
Abstract
Diagnostic and prognostic tools for risk stratification of concussion patients are limited in the early stages of injury in the acute setting. Research in the field of traumatic brain injury (TBI) biomarkers has increased exponentially over the last 20 years with a barrage of publications on the topic in the last decade. As with other organ-based diseases, the employment of a rapid, accurate, and widely available blood test to guide diagnosis and treatment of TBI and concussion would be a most welcomed clinical tool. Previously, human trials examined only moderate-to-severe TBI but are now expanding to include injuries on the milder end of the TBI spectrum, such as concussion and subconcussive injuries. Recently, two biomarkers have now been FDA approved for clinical use in adult patients with mild-to-moderate TBI to help determine the need for CT scan acutely after injury. More work is also being done to detect subclinical injuries. In an effort to prevent chronic traumatic encephalopathy (CTE) and long-term consequences of concussion/mild TBI, early diagnostic and prognostic tools are becoming increasingly important, particularly in sports injuries and in military personnel where concussions/mild TBI are common occurrences. Should biofluid biomarkers for TBI be validated and become widely available, they could have many roles. They could help with clinical decision-making by clarifying injury severity and help monitor the progression of injury and/or recovery. Biomarkers could have a role in managing patients at high risk of repeated brain injury and could be incorporated into guidelines for return to duty, work, or sports activities. As technology advances and integrates neuroproteomics, metabolomics, bioinformatics, genetics, and neuroimaging, the path from discovery to validation of potential TBI biomarkers will be swift. This chapter reviews the most widely studied proteomic biomarkers for mild TBI and concussion in humans and introduces a novel group of promising transcriptomic biomarkers.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Biomarkers
- Blood
- Serum
- Cerebrospinal fluid
- Concussion
- Mild TBI
- Head injury
- S100β[beta]
- GFAP
- NSE
- UCH-L1
- SBDP150
- SBDP145
- Tau
- MBP
- Neurofilament proteins
- Proteomics
- Diagnosis
- Prognosis
- Risk stratification
- Detection
- Pathophysiology
- Monitoring
- Biochemical markers
Introduction
Path Toward Blood Test for Concussion
Currently , concussion (which is also known as mild traumatic brain injury) is largely a clinical diagnosis based on injury history, neurologic examination, neuropsychological testing, and, at times, neuroimaging. Early and tailored management of athletes following a concussion can provide them with the best opportunity to avoid further injury. Brain-specific biomarkers measured through a simple blood test could complement the clinical evaluation of concussion and potentially guide management decisions [1,2,3,4,5]. The pursuit of these elusive markers has been most intense over the last decade [6,7,8]. Previously, human trials examined only moderate to severe TBI but are now expanding to include injuries on the milder end of the TBI spectrum, such as concussion, and subconcussive injuries and the effects of head acceleration events.
The degree of brain injury depends on the primary mechanism/magnitude of injury, secondary insults, and the patient’s genetic and molecular response. Following the initial injury, cellular responses and neurochemical and metabolic cascades contribute to secondary injury which may evolve over the ensuing hours and days. These secondary insults can be mediated through physiologic events which decrease the supply of oxygen and energy to the brain tissue or through a cascade of cytotoxic events mediated by molecular and cellular processes. The release of brain injury biomarkers is not a static process. Studying the time course of a biomarker is critical to optimizing timing and clinical use. The time course (or temporal profile) may be affected by source of the sample, lesion type (mass lesion versus diffuse injury) and location, concomitant extracranial injuries (fractures, solid organ injuries), secondary insults, and individual patient physiology. Biomarkers could reflect these secondary insults as well as blood-brain barrier disruption. Complicating the release of biomarkers is the potential for extracranial sources of release after trauma. In cases when the biomarkers are released from tissues other than the brain, caution must be taken when interpreting results. For instance, S100β can be released from soft tissues, cartilage, and bone after trauma and may not accurately reflect brain injury [9, 10]. Furthermore, individual physiology and pre-existing disease states, such as kidney or liver disease, may alter the metabolism or clearance of a given biomarker.
Key features that would make concussion biomarkers clinically useful include the following: (1) a high sensitivity (come from the brain) and specificity (low or undetectable in blood in non-injury states) for brain injury; (2) the ability to stratify patients by severity of injury (concentration of the biomarker should increase with worsening injury); (3) the timely appearance in accessible biological fluid such as serum, saliva, or urine; (4) a well-defined time course; (5) the ability to monitor injury and response to treatment; (6) the ability to predict functional outcome; and (7) be easily measured [8, 11].
To follow is a review of the most widely studied proteomic biomarkers for mild TBI and concussion in humans. Proteomic biomarkers are often represented by their neuroanatomic location in the central nervous system including astroglia (GFAP, S100β) and neuronal cells, with specific areas of the neuron such as the cell body (UCH-L1) and axon (Tau, neurofilament) (Fig. 13.1). Furthermore, a novel group of promising transcriptomic biomarkers called microRNAs will also be discussed.

