
Abstract
An important goal of cancer surgery is to achieve negative surgical margins and remove all disease completely. For pancreatic neoplasms, microscopic margins may remain positive despite gross removal of the palpable mass, and surgeons must then consider extending resection, even to the point of completion pancreatectomy, an option that renders the patient with significant adverse effects related to exocrine and endocrine insufficiency. Counterintuitively, extending resection to ensure clear margins may not improve patient outcome. Furthermore, the goal of improving survival by extending the resection may not be achieved, as an initial positive margin may indicate more aggressive underlying tumor biology. There is a growing body of literature on this topic, and this landmark series review will examine the key publications that guide our management for resection of pancreatic ductal adenocarcinoma, intraductal papillary mucinous neoplasms, and pancreatic neuroendocrine tumors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
For patients who successfully undergo surgical resection of pancreatic neoplasms, particularly pancreatic ductal adenocarcinoma (PDAC), several prognostic variables are thought to impact survival, such as postoperative complications, nodal status, receipt of multimodality therapy, and margin-negative resection.1,2,3 Pancreatic surgeons must use sound technique to minimize the risk of postoperative complications while performing a nodal dissection to ensure adequate staging information, and attempt to achieve a negative margin resection. However, controversy remains on the benefit of extending resection margins even to the point of completion pancreatectomy based on intraoperative frozen section analysis. It remains unclear if completion pancreatectomy improves patient survival or simply leaves patients with difficult-to-manage diabetes mellitus and malabsorption without adding any cancer-specific survival benefit. This landmark series will review the literature for intraoperative margin assessment for patients undergoing pancreaticoduodenectomy (PD) or distal pancreatectomy (DP) for PDAC, as well as address these principles for patients undergoing resection for non-PDAC tumor types, such as intraductal papillary mucinous neoplasms (IPMNs) or pancreatic neuroendocrine tumors (PanNET).
Pancreatic Ductal Adenocarcinoma
PDAC comprises only 3% of all cancer diagnoses each year in the US, yet it is the fourth leading cause of cancer-related mortality for each sex.4,5 Despite the steady improvement in survival of other gastrointestinal cancers, the 5-year survival for resected PDAC remains low at 10%,6,7 and fewer than 25% of patients presenting with PDAC are amenable to curative surgical resection.8,9,10 A critical factor affecting survival outcomes of patients undergoing surgical resection for PDAC is the status of resection margins. It is imperative that the surgical margins be evaluated thoroughly by an expert pathologist using a standardized protocol—axial slicing versus bisectioning of the pancreatic head and orange-peeling approach; both these methods result in an increase in the resection margin positivity rate.11,12
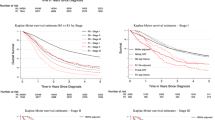
While sound surgical oncologic principles dictate that negative margin resections are associated with improved overall survival, recent evidence has challenged this surgical dogma for PDAC. A recent cohort-matched study in 202 patients demonstrated lack of improvement in survival after extending pancreatic neck resection margins based on initial positive intraoperative margin assessment at the time of PD.13 Patients who underwent extension of the neck margin to achieve a final negative margin (n = 17) had similar poor median survival (11 months; p = 0.001) as those patients who were left with a microscopic positive neck resection margin (n = 44, 13 months; p = 0.02), when compared with R0 resection (n = 141, 21 months), suggesting that the act of extending the margin to clear microscopic positive disease was an exercise in futility.13
The relationship between negative surgical margin resection and overall patient survival may however be an oversimplification, as margin-negative resection is likely easier to achieve when disease biology is more favorable, and a positive surgical margin may be a surrogate of disease biology. The definition of margin-negative resection for PDAC also requires further clarification, as some clinicians define a negative margin as >1 mm from the ink, while others classify a clear margin as any negative microscopic margin. The American Joint Committee on Cancer (AJCC) 8th Edition defines microscopic positive margin (R1) as cancer cells within 1 mm of the margin.14 Surgical margin assessment for PDAC can be further stratified by operation type: PD versus DP.
