
Abstract
Geriatric proximal femur fractures are some of the most commonly encountered injuries. These fractures encompass include femoral neck fractures, intertrochanteric hip fractures, subtrochanteric femur fractures. Understanding the fracture pattern and the patient’s medical comorbidities are crucial to successfully treat these injuries. As the majority of these fractures are operative, surgical management requires a multidisciplinary approach in the perioperative period to optimize long-term outcomes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Hip fracture
- Femoral neck fracture
- Intertrochanteric hip fracture
- Subtrochanteric femur fracture
- Intramedullary nailing
- Sliding hip screw (SHS)
- Hemiarthroplasty
- Total hip arthroplasty (THA)
1 Introduction to Geriatric Proximal Femur Fractures
Proximal femur fractures are significant injuries that affect the geriatric population from a medical and a financial standpoint. They remain one of the most common injuries in this age group and are expected to rise in frequency over the next few decades [1]. By 2025, the number of hip fractures worldwide is to rise to 2.6 million and 6.25 million by 2050 [2, 3]. Along with an increase in the number of these fractures, they represent a large financial burden in the USA with annual treatment costs at approximately $6 billion USD [4].
Proximal femur fractures can be classified as either intracapsular such as femoral neck fractures or extracapsular such as pertrochanteric or subtrochanteric femur fractures. Treatment of these injuries in this patient population is challenging due to poor bone quality, medical comorbidities, and patient frailty. The overall goal for any orthopedic intervention is to return patients to their pre-injury level of function; however, this may be impacted by the patient’s reliance on assistive devices, chronic systemic diseases, perioperative cognitive disorders, and the development of any postoperative complications. The hospital mortality rate is around 15% with 1-year mortality rate at around 30% [5]. This risk is increased with dependency, loss of walking capacity, preexisting cognitive decline, increased ASA classification, and severity of medical comorbidities [6]. Patients with higher ISS scores were noted to have higher mortality rates than previously quoted, and these rates increase with patient age [7, 8]. Risk stratified scores have now been developed in geriatric trauma patients to identify patients with higher mortality rates [9, 10].
Ultimately, patients fall into one of three categories: those who are independent ambulators without significant medical comorbidities, frail patients with multiple medical comorbidities who can perform activities of daily living but demonstrate difficulty with instrumental activities of daily living, and lastly dependent patients that require daily assistance and live in an institution [11]. Understanding and identifying patients’ pre-injury level of function and comorbid status can lead to improved perioperative management and decrease the risk of postoperative complications. While the ultimate goal following operative management of these injuries is to restore pre-injury level of function, the elderly patient’s ability to cope with the metabolic and physiologic demands from these injuries may reduce their level of function and independence [12].
2 Radiographic Workup
In order to fully evaluate the fracture characteristic, the authors recommend an AP pelvis radiograph with dedicated AP and lateral views of the affected hip and femur. A traction internal rotation view of the ipsilateral hip can assist with defining fracture pattern further [13]. The view is obtained by shooting an AP hip radiograph as the physician pulls traction at the ankle and internally rotates the hip 15 degrees (based on the average amount of anteversion seen in the adult femoral neck). Care should be taken to avoid shearing of the skin in the lower extremity while performing this maneuver.
It is important to assess the patient’s native femoral neck coronal alignment and as well as the presence of any excessive femoral bow on either view [14]. A cross-table lateral view of the injured hip is recommended over a frog lateral as this may not only mitigates discomfort but also prevents a non-displaced fracture from displacing.
In the setting of hip pain and difficulty/ inability to ambulate, patients may have sustained an occult femoral neck or intertrochanteric fracture. Patients may complain of pain slight pain in the groin, thigh or referred pain along the medial side of the knee. These fractures may not be recognized on initial radiographs and failure to diagnose them may lead to displacement following weight-bearing. Advanced imaging such as bone scans, CT, or MRI may be required for diagnosis. MRI has the highest accuracy, is simple to perform, and can diagnose injuries more acutely [15, 16]. Having adequate and appropriate radiographic information will allow the treating surgeon to not only fully understand the fracture pattern, but also choose the appropriate surgical technique for treatment.
3 Intracapsular Fractures (Femoral Neck Fractures)
Femoral neck fractures are uncommon in young patients and are usually the result of high-energy trauma. It is generally considered that femoral neck fractures in the geriatric population are “pathologic” secondary to osteoporosis/osteomalacia. Osteoporosis/osteomalacia in this region causes bone to lose its normal trabecular architecture [17]. As a consequence, there can be an increased amount of posterior comminution associated with fractures and this has been postulated to increase rates of failure of internal fixation [18]. Swinontkowski noted that the critical element in the stability of fixation of displaced femoral neck fractures is the quality of the bone [19].
The Garden classification is commonly used to describe femoral neck fractures based on the displacement of the fracture fragments. Garden 1 corresponds with a valgus impacted fracture, Garden 2 corresponds with a non-displaced fracture, Garden 3 and 4 corresponds to complete fractures with the Garden 4 having 100% displacement. Other descriptive methods include the direction of the fracture angle as well as the anatomic location of the fracture. While the Garden classification has poor interobserver reliability, it can be used to communicate whether or not the fractures are valgus impacted/minimally displaced or completely displaced [20]. Most have gone to using displaced and non-displaced as terminology. Despite this, Garden’s original classification continues to be utilized to guide treatment.
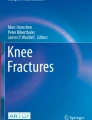
Fixation options range from parallel cannulated screws (2, 3, or 4), sliding hip screw (SHS) construct, hemiarthroplasty, and total hip arthroplasty (THA) depending upon the degree of fracture displacement. Arthroplasty options may be either cemented or press-fit depending on surgeon preference. Ultimately the treatment question becomes whether to fix the femoral neck fracture or perform an arthroplasty procedure [21]. Garden I and II Fractures (non-displaced) are typically treated with fixation in situ with cannulated screws (Fig. 28.1a–d). The inverted triangle position is the most common configuration; however, is conflicting evidence about number of pins and also the configuration of pin [22].

(a) AP radiograph demonstrates a valgus impacted fracture of the femoral neck (Sacks). (b) Lateral radiograph demonstrates a valgus impacted fracture of the femoral neck, note the lack of posterior comminution. (c) Postoperative AP radiograph of an inverted triangle cannulated screw configuration. (d) Postoperative Lateral radiograph of an inverted triangle cannulated screw configuration
4 Internal Fixation of Femoral Neck Fractures
Placement of cannulated screws can be performed on either a radiolucent flat top table or a fracture (traction) table; the authors prefer to use a fracture table as it can apply traction if needed and also holds the leg in a constant position negating the use of an assistant and allows for changes in fluoroscopy position without rotation of the affected leg (Fig. 28.2). It is important to screen the fluoroscopy after positioning to confirm that the fracture has not displaced in the interim. A small open incision is made laterally and the IT band is incised inferior to the vastus ridge for all wires or a percutaneous nick can be made for each wire separately. Guidewires are then introduced into the femoral neck using fluoroscopy. For the inverted triangle configuration, one guidewire is placed central and inferior along the calcar. The remaining two are then placed in a posterior superior and anterior superior position. The goal is to obtain spread; however, caution must be taken to ensure that the posterior superior screw which may look intraosseous on fluoroscopy could potentially be “in out in”. While the clinical implication of this is unknown, this screw is in close proximity to the vascular supply to the femoral head [23]. If a fourth screw is to be added, it should be placed posteriorly to support posterior comminution; typically, this is done for displaced fractures that require a reduction [24]. The most inferior screw should not be placed distal to the level of the lesser trochanter as this may create a stress riser in the subtrochanteric region [25].

