vaccines, many of these are only partially effective or completely inactive against some of the variants [7]. The SARS-CoV-2 Omicron variant (lineage B.1.1.529) was detected in Botswana and South Africa in November 2021, and this spreads rapidly across South Africa and most of the world within 3 months [8]. This rapid spread is likely to be due to the increased transmissibility and strong ability of this variant to escape immune detection by neutralizing antibodies [9]. The property of increased transmission of this variant has been attributed to the enhanced capability of host infection via stronger interactions with the angiotensin-converting enzyme 2 (ACE2) receptor. The immune escape characteristic is a likely consequence of the higher number of mutations compared with other SARS-CoV-2 strains, rendering Omicron less recognizable to the existing vaccines and to convalescent sera from those had been infected by earlier strains (Fig. 2.1) [10, 11].

Mutations of SARS-CoV-2 spike protein in the Omicron (B.1.1.529) BA.1 (top) and BA.2 (bottom) subvariants. The BA.1 subvariant contains 34 mutations and the BA.2 subvariant contains 31 mutations. Amino acid codes: A = alanine, D = aspartate, E = glutamate, F = phenylalanine, G = glycine, H = histadine, I = isoleucine, K = lysine, L = leucine, N = asparagine, P = proline, Q = glutamine, R = arginine, S = serine, T = threonine, V = valine, Y = tyrosine
This review describes the effects that the continuous variation in the SARS-CoV-2 genome has had on the efficacy of existing vaccines and treatments. This has created an urgent need to fine tune and advance new vaccine and drug development strategies to cope with this protein virus and to prepare for the next pandemic.
2 Current COVID-19 Vaccines
The current vaccines approved by the WHO are indicated in Table 2.1. These are based on different strategies which can be classified as mRNA (Fig. 2.2a), non-replicating viral vector (Fig. 2.2b), inactivated (Fig. 2.2c), and recombinant protein nanoparticle (Fig. 2.2d) vaccines. The first of these to be approved by the WHO on Dec 21, 2020, was originally designated BNT162b1 and produced by Pfizer/BioNTech [12]. The International Non-proprietary Name (INN) is Tozinameran, and it is now sold under the tradename Comirnaty®. This was followed by Vaxveria (Oxford/AstraZeneca) [13], Covishield (Serum Institute of India) [14], Spikevax (Moderna) [15], Covilo (Sinopharm) [16], Ad26.COV2.S (Janssen) [17], and CoronaVac (Sinovac) [18] within a 6-month time span. After this, four more vaccines were developed which were approved within the next year (Covaxin; Bharat Biotech [19], COVOVAX; Serum Institute of India [20], Nuvaxovid; Novavax [21], and Convidecia; CanSino [22]). The rapid production of the above vaccines was unprecedented considering that it normally takes at least 10 years from discovery research of a new product through the preclinical, clinical, regulatory approval, manufacturing, and delivery stages [23,24,25,26]. However, this was driven by the deadly and disruptive nature of the pandemic and made possible by the unprecedented worldwide cooperation building on existing technologies and with new streamlined approaches to research, development, approval, global manufacturing, and distribution, without sacrificing testing and safety steps [27,28,29,30,31,32].

Types of vaccines used as protection against COVID-19 disease. (a) mRNA-based vaccine (Comirnaty, SpikeVax). This type of vaccine consists of lipid nanoparticle-encapsulated mRNA molecules encoding a modified version of the SARS-CoV-2 spike protein. Once injected, this is translated by host immune cells to produce the modified spike protein molecules which stimulate an adaptive immune response. (b) Non-replicating viral vector (Vaxzevria, Covishield, Ad26.COV2.S, Convidecia). This vaccine type consists of a replication-deficient virus carrier containing the full-length DNA coding sequence of the SARS-CoV-2 spike protein which is transcribed into mRNA and then translated into proteins by the host cell to produce an immune response. (c) Inactivated vaccine (Covilo, CoronaVac, Covaxin). This type of vaccine contains the whole virus which has been inactivated either by deletion or chemical modification of the viral genetic material. (d) Recombinant spike protein nanoparticle (also known as a subunit vaccine and a virus-like particle vaccine; COVOVAX). These vaccines resemble virus particles to stimulate an immune response but contain no viral genetic material. (e) Recombinant spike protein nanoparticle containing adjuvant (Nuvaxovid). This type of vaccine is a virus-like particle containing an adjuvant to boost the host cell immune response
3 Treatments for COVID-19
The approved drugs for COVID-19 target different aspects of the SARS-CoV-2 infection cycle, for improving COVID-19 disease outcomes. These drugs include (1) monoclonal antibodies that interfere with binding of the receptor binding domain (RBD) of the SARS-CoV-2 spike protein to the ACE2 receptor (a critical step in viral entry into host cells) (Fig. 2.3a); (2) molecular compounds that minimize the damaging cytokine storm effects of viral infection (Fig. 2.3b); and (3) small molecules that prevent proteolytic activation of the SARS-CoV-2 non-structural proteins and replication of the viral RNA (Fig. 2.3c) (Table 2.2). The drugs which have been approved currently for use in either Europe, the United States, or by the World Health Organization (WHO), are indicated below in the order of approval date (earliest to most recent).

Types of drugs used for treatment of COVID-19. (a) Monoclonal antibodies against spike protein (regdanvimab, casirivimab/imdevimab, sotrovimab, tixagevimab/cilgavimab). These antibody-based treatments disrupt binding of the SARS-CoV-2 RBD to the ACE2 receptor on host cells. (b) Anti-inflammatory drugs (tocilizumab, anakinra). These drugs block interaction of key cytokines with their receptor signaling cascades and thereby inhibit the hyperactivation of pro-inflammatory factors involved in the cytokine storm effect. (c) Antiviral (remdesivir, PF-07321332/ritonavir). These drugs inhibit key stages of the viral replication cycle
3.1 Remdesivir
Remdesivir was the first antiviral drug to be authorized by the WHO as a treatment for COVID-19. In the United States, the Food and Drug Administration (FDA) approved Remdesivir for emergency use for people greater than 12 years old and heavier than 40 kg (88 lbs) [33], and it has now been approved for temporary use in more than 50 countries [34]. It was first developed in 2016 as an antivirus drug called GS-5734 by Gilead Sciences for the treatment of Ebola virus [35]. Remdesivir is a nucleotide analogue that inhibits viral RNA synthesis by stalling RNA-dependent RNA polymerase complex activity (Fig. 2.3c) [36]. Clinical trials on the use of Remdesivir to improve clinical outcomes in COVID-19 patients have shown mixed results. A meta-analysis conducted by Angamo et al. found that treatment with Remdesivir led to an increase in clinical recovery rate by 21% and 29% on days 7 and 14, respectively, and the need for supplemental oxygen or mechanical ventilation was reduced by 27% and 47%, respectively, compared to the placebo group [37]. The same study also found a 39% reduction in mortality on day 14 but with no significant difference in this outcome on day 28. One meta-analysis found that 10-day Remdesivir treatment was safe with some adverse effects in hospitalized COVID-19 patients, but there was no reduction in mortality compared to placebo [38]. A more recent meta-analysis of nine randomized controlled trials found no significant differences in mortality or use of mechanical ventilation between the Remdesivir and control groups [39]. However, the use of Remdesivir did significantly increase recovery (p = 0.004) and clinical improvement (p = 0.020) rates. Taken together, the results of these studies suggest that further work is required to determine if Remdesivir and related antiviral drugs are efficacious and safe for use in the treatment of COVID-19.
