
Abstract
Many causes of male infertility are unknown, and for this reason, numerous studies have been carried out, analyzing gene expression, epigenetics modifications, and mostly the role of reactive oxygen species (ROS) and antioxidants. It is well recognized that oxidative stress is a cause of male infertility, but the use of antioxidants as a treatment is still debated, and it is considered as a supportive therapy, rather than etiological or physiopathological, on the real effect of oral supplementation. Oxidative stress is determined when there is an imbalance between the production of ROS and the neutralizing activity of antioxidant system. It leads to a pathological and often irremediable cell damage. In particular spermatozoa are very susceptible to oxygen effects because their membranes are rich in polyunsaturated fatty acids that assure fluidity and flexibility; this one makes spermatozoa more vulnerable to lipid peroxidation.
The most important sources of ROS in semen are immature spermatozoa and leucocytes, and the protective antioxidant system in semen is divided into enzymatic factors, such as superoxide dismutase, catalase, glutathione peroxidase, and peroxiredoxins, and nonenzymatic factors. We focused our attention on the main natural antioxidants, the efficacy of which has been supported by clinical trials. In particular our group focused on the study of coenzyme Q10 and carnitine, but we will also review the other main antioxidants.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Key Points-
Oxidant radical excess has been associated with male infertility. In particular many authors have focused on the role of reactive oxygen species (ROS).
-
Spermatozoa are very susceptible to oxygen effects because their membranes are rich in polyunsaturated fatty acids that assure fluidity and flexibility; this one makes spermatozoa more vulnerable to lipid peroxidation.
-
The most important sources of ROS in semen are immature spermatozoa and leucocytes, and the protective antioxidant system in semen is divided into enzymatic factors, such as superoxide dismutase, catalase, glutathione peroxidase, and peroxiredoxins, and nonenzymatic factors.
-
Carnitine, coenzyme Q10, vitamin E, vitamin C, zinc, and myo-inositol are the most important nonenzymatic systems for which a seminal parameter improvement was demonstrated.
-
There are emerging evidences that herbal products can also improve male reproductive functions.
1 Introduction
Infertility is defined as the failure to establish a clinical pregnancy after 12 months of regular and unprotected sexual intercourse. Infertility affects an estimated 15% of couples globally, especially in developed countries, with around 20–50% due to male factors [1].
Unfortunately, many causes of male infertility are unknown, and for this reason, numerous studies have been carried out, analyzing gene expression, epigenetics modifications, and mostly the role of reactive oxygen species (ROS) and antioxidants.
It is well recognized that oxidative stress is a cause of male infertility, but the use of antioxidants as a treatment is still debated, and it is considered as a supportive therapy, rather than etiological or physiopathological, on the real effect of oral supplementation. Many models have been introduced to explore the role of different antioxidants in vitro, and some differences can be discovered regarding the protective effects exerted by specific enzymatic or nonenzymatic molecules.
2 The Role of Reactive Oxygen Species
An oxidant radical excess has been associated with male infertility. In particular many authors have focused on the role of ROS [2, 3, 4].
In the last 20 years, an assay called “TOSC” (total oxyradical scavenging capacity) was developed to measure the total capacity of the biologic fluids or cellular antioxidants that neutralize oxygen radical toxicity. This assay has been used by our group in andrology, and it helped us to show a reduced antioxidant capacity in infertile men’s seminal fluid and a correlation between the scavenging action versus oxygen radicals and sperm cell parameters, in particular the motility [5, 6, 7]. Another parameter of antioxidant evaluation is the determination of total antioxidant capacity (TAC), the method that we employed in our laboratory [8], which is a modification of the method of Rice-Evans and Miller [9]. It is a kinetic assay, based on the reaction of H2O2-metmyoglobin with a chromogen (ABTS), whose radical species is spectroscopically detected. The latency time before the appearance of radical ABTS (lag phase or LAG, measured in sec) is proportional to the amount of small-chain-breaking molecules, which interrupt the propagation of oxidative reactions, mainly urate, ascorbate, and glutathione, and moreover, the rapid increase of ABTS is followed by a more gradual increase, in which antioxidant properties of proteins are involved. The interest of these parameters is based on its modulation by hormonal milieu: in fact we have shown that plasma LAG is lower in hypogonadism [10] and hypoadrenalism [11] and is influenced by growth hormone [12], another hormone involved in the control of fertility [13]. Even in seminal plasma, TAC exhibits a modulation by endocrine factors, since it is inversely related to systemic thyroid hormone levels [14].
