
Abstract
Endoscopic approaches for enteral feeding access are the preferred method of long-term nutrition support. Compared to parenteral nutrition, enteral feeding provides physiological and structural benefits to the gastrointestinal tract, which in turn have systemic benefits. Additionally, endoscopic modalities are less invasive than surgical approaches, thereby reducing complication rates and duration of hospital stay. Percutaneous endoscopic gastrostomy was first introduced in 1980 and served as a cornerstone for the development of percutaneous endoscopic gastro-jejunostomy and percutaneous endoscopic jejunostomy. These procedures are commonly performed today for patients with various chronic, traumatic, or malignant conditions and who are in need of nutritional support. Although endoscopic enteral access provides many benefits, understanding its indications and limitations is critical for performing these procedures safely and effectively. This chapter provides an overview of current knowledge and practices in the rapidly evolving field of endoscopic enteral access, with emphasis on patient selection, preoperative considerations, technical conduct, and avoidance of complications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Percutaneous endoscopic gastrostomy
- Percutaneous endoscopic gastrostomy-jejunostomy
- Percutaneous endoscopic jejunostomy
- Indications
- Complications
- Technique
- Enteral access
- Enteral nutrition
Introduction
Enteral access is artificial access to the gastrointestinal tract to provide a means of nutritional support and gastrointestinal decompression. Enteral nutrition allows patients with a functional gastrointestinal tract and who have difficulty with oral intake of food to maintain nutritional status. Enteral feeding allows for more physiologic digestion and preserves gastrointestinal integrity and local defense. Enteral feeding is increasingly recognized as therapeutic for critically ill patients, attenuating severity and reducing complications of their underlying conditions.
Access for enteral feeding is established by placement of tubes through natural orifices or directly by percutaneous or surgical approaches. For short-term use (<4 weeks), enteral tubes are temporarily placed through the nasal or oral passage. However, prolonged use of oral or nasal enteral tubes is poorly tolerated and may create local complications; thus, direct access to the stomach or small intestine is recommended for the use of enteral tubes longer than 4 weeks. The percutaneous approach is a popular alternative to surgically-created stomas, albeit each has its own advantages and disadvantages.
Percutaneous endoscopic gastrostomy (PEG) was introduced in 1980 by Michael Gauderer, MD, and Jeffrey Ponsky, MD [1]. The procedure was performed on a 4 month-old infant with the intent to create a sutureless opposition of the stomach to the peritoneum and abdominal wall without laparotomy [2]. Although originally intended for children, PEG is now widely performed across all age groups. In the USA, more than 200,000 PEG procedures are performed annually by surgeons and gastroenterologists. The advantages of PEG include convenience and the use of moderate, conscious sedation compared to general anesthesia. Compared to the standard open Stamm gastrostomy, PEG is associated with reduced operative time, expense, the incidence of complications, and less recovery time [3]. The PEG procedure has also undergone several modifications and has led to the other modalities of enteral access, such as percutaneous endoscopic gastrojejunostomy (PEG-J) and percutaneous endoscopic jejunostomy (PEJ) [2].
Patient Selection
The suitability for enteral access should be assessed and confirmed by a multidisciplinary team, including an endoscopist and nutritional support team. Patients should be evaluated by history, physical examination, and risk factors prior to performing the operation. Proper patient selection is a key to achieving successful outcomes.
Gastric Feeding and Decompression
Gastrostomy is the most common route of prolonged enteral feeding (>4 weeks). Patients must have normal gastrointestinal motility and adequate stomach anatomy for gastric access. Patients selected for PEG often have impaired swallowing, contraindications to oral intake, metastatic disease, or neurologic impairment.
Patients with upper GI malignancy are candidates for PEG due to obstruction and side effects of tumor radiation impeding swallowing abilities. Up to 64% of patients with head and neck carcinoma have dysphagia and associated malnutrition. Malignancies in the upper gastrointestinal tract can cause gastric outlet or intestinal obstruction. PEG is performed in these patients for decompression of abdominal pressure, to alleviate nausea and vomiting, and to provide supplemental nutrition. However, PEG should not be performed if the patient has esophageal cancer and may require gastric conduit reconstruction.
Inability or difficulty to swallow due to neurologic disorders, such as stroke and ALS, are indicators for enteral feeding [4]. Indicators of prolonged dysphagia may include aspiration, pneumonia, and lesions of the frontal and insular cortex of the brain [5]. Because under-nutrition is associated with poor prognosis, stroke patients should be initiated for enteral feeding early as most require prolonged nutrition support [6]. However, one study did show that placement within seven days of a stroke may increase the risk of death [7]. Compared to NG tube feeding, PEG -tube feeding for neurologic disorders is associated with fewer treatment failures and GI bleeding and has higher feed delivery and albumin concentration. However, the placement of PEG in patients with advanced dementia or Alzheimer’s disease may not be useful. Although these patients have poor nutritional intake, PEG -tube feeding does not appear to prolong survival, according to seven observational studies [8, 9].
Patients with severe cerebral injury or trauma may also require enteral nutrition. Although recovery time and the expected duration of nutrition support are unclear, some studies suggest that PEG placement can be performed in 14 days to restore physiological digestive function [10].
PEG also allows patients with chronic inflammatory intestinal disorders, such as Crohn’s disease and cystic fibrosis, to meet their nutritional needs. Crohn’s disease was initially believed to be a contraindication due to disease occurrence within the gastrostomy tract. However, PEG placement is now commonly performed to improve weight and growth in children with Crohn’s disease. Similarly, patients with cystic fibrosis experience a greater improvement in nutritional status and pulmonary function with early intervention from PEG [11].
