
Abstract
Magnesium exhibits a range of neuronal and vascular actions that may ameliorate ischaemic CNS insults, including stroke. Significant neuroprotection with magnesium has been observed in different models of focal cerebral ischaemia in many laboratories, with infarct volume reductions between 25 and 61 %. Maximal neuroprotection is evident at readily attainable serum concentrations, and neuroprotection is still seen when administration is delayed up to 6 hours after onset of ischaemia.
Clinical use of magnesium in pre-eclampsia and acute myocardial infarction confirms its safety and tolerability. Five small trials in acute stroke have reported reduced odds of death or dependence with administration of magnesium, but confidence intervals are wide, and definitive data from ongoing large trials are awaited
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The magnesium ion has a range of effects on neurons and on vascular tissue that may contribute to a protective action in ischaemic stroke. Magnesium is a ubiquitous feature of biological systems, with physiological roles in cellular energy production [80% of magnesium being bound to adenosine triphosphate (ATP)], regulation of vascular smooth muscle tone, protein synthesis, and competitive antagonism of calcium entry at voltage- and ligand-gated ion channels [e.g. the N-methyl D-aspartate (NMDA) receptor complex].
There is evidence that magnesium affords neuroprotection in animal models of ischaemic stroke, and supportive evidence of a protective role in CNS pathology resulting from a wide variety of mechanistically relevant insults including global cerebral ischaemia and seizures. Limited clinical evidence of the efficacy of magnesium in stroke exists. This article reviews the current data on magnesium in ischaemic stroke.
1. Possible Neuroprotective Mechanisms of Magnesium
1.1 Excitotoxic and Neuronal Effects
Pathological release of glutamate and other excitatory neurotransmitters and consequent overstimulation of postsynaptic receptors is a key early feature in animal focal ischaemia models. The NMDA receptor is a particularly well documented mediator of such excitotoxic mechanisms, with consequent increases in calcium ion entry and activation of numerous downstream neurotoxic events including generation of free radicals, activation of apoptotic enzymes and initiation of proteolysis. Pharmacological blockade of excitotoxic pathways is a robust neuroprotective strategy in animal focal ischaemia models, irrespective of the precise mechanism chosen.[1]
Extracellular magnesium concentration declines in the acute phase after stroke, global forebrain ischaemia,[2] or head injury in animal models, while intracellular free magnesium concentration increases,[3] probably as a consequence of dissociation from ATP and intracellular acidosis.
Under normal conditions, active blood-brain barrier transport maintains a magnesium concentration that is higher in the brain than in the periphery. Preclinical and clinical studies show slow entry of magnesium into CSF and brain tissue,[4,5] with the peak level after a 15-minute intravenous infusion being achieved after 4 hours.[5] After intravenous or intramuscular doses that increase serum concentrations by 50 to 100%, the CSF total magnesium concentration rises by only approximately 20%,[5,6] even with a damaged blood-brain barrier.[7] While the overall increase in CSF magnesium concentration is small, much greater local concentrations around sites of pathological activity, such as seizure foci[8] or ischaemia,[9] are observed in animal models. CSF ionised (rather than total) magnesium concentrations did not increase after short intravenous infusion in patients with CNS injury,[10] but the importance of this is unclear in light of direct evidence of therapeutic effects.
By antagonising presynaptic calcium entry and potentiating adenosine action at adenosine A1 receptors,[11] magnesium inhibits glutamate release in vitro at physiological concentrations. It is unclear whether this action is important in ischaemia, but other inhibitors of glutamate release are neuroprotective.[12–14]
Magnesium ions provide a physiological voltage-dependent block of the NMDA receptor ion channel.[15] Depolarisation of the postsynaptic membrane is required in addition to glutamate binding in order to dissociate magnesium ions and permit calcium and sodium entry. Although it is not certain that increasing extracellular magnesium concentrations is able to re-establish blockade of the NMDA receptor under ischaemic conditions in vivo, this has been shown in cell culture models.[16,17] Increasing extracellular magnesium concentrations additionally contributes to an increase in intracellular concentrations that enhance NMDA receptor blockade.[18–20] More direct evidence of anti-excitotoxic actions of systemically administered magnesium come from studies indicating that magnesium reduces NMDA receptor antagonist binding characteristics at therapeutically achievable concentrations,[21] inhibits NMDA-induced seizures,[22] and is neuroprotective in a ‘pure excitotoxic’ model of neuronal injury involving intrastriatal NMDA injection.[23]
Magnesium ions antagoniseive in in vitro white matter ischaemia models,[26] probably by inhibiting sodium-calcium exchange; inorganic calcium antagonists are ineffective in these models.