Oxidative stress is determined when there is an imbalance between the production of ROS and the neutralizing activity of antioxidant system. It leads to a pathological and often irremediable cell damage. In particular spermatozoa are very susceptible to oxygen effects because their membranes are rich in polyunsaturated fatty acids that assure fluidity and flexibility; this one makes spermatozoa more vulnerable to lipid peroxidation [15]; in addition their cytoplasm is poor in scavenging systems. On the other hand, ROS are important for some processes like the sperm chromatin condensation, capacitation, acrosome reaction, cell signaling, and sperm motility [16].
The most important sources of ROS in semen are immature spermatozoa [17] and leucocytes [18], and the protective antioxidant system in semen is divided into enzymatic factors, such as superoxide dismutase, catalase, glutathione peroxidase, and peroxiredoxins [19], and nonenzymatic factors.
2.1 Nonenzymatic Systems
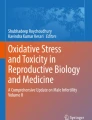
The first line of studies about antioxidants and fertility concerns dietary influences; in fact it is known that fertility is related to lifestyle [20, 21] and is an index of general health of men [22]. We have shown that modification of the diet in patients with metabolic syndrome, with enrichment of antioxidant by seasonal vegetable and fruits, has a synergy with metformin in reducing insulin resistance [23]; preliminary data shows that, in patients with metabolic syndrome during treatment with metformin , such kind of diet can influence testosterone levels (Fig. 43.1). Even if fertility has not been investigated in this pilot study, hormonal effects could be obviously important [24]. Moreover, a recent review of the literature about the influence of diet in male fertility indicated that a healthy diet improves at least one measure of semen quality, while diets high in lipophilic foods, soy isoflavones, and sweets lower semen quality [25]. However, the more diffuse approach was the effect of exogenous administration of antioxidants. We focused our attention on the main natural antioxidants, the efficacy of which has been supported by clinical trials. In particular our group focused on the study of coenzyme Q10 and carnitine, but we will also review the other main antioxidants.

Mean ± SEM levels of body mass index, HOMA-IR index, and testosterone levels in men with metabolic syndrome during metformin treatment: group A, hypocaloric diet; group B, hypocaloric diet enriched with natural antioxidants
2.1.1 Carnitine
L-carnitine (LC) or 3-aminobutyric acid is involved in intermediary metabolism being a shuttle of the activated long-chain fatty acids (acyl-Coa) into the mitochondria. The high levels found in epididymal fluid (2000 times higher than blood concentration) suggest the central role in sperm cell metabolism. There are evidences that show a positive correlation between an increase of L-carnitine in the epididymal lume and L-acetyl-carnitine (LAC) in sperm cells and initial sperm movement [26, 27]. Our group performed a 6-month double-blind randomized placebo-controlled trial using LC or LAC or combined LC and LAC treatment in infertile males affected by idiopathic asthenozoospermia [28]. The evaluation of the effectiveness of these treatments in improving semen kinetic parameters and the variation of TOSC in semen after treatment was the end points of the study. Sixty patients (mean age, 30 years) affected by idiopathic asthenozoospermia have been enrolled in the study, and all subjects underwent medical screening, including history and clinical examination, and presented a clinical history of primary infertility >2 years. The selected patients were submitted to a double-blind therapy of LC (10 ml phials containing 3 g/day orally of Carnitene – Sigma Tau, Italy, n. 15 patients), LAC (tablets containing 3 g/day orally of Zibren – Sigma Tau, n. 15 patients), and a combination of LC (10 ml phials containing 2 g/day orally of Carnitene) and LAC (tablets containing 1 g/day orally of Zibren) (n. 15 patients) or a seemingly identical placebo (each 10 ml placebo phial contains malic acid, sodium benzoate, sodium saccharinate dihydrate, anhydrous sodium citrate, pineapple flavoring, and demineralized water; each placebo tablet contains a core with l-hydro lactose, magnesium stearate, polyvinylpyrrolidone, and cornstarch and a coating with cellulose acetophtalate, dimethicone, and ethyl phthalate, Sigma Tau, Pomezia, Rome, Italy). All patients assumed a total of one phial and two tablets three times a day. The study design was 1-month run-in, 6 months of therapy (45 patients) or placebo (15 patients), and further 3 months of follow-up (controls at months T − 1, T0, T + 3, T + 6, and T + 9). Our results demonstrated that patients treated with the combination of the two molecules improved significantly during the first 3-month period of the administration. A significant improvement in total sperm motility was found in patients to whom LAC was administered, either alone or combined with LC. The analysis of forward sperm cell motility showed the same results. An improvement of forward motility was found when combined LC–LAC was compared with LC or LAC therapy alone, although the variations of kinetics sperm parameters were not significant. No significant modifications were found in placebo group. In all carnitine therapy groups, a significant dependence of the total and forward motility variations on the baseline values was found, and patients with lower baseline values of motility had a significantly higher probability to be responders to the treatment. Several controlled and uncontrolled studies support a potential positive effect of therapy with LC and its acyl derivatives in selected forms of oligo-astheno-teratozoospermia [29]. Lenzi et al. [30] demonstrated, in a controlled study, the efficacy of LC and LAC combined treatment in improving sperm motility , especially in patients with lower baseline levels. However, new evidence is needed to define the effective role and mechanisms of action of carnitine as an antioxidant.
