
Abstract
Near-infrared spectroscopy (NIRS) has several significant advantages over existing radiological techniques in clinical application. Humans do face any accumulation of deleterious x-rays. Unlike ultrasound methods, NIRS does not lead to excess heat, can differentiate between human tissues with varying optical absorption or scatter, can provide functional information, and can measure oxygenation in human tissues without the use of radioisotopes or other contrast agents. However, NIRS has some disadvantages. Quantifying changes with NIRS requires the use of magnetic resonance (MR) or computed tomography (CT) data. Converting measured optical density to Hb/Mb saturation requires the use of complex formulas. Due to their complexity, the formulas will yield inaccurate measurements arising from even small signal interferences.
As Erratum to this chapter is available at http://dx.doi.org/10.1007/978-1-4614-6252-1_10
An erratum to this chapter can be found at http://dx.doi.org/10.1007/978-1-4614-6252-1_10
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
4.1 Introduction
The possibility of a diagnostic method based on near-infrared light has been discussed for more than 80 years. Since Jöbsis’s introduction, near-infrared spectroscopy (NIRS) has been increasingly applied to measure tissue oxygenation in humans by detecting the levels of hemoglobin (Hb) and myoglobin (Mb) [1]. In this chapter, the recent advances in and prospects for clinical applications of NIRS are summarized.
There are several significant advantages that NIRS might offer over existing radiological techniques. The most obvious feature is its non-ionizing nature, which humans can be exposed to for a long time without harm due to accumulation of x-rays [2]. Similarly, NIRS does not lead to excess heat, unlike ultrasound, for which heating of tissues presents a significant hazard [2]. NIRS methods have potential uses as diagnostic tools because they can offer the ability to differentiate between human tissues with varying optical absorption or scatter. They can also allow functional information to be obtained based on specific absorption pattern. Therefore, NIRS can measure oxygenation in human tissues without the use of radioisotopes or other contrast agents. Nevertheless, NIRS has some disadvantages. One problem is a lack of quantification. There are options to quantify absolute changes in Hb levels, but it is not possible to measure these changes with NIRS. An additional magnetic resonance imaging (MRI) or computed tomography (CT) scan is necessary to quantify such changes. Another problem is difficulty in using complex formulas to convert measured optical density in order to quantify the amount of Hb circulating in the blood. These formulas have some limitations: due to their complexity, a small amount of interference can lead to data inaccuracies [3].
In order to appreciate the obstacles associated with the development of the NIRS method, the nature of the interactions that occur between near infrared light and human tissues should be considered. The most dominant interaction at near infrared wavelengths is elastic scattering. The scatter coefficient, μ s , of many tissues has been measured at a variety of near-infrared wavelengths. Measurements of transmitted intensity are greatly affected by scattered light. Choice of wavelength is complicated by a need to consider the relative optical features of different tissues, the availability of suitable sources, and detector sensitivity detectors [1, 2]. The characteristic scatter of tissue is expressed in terms of transport scatter coefficient \( {{\mu^{\prime}}_s} \), and the absorption coefficient is expressed by μ a .
Early applications of NIRS to measure oxygenation in various human tissues were made by Jöbsis [1] and Chance et al. [4]. The NIRS methodology involves detection of differences in light absorption from tissues and is comprised of different approaches, including: (1) continuous-wavelength spectroscopy [5], (2) spatially resolved spectroscopy [6], (3) time-resolved spectroscopy [7], and (4) phase-modulation spectroscopy [8]. The most versatile and widely used approach is continuous-wavelength spectroscopy. Near-infrared light in the range of 700–900 nm is used in an NIRS device because of its ability to penetrate into tissue.
To obtain a reflected-light signal from human tissues, the light source and photodetector (PD) are typically separated by 2.5–3.0 cm. The near-infrared light penetrates in a shallow arc, and the penetration depth is half the separation between the light source and PD (approximately 1.25–1.50 cm) [4, 6]. This indicates that longer separation distances result in deeper penetrations, but also translate into less light reaching the detector. The actual penetration depth and wavelength are very difficult to measure and vary with Hb concentration and tissue thickness (e.g., skin, fat, skull) between the light source and PD, as well as by human tissue type [9, 10]. This is the primary difference between the use of NIRS with reflected light and with transmitted light (such as pulse oximeters, where the light pathlength is known).
NIRS has been applied to measure oxygenation in a variety of human tissues, including muscle, blood vessels, brain, and connective tissue, and more recently has been used in a clinical setting to assess circulatory and metabolic abnormalities [1, 2].
4.2 Muscle Metabolism
Pulmonary ventilation supplies the alveoli with fresh air, which contains a high concentration of oxygen. The oxygen, combined with Hb, is transported to tissues via the circulation, and then consumed within tissues (e.g., muscle). A noninvasive method for oxidative phosphorylation is required to evaluate this process in humans. Nuclear magnetic resonance spectroscopy (NMRS) is currently used to measure the concentration of phosphorus atoms to monitor phosphocreatine, phosphate, ATP, and hydrogen ion concentrations [11, 12].
NIRS, however, offers another technique for indirectly measuring human muscle metabolism [11, 12]. It monitors tissue oxygen level by measuring optical absorption changes in oxygenated and deoxygenated Hb/Mb, and it allows for noninvasive measurement of the balance between oxygen consumption and oxygen supply. NIRS is assumed to map vascular PO2, and NMR monitors deoxygenated Mb as a reflection of intracellular PO2. A combined NIRS and NMR study has demonstrated that deoxygenated Mb kinetics from NMR matched those observed with NIRS from gastrocnemius muscle under planter flexion or pressure cuffing [13]. These results establish the feasibility and methodology to observe deoxygenated Mb and Hb signals in skeletal muscle and help to clarify the origin of the NIRS signal in skeletal muscle.
