
Abstract
Acute pelvic pain is a routine situation in an emergency department. Ultrasonography is classically the first and sometimes the only necessary imaging tool. MRI is the preferred technique in young woman. However, in clinical practice CT is being performed more and more often as the first-line imaging in patients for whom the clinical hypotheses are often not good ones. Many gynaecologic disorders, including pelvic inflammatory disease, endometriosis, adnexal torsion, hemorrhage or rupture, leiomyoma complications, and pregnancy or postpartum complications, demonstrate suggestive CT findings. However, interpretation of these CT findings must take into account the age of the patient and the patient’s hormonal status.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Although ultrasonography (US) is classically the modality of choice for diagnosing gynecologic emergencies, gynecologic disease is detected or suspected with increasing frequency by CT. However, CT is being performed more and more often as the first-line imaging in patients with acute pain of the lower quadrants. In clinical practice, a gastrointestinal cause is often evoked for explaining acute abdomen, making a CT scan indicated. Furthermore, CT may be performed if US findings are equivocal or if the abnormalities extend beyond the field of view achievable with the endovaginal probe (Bennett et al. 2002; Potter and Chandrasekhar 2008).
The two main causes of a surgical gynecologic emergency are ectopic pregnancy and ovarian torsion. The diagnostic argument must take into account the epidemiological context and particularly the age of the patient. So we will review the contribution of CT with regard to the age of the patient.
2 Premenopausal Patients
2.1 Pelvic Inflammatory Disease
2.1.1 Clinical Context
Pelvic inflammatory disease (PID) refers to infection and resultant inflammation of the upper female genital tract, including the endometrium, fallopian tubes, and ovaries. It constitutes one of the most common diseases in women. The source of the disease is typically an ascending lower genital tract infection, even though hematogenous spread and direct extension of an infection (e.g., from an adjacent abscess) are also possible. Neisseria gonorrhoeae or Chlamydia trachomatis is believed to be the offending agent in two thirds of cases, but polymicrobial infection has also been reported. PID is one of the most common diseases in women, representing about one quarter of visits to the emergency department for gynecologic pain. Prompt diagnosis and treatment of PID are important because of the severity of long-term sequelae of untreated PID, which include infertility due to fallopian tubal occlusion, ectopic pregnancy, recurrence of PID, and chronic pelvic pain. Patients usually present with a myriad of nonspecific symptoms, including fever, abdominal or pelvic pain, vaginal discharge, uterine bleeding, dyspareunia, dysuria, adnexal or cervical tenderness, nausea, vomiting, and other vague constitutional symptoms (McCormack 1994; Sam et al. 2002). The reference standard for diagnosing PID is laparoscopy, however, this is an expensive and invasive procedure that is seldom used in a clinical setting, making imaging useful for diagnosis. Furthermore, imaging is useful to stage the disease and to identify patients who require hospitalization as opposed to antibiotic therapy on an outpatient basis.
2.1.2 CT Findings
The CT findings in PID differ according to the stage of the disease.
In early PID, CT findings may be normal or may only show a nonspecific mild pelvic edema that results in thickening of the uterosacral ligaments and haziness of the pelvic fat with obscuration of the pelvic fascial planes. Suggestive findings show the presence of inflammatory thickening of the fallopian tubes with, in some cases, the identification of mural nodules corresponding to thickened endosalpingeal folds, which helps to differentiate fallopian tubes from a digestive structure such as appendicitis. Findings are usually bilateral, although one side may be affected more than the other. Early oophoritis may manifest itself as enlarged and abnormally enhanced ovaries that may demonstrate a polycystic appearance (Sam et al. 2002). Other findings include abnormal endometrial thickening, abnormal endometrial enhancement and endometrial fluid consistent with endometritis, enlargement of the cervix consistent with cervicitis, and periovarian stranding.
In more advanced PID, the fallopian tubes exhibit a greater degree of wall thickening and enhancement and are filled with complex fluid, findings that usually indicate pyosalpinx. Then frank tubo-ovarian abscess is shown by the presence of a thick-walled, complex fluid collection that may contain internal septa, a fluid–debris level, or gas. In pelvic peritonitis complicating PID, a peritoneal collection is present and salpinx involvement is generally bilateral (Fig. 1). Coronal and sagittal reformatting may be helpful in demonstrating continual fluid-filled cystic structures, thereby confirming a dilated fallopian tube rather than a complex multilocated cystic mass (Yitta 2009); they are also helpful to differentiate pyosalpinx, with its tubular form, from ovarian abscess (Fig. 2).

Pelvic peritonitis complicating a bilateral pyosalpinx. Bilateral solid and cystic masses are well seen on the axial slice (a) and coronal reformatting (b). Note the peritoneal collection (arrow) behind the uterus with an enhanced wall suggestive of peritonitis. Note also the presence of an intrauterine device

Tubo-ovarian abscess. The coronal reformatting well differentiates the left ovarian abscess (arrow) from the salpinx (double arrows) with its characteristic tubular shape
Occasionally in mild and in advanced PID, bacteria may spread by means of direct extension along the right paracolic gutter or through the lymphatic system, causing inflammation of the right upper quadrant peritoneal surfaces and the right lobe of the liver (Romo and Clarke 1992). This corresponds to the clinical finding of perihepatitis, known as Fitz–Hugh–Curtis syndrome. CT is used to look for a thickening of the perihepatic peritoneum which is abnormally enhanced in the arterial phase because of the inflammation or in the delayed phase because of an early capsular fibrosis (Kim et al. 2009; Cho et al. 2008). Other involvements of adjacent structures in PID include a bowel with small or large bowel obstruction or ileus and ureters with hydronephrosis (Cho et al. 2008).
2.1.3 CT Pitfalls
CT pitfalls may be due to unusual causes of tubo-ovarian abscess, difficulties in differentiating tubo-ovarian abscesses from other pelvis abscesses of other origin, or atypical forms of common causes of PID. Unusual causes of tubo-ovarian abscess mainly include actinomycosis and tuberculosis (Kim et al. 2004).