Pancreatoduodenectomy
PD is a complex operation with several defined margins, some of which are more amenable to surgical remediation at the time of surgery based on intraoperative frozen section results, while others are not. Resection margin assessment (Fig. 1) is classified into three categories: (1) transection margins, which include the pancreatic neck, bile duct, gastric or duodenal, and jejunal or enteric margins; (2) dissection (or mobilization) margins, which include the posterior margin, superior mesenteric vein/portal vein (SMV/PV) margin, and superior mesenteric artery (SMA) margin; and (3) anterior surface margin.15 The anterior margin is an anatomical surface and is not a true resection margin as no tissue is transected.14 Resection margin status is relevant as several multicenter studies and post hoc analyses of randomized controlled trials (RCTs) confirm the prognostic significance of margin-negative resection with PD.16,17,18,19

Resection margins after pancreatoduodenectomy. SMV superior mesenteric vein
Margin Assessment
Among resection margins, unlike the SMA margin, both the biliary and the pancreatic neck margin can often be extended if assessed positive on intraoperative frozen section. As the bile duct margin is rarely positive in PDAC cases,17 this review will focus on the pancreatic neck transection margin. This margin is the focus of several large retrospective multicenter studies (Table 1)13,17,20,21 as well as post hoc analyses of RCTs.16 Post hoc analyses of the European Study Group for Pancreatic Cancer 3 (ESPAC-3) trial revealed that in comparison with R0 margin, R1-direct tumor margin (tumor is present microscopically at the margin, not < 1 mm from the margin) and R1-direct posterior resection margin were independently associated with worse overall survival [hazard ratio (HR) 1.31, p = 0.003; and HR 1.34, p = 0.02, respectively] and recurrence- free survival (HR 1.34, p = 0.001; and HR 1.28, p = 0.047, respectively).16
The largest multicenter study on this topic is from the Central Pancreatic Consortium (CPC). This analysis of 1399 PD cases for PDAC (90% of whom were treatment-naïve, with 10% receiving neoadjuvant therapy [NAT]) reported the following difference in overall survival: re-resection of pancreatic neck parenchyma to achieve an R0 margin when microscopic margin was positive on frozen section (n = 72, 11.9 months) versus permanent R1 margin (n = 131, 13.7 months) versus R0 margin on permanent section without re-excision (n = 1196, 21.1 months; p < 0.001). The margins converted to R0 after R1 on frozen section predicted worse overall survival compared with R0 margin on permanent section without re-excision (HR 1.55; p = 0.009).17 In this study, patients with R1 margin on frozen section who were converted to R0 (RF) or R1 margin on permanent section (RP) had larger tumors (RF: 3.3 ± 1.2 cm and RP: 3.5 ± 1.2 cm vs. R0: 3 ± 1.4 cm; p = 0.001), higher rates of node-positive disease (RF: 76% and RP: 74% vs. R0: 67%; p = 0.08) and perineural invasion (RF: 81% and RP: 86% vs. R0: 73%; p = 0.02) compared with patients with R0 margin achieved without re-excision (R0), suggestive of a more aggressive tumor biology.22 There are several other smaller studies that support the findings of the CPC study.13,20,21,23
In contrast, others studies have demonstrated that re-resection may be beneficial for long-term survival.18,24,25 A study from the Dresden group (n = 483) re-examined the value of frozen section to guide additional pancreatic parenchyma resection at the time of surgery for PDAC from 1993 to 2014.25 The authors found that re-resection of positive margin on frozen section with conversion to a negative margin was associated with a similar survival time (36 months) to that of patients having an initial R0 resection margin (29 months, p = 0.849), and superior to that of patients having a final R1 margin on permanent section (12 months, p = 0.039). There are some important differences with regard to this study design and patient population compared with the CPC study. No information regarding postoperative therapy was provided, and only 7.6% of patients received NAT. Perhaps the key difference between the Dresden and CPC studies was the baseline tumor histology; while all patients included in the CPC study had PDAC without evidence of underlying mucinous neoplasm, 30.6% of the 483 Dresden patients had an underlying diagnosis other than true PDAC, obfuscating the interpretation of these results.25
The most recent report from the Massachusetts General Hospital and University of Verona (n = 986) reported an associated improvement in survival with R0 margin resection (without re-excision) of 28 months compared with persistent R1 margin on permanent section (19 months; p = 0.01).18 Re-excision to achieve R0 margin (when R1 was noted on frozen section) was also associated with improvement in survival (24 months) compared with persistent R1 margin on permanent section (19 months; p = 0.02). Total pancreatectomy was performed in 28% of patients in whom the margin was rendered R0 on permanent section after R1 determination on frozen section. NAT was administered in 21% of patients, and only 15% of patients had T3/T4 tumors, suggesting a different patient population than the CPC study. The initial positive margin rate was nearly double (20%) in comparison with the CPC study (11%), perhaps related to the difference in positive margin definition used, as this group used the ‘en face’ definition of 0 mm, compared with the AJCC 8th edition definition of >1 mm used by the CPC. Ultimately, these three studies continue to stimulate the controversy of checking frozen section margins to prompt additional pancreatic parenchymal resection.