The oxygen uptake estimated from pulmonary gas exchange parameters has been used as an indirect index of muscle metabolism. NIRS has made it possible to directly and noninvasively measure localized O2 extraction/consumption. A number of studies have used NIRS to measure the muscle oxygenation (Hb saturation and blood volume) of working/exercising muscles [14–21]. Figure 4.1 shows typical changes in oxygenated Hb that occur during cycling at five constant work rates [14]. With increasing work rate, oxygenated Hb at the vastus lateralis muscle decreased progressively. At the beginning of exercise, oxygenated Hb increased due to increased cardiac output and muscle blood flow. Thereafter, with increasing exercise intensity, it decreased due to increased oxygen consumption and oxygen extraction by working muscle. During recovery, oxygenated Hb increased rapidly due to greater oxygen supply to muscle (hyperemia). Previous studies have measured oxygenation in the thigh or calf muscles during cycling [14], rowing [15], skating [16], knee extension [17], ankle plantar flexion [9, 18], and in arm muscles during arm cranking [19], elbow flexion [20], and finger flexion/hand grip exercise [21].

Continuous recording of the oxygenated Hb trace of vastus lateralis muscle during incremental cycling: The symbol “S” indicates the starting point for each exercise and “F” the finishing point for each exercise. Note that a progressively decreasing signal (Hb desaturation) in the vastus lateralis muscle was found with increasing exercise intensity [14]
NIRS measures muscle oxygenation in the small blood vessels, or capillaries [11, 12]. Muscle oxygenation has been shown to correlate with localized muscle activity, as well as myoelectric activity and changes in blood lactate concentration [14]. NIRS measurements have also been correlated with phosphocreatine measurements taken using NMRS [22].
Some studies, however, have reported heterogeneity for muscle metabolism determined by multiple NIRS imaging devices [23–25]. As shown in Fig. 4.2, within the medial head of the gastrocnemius muscle during standing planter flexion, oxygenation was not uniformly distributed throughout the muscle, but instead was consistently different in the proximal and distal areas; the distal portion had greater deoxygenation and a higher decrease in blood volume during exercise, and it had greater oxygenation and increase in blood volume compared to the proximal portion [25].

Changes in oxygen saturation and blood volume during rest and muscle contraction: The symbol “pro” indicates the proximal portion and “dis” the distal portion of the medial head of the gastrocnemius muscle. Note that compared with the proximal portion, lower oxygen saturation and blood volume (sum of oxygenated Hb and deoxygenated Hb) were found during muscle contraction in the medial head of the gastrocnemius muscle [25]
4.2.1 Exercise Prescription/Training Effects
In order to keep/improve physical fitness or improve athletic performance, these NIRS measurements about muscle metabolism could be applied to prescribe exercise programs. Exercise intensity is usually determined by heart rate, oxygen uptake, or blood lactate concentration. These indicators can be used as a gauge of relative whole body exercise intensity. Changes in integrated myoelectric (iEMG) activity and degree of Hb saturation by NIRS in the vastus lateralis muscle were measured simultaneously during cycling with different constant work rates [14]. Changes in oxygenated Hb were observed to significantly correlate to iEMG for each subject (r = −0.947 to −0.993). The iEMG value has been used as an index for measuring the amount of muscle activity, degree of physical work, or amount of fatigue [26]. Therefore, it follows that Hb saturation levels provide reliable information regarding localized muscle activity during various exercise modes where many muscles are involved, such as arm and leg exercises.
Muscle oxygenation is also useful for evaluating either training effects or fitness level. The time course of post-exercise muscle oxygenation has been reported to be related to aerobic function [27, 28] and is accelerated after training in relation to changes in muscle oxidative enzymes or blood flow/capillarization [29]. Puente-Maestu et al. [27] reported the speed of the re-oxygenation determined by NIRS during recovery from exercise over vastus lateralis muscle to be positively modified by endurance training, thus indicating it to be related to changes in oxidative enzyme (citrate synthase). However, muscle oxygenation has also been monitored during functional electrical stimulation in patients with spinal cord injury [30] and in healthy subjects for improving muscle strength [31].
In summary, these NIRS approaches might be useful for evaluating localized exercise intensity and can be applied in determining an optimal exercise program for athletes or for rehabilitation of patients with paraplegia.
4.2.2 Congestive Heart Failure and Q10 Deficiency
The clinical uses of NIRS muscle findings in varied diseases have also been explored. Booushel et al. [32] applied NIRS in clinical evaluation of patients with idiopathic muscle myalgia and exercise intolerance to ascertain the extent to which this clinical condition is associated with altered oxidative metabolism. Other investigators have shown that patients with congestive heart failure desaturate their muscle at a lower work level compared to healthy subjects, indicating an insufficient blood flow to exercising muscle [33, 34].
Patients with coenzyme Q10 deficiency related to limited muscle oxidative phosphorylation also have an oxygenation pattern during exercise different from that in healthy subjects [34]. In fact, the impairment in muscle oxidative phosphorylation is so severe that there is no increase in arterial-to-venous oxygen difference [35]. Accessory respiratory muscle oxygenation during exercise has also been assessed in patients with heart failure and in heart transplant recipients [36, 37].
Compartment syndrome of the lower limb is a clinical phenomenon that is characterized by an increase in compartment pressure in the lower, leading to circulatory deterioration and inadequate tissue oxygenation [38]. Aratό et al. [39] reported that parallel observation of a subject’s clinical status, intracompartmental pressure, and tissue oxygen saturation in the gastrocnemius muscle as determined by NIRS might lead to a correct and reliable diagnosis, thus resulting in optimal timing of fasciotomy and proper evaluation of the efficiency of surgery. Measurements of both the intracompartmental pressure and tissue oxygen saturation can be helpful in making an accurate diagnosis, so that an optimal determination can be made about whether or not a fasciometomy is indicated, and in evaluating a patient’s status during postoperative follow-up.
4.3 Vessel Function
Several prospective studies have focused on the ability of arterial function to predict cardiovascular risk, which would allow for detection of atherosclerosis before the occurrence of critical events [40, 41]. Although they comprise the standard for a diagnosis of hypertension, systolic/diastolic blood pressure measurements are unsuitable for evaluating arterial function in the early stages of cardiovascular disease. Arterial compliance is determined by the functional and structural components related to the intrinsic elastic properties of arteries [42]. In order to evaluate endothelial function, it is necessary to measure the arterial structure, which can be carried out via cold pressor or flow-mediated dilation tests. These methods involve complicated techniques and take a long time.
The ankle-to-brachial index (ABI), however, is the standard for a diagnosis of arteriosclerosis obliterans (ASO). The ABI is determined using the systolic and brachial systolic blood pressure in the ankle. In order to conclusively evaluate/diagnose arteriosclerosis obliterans, it is necessary to measure arterial structure and function by MRI or CT. These methods also involve complicated techniques and take a long time, and CT results in exposure to radiation. Therefore, an easier screening tool is required at the clinical level.