Actinomycosis is a chronic suppurative infection by Actinomyces israelii. On CT, tubo-ovarian actinomycosis usually appears as a predominantly solid mass or a solid and cystic mass in the adnexal region, with contrast enhancement very prominent in the solid portion (Ha et al. 1993). The other key point in actinomycosis is the presence of thick, linear, and well-enhanced lesions extending directly from the mass into the adjacent tissue planes, which reflects the invasive nature of actinomycosis. These inflammatory extensions sometimes form perirectal masses or masses in the cul-de-sac, may mimic seeding masses from ovarian malignancies (Cho et al. 2008). The presence of an intrauterine device (IUD) is an ancillary diagnostic finding, by keeping in mind that IUDs are also commonly found with other causes of tubo-ovarian abscess and the absence of an IUD on CT scans does not mean the absence of a history of IUD use (Kim et al. 2004).
Genital involvement is rare in tuberculosis; the affected sites are predominantly the endometrium (72%) and the salpinx (34%) and less frequently ovaries (12.9%) and the cervix (2.4%) (Namavar Jahromi et al. 2001). CT findings mimic peritoneal carcinomatosis with thickened salpinges or nodularities along tubo-ovarian surfaces, cystic or both solid and cystic adnexal masses, usually bilateral, accompanied by ascites, omental or mesenteric infiltrations, and peritoneal thickening (Kim et al. 2004).
General pelvic abscess, resulting from an adjacent infection in the appendix, colon, or uncommonly bladder, may mimic tubo-ovarian abscess. An arguments for tubo-ovarian abscess is the anterior displacement of the broad ligament because of the posterior position of the mesoovarium, whereas an argument against is obviously the identification of normal ovaries.
In some cases, diagnosis may be difficult because salpinx involvement, adnexal involvement, or rarely a myometrium involvement is the consequence of a gastrointestinal tract infection, mainly diverticulitis and appendicitis (Fig. 3).

Appendicitis involving the right ovary. The upper axial slice (a) shows findings of appendicitis (arrow) with dilatation of the appendix, thickening and increased enhancement of the appendicular wall, and an appendicolith. The lower axial slice (b) shows an abscess of the right ovary (double arrows). Sagittal reformatting (c) shows the contiguity between appendicitis (arrow) and the involved right ovary (double arrows)
2.1.4 CT Impact
Endovaginal US is classically the modality of imaging recommended to diagnose PID. However, in clinical practice, CT indications for PID are common:
-
1.
Because a nongynecologic abnormality was suspected to be the cause of lower abdominal pain
-
2.
To stage the full extent of the disease especially when patients fail to respond to antibiotic therapy or when complications of PID such as abscess are suspected
-
3.
When US is difficult to perform or the findings are equivocal
By giving a complete assessment of the disease, it can provide arguments for hospitalization of patients who have PID (the indications for which as summarized by McWilliams et al. 2008 are given in Table 1) and can be used to monitor an eventual surgical treatment.
2.2 Endometriosis
Endometriosis results from the ectopic location of endometriosis glands and stroma outside the uterus. It affects an estimated 10% of premenopausal women, with as much as 80% of ectopic endometrial tissue found in the ovaries. Other sites include the uterine serosal surface, rectovaginal septum, fallopian tubes and bowel, most commonly the rectosigmoid colon. Although endometriosis is a common cause of chronic abdominal pain, an acute setting is rare but can occur in four clinical complications:
-
1.
Small or large bowel obstruction due to the site of endometriosis implantation in the bowel.
-
2.
Acute appendicitis resulting from endometriosis deposits in the appendix and obstructing its lumen.
-
3.
Acute parietal pain due to an endometrioma in the abdominal wall within the rectus muscle or extending into the subcutaneous fat. It complicates previous abdominal surgery (cesarian) or amniocentesis. Clinically, a peri-incisional abdominal wall hernia may be suspected. CT shows a mass within the abdominal wall with a marked contrast enhancement, which may be confused with a tumoral mass such as a dermoid tumor or a hypervascular metastasis (Bennett et al. 2010)
-
4.
Secondary rupture or infection of an endometrioma is very rare. It may be responsible for a complex adnexial mass that may simulate on CT PID, hemorrhagic cyst, or even malignancies (Potter 2008).
2.3 Adnexal Torsion
2.3.1 Clinical Context
Adnexal torsion is a gynecologic emergency caused by partial or complete twisting of the ovary, ispsilateral fallopian tube or both, resulting in vascular compromise. Adnexal torsion is frequently associated with a large ipsilateral ovarian tumor or with large cystic ovaries seen in ovarian hyperstimulation syndrome (McWilliams et al. 2008). Tumoral causes are benign, including predominantly teratomas, ovarian cysts, and cystadenomas and less often fibromas. Although, it can also occur in normal ovaries, usually in adolescents, this is very rare and was never present in a retrospective study of 135 adnexal torsions (Bouguizane et al. 2003). Early surgical intervention is needed to save the affected ovary in young women. So in the setting of acute pelvic pain, ovarian torsion is often a leading diagnostic consideration, especially when an ovarian mass is discovered.
Adnexal torsion accounts for about 3% of gynecologic emergencies in the USA (Schraga et al. 2007). It may occur in women of all ages, with the highest prevalence in women in their reproductive years and particularly in pregnant women. The classic presentation includes sharp, localized right or left lower abdominal pain, tenderness and peritoneal findings, and a pelvic mass; gastrointestinal complaints with nausea and vomiting are encountered in 70% of patients (McWilliams et al. 2008), whereas fever constitutes an argument for a necrosis complicating the ovarian torsion.