Fracture table set up
If two cannulated screws are to be used, one screw should be placed in the inferior/central along the calcar and the second screw placed more proximal in the femoral neck and in the central or posterior segment on the lateral position [26].
While used more often in younger patients, a SHS construct can be used for femoral neck fractures in the elderly. This implant is more than often used for basicervical fracture patterns. A de-rotational screw placed superior and parallel to the lag screw could be used to prevent rotation of the [27] neck during insertion of the large central lag screw [28] (Fig. 28.3a–c). The FAITH trial randomized large cohorts of patients to SHS or cannulated screws in both displaced and non-displaced femoral neck fractures [27]. Patients were included only if the surgeon felt that fixation was a better option than replacement. Overall, there was no significant difference in nonunion, implant failures, and infection. The reoperation rate was noted to be 14% for all causes in this large multinational observational study [27].

(a) AP Pelvis radiograph of a basicervical fracture pattern. (b) AP radiograph of a SHS with de-rotational screw. (c) Lateral radiograph of a SHS with de-rotational screw
5 Hemiarthroplasty and Total Hip Arthroplasty for Displaced Femoral Neck Fractures
There is a defined rate of revision surgery that occurs following internal fixation of femoral neck fractures even if non-displaced. Hemiarthroplasty, while associated with greater intraoperative time, higher blood loss, and greater complication rate, has a significantly lower rate of revision surgery after internal fixation of displaced femoral neck fractures in the elderly [29].
The higher the amount of displacement, the higher the likely hood of nonunion and fixation failure in the elderly population [30, 31]. Arthroplasty options include unipolar or bipolar hemiarthroplasty or THA. Each of these stems may be cemented or press fit. The surgical approach for an arthroplasty procedure can be either an anterior approach, anterolateral, or posterolateral (Table 28.1). The choice of approach is ultimately based on surgeon comfort, with the anterior-based approaches having a lower dislocation rate due to preservation of the posterior capsular structures [32].
Hemiarthroplasty may be performed with either a bipolar or unipolar implant. A bipolar hemiarthroplasty has a dual articulation between the inner head and shell and the shell and the acetabulum. In comparison, a unipolar hemiarthroplasty has a single articulation between the shell and the acetabulum (Fig. 28.4). The theoretical advantage of this dual articulation is to reduce wear and decrease acetabular protrusion; however, studies have demonstrated that this dual articulation ceases to function over time and the stem behaves as a unipolar arthroplasty [33,34,35,36]. Due to this, the bipolar hemiarthroplasty may not be as cost-effective as a unipolar arthroplasty. While these implants are available in cemented and non-cemented designs, controversy regarding fixation strategy remains. In a large metanalysis by Parker et al., cemented prostheses were associated with less pain and improved mobility at 1 year [37]. Furthermore, other studies have demonstrated a lower risk of peri-prosthetic fracture with the use of a cemented implant [38]. Ultimately, if the patient has thick femoral cortices a press fit stem may be used; however, in the setting of most of these fractures, the patulous bone often suggests the use of a cemented stem [39]. The ultimate goal is to restore femoral neck offset, leg length, and adequately tension the hip abductors. Achieving these goals ensures a low rate of dislocation and restores hip mechanics [40]. Unlike, elective hip arthroplasty, restoration of leg lengths may be difficult because the neck cut is dictated by the fracture (Fig. 28.5a, b).

AP Radiograph of a bipolar hemiarthroplasty

(a) AP pelvis of displaced femoral neck fracture. (b) AP pelvis of unipolar hemiarthroplasty
While hemiarthroplasty performs well in the postoperative period; THA has been noted to have improved functional outcomes that surpass hemi-arthroplasty [41] (Fig. 28.6a). THA is associated with increased cost, a greater magnitude of surgery, increased blood loss, and also an increased dislocation rate in patients with a femoral neck fracture [42]. It does play a definitive role in patients who have eroded through the acetabulum with a hemiarthroplasty prosthesis, patients with antecedent symptomatic hip arthritis, and salvage after nonunion or AVN of the femoral head after internal fixation [43, 44]. It is now recommended to be used in patients who are highly active and would potentially survive greater than 10 years.

(a) AP pelvis of displaced femoral neck fracture. (b) AP pelvis of THA after a femoral neck fracture
Internal fixation should be used with caution in treating displaced fractures in this cohort of patients as there is a significant rate of requiring revision surgery, up to 30–40%. This procedure should be reserved for the Garden 1 and 2 fractures in this patient population. Specific age cutoffs to define the elderly do not exist and decisions should be made on a case-by-case basis. Hemiarthroplasty is a reliable and predicable procedure in the treatment of displaced femoral neck fractures; however, in patients with preexisting arthritis and highly active patients, a THA can be a cost-effective treatment with improved long-term outcomes [45, 46].
6 Pertrochanteric Femur Fracture
Pertrochanteric hip fractures are extracapsular and are located distal to the femoral neck between the greater and lesser trochanters. Patients with these injuries tend to be older and more frail than those with intracapsular hip fractures with mortality rates similar or slightly lower than femoral neck fractures [47, 48]. Due to their anatomical location, these fractures have an abundant vascular supply leading to fewer healing complications relative to intracapsular femoral neck fractures.
7 Determining Stability
While there are a number of classification systems used to describe these fractures, the AO/OTA classification has an acceptable method of both intra- and interobserver reliability [49]. Intertrochanteric fractures are all described as 31 due to anatomical location. They are further subdivided by A1, A2, and A3. A1 fractures are two-part fractures and are considered stable. A2 fractures are comminuted and unstable and A3 fractures include subtrochanteric extension as well as reverse obliquity patterns.
Determining stability is dependent on multiple variables. A1 fractures are considered stable as they can have interdigitation of the fracture site following fixation. A2 fractures are considered unstable as they are multi-fragmentary and have compromised the medial buttress (Fig. 28.7a–e). A3 fractures have subtrochanteric extension or reverse obliquity fracture patterns. Ultimately, since both posteromedial and lateral buttresses are lacking, they may behave like subtrochanteric fractures.


(a) AP hip radiograph of an unstable intertrochanteric femur fracture. (b) Lateral hip radiograph of an unstable intertrochanteric femur fracture. (c) AP radiograph of an intertrochanteric femur fracture with an incompetent lateral wall. (d) AP hip radiograph of an unstable intertrochanteric femur fracture treated with an IMN. (e). Lateral hip radiograph of an unstable intertrochanteric femur fracture treated with an IMN
An A2 subtype exists where the lateral cortex is incompetent and should be recognized. An intact lateral wall acts as a buttress to prevent excessive medialization and subsequent failure. Thickness of the lateral wall, measured 3 cm distal to the vastus ridge, should be greater than 20.5 mm if the surgeon plans on using a SHS device [50]. Lateral cortices thinner than this are prone to intraoperative fracture when reaming for the insertion of the lag screw in a SHS [51,52,53]. In summary, unstable fractures radiographically contain increasing number of parts, a reverse obliquity orientation, increasing degree of posterior medial comminution, and decreased thickness of the lateral cortical buttress under the vastus ridge.