NIRS can monitor the balance between oxygen consumption and oxygen supply by measuring optical absorption changes in oxygenated and deoxygenated Hb. A previous study [24] suggested that oxygenation as determined by NIRS has an influence on arterial function and severity of cardiovascular disease (CVD). It is therefore possible that such NIRS measurements could be used to evaluate an individual’s risk of CVD.
4.3.1 Arterial Function
ASO is characterized by occlusive lesions consisting primarily of atheromas, which are often accompanied by fibrosis and calcification of the medial coat of the artery and that may be associated with thrombosis of varying severity. This disease is now considered to be an occlusive arterial disease predominantly affecting people with diabetes mellitus. ABI is the standard method for screening patients for ASO severity [43]. To evaluate basic physiological functions, however, rehabilitation practitioners require a simple method that is easy to follow and yields data critical to a diagnosis. Many researchers have attempted to evaluate or diagnose ASO severity using NIRS [44–47]. People with ASO have larger decreases in oxygenated Hb and blood volume during some tasks (walking/running, standing planter flexion, or occlusion), and they have slower recovery compared to healthy subjects. Figure 4.3 shows the typical changes in oxygenated Hb (ΔO2Hb) in the gastrocnemius muscle during the thigh occlusion test. Compared to healthy subjects (non-ASO), the ASO patients have a slower recovery and a shallower recovery rate gradient after occlusion [47]. ABI correlated with both recovery time (r = − 0.61, p < 0.01) and recovery rate (r = 0.80, p < 0.001). In the clinical setting, ASO patients have a faster recovery of their oxygenated Hb after taking medication to improve their circulation [46]. These patients reported reduced symptoms of ASO, including a greater ability to walk without pain, as determined by the subjective judgment of a medical doctor.

Change in delta oxygenated Hb during the occlusion test: Open squares represents data for an arteriosclerosis obliterans (ASO) patient and closed squares that of a healthy subject (non-ASO). Note that compared with the healthy subject, a slower recovery after thigh occlusion was found in the gastrocnemius muscle of the arteriosclerosis obliterans patient [47]
To evaluate endothelial function, the arterial structure must be measured, which can be carried out via the cold pressor test (CPT), which results in production of NO via sympathetic activation. This is a novel method for evaluating endothelial function [48]; however, it is also complicated and time consuming. The responses of oxygenation around the calf muscle and carotid artery diameter to a CPT have been measured simultaneously [49]. A greater decrease in oxygenated Hb and vasoconstriction during the test was found in elderly hypertensive patients compared with healthy elderly subjects. The response of oxygenated Hb was significantly correlated to vasodilation/vasoconstriction (r = 0.658, p < 0.001). These findings suggest that evaluation of oxygenation by NIRS might be able to provide valuable information about vascular endothelial function.
4.3.2 Microvascular Function
Assessment of microvascular compliance is a difficult task. Strain-gauge plethysmography, the standard method for evaluating vascular compliance, does not allow a distinction to be made between the venous and arterial blood volume shifts that occur for a given pressure change. Measurement of vascular compliance reflects the contribution of both compartments, even though in classic strain-gauge plethysmography the data obtained are attributable to only the dilation of the venous tree. Binzoni et al. [50] developed a novel method for measuring the compliance of the superficial veins of the lower limb by NIRS. This method is complementary to strain-gauge plethysmography. The NIRS data during head-up tilt allowed for assessment of superficial venous compliance of the lower limb at less than 24 mmHg of hydrostatic pressure (P), and also of changes in oxygenated and deoxygenated Hb levels in the P range −16 to 100 mmHg, which made it possible to assess the characteristics of the vasomotor response of the arteriolar system.
4.4 Brain Function
Similar to positron emission tomography (PET) and functional MRI (fMRI), NIRS can measure changes in cerebral blood flow and Hb saturation. A fast response to neuronal activation can be obtained with other related techniques, such as event-associated optical signals, which are derived from the near-infrared light scattering properties of active neurons. The NIRS method is used to measure brain oxygenation in adults [51], newborn infants [52], and the fetus during labor [53].
4.4.1 Vascular Dementia
The typical symptoms of subcortical vascular dementia (SVD) are slowness in motor performance and in cognitive processing, which results from early impairment of attention and executive functions [54]. Previous studies of SVD patients have observed a reduction in cerebral blood flow or the metabolic rate of oxygen during a resting or active state [55, 56]. In a recent study using simultaneous NIRS and fMRI [56], SVD patients showed decreased oxygenated Hb, total Hb, level-dependent blood concentration, and cerebral blood flow, and the metabolic rate of oxygen decreased during a simple motor task, which might explain the pathological small-vessel compromise, impaired vascular reactivity, and impaired neurovascular coupling. This NIRS method can therefore reveal various hemodynamic and metabolic changes, and may be useful in early detection or monitoring of subcortical vascular dementia.
4.4.2 Brain Oxygenation during Surgery
Many clinical studies and case reports have demonstrated that an ability to measure brain oxygenation aids in detecting clinically silent episodes of brain ischemia in a variety of clinical settings, thus helping to safeguard brain function. In patients with subarachnoid hemorrhage, episodes of angiographic cerebral vasospasm were associated with a reduction in ipsilateral NIRS signals [57]. Degree of spasm was associated with a greater reduction in same-side NIRS signal, demonstrating real-time detection of intracerebral ischemia.
The proper management of brain oxygenation is one of the principal endpoints of all anesthetic procedures, but the brain remains one of the last monitored organs during clinical anesthesiology. There are some medical procedures where iatrogenic brain ischemia is present, including carotid endarterectomy (CEA) in patients with high-grade carotid artery stenosis, temporary clipping in brain aneurysm surgery, hypothermic circulatory arrest for aortic arch procedures, and other cases in which the pathology itself generates brain ischemia, such as traumatic brain injury and stroke [58]. Proper monitoring of ischemia and response to treatment are essential for ensuring a good outcome.
There have been a number of case–control and retrospective studies of brain oximetry in cardiac surgeries that have shown improvements in outcome associated with brain oximetry monitoring and correlations between desaturation and adverse outcomes [59]. In a study utilizing brain oximetry during coronary artery bypass surgery where patients were randomized to active monitoring and a series of interventions designed to improve oxygen saturation, a significant association was found between brain desaturation and early cognitive decline, and also an increased risk of a prolonged hospital stay [60].