US constitutes the primary imaging modality when adnexal torsion is suspected. However, CT is often performed because adnexal torsion was not the first diagnosis envisaged by the physician since it may mimic other causes of acute abdominal pain such as appendicitis or colic pain, because US findings are equivocal, or because further characterization of the pelvic disease is necessary.
2.3.2 CT Findings
The main finding of adnexal torsion is the presence of an adnexal mass, which is generally totally or partially cystic with or without fat and which measures more than 5 cm in diameter (Hiller et al. 2007; Ghang et al. 2008; Lee et al. 2009) (Fig. 4).

Torsion of an ovary with a teratoma: Axial slices (a,b) show a fat-containing mass on the right side. Note some fluid collection around the teratoma. The normal right ovary is well seen (arrow). The uterus is deviated to the left side. Surgery confirmed torsion of the left ovary with teratoma
Several intra-adnexal as well as extra-adnexal CT findings are helpful to differentiate adnexal torsion from a common tumor of the ovary:
-
The presence of a thickening of the fallopian tube seen between the uterus and the ovarian mass. It appears on CT as a tubular masslike lesion or a target lesion (Fig. 5).
Fig. 5 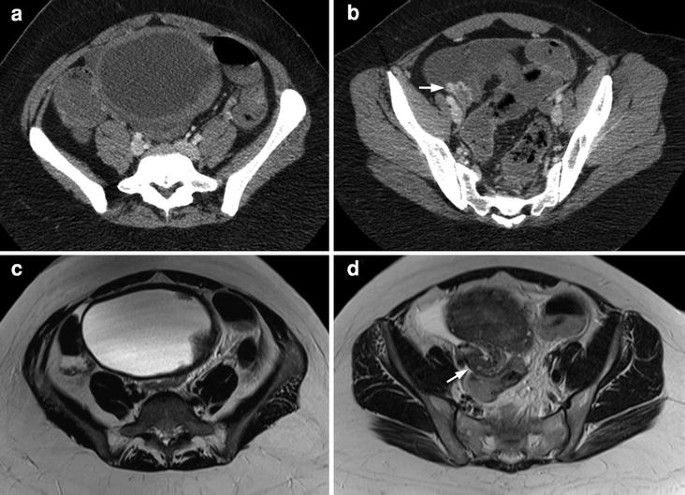
Torsion of an ovary with a serous cystadenoma. The axial CT slice (a) show a cystic medial mass with a smooth wall thickening more pronounced on its right side. A thickened and enhanced right fallopian tube is well seen on a lower slice (b) (arrow). Axial T2-weighted MRI slices show clearly the cystic mass with a smooth thickened wall and some papillary projections (c) and, better visualized, the abnormal right fallopian tube as a tubular masslike lesion (d) (arrow). Surgery confirmed the torsion of the right fallopian tube and of the right ovary with a serous cystadenoma
-
The identification of a smooth wall thickening without nodularity on the cystic mass. This thickening is more often eccentric than concentric (Rha et al. 2002) (Fig. 5).
-
The displacement of adnexa which may be on the controlateral side of the pelvis (Fig. 4) or on the midline in a far anterior position abutting the anteropelvic fascia or posterior in the pouch of Douglas (Fig. 6).
-
The deviation of uterus to side of the involved ovary (Fig. 4).
-
The noncontinuity of the ipsilateral gonadal vein with the twisted adnexal mass.


Torsion of an ovary with a serous cystadenoma. The lower CT slice (a) shows a cystic mass with an eccentric wall thickening. The mass is posterior in the pouch of Douglas and there is some fluid around the mass. The upper CT slice (b) shows a mass on the right side in front of the iliac vessels. On surgery, there was torsion of the right ovary with a serous cystadenoma
Other findings such as ascites or infiltration of pelvic space are less helpful in the setting of acute pelvic pain, but the site of the infiltration is a good indicator of the torsion side (Fig. 6).
2.3.3 CT Pitfalls
In clinical practice, the identification of an ovarian mass is a clue to diagnosing ovarian torsion in adults. However, most ovarian tumors are not complicated by torsion. So the identification of the location of the involved ovary (normal location, contralateral displacement, midline displacement) is important and needs the visualization of the uninvolved ovary, which is not constant. If serial CT is available, a change in the configuration of the ovary may aid in the diagnosis (Ghossian et al. 1997). Otherwise, visualization of the fallopian tube is challenging when a large complex adnexal mass is present on CT, explaining why tubal involvement may be found less commonly on CT than on pathologic examination (Hiller et al. 2007). Finally, if fat density characteristic of teratoma is missing, the underlying pathologic process causing torsion may not be characterized by CT. Fluid especially may mean either a cystic tumor or a necrosis complicating the torsion.
The differentiation between patients with hemorrhagic infarction and those without is difficult. Adnexal hemorrhage which can manifest itself on unenhanced images as an area of increased attenuation is in favor of infarction (Ghang et al. 2008) but this needs unenhanced CT, which is not commonly performed in the setting of acute abdomen. The lack of enhancement of the adnexa could theoretically be an argument for necrosis, but CT is not reliable to assess the flow within it.
2.3.4 CT Impact
Diagnosis of ovarian torsion remains difficult and is often made by ruling out other causes and by having a strong clinical suspicion (McWilliams et al. 2008). US is usually the first examination performed for this diagnosis, with an overall accuracy allowing an expeditious diagnosis (Ghang et al. 2008), and in most cases there is no need for CT (Hiller et al. 2007). However, CT may be helpful in the case of indeterminate US findings or for a better assessment of the mass responsible for the torsion. Furthermore, the CT diagnosis of adnexal torsion must be known since CT is often the first imaging performed in the clinical setting of acute abdomen. An early diagnosis can help prevent irreversible structural damage and may allow conservative, ovary-sparing treatment, with instead of performing a salpingo-oophorectomy a laparoscopic evaluation with a gentle untwisting of the ovary, the removal of the adnexal tumor, and an oophoropexy against the pelvic sidewall.