This classification is not only useful for describing the injury but can also guide implant decision. These injuries are treated with either intramedullary fixation with a cephalomedullary implant (CMN) or extramedullary fixation with a SHS (Fig. 28.8a–d).

(a) AP hip radiograph of a stable intertrochanteric femur fracture. (b) Lateral hip radiograph of a stable intertrochanteric femur fracture. (c) AP hip radiograph of a stable intertrochanteric femur fracture treated with an SHS. (d) Lateral hip radiograph of a stable intertrochanteric femur fracture treated with a SHS
8 Surgical Management
The authors prefer to use a fracture (traction) table for the treatment of these injuries. The fracture table will provide sustained traction without the use of an assistant. Positioning on the fracture table is of utmost importance as improper positioning can hinder obtaining an adequate reduction. The perineal post can act as a lever pushing the fracture into varus. The operative site should be shifted away from the post with the buttock hanging off the side of the table. The good leg should be in a heel-to-toe position to prevent the ipsilateral hemipelvis from rotating toward the post while traction is being pulled. Attention to detail in during this process will mitigate positioning-related malreductions.
9 CMN Versus Sliding Hip Screw
There has been an increasing trend in the use of intramedullary nailing devices (Fig. 28.9a, b) in the preference to SHSs for the treatment of intertrochanteric hip fracture, despite robust quality evidence to support their use [54]. Fracture stability has been used as a surrogate to guide implant choice [55]. As discussed in the prior section, a stable fracture is mainly comprised of two parts that once reduced can compress against one another and is able to withstand the forces of a single leg stance after fixation [56].

(a) Short IMN. (b) Long IMN
With the more unstable fracture patterns, the implant must bear more load to avoid loss of reduction through collapse. Implant options for fixation of intertrochanteric fractures include SHS with or without a trochanteric stabilization plate, short intramedullary nails, and long intramedullary nails. Intramedullary nails offer the advantage of less soft tissue disruption at the fracture site, potentially less operative time, and increased biomechanical superiority, most notably in unstable fracture patterns [57,58,59]. However, despite this, a large number of randomized controlled trials have failed to demonstrate any differences in outcomes between SHSs and intramedullary devices [60, 61].
Caution should be taken in A2 fractures with a thin lateral wall with the use of a SHS construct. In a retrospective series of 214 patients, there was a significantly higher rate of reoperation (22%) with postoperative findings of a fractured lateral wall. Furthermore, lateral wall incompetency was radiographically identified in more unstable fracture patterns per the AO/OTA classification (palm JBJS 2007). Even with an adequate TAD and reduction, lateral wall incompetence could potentially lead to catastrophic failure with incorrect implant choice. If a SHS is to be used, studies have shown decreased failure rates with the addition of a trochanteric stabilization plate which can act as a lateral buttress [62].
Intramedullary fixation of these fractures does prevent excessive collapse as the nail acts as a lateral buttress and by doing so, has less femoral neck shortening, shorter leg length discrepancy, and medialization of the shaft [63, 64]. Femoral medialization and excessive collapse have been demonstrated to alter hip biomechanics which can theoretically impair mobility; however, the results from clinical studies regarding this are conflicting [65, 66]. Regardless of implant choice, it is imperative to have an exacting reduction and mitigate technical errors in implant technique.
10 Cephalomedullary Fixation
Both intramedullary and extramedullary implants have cephalomedullary fixation with either a helical blade, a single screw, or two screws. Appropriate cephalomedullary fixation ideally deep and central within the femoral head can often be measured with the Tip Apex Distance (TAD) [67]. It should be noted that the original paper describing TAD was done in SHS constructs. Failure of cephalomedullary fixation can be described as either “cut out” or “cut through” and is often related to either quality of reduction or inadequate tip apex distance rather than the implant used [68,69,70]. A tip apex distance of less than 25 mm will mitigate the chances of screw cutout. This has applied to both cephalomedullary nails as well as SHS constructs [71] (Fig. 28.10a, b).

(a) AP radiograph demonstrating cutout of a SHS construct. (b) AP radiograph demonstrating cutout of a CMN construct
The use of a helical blade design for fixation has been shown in cadaveric models to resist rotational and translational forces by compaction of cancellous bone [72] (Fig. 28.11a, b). Despite the biomechanical advantage, there is limited clinical data supporting the use of a blade versus a lag screw. Helical blades have been [73]associated with a phenomenon of “cut-through” in which there is medial perforation of the blade. It is recommended that the blade is not fully predrilled and the tip of the blade should be less than 10 mm from the joint surface [74, 75].

(a) AP radiograph demonstrating a helical blade fixation of an intertrochanteric hip fracture. (b) Lateral radiograph demonstrating a helical blade fixation of an intertrochanteric hip fracture
Lag screw fixation can consist of either a single or a double lag screw design. Single lag screw fixation while more commonly used is limited by a single point of fixation and can hence be subject to rotational instability [76]. Biomechanically, a dual lag screw design has been shown to have a higher load to failure, decreased varus collapse, and neck rotation [73, 77]. It is important to note that a dual lag screw design can be subject to the Z effect, in which the cephalic screw is subject to more stress under weight-bearing and as a result, the proximal screw advances into the nail while the distal screw toggles and backs out laterally ultimately leading to collapse and penetration proximally [78]. This has also been described in single lag screws as well. To mitigate the risk of the Z-effect while still maintaining rotational control, integrated sliding lag screw designs have been developed. However, a multicenter trial noted no difference in functional mobility, hip function, and patient satisfaction between a SHS and nailing system with an integrated sliding lag screw [62, 79]. A separate clinical study comparing nailing systems with a single lag screw compared with an integrated sliding lag screw demonstrated increased varus collapse and neck shortening in the single lag screw radiographically at 1 year postoperatively; however, since no patient or clinical outcomes were recorded, the overall effect of these radiographic changes are unknown [80].
11 Long Versus Short Nail
Currently, both short and long cephalomedullary nails are used in the treatment of intertrochanteric hip fractures. Advantages of using a short CMN include decreased operative time, blood loss, decreased implant cost, and distal locking performed through a targeting jig [76]. However, the theoretical disadvantage is that short nails do not span the entire bone in patients who are prone to falls and are already osteoporotic. The anatomic bow of the femoral shaft needs to be taken into consideration with the use of a long cephalomedullary nail and the radius of curvature (ROC) mismatch between the implant and the femur can lead to anterior cortical perforation/impingement [81]. This finding can lead to a significant stress riser in the distal femur in osteoporotic patients. Newer implant designs have focused on improving this design aspect, with more anatomic ROC’s.
Regardless of the theoretical risks and benefits of either implant, clinical studies have shown that both are viable options in the treatment of intertrochanteric femur fractures in the absence of subtrochanteric extension. Kleweno et al retrospectively analyzed 559 geriatric patients with intertrochanteric hip fractures treated with either a long or short CMN and noted no difference in the rates of revision surgery; however, the long CMN was associated with statistically significant longer operative time [82]. Hou et al noted higher blood loss and longer operative times with the use of a long nail. Ultimately, both groups had similar rates of intraoperative and postoperative complications and similar rates of union amongst all fracture types [83].