Another novel feature of magnesium in animal models is its ability to prevent postanoxic depolarisations that may contribute significantly to energy failure in critically perfused neuronal tissue. This effect has been seen after intravenous administration of magnesium in a rat model of subarachnoid haemorrhage (SAH).[27]
1.2 Vascular Effects
Magnesium is a vasodilator, due to calcium channel antagonism at vascular smooth muscle and possibly more specific effects on myosin-binding proteins that regulate contraction. Magnesium administration stimulates synthesis of renin, and impairs that of aldosterone.[28] It may also promote endothelial prostacyclin synthesis.[29,30] It prevents or attenuates vasoconstriction induced by a variety of mediators including endothelin-1,[31] norepinephrine (noradrenaline), angiotensin II[32] and serotonin,[33] and counteracts vasospasm induced by SAH in animal models.[34] These effects have been observed in animal and human intracerebral vessels.[35,36] Synthetic endothelin-1 antagonists reduce the volume of cerebral infarction in focal ischaemia models.[37]
Magnesium acts as a vasodilator in human maternal and fetal circulations, including the cerebral circulation, when given as a treatment for pre-eclampsia.[38–40] In focal ischaemia in rats, magnesium infused 10 minutes after middle cerebral artery occlusion (MCAO) to serum concentrations of 3.21 mmol/L increased blood flow to the ischaemic cortex to the extent that there was no statistical difference between magnesium-treated animals and controls,[41] although no change in cerebral blood flow by laser Doppler flowmetry was seen in another MCAO model.[42]
calcium entry via voltage-gated calcium channels of all types. Excess calcium entry via postsynaptic voltage-gated channels contributes to the evolution of neuronal cell death, although quantitatively it may be less important than that via NMDA receptors.[24] Exogenous administration of magnesium may increase intracellular concentrations sufficiently to enhance postsynaptic voltage-gated calcium channel antagonism.[20] Calcium entry via voltage-gated channels may not, however, be mechanistically relevant in stroke, since there is limited preclinical evidence of significant neuroprotection with synthetic dihydropyridine calcium antagonists, and these agents have not proved beneficial in clinical trials involving over 7000 patients (see review by Horn and Limburg[25]).
Magnesium is also protectSystemic vasodilatation by magnesium infusion causes minor hypotension, but decreased systemic vascular resistance is accompanied by increased cardiac output, and retained renal function.[43]
1.3 Antiplatelet Effects
High serum concentrations of magnesium are associated with antagonism of ex vivo platelet aggregation, prolonged bleeding time and disaggregation of platelet thrombi.[44,45] Prolongation of bleeding time has also been observed in human volunteer studies using more typical therapeutic doses, with serum magnesium concentrations in the region of 1.50 mmol/L.[46,47] However, no clinically relevant bleeding complications have been observed in several large clinical trials of magnesium in patients with myocardial infarction (MI), even when coadministered with antiplatelet agents and thrombolytic drugs.[48]
2.Preclinical Data
2.1 Focal Ischaemia
Magnesium is neuroprotective in rodent models of reversible and permanent MCAO (see below). No studies using larger species have been reported. Unlike synthetic neuroprotective agents, systematic development of magnesium has not been undertaken. However, neuroprotective effects of magnesium have been confirmed in many different models, and by many different investigators, and magnesium therefore conforms to a recent key recommendation for neuroprotective drug development,[49] which emphasised the importance of obtaining robust preclinical evidence of neuroprotection before proceeding to clinical trials; this was supported by recognition that many synthetic compounds lacked such evidence.
An unexplained but consistent observation in animal models is that magnesium chloride is associated with hyperglycaemia, whereas magnesium sulphate is not.[42,50–53] Why this anion-specific effect should occur is not understood, and it has not been reported in humans. Hyperglycaemia is likely to attenuate any therapeutic effect of magnesium since it is associated with brain lactic acidosis, which is neurotoxic.[54] For example, after permanent MCAO in rats, intraperitoneal magnesium chloride reduced infarct volume by 26%, but by 44% when euglycaemia was maintained by coadministration of insulin.[50]
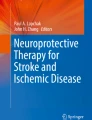
Magnesium reduces infarct volume after permanent MCAO,[50] reversible MCAO with reperfusion,[42,51] and after thrombotic MCAO.[52] The reductions in total infarct volume varied between 25% (with magnesium chloride)[42] and 61% (with magnesium sulphate).[52] As with synthetic agents, cortical infarct volumes are reduced to a greater extent than those in the basal ganglia,[42,50] but significant basal ganglia protection was also seen after reversible MCAO of 90 minutes’ duration (see figure 1).[51] Significant improvements in functional neurological recovery have been noted,[42,52] and in one study, magnesium-treated animals had significantly reduced mortality compared with controls.[52] A dosage of 90 mg/kg elevated the serum magnesium concentration to 1.49 mmol/L and was associated with a highly significant infarct volume reduction when administered prior to the induction of ischaemia[51] or, remarkably, up to 6 hours after onset of ischaemia (see figure 1).[52] Dose and time dependence of neuroprotection have been explored in two separate laboratories.