Proteomic biomarkers are often represented by their neuroanatomic location in the central nervous system including astroglia (GFAP, S100β) and neuronal cells, with specific areas of the neuron such as the cell body (UCH-L1) and axon (Tau, neurofilament). A novel group of promising TBI markers include transcriptomic biomarkers called microRNAs
Proteomic Biomarkers
Glial Fibrillary Acidic Protein (GFAP) and Ubiquitin C-Terminal Hydrolase (UCH-L1)
GFAP and UCH-L1 for Mild-to-Moderate Traumatic Brain Injury
Glial fibrillary acidic protein (GFAP) is a protein found in the astroglial skeleton of both white and gray brain matter and is used as a histological marker for glial cells. Ubiquitin C-terminal hydrolase-L1 (UCH-L1) is a protein in neurons that is involved in the addition and removal of ubiquitin from proteins that are destined for metabolism and is used as a histological marker for neurons [12, 13].
The specificity of GFAP and UCH-L1 for detecting brain injury has been examined in a number of studies. GFAP and UCH-L1 have been shown to distinguish mild and moderate TBI patients from orthopedic controls and motor vehicle crash controls as well as from those TBI patients with negative computed tomography (CT) scans [10, 14, 15]. In these studies, trauma control patients were exposed to significant trauma including the acceleration-deceleration vectors of motor vehicle collisions and substantial falls. Both GFAP and UCH-L1 showed a graded response to the severity of injury from uninjured to orthopedic trauma, to mild and moderate TBI. However, GFAP appears to be the most brain-specific in the setting of polytrauma with substantial extracranial injuries and fractures [2, 3, 9, 10, 14,15,16].
The temporal profiles of GFAP and UCH-L1 over a week following a mild traumatic brain injury have been clearly described in a large cohort of emergency department trauma patients. GFAP consistently identified concussion over 7 days. GFAP also detected with good accuracy traumatic intracranial lesions on head computed tomography (CT) and neurosurgical intervention over a week [15]. GFAP was detectible in serum within an hour of concussion and remained elevated for several days after rendering it a promising contender for clinical use for concussion diagnosis within a week of injury [15]. In contrast, UCH-L1 rose rapidly within 30 min of injury and peaked at 8 h after injury and decreased steadily over 48 h with small peaks and toughs over 7 days – making UCH-L1 a very early marker of concussion [15].
Over the last decade, glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal Hydrolase (UCH-L1) have been found in several distinct studies to detect traumatic intracranial CT scan lesions and predict neurosurgical intervention in adults with mild to moderate TBI [10, 14, 15, 17,18,19,20]. More recently, these findings have been replicated in children [2, 3, 21, 22]. In early 2018, GFAP and UCH-L1 were FDA approved for clinical use in adult patients with mild to moderate TBI to help determine the need for CT scan within 12 h of injury [23]. The approval was based on the ability to find lesions on a CT scan but was not approved to diagnose a concussion. Moreover, it was not approved for use in children.
GFAP and UCH-L1 for Concussion and Subconcussive Brain Injury
Computed tomography (CT) is the standard imaging modality for assessing damage in TBI during the acute phase of injury. CT scan can detect macroscopic traumatic lesions such as skull fractures, intracranial hematomas, contusions, subarachnoid hemorrhages, and swelling. However, the more subtle injuries associated with mild TBI are often not demonstrated by this imaging modality. This discrepancy is evidenced by the lack of CT abnormalities in patients with cognitive, physical, and behavioral dysfunction following a mild TBI. Therefore, CT does not have sufficient sensitivity to detect damage incurred in mild TBI. This group of TBI patients represents the greatest challenge to accurate diagnosis and outcome prediction. Metting et al. found that patients with axonal injury on MRI, but not CT, had elevated GFAP levels. Similarly, Yue et al. assessed GFAP in mild TBI patients with a negative CT scan and found GFAP was able to detect MRI lesions with an area under the curve of 0.78 despite the CT scan not showing any lesions [24]. UCH-L1 was not examined in either of these studies.
