
Abstract
Background
Liposarcomas are malignant tumours of adipocytic differentiation and their occurrence within the head and neck region is very uncommon. Lipomas are the most common types of benign mesenchymal tumours. The clinical, histological and imaging features of well-differentiated liposarcoma may resemble that of lipoma, causing challenges in the diagnosis. The management and prognosis of benign lipomas and well-differentiated liposarcoma are different.
Case presentation
A 73-year-old man presented with a painless soft mass in the left temporal region for 15 years with recent rapid growth. The scalp mass was clinically diagnosed as lipoma, while MRI suspected an atypical lipomatous lesion. Complete surgical resection was performed, and histopathological examination confirmed a well-differentiated liposarcoma.
The patient recovered completely and will be followed up with long-term surveillance.
Conclusion
This report is to highlight that clinicians must have a high index of suspicion for this rare entity when dealing with scalp masses and suspicious radiological findings, which can affect the overall management and prognosis.
Similar content being viewed by others


Background
Liposarcoma of the head and neck constitutes approximately 1% of all soft tissue sarcomas [1]. Liposarcoma is classified into four different histological subtypes: well-differentiated (also known as the atypical lipomatous tumour), dedifferentiated, myxoid and pleomorphic liposarcoma [2].Well-differentiated liposarcoma (WDLS) is the most common subtype which is associated with indolent behaviour mimicking lipoma [2]. Both simple lipomas and WDLS are well-circumscribed fatty masses [3]. Well-differentiated liposarcoma commonly present as a slow-growing mass in the retroperitoneum and proximal extremities and seldom appear in the scalp area [2]. Well-differentiated liposarcoma has increased levels of regional recurrence and well-documented predisposition to delayed dedifferentiation into higher grade sarcomas with metastatic potential [3]. Due to these characteristics, well-differentiated liposarcoma need wide local excision as initial treatment and long-term follow-up. Herein this report, we describe a rare case of well-differentiated liposarcoma of the scalp clinically mimicking lipoma.
Case presentation
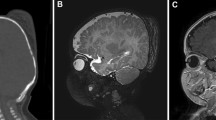
A 73-year-old man presented with a painless soft mass in the left temporal region, followed by his general practitioner during the last 15 years. The patient noticed an increase in its size for the past 6 months and consulted a head and neck surgeon. The physical examination revealed a non-tender, soft and mobile mass, apparently in the subcutaneous tissue of the left temporal region, compatible with a lipoma. There were no palpable cervical lymph nodes. An ultrasound concluded to a diagnosis of lipoma. Due to rapid growth of the lesion and to delineate its relation to the frontal branch of the facial nerve, a magnetic resonance imaging (MRI) was performed. A discrete heterogeneous fatty lesion of 8 × 11 cm with well-defined contours, located under the superficial part of the left temporal muscle, extending from the zygomatic arch anteriorly to the retro-auricular region was seen, in contrary to the clinical impression that the lesion was located subcutaneously (Fig. 1). This lesion was showing a distinct area of enhancement in the central part with a signal which was not completely suppressed on the fat saturation sequences (Fig. 2). The diagnosis of atypical lipomatous lesion was rendered and a wide surgical resection was performed under general anaesthesia with facial nerve monitoring. Macroscopically, it was a bilobed mass with homogenous yellowish tissue without necrosis or haemorrhage (Fig. 3). The microscopic examination demonstrated patches of adipose tissue intersected by fibrous septae, atypical stromal cells and enlarged nucleus (Fig. 4). There were striated musculature fibres within and around the lesion. In situ hybridization study shows MDM2 amplification of cell signals (Fig. 5). Histopathological examination confirmed a well-differentiated liposarcoma. This patient had an uneventful postoperative period. The patient will be followed up with long-term surveillance.

Coronal T2-weighted MRI image shows prominent low signal foci in the mass lesion

Coronal T1 image with fat saturation after gadolinium injection showing enhancement of the septa within the lesion

Gross appearance of liposarcoma showing well-circumscribed mass with homogenous yellowish tissue (lipoma-like texture)

Photomicrograph showing mature adipocytes intersected by fibrous septa with atypical stromal cells (haematoxylin and eosin, ×200)