Effect of magnesium sulphate on cerebral ischaemia in rat focal ischaemia models. (a) Dose of magnesium sulphate versus infarct volume in reversible middle cerebral artery suture occlusion for 1.5 hours followed by reperfusion for 24 hours. Magnesium sulphate was infused intra-arterially over 10 minutes before induction of ischaemia. Mean peak serum magnesium concentrations were 1.08 ± 0.13 mmol/L in the 30 mg/kg group and 1.49 ± 0.18 mmol/L in the 90 mg/kg group (reproduced from the Journal of Neurosurgery, Marinov et al.,[51] with permission). (b) Infarct volume and effects of delay in treatment after induction of ischaemia by thrombus injection to the middle cerebral artery. Animals were treated with magnesium sulphate 90 mg/kg intravenously 2, 4 or 8 hours after the induction of ischaemia (reprinted from Neuroscience Letters, Yang et al.,[52] with permission from Elsevier Science). * p < 0.05 vs control.
2.2 Other Relevant Models
Systemically administered magnesium significantly reduces cerebral infarction after SAH in rats induced by penetrating intraluminal carotid artery injury, and prevents the postanoxic depolarisation seen in this model.[27]
Amelioration of spinal cord ischaemia has been reported,[55–57] but comparisons with brain ischaemia studies are difficult since very high doses were given in the studies of spinal cord ischaemia (sufficient to cause neuromuscular blockade,[55] or 300 to 600 mg/kg[57]) or the route was intrathecal.[56] Improved functional recovery[56,58] and preservation of neurophysiological responses[57] were reported.
Systemic magnesium administration attenuates or abolishes the induction of seizures by administration of penicillin,[59] strychnine[60] and NMDA[22,61] or electrical stimulation,[8] but not status epilepticus induced by administration of pentylenetetrazol.[62]
In global forebrain ischaemia models, neuronal salvage has been reported even with very delayed postischaemic administration of magnesium, but these studies have involved direct brain infusion of high concentrations of magnesium and are of uncertain relevance.[63] In two studies using more therapeutically relevant dosing regimens, magnesium improved neurological function in dogs after global ischaemia and reperfusion,[64] but was histologically ineffective in rats when administered after 10 minutes of forebrain ischaemia.[53] Similar dissociation of functional recovery from histology was seen after spinal cord ischaemia in rats given intrathecal magnesium.[58]
Magnesium improves functional and histological outcomes after head trauma in a range of rodent models, including focal fluid-percussion injury, contusional or electrolytic lesions, and diffuse axonal injury, even if administered 30 minutes after injury.[65–70]
3. Clinical Data
3.1 Stroke
Data from four small clinical trials that have assessed the effects of magnesium in patients with stroke are available at present.[71–74] These include 162 patients treated within 12 or 24 hours of stroke onset. Outcomes were assessed between 30 days and 6 months after stroke. Details of administration regimen and trial design are given in table I.

Clinical trials of magnesium in patients with acute stroke
Systematic review of these trials (figure 2) yields an odds ratio for death and disability of 0.67 (95% confidence interval 0.35 to 1.26), and an absolute risk reduction for poor outcome of around 8%.[78] The wide confidence intervals reflect the small numbers of participants, and overall power to detect a difference of the observed magnitude was only 16%. A larger trial involving 510 participants reported a similar magnitude of benefit using unconventional outcome measures,[75] but was excluded from systematic review since randomisation and blinding procedures were not described.

Death and disability at final follow-up in all completed trials of magnesium for stroke. Randomisation and blinding procedures were not specified for one trial, which was therefore excluded from analysis. IMAGES = Intravenous Magnesium Efficacy in Acute Stroke trial; n/N = number with outcome/sample size.
For three studies in which blood pressure data were available, diastolic blood pressure was significantly lower in magnesium-treated patients at 24 hours, but not at earlier time points.[71–73] Overall mean peak serum magnesium concentration was 1.50 mmol/L, although this is derived from trials in which the majority of patients received loading infusions of 8 mmol; a dose-optimisation study found 16 mmol to achieve higher serum concentrations (mean peak concentration of 1.84 mmol/L) rapidly and without safety concerns.[72]
3.2 Other Conditions
Magnesium has predominantly been used in treatment of pre-eclampsia/eclampsia and acute MI.