3.2 Anti-Spike Protein Monoclonal Antibodies
One of the most promising therapies in the treatment of COVID-19 disease is the use of monoclonal antibodies that target different epitopes of the spike protein RBD (Fig. 2.3a) (Table 2.2).
3.2.1 Regdanvimab
Regdanvimab (originally designated CTP59) was identified through screening a peripheral blood mononuclear cell library from a convalescent patient as a monoclonal antibody targeting the SARS-CoV-2 spike protein RBD of the viral spike protein [40]. A recent meta-analysis identified seven studies including 1350 patients in the Regdanvimab arm and 1983 patients in the control group, which showed that Regdanvimab treatment led to decreased mortality and need for supplemental oxygen and/or progression to severe disease outcomes [41]. However, this did not account for the effects of SARS-CoV-2 variants of concern on the outcomes. It was approved for use in COVID-19 patients with mild or moderate levels of illness by the European Medicines Agency in November 2021.
3.2.2 Casirivimab/Imdevimab Cocktail
Ronapreve (also known as REGN-COV2) is a neutralizing antibody cocktail consisting of Casirivimab and Imdevimab, which target distinct regions of the SARS-Cov-2 spike protein RBD [42]. Theoretically, the antibody cocktail approach may offer advantages over a single monoclonal antibody therapeutic by targeting multiple epitopes and thereby diminishing the chances of immune evasion by emerging SARS-CoV-2 variants. A study of 949 patients with mild-to-moderate COVID-19 who were admitted to hospital during the SARS-CoV-2 Delta wave (July 24 to September 30, 2021) in Fukushima Prefecture, Japan, found that those who received the Casirivimab/Imdevimab cocktail showed significantly lower deterioration of symptoms [43]. It was approved for use in COVID-19 patients with mild or moderate levels of illness by the European Medicines Agency on the same date as Regdanvimab (November 12, 2021).
3.2.3 Sotrovimab
Sotrovimab was identified initially by screening antibodies from a convalescent patient from the SARS-CoV-1 epidemic in 2003 [44]. This antibody recognizes a conserved epitope in both the SARS-CoV-1 and SARS-CoV-2 spike proteins outside the RBD. This property suggested that this epitope might forestall the mutational escape seen in different SARS-CoV-2 variants [45]. A meta-analysis on the efficacy of different SARS-CoV-2 monoclonal antibody therapies found that Sotrovimab ranked first by causing a significant decrease in the incidence of hospitalization compared to placebo, [46] and two studies showed that it retained the most activity in neutralizing the Omicron variant [47, 48]. Sotrovimab was approved for use by the European Medicines Agency on December 17, 2021 for the treatment of COVID-19 patients over 12 years old and weighing over 40 kg who do not require supplemental oxygen or who have a severe disease risk.
3.2.4 Tixagevimab/Cilgavimab Cocktail
A combination of two monoclonal antibodies, Tixagevimab (also known as AZD8895) and Cilgavimab (AZD1061), was isolated from patients who had recovered from COVID-19 disease [49]. As with the other monoclonal antibody cocktails listed above, Tixagevimab/Cilgavimab binds to non-overlapping epitopes on the spike protein RBD. A trial of 3460 participants who received one dose of this cocktail had a relative risk reduction of 82.8% compared to 1731 individuals who had received placebo [50]. It received approval for medical use for the treatment of COVID-19 in the European Union on March 15, 2022. However, as with the other monoclonal antibody therapeutics, this combination treatment showed a significant reduction in efficacy against the Omicron BA.1 and BA.2 SARS-CoV-2 variants [46, 48]. This calls to attention the need for new monoclonal antibody therapeutics which target the various Omicron subvariants more effectively.
3.3 Tocilizumab
As the levels of the proinflammatory cytokine interleukin-6 (IL-6) have been found to positively correlate with COVID-19, disease severity and death outcomes drugs which counteract IL-6 signaling might play a role in mitigating these effects [51, 52]. Tocilizumab is a monoclonal antibody that acts as an IL-6 receptor antagonist and has been approved for the treatment of rheumatoid arthritis, cytokine release syndrome, and other disorders marked by hyper-inflammation (Fig. 2.3b and Table 2.2) [53]. In a meta-analysis carried out by Maraolo et al., Tocilizumab was associated with higher survival in severe COVID-19 disease patients (odds ratio [OR]: 0.83, 95% confidence interval [CI]: 0.74–0.93), although a larger study size accounting for different dosage regimes will be required to confirm this [54]. Zhang et al. carried out a meta-analysis of 11 studies consisting of 3406 and 3173 patients assigned to the Tocilizumab and control groups, respectively [55]. They found that the Tocilizumab group had showed significant reductions in the following: 1) the 28–30-day mortality risk, 2) need for mechanical ventilation, 3) time-to-hospital discharge, 4) intensive care unit admission, 5) serious disease trajectory, and 6) serious adverse events, compared to the control group. However, another meta-analysis found that although Tocilizumab significantly increased the rate of hospital discharges in COVID-19 patients, it had no effect on all-cause mortality or risk of secondary infections [56].
Some studies have now been carried out to assess the combined use of Tocilizumab and corticosteroid treatment in COVID-19 patients, and these have generally showed positive effects. Lim et al. carried out a meta-analysis of 13 randomized controlled trials and 24 case-control studies to compare the efficacy of Tocilizumab with corticosteroid treatment on mortality outcomes in 18,702 COVID-19 patients [57]. This revealed significant reductions in mortality following Tocilizumab-dexamethasone (odds ratio [OR]: 0.71, 95% confidence interval [CI]: 0.55–0.92) and Tocilizumab-Methylprednisolone (OR: 0.52, 95% CI: 0.36–0.75) therapies. No reduction in mortality was observed for mono-treatment with Methylprednisolone, and none of the drugs significantly reduced the need for mechanical ventilation (OR: 0.72, 95%CI: 0.32–1.60). Hong et al. carried out a retrospective cohort study of 33 COVID-19 patients receiving dexamethasone alone and 33 receiving dexamethasone plus Tocilizumab [58]. This showed that the combination treatment led to a significant benefit in a 30-day clinical recovery and reduced the need for supplemental oxygen compared to the dexamethasone mono-treatment group. Furthermore, meta-analysis found that the risk of death for COVID-19 patients treated with a corticosteroid-Tocilizumab combination compared with Tocilizumab alone or placebo control was 26% and 52% lower, respectively [59]. Considering these promising results, these studies call to attention the need for further testing on the use of COVID-19 treatments targeting different aspects of inflammation and immune signaling pathways.