MDM2 amplification by in situ hybridization (CISH, 400×)
Discussion
Well-differentiated liposarcomas are reported to be predominant among middle-aged males and often present as painless, slow-growing masses [3]. The lipoma is usually present as non-tender, mobile and well-defined mass and seldom present diagnostic problems for the pathologist. However, deep-seated or lipomas with atypical characteristics can mimic as liposarcoma [4]. Well-differentiated liposarcoma needs to be differentiated from benign lipoma due to its indolent course and histopathological examination is necessary for definitive diagnosis [2].
Imaging studies are notably helpful to evaluate the size, extent and location of the tumour and its relationship with the adjacent neurovascular structures in the areas of the head [4]. Ultrasonographic findings may not always be accurate in lipomatous lesions like in our patient. Computerised tomography (CT) and magnetic resonance imaging (MRI) can contribute relevant features to differentiate a lipoma from liposarcoma prior to surgical intervention [5]. The MRI shows the delineation of soft tissue and clearly defines the borders of the lesion from the subcutaneous tissue compared to CT. Infiltrative margins are more obvious on MRI with fat suppression techniques [6]. Amid the numerous lipomatous lesions, the radiological differentiation between lipoma and well-differentiated liposarcoma is challenging [4]. A distinct, well-encapsulated, homogeneous fatty mass with few or no septa and minimal or no enhancement or high T2 signal is assuredly a lipoma [3]. Simple lipoma also consists of fibrous septa, muscle fibres, areas of blood vessels and inflammation. These non-adipose components may mimic features of well-differentiated liposarcoma. The radiological findings which are suspicious of liposarcoma are non-adipose masses, thickened or nodular septa (>2 mm thick), prominent foci of low T2 signal and prominent areas of enhancement [3].
A study by Klijanienko et al. on fine-needle aspiration in liposarcoma demonstrated the difficulty to distinguish between lipomas and well-differentiated liposarcomas due to morphological overlap in cytological smears [7].
Macroscopically, liposarcomas are grossly well-circumscribed and not encapsulated neoplasms while lipomas are well-encapsulated masses. They may have a mucoid slimy surface with a bright yellow appearance mimicking a lipoma similar to our case [6]. The presence of atypical cells or vacuolated lipoblasts intermingled with fibroblasts-like spindle cells in the septa is the characteristic histological feature discerning well-differentiated liposarcomas from intramuscular lipomas [6].
The treatment modalities for lipomas can be divided into non-excisional and excisional techniques [5]. Most lipomas can be observed without treatment if the lipoma is small and asymptomatic. Excision is required in lesions of diagnostic dilemma, exponential growth, size of more than 10 cm, deep anatomical locations, associated pain or cosmetic issues [4].
Well-differentiated liposarcoma requires wide local excision with clear margins. Recurrence rates increase with incomplete excision, as they are often misdiagnosed as benign lipomas [4]. The extent of excision in head and neck lesions has been limited by the proximity of vital neurovascular structures which may impede the surgeons from wider resection with negative margins. Non-surgical treatment modalities like radiation therapy or chemotherapy are of limited use and remain controversial in liposarcomas. Well-differentiated liposarcomas are considered low-grade malignancies with little or no tendency to metastasis and good prognosis.
Conclusions
Our case report demonstrates that well-differentiated liposarcoma can mimic lipoma in its clinical presentation. Clinicians should be concerned about malignancy in patients with rapidly growing neck masses presenting clinically as lipomas. A rigorous clinical, radiological (preferably CT or MRI) and histopathological examination should be performed to avoid incomplete resection and thus prevent the recurrence of the tumour.
Availability of data and materials
Not applicable
Abbreviations
- CT:
-
Computerised tomography
- MRI:
-
Magnetic resonance imaging
- MDM2:
-
Murine double minute 2
- WDLS:
-
Well-differentiated liposarcoma
References
Golledge J, Fisher C, Rhys-Evans PH. Head and neck liposarcoma. Cancer. 1995;76(6):1051–8.
Piperi E, Tosios KI, Nikitakis NG, Kyriakopoulos VF, Tzerbos F, Koutlas IG et al (2012) Well-differentiated liposarcoma/atypical lipomatous tumor of the oral cavity: report of three cases and review of the literature. Head Neck Pathol. 6(3):354–363
Gaskin CM, Helms CA (2004) Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol. 182(3):733–739
Kim KS, Yang HS (2014) Unusual locations of lipoma: differential diagnosis of head and neck mass. Aust Fam Phys 43(12):867
Medina CR, Schneider S, Mitra A, Spears J, Mitra A (2007) Giant submental lipoma: case report and review of the literature. Can J Plast Surg. 15(4):219–222
McTighe S, Chernev I. Intramuscular lipoma: a review of the literature. Orthop Rev (Pavia). 2014;6(4):5618.
Klijanienko J, Caillaud J, Lagacé R (2004) Fine-needle aspiration in liposarcoma: cytohistologic correlative study including well-differentiated, myxoid, and pleomorphic variants. Diagn Cytopathol. 30(5):307–312
Acknowledgements
None
Funding
No funding
Author information
Authors and Affiliations
Contributions
Concept - STS; design - STS, FM; supervision - FM; data collection and/or processing - STS, FM, AS, KM; literature search and writing manuscript - STS; analysis and/or interpretation - FM, AS, KM; critical review - FM, AS, KM. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Verbal and written informed consent for publication was obtained from the parent of the patient. A copy of consent is available for the journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Subha, S.T., Sanjurjo, A., Poyet, K.M. et al. Liposarcoma of the scalp mimicking a lipoma: a case report. Egypt J Otolaryngol 38, 146 (2022). https://doi.org/10.1186/s43163-022-00334-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00334-7