Several large trials, and systematic review of data, confirm significant benefit in seizure prevention and treatment in pre-eclampsia and eclampsia.[79–82] Typical therapeutic regimens use high doses, e.g. intravenous magnesium sulphate 16 mmol is followed by either a 4 to 8 mmol/h intravenous infusion, or intramuscular administration of 40 mmol (10g) then 20 mmol 4-hourly, and serum concentrations maintained at around 2.1 to 2.6 mmol/L.[83]
In MI, initially positive results from systematic review[84] and one moderately large trial[85] were contradicted by the findings of the Fourth International Study of Infarct Survival (ISIS-4) megatrial,[48] where no benefit was found. However, debate continues, and some further small trials con- tinue to report the benefit of magnesium with respect to a reduced incidence of dysrhythmias.[86]
These data on the use of magnesium in these indications are pertinent since they confirm the safety and tolerability of magnesium infusions similar to those employed in stroke trials. They also provide supportive evidence of CNS effects at readily achieved serum magnesium concentrations that are well within the neuroprotective range seen in animal models of focal ischaemia.[51] The absence of a significant benefit in MI does not necessarily have implications for stroke trials, since the a priori hypothesis for mechanism of action centred around antiarrhythmic or antiplatelet effects that were not confirmed in ISIS-4, and experimental data are minimal. The multiple neuronal mechanisms that potentially contribute to (or cause) the neuroprotective effects of magnesium are also not relevant in this situation.
3.3 Ongoing Trials
The Intravenous Magnesium Efficacy in Stroke (IMAGES) trial is an academic multicentre trial powered to detect a 5.5% absolute difference in death and disability 3 months after stroke.[76] It is funded by the UK Medical Research Council and has recruited more than 67% of a planned 2700 patients at the time of writing. The sample size for IMAGES was calculated on the basis of pilot trial results[71] which have subsequently been supported by systematic review of all magnesium trial data. IMAGES is a worldwide study, with centres in the UK, mainland Europe, North and South America, Australasia, Singapore and China.
A substudy of IMAGES, MR-IMAGES, utilises magnetic resonance imaging techniques that allow comparison of lesion volume at acute and later time points; the promise of these parameters as biomarkers for efficacy has been shown in other neuroprotective trials.[87] MR-IMAGES will recruit 150 patients, which gives 80% power to detect a 25% difference in the proportion of patients exhibiting lesion growth.
The Field Administration of Stroke Therapy-Magnesium (FAST-MAG) trial is presently in its pilot phase, and a full trial is planned.[77] This study utilises prehospital treatment of patients with suspected stroke, commenced by paramedics and continued after hospital admission.
4. Conclusions
Preclinical data indicate significant neuroprotection by magnesium in several different models of ischaemic stroke, with maximal effect at readily achieved serum concentrations, and a protracted therapeutic window of 6 hours. Improvements in survival, brain oedema and functional outcome are all reported independently by a number of different laboratories. Similar benefits have been found in models of SAH, head trauma, seizures and spinal cord ischaemia. There is evidence of an action in specific neuronal pathways such as NMDA receptor-mediated excitotoxic injury, but other possibly pertinent actions include calcium antagonism, vasodilatation, endothelin antagonism, and enhanced regional cerebral blood flow. Peripherally administered magnesium enters the CSF and the brain, but does not have any known detrimental adverse effects at therapeutic concentrations.
Clinical data are presently too limited to permit definite conclusions on the effects of magnesium in patients with stroke. Stroke trials completed to date involve only 162 participants, and although point estimates of effect indicate reduced death and disability 1 to 6 months after stroke compared with controls, the confidence intervals are very wide. Estimates of effect size are comparable with existing stroke treatments.[88] One major trial (IMAGES) is ongoing, and a further (FAST-MAG) is planned.
Magnesium has a profile comparable with, or superior to, synthetic neuroprotective drugs. Nevertheless, no neuroprotective agent has so far been successful in clinical trials and there have been a large number of failures with compounds that had promising preclinical results (see review by Gorelick[89]).
A number of potential weaknesses in stroke trial design have been identified, many of which studies of magnesium that have been performed to date have avoided (e.g. reproducibility of preclinical data, pharmacokinetic problems leading to potential under-dosing).[49] The major compromise in the design of IMAGES is the long time window of 12 hours, which may reduce the study power by including a high proportion of patients with already established irreversible ischaemic damage. Such compromises are necessary to boost recruitment from smaller centres not used to participating in acute treatment trials since financial constraints prevent competition with industry-funded trials that dominate in large stroke centres. However, since earlier administration will be addressed in FAST-MAG, and biomarkers for efficacy will be available from the MR-IMAGES substudy, the neuroprotective potential of magnesium should be tested fully.