2.1.2 Coenzyme Q10
Coenzyme Q10 , also called ubiquinone, is an important component of the mitochondrial oxidative phosphorylation process because of its role of redox link between flavoproteins and cytochromes in the inner mitochondrial membrane [31]. CoQ10 also plays an import role as antioxidant; it contributes to membrane fluidity and can participate in many aspect of redox control of the cellular signaling origin and transmission; it has a probable involvement in cellular proliferation [32]. Clinically the significance of antioxidant action of ubiquinone has been clarified by many studies on lipoproteins. In fact LDL proteins are very susceptible to oxidative stress, and reduced CoQ10 present in LDL is oxidized before vitamin E, and the appearance of fatty acid hydroperoxides occurs after the oxidation of ubiquinol [33]. It can be suggested a possible role in male infertility; in fact spermatozoa are rich in mitochondria, and they are strongly subject to oxidative stress. The previous coenzyme Q10 studies were performed with the administration of this antioxidant in cohort of unselected infertile patients, and the endogenous levels of CoQ10 were not measured [34, 35]. The first analytical data are represented by two of our works. The first one shows that the levels of CoQ10 in seminal plasma correlated with sperm count and motility except in the varicocele population. We also studied the varicocele patients after surgical repair, and the correlation between cellular CoQ10 and motility was no more detectable in postoperative VAR patients.
We conducted two different studies that showed an increase in spermatozoa motility in idiopathic asthenospermic patients undergoing CoQ10 therapy [36, 37].
We investigated the potential therapeutic role of CoQ10 by administering CoQ10 to a group of 22 idiopathic asthenozoospermic infertile patients [37], classified according to the WHO 1999 criteria [38] as having <50% forward motile forms at two distinct sperm analyses and normal sperm morphology >30%.
An increase of CoQ10 was found in seminal plasma after treatment, the mean value rising significantly from 42.0 ± 5.1 at baseline to 127.1 ± 1.9 ng/ml after 6 months of exogenous CoQ10 administration (p < 0.005). A significant increase of CoQ10 content was also detected in sperm cells (from 3.1 ± 0.4 to 6.5 ± 0.3 ng/106 cells; p < 0.05). Similarly, PC levels increased significantly both in seminal plasma and sperm cells after treatment (from 1.49 ± 0.50 to 5.84 ± 1.15 μM, p < 0.05, and from 6.83 ± 0.98 to 9.67 ± 1.23 nmoles/106 cells, p < 0.05, respectively).
Regarding semen, a significant difference was found in forward motility of sperm cells after 6 months of CoQ10 dietary implementation (from 9.13 ± 2.50 to 16.34 ± 3.43%, p < 0.05). The improvement of motility was also confirmed by means of computer-assisted determination of kinetic parameters. A significant increase of VCL (from 26.31 ± 1.50 to 46.43 ± 2.28 μm/s, p < 0.05) and VSL (from 15.20 ± 1.30 to 20.40 ± 2.17 μm/s, p < 0.05) was found after treatment. No significant differences were found in sperm cell concentration and morphology.
This study indicates a significant improvement of kinetic features of sperm cells after 6 months of administration of CoQ10, both on the basis of manual and computer-assisted evaluation. Moreover, these results constitute the first demonstration that exogenous administration of CoQ10 increases its levels in seminal plasma and in spermatozoa.
Similar increases of CoQ10 concentration (two to three times higher than baseline value) are commonly found in blood plasma after chronic administration of the quinine [39]. Statistical analysis did not reveal any significant functional relationship among the therapy-induced variations of CoQ10 and kinetic parameters of spermatozoa, probably due to the low number of samples. Nevertheless, the good degree of association among these variables, according to Cramer’s V index of association, supports the hypothesis of a pathogenetic role of CoQ10 in asthenozoospermia, according to previously reported data [40]. Improvement of the spontaneous pregnancy rate also suggests that this therapeutic approach is beneficial.