With the improvements in chemotherapy and radiation therapy for treating PDAC, we need to understand the impact of NAT on margin status and patient outcome. In early-stage PDAC (cT1–2), NAT has been shown to significantly decrease the margin positivity rate compared with no NAT (NAT, 15.5% vs. no NAT, 21.8%; p < 0.0001), and more so with neoadjuvant chemoradiation therapy (NCRT) than chemotherapy (NCT) alone (NCRT, 13.4% vs. NCT, 18.6%; p < 0.001). Furthermore, positive margin was associated with worse overall survival (14.9 months) compared with negative margin resection (23.9 months; HR 1.702, p < 0.0001).26 In the phase III RCT (Unicancer GI PRODIGE 24/CCTG PA.6 trial), where patients with PDAC underwent the surgery-first approach prior to randomization to one of the two adjuvant therapy arms (FOLFIRINOX vs. gemcitabine), the incidence of R1 margin positivity was 42.8%.27 In the recently reported SWOG S1505 randomized trial in resectable PDAC patients who received 12 weeks of NAT (mFOLFIRINOX or gemcitabine/nab-paclitaxel), the margin-negative resection rate was 85%.28 These studies suggest a potential role of NAT in decreasing the margin positivity rate. Whether this impacts survival still remains unclear.
In a recently published multicenter retrospective study of 305 patients in Japan and the US who received NAT, R0 margin (>90%; 0 mm rule) was associated with an improved overall survival compared with R1 margin (31.3 vs. 16.3 months; p < 0.001).29 Overall survival in this study was measured from the date of surgery rather than from the date of diagnosis or the date of first treatment. This is important to note as the survival, when calculated from the date of surgery, ignores the variability in duration of NAT received by the patient, biasing the survival results and potentially resulting in a more pronounced survival difference. This pronounced survival difference was also noted during unpublished survival analyses, when determining the optimal timing between diagnosis and treatment of pancreatic cancer.30
Another single-institution study from Johns Hopkins assessed the impact of margin status on survival after NAT, where 484 patients with PDAC received NAT for ≥2 months between 2011 and 2018.31 Median duration of neoadjuvant chemotherapy was 119 days, with 67% of patients receiving FOLFIRINOX as first-line therapy and 73% receiving neoadjuvant radiation therapy. The majority of patients underwent PD (69%) and received at least one cycle of adjuvant therapy (56%). R1 margin (<1 mm from the surgical margin) compared with R0 margin (rate of R0 margin: 80%) was not associated with recurrence-free survival (HR 0.85; p = 0.521) or overall survival (HR 0.82; p = 0.461). On multivariable analyses, the results were maintained irrespective of the type of NAT.31 Certain differences in the two recent studies are important to note. The latter study from Johns Hopkins used the standard AJCC definition of R1 margin and included the patient population who received at least 2 months of NAT. In contrast, the multicenter study between Japan and the US defined R0 by the 0 mm rule (tumor at margin), resulting in an increased R0 rate (>90% vs. 80%). Furthermore, the duration of NAT was not clearly delineated, potentially influencing the differences in outcomes between the two studies. While these two recent studies discuss the importance of margin status on survival in the setting of NAT, they do not evaluate the specific cohort of patients with an intraoperative positive margin that was rendered negative by extending the pancreatic resection.
The existing data differ on the question of converting an R1 neck margin on frozen section to R0 by taking additional parenchyma, even to the point of completion pancreatectomy. The increased use of NAT may influence the incidence of R1 margins and their impact on survival further. Based on the available data, the authors support either forgoing intraoperative neck margin assessment or continuing the use of intraoperative frozen section of the pancreatic neck with consideration of re-resection for an additional single margin and not rechecking further. This assumes the mass is truly located in the pancreatic head/uncinate process and not overtly located in the pancreatic neck, and that the disease process is understood to be true ductal adenocarcinoma of the pancreas and not IPMNs. We feel extending the margin to the point of total pancreatectomy for PDAC may not provide therapeutic benefit for the patient.32
Distal Pancreatectomy
The question of assessing for a positive margin on frozen section for tumors in the pancreatic body and tail during DP is more challenging. Based on National Comprehensive Cancer Network (NCCN) guidelines (version 1.2021), the margins analyzed in DP include the transection (neck) margin, and anterior and posterior peripancreatic margins, which can be assessed similarly to the radial margin in rectal cancer. Involvement of the splenic vessels along with invasion of the spleen should be documented; splenic artery and vein margins can be assessed pathologically. The transection margin and the posterior resection margin are technically modifiable to achieve R0 resection. Because left-sided PDAC can present at a more advanced stage, clearing both the transection and posterior margins can sometimes be difficult.33,34 Radical antegrade modular pancreatosplenectomy (RAMPS) is a technique first described by Strasberg et al. in 2003 with the goal of improving R0 posterior dissection margin rates and harvesting more lymph nodes (Fig. 2).35

The resection bed after excision of the specimen (distal pancreatectomy). PV portal vein, CHA common hepatic artery, SMA superior mesenteric artery
A meta-analysis of six studies (378 patients) comparing RAMPS with standard pancreatosplenectomy (SPS) for PDAC demonstrated higher R0 resection rates (odds ratio [OR] 2.19; p = 0.02) and increased harvested lymph nodes favoring RAMPS (weighted mean difference [WMD] 7.06; p < 0.01) without any significant difference in recurrence rates (OR 0.66; p = 0.10), disease-free survival (HR 1.02; p = 0.93), and overall survival (HR 0.65; p = 0.05).36 A more recent meta-analysis of five studies (285 patients) comparing RAMPS with SPS revealed higher R0 resection rates (RR 2.37; p = 0.01), an increase in lymph node yield (WMD 7.08; p < 0.000013), and improvement in overall survival at 1 year, favoring RAMPS (RR 1.2; p = 0.02).37 No difference in postoperative pancreatic fistula, complications, hospital stay, and mortality or recurrence rates was noted (p > 0.05).