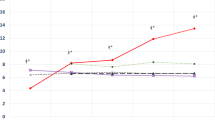
A significantly understudied group in whom biomarkers are rarely examined are individuals who experience head trauma without symptoms of concussion. They are often classified as having “no injury” when, in fact, they may represent milder forms of concussion that do not elicit the typical signs or symptoms associated with concussion. Such injuries have been referred to as subconcussive injuries or head acceleration events. Emerging data have demonstrated that significant alterations in brain function can occur in the absence of clinically obvious symptoms following even a single head trauma [25,26,27]. The issue of subconcussive trauma has been a particular concern in military personnel [28] and in athletes, as repetitive subconcussive impacts have the potential for long-term deleterious effects [27, 29, 30]. To address this deficiency, a recent study evaluated how GFAP and UCH-L1 behave in subconcussive trauma in a large cohort of children and adult trauma patients presenting to three-level I trauma centers with a Glasgow Coma Scale (GCS) score of 15 and a normal mental status. The biomarkers were measured at 20 distinct time-points in patients with concussive, subconcussive, and non-concussive trauma (Fig. 13.2). Although blood levels of both GFAP and UCH-L1 showed incremental increases from body trauma (lowest levels), to head trauma without concussion (higher levels than body trauma), to concussion (highest levels), GFAP was much better in distinguishing between the groups than UCH-L1. UCH-L1 was expressed at much higher levels than GFAP in those with non-concussive trauma, particularly in children, suggesting that UCH-L1 is either not completely brain-specific or ultrasensitive to subtle impacts [22]. In athletes, UCH-L1 has shown elevations in both concussive [31] and subconcussive trauma [32]. However, these results are not consistent in all studies [33, 34].

Temporal profile of GFAP and UCH-L1 in three groups of trauma patients. (a) Temporal profile of GFAP and UCH-L1 in body trauma control patients. Means with error bars representing SEM. (b) Temporal profile of GFAP and UCH-L1 in head trauma control patients. Means with error bars representing SEM. (c) Temporal profile of GFAP and UCH-L1 in trauma patients with concussion. Means with error bars representing SEM. GFAP, glialfibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase. (Taken from Papa et al. [22])
Other Potential Proteomic Biofluid Biomarkers of Concussion
A systematic review of biomarkers in sports-related concussion showed that there have been at least eleven different biomarkers assessed in athletes [5]. Besides GFAP and UCH-L1, other potential biomarkers include S100β, neuron-specific enolase, tau, neurofilament, amyloid beta, and brain-derived neurotrophic factor. Some correlate with the number of hits to the head (soccer), acceleration/deceleration forces (jumps, collisions, and falls), post-concussive symptoms, trauma to the body versus the head, and dynamics of injury [5]. Some of these and other novel markers are discussed below.
S100β
S100β is expressed in astrocytes and helps to regulate intracellular levels of calcium. It is considered a marker of astrocyte injury or death. Of note, it can also be found in cells that are not neuronal such as adipocytes, chondrocytes, and melanoma cells and, therefore, it is not brain-specific [35, 36]. Despite this, S100β is one of the most extensively studied biomarkers for TBI [4, 5, 37].
A number of studies have found correlations between elevated serum levels of S100β and CT abnormalities in adults and children [4, 38]. Elevated concentrations of S100β in serum have been associated with increased incidence of post-concussive symptoms, problems with cognition, and traumatic abnormalities on MRI [39,40,41,42,43]. However, there are also a number of studies negating these findings [16, 44,45,46]. Similarly, several studies have shown that serum S100β increases after concussive [31, 47, 48] and subconcussive brain injury [34, 49, 50]. However, a number of studies have shown a poor association with other prognostic parameters [33, 46, 51]. Peripheral sources of S100β complicate its use as a brain-specific marker, particularly in the setting of polytrauma. S100β has been shown to be elevated in injured patients with peripheral trauma who have had no direct head trauma [2, 10, 52]. Since many of these results have been inconsistently reproduced, the clinical value of S100β in TBI, particularly mild TBI and concussion, is still controversial. Despite these inconsistent findings, S100β has been approved for use by TBI patients in Europe.
Tau Protein
Tau is an intracellular, microtubule-associated protein that is amplified in axons and is involved with assembling axonal microtubule bundles and participating in anterograde axoplasmic transport [53]. Tau lesions are apparently related to axonal disruption such as in trauma or hypoxia [54, 55]. After release, it is proteolytically cleaved at the N- and C-terminals. In a study by Shaw et al., an elevated level of C-Tau was associated with a poor outcome at hospital discharge and with an increased chance of an intracranial injury on head CT [56]. However, these findings were not reproducible when C-Tau was measured in peripheral blood in mild TBI [57]. Two additional studies showed that C-Tau was a poor predictor of CT lesions and a poor predictor of post-concussive syndrome [44, 58]. Similarly, Bulut et al. found total Tau (T-Tau) differentiated patients with intracranial injury from those without intracranial injury [59]. However, they were not able to detect milder injuries.
In 2014, a study of professional hockey players showed that serum T-Tau out-performed S-100B and NSE in detecting concussion at 1 h after injury and that levels were significantly higher in post-concussion samples at all times compared with preseason levels [48]. T-Tau at 1 h after concussion also correlated with the number of days it took for concussion symptoms to resolve. Accordingly, T-Tau remained significantly elevated at 144 h in players with post-concussive symptoms (PCS) lasting more than 6 days versus players with PCS for less than 6 days [48].