If the ongoing trials are successful, the advantages would be considerable. Magnesium is inexpensive and readily available, and worldwide uptake would be anticipated. Since stroke is the second biggest cause of mortality worldwide, even modest reductions in death and disability may have huge consequences if treatment can be widely delivered.
References
McCulloch J. Excitatory amino acid antagonists and their potential for the treatment of ischaemic brain damage in man. Br J Clin Pharmacol 1992; 34: 106–14
Van de Linde AM, Chopp M, Chen H, et al. Chronic changes in the brain Mg2+ concentration after forebrain ischemia in the rat. Metab Brain Dis 1991; 6: 199–206
Helpern JA, Vande Linde AM, Welch KM, et al. Acute elevationand recovery of intracellular [Mg2+] following human focal cerebral ischemia. Neurology 1993; 43: 1577–81
Oppelt WW, MacIntyre I, Rall DP. Magnesium exchange between blood and cerebrospinal fluid. Am J Physiol 1963; 205: 959–62
Fuchs-Buder T, Tramer MR, Tassonyi E. Cerebrospinal fluid passage of intravenous magnesium sulfate in neurosurgical patients. J Neurosurg Anesthesiol 1997; 9: 324–8
Thurnau GR, Kemp DB, Jarvis A. Cerebrospinal fluid levels of magnesium in patients with preeclampsia after treatment with intravenous magnesium sulfate: a preliminary report. Am J Obstet Gynecol 1987; 157: 1435–8
Fong J, Gurewitsch ED, Volpe L, et al. Baseline serum and cerebrospinal fluid magnesium levels in normal pregnancy and preeclampsia. Obstet Gynecol 1995; 85: 444–8
Hallak M, Berman RF, Irtenkauf SM, et al. Peripheral magnesium sulfate enters the brain and increases the threshold for hippocampal seizures in rats. Am J Obstet Gynecol 1992; 167: 1605–10
Sjostrom LG, Wester P. Accumulation of magnesium in rat brain after intravenously induced hypermagnesemia [abstract]. Cerebrovasc Dis 1995; 5: 241
Brewer RP, Parra A, Hopkins MB, et al. Magnesium sulfate does not increase ventricular cerebrospinal fluid ionized magnesium concentration in patients with intracranial hypertension [abstract]. Stroke 2001; 32: 375
Bartrup JT, Stone TW. Presynaptic actions of adenosine are magnesium-dependent. Neuropharmacology 1988; 27: 761–3
Aronowski J, Strong R, Grotta JC. Treatment of experimental focal ischemia in rats with lubeluzole. Neuropharmacology 1996; 35: 689–93
MacKay KB, Kusumoto K, Graham DI, et al. Effect of the kappa-1 opioid agonist CI-977 on ischemic brain damage and cerebral blood flow after middle cerebral artery occlusion in the rat. Brain Res 1993; 629: 10–8
Meldrum BS, Smith SE, Lekieffre D, et al. Sodium channel blockade and glutamate release: the mechanism of cerebroprotection by lamotrigine, BW 1003C87 and BW 619C89. In: Krieglstein J, Oberpichler-Schwenk, editors. Pharmacology of cerebral ischemia. Stuttgart: Medpharm, 1994: 203–9
Nowak L, Bregestovski P, Ascher P, et al. Magnesium gates glutamate-activated channels in mouse central neurones. Nature 1984; 307: 462–5
Ascher P, Nowak L. The role of divalent cations in the N-methyl-D-aspartate responses of mouse central neurones in culture. J Physiol 1988; 399: 247–66
Frandsen A, Schousboe A. Effect of magnesium on NMDA mediated toxicity and increases in [Ca2+]i and cGMP in cultured neocortical neurons: evidence for distinct regulation of different responses. Neurochem Int 1994; 25: 301–8
Johnson JW, Ascher P. Voltage-dependent block by intracellular Mg2+ of N-methyl-D-aspartate-activated channels. Biophys J 1990; 57: 1085–90
Li-Smerin Y, Johnson JW. Kinetics of the block by intracellular Mg2+ of the NMDA-activated channel in cultured rat neurons. J Physiol 1996; 491: 121–35
Brocard JB, Rajdev S, Reynolds IJ. Glutamate-induced increases in intracellular free Mg2+ in cultured cortical neurons. Neuron 1993; 11: 751–7
Hallak M, Berman RF, Irtenkauf SM, et al. Magnesium sulfate treatment decreases N-methyl-D-aspartate receptor binding in the rat brain: an autoradiographic study. J Soc Gynecol Investig 1994; 1: 25–30