Jejunal Feeding
Jejunal feeding is achieved through percutaneous endoscopic gastrostomy-jejunostomy (PEG-J) or percutaneous endoscopic jejunostomy (PEJ). Although there is no difference in mortality between gastric feeding and jejunal feeding, jejunal feeding is considered in situations when the placement of a conventional PEG tube is unsuitable. Several meta-analyses show that there is no difference in mortality between jejunal feeding and gastric feeding. Both procedures are acceptable; however, jejunal feeding may be preferred due to anatomical factors and intolerance to PEG. Insufficient amount of stomach due to gastrectomy and gastrojejunostomy allows more proximal access to the jejunum by a standard endoscope. A common scenario for this is patients with a Roux-en-Y gastrojejunostomy, where the endoscope can access the roux limb in an ante-colic position. Thus, PEJ is often preferable compared to PEG-J or PEG in patients with previous upper gastrointestinal surgeries for nutrition support.
Jejunal feeding is also recommended in patients with recurrent aspiration, gastric outlet obstruction, altered gastric motility, or who had gastric feeding intolerance. Delivery of nutrients to the small bowel can attenuate problems with aspiration, vomiting, or reflux due to gastroparesis, GERD, or recurrent aspiration. If a PEG is already present, PEG can be converted to PEG-J. A PEG-J is also beneficial for simultaneous jejunal feeding and gastric decompression in the presence of gastric outlet obstruction.
Jejunal feeding may be physiologically beneficial for patients with severe chronic pancreatitis. Nutritional management for pancreatitis should include minimal stimulation of the exopancreas, while providing optimal nutrition. Oral or gastric feeding stimulates the cephalic, gastric, and intestinal phases of pancreatic secretion and thus leads to significant pancreatic secretions. Conversely, jejunal feeding has less disturbance or impact on normal gut hormone and exocrine pancreas secretions. Several case reports have reported successful outcomes from PEJ therapy in this subset of patients [12].
Special Considerations
Obesity With the emergence of the worldwide obesity epidemic over the last few decades, an increasing number of patients with obesity require enteral nutrition support. Obese patients can present a challenge due to increased difficulty of transillumination or digital palpation with a thicker abdomen and additional adipose tissue. However, recent studies report an 89.6–97% success rate and 0% mortality rate for PEG in overweight and obese patients [13,14,15].
Pregnancy Special precautions must be taken when performing PEG in pregnant women. PEG insertion may pose a risk of injury to uterus and fetus. However, PEG has been performed successfully in pregnant women without any major complications.
Absolute Contraindications
Prior to the placement of the natural access tube, the overall patients’ prognosis and ability to recover are important considerations. Although increasing studies suggest earlier initiation is acceptable, the consensus remains that enteral feeding is reserved for long-term feeding (>4 weeks). PEG, PEG-J, or PEJ tubes should not routinely be offered if life expectancy is <4 weeks or cannot improve the patient’s quality of life. Other contraindications are severe ascites, discontinuous esophagus, hemodynamic instability, septic shock, and coagulopathy (INR >1.4).
Preoperative Considerations
Antibiotic Prophylaxis
Wound infection is the most common complication associated with trans-abdominal enteral access. In addition, many patients who require enteral nutrition are inherently at high-risk for infection, such as old age, malnutrition, and immunosuppression, further emphasizing the need for prophylactic antibiotics. The risk for infection indicates the need for prophylactic antibiotics with broad-spectrum coverage, such as cefazolin. According to a meta-analysis of ten randomized clinical trials, cephalosporin and penicillin-based antibiotics have a similar relative risk reduction (64% and 62%) and absolute risk reduction (10% vs. 13%, respectively) [16]. Systemic antibiotics should be administered as prophylaxis 30 min prior to the procedure, unless the patient is already receiving broad-spectrum antibiotics. Decolonization of equipment prior to the procedure may also decrease risks of MRSA infection.
Sedation
Moderate or conscious sedation is frequently used for endoscopic procedures. However, comorbid conditions, such as obesity, seizure disorder, neurologically impaired consciousness, may indicate the need for anesthesia-assisted sedation. Accordingly, sedation is associated with the risk of cardiopulmonary complications. Patients should be carefully assessed for these risks preoperatively, and interventional equipment should be present during the procedure. Alternatively, a method for unsedated PEG placement has been described for highly select patients whose risk of anesthesia outweighs the benefit. Woodward et al. describe the nasal unsedated seated PEG using nasal endoscopes in patients with progressive neurodegenerative disorders that employ only the use of local anesthetic with acceptable success and complication rates [17].
Anticoagulation and Antiplatelet
Anticoagulation and antiplatelet therapy increase risk of hemorrhage during and after the procedure. In a prospective study of patients undergoing upper endoscopy, cessation of antiplatelet therapy 10–14 days prior to procedure was associated with less procedural bleeding. While the use of aspirin can be continued, discontinuation of warfarin and clopidrogrel is recommended. The concomitant use of heparin is contingent on the risk for thromboembolism. Cardiac consultation is recommended for patients with severe cardiac conditions or at high risk for cardiac occurrences.
Consent
Consent should be obtained from the patient, or family members or representative if the patient is unable. The concept of tube feeding, including nutritional benefits and the burden of tube placement and feeding in addition to complications, must be acceptable to the patient and family or caregivers. Although the goal of enteral tube placement is to improve nutritional status and prolong survival, tube feeding may have major implications on quality of life.