2.4 Hemorrhagic or Ruptured Ovarian Cysts
2.4.1 Clinical Context
Significant hemorrhage of an ovarian cyst is a common cause of acute pelvic pain. If there is cyst rupture, it can be life-threatening because of associated hemoperitoneum and hypotension, particularly in patients being treated with anticoagulation (Ghang et al. 2008). Hemorrhage is more frequent in a corpus luteum cyst than in a follicular cyst owing to the increased vascularity of the ovary during the luteal phase. Other ovarian masses, such as endometrioma, may rarely rupture. For instance, the content of a teratoma may spill into the peritoneum with chemical peritonitis and fat-containing peritoneal implants.
2.4.2 CT Findings
Hemorrhagic ovarian cyst before rupture often appears unilocular on CT images with an interval attenuation of 40–100 UH. A fluid–fluid level may be observed. If there is cyst rupture, hemoperitoneum will also be present and the ovary may even be normal if rupture has totally decompressed the cyst (Fig. 7). Contrast-enhanced CT may delineate the cyst wall with a ring of peripheral contrast enhancement, and delayed CT may be useful in demonstrating the site of pooling of contrast-enhanced blood in the pelvis if imaging is performed during active bleeding (Hertzberg et al. 1999).

Ruptured corpus luteum with hemoperitoneum. Axial (a) and coronal (b) views show a corpus luteum with an enhanced wall in the right ovary and a significant amount of high-attenuation pelvic fluid surrounding the corpus luteum. The free peritoneal fluid in Morrison’s pouch is hypodense and well seen on the coronal view
A ruptured ectopic pregnancy could manifest itself with a similar clinical picture, so correlation with β-HCG levels prior to imaging to exclude this possibility is essential. Hemorrhagic ovarian cyst and ectopic pregnancy constitute the two most common causes of hemoperitoneum of gynecologic origin (Table 2).
2.4.3 CT Impact
Management of hemorrhagic or ruptured cyst is conservative in the lack of hemodynamic instability with the need for follow-up US performed within one or two menstrual cycles to determine whether the cyst has resolved (Borders et al. 2004). So when hemorrhagic ovarian cysts are detected initially on CT, they need not be immediately evaluated with US for further comparisons.
The differentiation by imaging between hemorrhagic follicular and corpus luteum cyst is impossible. In uncomplicated cysts, the wall of luteal cysts is thicker than that of follicular cysts, but it is likely that in a complicated follicular cyst the wall becomes thicker. So, temporal correlation of a symptomatic cyst with the luteal phase of the menstrual cycle or with a positive β-HCG level favors the diagnosis of hemorrhagic corpus luteum (Potter 2008).
Consequently, in clinical practice, even if the CT diagnosis of hemorrhagic or ruptured cyst is a common occurrence, strict rules need to be followed in such a setting, including correlation with β-HCG levels to rule out an ectopic pregnancy, temporal correlation with the phase of the cycle, and second-look US for further comparisons.
2.5 Ovarian Hyperstimulation Syndrome
Ovarian hyperstimulation syndrome is a rare, potentially fatal, syndrome; it is usually iatrogenic secondary to ovarian stimulant drug therapy for infertility and occurs during the luteal phase or early pregnancy (Delvigne and Rozenberg 2003). But in some rare cases it may also be present as a spontaneous event in pregnancy. The syndrome consists of ovarian enlargement with abdominal discomfort through extravascular accumulation of exudates, leading to weight gain, ascites, pleural effusions, intravascular volume depletion with hemoconcentration, and oliguria in differing degrees. Pain, abdominal distention, nausea, and vomiting are frequently seen.
CT shows bilaterally enlarged ovaries due to multiple distended, peripherally located corpora lutea cysts of various sizes, producing the “spoke wheel” appearance with stromal ovarian tissue located centrally with surrounding cysts (Kim and Lee 1997). The appropriate clinical setting makes the differential diagnosis easy with a bilateral cystic ovarian neoplasm.
2.6 Ectopic Pregnancy
Ectopic pregnancy accounts for approximately 2% of all pregnancies and is the most common cause of pregnancy-related mortality in the first trimester. The main risk factors for ectopic pregnancy include a history of ectopic pregnancy, tubal surgery, and PID. Ninety-five percent of ectopic pregnancies are tubal, whereas other types of ectopic pregnancies include interstitial, cornual, ovarian, cervical, scar, intra-abdominal, and heterotopic pregnancy (Lin et al. 2008).
Early diagnosis and treatment of ectopic pregnancy are essential in reducing maternal mortality and preserving future fertility and workup of a patient with possible ectopic pregnancy entails hormonal assays and endovaginal pelvic US. However, with increased use of CT in the emergent setting, pregnant women may inadvertently undergo CT scanning when the pregnancy is not known at the time of the emergency.
CT findings of tubal ectopic pregnancy described in the few cases reported in the literature, as well as in our experience of three recent cases, are univocal.
CT shows an adnexal area of low attenuation with a dramatic enhanced ring (Pham and Lin 2007) (Fig. 8). This enhanced ring is equivalent to the ring of fire described by Pellerito et al. (1992) with color Doppler imaging to describe the high-velocity, low-impedance flow of trophoblastic tissue surrounding an ectopic adnexal pregnancy. The adnexal cystic structure is adjacent to the ipsilateral ovary and is often associated with hyperdense fluid in the peritoneum consistent with a hemoperitoneum.

Ruptured ectopic pregnancy: The axial slice in the arterial phase (a) shows an enhanced rim. Note also a huge amount of peritoneal fluid. In a delayed phase at the same level (b), the normal right ovary is well shown (arrow), proving that the cause of bleeding was not an ovarian cyst
The main CT differential diagnosis of ectopic pregnancy is a corpus luteum cyst for three reasons: the wall of a corpus luteum may have a strong enhancement, a corpus luteum cyst may rupture in the peritoneum, and a corpus luteum cyst may occur in the setting of early pregnancy. If clinical symptoms and β-HCG levels do not permit one to differentiate these two entities, the location of the adnexal cystic mass may be a clue, with an intraovarian location suggesting a corpus luteum cyst, since intraovarian ectopic pregnancy is very rare.