Another recent meta-analysis of seven studies (474 patients) comparing RAMPS with SPS that included patients who underwent surgery first (no NAT) for PDAC was published in 2019.38 This study favored RAMPS over SPS in terms of overall survival (HR 0.65; p = 0.046), recurrence rates (RR 0.8; p = 0.028), blood loss (WMD 153.19; p = 0.046), and number of lymph nodes harvested (WMD 4.74; p = 0.034). No significant differences were noted with respect to R0 resection margin rates (p = 0.125), postoperative pancreatic fistula (p = 0.577), operative times (p = 0.942), or hospital length of stay (p = 0.087).38
The approach to DP for PDAC arguably favors the minimally invasive approach. A small retrospective study published in 2013 revealed non-inferiority of minimally invasive DP (MIDP) compared with open DP (ODP) for PDAC in terms of postoperative outcomes and overall survival (HR 1.11; p = 0.8).39 A recent meta-analysis of 11 studies (4829 patients) favored MIDP over ODP in terms of R0 margin rates (WMD 0.71; p = 0.003), intraoperative blood loss (WMD −250.03; p < 0.00001), postoperative hospital length of stay (WMD −2.76, p < 0.00001) and postoperative morbidity (OR 0.57; p < 0.00001) and mortality (OR 0.50; p = 0.005), while noting no difference in 3-year (HR 1.03; p = 0.66) and 5-year (HR 0.91; p = 0.59) overall survival outcomes.40 Another recent meta-analysis of 21 studies (11,246 patients) concluded that MIDP was comparable with ODP with respect to overall survival (HR 0.86; p = 0.06), R0 resection rate (OR 1.24; p = 0.09), and use of adjuvant therapy (OR 1.07; p = 0.46).41 However, the lymph node yield was lower with MIDP (WMD −1.3, p = 0.03). In this study, fewer patients in MIDP received neoadjuvant chemotherapy and neoadjuvant radiation therapy. In addition, patients undergoing MIDP were more likely to have smaller tumors (WMD −0.46 cm; p < 0.001), less perineural invasion (OR 0.48; p < 0.001), and less lymphovascular invasion (OR 0.53; p < 0.001).41 A pan-European propensity score-matched study comparing MIDP with ODP for PDAC included 1212 patients from 34 centers in 11 countries.42 This observational study revealed comparable overall survival between groups (28 vs. 31 months; p = 0.929), with higher R0 resection rates (67% vs. 58%; p = 0.019) but lower lymph node yield (14 [8–22] vs. 22 [14–31]; p < 0.001) and Gerota’s fascia resection rates (31% vs. 60%; p < 0.001) with MIDP. The median blood loss (200 mL [60–400] vs. 300 mL [150–500]; p = 0.001) and length of hospital stay (8 [6–12] vs. 9 [7–14]; p < 0.001) favored MIDP.42 This paved the way for an international RCT (DIPLOMA) comparing the approach to RAMPS—MIDP versus ODP, with microscopic radical resection rate (R0, >1 mm) as the primary outcome. Currently, this trial just completed enrollment of 258 patients from 34 centers.
In our opinion, all surgeons operate on PDAC knowing it is a systemic disease. Despite the majority of the recurrence being distant disease, we have one opportunity in a technically resectable patient to perform an optimal operation. We favor RAMPS over SPS for all patients with PDAC of the body and tail. The disadvantage of RAMPS is insignificant and limited mainly by the technical ability of the operating surgeon. We await the results of the DIPLOMA trial (non-inferiority trial), where we anticipate higher R0 resection rates with a minimally invasive approach, compared with an open approach, based on the published retrospective data.