Techniques
Percutaneous Endoscopic Gastrostomy
In principle, PEG can be placed by thre methods: pull, push, or introducer techniques. The original method, referred to as the “pull” technique, was first described in 1980 by Ponsky and Guaderer and is the most frequently used method today. Prior to the procedure, feeding is suspended for 8 h and systemic antibiotic prophylaxis is administered. Patients undergo conscious sedation, often with topical sprays for posterior pharyngeal topical anesthesia. The procedure begins with a diagnostic upper endoscopy. The gastroscope is introduced trans-orally under direct vision and advanced through the esophagus and into the stomach and duodenum. The stomach anatomy is evaluated and its contents are aspirated. The abdomen is insufflated to ensure that the stomach is in close apposition to the abdominal wall.
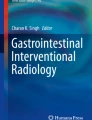
Next, an access site in the mid-epigastrium region, where the stomach and abdominal wall are in closest apposition, is chosen for PEG placement. This is marked by the area with maximal transillumination in the mid-epigastrium region and is ascertained with indentation of the anterior gastric wall by external digital pressure (Fig. 14.1). This position on the anterior gastric wall typically is the midway point between the greater and lesser curvatures, thus avoiding the associated vascular structures.

Transillumination of abdominal wall during initial needle access during PEG
At the site of gastric indentation, a small incision, approximately 0.5 cm in length is made. Under endoscopic visualization, the trocar and/or guidewire are inserted via puncture needle through the abdomen and grasped by the endoscope snare. As a unit, endoscope and snared guide wire are withdrawn through the mouth. The gastrostomy tube is connected to the guidewire from the mouth end and “pulled” back into the stomach via the guidewire from the abdominal end. An internal bumper is placed for fixation against the gastric wall, as well as an external bumper to secure the PEG tube in place (Fig. 14.2). An upper endoscopy is repeated to confirm positioning of the inner opening and bumper placement, as well as to confirm no bleeding from the gastrotomy site.

Endoscopic confirmation of internal bumper placement of PEG tube demonstrating absence of bleeding and opposition of both bumpers with the abdominal wall and gastric wall without ischemia
Push and Introducer Techniques
Modifications to the procedure or equipment have led to the development of other techniques for PEG. The Sack-Vine “push” method is similar to the “pull” technique, except that the tube is “pushed” through oral cavity and stomach with a more rigid introducer, until it emerges from the abdominal wall. Both “push” and “pull” technique have comparable success and complication rates [18, 19].
The Russell “introducer” method uses principles from insertion of central venous catheters and pacemaker wires. Using an introducer an after skin incision, the balloon-tube is inserted directly from the abdomen into the gastric lumen. With the catheter remaining, the introducer is removed and the balloon is inflated to affix against the stomach wall [16]. Proper placement of the catheter is confirmed endoscopically.
Safe Tract Technique
The safety of the site can be tested by performing the safe tract technique as described by Foutch et al. Using an aspirating, lidocaine-filled syringe, the needle is inserted into the stomach. If air bubble is simultaneously aspirated into the needle, then access to the stomach is successful and that a safe tract is achieved. If air or viscous fluid appears prior to entry to the stomach, then the small bowel or colon was punctured, in which case the tube insertion site should be re-selected. Some experts suggest that this step may be more favorable than transillumination. The effectiveness of transillumination has been challenged. Conversely, according to Foutch, no procedural failure occurred when a successful safety tract was achieved [20].
Percutaneous Endoscopic Gastrjejunostomy
In a PEG-J procedure, a jejunal extension tube is placed through a PEG tube. Like PEG, PEG-J uses a gastrostomy site Fig. 14.3. In the past, jejunal tubes were inserted through the gastrostomy site but this often resulted in tube migration when the endoscope was withdrawn. Recent techniques and kits use an over-the-wire guide to insert a thinner jejunostomy. The procedure begins similarly to PEG with placement of a PEG tube. From the PEG insertion site, a guidewire is inserted through the PEG tube and advanced into the small bowel with endoscopic assistance. Tube placement distal to the ligament of Treitz is recommended for jejunal feeding to prevent retrograde migration. The tube is also secured by endoscopically-placed clips. Then the endoscope is then withdrawn. With the guidewire remaining, the jejunal tube is then positioned over the guidewire through the PEG tube and into the jejunum.

Standard PEG kit
Percutaneous Endoscopic Jejunostomy
Jejunal feeding tubes can also be placed directly into the jejunum via direct PEJ. The PEJ procedure evolved as a modification of the PEG procedure. Patients are prepared similarly, with conscious sedation and prophylactic antibiotics. Beginning with upper endoscopy, a longer endoscope is passed into the intestine, distal to the ligament of Treitz. In the jejunum, an insertion site is identified with maximal transillumination and intrajejunal finger indentation.
Following standard skin preparation, the insertion needle is inserted percutaneously into the jejunum. The puncture should be performed quickly as peristalsis may interfere with transillumination and cause the intestine to slide. The needle is grasped with endoscope forceps to stabilize the jejunal segment and facilitate subsequent insertion of trocar and thread. The remainder of the procedure proceeds similar to the pull-PEG technique. The thread is snared endoscopically and withdrawn from the mouth. The jejunal tube is attached to the guidewire from the oral end and pulled into the jejunum from the insertion site. PEJ tube is secured with a bumper and proper position is confirmed by repeat endoscopy.