12 Implant-related Complications
Ultimately, two-part stable fractures treated with SHSs have minimal complication rates [84]. However, discussed in prior sections, patients with potentially unstable fractures or grossly unstable fractures can have failure rates of the SHS by over 15% [85]. Excluding improper surgical technique, the failure rates can be as low as 5% [86]. Failure occurs with progressive varus collapse of the femoral head leading to cutting out of the cephalomedullary screw. It important to recognize that the use of the SHS in unstable fractures despite proper surgical technique can have a greater amount of postoperative collapse compared to a cephalomedullary device [86]. While this collapse is not considered a failure of fixation and does not fall into screw “cut out”, it may alter hip biomechanics and gait quality most notably when collapse surpasses 2 CM [87].
Cephalomedullary nails due to biomechanical superiority have had an increased trend in usage. Original designs of cephalomedullary nails were fraught with postoperative femoral shaft fracture, which ranged anywhere from 5 to 15% [88,89,90]. After design modifications made to the proximal end of the cephalomedullary nails and increased surgeon familiarity, the number of peri-implant fractures decreased significantly [91]. In a large retrospective study of cephalomedullary nails for the treatment of intertrochanteric femur fractures, the overall reported rate of postoperative femoral shaft fractures was about 0.6%. Despite the theoretical risks of a short nail ending in a region of a stress riser, a sub-analysis in this cohort did not demonstrate any increased risk of a short versus long nail [92].
13 Value-Based Care Algorithm
As mentioned before, the increasing trend in using cephalomedullary fixation has not decreased the perioperative mortality and morbidity of these injuries nor has it demonstrated any superiority in functional outcomes [93, [94]. Intramedullary nail implants can be up to 100% more expensive than the SHSs and its increased use has raised concerns regarding cost [56]. Surgeon comfort with the implant, risk of failure, implant costs, as well as industry influence are the driving variables for implant choice. Swart et al noted by analyzing failure rates, the intramedullary nail was more cost-effective as the risk of SHS failure increased. Hence in the A1 fractures, the SHS was more cost-effective and in A3 fractures the intramedullary nail was more cost-effective. In A2 fractures, the SHS was more cost-effective 70% of the time; however, they noted that fixation failure rate was the major driver of cost [95]. Egol et al implemented an algorithm treating stable intertrochanteric fractures with a SHS, unstable fractures with a short cephalomedullary nail, and fractures with distal extension such as reverse obliquity patterns or subtrochanteric extension with a long cephalomedullary nail. Adherence to this algorithm not only decreased rates of postoperative complications, it also led to significant cost savings [96].
14 Subtrochanteric Femur Fractures
Subtrochanteric femur fractures are defined as those occurring within 5 cm of the distal aspect of the lesser trochanter. These fractures have had an increase in incidence in the hip fracture population and are often a result of low-energy trauma in this population [97]. Over two-thirds of all subtrochanteric femur fractures occur in patients over the age of 50 [98]. Due to the presence of osteoporosis in this patient population, a portion of these patients may be on bisphosphonate therapy care must be taken to recognize patients who fall under this category of bisphosphonate-related (atypical) subtrochanteric femur fractures [99]. These fractures may not only occur from ground-level falls, but may also occur spontaneously with or without prodromal pain [99].
These fractures present a challenge as the deforming forces of the proximal femur are an obstacle to overcome. Furthermore, these fractures have a short working length, making manipulation and reduction at times challenging to gain and maintain. The classic deformity of the proximal femur is brought on by its multiple muscle attachments. The Iliopsoas acts as a strong flexor and external rotator, the short external rotators add an additional external rotation moment, and the gluteus medius and minimus abduct the proximal femur [100].
15 Atypical Subtrochanteric Femur Fractures
Atypical femur fractures are a relatively recent recognized fracture pattern and fall within the subcategory of subtrochanteric femur fractures. These fractures have increased morbidity and poor healing and have had an association with the long-term use of bisphosphonates. Despite this, there is still much research that is pending to understand the true pathogenesis behind these fracture patterns. What is though is that the use of bisphosphates inhibits osteoclastic function from allowing repair in the area of high tensile and compressive forces leading to microdamage and stress reactions [101]. Furthermore, the collagen cross-linking from bisphosphonates creates more brittle bone. This combination leads to eventual failure in high areas of stress such as the subtrochanteric region. While the awareness of this injury has increased, the overall incidence is still low and is thought to be between 1.5 and 23 cases per 100,000 person years [102].
Upon treating a patient, a thorough history is required to assist in identifying potential risk factors linking them toward having an atypical femur fracture. Patients should be asked if they not only have been on bisphosphonate therapy but also for the duration of time. Furthermore, it is important to understand the mechanism behind the injury and also if there are any prodromal symptoms such as thigh or groin pain [102]. The Task Force of the American Society for Bone and Mineral Research have defined the following major criteria for which the patient must meet four of to have an atypical femur fracture [102]. Minor criteria may be present or not (Table 28.2).
Ultimately, patients should also be questioned about the contralateral extremity as well. In the setting of prodromal symptoms without an obvious fracture, an MRI can demonstrate focal lateral cortical thickening or signs of a fracture line [103].
16 Surgical Management of Subtrochanteric Femur Fractures
Generally, all subtrochanteric femur fractures will require surgical treatment, unless the patient is nonambulatory or has medical comorbidities that would preclude surgical treatment. Options for treatment include IM Nails and fixed-angle plate and screw constructs. Specific implants utilized with these fractures include: centromedullary nails, cephalomedullary nails, SHSs, proximal femur locking plates, and a 95-degree blade plate. Nailing can be performed with either a piriformis start point or through a trochanteric entry with equivalent results; however, it is important to understand the geometry of the nail being used as well as proximal locking options [104]. Trochanteric start points have been utilized more frequently for theoretical ease of obtaining a start point on a more subcutaneous portion of the proximal femur. Depending on the manufacturer, each nail will have a various-proximal bend; however, this bend may induce a varus or valgus force on the nail depending on the start point [105]. A lateral start point on the trochanter, even with an adequate reduction, may induce a varus deformity once the nail is finally seated (Fig. 28.12). Due to patient’s proximal femur morphology, there is no true ideal starting point for a trochanteric entry nail; however, starting at the tip of the trochanter or slightly medial may avoid a malreduction caused by the proximal bend of the nail [106].

(a–d) Demonstrate the effect of a lateral start point for different cephallomedullary nails in a subtrochanteric femur fracture resulting in a varus malunion. Courtesy of Ostrum et al.