3.4 Anakinra
Considering that hyper-inflammation is a key factor in driving severe COVID-19 infections, elevated concentrations of pro-inflammatory biomarkers such as interleukin 1 (IL-1) have been identified in COVID-19 patients who experienced a severe or critically ill outcome (Fig. 2.3b) [60]. Anakinra is a recombinant IL-1 receptor antagonist which has been approved for use in the European Union as an anti-inflammatory drug to reduce severity and mortality in COVID-19 patients (Table 2.2) [61]. A meta-analysis which assessed the effects of Anakinra treatment on key inflammatory biomarkers found that the serum levels of c-reactive protein (CRP), ferritin, and d-dimer were all reduced in the Anakinra compared to the standard care group [62]. Another meta-analysis found a significant reduction in mortality (OR = 0.34) and need for mechanical ventilation (OR = 0.68) in the Anakinra treatment arm compared with the standard care group [63]. However, the same study called to attention the need for further studies investigating the safety profile of this drug. These findings were confirmed by another meta-analysis, although this reported no difference in adverse events between the treatment and standard care groups [64].
3.5 Ritonavir
Ritonavir was originally developed as an inhibitor of the human immunodeficiency virus (HIV) protease [65, 66] and has been repurposed for similar use in COVID-19 patients via its ability to inhibit the SARS-CoV-2 3C-like protease enzyme (Fig. 2.3c and Table 2.2) [67]. Thus far, no meta-analyses have demonstrated the efficacy of this compound, either alone or in combination, in preventing serious disease in COVID-19 patients, with several reports of adverse effects [66, 68]. We suggest that further studies should be conducted to identify other more efficacious and safer antiviral drug candidates for COVID-19.
4 Effect of SARS-CoV-2 Variants on the Efficacy of Vaccines and Monoclonal Antibody Therapeutics
Although most of the developed vaccines worked well at preventing infections and serious illness courses with the original strain of the virus, most worked less efficaciously against the emerging SARS-CoV-2 variants. Planas et al. tested the sensitivity of Omicron compared to the Delta variant of the WHO-approved monoclonal antibody therapeutics using the S-Fuse assay [48]. All of these antibodies and antibody mixtures neutralized the Delta variant with IC50 concentrations ranging from 16 to 369 ng/mL (Table 2.3). However, the Tixagevimab/Cilgavimab combination (Evushield; AstarZeneca) and the Sotrovimab monotherapy (Xevudy; GlaxoSmithKline and Vir Biotechnology, Inc.) showed 85- and three-fold decreases in sensitivity, respectively, against Omicron compared to the Delta variant, and the Casirivimab/Imdevimab combination (Ronapreve; Regeneron) and Regdanvimab (Regkirona; Celltrion) had no detectable neutralizing activity towards the Omicron variant. The same study also tested the potency of antibodies elicited by the Comirnaty (Pfizer/BioNTech) and Vaxzevria (AstraZeneca) vaccines to neutralize the Omicron variant relative to the original SARS-CoV-2 strain and the Delta variant [48]. For both vaccines, sera were sampled 5 months after a two-dose vaccination schedule. This showed that the neutralizing antibody activity in sera was 3.6-fold lower against the Delta variant compared to the original strain of the Comirnaty vaccine, with no neutralization activity detected against the Omicron variant at the highest concentration. Similarly, the levels of antibodies in sera from Vaxzevria-vaccinated individuals were 2.8-fold lower in the neutralizing the Delta variant compared to the original strain, and no activity was observed against the Omicron variant. Similar findings were reported by Zhang et al. [69], Cao et al. [70], and Carreño et al. [71]. This underscores the capacity of the Omicron variant to escape the existing therapeutic monoclonal antibody treatments and vaccines.
As a means of predicting the capability of SARS-CoV-2 variants to escape antibody neutralization, Hu et al. developed a computational model to estimate the effect of mutations in the spike protein RBD on antibody neutralization titers [72]. Their results were similar to the experimentally determined neutralization titers of the known variants of concern, and they predicted a 17.4-fold decrease in the susceptibility of Omicron to neutralization.
5 Identification of Monoclonal Antibodies and Development of New Vaccines to Overcome the Immune Escape Capabilities of SARS-CoV-2 Variants
5.1 Monoclonal Antibodies
Zakir et al. identified a broadly neutralizing monoclonal antibody (mAb 9G8) which potently neutralizes the SARS-CoV-2 wild-type, Alpha, and Delta variants [73]. However, this has not been tested with the Omicron variant. A similar result was obtained with mAb 2G1 with respect to neutralizing all SARS-CoV-2 strains, but without testing on the Omicron variant as above [74]. In two in vitro and in vivo studies, Wang et al. found that another monoclonal antibody (mAb 35B5) was capable of neutralizing the original SARS-CoV-2 virus and other variants of concern such as Delta [75] and Omicron [76]. By using cryo-electron microscopy, they showed that this antibody targets a unique epitope outside the RBD, and this likely disrupts the conformational changes that allow SARS-CoV-2 binding to host ACE2 receptors [75, 76]. In a study of 30 healthy volunteers administering a mAb 35B5 nasal spray formulation, it was revealed that nasal mucosal samples collected within 24 h showed effective neutralization against pseudoviruses coated with SARS-CoV-2 spike protein variants including both Delta and Omicron [77]. However, full protection required daily inhalation of the spray, suggesting the need for further studies with optimized formulations to extend the duration of the antibody in the nasal mucosa.
Du et al. identified a monoclonal antibody (mAb 87G7) with potent in vitro neutralizing activity in vitro against all SARS-CoV-2 variants including the Omicron BA.1/BA.2 subvariants [78]. Using cryo-electron microscopy and site-directed mutagenesis, they showed that mAb 87G7 targets a conserved hydrophobic amino acid cluster in the ACE2 receptor binding site. Another study isolated two antibodies (EV053273 and EV053286) from convalescent patients after they had been infected with the wild-type version SARS-CoV-2 [79]. One of these antibodies (EV053273) had potent antiviral activity against wild-type SARS-CoV-2 and the Alpha and Delta variants, and the other (EV053286) had lower activity but neutralized all SARS-CoV-2 variants, including the Omicron BA.1 and BA.2 subvariants. They also found that a combination of these two antibodies blocked infection in vivo using a mouse model. In a similar study, Kovavech et al. identified a cocktail of two distinct monoclonal antibodies (AX290 and AX677) with high affinity to the SARS-CoV-2 spike protein RBD in all SARS-CoV-2 variants, including Omicron, and administration of this cocktail reduced viral burden and inflammation in the lungs of an infected mouse model in vivo [80]. Finally, another study developed monoclonal antibodies against Omicron and other SARS-CoV-2 variants elicited by vaccination with Convidecia [81]. One of these antibodies (ZWD12) showed potent neutralization against all strains of concern, including the Omicron variant.
