
Abstract
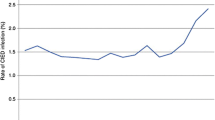
The rates of cardiovascular implantable electronic device (CIED) implantation have increased significantly since their introduction in 1958. Not only advances in CIED technology but also the expanding number of indications for device therapy, such as the use of the implantable cardioverter-defibrillator (ICD) and cardiac resynchronization therapy (CRT), led to this increase. In parallel, the rate of CIED infection (CIEDI) has increased as well. The probability of CIEDI was higher among patients with ICDs than among those with pacemakers. Infection after CIED implantation remains a major complication with significant morbidity and mortality. Scientific statements from the American Heart Association (AHA) and the Heart Rhythm Society (HRS) both recommend complete device and lead removal in patients with definite CIEDI. In this chapter, data will be presented on reimplantation, recurrent infection and mortality among patients who underwent removal of the infected device and lead system. In addition, strategies to minimize the risk of adverse outcome are presented.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keyword
8.1 Reimplantation
Complete device removal is a class I recommendation in all cases of pocket infection and endocarditis, regardless of whether there is definitive evidence of device involvement [1]. When considering device reimplantation after infection, there is a variety of reimplantation strategies. The vast majority of patients who underwent CIED extraction undergo device reimplantation. However, up to 40% of patients do not require reimplantation as reported in several series [2,3,4,5,6]. The Multicenter Electrophysiologic Device Infection Cohort (MEDIC) prospective registry enrolled 434 patients with device infections [3]. Of these, device removal was completed in 381 patients (88%) and 53 patients (12%) did not undergo device removal due to various physician justifications. Among the 381 patients who had device removal, 220 (58%) underwent reimplantation and 161 (42%) did not require reimplantation. Reasons for not reimplanting devices include improved ejection fraction, recovery of sinus function and improvement of symptomatic bradycardia. The study by Al-Hijji et al. reported that approximately 14% of patients do not receive CIED reimplant after extraction [2]. Approximately 70% of the patients without reimplant either did not meet any indication for ongoing device therapy or their device was not indicated at the index implantation according to current guidelines. During follow-up, the mortality rate was higher in the no-reimplant group compared to the reimplant group. However, the higher mortality rate was mainly driven by noncardiac comorbidity, device complications and infection (Fig. 8.1).

Survival and cause of death of reimplanted versus not reimplanted patients after TLE for CIEDI (Kaplan-Meier curve figure reproduced from Al-Hijji et al [2] with permission). The table on the right shows the cause of deaths reported by authors and the result of multivariate analysis as reported in the paper (main independent predictors of mortality were CIED-related complication and extraction for infective cause). Legend: HR, hazard ratio; TLE, transvenous lead extraction
The timing and approach to reimplant devices are major concerns in managing CIEDI. The 2017 HRS expert consensus report on transvenous lead extraction (TLE) recommends new device implantation in patients treated by antimicrobial therapy for 3 to 14 days after extraction [1]. In fact, new CIED implantation can reasonably be postponed until blood cultures are negative for 3 days. The timing of reimplantation in the MEDIC registry varied considerably among the study population [3]. The median time was 10 days, interquartile range of 6 to 19 days; in all, 70% of patients were reimplanted within 2 weeks. As suggested by existing guidelines, patients were treated differently when they had confirmed infective endocarditis (IE). Patients with IE were reimplanted at a median of 13 days, while those without IE were treated at a median of 8 days. Considering the potential gravity of prosthetic material infections, CIED should be reimplanted while taking the greatest precautions to prevent recurrent infections. [For additional information on CIED reimplant approaches see Chap. 7.]