2.7 Uterine Causes
Uterine causes of acute abdominal pain may be linked to a complication of leiomyomas or in particular conditions to rupture or torsion of the uterus itself.
2.7.1 Complications of a Leiomyoma
Leiomyomas, also known as myomas or fibroids, are the most common gynecologic neoplasm, occurring in 20–30% of women of reproductive age. However, acute pelvic pain is rare in leiomyoma. It may be due to different complications, including acute degeneration and particularly hemorrhagic degeneration, torsion of a pedunculated subserosal leiomyoma, prolapse of pedunculated submucosal leiomyomas, or rupture within the peritoneum.
Acute degeneration is the most common cause of acute pain due to leiomyomas. It can occur spontaneously or following an interventional procedure such as uterine embolization. It is typically seen on CT as a low-attenuation mass in the uterus. Hemorrhagic or red degeneration of a uterine leiomyoma is attributed to obstruction of peripheral veins and is most likely to happen during the period of gestation. Usually, it does not require surgical treatment in an emergency. It is characterized on CT by a hypodense and heterogeneous central component (Bennett et al.2003).
Torsion may complicate pedunculated subserosal leiomyomas and constitutes a surgical emergency. Clinical symptoms depend on the degree of the rotation and the speed at which the torsion develops. CT shows a mass contiguous to the uterus, which is hypodense with small higher attenuation on unenhanced images indicating hemorrhagic infarction; enhancement of the wall of the mass as a regular rim corresponds to obstructed peripheral veins. In some cases (Roy et al. 2005), a shaggy localized zone within the myometrium against the mass is identified, representing the twisted pedicle.
Pedunculated submucosal leiomyomas may prolapse or abort into the vaginal canal. This may lead to acute pelvis pain due to uterine contractions and vaginal bleeding. Although aborting submucosal leiomyomas are better analyzed with MRI, sagittal and coronal multiplanar reformation images are useful in demonstrating the prolapse of the submucosal leiomyoma and its relationship to the cervix and vagina (Yitta 2009).
Rupture of a uterine leiomyoma is a very rare complication of leiomyoma and may be the result of trauma, torsion, or spontaneous rupture of superficial blood vessels. CT can show the myometrial mass. Leiomyomas may have a variety of appearances depending on their degeneration, with the most specific finding, solid “mass-type” calcifications, being rarely encountered. However, the great majority of myometrial masses are leiomyomas, making this diagnosis likely in patients with myometrial masses. CT diagnosis of rupture of uterine leiomyoma is performed on the presence of a myometrial mass, a sentinel clot with its characteristic high attenuation closed to the mass and which permits one to identify the source of hemoperitoneum (Lubner et al. 2007) (Fig. 9), and helps one to differentiate rupture of uterine leiomyoma from other causes of bleeding due to gynecologic conditions (Lotterman 2008; Gupta et al. 2008).

Rupture of uterine leiomyoma with hemoperitoneum. Axial slices before (a) and after (b) intravenous contrast material administration show a hyperdense collection consistent with hemoperitoneum (arrow), in front of an enhanced mass. Note also free hypodense peritoneal fluid in the paracolic gutters. The lower axial slice (c) and sagittal reformatting (d) show multiple leiomyomas. Surgery confirmed the diagnosis of rupture of uterine leiomyoma within the peritoneum
2.7.2 Rupture and Torsion of the Uterus
Rupture and torsion of the uterus are very rare events, especially in the nonpregnant woman. Rupture of the uterus in the nonpregnant woman is usually iatrogenic, resulting from dilatation or curettage. Uterine rupture may be complete, involving the full thickness of the wall and potentially life-threatening, or incomplete, as is generally the case in the 0.1% of perforations complicating IUD placement. In uterine perforation, CT with, in particular, sagittal and coronal reconstructions is helpful for the diagnosis and staging by showing a myometrial defect and assessing its location, size, and depth. In perforation complicating IUD placement, which may be not symptomatic, CT easily shows the hyperdense IUD outside the uterine lumen (Fig. 10).

Migration of an intrauterine device. The axial CT slice (a) shows a metallic foreign body within the greater omentum, with its characteristic T shape displaying an intrauterine device well demonstrated on the scout view (b). This migration means a perforation of the uterus which was not symptomatic
Torsion of a nonpregnant uterus is exceptional, with fewer than ten cases reported. Uterine torsion is always along the transition between the corpus and cervix uteri and is defined as rotation of more than 45º around the long axis of the uterus. It is favored by the presence of a big leiomyoma. CT can show a nonenhancement of the uterine corpus in contrast with a normal enhancement of the cervix and a whorled enhanced structure in the cervix suggesting the mechanism of torsion (Jeong et al. 2003; Matsumoto et al. 2007).