5.2 SARS-CoV-2 Vaccines
5.2.1 Updated Vaccines
From the above findings, it is clear that the production of new vaccines against the current variant of concern is a pressing matter in gaining control over this pandemic. This includes the production of new vaccines specifically targeting the Omicron subvariants [82]. With this objective in mind, a recent study showed that the original Spikevax and Omicron-specific mRNA vaccines produced by Moderna elicited similar neutralizing responses to the Omicron BA.1 and BA.2 subvariants [83]. However, multiple countries and territories are now faced with outbreaks of Omicron BA.4 and BA.5, which may not be recognized by the time the above vaccines are rolled out. It is also possible that a new variant will branch out from a different part of the SARS-CoV-2 family tree. Thus, most scientists agree that constant updates to the existing vaccines are essential. Other pharmaceutical companies are testing Omicron-specific vaccines. For example, Pfizer–BioNTech reported that their new Omicron BA.1-based vaccine produced neutralizing antibody responses against this subvariant that were 2–3 times higher than that seen with a booster dose of their original Comirnaty vaccine [84]. Another study tested adults who had been doubly vaccinated with Comirnaty and had never tested positive for COVID-19 and then received a booster vaccination with either 1) a third dose of Comirnaty; 2) a recombinant spike protein (MVD614) based on the original SARS-CoV-2 strain or 3) a recombinant spike protein (MVB.1.351) based on the Beta variant [85]. The results showed that boosting with the MVB.1.351 vaccine resulted in a higher neutralizing antibody response against the original virus as well as the Beta, Delta, and Omicron BA.1 strains, compared to boosting with either the Comirnaty or MVD614 vaccines.
5.2.2 Multivalent Vaccines
One approach that can be taken with vaccines is that of multivalent administrations that simultaneously neutralize multiple variants. This is not a new concept as it has been used for decades with influenza vaccines each year, such as the simultaneous targeting of different varieties of influenza A and B strains [86]. It follows that a similar approach could be used to spike RBD sequences from multiple SARS-CoV-2 variants of concern. In line with this objective, Moderna has now developed a bivalent vaccine called mRNA-1273.214, which targets the spike protein of the original SARS-CoV-2 virus as well as the highly mutated Omicron variant [87]. Initial reports from a small trial of 439 participants suggested that this vaccine met the clinical endpoints. The data showed that the mean titer was 2372 for the bivalent vaccine, compared to 1473 for the original Moderna mRNA-1273 vaccine [88,89,90]. The bivalent vaccine was also well tolerated with a similar side effect profile as the current vaccine. Moderna plans to submit the results of this analysis over the coming weeks to regulators.
6 Natural Products for Improved Management of COVID-19 Patients
Herb-derived natural products have long been used in the management of numerous human ailments since ancient times. With the aid of technical advances in instrumental and biological fields, numerous phytochemicals have been isolated and identified as active ingredients responsible for the pharmacological actions exerted by famous medicinal plants. With respect to COVID-19, several medicinal plants and phytochemicals have been suggested and explored as potential candidates for the treatment of the disease or alleviation of the symptoms [91,92,93]. In fact, herbal medicines have been among the first options to enter clinical phase testing for COVID-19, owing to their availability and generally good safety and tolerability since most of the medicinal plants have a strong ethnobotanical background of use. From the mechanistic standpoint, phytochemicals might exert protective effects against COVID-19 through several mechanisms, including a direct impact on SARS-CoV-2 replication, and infectivity, regulation of ACE2 receptors and the renin-angiotensin system, anti-inflammatory action, and immunomodulatory properties [93, 94].
Among the phytochemicals, polyphenols have been the subject of a particular focus for their therapeutic potential in COVID-19 [91]. As a leading polyphenol, curcumin, the active ingredient of turmeric, has been the subject of several trials in patients at different stages of COVID-19 [95, 96]. A systematic review of clinical trials suggested the beneficial effects of different curcuminoid preparations, including nanoformulations and curcumin-piperine combinations, on symptom relief, hospitalization length, and mortality in patients suffering from COVID-19 [96]. The main mechanism suggested to explain the protective effects of curcumin in COVID-19 is the mitigation of inflammatory responses as well as the cytokine storm that is closely associated with end-stage adverse COVID-19 complications [95, 97, 98].
Another herbal product which has shown positive effects in clinical practice is the combination of glycyrrhizin and boswellic acids. Besides anti-inflammatory and immunomodulatory activities, both compounds have been reported to exert antiviral effects against SARS-CoV-2 [99, 100]. Glycyrrhizin has been proposed to inhibit the main protease (Mpro) of SARS-CoV-2, thereby interfering with viral replication [101]. Additionally, both glycyrrhizin and boswellic acids can interact with the functional spike protein of SARS-CoV-2 and reduce virus infectivity through mitigation of viral entry into the host cells [102, 103]. In a randomized, double-blind, and placebo-controlled trial, 50 hospitalized patients with moderate COVID-19 received either the combination of glycyrrhizin (60 mg twice daily) and boswellic acids (200 mg twice daily) or placebo for 14 days [104]. The findings revealed a significantly lower rate of mortality in the supplemented (n = 0) vs. placebo (n = 5) group. Moreover, there were significant improvements in terms of time to recovery, clinical status, serum CRP levels, and percentage of lymphocytes in the herbal combination group compared with the placebo group.
Chinese herbal medicine (CHM) is a comprehensive system of medicine with a strong ethnobotanical background dating to over 2000 years ago. Since the onset of the pandemic, CHM has been among the first therapeutic approaches tested for the management of COVID-19. Thus far, numerous herbs and formulae have been studied in patients with COVID-19, and several systematic review has been published [105,106,107]. However, the methodological limitations and risk of bias in several of the included trials precluded the possibility of reaching a definitive judgment on the efficacy and safety of CHM for the management of COVID-19. Recently, a systematic review and meta-analysis of 22 high-quality randomised controlled trials involving 1789 subjects assessed the value of adding CHM to Western medicine in controlling COVID-19 [108]. The results suggested the safety as well as the benefit of combining CHM with Western medicine in improving clinical, hematological, and virological indices of COVID-19, particularly in those with mild-to-moderate symptoms [108]. Nevertheless, evidence from long-term and multicenter trials is still required to better clarify the role of CHM in the management of COVID-19.
7 Conclusions and Future Perspectives
The emergence of new highly infective SARS-CoV-2 variants such as Omicron has wreaked havoc around the world by allowing the persistence of a pandemic that has already resulted in considerable damage at the individual, societal, and financial levels. Although unprecedented achievements have been made in attempts to stop the spread of COVID-19 disease, the problem has continued due to the mutability of the virus, which renders it with new properties such as increased infectivity and the ability to evade our immune defenses. This review has described efforts aimed at developing new vaccination strategies to keep pace with new SARS-CoV-2 variants as they appear, including variant-specific and multivalent vaccine designs. This included the use of vaccines that target the spike protein of specific SARS-CoV-2 strains and multivalent approaches that are directed simultaneously against the original SARS-CoV-2 isolate as well as the Omicron variant. Another possibility is the targeting of other antigenic domains within the virus that lie outside the spike protein RBD, as this may allow the development of a universal coronavirus vaccine [109].