Cotton DB, Hallak M, Janusz C, et al. Central anticonvulsant effects of magnesium sulfate on N-methyl-D-aspartate-induced seizures. Am J Obstet Gynecol 1993; 168: 974–8
McDonald JW, Silverstein FS, Johnston MV. Magnesium reduces N-methyl-D-aspartate (NMDA)-mediated brain injury in perinatal rats. Neurosci Lett 1990; 109: 234–8
Eimerl S, Schramm M. The quantity of calcium that appears to induce neuronal death. J Neurochem 1994; 62: 1223–6
Horn J, Limburg M. Calcium antagonists for ischemic stroke: a systematic review. Stroke 2001; 32: 570–6
Stys PK, Ransom BR, Waxman SG. Effects of polyvalent cations and dihydropyridine calcium channel blockers on recovery of CNS white matter from anoxia. Neurosci Lett 1990; 115: 293–9
van den Bergh W, Zuur K, Kamerling N, et al. Magnesium reduces depolarization time and lesion volume after subarachnoid hemorrhage in the rat [abstract]. Cerebrovasc Dis 2001; 11: 109
Ichihara A, Suzuki H, Saruta T. Effects of magnesium on the renin-angiotensin-aldosterone system in human subjects. J Lab Clin Med 1993; 122: 432–40
Nadler JL, Goodson S, Rude RK. Evidence that prostacyclin mediates the vascular action of magnesium in humans. Hypertension 1987; 9: 379–83
O’Brien WF, Williams MC, Benoit R, et al. The effect of magnesium sulfate infusion on systemic and renal prostacyclin production. Prostaglandins 1990; 40: 529–38
Kemp PA, Gardiner SM, March JE, et al. Assessment of the effects of endothelin-1 and magnesium sulphate on regional blood flows in conscious rats, by the coloured microsphere reference technique. Br J Pharmacol 1999; 126: 621–6
Aisenbrey GA, Corwin E, Catanzarite V. Effect of magnesium sulfate on the vascular actions of norepinephrine and angiotensin II. Am J Perinatol 1992; 9: 477–80
Torregrosa G, Perales AJ, Salom JB, et al. Different effects of Mg2+ on endothelin-1- and 5-hydroxytryptamine-elicited responses in goat cerebrovascular bed. J Cardiovasc Pharmacol 1994; 23: 1004–10
Ram Z, Sadeh M, Shacked I, et al. Magnesium sulfate reverses experimental delayed cerebral vasospasm after subarachnoid hemorrhage in rats. Stroke 1991; 22: 922–7
Perales AJ, Torregrosa G, Salom JB, et al. In vivo and in vitro effects of magnesium sulfate in the cerebrovascular bed of the goat. Am J Obstet Gynecol 1991; 165: 1534–8
Alborch E, Salom JB, Perales AJ, et al. Comparison of the anticonstrictor action of dihydropyridines (nimodipine and nicar-dipine) and Mg2+ in isolated human cerebral arteries. Eur J Pharmacol 1992; 229: 83–9
Patel TR, Galbraith S, Graham DI, et al. Endothelin receptor antagonist increases cerebral perfusion and reduces ischaemic damage in feline focal cerebral ischaemia. J Cereb Blood Flow Metab 1996; 16: 950–8
Belfort MA, Saade GR, Moise Jr KJ. The effect of magnesium sulfate on maternal retinal blood flow in preeclampsia: a randomized placebo-controlled study. Am J Obstet Gynecol 1992; 167: 1548–53
Belfort MA, Moise Jr KJ. Effect of magnesium sulfate on maternal brain blood flow in preeclampsia: a randomized, placebo-controlled study. Am J Obstet Gynecol 1992; 167: 661–6
Scardo JA, Hogg BB, Newman RB. Favorable hemodynamic effects of magnesium sulfate in preeclampsia. Am J Obstet Gynecol 1995; 173: 1249–53
Chi OZ, Pollak P, Weiss HR. Effects of magnesium sulfate and nifedipine on regional cerebral blood flow during middle cerebral artery ligation in the rat. Arch Int Pharmacodyn Ther 1990; 304: 196–205
Schmid-Elsaesser R, Zausinger S, Hungerhuber E, et al. Neuro-protective effects of combination therapy with tirilazad and magnesium in rats subjected to reversible focal cerebral ischemia. Neurosurgery 1999; 44: 163–71
Crozier TA, Radke J, Weyland A, et al. Haemodynamic and endocrine effects of deliberate hypotension with magnesium sulphate for cerebral-aneurysm surgery. Eur J Anaesthesiol 1991; 8: 115–21
Adams JH, Mitchell Jr. The effect of agents which modify platelet behaviour and of magnesium ions on thrombus formation in vivo. Thromb Haemost 1979; 42: 603–10