8.2 Recurrent Infection After Transvenous Lead Extraction
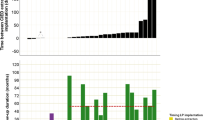
The true incidence of recurrent infection after TLE for infection is hampered due to limited data on long-term outcome after TLE [7,8,9]. Reported data are primarily based on single-centre studies (Fig. 8.2). A recent single-centre study demonstrated an overall repeat TLE rate of 6% (including all indications) during a mean follow-up of 5.5 years [9]. Of the patients who underwent initial TLE for infection, the incidence of recurrent infection requiring TLE was 4% (15 of 419 patients). Maytin et al. demonstrated an incidence of recurrent infection requiring TLE of 2% (10 of 520 patients) during a mean follow-up of 3.7 years [7]. Patients underwent the repeat TLE procedure for infection at a mean of 21 months (range 1–53 months) after the initial procedure. It is important to realize that not all patients experiencing a CIED recurrent infection undergo TLE due to poor candidacy (e.g., elderly patients with multiple comorbidities) or patient refusal. Therefore, the true incidence of CIED recurrent infection post-TLE may be higher. This is demonstrated by a single-centre study from Australia [8]. In this study, the incidence of recurrent device infection was 6% (20 of 331 patients) post-TLE for infection. Of the patients with recurrent device infection, 7 (35%) were medically managed and 13 (65%) underwent repeat TLE (thus 4% repeat TLE rate for infection). Based on above-mentioned data from high-volume centres, the incidence of CIED recurrent infection post-TLE is estimated at 6% and the CIED reinfection rate requiring repeat TLE is around 2–4%.

Main studies on follow-up after TLE. Main studies on long-term follow-up for reinfection after TLE [7,8,9]. The graphic reports the size of the cohort, the rate of patients with an indication of TLE for infection (splitted by local or systemic infection when data were provided from the paper), the rate of relapse (among those admitted for infection) and the percentage of patients who repeated TLE. Legend: LI, local infections; N, number of patients; SI, systemic infections; TLE, transvenous lead extraction
Considering the risk of recurrent infection, one may wonder whether this is due to an ongoing (latent) infection despite initial TLE. In a retrospective single-centre study, five patients had positive microbiology at initial and repeat TLE of which the same organism was identified at initial and repeat TLE in the same individual in only two cases (coagulase-negative staphylococcus in both cases) [9]. Thus, it is more likely that patients have a predisposition to infection even if there is apparent sterilization at the initial procedure [9, 10]. There are several clinical and procedural factors associated with CIEDI, including end-stage renal disease, diabetes mellitus, chronic obstructive pulmonary disease, use of immunosuppressive drugs, older age, pocket hematoma and longer procedure duration [11, 12]. It is likely that these risk factors are also important for reinfection after TLE for infection. With regard to the TLE procedure, it is important to aim for complete lead removal. Retained lead fragments have been associated with a higher reinfection rate [3, 8].
The occurrence of reinfection requiring TLE seems to be associated with a poorer outcome (Fig. 8.3) [13]. In a single-centre study, all-cause mortality was 36% for those who underwent repeat TLE for infection compared to 5% in those where repeat TLE was indicated for lead problems [9]. The 36% mortality rate was also higher when compared with patients who had undergone a single TLE for infection (23%, P = 0.02). In addition, multiple studies have shown a higher all-cause mortality in patients undergoing initial TLE for infectious indications in comparison to patients undergoing TLE for other indications [3, 7, 8]. Thus, the prognosis of patients undergoing a repeat TLE for infection is poor. Every effort should be taken to lower the risk of recurrent infection. This could be achieved with early diagnosis of CIEDI and performing complete device and lead removal within a relatively short time after diagnosis.

Comparison of survival from death alone or the composite endpoint of death or CIED infection in a prospective cohort of patients undergoing TLE for CIEDI. No statistic difference was shown at the long-rank test between these two curves at any timepoint: 30, 60, 90, 180 and 365 days or complete follow-up. (Reproduced from Diemberger et al. [13] with permission)
8.3 Mortality After Transvenous Lead Extraction
Transvenous lead extraction has been associated with a risk of major adverse events, including vascular laceration, cardiac avulsion, pericardial effusion, hemothorax and death [1]. Recently, data of 11,304 extraction procedures from the National Cardiovascular Data Registry ICD Registry were analysed [14]. In-hospital mortality during TLE was observed in 98 (0.9%) patients. Among these, 44 (44%) patients underwent TLE for CIEDI. Urgent cardiac surgery was required in 41 (0.36%) patients, of which 14 died either during surgery or immediately post-op. The European Lead Extraction ConTRolled Registry (ELECTRa) reported on the outcomes of 3555 patients who underwent TLE [15]. The in-hospital procedure-related major complication rate was 1.7% including a mortality rate of 0.5%. Major conclusions of both registries were high success rates and low major procedure-related complications. Most importantly, it was clearly demonstrated that procedure-related complication and peri-procedural mortality rates are the lowest among high-volume and experienced centres.