These results were confirmed by a double-blind, placebo-controlled clinical trial, also from our group [36]. The selected patients underwent a double-blind therapy with CoQ10 (Q-Absorb softgels, Jarrow Formulas LA, USA), containing 100 mg of CoQ10, lecithin, and medium-chain glycerides. Placebo had the same composition but the softgels did not contain any CoQ10. All patients were given a total of two soft capsules in two separate daily administrations, with meals. The CoQ10 dose was similar to that used in our previous open trial on male infertility.
The study design was 1-month run-in, 6 months of therapy (30 patients) or placebo (30 patients), and further 3 months of follow-up (controls at months T − 1, T0, T + 3, T + 6, and T + 9).
CoQ10 levels increased in seminal plasma after treatment, and a significant increase of CoQ10 content was also detected in sperm cells (from 2.44 ± 0.97 to 4.57 ± 2.46 ng/106 cells, p < 0.0001). Similarly, QH2 levels increased significantly both in seminal plasma and sperm cells after treatment (from 31.54 ± 10.05 to 51.93 ± 16.44 ng/ml, p < 0.0001, and from 0.95 ± 0.46 to 1.84 ± 1.03 ng/106 cells, p < 0.0001, respectively). No statistically significant modifications were found in the placebo group.
A significant improvement of sperm cell total motility (from 33.14 ± 7.12 to 39.41 ± 6.80%, p < 0.0001) and forward motility (from 10.43 ± 3.52 to 15.11 ± 7.34%, p = 0.0003) was observed in the treated group after 6 months (T + 6) of CoQ10 administration. No statistically significant modifications in kinetic parameters were found in placebo group.
A significant inverse correlation between baseline (T0) and T + 6 relative variations of seminal plasma or intracellular CoQ10 or QH2 content and kinetic parameters was also found in treated group. In fact, patients with lower baseline value of motility and levels of CoQ10 had a statistically significant higher probability to be responders to the treatment.
After washout (T + 9), sperm cell kinetic features (total and forward motility, VSL) resulted to be significantly reduced in treatment groups when compared with month T + 6.
Also the group of Safarinejad confirmed a positive effect of CoQ10 treatment on sperm motility [41], in particular in improving sperm count, motility, and morphology. Our more recent work investigated the protective effects of coenzyme Q10 and aspartic acid on oxidative stress and DNA damage in subjects affected by idiopathic asthenozoospermia [42]. We found that only CoQ10 seemed to play a protective role against oxidative stress and DNA damage, thus contradicting some previous findings, which suggested these effects also for D-Asp.
2.2 Vitamin E
Vitamin E (alpha-tocopherol) is a fat-soluble antioxidant vitamin that can neutralize free radicals and protect cell membranes against ROS. Vitamin E can also protect against DNA damage, as demonstrated by Greco et al. in a placebo-controlled study of infertile men [43]. In this study vitamin E didn’t improve seminal parameters (motility and concentration). Other studies, instead, reported an improvement in motility or morphology or both with a combination of vitamin E and selenium [44].
2.3 Vitamin C
Vitamin C , known as ascorbic acid, is a water-soluble vitamin that plays a role as cofactor in several hydroxylation and amidation processes, and it can be found in seminal plasma. There are several studies that demonstrated that a vitamin C oral integration can improve sperm motility and count in men with idiopathic oligozoospermia [45]. Cyrus et al. demonstrated, in a double-blind randomized controlled trial, that ascorbic acid improved sperm motility but not sperm count [46]. Other studies investigated the effect of administration of vitamin C with other antioxidants with good results in terms of sperm concentration and motility [47].
2.4 Zinc
It has been hypothesized that even a zinc deficiency may contribute to unexplained forms of infertility. In fact zinc plays an important role in testicular development as well as in sperm maturation [48, 49]. A recent review demonstrated that seminal zinc levels were lower in infertile men and that zinc supplementation increased semen volume, sperm morphology, and motility [50]. Some studies have demonstrated that oral supplementation of zinc can improve sperm motility in men with idiopathic oligozoospermia and/or asthenozoospermia [51]. Low seminal plasma zinc levels have been associated with a decrease in fertility, and in oligospermic patients, there are lower zinc levels than in normozoospermic men [52]. Also in this case, the data are contradictory as numerous studies have not shown a statistically significant association between the zinc levels and the seminal parameters [53, 54].
2.5 Myo-inositol
Inositol is a polyalcohol and in nature is present in nine isoforms, and myo-inositol (MYO) is the most abundant. Recently it was studied the important role of MYO on male reproduction. Its concentrations are higher in seminiferous tubules than in serum, and it is secreted in response to FSH.
It has been suggested that MYO could be involved in some processes such as the regulation of motility, capacitation, and acrosome reaction of spermatozoa [55, 56].