Kurgan A, Gertz SD, Wajnberg RS, et al. Effect of magnesium sulfate on platelet deposition in rabbits following temporary arterial occlusion with surgical clips. Surgery 1980; 87: 390–6
Ravn HB, Vissinger H, Kristensen SD, et al. Magnesium inhibits platelet activity — an infusion study in healthy volunteers. Thromb Haemost 1996; 75: 939–44
Kynczl-Leisure M, Cibils LA. Increased bleeding time aftermagnesium sulfate infusion. Am J Obstet Gynecol 1996; 175: 1293–4
ISIS-4 Collaborative Group. ISIS-4: arandomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58050 patients with suspected acute myocardial infarction. Lancet 1995; 345: 669–85
Stroke Therapy Academic Industry Roundtable (STAIR). Recommendations for standards regarding preclinical neuro-protective and restorative drug development. Stroke 1999; 30: 2752–8
Izumi Y, Roussel S, Pinard E, et al. Reduction of infarct volume by magnesium after middle cerebral artery occlusion in rats. J Cereb Blood Flow Metab 1991; 11: 1025–30
Marinov MB, Harbaugh KS, Hoopes PJ, et al. Neuroprotective effects of preischemia intraarterial magnesium sulfate in reversible focal cerebral ischemia. J Neurosurg 1996; 85: 117–24
Yang Y, Li Q, Ahmad F, et al. Survival and histological evaluation of therapeutic window of post-ischemia treatment with magnesium sulfate in embolic stroke model of rat. Neurosci Lett 2000; 285: 119–22
Blair JL, Warner DS, Todd MM. Effects of elevated plasma magnesium versus calcium on cerebral ischemic injury in rats. Stroke 1989; 20: 507–12
Peek KE, Lockwood AH, Izumiyama M, et al. Glucose metabolism and acidosis in the metabolic penumbra of rat brain. Metab Brain Dis 1989; 4: 261–2
Vacanti FX, Ames III A. Mild hypothermia and Mg++ protect against irreversible damage during CNS ischemia. Stroke 1984; 15: 695–8
Simpson JI, Eide TR, Schiff GA, et al. Intrathecal magnesium sulfate protects the spinal cord from ischemic injury during thoracic aortic cross-clamping. Anesthesiology 1994; 81: 1493–9
Suzer T, Coskun E, Islekel H, et al. Neuroprotective effect of magnesium on lipid peroxidation and axonal function after experimental spinal cord injury. Spinal Cord 1999; 37: 480–4
Follis F, Miller K, Scremin OU, et al. NMD A receptor blockade and spinal cord ischemia due to aortic crossclamping in the rat model. Can J Neurol Sci 1994; 21: 227–32
Borges LF, Gucer G. Effect of magnesium on epileptic foci. Epilepsia 1978; 19: 81–91
Decollogne S, Tomas A, Lecerf C, et al. NMDA receptor complex blockade by oral administration of magnesium: comparison with MK-801. Pharmacol Biochem Behav 1997; 58: 261–8
Mason BA, Standley CA, Irtenkauf SM, et al. Magnesium is more efficacious than phenytoin in reducing N-methyl-D-aspartate seizures in rats. Am J Obstet Gynecol 1994; 171: 999–1002
Link MJ, Anderson RE, Meyer FB. Effects of magnesium sulfate on pentylenetetrazol-induced status epilepticus. Epilepsia 1991; 32: 543–9
Tsuda T, Kogure K, Nishioka K, et al. Mg2+ administered up to twenty-four hours following reperfusion prevents ischemic damage of the CA1 neurons in the rat hippocampus. Neuroscience 1991; 44: 335–41
Okawa M. Effects of magnesium sulfate on brain damage by complete global brain ischemia [in Japanese]. Masui 1992; 41: 341–55
McIntosh TK, Vink R, Yamakami I, et al. Magnesium protects against neurological deficit after brain injury. Brain Res 1989; 482: 252–60
Smith DH, Okiyama K, Gennarelli TA, et al. Magnesium and ketamine attenuate cognitive dysfunction following experimental brain injury. Neurosci Lett 1993; 157: 211–4
Okiyama K, Smith DH, Gennarelli TA, et al. The sodium channel blocker and glutamate release inhibitor BW1003C87 and magnesium attenuate regional cerebral edema following experimental brain injury in the rat. J Neurochem 1995; 64: 802–9
Hoane MR, Irish SL, Marks BB, et al. Preoperative regimens of magnesium facilitate recovery of function and prevent sub-cortical atrophy following lesions of the rat sensorimotor cortex. Brain Res Bull 1998; 45: 45–51