Various studies have shown that cerebral oximetry monitoring during CEA can be a valuable tool for detecting cerebral ischemia [61, 62]. A large cohort of NIRS findings from CEA performed under general anesthesia was studied to determine the sensitivity, specificity, and predictive values of regional cerebral tissue oxygen saturation cut-off points in predicting the need for shunting or for levels resulting in neurological complications [63]. In comparison with other devices, NIRS can provide continuous measurement of frontal cortex oxygenation in a simple and noninvasive way. Most studies utilizing NIRS during CEA have defined the sensitivity and specificity of changes in brain desaturation as correlated with either clinical signs of brain ischemia or other neuromonitoring modalities. Kirkpatrick et al. [64] reported a positive correlation between changes in cerebral flow velocity as detected by transcranial Doppler and changes in Hb saturation.
4.4.3 Brain Oxygenation in Children
In such complex settings as pediatric cardiac surgery, pediatric neurosurgery, and pediatric/neonatal intensive care, NIRS has been used to monitor and detect episodes of cerebral ischemia intraoperatively when combined with bispectral index monitoring [65]. NIRS monitors have been continuously and safely employed on the many neonates who suffer from dysfunction in brain oxygenation. Optical absorption by Hb provides a natural contrast agent to study oxygenation and dynamic processes, including evoked responses. The fact that the neonatal head is relatively transparent to light has been known for a long time, and transillumination of the head has been widely used to observe abnormalities near the brain surface, including development of hydrocephalus and subdural hemorrhage [2].
Brain oximetry has been employed to evaluate variations in the cerebral circulation in preterm infants presenting with apneic episodes [66]. An increased total Hb and decreased oxygen saturation were found during apneic episodes. In neonatal birth asphyxia, mild brain cooling has been utilized in an attempt to minimize subsequent brain hyperanemia and intravenous hyperalimentation. Ancora et al. [67] reported changes in brain oxygenation and EEG in an asphyxiated newborn during and after cool cap treatment, and suggested that NIRS might be useful during hypothermia treatments in order to monitor changes in brain oxygenation as possible indicators of the efficacy of cool cap treatment.
These findings suggest that the use of NIRS in monitoring brain oxygenation can provide indications of compromised brain perfusion in a clinical setting. The simple operation and continuous nature of the NIRS method must be considered with regard to the method’s relative sensitivity and specificity versus other monitoring modalities.
4.5 Cancer Detection
There are many medical devices available to clinicians who diagnose, stage, and treat human cancer: CT, ultrasound, single-photon emission computed tomography, PET, MRI, and NIRS [68]. The NIRS method has been used more often in recent times. Its use NIRS as a supplement to conventional techniques in clinical areas has generated considerable interest. NIRS has such advantages as being noninvasive, fast, and relatively inexpensive. In addition, it poses no risk of ionizing radiation, and NIR light can easily penetrate centimeter-thick tissues. Differences in the NIRS signals between tissues are manifestations of multiple physiological changes, which are in turn associated with such factors as vascularization, cellularity, oxygen consumption, or remodeling [69].
The NIRS method offers the promise of a dramatic improvement in screening, and will continue to improve over the next decade. Diagnostically significant results in terms of sensitivity and specificity have been reported for breast, skin, pancreatic, and colorectal cancers. An accuracy between 72% and 97% has been achieved for the different types of tumors studied [70].
4.5.1 Breast Tissue
X-ray mammography is widely used in screening patients for breast cancer, the most common form of carcinoma in females. Because of uncertainties associated with radiographic density, mammography has an up to 22% false-negative rate, as well as a high false-positive rate in patients under 50 years of age [71]. A recent study found that routine initial mammography was not clinically advantageous for subjects under 35 years of age [72]. Furthermore, the use of hormone replacement therapy in postmenopausal patients is known to increase mammographic density [73] and has recently been shown to impede the efficacy of mammographic screening [74]. Techniques such as MRI and ultrasound are used only as secondary procedures because of such factors as high cost and poor specificity or low sensitivity.
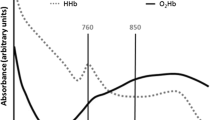
NIRS methods are advantageous for screening because they are noninvasive, quantitative, and relatively inexpensive. They do not require compression and pose no risk of ionizing radiation. Chance’s group [75] introduced the endogenous contrast method, tomographic near-infrared imaging of the human breast, in 1994 [75]. With this technique the inherent properties of normal and malignant tissue can be examined noninvasively using invisible near-infrared light. Recent improvements include the development of a handheld device for breast cancer detection [76] and the use of MRI to improve 3D reconstruction of optical images [77]. Diffuse optical spectroscopy by increasing the wavelength range and resolution has also been employed to characterize malignant tumors (Fig. 4.4) [78].

Specific tumor component index-based image of a malignant tumor: Diffuse optical spectroscopic imaging-mapped regions of the breast are superimposed onto a breast picture. The vertical boxes indicate a subset of the region of interest corresponding to the spectra below. Dots on the image indicate locations at which imaging measurements were obtained. Spectra are shown in two regions: malignant (left) and normal tissue (right). Note that the specific tumor component absorption spectrum is found only in the tumor-containing region and not in surrounding normal tissue [78]
The use of invasive procedures such as fine-needle aspiration or surgical biopsy have also been implemented to provide a definitive diagnosis for breast cancer. Given the suboptimal performance of x-ray mammography in premenopausal and perimenopausal patients, the majority of invasive follow-up procedures are performed on normal or benign tissue that present no malignant disease [79]. As a result, the use of noninvasive NIR methods as a supplement to present techniques for diagnosing and detecting breast cancer has generated considerable interest.
4.5.2 Skin Lesion
Skin cancer is one the most common human carcinomas. The clinical diagnosis is often difficult, as many benign skin lesions resemble malignancies upon visual examination. Therefore, a histopathologic analysis of skin biopsies remains the standard for confirmation. McIntosh et al. [80] collected visible and near-infrared spectra of skin neoplasms in vivo and found significant differences between normal skin and skin lesions in several areas. NIRS is therefore a promising noninvasive technique for screening of skin lesions.