Phosphorylated-Tau (P-Tau) is also being examined as a potential biomarker for brain trauma. Following TBI, axonal injury is coupled to Tau hyperphosphorylation, leading to microtubule instability and Tau-mediated neurodegeneration [60]. The P-tau level has been shown to outperform the T-tau level in distinguishing CT positive from CT negative cases and identifying patients with poor outcome [61]. Moreover, several months after TBI, P-Tau has been shown to be elevated in TBI patients compared to healthy controls. The ratio between P-Tau and T-Tau has shown similar results [61]. High levels of total and phosphorylated Tau have been found in postmortem samples of TBI patients and athletes [62, 63]. Further study is needed to elucidate the role of T-Tau and P-Tau in detecting chronic encephalopathy.
Neurofilaments
Neurofilaments are heteropolymeric components of the neuron cytoskeleton that consist of a 68 kDa light neurofilament subunit (NF-L) backbone with either 160 kDa medium (NF-M) or 200 kDa heavy subunit (NF-H) side-arms [64]. Following TBI, calcium influx into the cell contributes to a cascade of events that activates calcineurin, a calcium-dependent phosphatase that dephosphorylates neurofilament side-arms, presumably contributing to axonal injury [65]. Phosphorylated NF-H has been found to be elevated in the CSF of adults and children with severe TBI [66, 67]. It remains significantly elevated after a few days in children with poor outcome and diffuse axonal injury (DAI) on initial CT scan [67]. Similarly, in a study by Vajtr et al. serum NF-H was much higher in patients with DAI over 10 days after admission with highest levels from day 4 to day 10 [68].
In a cohort of professional hockey players who underwent blood biomarker assessment at 1, 12, 36, and 144 h after concussion and at return-to-play, serum NF-L increased over time and returned to normal at return-to-play. Also, serum NF-L levels were higher in players with prolonged post-concussive symptoms [69]. In a group of amateur boxers, serum NF-L concentrations showed elevations 7–10 days after about and subsequently decreased following 3 months of rest. Levels were also significantly correlated with the number of hits to the head [69]. Moreover, NF-L has been shown to increase in adult soccer players following repetitive subconcussive head impacts compared to baseline levels, however, only after 24 h of the impacts [70]. In contrast, NF-L levels in blood taken at baseline and at 6- and 14-days post-concussion in contact sport athletes showed no differences between any of the pre-post timepoints [71].
Transcriptomic Biomarkers
MicroRNAs as the Next Generation of Biomarkers for Concussion
Initial exploration of TBI biomarkers began using animal models. These models have been helpful in providing histologic and pathophysiologic information on potential biomarkers. As a result, the selection of TBI biomarkers has been based on neuroanatomic location and on mechanisms of injury induced by trauma such as neuroinflammation and ischemia.
A novel set of biomarkers, called microRNAs (miRNA), are now being studied as the next generation of biomarkers for many diseases and disorders such as cancer, cardiovascular, and neurodegenerative diseases [72]. MiRNAs are small (19–28 nucleotides) endogenous RNA molecules that regulate protein synthesis at the post transcriptional level. MiRNAs can be detected in serum and can be an indicator of disease pathology in neuronal cells. MiRNAs are relatively abundant in biofluids such as cerebrospinal fluid, serum, and urine and are relatively stable at variable pH conditions, resistant to repeated freeze thaw and enzymatic degradation. Due to these properties, miRNA has advantages over protein-based markers. The utility of miRNAs as diagnostic markers of mild TBI or concussion has recently been explored [73,74,75,76,77]. In 2016, Bhomia et al. identified specific and sensitive miRNA-based biomarkers for mild and moderate TBI using real-time PCR methodology [74]. Samples from human subjects with mild to severe TBI were compared to trauma and normal controls and identified 10 miRNA signatures miR-151-5p, miR-328, miR-362-3p, miR-486, miR-505*, miR-451, miR-30d, miR-20a, miR-195, and miR-92a. Moreover, Johnson et al. identified 6 salivary miRNAs with overlapping CSF alterations (miR-182-5p, miR-221-3p, miR-26b-5p, miR-320c, miR-29c-3p, and miR-30e-5p) that distinguished children with TBI from healthy controls [75]. In a study by the same group, 52 children with concussion had 5 salivary miRNAs (miR-320c, miR-133a-5p, miR-769-5p, let-7a-3c, and miR-1307-3p) that were associated with prolonged post-concussive symptoms [76].