Whether treatment is done on a flat top table or on a fracture table, the deforming forces of the proximal femur make imaging to obtain a starting point challenging. The C-arm will have to come over the top of the patient to account for the external rotation deformity. It is imperative to obtain a proper AP and lateral view of the proximal femur as the nail entry site is crucial for intramedullary nailing. If the deformity is such that reduction is difficult, percutaneous schanz pins or a ball spike pusher can be used to counteract the deforming forces to easier obtain imaging for a start point. A variety of methods exist in obtaining reduction for the proximal femur and should be done by graduated closed reduction methods. Options include a mallet, manual pressure, and use of an intramedullary reduction tool or “finger” [107]. Graduated open techniques can consist of ball spike pushers, schanz pins, and bone hooks which can be used to manipulate the proximal and distal fragments for reduction (Fig. 28.13a–d). Ultimately if unable to close reduce an open reduction is required. Following an open lateral approach to the proximal femur clamp assisted reduction can be performed in a biologically friendly manner to obtain and maintain a reduction of the proximal femur for efficient and accurate nailing with good clinical results [108]. Regardless of the technique used, the goals of surgery include spending time obtaining an appropriate start point and maintaining reduction while reaming to avoid malreduction that could occur prior to nail placement. “Push past” reaming can be used as a reduction aid as to not eccentrically ream at the fracture site and allow to nail assist with correction [109]. It must be noted that this technique is not as powerful in the metaphyseal region. In terms of proximal screw orientation, while crossed proximal screws are biomechanically stronger than parallel screws in the femoral head, they are often reserved for more distal or diaphyseal fracture patterns [110]. In geriatric patients, a large diameter cephalomedullary screw is used for increased fixation due to its larger size within the femoral head.

(a) AP radiograph demonstrating a comminuted subtrochanteric femur fracture. (b) Fluoroscopy demonstrates the use of percutaneous schanz pins to act as blocking drill bits as well as to manipulate the proximal fragment. (c) Fluoroscopy demonstrates placement of the nail around the percutaneous schanz pins. (d) Final AP demonstrates interval reduction and alignment after nail placement
17 Surgical Management of Atypical Femur Fractures
While the primary goal for surgical management of these fractures remains the same as non-atypical subtrochanteric femur fractures, atypical femur fractures are pathologic in nature and require special attention [111]. One of the most common complications during intramedullary nailing includes fracture propagation or iatrogenic fracture due to the brittle nature of the bone [112]. Care should be taken to not only measure the canal diameter, but also to scrutinize and locate the size of any bony pedestals. These bony pedestals or areas of lateral intramedullary sclerosis can deflect reamers leading to reaming of the medial cortex [101]. To avoid a translational or angular deformity, this area can be over-reamed after fracture reduction with a larger diameter reamer or ultimately may an open approach and burred down. For patients with MRI/radiographic evidence of stress reaction with prodromal symptoms, Egol et al reported a 100% healing rate with 81% relief of pain following prophylactic treatment [113].
18 Managing Complications in Subtrochanteric Femur Fractures
The main causes of malunion are often due to the inability to obtain an adequate reduction intraoperatively or with improper placement of a nail. A lateral start point can be salvaged by eccentrically reaming out the medial bone with a large diameter reamer to walk the start point more medial. However, varus mal-reduction and flexion of the proximal segment if not addressed can not only cause failure of the proximal femur fixation but also severely affect hip biomechanics. While there is a dearth of literature on treatment for this, the authors preference is to remove the intramedullary implant, osteotomized the fracture site, and place a blade plate (Fig. 28.14a–c).

(a) AP hip radiograph demonstrating varus failure of a subtrochanteric femur fracture. (b) AP hip radiograph postoperative revision of subtrochanteric malunion with blade plate. (c) Lateral hip radiograph of postoperative revision of subtrochanteric malunion with blade plate
Risks of nonunion and malunion are particularly noted to be higher in atypical femoral fractures due to the pathologic nature of the bone as well as varus malalignment [114, 115]. In a large multicenter series, the revision rate for these fractures was noted to be about 12% with a union rate of 5.2 months in those who did not need a reoperation [111]. This could be partly due to the fact that these fractures were able to be identified preoperatively allowing for appropriate surgical planning.
19 Conclusion
Proximal femur fractures whether they are intracapsular or extracapsular in the geriatric population continue to increase in numbers. Treatment of these injuries has a major impact on the health care system and is one of the most expensive diagnoses. While surgical techniques and implants continue to evolve, the rate of mortality after these injuries continues to remain the same. Risk stratification and dedicated geriatric hip fracture services have been utilized to identify patients at risk for increased complications and optimize patients as necessary prior to surgery.
Regardless of injury type, a thorough patient history should be completed and the preoperative radiographs should be scrutinized for appropriate preoperative planning. All current literature points to an anatomic reduction of the proximal femur and technically sound application of the implant to avoid both intraoperative and postoperative pitfalls. Sound evidence-based algorithms have also been developed for the surgical management of proximal femur fractures to optimize outcomes and improve cost.
While the primary goal of surgical intervention is to allow immediate mobilization and to return patients to their pre-injury level of function, poor bone quality, medical comorbidities, and patient frailty can make this difficult.
References
Bergstrom U, Jonsson H, Gustafson Y, Pettersson U, Stenlund H, Svensson O. The hip fracture incidence curve is shifting to the right. Acta Orthop. 2009;80(5):520–4.
Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int. 1997;7(5):407–13.
Cooper C, Campion G, Melton LJ 3rd. Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2(6):285–9.
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007;22(3):465–75.
Hung WW, Egol KA, Zuckerman JD, Siu AL. Hip fracture management: tailoring care for the older patient. JAMA. 2012;307(20):2185–94.
Khan MA, Hossain FS, Ahmed I, Muthukumar N, Mohsen A. Predictors of early mortality after hip fracture surgery. Int Orthop. 2013;37(11):2119–24.
Tornetta P 3rd, Mostafavi H, Riina J, et al. Morbidity and mortality in elderly trauma patients. J Trauma. 1999;46(4):702–6.
Gallagher SF, Williams B, Gomez C, et al. The role of cardiac morbidity in short- and long-term mortality in injured older patients who survive initial resuscitation. Am J Surg. 2003;185(2):131–4.
Wilson MS, Konda SR, Seymour RB, Karunakar MA. Carolinas trauma network research G. early predictors of mortality in geriatric patients with trauma. J Orthop Trauma. 2016;30(9):e299–304.
Konda SR, Lack WD, Seymour RB, Karunakar MA. Mechanism of injury differentiates risk factors for mortality in geriatric trauma patients. J Orthop Trauma. 2015;29(7):331–6.
Merloz P. Optimization of perioperative management of proximal femoral fracture in the elderly. Orthop Traumatol Surg Res. 2018;104(1S):S25–30.
Rosell PA, Parker MJ. Functional outcome after hip fracture. A 1-year prospective outcome study of 275 patients. Injury. 2003;34(7):529–32.
Koval KJ, Oh CK, Egol KA. Does a traction-internal rotation radiograph help to better evaluate fractures of the proximal femur? Bull NYU Hosp Jt Dis. 2008;66(2):102–6.
Bazylewicz DB, Egol KA, Koval KJ. Cortical encroachment after cephalomedullary nailing of the proximal femur: evaluation of a more anatomic radius of curvature. J Orthop Trauma. 2013;27(6):303–7.
Sadozai Z, Davies R, Warner J. The sensitivity of CT scans in diagnosing occult femoral neck fractures. Injury. 2016;47(12):2769–71.
Pejic A, Hansson S, Rogmark C. Magnetic resonance imaging for verifying hip fracture diagnosis why, when and how? Injury. 2017;48(3):687–91.
Heijckmann AC, Huijberts MS, Geusens P, de Vries J, Menheere PP, Wolffenbuttel BH. Hip bone mineral density, bone turnover and risk of fracture in patients on long-term suppressive L-thyroxine therapy for differentiated thyroid carcinoma. Eur J Endocrinol. 2005;153(1):23–9.