Intraductal Papillary Mucinous Neoplasm
The diagnosis of IPMN is increasing due to the liberal use of high-resolution imaging.43 Indications for resection are well documented with supporting literature in the revisions of international consensus guidelines.43 Recommendations include frozen section analysis to determine the extent of resection.44,45 There appears to be less controversy over resection of additional pancreas when margin is positive for high-grade dysplasia (HGD) or invasive cancer, as well as avoiding additional resection for low-grade dysplasia (LGD) at the margin.46,47,48,49,50 There appears to be a tendency for overtreating patients with main-duct IPMN (MD-IPMN) or mixed-type IPMN in 19% of patients due to unnecessary or too-extensive resections.51
The CPC recently conducted a retrospective multicenter study analyzing the resection margin status of 330 patients with non-invasive IPMNs who underwent surgery.52 Positive margin was defined as any degree of dysplasia or pancreatic intra-epithelial neoplasia (PanIN). Positive surgical margin was encountered in 19.7% of patients, with only 1.8% being HGD or PanIN-3. Recurrences were documented in 8.9% of margin-negative resections, 16.9% with LGD or PanIN-1/2 at the margin, and 33.3% with HGD or PanIN-3 at the margin. The recurrence-free survival of these patients with respect to negative or positive margin did not reach statistical significance (p = 0.06), likely due to the low number of patients with positive margins and the fact that the majority of patients with positive margin had LGD at the margin. The presence of multifocal disease was significantly associated with an increase in the incidence of positive resection margin (OR 2.13; p = 0.02).52 The conclusions of that study were congruent with international consensus recommendations of resecting additional pancreas with HGD at the margin.43
Another multicenter retrospective study was conducted in Japan to determine recurrence patterns in 1074 patients with IPMNs.53 Recurrence of 14.4% was documented at 24 months. This study showed no association between positive pancreatic transection margin and frequency of metachronous high-risk lesions in the remnant pancreas. On multivariable analysis, only preoperative symptoms, location of IPMNs in the body/tail, main pancreatic duct ≥ 1 cm, and presence of HGD/invasive IPMNs (not transection margin) were associated with metachronous high-risk lesions in the remnant pancreas.53
Other studies also show no association of positive transection margin with IPMN recurrence rates.54,55 A study published in 2013 included 192 patients who underwent resection for non-invasive IPMNs, with ductal dysplasia identified in 86 patients (45%) at the final surgical margin (IPMN or PanIN).56 IPMN was noted at the final surgical margin in 38 specimens (20%)—LGD (9%), moderate-grade dysplasia (8%), and HGD (3%). PanIN was noted at the final surgical margin in 54 specimens (28%)—PanIN-1 (17%), PanIN-2 (9%), and PanIN3 (2%). Six patients had IPMN and PanIN at the final surgical margin. On multivariable analysis, margin dysplasia predicted a threefold increase in the risk of recurrence (p = 0.02) in the remnant gland, but not at the resection margin. In contrast, another study of 173 patients with MD-IPMN reported lower disease-free survival with positive transection margin (defined as HGD or invasive carcinoma) compared with negative margins (46 vs. 89 months; p < 0.001), and positive margin was associated with decreased overall survival (HR 2.6; p = 0.046).44
Based on the available data, given the more indolent behavior of IPMNs compared with PDAC, we support routine frozen section evaluation of the transection margin and resecting additional pancreas for HGD or invasive cancer at the margin when possible, as the presence of HGD or invasive cancer at the margin may increase recurrence rates and potentially have a negative impact on overall survival. Total pancreatectomy in an attempt to eliminate HGD at the margin should be applied very selectively for young and functional patients with an appropriate social situation, where handling the complications of exocrine insufficiency and brittle diabetes is feasible. Due to the multifocal nature of the IPMNs, we recommend long-term follow-up with imaging studies of patients with resected IPMNs.
Neuroendocrine Tumors
The incidence of PanNETs has been gradually increasing over the last decade, with nearly double the number of non-functional PanNETs being diagnosed annually.57 PanNETs account for approximately 7% of all NETs, with an incidence of 0.8 per 100,000 people.58,59 Surgical resection remains the mainstay of therapy for a potential cure. Two major categories include tumor enucleation and standard resection (central pancreatectomy, PD, DP). Existing data on margin analysis remain limited for both enucleation and standard resection.
In a retrospective multicenter study of 205 patients, 29% underwent enucleation, 31% underwent PD, 35% underwent DP, and 4% underwent central pancreatectomy.60 R1 resection margin was defined as microscopic margin involvement <1 mm, including resection margin, anterior and posterior margin, median margin (close to the portal vein and mesenteric artery), and unclear margins caused by coagulation artifact. R1 resection margins were more than twofold greater after enucleation of pancreatic head tumors compared with PD (37% vs. 17%; p = 0.052). R1 resection margins after enucleation of pancreatic body/tail tumors were analogous to DP (24% vs. 17%; p = 0.5). The recurrence rate was 19% after enucleation of non-functioning PanNETs, favoring standard resection. Postoperative morbidity after enucleation was comparable with PD or DP; however, endocrine and exocrine insufficiency was significantly higher after PD.60
The prognostic role of resection margin status on overall survival has been evaluated in only one large retrospective multicenter study.61 In this study, R1 resection margin was associated with a worse 10-year recurrence-free survival compared with R0 (47.3% vs. 62.8%; p = 0.002); however, overall survival was not impacted. The study also evaluated conversion of R1 to R0 margin based on intraoperative frozen section, and demonstrated re-resection of an initially positive surgical margin was not associated with improved overall survival.61
Based on the existing literature, the decision to assess resection margins remains at the discretion of the operating surgeon, while considering tumor location, tumor biology and the risks and benefits of margin re-resection.