More recently, studies have been evaluating the role of microRNA in sports-related concussion. In one recent study, microRNA biomarkers measured pre- and post-season in collegiate football players were associated with worsening neurocognitive functioning over the course of a season in those with no concussions [78]. The study found significant elevations in circulating miRNA measured before the athletic season began and prior to any contact practices. All the players had significantly elevated levels compared to non-athlete controls (p < 0.001) suggesting residual circulating miRNA biomarkers from prior concussive and subconcussive impacts [78, 79]. Pre-season miRNA levels predicted baseline SAC scores with very good areas under the curve, the highest being miR-195 (0.90), miR-20a (0.89), miR-151-5p (0.86), miR-505* (0.85), and miR-9-3p (0.77). Athletes who demonstrated worsening neurocognitive function from pre- to post-season showed elevations in concentrations of miRNAs over the same period. The miRNAs with the most significant increases over the course of the season were miR-505*, miR-362-3p, miR-30d, miR-92a, and miR-486. Similarly, a study of saliva miRNA levels from 32 rugby players detected 5 miRNAs (miR-27b-3p, miR-142-3p, let-7i, miR-107, and miR-135b-5p) at 48 to 72 h after sports-related concussion that correlated with reaction time on ImPACT testing and predicted concussion better than other protein biomarkers [80].
Conclusion
TBI biomarkers measured through a simple blood test have the potential to provide invaluable information for the management of concussion by facilitating diagnosis and risk stratification; offering timely information about the pathophysiology of injury; monitoring recovery; and furnishing opportunities for drug target identification and surrogate measures for future clinical trials. In light of their timeliness, accuracy, and risk stratification potential, biofluid biomarkers with reliable sensitivity and specificity would be welcomed tools in treating concussion. This is especially so in settings limited by acute care resources such as in rural settings and non-hospital environments such as the playing field, battlefield, and primary care practices.
References
Papa L. Potential blood-based biomarkers for concussion. Sports Med Arthrosc Rev. 2016;24:108–15.
Papa L, Mittal MK, Ramirez J, et al. In children and youth with mild and moderate traumatic brain injury, glial fibrillary acidic protein out-performs S100beta in detecting traumatic intracranial lesions on computed tomography. J Neurotrauma. 2016;33:58–64.
Papa L, Zonfrillo MR, Ramirez J, et al. Performance of glial fibrillary acidic protein in detecting traumatic intracranial lesions on computed tomography in children and youth with mild head trauma. Acad Emerg Med. 2015;22:1274–82.
Papa L, Ramia MM, Kelly JM, Burks SS, Pawlowicz A, Berger RP. Systematic review of clinical research on biomarkers for pediatric traumatic brain injury. J Neurotrauma. 2013;30:324–38.
Papa L, Ramia MM, Edwards D, Johnson BD, Slobounov SM. Systematic review of clinical studies examining biomarkers of brain injury in athletes after sports-related concussion. J Neurotrauma. 2015;32:661–73.
Papa L. Exploring the role of biomarkers for the diagnosis and management of traumatic brain injury patients. In: Man TK, Flores RJ, editors. Poteomics – human diseases and protein functions. 1st ed. In Tech Open Access Publisher; 2012.
Papa L, Edwards D, Ramia M. Exploring serum biomarkers for mild traumatic. In: Kobeissy FH, editor. Brain neurotrauma: molecular, neuropsychological, and rehabilitation aspects. Boca Raton: Taylor & Francis Group; 2015.
Papa L, Wang KKW. Raising the bar for traumatic brain injury biomarker research: methods make a difference. J Neurotrauma. 2017;34:2187–9.
Pelinka LE, Kroepfl A, Leixnering M, Buchinger W, Raabe A, Redl H. GFAP versus S100B in serum after traumatic brain injury: relationship to brain damage and outcome. J Neurotrauma. 2004;21:1553–61.
Papa L, Silvestri S, Brophy GM, et al. GFAP out-performs S100beta in detecting traumatic intracranial lesions on computed tomography in trauma patients with mild traumatic brain injury and those with extracranial lesions. J Neurotrauma. 2014;31:1815–22.
Papa L, Robinson G, Oli M, et al. Use of biomarkers for diagnosis and management of traumatic brain injury patients. Expert Opin Med Diagn. 2008;2:937–45.
Tongaonkar P, Chen L, Lambertson D, Ko B, Madura K. Evidence for an interaction between ubiquitin-conjugating enzymes and the 26S proteasome. Mol Cell Biol. 2000;20:4691–8.
Gong B, Leznik E. The role of ubiquitin C-terminal hydrolase L1 in neurodegenerative disorders. Drug News Perspect. 2007;20:365–70.
Papa L, Lewis LM, Falk JL, et al. Elevated levels of serum glial fibrillary acidic protein breakdown products in mild and moderate traumatic brain injury are associated with intracranial lesions and neurosurgical intervention. Ann Emerg Med. 2012;59:471–83.
Papa L, Brophy GM, Welch RD, et al. Time course and diagnostic accuracy of glial and neuronal blood biomarkers GFAP and UCH-L1 in a large cohort of trauma patients with and without mild traumatic brain injury. JAMA Neurol. 2016;73:551–60.
