
Abstract
We present a case report on a postpartum uterine rupture with the history of a previous cesarean section. During the diagnosis of rupture, ultrasound, computerized tomography (CT) and magnetic resonance imaging of the uterus were obtained. Ultrasound examination did not result in substantial information. CT and magnetic resonance imaging established the correct diagnosis. The patient underwent exploratory laparotomy, and the diagnosis was confirmed. Diagnostic qualifications of these three instruments were compared.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Uterine rupture is a relatively uncommon but potentially devastating obstetric complication [1]. Ultrasonograpy (US) can depict most of the rupture cases, but it fails to demonstrate the uterine wall defects. This paper presents a case of uterine rupture complicated by pelvic infection and peritonitis in the postpartum period. During the pre-operative course, US, computerized tomography (CT) and magnetic resonance imaging (MRI) of the ruptured uterus were obtained and diagnostic qualifications of these three instruments were compared.
Case report
A 23-year-old woman with the history of a previous cesarean section was referred to our clinic on the postpartum second day. She had vaginally delivered at home without medical assistance and the umbilical cord was cut with a razor. She developed a severe abdominal pain and was taken to hospital. She had significant tachypnea and dyspnea on admission. Her blood pressure was 130/90 mmHg, heart rate 90 per min, and axillary body temperature was 38°C. Laboratory tests were within normal range. Abdominal examination showed extensive tenderness without significant rebound and defense. On vaginal examination with speculum, there was malodorous bloody vaginal discharge and the cervix had an edematous appearance. Trans-abdominal US examination revealed a mild amount of free fluid in the abdomen, and the uterus was of expected postpartum size with normal thickness of endometrium. However, visualization of the uterine lower segment was not clear enough to make a definite diagnosis of uterine rupture (Fig. 1). Under the guidance of ultrasonography abdominal fluid was drained by a needle and serous-purulent fluid was sampled. Antibiotics (clindamycin 2 × 600 mg/day, gentamycin 120 mg/day) were initiated. An abdominal MRI was obtained to investigate the extent of the intra-abdominal infection, abscess formation and for other probable pathologies. The ruptured myometrium was clearly demonstrated on the left lateral wall of the uterus with axial and sagittal images (Fig. 2A, B). An abdominal CT of the patient had been also obtained at the previous hospital and sent to us later. CT showed appearance of ileus and focal fluid accumulations compatible with peritonitis. There was a string of air bubbles extending from the endometrial cavity to the abdominal cavity (Fig. 3). This finding was clearly demonstrating the uterine rupture site.

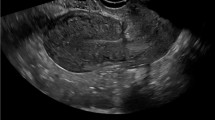
Trans-abdominal ultrasound shows a mild amount of free fluid in the Cul de Sac. Visualization of the uterine lower segment is not clear but the endometrium is regular.

A Axial T2-weighted MRI (TR, 3569; TE, 90) reveals the ruptured myometrium on the left lateral wall of the uterus (arrows). B Sagittal T2-weighted (TR, 3569; TE, 90) MRI reveals the exact rupture site at the anterior wall of the uterus (arrow).