Conclusion
Margin assessment for pancreatic neoplasms remains a work in progress, with the most mature data around the pancreatic neck margins at the time of PD for patients with ductal adenocarcinoma. Extent of resection may be dictated by consideration of factors such as functional status of the patient, tumor biology, and technical challenges, especially based on the involvement of peripancreatic vasculature. Future exploration of novel mutations and development of additional targeted therapy may further define the role of margin status in patients with PDAC.
References
Campbell F, Smith RA, Whelan P, et al. Classification of R1 resections for pancreatic cancer: the prognostic relevance of tumour involvement within 1 mm of a resection margin. Histopathology. 2009;55(3):277–83.
Hartwig W, Hackert T, Hinz U, et al. Pancreatic cancer surgery in the new millennium: better prediction of outcome. Ann Surg. 2011;254(2):311–9.
Jamieson NB, Foulis AK, Oien KA, et al. Positive mobilization margins alone do not influence survival following pancreatico-duodenectomy for pancreatic ductal adenocarcinoma. Ann Surg. 2010;251(6):1003–10.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Cancer stat facts: pancreatic cancer. https://seer.cancer.gov/statfacts/html/pancreas.html. Accessed 25 Apr 2019.
Neoptolemos JP, Palmer DH, Ghaneh P, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet. 2017;389(10073):1011–24.
Oettle H, Neuhaus P, Hochhaus A, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA. 2013;310(14):1473–81.
Cid-Arregui A, Juarez V. Perspectives in the treatment of pancreatic adenocarcinoma. World J Gastroenterol. 2015;21(31):9297–316.
DiMagno EP. Pancreatic cancer: clinical presentation, pitfalls and early clues. Ann Oncol. 1999;10(Suppl 4):140–2.
Kaur S, Baine MJ, Jain M, Sasson AR, Batra SK. Early diagnosis of pancreatic cancer: challenges and new developments. Biomark Med. 2012;6(5):597–612.
Adsay NV, Basturk O, Saka B, et al. Whipple made simple for surgical pathologists: orientation, dissection, and sampling of pancreaticoduodenectomy specimens for a more practical and accurate evaluation of pancreatic, distal common bile duct, and ampullary tumors. Am J Surg Pathol. 2014;38(4):480–93.
Verbeke CS, Leitch D, Menon KV, McMahon MJ, Guillou PJ, Anthoney A. Redefining the R1 resection in pancreatic cancer. Br J Surg. 2006;93(10):1232–7.
Hernandez J, Mullinax J, Clark W, et al. Survival after pancreaticoduodenectomy is not improved by extending resections to achieve negative margins. Ann Surg. 2009;250(1):76–80.
Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–9.
Chandrasegaram MD, Goldstein D, Simes J, et al. Meta-analysis of radical resection rates and margin assessment in pancreatic cancer. Br J Surg. 2015;102(12):1459–72.
Ghaneh P, Kleeff J, Halloran CM, et al. The impact of positive resection margins on survival and recurrence following resection and adjuvant chemotherapy for pancreatic ductal adenocarcinoma. Ann Surg. 2019;269(3):520–9.
Kooby DA, Lad NL, Squires MH 3rd, et al. Value of intraoperative neck margin analysis during Whipple for pancreatic adenocarcinoma: a multicenter analysis of 1399 patients. Ann Surg. 2014;260(3):494–501 (discussion 493–501).
Zhang B, Lee GC, Qadan M, et al. Revision of pancreatic neck margins based on intraoperative frozen section analysis is associated with improved survival in patients undergoing pancreatectomy for ductal adenocarcinoma. Ann Surg. 2021;274(2):e134–42.
Neoptolemos JP, Stocken DD, Dunn JA, et al. Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial. Ann Surg. 2001;234(6):758–68.
Dillhoff M, Yates R, Wall K, et al. Intraoperative assessment of pancreatic neck margin at the time of pancreaticoduodenectomy increases likelihood of margin-negative resection in patients with pancreatic cancer. J Gastrointest Surg. 2009;13(5):825–30.
Lad NL, Squires MH, Maithel SK, et al. Is it time to stop checking frozen section neck margins during pancreaticoduodenectomy? Ann Surg Oncol. 2013;20(11):3626–33.