Laparoscopic Jejunostomy
There are two methods described to place jejunostomy tubes laparoscopically using a suturing technique or a T-fastener facilitated technique. After induction of general anesthesia and routine prophylactic antibiotics, pneumoperitoneum is obtained. In the laparoscopic technique, additional working ports are typically placed in the right lower quadrant and epigastrium. The jejunostomy tube insertion site is selected 10–30 cm distal to the ligament of Treitz and three nonabsorbable seromuscular sutures are used to adhere the antimesenteric side of the jejunum to the abdominal wall using the surgeon’s preferred laparoscopic knot tying technique. Under laparoscopic visualization, the lumen is accessed by the 12Fr venous introducer kit. Using an adaptation of the Russell percutaneous technique, the 10Fr jejunostomy tube is inserted to the bowel and placement is confirmed with direct visualization or a fluoroscopic contrast injection study.
The T-fasteners technique is similar to that described for gastrostomy tube placement. With this technique, working ports are placed in the right lower and right upper quadrants after pneumoperitoneum is achieved. The jejunum is insufflated with air through the nasogastric tube. Laparoscopic graspers position the bowel to the abdominal wall and four T-fasteners are inserted to the antimesenteric border of the jejunum in a diamond pattern. The jejunostomy tube is inserted and placement is confirmed in the same manner described above. At the level of the skin, the fasteners are tightened, which secures the jejunum to the abdominal wall. After 2 weeks, the sutures may be cut and the T-pieces pass in the stool [21].
Complications
The evolution of procedural techniques and equipment have improved outcomes of PEG, with an overall success rate of 95–100% [22,23,24]. Failure is often attributed to improper placement of the tube due to insufficient transillumination. Procedural and 30-day mortality associated with PEG placement are low (0–2% and 1.5–2.1%, respectively) [25,26,27]. Up to 40% of patients develop minor complications, and 3–4% experience major complications that require hospitalization and/or surgical intervention. However, much of the complications that develop are usually attributed to underlying co-morbidities and improper patient selection, rather than the procedure itself [18, 28,29,30]. PEG tubes can last as long as 1–2 years before requiring replacement due to tube degradation [18].
The success rate of PEG-J is approximately 93%. PEG-J tubes have a mean functional duration of 55 days in adults and 39 days in children. Re-intervention is common due to tube malfunction, such as clogging and migration. Conversely, PEJ uses a larger tube that is anchored directly to the intestine. The functional duration of PEJ tubes is longer, 113 days. PEJ is technically more difficult but success rates remain acceptable at 72–88% [31].
To ensure successful outcomes, three safety tenets have been postulated. Although intended for PEG, these may also apply to PEG-J and PEJ. These steps include: (1) endoscopic gastric distention via insufflation, (2) endoscopically visible finger-pressure indentation, and (3) transillumination. Adherence to these steps enables successful tube placement and decreases procedural complications. These techniques promote close apposition of the stomach to the abdominal wall, with no other organs interposed, and puncture of the intended organ. Performing the safe tract technique has also been shown to facilitate success of procedure.
Injury to Internal Organs
Injury to internal organs can occur from improper placement of enteral tube. Over distention of the stomach and small bowel can cause displacement of transverse colon and increase risk of injury. Injury to the small bowel is less likely due to protection by the greater omentum. However, patients who have had prior abdominal surgery may cause adhesion of the small bowel into the upper abdomen. Injury to the liver is also unusual but has been reported in a few patients. Most cases are rare but depending on the organ or severity of injury, conservative management with careful observation may be sufficient. Hemodynamically stable patients without signs of sepsis can be managed non-operatively. Conversely, colonic injury with peritonitis or liver laceration with intraperitoneal bleeding may require surgery. To avoid injury to internal organs, the safety tenets described previously should be employed for successful insertion of enteral tube. The safe tract technique and adjunctive abdominal imaging, such as ultrasound or CT, may also facilitate insertion and ensure proper placement of tube [15].
Fistula
Fistulas may occur as a result of penetration or misplacement of PEG tube into the colon, small bowel or percutaneously to the atmosphere. Fistulas are rare but can be a potentially serious complication. Many patients remain asymptomatic for months, thus the diagnosis is often delayed [32, 33]. Factors that could lead to fistula include insufficient gastric insufflation and excessive adhesions, often from the previous laparotomy. Up to 45% of colocutaneous fistulae after attempted PEG are observed in patients with prior abdominal history [32]. If there is no leakage, fistulas can be managed conservatively with removal of the PEG tube to allow spontaneous closure. In the presence of peritonitis, abscess, or leakage, operative intervention, including exploration and colonic repair or resection, may be required [34].
Tube misplacement can be minimized with adequate insufflation and choosing the proper PEG tube insertion site carefully. Transillumination, identification of digital pressure, and the safe tract technique endoscopically ensure close apposition of stomach to abdominal wall without interposition of colon or small bowel.
Additionally, chronic gastrocutaneous fistulas following removal of PEGs present with an incidence of 5.7% as noted by Currais et al. [35]. Medical treatment options include PPI, prokinetics, and antibiotics for local wound infections. Currais et al. noted clinical success in 63.2% of patients who underwent medical treatment. Morrell et al. described a success rate of 60% closure in upper gastrointestinal tract fistula’s utilizing over the scope clip application [36]. Surgical intervention for closure of a chronic fistula is indicated when both medical and endoscopic modalities have failed [35, 36].
Volvulus
Gastric and small bowel volvulus are rare complications of PEG and PEJ. Gastric volvulus is more commonly observed in children as the ligamentous and omental attachments of the stomach may be more mobile. A case report has described a scenario of incorrect insertion of a PEG into the the posterior gastric wall [37]. Small bowel volvulus after PEJ has also been reported and attributed to internal hernias, adhesions, or bowel motility disorders. Additionally, the single site of attachment of the tube to the abdominal wall may predispose direct PEJ to torsion, in contrast to surgically placed jejunostomy tubes which are typically anchored at multiple sites to prevent rotation. Detorsion of volvulus is performed surgically. Volvulus can be prevented by careful placement of the enterestomy tube on the anterior gastric wall and addressing predisposing factors [38, 39].