In addition to the developments in SARS-CoV-2 vaccination strategies, we described pharmaceutical approaches that are currently in use for the treatment of individuals who become ill or suffer from postviral sequelae. Most of the existing drugs consist of either repurposed medicines, such as antiviral compounds and anti-inflammatory agents, or monoclonal antibodies obtained from convalescent or vaccinated patients. In addition, other approaches are currently under development to help overcome the limitations of the current methods. In the case of antibody-based therapeutics, one potential strategy is the use of broad coronavirus-directed nanobodies isolated from dromedary camels, which are natural reservoirs of coronaviruses, as these molecules can recognize cavities in proteins that are inaccessible to larger conventional antibodies. With this in mind, Hong et al. constructed a phage display library from camels containing nanobodies capable of protecting transgenic mice-expressing human ACE2 receptors against challenge with the SARS-CoV-2 Beta and Delta variants [110]. In addition, several studies have been conducted which have attempted to identify small molecules that disrupt binding of the SARS-CoV-2 spike protein RBD to the ACE2 receptor. Mediouni et al. screened a library of 15,000 small molecules and identified a compound called calpeptin, which blocked the entry of some of the SARS’CoV-2 variants in whole cell infectivity assays [111]. Another study found that an engineered soluble ACE2 peptide had high binding affinity to the spike protein of the original SARS-CoV-2 isolate as well as to the Alpha, Beta, Gamma, and Delta variants [112]. The same study found that this peptide reduced disease severity and improved survival in a transgenic human ACE2 mouse model infected with both the original SARS-CoV-2 strain and the Gamma variant. Due to the timing of the above studies, the effects of the SARS-CoV-2, RBD, and ACE2 inhibitors on the Omicron subvariants were not assessed. However, a recent study by Li et al. showed that an engineered ACE2 decoy protein had potent preventative and therapeutic efficacy against both Delta and Omicron in in vivo assays [113]. Finally, we described how several natural products are undergoing preclinical and clinical testing to determine their efficacy as preventative or therapeutic agents to prevent serious outcomes following SARS-CoV-2 infection. The advantage of these approaches is that the molecules concerned generally have good safety profiles and are predicted to work across all SARS-CoV-2 variants since they target the effects on the body and not the virus itself.
In conclusion, this review has described the importance of developing vaccines and treatment strategies that keep pace with the new SARS-CoV-2 variants as these emerge. In the case of vaccines and therapeutic antibodies, this could involve the production of broadly neutralizing or variant-specific products. For treatment approaches, considerable further work is required to identify the most efficacious approaches without the trade-off of poor safety profiles. Most of all, it will be important to lay the foundations for a procedural pipeline to cope with the likely appearance of new coronavirus variants.
References
Our World in Data; Coronavirus (COVID-19) Vaccinations. https://ourworldindata.org/covid-vaccinations. Accessed June 24, 2022
United Nations; Press Release; Unequal Vaccine Distribution Self-Defeating, World Health Organization Chief Tells Economic and Social Council’s Special Ministerial Meeting. https://www.un.org/press/en/2021/ecosoc7039.doc.htm#:~:text=With%20the%20number%20of%20new,head%20of%20the%20United%20Nations. Accessed June 24, 2022
Yogesh R, Srivastava N, Abbas Bukhari SN (2022) COVID-19 Challenge: A Quest for Effective Vaccine Strategies Against Circulating and Emerging SARS-CoV-2 Variants. Curr Pharm Des. https://doi.org/10.2174/1381612828666220701160116
Sallam M, Al-Sanafi M, Sallam M (2022) A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. Journal of Multidisciplinary Healthcare 15:21–45. https://doi.org/10.2147/JMDH.S347669
Stokel-Walker C (2022) How are vaccines being adapted to meet the changing face of SARS-CoV-2? BMJ 377. https://doi.org/10.1136/bmj.o1257
Gov.uk; COVID-19: guidance for people whose immune system means they are at higher risk; Updated 16 June 2022. https://www.gov.uk/government/publications/covid-19-guidance-for-people-whose-immune-system-means-they-are-at-higher-risk/covid-19-guidance-for-people-whose-immune-system-means-they-are-at-higher-risk. Accessed July 09, 2022
van der Straten K, van Gils MJ, de Taeye SW, de Bree GJ (2022) Optimization of Anti-SARS-CoV-2 Neutralizing Antibody Therapies: Roadmap to Improve Clinical Effectiveness and Implementation. Front Med Technol 4:867982. https://doi.org/10.3389/fmedt.2022.867982
Statistica. Number of SARS-CoV-2 Omicron variant cases worldwide as of May 16, 2022, by country or territory. https://www.statista.com/statistics/1279100/number-omicron-variant-worldwide-by-country/. Accessed June 24, 2022
Islam F, Dhawan M, Nafady MH, et al (2022) Understanding the omicron variant (B.1.1.529) of SARS-CoV-2: Mutational impacts, concerns, and the possible solutions. Ann Med Surg (Lond) 78:103737. https://doi.org/10.1016/j.amsu.2022.103737
Lubin JH, Markosian C, Balamurugan D, et al (2021) Structural models of SARS-CoV-2 Omicron variant in complex with ACE2 receptor or antibodies suggest altered binding interfaces. bioRxiv 2021.12.12.472313. https://doi.org/10.1101/2021.12.12.472313
Kannan SR, Spratt AN, Sharma K, et al (2022) Omicron SARS-CoV-2 variant: Unique features and their impact on pre-existing antibodies. J Autoimmun 126:102779. https://doi.org/10.1016/j.jaut.2021.102779
COMIRNATY®▼(TOZINAMERAN) COVID-19 mRNA VACCINE (NUCLEOSIDE MODIFIED). https://www.pfizer.co.uk/products/prescription-medicines/comirnaty. Accessed June 29, 2022
Vaxzevria (previously COVID-19 Vaccine AstraZeneca). https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria-previously-covid-19-vaccine-astrazeneca. Accessed July 09, 2022
Serum Institute of India: Covishield (Oxford/ AstraZeneca formulation). https://covid19.trackvaccines.org/vaccines/48/. Accessed July 09, 2022
Spikevax (previously COVID-19 Vaccine Moderna). https://www.ema.europa.eu/en/medicines/human/EPAR/spikevax. Accessed July 09, 2022
Sinopharm (Beijing): Covilo. https://covid19.trackvaccines.org/vaccines/5/. Accessed July 09, 2022
Jcovden (previously COVID-19 Vaccine Janssen). https://www.ema.europa.eu/en/medicines/human/EPAR/jcovden-previously-covid-19-vaccine-janssen. Accessed July 09, 2022
Sinovac: CoronaVac. https://covid19.trackvaccines.org/vaccines/7/. Accessed July 09, 2022
COVAXIN® – India’s First Indigenous COVID-19 Vaccine. https://www.bharatbiotech.com/covaxin.html. Accessed July 09, 2022
Serum Institute of India: COVOVAX (Novavax formulation). https://covid19.trackvaccines.org/vaccines/123/. Accessed July 09, 2022
Nuvaxovid. https://www.ema.europa.eu/en/medicines/human/EPAR/nuvaxovid. Accessed July 09, 2022
CanSino: Convidecia. https://covid19.trackvaccines.org/vaccines/2/. Accessed July 09, 2022
von Gabain A, Klade C (Eds) (2012) Development of Novel Vaccines: Skills, Knowledge and Translational Technologies. Springer; New York, NY, USA. ISBN-13: 978-3709107089
Leroy O, Geels M, Korejwo J, et al (2014) Roadmap for the establishment of a European vaccine R & D infrastructure. Vaccine 32(51):7021–7024
Wen EP, Ellis R, Pujar NS (2015) Vaccine Development and Manufacturing (Wiley Series in Biotechnology and Bioengineering): 5. Wiley; New York, NY, USA. ISBN-13: 978-0470261941
Rahmoune H, Guest PC (2017) Application of Multiplex Biomarker Approaches to Accelerate Drug Discovery and Development. Methods Mol Biol 1546:3–17
Mellet J, Pepper MS (2021) A COVID-19 Vaccine: Big Strides Come with Big Challenges. Vaccines (Basel) 9(1):39. https://doi.org/10.3390/vaccines9010039
Carneiro DC, Sousa JD, Monteiro-Cunha JP (2021) The COVID-19 vaccine development: A pandemic paradigm. Virus Res 301:198454. https://doi.org/10.1016/j.virusres.2021.198454.