Wasif N, Bentrem DJ, Farrell JJ, et al. Invasive intraductal papillary mucinous neoplasm versus sporadic pancreatic adenocarcinoma: a stage-matched comparison of outcomes. Cancer. 2010;116(14):3369–77.
Mathur A, Ross SB, Luberice K, et al. Margin status impacts survival after pancreaticoduodenectomy but negative margins should not be pursued. Am Surg. 2014;80(4):353–60.
Fatima J, Schnelldorfer T, Barton J, et al. Pancreatoduodenectomy for ductal adenocarcinoma: implications of positive margin on survival. Arch Surg. 2010;145(2):167–72.
Nitschke P, Volk A, Welsch T, et al. Impact of intraoperative re-resection to achieve R0 status on survival in patients with pancreatic cancer: a single-center experience with 483 patients. Ann Surg. 2017;265(6):1219–25.
Greco SH, August DA, Shah MM, et al. Neoadjuvant therapy is associated with lower margin positivity rates after Pancreaticoduodenectomy in T1 and T2 pancreatic head cancers: an analysis of the National Cancer Database. Surg Open Sci. 2021;3:22–8.
Conroy T, Hammel P, Hebbar M, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. 2018;379(25):2395–406.
Ahmad SA, Duong M, Sohal DPS, et al. Surgical outcome results from SWOG S1505: a randomized clinical trial of mFOLFIRINOX versus Gemcitabine/Nab-paclitaxel for perioperative treatment of resectable pancreatic ductal adenocarcinoma. Ann Surg. 2020;272(3):481–6.
Maeda S, Moore AM, Yohanathan L, et al. Impact of resection margin status on survival in pancreatic cancer patients after neoadjuvant treatment and pancreatoduodenectomy. Surgery. 2020;167(5):803–11.
Gamboa AC, Rupji M, Switchenko JM, et al. Optimal timing and treatment strategy for pancreatic cancer. J Surg Oncol. 2020;122(3):457–68.
Schmocker RK, Delitto D, Wright MJ, et al. Impact of margin status on survival in patients with pancreatic ductal adenocarcinoma receiving neoadjuvant chemotherapy. J Am Coll Surg. 2021;232(4):405–13.
Datta J, Willobee BA, Ryon EL, et al. Contemporary reappraisal of intraoperative neck margin assessment during pancreaticoduodenectomy for pancreatic ductal adenocarcinoma: a review. JAMA Surg. 2021;156(5):489–95.
Esposito I, Kleeff J, Bergmann F, et al. Most pancreatic cancer resections are R1 resections. Ann Surg Oncol. 2008;15(6):1651–60.
Gebauer F, Tachezy M, Vashist YK, et al. Resection margin clearance in pancreatic cancer after implementation of the Leeds Pathology Protocol (LEEPP): clinically relevant or just academic? World J Surg. 2015;39(2):493–9.
Strasberg SM, Drebin JA, Linehan D. Radical antegrade modular pancreatosplenectomy. Surgery. 2003;133(5):521–7.
Cao F, Li J, Li A, Li F. Radical antegrade modular pancreatosplenectomy versus standard procedure in the treatment of left-sided pancreatic cancer: a systemic review and meta-analysis. BMC Surg. 2017;17(1):67.
Zhou Q, Fengwei G, Gong J, et al. Assessement of postoperative long-term survival quality and complications associated with radical antegrade modular pancreatosplenectomy and distal pancreatectomy: a meta-analysis and systematic review. BMC Surg. 2019;19(1):12.
Huo Z, Zhai S, Wang Y, et al. Comparison of radical antegrade modular pancreatosplenectomy with standard retrograde pancreatosplenectomy for left-sided pancreatic cancer: a meta-analysis and experience of a single center. Med Sci Monit. 2019;25:4590–601.
Magge D, Gooding W, Choudry H, et al. Comparative effectiveness of minimally invasive and open distal pancreatectomy for ductal adenocarcinoma. JAMA Surg. 2013;148(6):525–31.
Yang DJ, Xiong JJ, Lu HM, et al. The oncological safety in minimally invasive versus open distal pancreatectomy for pancreatic ductal adenocarcinoma: a systematic review and meta-analysis. Sci Rep. 2019;9(1):1159.
van Hilst J, Korrel M, de Rooij T, et al. Oncologic outcomes of minimally invasive versus open distal pancreatectomy for pancreatic ductal adenocarcinoma: a systematic review and meta-analysis. Eur J Surg Oncol. 2019;45(5):719–27.
van Hilst J, de Rooij T, Klompmaker S, et al. Minimally invasive versus open Distal Pancreatectomy for Ductal Adenocarcinoma (DIPLOMA): a Pan-European Propensity Score matched study. Ann Surg. 2019;269(1):10–7.