Data concerning short- and long-term outcomes is steadily increasing. In a retrospective cohort analysis of 176 patients who required TLE, mortality rates of 3.4% at 30 days and 8.5% at 1 year were reported [16]. Among patients who required TLE because of CIED systemic infection, mortality rates increased to 19% at 30 days, 32% at 1 year and 39% during long-term follow-up, as compared with a long-term mortality of only 12% in patients who required TLE for other reasons. In a similar study, Maytin et al. also demonstrated an increased risk of mortality associated with CIEDI [7]. In their cohort, mortality at 1 year was nearly 25% among patients with systemic infection compared to less than 10% among those with local infection. Henrikson et al. reported the outcomes of 67 patients undergoing TLE because of infective indications [17]. The overall mortality rate of patients with systemic infection was 44%. Considering the data from NCDR ICD registry and ELECTRa, mortality risk directly related to the TLE procedure is relatively low (<1%), but 1-year mortality rate as observed in single-centre studies is high, particularly in patients with systemic infection. Risk assessment in patients undergoing TLE is underestimated and may be related to the focus on procedural risk. A few studies focused on predictors for long-term outcome after TLE.
Tarakji et al. evaluated risk factors for 1-year mortality among patients with CIEDI and examined the association between the type of infection and the mortality risk [18]. Data of 502 consecutive patients who underwent CIED removal for the indication of device-related infection were analysed. A total of 102 (20.3%) patients died within the first year after CIED removal. Risk factors for 1-year mortality among patients with CIEDI undergoing system removal include dementia, renal insufficiency, worse functional class, use of anticoagulation, bleeding requiring transfusion and CIED-related systemic infection as opposed to pocket infection. Higher mortality risk among patients with systemic infection seems unrelated to the presence of vegetations on TEE. Habib et al. evaluated data of 415 patients with CIEDI in order to identify risk factors associated with short-term (30 days) and long-term (>30 days) mortality [19]. Factors associated with long-term mortality included patient age, heart failure, metastatic malignancy, corticosteroid therapy, renal failure and CIED-related systemic infection. Another study found the presence of chronic kidney disease, increased numbers of leads to extract, lower ejection fraction and procedural failure as predictors of mortality [20]. Caution must be taken as in this study, the majority of patients underwent TLE particularly for non-infectious reasons. Taken the studies together, the data suggest that the development of CIED-related systemic infection and the presence of co-morbid conditions are associated with short- and long-term mortality in patients with CIEDI (Table 8.1) [7, 13, 16,17,18,19,20,21].
When most risk factors are taken into account such as in the IKAR risk score model, mortality can be predicted with a reasonable accuracy [21]. The IKAR risk score was derived in a single-centre cohort of 130 patients; the abbreviation of IKAR stands for: I, infectious; K, kidney; A, age; and R, removal of high-voltage leads. Patients with IKAR score ≥3 points were characterized by 79% mortality as compared to 16% for those with a score of 1–2 points. The proposed risk score may be helpful in making individual statements on mortality risk prior to TLE. However, the proposed risk should not disqualify patients from the TLE procedure. To determine the performance of this score, analysis in a larger multicentre series is warranted.
8.4 Strategies to Minimize the Risk of Adverse Outcomes
In clinical practice, CIED removal is often delayed in favour of initial trials of antimicrobial therapy alone. The consequences of sustained infection despite appropriate antimicrobial therapy and recurrent infection are well recognized. Early diagnosis of CIED-related infection and performing TLE within 3 days of diagnosis has been associated with lower in-hospital mortality. Based on this, early and complete CIED removal is critical in the management of CIED-related infection, regardless of the timing of the start of antimicrobial therapy.