Wagner R, Hildt E, Grabski E, et al (2021) Accelerated Development of COVID-19 Vaccines: Technology Platforms, Benefits, and Associated Risks. Vaccines (Basel) 9(7):747. https://doi.org/10.3390/vaccines9070747
Guest PC, Ozanne SE (2021) The Worldwide Effort to Develop Vaccines for COVID-19. Adv Exp Med Biol 1327:215–223
Gasmi A, Srinath S, Dadar M, et al (2022) A global survey in the developmental landscape of possible vaccination strategies for COVID-19. Clin Immunol 237:108958. https://doi.org/10.1016/j.clim.2022.108958
How have Covid-19 vaccines been made quickly and safely? https://wellcome.org/news/quick-safe-covid-vaccine-development. Accessed July 11, 2022
U.S. Food and Drud Administration. FDA Approves First Treatment for COVID-19. https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19. Accessed June 30, 2022
Gilead Press Releases (Jan 21, 2022) FDA Approves Veklury® (Remdesivir) for the Treatment of Non-Hospitalized Patients at High Risk for COVID-19 Disease Progression. https://www.gilead.com/news-and-press/press-room/press-releases/2022/1/fda-approves-veklury-remdesivir-for-the-treatment-of-nonhospitalized-patients-at-high-risk-for-covid19-disease-progression. Accessed Jun 30, 2022
Warren TK, Jordan R, Lo MK, et al (2016) Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 531(7594):381–5
Tchesnokov EP, Feng JY, Porter DP, Götte M (2019) Mechanism of Inhibition of Ebola Virus RNA-Dependent RNA Polymerase by Remdesivir. Viruses 11(4):326. https://doi.org/10.3390/v11040326
Angamo MT, Mohammed MA, Peterson GM (2022) Efficacy and safety of remdesivir in hospitalised COVID-19 patients: a systematic review and meta-analysis. Infection 50(1):27–41
Santenna C, Vidyasagar K, Amarneni KC, et al (2021) The safety, tolerability and mortality reduction efficacy of remdesivir; based on randomized clinical trials, observational and case studies reported safety outcomes: an updated systematic review and meta-analysis. Ther Adv Drug Saf 12:20420986211042517. https://doi.org/10.1177/20420986211042517
Tanni SE, Silvinato A, Floriano I, et al (2022) Use of remdesivir in patients with COVID-19: a systematic review and meta-analysis. J Bras Pneumol 48(1):e20210393. https://doi.org/10.36416/1806-3756/e20210393
Kim C, Ryu DK, Lee J, et al (2021) A therapeutic neutralizing antibody targeting receptor binding domain of SARS-CoV-2 spike protein. Nat Commun 12(1):288. https://doi.org/10.1038/s41467-020-20602-5.
Yang M, Li A, Jiang L, et al (2022) Regdanvimab improves disease mortality and morbidity in patients with COVID-19: A meta-analysis. J Infect S0163-4453(22)00369-3. https://doi.org/10.1016/j.jinf.2022.05.044
Weinreich DM, Sivapalasingam S, Norton T, et al (2021) REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients with Covid-19. N Engl J Med 384(3):238–251
Suzuki Y, Shibata Y, Minemura H, et al (2022) Real-world clinical outcomes of treatment with casirivimab-imdevimab among patients with mild-to-moderate coronavirus disease 2019 during the Delta variant pandemic. Int J Med Sci 19(5):834–841
Pinto D, Park YJ, Beltramello M, et al (2020) Cross-neutralization of SARS-CoV-2 by a human monoclonal SARS-CoV antibody. Nature 583(7815):290–295
Menéndez R, González P, Latore A, Méndez R (2022) Immune treatment in COVID-19. Rev Esp Quimioter 35 Suppl 1(Suppl 1):59–63
Tao K, Tzou PL, Kosakovsky Pond SL, et al (2022) Susceptibility of SARS-CoV-2 Omicron Variants to Therapeutic Monoclonal Antibodies: Systematic Review and Meta-analysis. Microbiol Spectr. Jun 14:e0092622. https://doi.org/10.1128/spectrum.00926-22
Zhou H, Dcosta BM, Landau NR, Tada T (2022) Resistance of SARS-CoV-2 Omicron BA.1 and BA.2 Variants to Vaccine-Elicited Sera and Therapeutic Monoclonal Antibodies. Viruses 14(6):1334. https://doi.org/10.3390/v14061334
Planas D, Saunders N, Maes P, et al (2022) Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature 602(7898):671–675
Zost SJ, Gilchuk P, Case JB, et al (2020) Potently neutralizing and protective human antibodies against SARS-CoV-2. Nature 584(7821):443–449
Levin MJ, Ustianowski A, De Wit S, et al (2022) Intramuscular AZD7442 (Tixagevimab-Cilgavimab) for Prevention of Covid-19. N Engl J Med 386(23):2188–2200
Herold T, Jurinovic V, Arnreich C, et al (2020) Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy Clin Immunol 146(1):128–136.e4
Laguna-Goya R, Utrero-Rico A, Talayero P, et al (2020) IL-6-based mortality risk model for hospitalized patients with COVID-19. J Allergy Clin Immunol 146(4):799–807.e9
Scott LJ (2017) Tocilizumab: A review in rheumatoid arthritis. Drugs 77(17):1865–1879
Maraolo AE, Crispo A, Piezzo M, et al (2021) The Use of Tocilizumab in Patients with COVID-19: A Systematic Review, Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Studies. J Clin Med. 2021 Oct 25;10(21):4935. https://doi.org/10.3390/jcm10214935
Zhang J, Chen C, Yang Y, Yang J (2022) Effectiveness of tocilizumab in the treatment of hospitalized adults COVID-19: A systematic review and meta-analysis. Medicine (Baltimore) 101(9):e28967. https://doi.org/10.1097/MD.0000000000028967
Peng J, She X, Mei H, et al (2022) Association between tocilizumab treatment and clinical outcomes of COVID-19 patients: a systematic review and meta-analysis. Aging (Albany NY) 14(2):557–571
Lim PC, Wong KL, Rajah R, et al (2022) Comparing the efficacy of tocilizumab with corticosteroid therapy in treating COVID-19 patients: a systematic review and meta-analysis. Daru 30(1):211–228
Hong JY, Ko JH, Yang J, et al (2022) Severity-Adjusted Dexamethasone Dosing and Tocilizumab Combination for Severe COVID-19. Yonsei Med J 63(5):430–439