MYO probably has a role in the osmoregulation of seminal fluid contributing to reduce viscosity and improve the progressive motility and velocities [57, 58].
Few studies have investigated the role of MYO as a possible antioxidant agent for the treatment of male infertility and to improve the quality of sperm used to medically assisted reproductive procedures . Colone et al. [59] demonstrated that MYO reduces the presence of amorphous material. At a functional level, MYO seems to increase the membrane potential [60] and improve the synthesis of DNA, tRNA, and proteins [61].
2.6 Herbal Remedy
There are emerging evidences that herbal products can also improve male reproductive functions. Recently it was demonstrated that Eurycoma longifolia Jack extract has, in an in vivo study, androgenic and pro-fertility effect [62, 63].
Cardiospermum halicacabum has been found to increase testosterone levels and sperm count and motility [64]. Also the Tribulus terrestris has long been identified for treating male infertility in Asia and Europe [65].
“MARJORAM essential oil ” has demonstrated faculty to increase spermatogenic and sperm cells in a study in which degenerative changes in seminiferous tubules were determined by fatty diet [65].
3 Perspectives
Although several specific genetic causes of male infertility have been acknowledged, the etiology of many forms of infertility remains unknown. It would be desirable to deepen the study of the exogenous antioxidants in order to hypothesize new therapeutic horizons, especially for those patients who do not benefit from conventional therapies, and we will hope to standardize the dosage to produce new evidences.
4 Conclusion
Oxidant radical excess has been associated with male infertility; in fact spermatozoa are very susceptible to oxygen effects. Also healthy diet and antioxidant agents (such as carnitine, coenzyme Q10, vitamin E, vitamin C, zinc, and myo-inositol) are the most important systems for which it was demonstrated a seminal parameter improvement. There are emerging evidences that herbal products can also improve male reproductive functions. It needs more studies to confirm and refresh data from literature and to standardize new therapy for infertility.
5 Review Criteria
We performed an extensive research of reviews examining the relationship between antioxidants and male infertility using PubMed and MEDLINE. We considered the reviews published in the last 5 years, including the articles researched by the following keywords: “nutraceutical,” “coenzyme Q10,” “nutrition,” “reactive oxygen species,” “diet,” “male infertility,” “semen parameters,” and “reproduction.” Articles published in languages other than English were not considered.
References
Agarwal A, Mulgund A, Hamada A, Chyatte MR. A unique view on male infertility around the globe. Reprod Biol Endocrinol. 2015 Apr 26;13:37.
Aitken RJ, Clarkson JS. Cellular basis of defective sperm function and its association with the genesis of reactive oxygen species by human spermatozoa. J Reprod Fertil. 1987;81:459–69.
Aitken RJ, Clarkson JS, Fishel S. Generation of reactive oxygen species, lipid peroxidation and human sperm function. Biol Reprod. 1989;40:183–97.
Aitken RJ, Krausz C. Oxidative stress, DNA damage and the Y chromosome. Reproduction. 2001;122:497–506. Aitken RJ, Baker MA. Reactive oxygen species generation by human spermatozoa: a continuing enigma. Int J Androl. 2002;25:191–4.
Winston GW, Regoli F, Dugas AJ Jr, Fong JH, Blanchard KA. A rapid chromatographic assay for determining oxyradical scavenging capacity of antioxidants and biological fluids. Free Radic Biol Med. 1998;24:480–93.
Regoli F, Winston GW. Quantification of total antioxidant scavenging capacity (TOSC) of antioxidants for peroxynitrite, peroxyl radicals and hydroxyl radicals. Toxicol Appl Pharmacol. 1999;156:96–105.
Balercia G, Mantero F, Armeni T, Principato G, Regoli F. Oxyradical scavenging capacity toward different reactive species in seminal plasma and sperm cells. A possible influence on kinetic parameters. Clin Chem Lab Med. 2003;41:13–9.
Mancini A, Leone E, Festa R, Grande G, Di Donna V, De Marinis L, Pontecorvi A, Tacchino RM, Littarru GP, Silvestrini A, Meucci E. Evaluation of antioxidant systems (coenzyme Q10 and total antioxidant capacity) in morbid obesity before and after biliopancreatic diversion. Metab Clin Exp, USA. Oct 2008;57(10):1384–9.
Rice-Evans C, Miller NJ. Total antioxidant status in plasma and body fluids. Methods Enzymol. 1994;234:279–93.
Mancini A, Leone E, Festa R, Grande G, Silvestrini A, de Marinis L, Pontecorvi A, Maira G, Littarru GP, Meucci E. Effects of testosterone on antioxidant systems in male secondary hypogonadism. J Androl, USA. 2008 Nov–Dec;29(6):622–9.