4.5.3 Therapeutic Application
Various treatments are used to cure cancer, control its growth, shrink tumors, or to destroy microscopic cancer cells. Chemotherapy, and radiation/photon dynamic therapy are two of the most often-used procedures in cancer treatment. NIRS can offer options for optimizing the biological effect, accurate dosimetry, and for monitoring treatment progression and efficacy. In a previous study [69], the tissue optical index, developed as a contrast function by combining diffuse optical spectroscopy (DOS) measurements, was monitored following a single dose of adriamycin and cyclophosphamide neoadjuvant chemotherapy. DOS can be used as a quantitative diffuse optical method, which is conceptually similar to the relationship between MRI and MRS. In general, DOS employs a limited number of source-detector positions; however, it employs broadband content in the temporal and spectral domains in order to recover complete absorption and scattering spectra measuring approximately 650–1,000 nm [69]. Figure 4.5 shows the tissue oxygen index (TOI) prior to and on days 1, 2, 3, 6, and 8 following therapy. Note the dramatic drop in TOI within just 1 day: 2.5 prior to therapy to 1.7 on day 1. By day 8, peak TOI levels were approximately equal to normal baseline levels, thus representing a 60% reduction in 1 week. NIRS can therefore be used to quantitatively assess the biochemical composition of the tumor and its response to treatment.

Changes in tissue oxygen index observed post-therapy: Time point 0 was prior to treatment. The error bars represent the standard deviation of measurements. Note that changes were observed in the tissue oxygen index of the tumor (triangles) as soon as 1 day post-therapy [69]
From these findings it can be concluded that NIRS may play an important role in detecting cancer, predicting responders early in the course of therapy, and developing an optimal strategy for care.
4.6 Others
Although it has already been applied to muscle/brain metabolism, vessel function, and cancer detection, NIRS is also quite useful in evaluating and diagnosing various diseases in the clinical setting.
Preterm labor is responsible for 70% of perinatal mortality and nearly half of long-term neurological morbidity [81], and is one of the most challenging problems in modern obstetrics and gynecology. One of the keys to treating preterm labor and preventing severe neonatal complications is early identification of at-risk patients. Hornung et al. [82] used frequency-domain NIRS to monitor changes in the optical properties of the uterine cervix that occur during regular pregnancies, and thus showed that oxygenated Hb and total Hb are significantly correlated with gestational age. Therefore, this kind of NIRS device can be applied to assess the cervix for prediction of risk of preterm labor or for distinguishing between true and false labor.
Surgical site infections (SSIs) comprise the most common serious complication of anesthesia and surgery. The transition from contamination to an established infection occurs during a decisive period, even though infections are typically detected a week or more following surgery [83]. Antibiotics administered during this decisive period are more effective in reducing infection risk. Previous studies have suggested that tissue oxygen tension is one of the best factors for predicting SSIs [84, 85]. Govinda et al. [86] measured changes in tissue oxygen saturation (StO2) as determined by NIRS after colorectal surgery in order to establish the parameters for predicting development of an SSI. StO2 measured at the upper arm was found to be lower in patients with an SSI than in those without, and these measurements had a high sensitivity and specificity for predicting development of an SSI. NIRS may thus be able to predict surgical site infections and so allow earlier preventive or treatment measures to be implemented.
Severe sepsis is an inflammatory response to infection that results in acute organ dysfunction [87]. Despite a hyperdynamic systemic blood flow and elevated mixed venous oxygen saturations, elevated blood lactate concentrations are common in sepsis and suggest that a maldistribution of oxygen within the tissues may contribute to organ failure and death. In human sepsis, impaired microvascular reactivity is related to tissue dysoxia as well as organ dysfunction. Doerschug et al. [88] measured microvascular Hb and StO2 using NIRS both before and after forearm ischemia in patients with sepsis and found StO2 to decrease and the rate of tissue reoxygenation to be impaired with sepsis. Additionally, the rate of tissue reoxygenation was shown to be related to degree of organ dysfunction. NIRS measurements of tissue microvascular perfusion and reactivity may provide important information about sepsis, and such information may serve as endpoints in future therapeutic interventions aimed at improving microvascularization [88].
4.7 Summary
Improvements in NIRS during the past eight decades have matured this technique to the point where it is now effective in a wide range of applications.
However, most of the NIRS investigations reported thus far are feasibility studies. In order to become a major part of a monitoring system, more technological improvements will be needed. Further studies with a larger number of patients and/or normal subjects are also required to further understand the problems associated with this technique, and to confirm its efficacy. Such clinical trials are expected to be carried out over the next decade and will likely have an impact in both research and clinical settings. In sum, NIRS is a prospective technology, an d this kind of tool might play a crucial role in diagnosing and treating human disease, or for defining response to therapy.