Metastasis at PEG Site
Abdominal wall metastasis, typically from head and neck carcinoma, is a devastating complication occurring in <1% of patients. Cases of tumor have been reported with the “pull” method and overall have a poor prognosis. In patients with oropharyngeal or esophageal malignancies, the “introducer” technique, which does not involve contact of catheter or guidewire with the mouth or esophagus, may be a safer technique of choice [40]. Alternatively, a surgical gastrostomy or jejunostomy may be placed, or PEG may be withheld until surgical removal of cancer.
Aspiration and Pneumonia
Aspiration is a common concern associated with enteral feeding. Its incidence ranges from 0.3% to 18% after PEG or PEJ and is likely correlated to the patient’s underlying medical conditions [21, 41,42,43]. Aspiration can range from minor to severe and may result in pneumonia and sepsis, if unresolved. Aspiration typically presents weeks after the procedure, but few reports showed occurrence during the procedure. Aspiration is common in patients with neurologic impairments, such as stroke or brain injury, or gastrointestinal motility disorder, such as gastroparesis. Jejunal feeding via PEJ or jejunostomy is recommended for patients at high risk for aspiration. Patients should be assessed preoperatively in order to perform the correct method for enteral nutrition. Patients with PEG recurrent aspiration can be converted to PEG-J.
Necrotizing Fasciitis
Necrotizing fasciitis is a rare but potentially fatal complication of PEG [44]. Necrotizing fasciitis can occurr in patients who have tube displacement and/or leakage [45]. Excessive traction and pressure on PEG tubes leading to ulceration or infection can also increase the likelihood for progression to necrotizing fasciitis. Other risk factors include diabetes, wound infections, malnutrition, and impaired immunity. Allowing 3 cm space between PEG bolster and abdomen may decrease risk for wound infection, peristomal drainage, and necrotizing fasciitis, as observed in one study [15, 46].
Buried Bumper Syndrome
Buried bumper syndrome is a rare complication, in which the bumper migrates and lodges in the gastric wall or gastric lumen. Its incidence is 1.9% and presents after at least 4 months of PEG procedure. BBS is mainly caused by excessive traction between the internal and external bumper, but can also occur due to malnutrition, poor wound healing, or a stiff internal bumper. BBS is diagnosed by inability to infuse feed through tube, leakage, and abdominal pain, and is confirmed with endoscopy. Once diagnosed, the buried bumper must be removed in order to prevent further complications and death.
To prevent BBS, additional space (approximately 1.5 cm) should be allowed between external bumper and skin. Mobilizing and loosening PEG tube daily could reduce mucosal overgrowth of the inner bumper. Patients with balloon-assisted PEG introducer devices have been found to have a lower incidence of BBS compared to those with traditional bumpered- PEG devices.
Peristomal Infection
Peristomal wound infections are the most common complication after PEG, with an incidence ranging from 4–30%, depending on definitions [47]. Wound infections are often minor and most resolve with conservative treatment, including local wound care and administration of antibiotics. Preprocedural, prophylactic antibiotics should be given, unless the patient is already taking broad-spectrum antibiotics prior to the procedure. In a pooled analysis of 13 randomized trials, preoperative administration of systemic antibiotics reduced the incidence of peristomal infection (OR = 0.36) [48]. Cephalosporin or penicillin-based antibiotics were similarly effective, but one study demonstrated that co-amoxiclav was associated with less MRSA infections [49]. Nonetheless, the emergence of Methicillin-resistant Staphylococcus aureus (MRSA) infections indicates decontamination of oral and nasally-delivered preparations and equipment. Postoperatively, regular skin and stomal care are also important in preventing local infections.
Gastrointestinal Bleeding and Ulceration
The incidence of acute bleeding after PEG tube placement is 1–2.5%. Acute bleeding usually results from direct injury to gastroepiploic arteries. Tightening internal and external bolsters may stop bleeding, however compression should be released within 48 h to prevent necrosis or ulceration. Alternatively, delayed bleeding can occur due to esophagitis, gastric pressure ulcer, or the buried bumper syndrome. Esophagitis is the most common cause of gastrointestinal bleeding, occurring in up to 39% of patients undergoing PEG placement. Studies demonstrate that PPIs may prevent and treat bleeding associated with esophagitis. Additionally, warfarin or clopidrogrel use should be temporarily discontinued when appropriate [50].
Pressure necrosis of the gastric mucosa by the internal bolster can cause ulceration of the anterior gastric wall. Pressure ulcers can be prevented by avoidance of excessive traction or tension by the internal bolster. Ulceration in the posterior gastric wall is more commonly attributed to mechanical injury from long protruding gastrostomy tubes or tall internal bumpers [51]. Ulceration from PEG tubes is treated by replacement of PEG tube at a different location or using a small internal bumper. H2 receptors may not provide protection from development of ulcers.
Leakage
Peristomal leakage is common but multifactorial. Its occurrence has been reported from excessive cleansing with hydrogen peroxide, lack of tube stabilization, infection, and gastric hypersecretion. Patients with comorbidities associated with poor wound healing are also at increased risk for peristomal leakage. Peristomal leakage is prevented and treated by management of contributing factors and examining securement of the tube and bolsters. Application of zinc-containing barrier creams may be beneficial to limit skin excoriation. If leakage persists, tube be removed and replaced after 4–6 days. Larger PEG tubes should not be inserted to avoid further injury and subsequent dilation of the tract.
