
Abstract
We present a case of a 37-year-old woman who presented with acute right lower quadrant abdominal pain. Work up with contrast enhanced CT to rule out appendicitis revealed dramatic ring enhancing cystic structure in the right adnexa corresponding to tubal ring sign of ectopic pregnancy seen on subsequent pelvic ultrasound. Right tubal ectopic pregnancy was confirmed at surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Ectopic pregnancy is a common cause of acute pelvic pain in women of child-bearing age. The primary imaging modality for evaluating suspected ectopic pregnancy is ultrasound. The sonographic findings in ectopic pregnancy are well-described [1]. Computed tomography (CT) should generally not be performed in pregnant patients. However with increased use of CT in the emergent setting, pregnant patients may inadvertently undergo CT scanning when the pregnancy is not known at the time of the study. To our knowledge, the CT findings of tubal ectopic pregnancy have not previously been described. We describe a case in which the classic color Doppler “ring of fire” sign of ectopic pregnancy was detected on contrast-enhanced CT.
Case report
A 37-year-old woman G6, P4 presented to the emergency department for evaluation of acute right lower quadrant abdominal pain. The patient indicated oral contraceptive use for over a year and her last menstrual period by history was within one week prior to presentation. Given the clinical presentation the clinician sought to rule out appendicitis with CT scan.
CT of the abdomen and pelvis was performed with both oral and intravenous contrast. The CT scan showed a large amount of high attenuation fluid in the pelvis suggestive of hemorrhage and a dramatically enhancing ring with a central area of low attenuation adjacent to the right ovary in the right adnexa (Fig. 1). Findings raised the suspicion of ectopic pregnancy and patient underwent pelvic US which showed a cystic structure with a thick echogenic wall in the right adnexa consistent with trophoblastic tissue around an extrauterine gestation (the “tubal ring” sign). There was associated increased color Doppler flow in this rim of tissue consistent with high-velocity low-impedance flow to trophoblastic tissue (the “ring of fire” sign) (Fig. 2). Urine pregnancy test was obtained which was positive. The patient was taken to surgery and a ruptured ectopic pregnancy of the right fallopian tube with hemoperitoneum was found.

Thirty-seven-year-old female with ruptured ectopic pregnancy. Contrast-enhanced CT scan shows a dramatic increased enhancement around a fluid density mass in the right adnexa (arrowhead) medial to the right ovary (short arrow). Note that there is a less degree of enhancement posteriorly. Hyperdense fluid in the peritoneum is consistent with hemorrhage (long arrow).

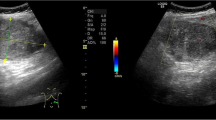
Thirty-seven-year-old female with ectopic pregnancy. Ultrasound with color Doppler shows a cystic structure medial to the right ovary with a thick echogenic rim with dramatic increased color flow. This has been termed the “ring of fire” sign. The posterior aspect has relative decreased flow, corresponding to region of relative decreased contrast enhancement seen on CT.
Discussion
Ectopic pregnancy occurs in approximately 2% of pregnancies and is the most common cause of first trimester maternal death [1]. Along with [beta]-human chorionic gonadotrophin determination, sonography is the standard of care for evaluation of ectopic pregnancies. Sonographic diagnosis of ectopic pregnancy is only definitive when a live embryo is detected in an extrauterine location. However, this is a rare finding. Common sonographic findings include one or a combination of intrauterine and extrauterine findings. The primary intrauterine finding is the lack of a normal intrauterine pregnancy. Extrauterine findings include cystic or solid adnexal mass, dilated and thick-walled fallopian tube, echogenic free fluid, and extrauterine gestational sac containing a yolk sac with or without an embryo [1]. One of the most common and most highly predictive sonographic finding is a thick-walled adnexal cyst occurring in 78% of ectopic pregnancies [2]. This has been referred to as a tubal ring; the ring consists of concentric trophoblastic tissue surrounding the chorionic sac of the ectopic pregnancy and can be distinguished from a corpus luteum cyst as the latter is located within the ovary [3]. Color doppler evaluation demonstrates increased flow surrounding the gestational sac due to the high velocity and low impedance flow of trophoblastic tissue [4]. This has been reported in 85–93% [2] of trophoblastic rings in ectopic pregnancy and has been termed the “ring of fire” sign.