References
Jöbsis FF (1977) Non-invasive infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science 198:1264–1267
Hebden JC, Delpy DT (1997) Diagnostic imaging with light. Br J Radiol 70:S206–S214
Watkin SL, Spencer SA, Dimmock PW, Wickramasinghe YA, Rolfe P (1999) A comparison of pulse oximetry and near infrared spectroscopy (NIRS) in the detection of hypoxaemia occurring with pauses in nasal airflow in neonates. J Clin Monit Comput 15(7–8):441–447
Chance B, Nioka S, Kent J, McCully K, Fountain M, Greenfeld R, Holtom G (1988) Time-resolved spectroscopy of hemoglobin and myoglobin in resting and ischemic muscle. Anal Biochem 174(2):698–707
Cope M, Delpy DT (1988) System for long-term measurement of cerebral blood and tissue oxygenation on newborn infants by near infrared transillumination. Med Biol Eng Comput 26(3):289–294
Suzuki S, Takasaki S, Ozaki T, Kobayashi Y (1999) Tissue oxygenation monitor using NIR spatially resolved spectroscopy. Proc SPIE 3597:582–592
Miwa M, Ueda Y, Chance B (1995) Development of time-resolved spectroscopy system for quantitative noninvasive tissue measurement. Proc SPIE 2389:142–149
Duncan A, Whitlock TL, Cope M, Delpy DT (1993) Multiwavelength, wideband, intensity-modulated optical spectrometer for near-infrared spectroscopy and imaging. Proc SPIE 1888:248–257
McCully KK, Landsberg L, Suarez M, Hofmann M, Posner JD (1997) Identification of peripheral vascular disease in elderly subjects using optical spectroscopy. J Gerontol A Biol Sci Med Sci 52(3):B159–B165
Boushel R, Langberg H, Olesen J, Gonzales-Alonzo J, Bülow J, Kjaer M, Scand J (2001) Monitoring tissue oxygen availability with near infrared spectroscopy (NIRS) in health and disease. Med Sci Sports 11(4):213–222
Hamaoka T, McCully K, Chance B, Iwane H (1994) Noninvasive measures of muscle metabolism. In: Sen C, Packer L, Hanninen O (eds) Exercise and oxygen toxicity. Elsevier Science, Amsterdam, pp 481–510
Cerretelli P, Binzoni T (1997) The contribution of NMR, NIRS and their combination to the functional assessment of human muscle. Int J Sports Med 18(Suppl 4):S270–S279
Tran TK, Sailasuta N, Kreutzer U, Hurd R, Chung Y, Mole P, Kuno S, Jue T (1999) Comparative analysis of NMR and NIRS measurements of intracellular PO2 in human skeletal muscle. Am J Physiol 276(6 Pt 2):R1682–R1690
Miura H, Araki H, Matoba H, Kitagawa K (2000) Relationship among oxygenation, myoelectric activity, and lactic acid accumulation in vastus lateralis muscle during exercise with constant work rate. Int J Sports Med 21(3):180–184
Chance B, Dait MT, Zhang C, Hamaoka T, Hagerman F (1992) Recovery from exercise-induced desaturation in the quadriceps muscles of elite competitive rowers. Am J Physiol 262(3 Pt 1):C766–C775
Rundell KW, Nioka S, Chance B (1997) Hemoglobin/myoglobin desaturation during speed skating. Med Sci Sports Exerc 29(2):248–258
Shinohara M, Kouzaki M, Yoshihisa T, Fukunaga T (1998) Mechanomyogram from the different heads of the quadriceps muscle during incremental knee extension. Eur J Appl Physiol Occup Physiol 78(4):289–295
Colier WN, Meeuwsen IB, Degens H, Oeseburg B (1995) Determination of oxygen consumption in muscle during exercise using near-infrared spectroscopy. Acta Anaesthesiol Scand 107(Suppl):151–155
Bhambhani Y, Maikala R, Buckley S (1998) Muscle oxygenation during incremental arm and leg exercise in men and women. Eur J Appl Physiol Occup Physiol 78(5):422–431
Kahn JF, Jouanin JC, Bussière JL, Tinet E, Avrillier S, Ollivier JP, Monod H (1998) The isometric force that induces maximal surface muscle deoxygenation. Eur J Appl Physiol Occup Physiol 78(2):183–187
Boushel R, Pott F, Madsen P, Rådegran G, Nowak M, Quistorff B, Secher N (1998) Muscle metabolism from near-infrared spectroscopy during rhythmic handgrip in humans. Eur J Appl Physiol Occup Physiol 79(1):41–48
McCully KK, Iotti S, Kendrick K, Wang Z, Posner JD, Leigh J Jr, Chance B (1994) Simultaneous in vivo measurements of HbO2 saturation and PCr kinetics after exercise in normal humans. J Appl Physiol 77(1):5–10
Miura H, McCully K, Hong L, Nioka S, Chance B (2001) Regional difference of muscle oxygen saturation and blood volume during exercise determined by near infrared imaging device. Jpn J Physiol 51(5):599–606
Miura H, McCully K, Chance B (2003) Application of multiple NIRS imaging device to the exercising muscle metabolism. Spectroscopy 17:549–558
Miura H, McCully K, Nioka S, Chance B (2004) Relationship between muscle architectural features and oxygenation status determined by near infrared device. Eur J Appl Physiol 91(2–3):273–278
Moritani T, Nagata A, Muro M (1982) Electromyographic manifestations of muscular fatigue. Med Sci Sports Exerc 14(3):198–202
Puente-Maestu L, Tena T, Trascasa C, Pérez-Parra J, Godoy R, García MJ, Stringer WW (2003) Training improves muscle oxidative capacity and oxygenation recovery kinetics in patients with chronic obstructive pulmonary disease. Eur J Appl Physiol 88(6):580–587
Ichimura S, Murase N, Osada T, Kime R, Homma T, Ueda C, Nagasawa T, Motobe M, Hamaoka T, Katsumura T (2006) Age and activity status affect muscle reoxygenation time after maximal cycling exercise. Med Sci Sports Exerc 38(7):1277–1281
Kime R, Karlsen T, Nioka S, Lech G, Madsen O, Sæterdal R, Im J, Chance B, Stray-Gundersen J (2003) Discrepancy between cardiorespiratory system and skeletal muscle in elite cyclists after hypoxic training. Dyn Med 2(1):4
Bhambhani Y, Tuchak C, Burnham R, Jeon J, Maikala R (2000) Quadriceps muscle deoxygenation during functional electrical stimulation in adults with spinal cord injury. Spinal Cord 38(10):630–638
Aldayel A, Muthalib M, Jubeau M, McGuigan M, Nosaka K (2010) Muscle oxygenation of vastus lateralis and medialis muscles during alternating and pulsed current electrical stimulation. Eur J Appl Physiol 111(5):779–787