Dislodgement and Inadvertent Removal
Incidental PEG dislodgement is a significant clinical and financial burden on health care systems [52] with an incidence of 1.6–4.4% [21, 53], and can be serious if a mature tract has not formed with resultant peritonitis. The maturation period of a PEG tract is 7–10 days but may be delayed to 3–4 weeks in patients with compromised healing. Immediate detection of removal allows for replacement of PEG tube at or near the original site. However, if detection is delayed in an immature site, the PEG procedure may need to be repeated with the administration of broad-spectrum antibiotics. After the maturation of the stoma, the tube can be replaced at the bedside without endoscopy. Once a PEG tube is removed, spontaneous closure of the PEG tract typically occurs rapidly. Temporary placement of PEG tract dilators or Foley tubes may prevent tract closure.
Circumstances leading to inadvertent removal should be corrected to prevent a recurrence. In general, internal bumpers anchor the tube and prevent dislodgement. The optimal placement of bumpers should secure the tube while allowing enough distance to prevent necrosis or ulceration. Steri-strips or abdominal binders may also be beneficial. Use of a shorter tube (<18 cm) may prevent the tube from getting caught on other objects and decrease pulling by patients, especially in the setting of neurologic disorders.
Gastrointestinal Obstruction
In rare cases, dislocation of internal bolster or migration of the PEG tube into the pylorus or duodenum can cause obstruction. This complication has been observed in both children and adults and has a higher occurrence with Foley-type peg tubes. Patients with gastric outlet obstruction experience abdominal cramping and vomiting and confirmed by an upper gastrointestinal study. Treatment involves withdrawal of dislocated tube or retrieval of bumpers. Gastric outlet obstruction can be avoided by securement of PEG tubes with an external bolster, placed 1–2 cm space from the skin. In PEJ, internal bumpers <2 cm should be utilized to prevent luminal obstruction.
Clogged PEG Tube
Clogging of enteral tubes is a common minor complication of PEG due to thick feed or undissolved medications. Clogging of PEG-J tubes may also be mechanical due to kinking. To prevent this tube malfunction, the use of bulking agents should be minimized, and medications should be dissolved. Clogged tubes can be prevented and cleared by frequent water irrigation. Some studies suggest the beneficial effects of pancreatic enzymes.
Pneumoperitoneum
Pneumoperitoneum is reported in up to 18–50% of cases [54, 55]. Pneumoperitoneum related to gas insufflation or needle puncture is usually benign and self-resolving. Intervention is not warranted unless when there is a clinical concern of worsening of intra-abdominal air, or presence of peritonitis, portal and/or mesenteric venous gas, systemic inflammatory response, and/or sepsis [56]. Symptoms persisting for >72 h may suggest the presence of a more serious complication, such as bowel injury.
Removal and Replacement of PEG
PEG tubes should be removed when it is no longer needed. The resultant gastrocutaneous fistula typically closes spontaneously within 24–72 h. Occasionally, surgical or endoscopic closure of gastrocutaneous fistula is needed, especially in children. After 2–3 weeks, the fistula tract is well epithelialized. If there is inadvertent tube removal prior to this, efforts should be made to maintain the tract to spare the patient an additional procedure. If the endoscopy unit cannot be easily accessed or replacement tubes are not readily available, a Foley catheter with an inflated balloon is a temporizing measure to maintain the tract [57].
Conclusion
The percutaneous endoscopic approach has become a widely accepted modality for enteral access. PEG, PEG-J, and PEJ have numerous applications and have been demonstrated to improve the nutritional and disease status of select chronically ill patients. Success rates for all three procedures are high, and overall procedural morbidity and mortality are low. The evolution of techniques and equipment has continued to improve patient outcomes since the first introduction of PEG.
Abbreviations
- PEG:
-
Percutaneous endoscopic gastrostomy
- PEG-J:
-
Percutaneous endoscopic gastrostomy-jejunostomy
- PEJ:
-
Percutaneous endoscopic jejunostomy
References
Ponsky JL, Gauderer MWL. Percutaneous endoscopic gastrostomy: a nonoperative technique for feeding gastrostomy. Gastrointest Endosc. 1981;27:9–11.
El-Matary W. Percutaneous endoscopic gastrostomy in children. Can J Gastroenterol. 2008;22:993–8.
Grant JP. Comparison of percutaneous endoscopic gastrostomy with Stamm gastrostomy. Ann Surg. 1988;207:598–603.
Mitchell SL, Teno JM, Kiely DK, Shaffer ML, Jones RN, Prigerson HG, et al. The clinical course of advanced dementia. N Engl J Med. 2009;361:1529–38.
Broadley S, Croser D, Cottrell J, Creevy M, Teo E, Yiu D, et al. Predictors of prolonged dysphagia following acute stroke. J Clin Neurosci. 2003;10:300–5.
FOOD Trial Collaboration. Poor nutritional status on admission predicts poor outcomes after stroke: observational data from the FOOD trial. Stroke. 2003;34:1450–6.
Dennis MS, Lewis SC, Warlow C, FOOD Trial Collaboration. Effect of timing and method of enteral tube feeding for dysphagic stroke patients (FOOD): a multicentre randomised controlled trial. Lancet. 2005;365:764–72.
Dharmarajan T. Percutaneous endoscopic gastrostomy and outcome in dementia. Am J Gastroenterol. 2001;96:2556–63.
Sampson EL, Candy B, Jones L. Enteral tube feeding for older people with advanced dementia. Cochrane Database Syst Rev. 2009;2009(2):CD007209. https://doi.org/10.1002/14651858.CD007209.pub2.