Metting Z, Wilczak N, Rodiger LA, Schaaf JM, van der Naalt J. GFAP and S100B in the acute phase of mild traumatic brain injury. Neurology. 2012;78:1428–33.
Papa L, Lewis LM, Silvestri S, et al. Serum levels of ubiquitin C-terminal hydrolase distinguish mild traumatic brain injury from trauma controls and are elevated in mild and moderate traumatic brain injury patients with intracranial lesions and neurosurgical intervention. J Trauma Acute Care Surg. 2012;72:1335–44.
Welch RD, Ellis M, Lewis LM, et al. Modeling the kinetics of serum glial fibrillary acidic protein, ubiquitin carboxyl-terminal hydrolase-L1, and S100B concentrations in patients with traumatic brain injury. J Neurotrauma. 2017;34:1957–71.
Lewis LM, Schloemann DT, Papa L, et al. Utility of serum biomarkers in the diagnosis and stratification of mild traumatic brain injury. Acad Emerg Med. 2017;24:710–20.
Bazarian JJ, Biberthaler P, Welch RD, et al. Serum GFAP and UCH-L1 for prediction of absence of intracranial injuries on head CT (ALERT-TBI): a multicentre observational study. Lancet Neurol. 2018;17:782–9.
Papa L, Mittal MK, Ramirez J, et al. Neuronal biomarker ubiquitin C-terminal hydrolase detects traumatic intracranial lesions on computed tomography in children and youth with mild traumatic brain injury. J Neurotrauma. 2017;34:2132–40.
Papa L, Zonfrillo MR, Welch RD, et al. Evaluating glial and neuronal blood biomarkers GFAP and UCH-L1 as gradients of brain injury in concussive, subconcussive and non-concussive trauma: a prospective cohort study. BMJ Paediatr Open. 2019;3:e000473.
FDA authorizes marketing of first blood test to aid in the evaluation of concussion in adults. US Food & Drug Administration. 2018. Accessed July 2, 2018.
Yue JK, Yuh EL, Korley FK, et al. Association between plasma GFAP concentrations and MRI abnormalities in patients with CT-negative traumatic brain injury in the TRACK-TBI cohort: a prospective multicentre study. Lancet Neurol. 2019;18:953–61.
Zhou Y, Kierans A, Kenul D, et al. Mild traumatic brain injury: longitudinal regional brain volume changes. Radiology. 2013;267:880–90.
Bailes JE, Petraglia AL, Omalu BI, Nauman E, Talavage T. Role of subconcussion in repetitive mild traumatic brain injury. J Neurosurg. 2013;119:1235–45.
Bailes JE, Dashnaw ML, Petraglia AL, Turner RC. Cumulative effects of repetitive mild traumatic brain injury. Prog Neurol Surg. 2014;28:50–62.
Tate CM, Wang KK, Eonta S, et al. Serum brain biomarker level, neurocognitive performance, and self-reported symptom changes in soldiers repeatedly exposed to low-level blast: a breacher pilot study. J Neurotrauma. 2013;30:1620–30.
Gavett BE, Stern RA, McKee AC. Chronic traumatic encephalopathy: a potential late effect of sport-related concussive and subconcussive head trauma. Clin Sports Med. 2011;30:179–88, xi.
Huber BR, Alosco ML, Stein TD, McKee AC. Potential long-term consequences of concussive and subconcussive injury. Phys Med Rehabil Clin N Am. 2016;27:503–11.
Meier TB, Nelson LD, Huber DL, Bazarian JJ, Hayes RL, McCrea MA. Prospective assessment of acute blood markers of brain injury in sport-related concussion. J Neurotrauma. 2017;34:3134–42.
Joseph JR, Swallow JS, Willsey K, et al. Elevated markers of brain injury as a result of clinically asymptomatic high-acceleration head impacts in high-school football athletes. J Neurosurg. 2018:1–7.
Asken BM, Bauer RM, DeKosky ST, et al. Concussion BASICS III: serum biomarker changes following sport-related concussion. Neurology. 2018;91:e2133–e43.
Puvenna V, Brennan C, Shaw G, et al. Significance of ubiquitin carboxy-terminal hydrolase L1 elevations in athletes after sub-concussive head hits. PLoS One. 2014;9:e96296.
Zimmer DB, Cornwall EH, Landar A, Song W. The S100 protein family: history, function, and expression. Brain Res Bull. 1995;37:417–29.
Olsson B, Zetterberg H, Hampel H, Blennow K. Biomarker-based dissection of neurodegenerative diseases. Prog Neurobiol. 2011;95:520–34.
Schulte S, Podlog LW, Hamson-Utley JJ, Strathmann FG, Struder HK. A systematic review of the biomarker S100B: implications for sport-related concussion management. J Athl Train. 2014;49:830–50.