Mancini A, Leone E, Silvestrini A, Festa R, Di Donna V, de Marinis L, Pontecorvi A, Littarru GP, Meucci E. Evaluation of antioxidant systems in pituitary-adrenal axis diseases. Pituitary, Springer-Verlag, Heidelberg-New York. 2010;13(2):138–45.
Mancini A, Di Segni C, Bruno C, Olivieri G, Guidi F, Silvestrini A, Meucci E, Orlando P, Silvestri S, Tiano L, Pontecorvi A. Oxidative stress in adult growth hormone deficiency: different plasma antioxidant patterns in comparison with metabolic syndrome. Endocrine. 2017 Nov 15; https://doi.org/10.1007/s12020-017-1468-1.
Cutini M, Balercia G. Growth hormone and male reproduction, In: Mancini A, editor. Adult growth hormone deficiency: physiopathological and clinical aspects. Minerva Med. 1989;80(4):325–34.
Mancini A, Festa R, Silvestrini A, Nicolotti N, Di Donna V, La Torre G, Pontecorvi A, Meucci E. Hormonal regulation of total antioxidant capacity in seminal plasma. J Androl, USA. 2009 Sep–Oct;30(5):534–40.
Agarwal A, Saleh R, Bedaiwy M. Role of reactive oxygen species in the pathophysiology of human reproduction. Fertil Steril. 2003;79:829–43. https://doi.org/10.1016/S0015-0282(02)04948-8.
Fraczek M, Kurpisz M. The redox system in human semen and peroxidative damage of spermatozoa. Postepy Hig Med Dosw. 2005;59:523–34.
Fisher HM, Aitken RJ. Comparative analysis of the ability of precursor germ cells and epididymal spermatozoa to generate reactive oxygen metabolites. J Exp Zool. 1997;277:390–400.
Henkel RR. Leukocytes and oxidative stress: dilemma for sperm function and male infertility. Asian J Androl. 2011;13:43–52. https://doi.org/10.1038/aja.2010.76.
O’Flaherty C. Peroxiredoxin 6: the protector of male fertility. Antioxidants (Basel). 2018 Nov 24;7(12):pii: E173. https://doi.org/10.3390/antiox7120173.
Gaskin AJ, Chavarro JE. Diet and fertility: a review. Am J Obstet Gynecol. 2018;218(4):379–89.
Yao DF, Mills JN. Male infertility: lifestyle factors and holistic, complementary and alternative therapies. Asian J Androl. 2016;18:410–8.
Pisarka MD. Fertility status and overall health. Semin Reprod Med. 2017;35(3):203–4.
Mancini A, Martorana GE, Magini M, Festa R, Raimondo S, Silvestrini A, Nicolotti N, Mordente A, Mele MC, Miggiano GAD, Meucci E. Oxidative stress and metabolic syndrome: effects of a natural antioxidants enriched diet on insulin resistance. Clin Nutr ESPEN, Edinburgh (Scotland). 2015;10:e52–60.
Festa R, Martorana GE, Magini M, Miggiano GAD, Mele C, Raimondo S, Pontecorvi A, Mancini A. Effetti di una dieta ricca di antiossidanti naturali sui livelli di testosterone in soggetti con insulino-resistenza. In: Foresta C, Lenzi A, Ferlin A, Garolla A, editors. Riproduzione e Sessualità. Padova: CLEUP; 2012 Febbraio. p. 337–9.
Giahi L, Mohammadmoradi S, Javidan A, Sadeghi MR. Nutritional modifications in male infertility: a systematic review covering 2 decades. Nutr Rev. 2015;74(2):118–30.
Bohmer T, Johansen L. Carnitine-binding related suppressed oxygen uptake by spermatozoa. Arch Androl. 1978;1:321–4.
Jeulin C, Lewin LM. Role of free l-carnitine and acetyl-l-carnitine in post-gonadal maturation of mammalian spermatozoa. Hum Reprod Update. 1996;2:87–102.
Balercia G, Regoli F, Armeni T, Koverech A, Mantero F, Boscaro M. Placebo-controlled double-blind randomized trial on the use of l-carnitine, l-acetylcarnitine, or combined l-carnitine and l-acetylcarnitine in men with idiopathic asthenozoospermia. Fertil Steril. 2005;84:662–71.
Costa M, Canale D, Filicori M, D’Iddio S, Lenzi A. L-carnitine in idiopathic asthenozoospermia: a multicenter study. Andrologia. 1994;26:155–9. Vicari E, Calogero AE. Effects of treatment with carnitines in infertile patients with prostato-vesiculo-epididymitis. Hum Reprod. 2001;16:2338–42.