3 Patients Whose Pregnancy Is Known
All the diseases seen in nonpregnant women may be encountered in pregnant women, with an increased occurrence of some of these diseases. Complications of leiomyomas are more frequent with a predisposition for hemorrhagic degeneration, especially during the period of greatest increase in myometrial volume, generally before 10 weeks of gestation (Eyvazzadeh and Levine 2006). Uterine leiomyoma torsion and uterine torsion are less rare in pregnant women than in nonpregnant women. For ovarian torsion, it has been shown that patients with ovarian hyperstimulation syndrome have a greater risk of torsion (16%) than those who do not become pregnant (Mashiach et al. 1990). Last pregnancy increases the risk of rupture of a corpus puteum (Hallatt et al. 1984). However, during pregnancy, the risk of exposure of the fetus to radiation is increased, so more than the usual benefit is necessary to justify CT. Consequently, gynecologic acute diseases are not investigated by CT. In a retrospective study including 78 pregnant women who underwent CT for abdominal pain (Lazarus et al. 2007), CT established the diagnosis in 35% of cases. The main diagnoses performed by CT were appendicitis, urinary tract calculi, bowel obstruction, and cholelithiasis and there were no cases of gynecologic emergencies, demonstrating that for performing gynecologic diagnoses, CT had not been indicated. It must be kept in mind that some nongynecologic common acute diseases have an incidence that is even increased during pregnancy (Augustin and Majerovic 2007; Rooholamini et al. 1993): colic pain, cecal and sigmoid volvulus, acute cholecystitits, liver disease including acute fatty liver of pregnancy, HELLP syndrome, hepatic rupture, and acute pancreatitis. It may be necessary to perform a CT examination for diagnosis; CT findings in these diseases are dealt with in the corresponding chapters.
4 Postpartum Patients
Conversely to pregnancy, in which CT is of limited use, CT is the primary modality in making the diagnosis or determining the severity of peripartum and postpartum complications, including endometritis, abscess, ovarian vein thrombosis and thrombophlebitis, retained product of conception, and hemorrhage.
4.1 Endometritis and Pelvic Abscess
Endometritis is the most common cause of fever during the postpartum period. The incidence of postpartum endometritis after a vaginal delivery in comparison with cesarean delivery is low (2–3%). The incidence of endometritis is particularly high when there is a delay between membrane rupture and cesarean delivery. Other risk factors for endometritis are prolonged labor, premature rupture of the membranes, clot, and retained product of conception (Zuckerman et al. 1997). CT may show fluid or air in the cavity as well as endometrial enhancement on postcontrast images (Menias et al. 2007). However, these findings are nonspecific, and it has been shown by both US and CT that intrauterine air may be present in about 20% of healthy postpartum women and it may persist for as long as 3 weeks after delivery.
Pelvic abscesses may complicate endometritis. They are more frequent after cesarean delivery for several reasons: endometritis is more common, infection may occur in the region of incision, and infection can spread to the parametrium after a cesarean delivery because the parametrial space between the leaves of the broad ligaments may be entered during the development of the bladder flap (Zuckerman et al. 1997). CT shows classic findings suggesting an abscess with a thick-walled, rim-enhanced, fluid-filled structure with adjacent inflammatory stranding and in some cases air–fluid levels and internal septations (Menias et al. 2007).
4.2 Ovarian Vein Thrombosis and Thrombophlebitis
Although ovarian vein thrombosis is classically seen as a postpartum complication, with an overall incidence of about 1 in 1,000 deliveries, it may occur in the setting of PID, oncologic patients, and recent pelvic surgery. The enlarging uterus compresses the ovarian veins, causing venous stasis and thrombosis. Ovarian vein thrombosis is unilateral in most patients on the right (80%) more commonly than on the left (6%) and bilateral in 15% of patients (Munsik and Gillanders 1981). The predilection for right-sided involvement results from uterine dextroversion during pregnancy and from retrograde flow from the left renal vein preventing the left ovarian vein from the stasis. CT shows a tubular structure with wall enhancement corresponding to the dilated gonadal vein with central low-attenuation thrombus. Following the course of the gonadal vein from the pelvis to the inferior vena cava for the right ovarian vein and to the left renal vein for the left ovarian vein helps one to distinguish it from the ureter or appendix. In some cases, thrombosis of ovarian vein collateral vessels when they are retrocecal in location may mimic retrocecal appendicitis (Fig. 11).

Thrombosis of periovarian collaterals in a postpartum woman. The axial slice (a) and coronal reformatting (b) before intravenous contrast matarial administration show a tubular structure which is spontaneously hyperdense lateral to the right kidney. This structure was not enhanced after contrast material administration (c). Note also the big uterus related to the postpartum condition and the structure (arrow) corresponding to ovarian collaterals with thrombosis, posterolaterally to the uterus (d)
Thrombophlebitis may complicate a bland thrombus, particularly in postpartum patients with endometritis. Patients with thrombophlebitis usually present with fever and acute frank pain. Perivascular stranding associated with an enlarged gonadal vein helps to support the diagnosis of thrombophlebitis and distinguish it from bland thrombus (Zuckerman et al. 1997).
4.3 Retained Product of Conception
Uterine atony and retained product of conception constitute the most common causes of postpartum hemorrhage. Less often, hemorrhage reveals a trophoblastic disease. The differentiation between these entities is essential since uterine atony is medically treated, a retained product of conception needs curettage, and a choriocarcinoma needs chemotherapy. US remains the radiological investigation of choice for initial diagnosis, whereas MRI is of invaluable use in assessing extrauterine tumor spread (Allen et al. 2006, Green et al. 1996). If performed, CT gives strong arguments for differentiating placental tissue from a clot by showing an enhancement of retained product of conception (Fig. 12), whereas a clot, often hyperdense, is not enhanced. The presence of calcification, also well seen on US, is an ancillary finding for placental tissue. The imaging appearance of retained product of conception may overlap with that of gestational trophoblastic neoplasia. Myometrial or extrauterine invasion shown by MRI or CT and overall a high and persistent level of β-HCG are key points for the diagnosis of gestational trophoblastic neoplasia.

Retained product of conception responsible for postpartum hemorrhage: The axial slice (a) in the arterial phase and sagittal reformatting (b) in a portal phase show a dilatation of the uterine lumen, with enhanced structure displaying the presence of placental tissue within the uterus
4.4 Uterine Rupture
This rare complication may occur before or during labor or during the delivery. It occurs most frequently in patients with previous surgery of the uterus (myomectomy, cesarean section). Uterine rupture may occur before or during labor or during delivery. The clinical presentation is often alarming, with severe abdominal pain and intraperitoneal and vaginal bleeding making the diagnosis clinical with an immediate laparotomy. However, less severe cases may prompt CT evaluation. CT will show a low-attenuation defect within the normally enhanced myometrium, meaning the disruption of the uterine wall, and a periuterine hematoma (Has et al. 2008).