Boushel R, Langberg H, Olesen J, Gonzales-Alonzo J, Bülow J, Kjaer M (2001) Monitoring tissue oxygen availability with near infrared spectroscopy (NIRS) in health and disease. Scand J Med Sci Sports 11(4):213–222
Wilson JR, Mancini DM, McCully K, Ferraro N, Lanoce V, Chance B (1989) Noninvasive detection of skeletal muscle underperfusion with near-infrared spectroscopy in patients with heart failure. Circulation 80(6):1668–1674
Mancini DM, Wilson JR, Bolinger L, Li H, Kendrick K, Chance B, Leigh JS (1994) In vivo magnetic resonance spectroscopy measurement of deoxymyoglobin during exercise in patients with heart failure: demonstration of abnormal muscle metabolism despite adequate oxygenation. Circulation 90(1):500–508
Wariar R, Gaffke JN, Haller RG, Bertocci LA (2000) A modular NIRS system for clinical measurement of impaired skeletal muscle oxygenation. J Appl Physiol 88(1):315–325
Mancini DM, Ferraro N, Nazzaro D, Chance B, Wilson JR (1991) Respiratory muscle deoxygenation during exercise in patients with heart failure demonstrated with near-infrared spectroscopy. J Am Coll Cardiol 8(2):492–498
Mancini DM, La Manca J, Donchez L, Henson D, Levine S (1996) The sensation of dyspnea during exercise is not determined by the work of breathing in patients with heart failure. J Am Coll Cardiol 28(2):391–395
Matsen FA 3rd, Winquist RA, Krugmire RB Jr (1980) Diagnosis and management of compartmental syndromes. J Bone Joint Surg Am 62(2):286–291
Arató E, Kürthy M, Sínay L, Kasza G, Menyhei G, Masoud S, Bertalan A, Verzár Z, Kollár L, Roth E, Jancsó G (2009) Pathology and diagnostic options of lower limb compartment syndrome. Clin Hemorheol Microcirc 41(1):1–8
Corretti MC, Plotnick GD, Vogel RA (1995) The effects of age and gender on brachial artery endothelium-dependent vasoactivity are stimulus-dependent. Clin Cardiol 18(8):471–476
Najjar SS, Scuteri A, Lakatta EG (2005) Arterial aging: is it an immutable cardiovascular risk factor? Hypertension 46(3):454–462
Cameron JD, Dart AM (1994) Exercise training increases total systemic arterial compliance in humans. Am J Physiol 266(2 Pt 2):H693–H701
Weitz JI, Byrne J, Clagett GP, Farkouh ME, Porter JM, Sackett DL, Strandness DE Jr, Taylor LM (1996) Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation 94(11):3026–3049
Komiyama T, Shigematsu H, Yasuhara H, Muto T (1994) An objective assessment of intermittent claudication by near-infrared spectroscopy. Eur J Vasc Surg 8(3):294–296
Kooijman HM, Hopman MT, Colier WN, van der Vliet JA, Oeseburg B (1997) Near infrared spectroscopy for noninvasive assessment of claudication. J Surg Res 72(1):1–7
Miura H, McCully K, Hong L, Nioka S, Chance B (2000) Exercise-induced changes in oxygen status in calf muscle of elderly subjects with peripheral vascular disease using functional near infrared imaging machine. Ther Res 21(6):79–84
Miura H, Okumura N (2010) A novel approach to evaluate the vessel function determined by near infrared spectroscopy. Adv Exp Med Biol 662:467–471
Tousoulis D, Davies G, Tentolouris C, Crake T, Toutouzas P (1997) Inhibition of nitric oxide synthesis during the cold pressor test in patients with coronary artery disease. Am J Cardiol 79(12):1676–1679
Miura H, Takahashi Y, Okumura N (2011) Response of peripheral vascular system to cold pressor test measured by near infrared spectroscopy. J Jpn Coll Angiol 51:255–257
Binzoni T, Quaresima V, Ferrari M, Hiltbrand E, Cerretelli P (2000) Human calf microvascular compliance measured by near-infrared spectroscopy. J Appl Physiol 88(2):369–372
Wyatt JS (1993) Near-infrared spectroscopy in asphyxial brain injury. Clin Perinatol 20(2):369–378
Elwell CE, Owen-Reece H, Cope M, Wyatt JS, Edwards AD, Delpy DT, Reynolds EO (1993) Measurement of adult cerebral haemodynamics using near infrared spectroscopy. Acta Neurochir Suppl 59:74–80
Wyatt JS, Peebles DM (1993) Near infrared spectroscopy and intrapartum fetal surveillance. In: Spencer JAD (ed) Intrapartum fetal surveillance. RCOG Press, London, pp 329–345
Román GC (1987) Senile dementia of the Binswanger type: a vascular form of dementia in the elderly. JAMA 258(13):1782–1788
Yoshikawa T, Murase K, Oku N, Kitagawa K, Imaizumi M, Takasawa M, Nishikawa T, Matsumoto M, Hatazawa J, Hori M (2003) Statistical image analysis of cerebral blood flow in vascular dementia with small-vessel disease. J Nucl Med 44(4):505–511
Tak S, Yoon SJ, Jang J, Yoo K, Jeong Y, Ye JC (2011) Quantitative analysis of hemodynamic and metabolic changes in subcortical vascular dementia using simultaneous near-infrared spectroscopy and fMRI measurements. Neuroimage 55(1):176–184
Bhatia R, Hampton T, Malde S, Kandala NB, Muammar M, Deasy N, Strong A (2007) The application of near-infrared oximetry to cerebral monitoring during aneurysm embolization: a comparison with intraprocedural angiography. J Neurosurg Anesthesiol 19(2):97–104
Murkin JM, Arango M (2009) Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br J Anaesth 103(Suppl 1):i3–i13
Edmonds HL Jr, Ganzel BL, Austin EH III (2004) Cerebral oximetry for cardiac and vascular surgery. Semin Cardiothorac Vasc Anesth 8(2):147–166
Slater JP, Guarino T, Stack J, Vinod K, Bustami RT, Brown JM 3rd, Rodriguez AL, Magovern CJ, Zaubler T, Freundlich K, Parr GV (2009) Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg 87(1):36–45
Moritz S, Kasprzak P, Arlt M, Taeger K, Metz C (2007) Accuracy of cerebral monitoring in detecting cerebral ischemia during carotid endarterectomy: a comparison of transcranial Doppler sonography, near-infrared spectroscopy, stump pressure, and somatosensory evoked potentials. Anesthesiology 107(4):563–569
Yamamoto K, Miyata T, Nagawa H (2007) Good correlation between cerebral oxygenation measured using near infrared spectroscopy and stump pressure during carotid clamping. Int Angiol 26(3):262–265
Mille T, Tachimiri ME, Klersy C, Ticozzelli G, Bellinzona G, Blangetti I, Pirrelli S, Lovotti M, Odero A (2004) Near infrared spectroscopy monitoring during carotid endarterectomy: which threshold value is critical? Eur J Vasc Endovasc Surg 27(6):646–650