Tanaka M, Fernandez-Del Castillo C, Kamisawa T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017;17(5):738–53.
Marchegiani G, Mino-Kenudson M, Sahora K, et al. IPMN involving the main pancreatic duct: biology, epidemiology, and long-term outcomes following resection. Ann Surg. 2015;261(5):976–83.
Couvelard A, Sauvanet A, Kianmanesh R, et al. Frozen sectioning of the pancreatic cut surface during resection of intraductal papillary mucinous neoplasms of the pancreas is useful and reliable: a prospective evaluation. Ann Surg. 2005;242(6):774–8 (discussion 778–780).
Chari ST, Yadav D, Smyrk TC, et al. Study of recurrence after surgical resection of intraductal papillary mucinous neoplasm of the pancreas. Gastroenterology. 2002;123(5):1500–7.
Farnell MB. Surgical management of intraductal papillary mucinous neoplasm (IPMN) of the pancreas. J Gastrointest Surg. 2008;12(3):414–6.
Fujii T, Kato K, Kodera Y, et al. Prognostic impact of pancreatic margin status in the intraductal papillary mucinous neoplasms of the pancreas. Surgery. 2010;148(2):285–90.
Jang JY, Kim SW, Ahn YJ, et al. Multicenter analysis of clinicopathologic features of intraductal papillary mucinous tumor of the pancreas: is it possible to predict the malignancy before surgery? Ann Surg Oncol. 2005;12(2):124–32.
White R, D’Angelica M, Katabi N, et al. Fate of the remnant pancreas after resection of noninvasive intraductal papillary mucinous neoplasm. J Am Coll Surg. 2007;204(5):987–93 (discussion 985–993).
Crippa S, Pergolini I, Rubini C, et al. Risk of misdiagnosis and overtreatment in patients with main pancreatic duct dilatation and suspected combined/main-duct intraductal papillary mucinous neoplasms. Surgery. 2016;159(4):1041–9.
Dhar VK, Merchant NB, Patel SH, et al. Does surgical margin impact recurrence in noninvasive intraductal papillary mucinous neoplasms? A multi-institutional study. Ann Surg. 2018;268(3):469–78.
Hirono S, Shimizu Y, Ohtsuka T, et al. Recurrence patterns after surgical resection of intraductal papillary mucinous neoplasm (IPMN) of the pancreas; a multicenter, retrospective study of 1074 IPMN patients by the Japan Pancreas Society. J Gastroenterol. 2020;55(1):86–99.
He J, Cameron JL, Ahuja N, et al. Is it necessary to follow patients after resection of a benign pancreatic intraductal papillary mucinous neoplasm? J Am Coll Surg. 2013;216(4):657–65 (discussion 657–665).
Kang MJ, Jang JY, Lee KB, Chang YR, Kwon W, Kim SW. Long-term prospective cohort study of patients undergoing pancreatectomy for intraductal papillary mucinous neoplasm of the pancreas: implications for postoperative surveillance. Ann Surg. 2014;260(2):356–63.
Frankel TL, LaFemina J, Bamboat ZM, et al. Dysplasia at the surgical margin is associated with recurrence after resection of non-invasive intraductal papillary mucinous neoplasms. HPB (Oxford). 2013;15(10):814–21.
Kasumova GG, Tabatabaie O, Eskander MF, Tadikonda A, Ng SC, Tseng JF. National rise of primary pancreatic carcinoid tumors: comparison to functional and nonfunctional pancreatic neuroendocrine tumors. J Am Coll Surg. 2017;224(6):1057–64.
Partelli S, Giannone F, Schiavo Lena M, et al. Is the real prevalence of pancreatic neuroendocrine tumors underestimated? A retrospective study on a large series of pancreatic specimens. Neuroendocrinology. 2019;109(2):165–70.
Lawrence B, Gustafsson BI, Chan A, Svejda B, Kidd M, Modlin IM. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin N Am. 2011;40(1):1–18.
Jilesen AP, van Eijck CH, Busch OR, van Gulik TM, Gouma DJ, van Dijkum EJ. Postoperative outcomes of enucleation and standard resections in patients with a pancreatic neuroendocrine tumor. World J Surg. 2016;40(3):715–28.
Zhang XF, Wu Z, Cloyd J, et al. Margin status and long-term prognosis of primary pancreatic neuroendocrine tumor after curative resection: results from the US Neuroendocrine Tumor Study Group. Surgery. 2019;165(3):548–56.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Mihir M. Shah, Jashodeep Datta, Nipun B. Merchant, and David A. Kooby have no relevant financial or commercial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shah, M.M., Datta, J., Merchant, N.B. et al. Landmark Series: Importance of Pancreatic Resection Margins. Ann Surg Oncol 29, 1542–1550 (2022). https://doi.org/10.1245/s10434-021-11168-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-11168-7