Heetveld MJ, Raaymakers EL, van Eck-Smit BL, van Walsum AD, Luitse JS. Internal fixation for displaced fractures of the femoral neck. Does bone density affect clinical outcome? J Bone Joint Surg Br. 2005;87(3):367–73.
Swiontkowski MF, Harrington RM, Keller TS, Van Patten PK. Torsion and bending analysis of internal fixation techniques for femoral neck fractures: the role of implant design and bone density. J Orthop Res. 1987;5(3):433–44.
Zlowodzki M, Bhandari M, Keel M, Hanson BP, Schemitsch E. Perception of Garden’s classification for femoral neck fractures: an international survey of 298 orthopaedic trauma surgeons. Arch Orthop Trauma Surg. 2005;125(7):503–5.
Kakar S, Tornetta P 3rd, Schemitsch EH, et al. Technical considerations in the operative management of femoral neck fractures in elderly patients: a multinational survey. J Trauma. 2007;63(3):641–6.
Panteli M, Rodham P, Giannoudis PV. Biomechanical rationale for implant choices in femoral neck fracture fixation in the non-elderly. Injury. 2015;46(3):445–52.
Hoffmann JC, Kellam J, Kumaravel M, Clark K, Routt MLC, Gary JL. Is the cranial and posterior screw of the “inverted triangle” configuration for femoral neck fractures safe? J Orthop Trauma. 2019;33(7):331–4.
Wang J, Jiang B, Marshall RJ, Zhang P. Arthroplasty or internal fixation for displaced femoral neck fractures: which is the optimal alternative for elderly patients? A meta-analysis. Int Orthop. 2009;33(5):1179–87.
Bray TJ. Femoral neck fracture fixation. Clinical decision making. Clin Orthop Relat Res. 1997;339:20–31.
Krastman P, van den Bent RP, Krijnen P, Schipper IB. Two cannulated hip screws for femoral neck fractures: treatment of choice or asking for trouble? Arch Orthop Trauma Surg. 2006;126(5):297–303.
Fixation using alternative implants for the treatment of hip fractures I. fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet. 2017;389(10078):1519–27.
Ort PJ, LaMont J. Treatment of femoral neck fractures with a sliding compression screw and two Knowles pins. Clin Orthop Relat Res. 1984;190:158–62.
Parker MJ. Hemiarthroplasty versus internal fixation for displaced intracapsular fractures of the hip in elderly men: a pilot randomised trial. Bone Joint J. 2015;97-B(7):992–6.
Parker MJ, Stockton G. Internal fixation implants for intracapsular proximal femoral fractures in adults. Cochrane Database Syst Rev 2001(4):CD001467.
Broderick JM, Bruce-Brand R, Stanley E, Mulhall KJ. Osteoporotic hip fractures: the burden of fixation failure. Scientific World Journal. 2013;2013:515197.
Parker MJ. Lateral versus posterior approach for insertion of hemiarthroplasties for hip fractures: a randomised trial of 216 patients. Injury. 2015;46(6):1023–7.
Yamagata M, Chao EY, Ilstrup DM, Melton LJ 3rd, Coventry MB, Stauffer RN. Fixed-head and bipolar hip endoprostheses. A retrospective clinical and roentgenographic study. J Arthroplast. 1987;2(4):327–41.
Kanto K, Sihvonen R, Eskelinen A, Laitinen M. Uni- and bipolar hemiarthroplasty with a modern cemented femoral component provides elderly patients with displaced femoral neck fractures with equal functional outcome and survivorship at medium-term follow-up. Arch Orthop Trauma Surg. 2014;134(9):1251–9.
Hedbeck CJ, Blomfeldt R, Lapidus G, Tornkvist H, Ponzer S, Tidermark J. Unipolar hemiarthroplasty versus bipolar hemiarthroplasty in the most elderly patients with displaced femoral neck fractures: a randomised, controlled trial. Int Orthop. 2011;35(11):1703–11.
Coleman SH, Bansal M, Cornell CN, Sculco TP. Failure of bipolar hemiarthroplasty: a retrospective review of 31 consecutive bipolar prostheses converted to total hip arthroplasty. Am J Orthop (Belle Mead NJ). 2001;30(4):313–9.
Azegami S, Gurusamy KS, Parker MJ. Cemented versus uncemented hemiarthroplasty for hip fractures: a systematic review of randomised controlled trials. Hip Int. 2011;21(5):509–17.
Berend ME, Smith A, Meding JB, Ritter MA, Lynch T, Davis K. Long-term outcome and risk factors of proximal femoral fracture in uncemented and cemented total hip arthroplasty in 2551 hips. J Arthroplast. 2006;21(6 Suppl 2):53–9.
Ahn J, Man LX, Park S, Sodl JF, Esterhai JL. Systematic review of cemented and uncemented hemiarthroplasty outcomes for femoral neck fractures. Clin Orthop Relat Res. 2008;466(10):2513–8.
Tannast M, Mack PW, Klaeser B, Siebenrock KA. Hip dislocation and femoral neck fracture: decision-making for head preservation. Injury. 2009;40(10):1118–24.
Macaulay W, Pagnotto MR, Iorio R, Mont MA, Saleh KJ. Displaced femoral neck fractures in the elderly: hemiarthroplasty versus total hip arthroplasty. J Am Acad Orthop Surg. 2006;14(5):287–93.
Gregory RJ, Wood DJ, Stevens J. Treatment of displaced subcapital femoral fractures with total hip replacement. Injury. 1992;23(3):168–70.
Keating JF, Grant A, Masson M, Scott NW, Forbes JF. Randomized comparison of reduction and fixation, bipolar hemiarthroplasty, and total hip arthroplasty. Treatment of displaced intracapsular hip fractures in healthy older patients. J Bone Joint Surg Am. 2006;88(2):249–60.
Mahmoud SS, Pearse EO, Smith TO, Hing CB. Outcomes of total hip arthroplasty, as a salvage procedure, following failed internal fixation of intracapsular fractures of the femoral neck: a systematic review and meta-analysis. Bone Joint J. 2016;98-B(4):452–60.
Swart E, Roulette P, Leas D, Bozic KJ, Karunakar M. ORIF or arthroplasty for displaced femoral neck fractures in patients younger than 65 years old: an economic decision analysis. J Bone Joint Surg Am. 2017;99(1):65–75.
Slover J, Hoffman MV, Malchau H, Tosteson AN, Koval KJ. A cost-effectiveness analysis of the arthroplasty options for displaced femoral neck fractures in the active, healthy, elderly population. J Arthroplast. 2009;24(6):854–60.
Parker MJ, Pryor GA, Anand JK, Lodwick R, Myles JW. A comparison of presenting characteristics of patients with intracapsular and extracapsular proximal femoral fractures. J R Soc Med. 1992;85(3):152–5.
Forte ML, Virnig BA, Swiontkowski MF, et al. Ninety-day mortality after intertrochanteric hip fracture: does provider volume matter? J Bone Joint Surg Am. 2010;92(4):799–806.
Schipper IB, Steyerberg EW, Castelein RM, van Vugt AB. Reliability of the AO/ASIF classification for pertrochanteric femoral fractures. Acta Orthop Scand. 2001;72(1):36–41.
Hsu CE, Shih CM, Wang CC, Huang KC. Lateral femoral wall thickness. A reliable predictor of post-operative lateral wall fracture in intertrochanteric fractures. Bone Joint J. 2013;95-B(8):1134–8.