4.5 Pelvic Hematomas
Hemorrhage is a classic complication of cesarean section. Bleeding generally occurs at the site of the lower uterine incision with the development of a hematoma in the potential extraperitoneal space between the bladder and the lower uterine segment, the so-called bladder flap hematoma. Broad-ligament and rectus sheath hematomas (Rooholamini et al. 1993) or intraperitoneal hemorrhage is more rarely encountered.
5 Postmenopausal Patients
In postmenopausal patients, gynaecologic emergencies are rarer but remain possible.
Findings of PID must be due to the propagation to the fallopian tube or to the ovaries of a bowel inflammation, and in postmenopausal patients, pyosalpinx or ovarian abscesses must lead to a search for diverticulitis or a bowel perforation within the salpinx or the ovaries.
In a retrospective series including 14 women with adnexal involvement from diverticulitis, a gas collection within the adnexa was both sensitive and a specific sign of colosalpingeal fistula, allowing differentiation between fistula and contiguous periadnexal inflammation without fistula (Panghaal et al. 2009). In the same way, ovarian abscess may be the consequence of a perforated sigmoid cancer within the ovary (Fig. 13).

Perforated sigmoid cancer within the right ovary. The axial slice (a) and coronal reformatting (b) show a hypodense mass above the bladder on the right side of the pelvis with a thick wall; the mass contains an air bubble. The relationship between the mass and the sigmoid colon (arrow) with a thickened and irregular wall is clearly demonstrated by a perforation of the tumoral colon within the ovary
Women of reproductive age and particularly pregnant women have the highest prevalence of ovarian torsion. However, ovarian torsion can occur in women of all ages and consequently in postmenopausal women. In a study focused on CT features of adnexal torsion (Hiller et al. 2007), it occurred in 29% of the 35 patients included in the study who were postmenopausal.
Complications of a leiomyoma with acute clinical findings are relatively uncommon, whatever the age of the patient, without any specificity in postmenopausal patients. By contrast, in a postmenopausal patient with acute pelvic pain and a pelvic mass, the acute revelation of a malignant tumor of the ovary must be kept in mind. Acute abdomen may be due to a hemorrhage within the tumor, a rupture, or torsion (Genevois 2008). However, these conditions are rare, and, for instance, in a series including 135 ovarian torsions (Bouguizane et al. 2003), the torsion was due to a malignancy only in two cases. In our experience, ovarian malignancies are more often responsible for acute abdomen by extension to the bowel or by peritoneal carcinomatosis with, in both cases, a bowel obstruction.
References
Allen SD, Lim AK, Seckl MJ, Blunt DM, Mitchell AW (2006) Radiology of gestational trophoblastic neoplasia. Clin Radiol 61:301–313
Augustin G, Majerovic M (2007) Non-obstetrical acute abdomen during pregnancy. Eur J Obstet Gynecol Reprod Biol 131:4–12
Bennett GL, Slywotzky CM, Giovanniello G (2002) Gynecologic causes of acute pelvic pain: spectrum of CT findings. Radiographics 22:785–801
Bennett GL, Harvey WB, Slywotzky CM, Birnbaum BA (2003) CT of the acute abdomen: gynecologic etiologies. Abdom Imaging 28:416–432
Bennett GL, Slywotzky CM, Cantera M, Hecht EM (2010) Unusual manifestations and complications of endometriosis. Spectrum of imaging findings: pictorial review. AJR Am J Roentgenol 194:34–46
Borders RJ, Breiman RS, Yeh BM, Qayyum A, Coakley FV (2004) Computed tomography of corpus luteal cysts. J Comput Assist Tomogr 28:340–342
Bouguizane S, Bibi H, Farhat Y et al (2003) Les torsions des annexes de l’utérus. Aspects cliniques et thérapeutiques: à propos d’une série de 135 cas. J Gynecol Obstet Biol Reprod 32:535–540
Cho HJ, Kim HK, Suh JH, Lee GJ, Shim JC, Kim YH (2008) Fitz-Hugh-Curtis syndrome: CT findings of three cases. Emerg Radiol 15:43–46
Delvigne A, Rozenberg S (2003) Review of clinical course and treatment of ovarian hyperstimulation syndrome (OHSS). Hum Reprod Update 9:77–96
Eyvazzadeh AD, Levine D (2006) Imaging of pelvic pain in the first trimester of pregnancy. Radiol Clin North Am 44:863–877
Genevois A, Marouteau N, Lemercier E, Dacher JN, Thiebot J (2008) Imagerie de la douleur pelvienne aiguë. J Radiol 89:92–106
Ghang HG, Bhatt S, Dogra VS (2008) Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics 28:1655–1668
Ghossian MA, Buy JN, Sciot C, Jacob H, Hugol D, Vadrot D (1997) CT findings before and after adnexal torsion: rotation of a focal solid element of a cystic adjunctive sign in diagnosis. AJR Am J Roentgenol 169:1343–1346
Green CL, Angtuaco TL, Shah HR, Parmley TH (1996) Gestational trophoblastic disease: a spectrum of radiologic diagnosis. Radiographics 16:1371–1384
Gupta N, Dadhwal V, Misra R, Mittal S, Kiran S (2008) Atypical presentation of a leiomyoma as spontaneous massive haemoperitoneum. Eur J Obstet Gynecol Reprod Biol 138:114–124