Heidari K, Vafaee A, Rastekenari AM, et al. S100B protein as a screening tool for computed tomography findings after mild traumatic brain injury: systematic review and meta-analysis. Brain Inj. 2015;29:1146–57.
Ingebrigtsen T, Romner B. Management of minor head injuries in hospitals in Norway. Acta Neurol Scand. 1997;95:51–5.
Waterloo K, Ingebrigtsen T, Romner B. Neuropsychological function in patients with increased serum levels of protein S-100 after minor head injury. Acta Neurochir. 1997;139:26–31; discussion 31−2.
Ingebrigtsen T, Romner B. Serial S-100 protein serum measurements related to early magnetic resonance imaging after minor head injury. Case report. J Neurosurg. 1996;85:945–8.
Ingebrigtsen T, Waterloo K, Jacobsen EA, Langbakk B, Romner B. Traumatic brain damage in minor head injury: relation of serum S-100 protein measurements to magnetic resonance imaging and neurobehavioral outcome. Neurosurgery. 1999;45:468–75; discussion 75–6.
Heidari K, Asadollahi S, Jamshidian M, Abrishamchi SN, Nouroozi M. Prediction of neuropsychological outcome after mild traumatic brain injury using clinical parameters, serum S100B protein and findings on computed tomography. Brain Inj. 2015;29:33–40.
Bazarian JJ, Zemlan FP, Mookerjee S, Stigbrand T. Serum S-100B and cleaved-tau are poor predictors of long-term outcome after mild traumatic brain injury. Brain Inj. 2006;20:759–65.
Lima DP, Simao Filho C, Abib Sde C, de Figueiredo LF. Quality of life and neuropsychological changes in mild head trauma. Late analysis and correlation with S100B protein and cranial CT scan performed at hospital admission. Injury. 2008;39:604–11.
Dorminy M, Hoogeveen A, Tierney RT, Higgins M, McDevitt JK, Kretzschmar J. Effect of soccer heading ball speed on S100B, sideline concussion assessments and head impact kinematics. Brain Inj. 2015;29:1158–64.
Kiechle K, Bazarian JJ, Merchant-Borna K, et al. Subject-specific increases in serum S-100B distinguish sports-related concussion from sports-related exertion. PLoS One. 2014;9:e84977.
Shahim P, Tegner Y, Wilson DH, et al. Blood biomarkers for brain injury in concussed professional ice hockey players. JAMA Neurol. 2014;71:684–92.
Kawata K, Rubin LH, Takahagi M, et al. Subconcussive impact-dependent increase in plasma S100beta levels in collegiate football players. J Neurotrauma. 2017;34:2254–60.
Zonner SW, Ejima K, Bevilacqua ZW, et al. Association of increased serum S100B levels with high school football subconcussive head impacts. Front Neurol. 2019;10:327.
Babcock L, Byczkowski T, Wade SL, Ho M, Bazarian JJ. Inability of S100B to predict postconcussion syndrome in children who present to the emergency department with mild traumatic brain injury: a brief report. Pediatr Emerg Care. 2013;29:458–61.
Pelinka LE, Kroepfl A, Schmidhammer R, et al. Glial fibrillary acidic protein in serum after traumatic brain injury and multiple trauma. J Trauma. 2004;57:1006–12.
Teunissen CE, Dijkstra C, Polman C. Biological markers in CSF and blood for axonal degeneration in multiple sclerosis. Lancet Neurol. 2005;4:32–41.
Kosik KS, Finch EA. MAP2 and tau segregate into dendritic and axonal domains after the elaboration of morphologically distinct neurites: an immunocytochemical study of cultured rat cerebrum. J Neurosci. 1987;7:3142–53.
Higuchi M, Lee VM, Trojanowski JQ. Tau and axonopathy in neurodegenerative disorders. NeuroMolecular Med. 2002;2:131–50.
Shaw GJ, Jauch EC, Zemlan FP. Serum cleaved tau protein levels and clinical outcome in adult patients with closed head injury. Ann Emerg Med. 2002;39:254–7.
Chatfield DA, Zemlan FP, Day DJ, Menon DK. Discordant temporal patterns of S100beta and cleaved tau protein elevation after head injury: a pilot study. Br J Neurosurg. 2002;16:471–6.
Ma M, Lindsell CJ, Rosenberry CM, Shaw GJ, Zemlan FP. Serum cleaved tau does not predict postconcussion syndrome after mild traumatic brain injury. Am J Emerg Med. 2008;26:763–8.
Bulut M, Koksal O, Dogan S, et al. Tau protein as a serum marker of brain damage in mild traumatic brain injury: preliminary results. Adv Ther. 2006;23:12–22.
Rubenstein R, Chang B, Davies P, Wagner AK, Robertson CS, Wang KK. A novel, ultrasensitive assay for tau: potential for assessing traumatic brain injury in tissues and biofluids. J Neurotrauma. 2015;32:342–52.