Lenzi A, Lombardo F, Sgro P, Salacone P, Caponecchia L, Dondero F, et al. Use of carnitine therapy in selected cases of male factor infertility: a double blind cross-over trial. Fertil Steril. 2003;79:292–300.
Crane FL. Biochemical functions of coenzyme Q10. J Am Coll Nutr. 2001;20(6):591–8.
Sun IL, Sun EE, Crane FL. Comparison of growth stimulation of HeLa cells, HL-60 cells and mouse fibroblasts by coenzyme Q. Protoplasma. 1995;184:214–9.
Stocker R, Bowry VW, Frei B. Ubiquinol-10 protects human low density lipoprotein more efficiently against lipid peroxidation than does alpha-tocopherol. Proc Natl Acad Sci U S A. 1991;88(5):1646–50.
Mazzilli F, Cerasaro M, Bisanti A, Rossi T, Dondero F. Seminal parameters and the swelling test in patients with sperm before and after treatment with ubiquinone (CoQ10). In: 2nd international symposium on reproductive medicine, Fiuggi, vol. 71. Rome: Acta Medica, Edizioni e Congressi; 1988.
Mazzilli F, Bisanti A, Rossi T, DeSantis L, Dondero F. Seminal and biological parameters in dysspermic patients with sperm hypomotility before and after treatment with ubiquinone (CoQ10). J Endocrinol Investig. 1990;13S(1):88.
Balercia G, Buldreghini E, Vignini A, Tiano L, Paggi F, Amoroso S, Ricciardo-Lamonica G, Boscaro M, Lenzi A, Littarru G. Coenzyme Q10 treatment in infertile men with idiopathic asthenozoospermia: a placebo-controlled, double-blind randomized trial. Fertil Steril. 2009;91:1785–92.
Balercia G, Mosca F, Mantero F, Boscaro M, Mancini A, Ricciardo-Lamonica G, Littarru G. Coenzyme Q(10) supplementation in infertile men with idiopathic asthenozoospermia: an open, uncontrolled pilot study. Fertil Steril. 2004;81:93–8.
World Health Organization (WHO). Laboratory manual for the examination of human semen and semen-cervical mucus interaction. 4th ed. Cambridge: Cambridge University; 1999.
Langsjoen P, Langsjoen A, Willis R, Folkers K. Treatment of hypertrophic cardiomyopathy with coenzyme Q10. Mol Asp Med. 1997;8:145–151s.
Balercia G, Arnaldi G, Fazioli F, Serresi M, Alleva R, Mancini A, Mosca F, Lamonica GR, Mantero F, Littarru GP. Coenzyme Q10 levels in idiopathic and varicocele-associated asthenozoospermia. Andrologia. 2002;34:107–11.
Safarinejad MR. Efficacy of coenzyme Q10 on semen parameters, sperm function and reproductive hormones in infertile men. J Urol. 2009;182:237–48.
Tirabassi G, Vignini A, Tiano L, Buldreghini E, Brugè F, Silvestri S, Orlando P, D’Aniello A, Mazzanti L, Lenzi A, Balercia G. Protective effects of coenzyme Q10 and aspartic acid on oxidative stress and DNA damage in subjects affected by idiopathic asthenozoospermia. Endocrine. 2015 Jun;49(2):549–52.
Greco E, Iacobelli M, Rienzi L, Ubaldi F, Ferrero S, Tesarik J. Reduction of the incidence of sperm DNA fragmentation by oral antioxidant treatment. J Androl. 2005;26:349–53.
Moslemi MK, Tavanbakhsh S. Selenium-vitamin E supplementation in infertile men: effects on semen parameters and pregnancy rate. Int J Gen Med. 2011;4:99–104.
Akmal M, Qadri JQ, Al-Waili NS, Thangal S, Haq A, Saloom KY. Improvement in human semen quality after oral supplementation of vitamin C. J Med Food. 2006;9:440–2.
Cyrus A, Kabir A, Goodarzi D, Moghimi M. The effect of adjuvant vitamin C after varicocele surgery on sperm quality and quantity in infertile men: a double blind placebo controlled clinical trial. Int Braz J Urol. 2015;41:230–8.
Kobori Y, Ota S, Sato R, Yagi H, Soh S, Arai G, et al. Antioxidant cosupplementation therapy with vitamin C, vitamin E, and coenzyme Q10 in patients with oligoasthenozoospermia. Arch Ital Urol Androl. 2014;86:1–4.