Gotfried Y. The lateral trochanteric wall: a key element in the reconstruction of unstable pertrochanteric hip fractures. Clin Orthop Relat Res. 2004;425:82–6.
Parker MJ. Trochanteric hip fractures. Fixation failure commoner with femoral medialization, a comparison of 101 cases. Acta Orthop Scand. 1996;67(4):329–32.
Im GI, Shin YW, Song YJ. Potentially unstable intertrochanteric fractures. J Orthop Trauma. 2005;19(1):5–9.
Chen F, Wang Z, Bhattacharyya T. Convergence of outcomes for hip fracture fixation by nails and plates. Clin Orthop Relat Res. 2013;471(4):1349–55.
Roberts KC, Brox WT, Jevsevar DS, Sevarino K. Management of hip fractures in the elderly. J Am Acad Orthop Surg. 2015;23(2):131–7.
Socci AR, Casemyr NE, Leslie MP, Baumgaertner MR. Implant options for the treatment of intertrochanteric fractures of the hip: rationale, evidence, and recommendations. Bone Joint J. 2017;99-B(1):128–33.
Leung KS, So WS, Shen WY, Hui PW. Gamma nails and dynamic hip screws for peritrochanteric fractures. A randomised prospective study in elderly patients. J Bone Joint Surg Br. 1992;74(3):345–51.
Adams CI, Robinson CM, Court-Brown CM, McQueen MM. Prospective randomized controlled trial of an intramedullary nail versus dynamic screw and plate for intertrochanteric fractures of the femur. J Orthop Trauma. 2001;15(6):394–400.
Curtis MJ, Jinnah RH, Wilson V, Cunningham BW. Proximal femoral fractures: a biomechanical study to compare intramedullary and extramedullary fixation. Injury. 1994;25(2):99–104.
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev 2010(9):CD000093.
Bohl DD, Basques BA, Golinvaux NS, Miller CP, Baumgaertner MR, Grauer JN. Extramedullary compared with intramedullary implants for intertrochanteric hip fractures: thirty-day outcomes of 4432 procedures from the ACS NSQIP database. J Bone Joint Surg Am. 2014;96(22):1871–7.
Matre K, Vinje T, Havelin LI, et al. TRIGEN INTERTAN intramedullary nail versus sliding hip screw: a prospective, randomized multicenter study on pain, function, and complications in 684 patients with an intertrochanteric or subtrochanteric fracture and one year of follow-up. J Bone Joint Surg Am. 2013;95(3):200–8.
Bretherton CP, Parker MJ. Femoral medialization, fixation failures, and functional outcome in trochanteric hip fractures treated with either a sliding hip screw or an intramedullary nail from within a randomized trial. J Orthop Trauma. 2016;30(12):642–6.
Ahrengart L, Tornkvist H, Fornander P, et al. A randomized study of the compression hip screw and gamma nail in 426 fractures. Clin Orthop Relat Res. 2002;401:209–22.
Pajarinen J, Lindahl J, Michelsson O, Savolainen V, Hirvensalo E. Pertrochanteric femoral fractures treated with a dynamic hip screw or a proximal femoral nail. A randomised study comparing post-operative rehabilitation. J Bone Joint Surg Br. 2005;87(1):76–81.
Reindl R, Harvey EJ, Berry GK, Rahme E. Canadian orthopaedic trauma S. intramedullary versus extramedullary fixation for unstable intertrochanteric fractures: a prospective randomized controlled trial. J Bone Joint Surg Am. 2015;97(23):1905–12.
Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77(7):1058–64.
Huang X, Leung F, Liu M, Chen L, Xu Z, Xiang Z. Is helical blade superior to screw design in terms of cut-out rate for elderly trochanteric fractures? A meta-analysis of randomized controlled trials. Eur J Orthop Surg Traumatol. 2014;24(8):1461–8.
Stern R, Lubbeke A, Suva D, Miozzari H, Hoffmeyer P. Prospective randomised study comparing screw versus helical blade in the treatment of low-energy trochanteric fractures. Int Orthop. 2011;35(12):1855–61.
Ibrahim I, Appleton PT, Wixted JJ, DeAngelis JP, Rodriguez EK. Implant cut-out following cephalomedullary nailing of intertrochanteric femur fractures: are helical blades to blame? Injury. 2019;50(4):926–30.
Geller JA, Saifi C, Morrison TA, Macaulay W. Tip-apex distance of intramedullary devices as a predictor of cut-out failure in the treatment of peritrochanteric elderly hip fractures. Int Orthop. 2010;34(5):719–22.
Goffin JM, Pankaj P, Simpson AH, Seil R, Gerich TG. Does bone compaction around the helical blade of a proximal femoral nail anti-rotation (PFNA) decrease the risk of cut-out?: a subject-specific computational study. Bone Joint Res. 2013;2(5):79–83.
Kubiak EN, Bong M, Park SS, Kummer F, Egol K, Koval KJ. Intramedullary fixation of unstable intertrochanteric hip fractures: one or two lag screws. J Orthop Trauma. 2004;18(1):12–7.
Frei HC, Hotz T, Cadosch D, Rudin M, Kach K. Central head perforation, or “cut through,” caused by the helical blade of the proximal femoral nail antirotation. J Orthop Trauma. 2012;26(8):e102–7.
Flores SA, Woolridge A, Caroom C, Jenkins M. The utility of the tip-apex distance in predicting axial migration and Cutout with the trochanteric fixation nail system helical blade. J Orthop Trauma. 2016;30(6):e207–11.
Baldwin PC 3rd, Lavender RC, Sanders R, Koval KJ. Controversies in intramedullary fixation for intertrochanteric hip fractures. J Orthop Trauma. 2016;30(12):635–41.
Kouvidis GK, Sommers MB, Giannoudis PV, Katonis PG, Bottlang M. Comparison of migration behavior between single and dual lag screw implants for intertrochanteric fracture fixation. J Orthop Surg Res. 2009;4:16.
Strauss EJ, Kummer FJ, Koval KJ, Egol KA. The “Z-effect” phenomenon defined: a laboratory study. J Orthop Res. 2007;25(12):1568–73.
Santoni BG, Nayak AN, Cooper SA, et al. Comparison of femoral head rotation and Varus collapse between a single lag screw and integrated dual screw intertrochanteric hip fracture fixation device using a cadaveric hemi-pelvis biomechanical model. J Orthop Trauma. 2016;30(4):164–9.
Serrano R, Blair JA, Watson DT, et al. Cephalomedullary nail fixation of intertrochanteric femur fractures: are two proximal screws better than one? J Orthop Trauma. 2017;31(11):577–82.
Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma. 2004;18(7):410–5.
Kleweno C, Morgan J, Redshaw J, et al. Short versus long cephalomedullary nails for the treatment of intertrochanteric hip fractures in patients older than 65 years. J Orthop Trauma. 2014;28(7):391–7.
Hou Z, Bowen TR, Irgit KS, et al. Treatment of pertrochanteric fractures (OTA 31-A1 and A2): long versus short cephalomedullary nailing. J Orthop Trauma. 2013;27(6):318–24.