Rubenstein R, Chang B, Yue JK, et al. Comparing plasma phospho tau, total tau, and phospho tau-total tau ratio as acute and chronic traumatic brain injury biomarkers. JAMA Neurol. 2017;74:1063–72.
Puvenna V, Engeler M, Banjara M, et al. Is phosphorylated tau unique to chronic traumatic encephalopathy? Phosphorylated tau in epileptic brain and chronic traumatic encephalopathy. Brain Res. 2016;1630:225–40.
Alosco ML, Tripodis Y, Fritts NG, et al. Cerebrospinal fluid tau, Abeta, and sTREM2 in Former National Football League Players: modeling the relationship between repetitive head impacts, microglial activation, and neurodegeneration. Alzheimers Dement. 2018;14:1159–70.
Julien JP, Mushynski WE. Neurofilaments in health and disease. Prog Nucleic Acid Res Mol Biol. 1998;61:1–23.
Buki A, Povlishock JT. All roads lead to disconnection?--traumatic axonal injury revisited. Acta Neurochir. 2006;148:181–93; discussion 93-4.
Siman R, Toraskar N, Dang A, et al. A panel of neuron-enriched proteins as markers for traumatic brain injury in humans. J Neurotrauma. 2009;26:1867–77.
Zurek J, Bartlova L, Fedora M. Hyperphosphorylated neurofilament NF-H as a predictor of mortality after brain injury in children. Brain Inj. 2012;25:221–6.
Vajtr D, Benada O, Linzer P, et al. Immunohistochemistry and serum values of S-100B, glial fibrillary acidic protein, and hyperphosphorylated neurofilaments in brain injuries. Soud Lek. 2013;57:7–12.
Shahim P, Zetterberg H, Tegner Y, Blennow K. Serum neurofilament light as a biomarker for mild traumatic brain injury in contact sports. Neurology. 2017;88:1788–94.
Wirsching A, Chen Z, Bevilacqua ZW, Huibregtse ME, Kawata K. Association of acute increase in plasma neurofilament light with repetitive subconcussive head impacts: a pilot randomized control trial. J Neurotrauma. 2019;36:548–53.
Wallace C, Zetterberg H, Blennow K, van Donkelaar P. No change in plasma tau and serum neurofilament light concentrations in adolescent athletes following sport-related concussion. PLoS One. 2018;13:e0206466.
Jin XF, Wu N, Wang L, Li J. Circulating microRNAs: a novel class of potential biomarkers for diagnosing and prognosing central nervous system diseases. Cell Mol Neurobiol. 2013;33:601–13.
Balakathiresan N, Bhomia M, Chandran R, Chavko M, McCarron RM, Maheshwari RK. MicroRNA let-7i is a promising serum biomarker for blast-induced traumatic brain injury. J Neurotrauma. 2012;29:1379–87.
Bhomia M, Balakathiresan NS, Wang KK, Papa L, Maheshwari RKA. Panel of serum MiRNA biomarkers for the diagnosis of severe to mild traumatic brain injury in humans. Sci Rep. 2016;6:28148.
Hicks SD, Johnson J, Carney MC, et al. Overlapping microRNA expression in saliva and cerebrospinal fluid accurately identifies pediatric traumatic brain injury. J Neurotrauma. 2017;35(1):64–72.
Johnson JJ, Loeffert AC, Stokes J, Olympia RP, Bramley H, Hicks SD. Association of salivary microRNA changes with prolonged concussion symptoms. JAMA Pediatr. 2018;172:65–73.
Mitra B, Rau TF, Surendran N, et al. Plasma micro-RNA biomarkers for diagnosis and prognosis after traumatic brain injury: a pilot study. J Clin Neurosci. 2017;38:37–42.
Papa L, Slobounov SM, Breiter HC, et al. Elevations in microRNA biomarkers in serum are associated with measures of concussion, neurocognitive function, and subconcussive trauma over a single National Collegiate Athletic Association Division I Season in collegiate football players. J Neurotrauma. 2019;36:1343–51.
Abbas K, Shenk TE, Poole VN, et al. Alteration of default mode network in high school football athletes due to repetitive subconcussive mild traumatic brain injury: a resting-state functional magnetic resonance imaging study. Brain Connect. 2015;5:91–101.
Di Pietro V, Porto E, Ragusa M, et al. Salivary microRNAs: diagnostic markers of mild traumatic brain injury in contact-sport. Front Mol Neurosci. 2018;11:290.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Papa, L. (2021). Biomarkers for Concussion. In: Slobounov, S.M., Sebastianelli, W.J. (eds) Concussions in Athletics. Springer, Cham. https://doi.org/10.1007/978-3-030-75564-5_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-75564-5_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-75563-8
Online ISBN: 978-3-030-75564-5
eBook Packages: MedicineMedicine (R0)