Patients requiring TLE should be referred to dedicated centres with appropriate training and experience. Optimal cardiothoracic surgical backup at centres performing is imperative as a 16% incidence of requiring urgent cardiac surgery with a high mortality rate among these patients was observed in the NCDR ICD registry.
After CIED removal, reassessment of the need for a new CIED is imperative. Some patients may no longer meet guideline indications for permanent bradycardia pacing, ICD or CRT, and some patients might not wish to receive a new device. A new CIED implantation can reasonable be postponed until blood cultures are negative for 3 days. Reimplantation should be performed in an alternative location such as the contralateral side or using epicardial or subcutaneous implantation. Patients without the indication for bradycardia pacing, antitachycardia pacing or CRT are eligible for a subcutaneous ICD (S-ICD) system. The S-ICD involves no hardware exposed to the intravascular system, which reduces the risk of systemic infection. In a sub-analysis of the EFFORTLESS registry (Fig. 8.4), the S-ICD is a viable alternative for patients who underwent removal of a transvenous ICD system [22]. The risk of recurrent infection remains low even in patients whose devices were removed because of infection. [For additional information on new CIED devices to minimize CIEDI see Chap. 10.]

Subcutaneous implantable defibrillator (S-ICD) represents a safe option for reimplantation of patients after transvenous lead extraction. Kaplan-Meier curves for freedom from infection and for mortality show a favourable outcome in patients implanted with S-ICD after a lead extraction for infection (blue line). From Boersma et al [22] (Reproduced with permission)
A method to reduce recurrent infection after TLE may be the use of antibacterial envelope (TYRX™) in patients at high risk for mortality. Data from non-randomized cohort studies have indicated that the use of an antibacterial envelope can reduce the incidence of CIEDI by more than 80% in high-risk patients. Data from the Worldwide Randomized Antibiotic Envelope Infection Prevention Trial (WRAP-IT) demonstrated that the use of an antibacterial envelope resulted in a 40% lower incidence of CIEDI compared to standard-of-care infection prevention strategies alone [23]. However, the antibacterial envelope was used at initial implant, replacement, or upgrade. Data regarding implantation after TLE is lacking. [For additional information see Chap. 11.]
References
Kusumoto FM, Schoenfeld MH, Wilkoff BL, Berul CI, Birgersdotter-Green UM, Carrillo R, et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017;14(12):e503–e51.
Al-Hijji MA, Killu AM, Yousefian O, Hodge DO, Park JY, Hebsur S, et al. Outcomes of lead extraction without subsequent device reimplantation. Europace. 2017;19(9):1527–34.
Boyle TA, Uslan DZ, Prutkin JM, Greenspon AJ, Baddour LM, Danik SB, et al. Reimplantation and repeat infection after cardiac-implantable electronic device infections: experience from the MEDIC (multicenter Electrophysiologic device infection cohort) database. Circ Arrhythm Electrophysiol. 2017;10(3)
Deharo JC, Quatre A, Mancini J, Khairy P, Le Dolley Y, Casalta JP, et al. Long-term outcomes following infection of cardiac implantable electronic devices: a prospective matched cohort study. Heart. 2012;98(9):724–31.
Sohail MR, Uslan DZ, Khan AH, Friedman PA, Hayes DL, Wilson WR, et al. Management and outcome of permanent pacemaker and implantable cardioverter-defibrillator infections. J Am Coll Cardiol. 2007;49(18):1851–9.
Tarakji KG, Chan EJ, Cantillon DJ, Doonan AL, Hu T, Schmitt S, et al. Cardiac implantable electronic device infections: presentation, management, and patient outcomes. Heart Rhythm. 2010;7(8):1043–7.
Maytin M, Jones SO, Epstein LM. Long-term mortality after transvenous lead extraction. Circ Arrhythm Electrophysiol. 2012;5(2):252–7.
Gomes S, Cranney G, Bennett M, Giles R. Long-term outcomes following Transvenous Lead extraction. Pacing Clin Electrophysiol. 2016;39(4):345–51.
Claridge S, Johnson J, Sadnan G, Behar JM, Porter B, Sieniewicz B, et al. Predictors and outcomes of patients requiring repeat transvenous lead extraction of pacemaker and defibrillator leads. Pacing Clin Electrophysiol. 2018;41(2):155–60.