Feldman Z, Gurevitch B, Artru AA, et al. Effect of magnesium given 1 hour after head trauma on brain edema and neurological outcome. J Neurosurg 1996; 85: 131–7
Heath DL, Vink R. Neuroprotective effects of MgSO4 and MgC12 in closed head injury: a comparative phosphorus NMR study. J Neurotrauma 1998; 15: 183–9
Muir KW, Lees KR. A randomised, double-blind, placebo-controlled pilot trial of intravenous magnesium sulfate in acute stroke. Stroke 1995; 26: 183–8
Muir KW, Lees KR. Dose optimization of intravenous magnesium sulfate after acute stroke. Stroke 1998; 29: 918–23
IMAGES Study Group, Bradford APJ, Muir KW, et al. IMAGES pilot study of intravenous magnesium in acute stroke [abstract]. Cerebrovasc Dis 1998; 8: 86
Wester PO, Asplund K, Eriksson S, et al. Infusion of magnesium in patients with acute brain infarction [abstract]. Acta Neurol Scand 1984; 70: 143
Galeas T, Contos T, Exarhos P, et al. The role of magnesium (Mg) a natural calcium (Ca) antagonist in the treatment of acute ischaemic stroke (clinical study) [abstract]. Cerebrovasc Dis 1999; 9: 102
Bradford APJ, Lees KR. Design of the Intravenous Magnesium Efficacy in Acute Stroke (IMAGES) trial. Curr Control Trial Cardiovasc Med 2000; 1: 184–90
Saver JL, Kidwell CS, Leary MC, et al. The Field Administration of Stroke Therapy-Magnesium (FAST-MAG) pilot trial: a study of prehospital neuroprotective therapy. Proceedings of the 26th International Stroke Conference; 2001 Feb 14–16; Fort Lauderdale (FL)
Muir KW. Systematic review of clinical trials of magnesium for acute stroke [abstract]. Stroke 2001; 31: 379
Lucas MJ, Leveno KJ, Cunningham FG. A comparison of magnesium sulfate with phenytoin for the prevention of eclampsia. N Engl J Med 1995; 333: 201–5
The Eclampsia Trial Collaborative Group. Which anticonvulsant for women with eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet 1995; 345: 1455–63
Chien PF, Khan KS, Arnott N. Magnesium sulphate in the treatment of eclampsia and pre-eclampsia: an overview of the evidence from randomised trials. Br J Obstet Gynaecol 1996; 103: 1085–91
Coetzee EJ, Dommisse J, Anthony J. A randomised controlled trial of intravenous magnesium sulphate versus placebo in the management of women with severe pre-eclampsia. Br J Obstet Gynaecol 1998; 105: 300–3
Sibai BM, Graham JM, McCubbin JH. A comparison of intravenous and intramuscular magnesium sulfate regimens in preeclampsia. Am J Obstet Gynecol 1984; 150: 728–33
Teo KK, Yusuf S, Collins R, et al. Effects of intravenous magnesium in suspected acute myocardial infarction: an overview of the randomised trials. BMJ 1991; 303: 1499–503
Woods KL, Fletcher S, Roffe C, et al. Intravenous magnesium sulphate in suspected acute myocardial infarction: results of the second Leicester Intravenous Magnesium Intervention Trial (LIMIT-2). Lancet 1992; 339: 1553–8
Thogersen AM, Johnson O, Wester PO. Effects of intravenous magnesium sulphate in suspected acute myocardial infarction on acute arrhythmias and long-term outcome. Int J Cardiol 1995; 49: 143–51
Warach S, Pettigrew LC, Dashe JF, et al. Effect of citicoline on ischemic lesions as measured by diffusion-weighted magnetic resonance imaging. Citicoline 010 Investigators. Ann Neurol 2000; 48: 713–22
The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995; 333: 1581–7
Gorelick PB. Neuroprotection in acute ischaemic stroke: a tale of for whom the bell tolls? Lancet 2000; 355: 1925–6
Acknowledgements
Dr Muir is supported by Chest, Heart and Stroke, Scotland, a registered charity. He is co-principal investigator of the IMAGES trial, sponsored by the UK Medical Research Council, and is a member of the steering committee of MR-IMAGES.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Muir, K.W. Magnesium for Neuroprotection in Ischaemic Stroke. CNS Drugs 15, 921–930 (2001). https://doi.org/10.2165/00023210-200115120-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00023210-200115120-00002