Akkersdijk WL, Roukema JA, van der Werken C. Percutaneous endoscopic gastrostomy for patients with severe cerebral injury. Injury. 1998;29:11–4.
Shepherd RW, Holt TL, Thomas BJ, Kay L, Isles A, Francis PJ, et al. Nutritional rehabilitation in cystic fibrosis: controlled studies of effects on nutritional growth retardation, body protein turnover, and course of pulmonary disease. J Pediatr. 1986;109:788–94.
Zhu Y, Shi L, Tang H, Tao G. Current considerations in direct percutaneous endoscopic jejunostomy. Can J Gastroenterol. 2012;26:92–6.
Bender JS. Percutaneous endoscopic gastrostomy placement in the morbidly obese. Gastrointest Endosc. 1992;38:97–8.
Wiggins TF, Garrow DA, DeLegge MH. Evaluation of percutaneous endoscopic feeding tube placement in obese patients. Nutr Clin Pract Off Publ Am Soc Parenter Enter Nutr. 2009;24:723–7.
Schrag SP, Sharma R, Jaik NP, Seamon MJ, Lukaszczyk JJ, Martin ND, et al. Complications related to percutaneous endoscopic gastrostomy (PEG) tubes. A comprehensive clinical review. J Gastrointest Liver Dis JGLD. 2007;16:407–18.
Jafri NS, Mahid SS, Minor KS, Idstein SR, Hornung CA, Galandiuk S. Meta-analysis: antibiotic prophylaxis to prevent peristomal infection following percutaneous endoscopic gastrostomy. Aliment Pharmacol Ther. 2007;25:647–56.
McCulloch A, Roy O, Massey D, Hedges R, Skerratt S, Wilson N, Woodward J. Nasal unsedated seated percutaneous endoscopic gastrostomy (nuPEG): a safe and effective technique for percutaneous endoscopic gastrostomy placement in high-risk candidates. Frontline Gastroenterol. 2018;9(2):105–9. https://doi.org/10.1136/flgastro-2017-100894. Epub 2017 Dec 5. PMID: 29588837; PMCID: PMC5868436
Kozarek RA, Ball TJ, Ryan JA. When push comes to shove: a comparison between two methods of percutaneous endoscopic gastrostomy. Am J Gastroenterol. 1986;81:642–6.
Hogan RB, DeMarco DC, Hamilton JK, Walker CO, Polter DE. Percutaneous endoscopic gastrostomy—to push or pull. Gastrointest Endosc. 1986;32:253–8.
Foutch PG, Talbert GA, Waring JP, Sanowski RA. Percutaneous endoscopic gastrostomy in patients with prior abdominal surgery: virtues of the safe tract. Am J Gastroenterol. 1988;83:147–50.
Jones DB, Mathiel SK, Schneider BE. Atlas of minimally invasive surgery. 1st ed. Woodbury, CT: Cine-Med, Inc; 2006. p. 276–97.
Kwon RS, Banerjee S, Desilets D, Diehl DL, Farraye FA, Kaul V, et al. Enteral nutrition access devices. Gastrointest Endosc. 2010;72:236–48.
Larson DE, Burton DD, Schroeder KW, Dimagno EP. Percutaneous endoscopic gastrostomy: indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology. 1987;93:48–52.
Taylor CA, Larson DE, Ballard DJ, Bergstrom LR, Silverstein MD, Zinsmeister AR, et al. Predictors of outcome after percutaneous endoscopic gastrostomy: a community-based study. Mayo Clin Proc. 1992;67:1042–9.
Loser C, Wolters S, Folsch UR. Enteral long-term nutrition via percutaneous endoscopic gastrostomy (PEG) in 210 patients a four-year prospective study. Dig Dis Sci. 1998;43:2549–57.
Kohli H, Bloch R. Percutaneous endoscopic gastrostomy: a community hospital experience. Am Surg. 1995;61:191–4.
Davis JB Jr, Bowden TA Jr, Rives DA. Percutaneous endoscopic gastrostomy. Do surgeons and gastroenterologists get the same results? Am Surg. 1990;56:47–51.
Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505–24.
Longcroft-Wheaton G, Marden P, Colleypriest B, Gavin D, Taylor G, Farrant M. Understanding why patients die after gastrostomy tube insertion: a retrospective analysis of mortality. J Parenter Enter Nutr. 2009;33:375–9.
DiSario JA, Baskin WN, Brown RD, DeLegge MH, Fang JC, Ginsberg GG, et al. Endoscopic approaches to enteral nutritional support. Gastrointest Endosc. 2002;55:901–8.
Rumalla A, Baron TH. Results of direct percutaneous endoscopic Jejunostomy, an alternative method for providing Jejunal feeding. Mayo Clin Proc. 2000;75:807–10.
Yamazaki T, Sakai Y, Hatakeyama K, Hoshiyama Y. Colocutaneous fistula after percutaneous endoscopic gastrostomy in a remnant stomach. Surg Endosc. 1999;13:280–2.
Patwardhan N, McHugh K, Drake D, Spitz L. Gastroenteric fistula complicating percutaneous endoscopic gastrostomy. J Pediatr Surg. 2004;39:561–4.
Kim HS, Lee DK, Baik SK, Kwon SO. Endoscopic management of Colocutaneous Fistula after percutaneous endoscopic gastrostomy. Endoscopy. 2002;34:430.