Ha HK, Lee HJ, Kim H et al (1993) Abdominal actino-mucosis: CT findings in 10 patients. AJR Am J Roentgenol 161:791–794
Hallatt JG, Steele GH Jr, Snyder M (1984) Ruptured corpus luteum with hemoperitoneum: a study of 173 surgical cases. Am J Obstet Gynecol 149:5–9
Has R, Topuz S, Kalelioglu I, Tagrikulu D (2008) Imaging features of postpartum uterine rupture: a case report. Abdom Imaging 33:101–103
Hertzberg BS, Kliewer MA, Paulson EK (1999) Ovarian cyst rupture causing hemoperitoneum: imaging features and the potential for misdiagnosis. Abdom Imaging 24:304–308
Hiller N, Appelbaum L, Simanovsky N, Lev-Sagi A, Aharoni D, Sella T (2007) CT features of adnexal torsion. AJR Am J Roentgenol 189:124–129
Jeong YY, Kang HK, Park JG, Ghoi HS (2003) CT features of uterine torsion. Eur Radiol 13:249–250
Kim IY, Lee BH (1997) Ovarian hyprestimulation syndrome: US and CT appearances. Clin Imaging 21:284–286
Kim SH, Kim SH, Yang DM, Kim KA (2004) Unusual causes of tubo-ovarian abscess: CT and MR imaging findings. Radiographics 24:1575–1589
Kim JY, Kim Y, Jeong WK, Song SY, Cho OK (2009) Perihepatitis with pelvic inflammatory disease (PID) on MDCT: characteristic findings and relevance to PID. Abdom Imaging 34:737–742
Lazarus E, Mayo-Smith W, Mainiero MB, Spencer PK (2007) CT in the evaluation of nontraumatic abdominal pain in pregnant women. Radiology 244:784–790
Lee JH, Park SB, Shin SH et al (2009) Value of intra-adnexal and extra-adnexal computed tomographic imaging features diagnosing torsion of adnexal tumor. J Comput Assist Tomogr 33:872–876
Lin EP, Bhatt S, Dogra VS (2008) Diagnostic clues to ectopic pregnancy. Radiographics 28:1661–1671
Lotterman S (2008) Massive hemoperitoneum resulting from spontaneous rupture of uterine leiomyoma. Am J Emerg Med 26:974e1–974e2
Lubner M, Menias C, Rucker C (2007) Blood in the belly: CT findings of hemoperitoneum. Radiographics 27:109–125
Mashiach S, Bider D, Moran O, Goldenberg M, Ben-Rafael Z (1990) Adnexal torsion of hyperstimulated ovaries in pregnancies after gonadotropin therapy. Fertil Steril 53:76–80
Matsumoto H, Ohta T, Nakahara K, Kojimahara T, Kurachi H (2007) Torsion of a nongravid uterus with a large ovarian cyst: usefulness of contrast MR image. Gynecol Obstet Invest 63:163–165
McCormack WM (1994) Pelvic inflammatory disease. N Engl J Med 330:115–119
McWilliams G, Hill MJ, Dietrich CS (2008) Gynecologic emergencies. Surg Clin N Am 88:265–283
Menias CO, Elsayes KM, Peterson CM et al (2007) CT of pregnancy-related complications. Emerg Radiol 13:299–306
Munsik R, Gillanders L (1981) A review of the syndrome of puerperal ovarian vein thrombophlebitis. Obstet Gynecol Surv 36:57–66
Namavar Jahromi B, Parsanezhad ME, Ghane-Shirazi R (2001) Female genital tuberculosis and infertility. Int J Gynaecol Obstet 75:269–272
Panghaal VS, Chernyak V, Patlas M, Rozenblit AM (2009) CT features of adnexal involvement in patients with diverticulitis. AJR Am J Roentgenol 192:963–966
Pellerito JS, Taylor KJ, Quedens-Case C et al (1992) Ectopic pregnancy: evaluation with endovaginal color flow imaging. Radiology 183:407–411
Pham H, Lin EC (2007) Adnexal ring of ectopic pregnancy detected by contrast-enhanced CT. Abdom Imaging 32:56–58
Potter W, Chandrasekhar CA (2008) US and CT evaluation of acute pelvic pain of gynecologic origin in nonpregnant premenopausal patients. Radiographics 28:1645–1659
Rha SE, Byun JY, Jung SE et al (2002) CT and MR imaging features of adnexal torsion. Radiographics 22:283–294
Romo LV, Clarke PD (1992) Fitz-Hugh-Curtis syndrome: pelvic inflammatory disease with an unusual CT presentation. J Comput Assist Tomogr 16:832–833
Rooholamini SA, Hansen GC, Kioumehr F et al (1993) Imaging of pregnancy related complications. Radiographics 13:753–770
Roy C, Bierry G, El Ghali S, Buy X, Rossini A (2005) Acute torsion of uterine leiomyoma: CT features. Abdom Imaging 30:120–123
Sam JW, Jacobs JE, Birnbaum BA (2002) Spectrum of CT findings in acute pyogenic pelvic inflammatory disease. Radiographics 22:1327–1334
Schraga ED, Kulkarni R, Blanda M (2008) Ovarian torsion. http://www.emedicine.com/emerg/topic353htm. Accessed 14 Mar 2007
Yitta S, Hecht ME, Sliwotzky CM, Bennett GL (2009) Added value of multiplanar reformation in the multidetector CT evaluation of the femal pelvis: a pictorial review. Radiographics 29:1987–2005
Zuckerman J, Levine D, McNicholas MJ et al (1997) Imaging of pelvic postpartum complications. AJR Am J Roentgenol 168:663–668
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Taourel, P., Curros Doyon, F., Millet, I. (2010). Gynecologic Emergencies. In: Taourel, P. (eds) CT of the Acute Abdomen. Medical Radiology(). Springer, Berlin, Heidelberg. https://doi.org/10.1007/174_2010_89
Download citation
DOI: https://doi.org/10.1007/174_2010_89
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-540-89231-1
Online ISBN: 978-3-540-89232-8
eBook Packages: MedicineMedicine (R0)