Moosazadeh M, Mousavi T (2022) Combination therapy of tocilizumab and steroid for COVID-19 patients: A meta-analysis. J Med Virol 94(4):1350–1356
Yuan X, Huang W, Ye B, et al (2020) Changes of hematological and immunological parameters in COVID-19 patients. Int J Hematol 112(4):553–559
Iglesias-Julián E, López-Veloso M, de-la-Torre-Ferrera N, et al (2020) High dose subcutaneous Anakinra to treat acute respiratory distress syndrome secondary to cytokine storm syndrome among severely ill COVID-19 patients. J Autoimmun 115:102537. https://doi.org/10.1016/j.jaut.2020.102537
Naveed Z, Sarwar M, Ali Z, et al (2022) Anakinra treatment efficacy in reduction of inflammatory biomarkers in COVID-19 patients: A meta-analysis. J Clin Lab Anal 36(6):e24434. https://doi.org/10.1002/jcla.24434
Somagutta MKR, Lourdes Pormento MK, et al (2021) The Safety and Efficacy of Anakinra, an Interleukin-1 Antagonist in Severe Cases of COVID-19: A Systematic Review and Meta-Analysis. Infect Chemother 53(2):221–237
Barkas F, Filippas-Ntekouan S, Kosmidou M, et al (2021) Anakinra in hospitalized non-intubated patients with coronavirus disease 2019: a Systematic review and meta-analysis. Rheumatology (Oxford) 60(12):5527–5537
Carr A, Cooper DA (1996) HIV protease inhibitors. AIDS 10 Suppl A:S151–157. https://doi.org/10.1097/00002030-199601001-00021
Patel TK, Patel PB, Barvaliya M, et al (2021) Efficacy and safety of lopinavir-ritonavir in COVID-19: A systematic review of randomized controlled trials. J Infect Public Health 14(6):740–748
Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB (2020) Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA 323(18):1824–1836
Deng J, Zhou F, Hou W, et al (2021) Efficacy of lopinavir-ritonavir combination therapy for the treatment of hospitalized COVID-19 patients: a meta-analysis. Future Virol. https://doi.org/10.2217/fvl-2021-0066
Zhang L, Li Q, Liang Z, et al (2022) The significant immune escape of pseudotyped SARS-CoV-2 variant Omicron. Emerg Microbes Infect 11(1):1–5
Cao Y, Wang J, Jian F, et al (2022) Omicron escapes the majority of existing SARS-CoV-2 neutralizing antibodies. Nature 602(7898):657–663
Carreño JM, Alshammary H, Tcheou J, et al (2022) Activity of convalescent and vaccine serum against SARS-CoV-2 Omicron. Nature 602(7898):682–688
Hu YF, Hu JC, Gong HR, et al (2022) Computation of Antigenicity Predicts SARS-CoV-2 Vaccine Breakthrough Variants. Front Immunol 13:861050. https://doi.org/10.3389/fimmu.2022.861050
Zakir TS, Meng T, Carmen LCP, et al (2022) Characterization of a Broadly Neutralizing Monoclonal Antibody against SARS-CoV-2 Variants. Viruses 14(2):230. https://doi.org/10.3390/v14020230
Ma H, Guo Y, Tang H, et al (2022) Broad ultra-potent neutralization of SARS-CoV-2 variants by monoclonal antibodies specific to the tip of RBD. Cell Discov 8(1):16. https://doi.org/10.1038/s41421-022-00381-7
Wang X, Hu A, Chen X, et al (2022) A potent human monoclonal antibody with pan-neutralizing activities directly dislocates S trimer of SARS-CoV-2 through binding both up and down forms of RBD. Signal Transduct Target Ther 7(1):114. https://doi.org/10.1038/s41392-022-00954-8
Wang X, Chen X, Tan J, et al (2022) 35B5 antibody potently neutralizes SARS-CoV-2 Omicron by disrupting the N-glycan switch via a conserved spike epitope. Cell Host Microbe 30(6):887–895.e4
Lin Y, Yue S, Yang Y, et al (2022) Nasal Spray of Neutralizing Monoclonal Antibody 35B5 Confers Potential Prophylaxis Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Variants of Concern (VOCs): A Small-scale Clinical Trial. Clin Infect Dis; ciac448. https://doi.org/10.1093/cid/ciac448
Du W, Hurdiss DL, Drabek D, et al (2022) An ACE2-blocking antibody confers broad neutralization and protection against Omicron and other SARS-CoV-2 variants of concern. Sci Immunol: eabp9312. https://doi.org/10.1126/sciimmunol.abp9312
Ueno M, Iwata-Yoshikawa N, Matsunaga A, et al (2022) Isolation of human monoclonal antibodies with neutralizing activity to a broad spectrum of SARS-CoV-2 viruses including the Omicron variants. Antiviral Res 201:105297. https://doi.org/10.1016/j.antiviral.2022.105297
Kovacech B, Fialova L, Filipcik P, et al (2022) Monoclonal antibodies targeting two immunodominant epitopes on the Spike protein neutralize emerging SARS-CoV-2 variants of concern. EBioMedicine 76:103818. https://doi.org/10.1016/j.ebiom.2022.103818
Chi X, Guo Y, Zhang G, et al (2022) Broadly neutralizing antibodies against Omicron-included SARS-CoV-2 variants induced by vaccination. Signal Transduct Target Ther 7(1):139. https://doi.org/10.1038/s41392-022-00987-z
Marta RA, Nakamura GEK, de Matos Aquino B, Bignardi PR (2022) Vacunas. https://doi.org/10.1016/j.vacun.2022.06.003
Gagne M, Moliva J, Foulds KE, et al (2022) mRNA-1273 or mRNA-Omicron boost in vaccinated macaques elicits similar B cell expansion, neutralizing responses, and protection from Omicron. Cell 185(9):1556–1571.e18
Callaway E (2022) Fast-evolving COVID variants complicate vaccine updates. Nature 607(7917):18–19
Launay O, Cachanado M, Nguyen LBL, et al (2022) Immunogenicity and Safety of Beta Adjuvanted Recombinant Booster Vaccine. N Engl J Med; NEJMc2206711. https://doi.org/10.1056/NEJMc2206711
European Medicines Agency. Flucelvax Tetra (influenza vaccine). https://www.ema.europa.eu/en/documents/overview/flucelvax-tetra-epar-medicine-overview_en.pdf. Accessed July 09, 2022
Moderna’s Omicron-targeted booster shot shows promise. Center for Infectious Disease Research and Policy. https://www.cidrap.umn.edu/news-perspective/2022/06/modernas-omicron-targeted-booster-shot-shows-promise. Accessed June 16, 2022