Alagna L, Park LP, Nicholson BP, Keiger AJ, Strahilevitz J, Morris A, et al. Repeat endocarditis: analysis of risk factors based on the international collaboration on endocarditis - prospective cohort study. Clin Microbiol Infect. 2014;20(6):566–75.
Guha A, Maddox WR, Colombo R, Nahman NS Jr, Kintziger KW, Waller JL, et al. Cardiac implantable electronic device infection in patients with end-stage renal disease. Heart Rhythm. 2015;12(12):2395–401.
Polyzos KA, Konstantelias AA, Falagas ME. Risk factors for cardiac implantable electronic device infection: a systematic review and meta-analysis. Europace. 2015;17(5):767–77.
Diemberger I, Biffi M, Lorenzetti S, Martignani C, Raffaelli E, Ziacchi M, Rapezzi C, Pacini D, Boriani G. Predictors of long-term survival free from relapses after extraction of infected CIED. Europace. 2018;20(6):1018–27.
Sood N, Martin DT, Lampert R, Curtis JP, Parzynski C, Clancy J. Incidence and predictors of perioperative complications with Transvenous Lead extractions: real-world experience with National Cardiovascular Data Registry. Circ Arrhythm Electrophysiol. 2018;11(2):e004768.
Bongiorni MG, Kennergren C, Butter C, Deharo JC, Kutarski A, Rinaldi CA, et al. The European Lead Extraction ConTRolled (ELECTRa) study: a European Heart Rhythm Association (EHRA) registry of transvenous lead extraction outcomes. Eur Heart J. 2017;38(40):2995–3005.
Deckx S, Marynissen T, Rega F, Ector J, Nuyens D, Heidbuchel H, et al. Predictors of 30-day and 1-year mortality after transvenous lead extraction: a single-Centre experience. Europace. 2014;16(8):1218–25.
Henrikson CA, Zhang K, Brinker JA. High mid-term mortality following successful lead extraction for infection. Pacing Clin Electrophysiol. 2011;34(1):32–6.
Tarakji KG, Wazni OM, Harb S, Hsu A, Saliba W, Wilkoff BL. Risk factors for 1-year mortality among patients with cardiac implantable electronic device infection undergoing transvenous lead extraction: the impact of the infection type and the presence of vegetation on survival. Europace. 2014;16(10):1490–5.
Habib A, Le KY, Baddour LM, Friedman PA, Hayes DL, Lohse CM, et al. Predictors of mortality in patients with cardiovascular implantable electronic device infections. Am J Cardiol. 2013;111(6):874–9.
Merchant FM, Levy MR, Kelli HM, Hoskins MH, Lloyd MS, Delurgio DB, et al. Predictors of long-term survival following transvenous extraction of defibrillator leads. Pacing Clin Electrophysiol. 2015;38(11):1297–303.
Oszczygiel E, Kutarski A, Oszczygiel A, Mankowska-Zaluska B, Chudzik M, Wranicz JK, et al. Risk score to assess mortality risk in patients undergoing transvenous lead extraction. Pacing Clin Electrophysiol. 2017;40(8):918–23.
Boersma L, Burke MC, Neuzil P, Lambiase P, Friehling T, Theuns DA, et al. Infection and mortality after implantation of a subcutaneous ICD after transvenous ICD extraction. Heart Rhythm. 2016;13(1):157–64.
Tarakji KG, Mittal S, Kennergren C, Corey R, Poole JE, Schloss E, et al. Antibacterial envelope to prevent cardiac implantable device infection. NEJM. 2019;380:1895–05. https://doi.org/10.1056/NEJMoa1901111.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Theuns, D.A., Yap, SC., Szili-Torok, T. (2020). Follow-Up and Prognosis After System Removal for Cardiac Device Infection. In: Diemberger, I., Boriani, G. (eds) Infections of Cardiac Implantable Devices. Springer, Cham. https://doi.org/10.1007/978-3-030-46255-0_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-46255-0_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-46254-3
Online ISBN: 978-3-030-46255-0
eBook Packages: MedicineMedicine (R0)