Harrington P, Nihal A, Singhania AK, Howell FR. Intramedullary hip screw versus sliding hip screw for unstable intertrochanteric femoral fractures in the elderly. Injury. 2002;33(1):23–8.
Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br. 1990;72(1):26–31.
Whale CS, Hulet DA, Beebe MJ, et al. Cephalomedullary nail versus sliding hip screw for fixation of AO 31 A1/2 intertrochanteric femoral fracture: a 12-year comparison of failure, complications, and mortality. Curr Orthop Pract. 2016;27(6):604–13.
Zielinski SM, Keijsers NL, Praet SF, et al. Femoral neck shortening after internal fixation of a femoral neck fracture. Orthopedics. 2013;36(7):e849–58.
Bridle SH, Patel AD, Bircher M, Calvert PT. Fixation of intertrochanteric fractures of the femur. A randomised prospective comparison of the gamma nail and the dynamic hip screw. J Bone Joint Surg Br. 1991;73(2):330–4.
Radford PJ, Needoff M, Webb JK. A prospective randomised comparison of the dynamic hip screw and the gamma locking nail. J Bone Joint Surg Br. 1993;75(5):789–93.
Butt MS, Krikler SJ, Nafie S, Ali MS. Comparison of dynamic hip screw and gamma nail: a prospective, randomized, controlled trial. Injury. 1995;26(9):615–8.
Bhandari M, Schemitsch E, Jonsson A, Zlowodzki M, Haidukewych GJ. Gamma nails revisited: gamma nails versus compression hip screws in the management of intertrochanteric fractures of the hip: a meta-analysis. J Orthop Trauma. 2009;23(6):460–4.
Bojan AJ, Beimel C, Speitling A, Taglang G, Ekholm C, Jonsson A. 3066 consecutive gamma nails. 12 years experience at a single Centre. BMC Musculoskelet Disord. 2010;11:133.
Anglen JO, Weinstein JN. American Board of Orthopaedic Surgery Research C. nail or plate fixation of intertrochanteric hip fractures: changing pattern of practice. A review of the American board of orthopaedic surgery database. J Bone Joint Surg Am. 2008;90(4):700–7.
Radcliff TA, Regan E, Cowper Ripley DC, Hutt E. Increased use of intramedullary nails for intertrochanteric proximal femoral fractures in veterans affairs hospitals: a comparative effectiveness study. J Bone Joint Surg Am. 2012;94(9):833–40.
Swart E, Makhni EC, Macaulay W, Rosenwasser MP, Bozic KJ. Cost-effectiveness analysis of fixation options for intertrochanteric hip fractures. J Bone Joint Surg Am. 2014;96(19):1612–20.
Egol KA, Marcano AI, Lewis L, Tejwani NC, McLaurin TM, Davidovitch RI. Can the use of an evidence-based algorithm for the treatment of intertrochanteric fractures of the hip maintain quality at a reduced cost? Bone Joint J. 2014;96-B(9):1192–7.
Sullivan MP, Baldwin KD, Donegan DJ, Mehta S, Ahn J. Geriatric fractures about the hip: divergent patterns in the proximal femur, acetabulum, and pelvis. Orthopedics. 2014;37(3):151–7.
Ng AC, Drake MT, Clarke BL, et al. Trends in subtrochanteric, diaphyseal, and distal femur fractures, 1984-2007. Osteoporos Int. 2012;23(6):1721–6.
Thompson RN, Phillips JR, McCauley SH, Elliott JR, Moran CG. Atypical femoral fractures and bisphosphonate treatment: experience in two large United Kingdom teaching hospitals. J Bone Joint Surg Br. 2012;94(3):385–90.
Jackson C, Tanios M, Ebraheim N. Management of Subtrochanteric Proximal Femur Fractures: a review of recent literature. Adv Orthop. 2018;2018:1326701.
Githens M, Garner MR, Firoozabadi R. Surgical Management of Atypical Femur Fractures Associated with Bisphosphonate Therapy. J Am Acad Orthop Surg. 2018;26(24):864–71.
Shane E, Burr D, Abrahamsen B, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2014;29(1):1–23.
Black JD, Kancherla VK, De Long WG Jr. A review of atypical femoral fractures from a tertiary care teaching hospital: an alarming trend? J Orthop Trauma. 2016;30(4):182–8.
Starr AJ, Hay MT, Reinert CM, Borer DS, Christensen KC. Cephalomedullary nails in the treatment of high-energy proximal femur fractures in young patients: a prospective, randomized comparison of trochanteric versus piriformis fossa entry portal. J Orthop Trauma. 2006;20(4):240–6.
Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccentric starting point for trochanteric intramedullary femoral nailing. J Orthop Trauma. 2005;19(10):681–6.
Streubel PN, Wong AH, Ricci WM, Gardner MJ. Is there a standard trochanteric entry site for nailing of subtrochanteric femur fractures? J Orthop Trauma. 2011;25(4):202–7.
Yoon RS, Donegan DJ, Liporace FA. Reducing subtrochanteric femur fractures: tips and tricks, do’s and don’ts. J Orthop Trauma. 2015;29(Suppl 4):S28–33.
Afsari A, Liporace F, Lindvall E, Infante A Jr, Sagi HC, Haidukewych GJ. Clamp-assisted reduction of high subtrochanteric fractures of the femur: surgical technique. J Bone Joint Surg Am. 2010;92(Suppl 1 Pt 2):217–25.
Gary JL, Munz JW, Burgess AR. "push-past" reaming as a reduction aid with intramedullary nailing of metadiaphyseal and diaphyseal femoral shaft fractures. Orthopedics. 2014;37(6):393–6.
Grisell M, Moed BR, Bledsoe JG. A biomechanical comparison of trochanteric nail proximal screw configurations in a subtrochanteric fracture model. J Orthop Trauma. 2010;24(6):359–63.
Bogdan Y, Tornetta P 3rd, Einhorn TA, et al. Healing time and complications in operatively treated atypical femur fractures associated with bisphosphonate use: a Multicenter retrospective cohort. J Orthop Trauma. 2016;30(4):177–81.
Prasarn ML, Ahn J, Helfet DL, Lane JM, Lorich DG. Bisphosphonate-associated femur fractures have high complication rates with operative fixation. Clin Orthop Relat Res. 2012;470(8):2295–301.
Egol KA, Park JH, Rosenberg ZS, Peck V, Tejwani NC. Healing delayed but generally reliable after bisphosphonate-associated complete femur fractures treated with IM nails. Clin Orthop Relat Res. 2014;472(9):2728–34.
Favinger JL, Hippe D, Ha AS. Long-term radiographic follow-up of bisphosphonate-associated atypical femur fractures. Skelet Radiol. 2016;45(5):627–33.
Schilcher J. High revision rate but good healing capacity of atypical femoral fractures. A comparison with common shaft fractures. Injury. 2015;46(12):2468–73.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ganta, A., Egol, K.A. (2022). Specifics of Surgical Management: Proximal Femur Fractures. In: Pape, HC., Kates, S.L., Hierholzer, C., Bischoff-Ferrari, H.A. (eds) Senior Trauma Patients . Springer, Cham. https://doi.org/10.1007/978-3-030-91483-7_28
Download citation
DOI: https://doi.org/10.1007/978-3-030-91483-7_28
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-91482-0
Online ISBN: 978-3-030-91483-7
eBook Packages: MedicineMedicine (R0)