Favier AE. The role of zinc in reproduction: hormonal mechanisms. Biol Trace Elem Res. 1992;32:363–82.
Elgazar V, Razanov V, Stoltenberg M, Hershfinkel M, Huleihel M, Nitzan YB, et al. Zinc-regulating proteins, ZnT-1, and metallothionein I/II are present in different cell populations in the mouse testis. J Histochem Cytochem. 2005;53:905–12.
Zhao J, Dong X, Hu X, Long Z, Wang L, Liu Q, et al. Zinc levels in seminal plasma and their correlation with male infertility: a systematic review and meta-analysis. Sci Rep. 2016;6:22386.
Hunt CD, Johnson PE, Herbel J, Mullen LK. Effects of dietary zinc depletion on seminal volume and zinc loss, serum testosterone concentrations, and sperm morphology in young men. Am J Clin Nutr. 1992;56(1):148–57.
Carpino A, Siciliano L, Petroni M, De Stefano C, Aquila S, Ando S, et al. Low seminal zinc bound to high molecular weight proteins in asthenozoospermic patients: evidence of increased sperm zinc content in oligoasthenozoospermic patients. Hum Reprod. 1998;13(1):111–4.
Lin YC, Chang TC, Tseng YJ, Lin YL, Huang FJ, Kung FT, et al. Seminal plasma zinc levels and sperm motion characteristics in infertile samples. Chang Gung Med J. 2000;23(5):260–6.
Eggert-Kruse W, Zwick EM, Batschulat K, Rohr G, Armbruster FP, Petzoldt D, et al. Are zinc levels in seminal plasma associated with seminal leukocytes and other determinants of semen quality? Fertil Steril. 2002;77(2):260–9.
Calogero AE, Gullo G, La Vignera S, Condorelli RA, Vaiarelli A. Myoinositol improves sperm parameters and serum reproductive hormones in patients with idiopathic infertility: a prospective double-blind randomized placebo-controlled study. Andrology. 2015;3:491–5.
Condorelli RA, La Vignera S, Mongioì LM, Vitale SG, Laganà AS, Cimino L, Calogero AE. Myo-inositol as a male fertility molecule: speed them up. Eur Rev Med Pharmacol Sci. 2017 Jun;21(2 Suppl):30–5.
Liu DY, Clarke GN, Baker HW. Hyper-osmotic condition enhances protein tyrosine phosphorylation and zona pellucida binding capacity of human sperm. Hum Reprod. 2006;21:745–52.
Artini PG, Casarosa E, Carletti E, Monteleone P, Di Noia A, Di Berardino OM. In vitro effect of myo-inositol on sperm motility in normal and oligoasthenospermia patients undergoing in vitro fertilization. Gynecol Endocrinol. 2017;33:109–12.
Colone M, Marelli G, Unfer V. Bozz Uto G, Molinari a, Stringaro a. inositol activity in oligoasthenoteratospermia-an in vitro study. Eur Rev Med Pharmacol Sci. 2010;14:891–6.
Condorelli RA, La Vignera S, Di Bari F, Unfer V, Calogero AE. Effects of myoinositol on sperm mitochondrial function in-vitro. Eur Rev Med Pharmacol Sci. 2011;15:129–34.
Fox JT, Stover PJ. Folate-mediated one-carbon metabolism. Vitam Horm. 2008;79:1–44.
Tambi MIBM, Imran MK, Henkel RR. Standardised water-soluble extract of Eurycoma longifolia, Tongkat Ali, as testosterone booster for managing men with late-onset hypogonadism? Andrologia. 2012;44:226–30.
Solomon MC, Erasmus N, Henkel RR. In vivo effects of Eurycoma longifolia Jack (Tongkat Ali) extract on reproductive functions in the rat. Andrologia. 2014;46:339–48.
Peiris LDC, Dhanushka MAT, Jayathilake TAHDG. Evaluation of aqueous leaf extract of Cardiospermum halicacabum (L.) on fertility of male rats. Biomed Res Int. 2015;2015:175726.
Elahi RK, Asl S, Shahian F. Study on the effects of various doses of Tribulus terrestris extract on epididymal sperm morphology and count in rat. Global Vet. 2013;10:13–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Cutini, M., Bruno, C., Mancini, A., Balercia, G. (2020). Antioxidants and Male Infertility. In: Parekattil, S., Esteves, S., Agarwal, A. (eds) Male Infertility. Springer, Cham. https://doi.org/10.1007/978-3-030-32300-4_43
Download citation
DOI: https://doi.org/10.1007/978-3-030-32300-4_43
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-32299-1
Online ISBN: 978-3-030-32300-4
eBook Packages: MedicineMedicine (R0)