To our knowledge the findings of a tubal ectopic pregnancy on CT have not been previously reported, although there is a report of an intrahepatic pregnancy detected on CT [5]. Pregnant patients generally do not undergo CT examination due to radiation to the fetus. Intravenous contrast is also not generally employed in pregnant patients, particularly in the first trimester. However, given the continued increased use of CT in emergent settings the possibility of patients with ectopic pregnancy being inadvertently imaged with contrast-enhanced CT may be greater than in the past.
Given the known sonographic findings of ectopic pregnancy, we can expect that some of the findings on ultrasound can be seen on CT as well, more specifically, the extrauterine findings such as hemoperitoneum and an adnexal mass. Peritoneal blood can be detected as high attenuation fluid on CT, but this finding is nonspecific in patients with acute abdominal pain who are not known to be pregnant. An adnexal mass in ectopic pregnancy would have a nonspecific appearance on CT. A tubal ring would also likely not be well-visualized morphologically by CT. However, the tubal ring might be expected to have increased enhancement on CT compared with normal surrounding structures due to increased high velocity and low impedance flow of trophoblastic tissue. Thus we would hypothesize that the greatly increased peripheral adnexal enhancement seen on the CT in this case would be the most specific contrast-enhanced CT sign of ectopic pregnancy. The sensitivity of this finding is unknown. A reported case of intrahepatic pregnancy identified on CT did not demonstrate this finding [5].
Other potential etiologies of a peripherally enhancing structure in the adnexa on CT include tubo-ovarian abscess, cystic ovarian neoplasm, and corpus luteum cyst. While tubo-ovarian abscesses and ovarian neoplasms can have low-impedance flow on Doppler ultrasound [6], and wall enhancement on CT [7], the degree of increased enhancement on CT seen in this case is substantially greater than that reported for tubo-ovarian abscesses and ovarian neoplasms [8]. A corpus luteum cyst is most likely to cause confusion with the tubal ring of ectopic pregnancy on contrast-enhanced CT. A corpus luteum cyst has greatly increased mural flow. A tubal ring and corpus luteum cyst cannot be differentiated by mural flow on ultrasound [2]. Although the appearance of corpus luteum cysts on contrast-enhanced CT has not been described, it might be expected that a similar degree of increased enhancement could be seen. Findings that could differentiate a corpus luteum cyst and ectopic pregnancy on CT are location and presence of hemoperitoneum. As intraovarian ectopic pregnancy is very rare, an intraovarian location suggests a corpus luteum cyst. In addition, the hemoperitoneum seen in this case is not associated with a corpus luteum cyst [2].
In conclusion, visualization of dramatic peripheral enhancement on contrast-enhanced CT in an adnexal cystic structure is the CT correlate of the sonographic “ring of fire” sign. Ectopic pregnancy should be suspected if this finding is seen in the adnexa outside the ovary, particularly with associated signs such as hemoperitoneum.
References
Dialani V, Levine D (2004) Ectopic pregnancy: a review. Ultrasound Q 20(3):105–117
Stein MW, Ricci ZJ, Novac L, Roberts JH, Koenigsberg M (2004) Sonographic comparison of the tubal ring of ectopic pregnancy with the corpus luteum. J Ultrasound Med 23:57–62
Fleischer AC, Pennell RG, McKee MS, Worrell JA, Keefe B, Herbert CM, Hill GA, Cartwright PS, Kepple DM (1990) Ectopic pregnancy: features at transvaginal sonography. Radiology 174:375–378
Taylor KJW, Ramos IM, Feyock AL, Snower DP, Carter D, Shapiro BS, Meyer WR, De Cherney AL (1989) Ectopic pregnancy: duplex Doppler evaluation. Radiology 173:93–97
Delabrousse E, Site O, Le Mouel A, Riethmuller D, Kastler B (1999) Intrahepatic pregnancy: sonography and CT findings. AJR 173:1377–1378
Pellerito JS, Taylor KJW, Quedens-Case C, Hammers LW, Scoutt LM, Ramos IM, Meyer WR (1992) Ectopic pregnancy: evaluation with endovaginal color flow imaging. Radiology 183:407–411
Jung SE, Lee JM, Rha SE, Byun JY, Jung JI, Hahn ST (2002) CT and MR imaging of ovarian tumors with emphasis on differential diagnosis. Radiographics 22(6):1305–1325
Jeong YY, Outwater EK, Kang HK (2000) Imaging evaluation of ovarian masses. Radiographics 20:1445–1470
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pham, H., Lin, E.C. Adnexal ring of ectopic pregnancy detected by contrast-enhanced CT. Abdom Imaging 32, 56–58 (2007). https://doi.org/10.1007/s00261-006-9039-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-006-9039-6