Kirkpatrick PJ, Lam J, Al-Rawi P, Smielewski P, Czosnyka M (1998) Defining thresholds for critical ischemia by using near-infrared spectroscopy in the adult brain. J Neurosurg 89(3):389–394
Hayashida M, Kin N, Tomioka T, Orii R, Sekiyama H, Usui H, Chinzei M, Hanaoka K (2004) Cerebral ischaemia during cardiac surgery in children detected by combined monitoring of BIS and near-infrared spectroscopy. Br J Anaesth 92(5):662–669
Yamamoto A, Yokoyama N, Yonetani M, Uetani Y, Nakamura H, Nakao H (2003) Evaluation of change of cerebral circulation by SpO2 in preterm infants with apneic episodes using near infrared spectroscopy. Pediatr Int 45(6):661–664
Ancora G, Maranella E, Locatelli C, Pierantoni L, Faldella G (2009) Changes in cerebral hemodynamics and amplitude integrated EEG in an asphyxiated newborn during and after cool cap treatment. Brain Dev 31(6):442–444
Frangioni JV (2008) New technologies for human cancer imaging. J Clin Oncol 26(24):4012–4021
Tromberg BJ, Cerussi A, Shah N, Compton M, Durkin A, Hsiang D, Butler J, Mehta R (2005) Imaging in breast cancer: diffuse optics in breast cancer: detecting tumors in pre-menopausal women and monitoring neoadjuvant chemotherapy. Breast Cancer Res 7(6):279–285
Kondepati VR, Heise HM, Backhaus J (2008) Recent applications of near-infrared spectroscopy in cancer diagnosis and therapy. Anal Bioanal Chem 390(1):125–139
Kerlikowske K, Barclay J (1997) Outcomes of modern screening mammography. J Natl Cancer Inst Monogr 22:105–111
Hindle WH, Davis L, Wright D (1999) Clinical value of mammography for symptomatic women 35 years of age and younger. Am J Obstet Gynecol 180(6 Pt 1):1484–1490
Baines CJ, Dayan R (1999) A tangled web: factors likely to affect the efficacy of screening mammography. J Natl Cancer Inst 91(10):833–838
Laya MB, Larson EB, Taplin SH, White E (1996) Effect of estrogen replacement therapy on the specificity and sensitivity of screening mammography. J Natl Cancer Inst 88(10):643–649
Nioka S, Miwa M, Orel S, Shnall M, Haida M, Zhao S, Chance B (1994) Optical imaging of human breast cancer. Adv Exp Med Biol 361:171–179
Hsiang D, Shah N, Yu H, Su MY, Cerussi A, Butler J, Baick C, Mehta R, Nalcioglu O, Tromberg B (2005) Coregistration of dynamic contrast enhanced MRI and broadband diffuse optical spectroscopy for characterizing breast cancer. Technol Cancer Res Treat 4(5):549–558
Carpenter CM, Pogue BW, Jiang S, Dehghani H, Wang X, Paulsen KD, Wells WA, Forero J, Kogel C, Weaver JB, Poplack SP, Kaufman PA (2007) Image-guided optical spectroscopy provides molecular-specific information in vivo: MRI-guided spectroscopy of breast cancer hemoglobin, water, and scatterer size. Opt Lett 32(8):933–935
Kukreti S, Cerussi AE, Tanamai W, Hsiang D, Tromberg BJ, Gratton E (2010) Characterization of metabolic differences between benign and malignant tumors: high-spectral-resolution diffuse optical spectroscopy. Radiology 254(1):277–284
Fletcher SW (1997) Breast cancer screening among women in their forties: an overview of the issues. J Natl Cancer Inst Monogr 22:5–9
McIntosh LM, Summers R, Jackson M, Mantsch HH, Mansfield JR, Howlett M, Crowson AN, Toole JW (2001) Towards non-invasive screening of skin lesions by near-infrared spectroscopy. J Invest Dermatol 116(1):175–181
Goldenberg RL, Hauth JC, Andrews WW (2000) Intrauterine infection and preterm delivery. N Engl J Med 342(20):1500–1507
Hornung R, Spichtig S, Baños A, Stahel M, Zimmermann R, Wolf M (2011) Frequency-domain near-infrared spectroscopy of the uterine cervix during regular pregnancies. Lasers Med Sci 26(2):205–212
Polk HC Jr (1974) The prophylaxis of infection following operative procedures. J Ky Med Assoc 72(3):139–143
Hopf HW, Hunt TK, West JM, Blomquist P, Goodson WH 3rd, Jensen JA, Jonsson K, Paty PB, Rabkin JM, Upton RA, von Smitten K, Whitney JD (1997) Wound tissue oxygen tension predicts the risk of wound infection in surgical patients. Arch Surg 132(9):997–1004
Knighton DR, Halliday B, Hunt TK (1984) Oxygen as an antibiotic: the effect of inspired oxygen on infection. Arch Surg 119(2):199–204
Govinda R, Kasuya Y, Bala E, Mahboobi R, Devarajan J, Sessler DI, Akça O (2010) Early postoperative subcutaneous tissue oxygen predicts surgical site infection. Anesth Analg 111(4):946–952
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis: the ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101(6):1644–1655
Doerschug KC, Delsing AS, Schmidt GA, Haynes WG (2007) Impairments in microvascular reactivity are related to organ failure in human sepsis. Am J Physiol Heart Circ Physiol 293(2):H1065–H1071
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Appendices
Problem
-
4.1
How does NIRS help us better understand the relationship between vasculature and tissue function?
Further Reading
Boushel R, Langberg H, Olesen J, Gonzales-Alonzo J, Bülow J, Kjaer M (2001) Monitoring tissue oxygen availability with near infrared spectroscopy (NIRS) in health and disease. Scand J Med Sci Sports 11(4):213–222
Hebden JC, Delpy DT (1997) Diagnostic imaging with light. Br J Radiol 70:S206–S214
Kondepati VR, Heise HM, Backhaus J (2008) Recent applications of near-infrared spectroscopy in cancer diagnosis and therapy. Anal Bioanal Chem 390(1):125–139
Murkin JM, Arango M (2009) Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br J Anaesth 103(Suppl 1):i3–i13
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Hajime, M. (2013). Clinical Application of NIRS. In: Jue, T., Masuda, K. (eds) Application of Near Infrared Spectroscopy in Biomedicine. Handbook of Modern Biophysics, vol 4. Springer, Boston, MA. https://doi.org/10.1007/978-1-4614-6252-1_4
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6252-1_4
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4614-6251-4
Online ISBN: 978-1-4614-6252-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)