National Institutes of Health. Promising Interim Results from Clinical Trial of NIH-Moderna COVID-19 Vaccine. https://www.nih.gov/news-events/news-releases/promising-interim-results-clinical-trial-nih-moderna-covid-19-vaccine. Accessed June 16, 2022
Jackson LA, Anderson EJ, Rouphael NG, Roberts PC, Makhene M, Coler RN et al (2020) An mRNA Vaccine against SARS-CoV-2 – Preliminary Report. N Engl J Med 383(20):1920–1931
Noor R (2021) Developmental Status of the Potential Vaccines for the Mitigation of the COVID-19 Pandemic and a Focus on the Effectiveness of the Pfizer-BioNTech and Moderna mRNA Vaccines. Curr Clin Microbiol Rep 8(3):178–185
Paraiso IL, Revel JS, Stevens JF (2020) Potential use of polyphenols in the battle against COVID-19. Curr Opin Food Sci 32:149–155
Hosseini SA, Zahedipour F, Sathyapalan T, et al (2021) Pulmonary fibrosis: Therapeutic and mechanistic insights into the role of phytochemicals. Biofactors 47(3):250–269
Demeke CA, Woldeyohanins AE, Kifle ZD (2021) Herbal medicine use for the management of COVID-19: A review article. Metabol Open 12:100141. https://doi.org/10.1016/j.metop.2021.100141
Adhikari B, Marasini BP, Rayamajhee B, et al (2021) Potential roles of medicinal plants for the treatment of viral diseases focusing on COVID-19: A review. Phytother Res 35(3):1298–1312
Zahedipour F, Hosseini SA, Sathyapalan T, et al (2020) Potential effects of curcumin in the treatment of COVID-19 infection. Phytother Res 34(11):2911–2920
Vahedian-Azimi A, Abbasifard M, Rahimi-Bashar F, et al (2022) Effectiveness of Curcumin on Outcomes of Hospitalized COVID-19 Patients: A Systematic Review of Clinical Trials. Nutrients 14(2):256. https://doi.org/10.3390/nu14020256
Heidari Z, Mohammadi M, Sahebkar A (2021) Possible Mechanisms and Special Clinical Considerations of Curcumin Supplementation in Patients with COVID-19. Adv Exp Med Biol 1308:127–136
Miryan M, Soleimani D, Askari G, et al (2021) Curcumin and Piperine in COVID-19: A Promising Duo to the Rescue? Adv Exp Med Biol 1327:197–204
Gomaa AA, Abdel-Wadood YA (2021) The potential of glycyrrhizin and licorice extract in combating COVID-19 and associated conditions. Phytomedicine plus 1:100043. https://doi.org/10.1016/j.phyplu.2021.100043
Gomaa AA, Mohamed HS, Abd-Ellatief RB, Gomaa MA (2021) Boswellic acids/Boswellia serrata extract as a potential COVID-19 therapeutic agent in the elderly. Inflammopharmacology 29(4):1033–1048
van de Sand L, Bormann M, Alt M, et al (2021) Glycyrrhizin effectively inhibits SARS-CoV-2 replication by inhibiting the viral main protease. Viruses 13(4):609. https://doi.org/10.3390/v13040609
Li J, Xu D, Wang L, et al (2021) Glycyrrhizic acid inhibits SARS-CoV-2 infection by blocking spike protein-mediated cell attachment. Molecules 26(20):6090. https://doi.org/10.3390/molecules26206090
Caliebe RH, Scior T, Ammon HP (2021) T (2021) Binding of boswellic acids to functional proteins of the SARS-CoV-2 virus: Bioinformatic studies. Arch Pharm 354:2100160. https://doi.org/10.1002/ardp.202100160
Gomaa AA, Mohamed HS, Abd-ellatief RB et al (2022) Advancing combination treatment with glycyrrhizin and boswellic acids for hospitalized patients with moderate COVID-19 infection: a randomized clinical trial. Inflammopharmacol 30(2):477–486
Luo X, Ni X, Lin J, et al (2021) The add-on effect of Chinese herbal medicine on COVID-19: a systematic review and meta-analysis. Phytomedicine 16(8):e0256429. https://doi.org/10.1371/journal.pone.0256429
Liu M, Gao Y, Yuan Y, et al (2020) Efficacy and safety of integrated traditional Chinese and western medicine for Corona Virus Disease 2019 (COVID-19): a systematic review and meta-analysis. Pharmacol Res 158:104896. https://doi.org/10.1016/j.phrs.2020.104896
Zhou LP, Wang J, Xie RH, et al (2021) The effects of traditional chinese medicine as an auxiliary treatment for COVID-19: a systematic review and meta-analysis. J Altern Complement Med 27(3):225–237
Li L, Xie H, Wang L, et al (2022) The efficacy and safety of combined chinese herbal medicine and western medicine therapy for COVID-19: a systematic review and meta-analysis. Chin Med 17(1):77. https://doi.org/10.1186/s13020-022-00600-z
Yoon E, Kim D, Jeon H, et al (2022) Severe Acute Respiratory Syndrome Coronavirus 2 Variants-Possibility of Universal Vaccine Design: A Review. Comput Struct Biotechnol J. https://doi.org/10.1016/j.csbj.2022.06.043
Hong J, Kwon HJ, Cachau R, et al (2022) Dromedary camel nanobodies broadly neutralize SARS-CoV-2 variants. Proc Natl Acad Sci U S A. 2022 May 3;119(18):e2201433119. https://doi.org/10.1073/pnas.2201433119
Mediouni S, Mou H, Otsuka Y, et al (2022) Identification of potent small molecule inhibitors of SARS-CoV-2 entry. SLAS Discov 27(1):8–19
Zhang L, Dutta S, Xiong S, et al (2022) Engineered High-Affinity ACE2 Peptide Mitigates ARDS and Death Induced by Multiple SARS-CoV-2 Variants. Nat Chem Biol 18(3):342–351
Li M, Ye ZW, Tang K, et al (2022) Enhanced trimeric ACE2 exhibits potent prophylactic and therapeutic efficacy against the SARS-CoV-2 Delta and Omicron variants in vivo. Cell Res 32(6):589–592
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Sahebkar, A., Jamialahmadi, T., Rahmoune, H., Guest, P.C. (2023). Long-Term Vaccination and Treatment Strategies for COVID-19 Disease and Future Coronavirus Pandemics. In: Guest , P.C. (eds) Application of Omic Techniques to Identify New Biomarkers and Drug Targets for COVID-19. Advances in Experimental Medicine and Biology(), vol 1412. Springer, Cham. https://doi.org/10.1007/978-3-031-28012-2_2
Download citation
DOI: https://doi.org/10.1007/978-3-031-28012-2_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-28011-5
Online ISBN: 978-3-031-28012-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)