Currais P, Faias S, Francisco F, Sousa L, Gramacho J, Pereira AD. Gastrocutaneous fistulas after PEG removal in adult cancer patients: frequency and treatment options. Surg Endosc. 2021 May;35(5):2211–6. https://doi.org/10.1007/s00464-020-07627-z.
Morrell DJ, Winder JS, Johri A, Docimo S, Juza RM, Witte SR, Alli VV, Pauli EM. Over-the-scope clip management of non-acute, full-thickness gastrointestinal defects. Surg Endosc. 2020 Jun;34(6):2690–702. https://doi.org/10.1007/s00464-019-07030-3.
Sookpotarom P, Vejchapipat P, Chongsrisawat V, Mahayosnond A. Gastric volvulus caused by percutaneous endoscopic gastrostomy: a case report. J Pediatr Surg. 2005;40:e21–3.
Freeman C, Delegge MH. Small bowel endoscopic enteral access. Curr Opin Gastroenterol. 2009;25:155–9.
Potter MB, Bowers SB, Pruitt A. Internal hernia with small bowel volvulus in a patient with altered gut motility: a complication of direct percutaneous endoscopic jejunostomy. Dig Dis Sci. 2007;52:1910–3.
Sinclair J, Scolapio J, Stark M, Hinder R. Metastasis of head and neck carcinoma to the site of percutaneous endoscopic gastrostomy: case report and literature review. J Parenter Enter Nutr. 2001;25:282–5.
James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy feeding in patients with dysphagic stroke. Age Ageing. 1998;27:671–6.
Grant JP. Percutaneous endoscopic gastrostomy. Initial placement by single endoscopic technique and long-term follow-up. Ann Surg. 1993;217:168–74.
Kadakia SC, Sullivan HO, Starnes E. Percutaneous endoscopic gastrostomy or jejunostomy and the incidence of aspiration in 79 patients. Am J Surg. 1992;164:114–8.
Greif JM, Ragland JJ, Gage Ochsner M, Riding R. Fatal necrotizing fasciitis complicating percutaneous endoscopic gastrostomy. Gastrointest Endosc. 1986;32:292–4.
Cave DR, Robinson WR, Brotschi EA. Necrotizing fasciitis following percutaneous endoscopic gastrostomy. Gastrointest Endosc. 1986;32:294–6.
Chung RS, Schertzer M. Pathogenesis of complications of percutaneous endoscopic gastrostomy. A lesson in surgical principles. Am Surg. 1990;56:134–7.
Safadi BY, Marks JM, Ponsky JL. Percutaneous endoscopic gastrostomy. Gastrointest Endosc Clin N Am. 1998;8:551–68.
Lipp A, Lusardi G. Systemic antimicrobial prophylaxis for percutaneous endoscopic gastrostomy. Cochrane Database Syst Rev. 2013;11:CD005571.
Gurusamy KS, Koti R, Wilson P, Davidson BR. Antibiotic prophylaxis for the prevention of methicillin-resistant Staphylococcus aureus (MRSA) related complications in surgical patients. Cochrane Database Syst Rev. 2013;19(8):CD010268. https://doi.org/10.1002/14651858.CD010268.pub2.
Anderson MA, Ben-Menachem T, Gan SI, Appalaneni V, Banerjee S, Cash BD, et al. Management of antithrombotic agents for endoscopic procedures. Gastrointest Endosc. 2009;70:1060–70.
Kanie J, Akatsu H, Suzuki Y, Shimokata H, Iguchi A. Mechanism of the development of gastric ulcer after percutaneous endoscopic gastrostomy. Endoscopy. 2002;34:480–3.
Odom SR, Barone JE, Docimo S, Bull SM, Jorgensson D. Emergency department visits by demented patients with malfunctioning feeding tubes. Surg Endosc. 2003 Apr;17(4):651–3. https://doi.org/10.1007/s00464-002-8599-y.
Dwyer KM, Watts DD, Thurber JS, Benoit RS, Fakhry SM. Percutaneous endoscopic gastrostomy: the preferred method of elective feeding tube placement in trauma patients. J Trauma. 2002;52:26–32.
Wiesen AJ, Sideridis K, Fernandes A, Hines J, Indaram A, Weinstein L, et al. True incidence and clinical significance of pneumoperitoneum after PEG placement: a prospective study. Gastrointest Endosc. 2006;64:886–9.
Nazarian A, Cross W, Kowdley GC. Pneumoperitoneum after percutaneous endoscopic gastrostomy among adults in the intensive care unit: incidence, predictive factors, and clinical significance. Am Surg. 2012;78:591–4.
Wojtowycz M, Arata J, Micklos T, Miller F. CT findings after uncomplicated percutaneous gastrostomy. Am J Roentgenol. 1988;151:307–9.
Friginal-Ruiz A, Lucendo A, PhD MD. Percutaneous endoscopic gastrostomy: a practical overview on its indications, placement conditions, management, and nursing care. Gastroenterol Nurs. 2015;38(5):354–66. https://doi.org/10.1097/SGA.0000000000000150.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 SAGES
About this chapter

Cite this chapter
Ifuku, K., Tsuda, S. (2023). Enteral Access: Percutaneous Endoscopic Gastrostomy, Gastrostomy-Jejunostomy, and Jejunostomy. In: Kroh, M., Docimo Jr., S., El Djouzi, S., Shada, A., Reavis, K.M. (eds) The SAGES Manual Operating Through the Endoscope. Springer, Cham. https://doi.org/10.1007/978-3-031-21044-0_14
Download citation
DOI: https://doi.org/10.1007/978-3-031-21044-0_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-21043-3
Online ISBN: 978-3-031-21044-0
eBook Packages: MedicineMedicine (R0)