Computerized tomography of ruptured uterus. A string of air bubbles extending from the endometrial cavity to the abdominal cavity is clearly demonstrating the uterine rupture site on the left (arrow).
Laparotomy using a median abdominal incision was performed and 1200 cc hemorrhagic fluid from the abdominal cavity was drained. There was a rupture site beginning in the middle of the previous Kerr incision line, extending very close to the left uterine artery and then turning downwards including the cervix to a level close to the vagina. This line of rupture was almost completely covered with adhesions. The margins of the rupture were clearly delineated and sutured with no. 1 vicryl. The postoperative course was uneventful, except a moderate fever necessitating antibiotics and the patient was discharged on the tenth postoperative day without any problem.
Discussion
Uterine rupture is still one of the most important causes of maternal mortality and it is reported that 20% of maternal deaths from hemorrhage were due to ruptured uterus [1]. More than 90% of the cases are associated with a prior cesarean delivery and occurs in 0.2–1.5% of patients following a low transverse incision, and 4–9% following a classical incision [2–4].
Manual examination of uterine cavity may reveal the rupture. However, failure to detect the tear manually does not rule out the diagnosis. US is very useful in detecting the postpartum uterine pathologic conditions and able to make a diagnosis of uterine rupture by demonstrating intra- or extra-peritoneal hematoma in the correct clinical setting [5]. Although the rupture site was never directly visualized by sonography, the combination of sonography and clinical findings was strongly suggestive of the correct diagnosis in the present case. Ultrasound should be considered a first step, because it can be performed bedside, does not require ionizing radiation, and is cost-effective. Although ultrasound has been successful in detecting some indirect signs of uterine rupture, thus far it has shown little success in demonstrating the myometrial defects.
CT and MRI may helpful in establishing a correct diagnosis [6–9]. MRI with better contrast resolution provides multiplanar images of the body with excellent soft-tissue contrast and without ionizing radiation. In the present case, indirect findings of the uterine rupture were obtained with US. The diagnosis was confirmed with the accurate and clear findings of MRI. CT also provided very valuable images for the diagnosis of uterine rupture. MRI gave more accurate information about the condition of the ruptured myometrium than ultrasound, and thus measurements of the rupture distance. Image quality of body, lateral and anterior wall of the uterus was better with MRI than with CT and especially with US. There was a good correlation between imaging findings and intra-operative observation in our case.
CT and MR imaging are not superior to each other in demonstrating the extent of the abnormality, but contribute in the differential diagnosis of complications of pregnancy [6]. Among the complications diagnosed with these various techniques; venous thromboembolic disorders, pyometra, hepatic hematoma and rupture, fatty liver, various hematomas, foreign bodies and tubo-ovarian abscess can be mentioned [7–9].
In conclusion, US is the first imaging modality to make the diagnose of uterine rupture. CT, particularly MRI should be reserved for the cases in which results of ultrasonography are inconclusive and patient care depends on further imaging.
References
Nagaya K, Fetters MD, Ishikawa M, et al. (2000) Causes of maternal mortality in Japan. JAMA 283:2661–2667
Miller DA, Goodwin TM, Gherman RB, et al. (1997) Intrapartum rupture of the unscarred uterus. Obstet Gynecol 89:671–673
Neuhaus W, Bauerschmitz G, Gohring U, et al. (2001) Risk of uterine rupture after cesarean section–analysis of 1,086 births. Zentralbl Gynakol 123:148–152
Brill Y, Kingdom J, Thomas J, et al. (2003) The management of VBAC at term: a survey of Canadian obstetricians. J Obstet Gynaecol Can 25:300–310
Sherer DM, Abulafia O, Anyaegbunam AM (1998) Intra- and early postpartum ultrasonography: a review. Part I. Obstet Gynecol Surv 53:107–116
Lowdermilk C, Gavant ML, Qaisi W, et al. (1999) Screening helical CT for evaluation of blunt traumatic injury in the pregnant patient. Radiographics 19:S243–S255; discussion S256–248
Rooholamini SA, Au AH, Hansen GC, et al. (1993) Imaging of pregnancy-related complications. Radiographics 13:753–770
Nishino M, Hayakawa K, Iwasaku K, et al. (2003) Magnetic resonance imaging findings in gynecologic emergencies. J Comput Assist Tomogr 27:564–570
Leyendecker JR, Gorengaut V, Brown JJ (2004) MR imaging of maternal diseases of the abdomen and pelvis during pregnancy and the immediate postpartum period. Radiographics 24:1301–1316
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Has, R., Topuz, S., Kalelioglu, I. et al. Imaging features of postpartum uterine rupture: a case report. Abdom Imaging 33, 101–103 (2008). https://doi.org/10.1007/s00261-007-9206-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-007-9206-4