
Abstract
Background
This study set out to look at how naringenin affected the pharmacokinetics of ranolazine in rats. The pharmacokinetic investigation of ranolazine in rats following oral administration of ranolazine with or without coadministration of naringenin was successfully conducted using the established technique. Animals were administered the same medications for 7 days as part of a multiple dosage study (MDS), and the amount of ranolazine in plasma was calculated on 18 days. The intestinal transit of ranolazine in the presence and absence of naringenin and verapamil was examined in an in vitro experiment using the intestinal sacs of rats and chickens (P-glycoprotein inhibitor).
Results
Naringenin raised the maximal level (Cmax) of ranolazine from 231 ± 10.16 to 303.67 ± 9.46 and 325.67 ± 21.81 ng/mL in SDS and MDS, respectively. Moreover, naringenin elevated the area under the curve (AUC) of ranolazine from 1293.54 ± 37.18 to 1505.38 ± 100.30 and 1575.42 ± 76.98 ng/mL/h in SDS and MDS. In the presence of naringenin, there was an increase in the transfer of ranolazine from the mucosal side to the serosal side. Naringenin inhibits the enzymes Cytochrome P450 (3A4) or (CYP3A4) and P-glycoprotein (P-gp). The findings showed that naringenin might have a considerable impact on ranolazine pharmacokinetics, including extending its t1/2 and raising its AUC.
Conclusions
The findings of the study showed that naringenin inhibits the enzymes CYP3A4 and P-gp. Therefore, naringenin might have a considerable impact on ranolazine pharmacokinetics, including extending its t1/2 and raising its AUC.
Graphical abstract

Similar content being viewed by others

Background
Ischemic heart diseases are the leading cause of mortality worldwide [1,2,3]. Myocardial infarction, a kind of coronary artery disease, and stable angina pectoris are the two most aggressive forms of this condition's progression [4, 5]. The greatest way to reduce the size of myocardial infarcts and restore health is by leading percutaneous coronary or rapid myocardial reperfusion with thrombolytic therapy [6]. Different features of stable angina can be prevented generally with the help of statins and aspirin along with first-line therapy groups, such as nitrates, β-blockers, and calcium channel blockers, according to research [7].
Despite the fact that its precise function is yet unknown, the medicine ranolazine, which is a particular inhibitor of belated sodium ion entry, is likely to minimize the abnormalities of ventricular action potentials and contractility connected to ischemia [8]. The treatment of chronic stable angina pectoris with the distinctive novel medication called ranolazine has been approved, although it is not entirely apparent how it works [9]. Furthermore, ranolazine illustrates potential benefits for hyperglycemia, cardiac arrest, and arrhythmias [10].
A fundamental change in the practice of medicine has been brought about by recent improvements in the bioavailability optimization of pharmaceuticals by substances of botanical origins. Because a considerable amount of a dosage never reaches the plasma or does not exert its pharmacological action until extremely large doses are administered, which may induce serious adverse effects, poorly bioavailable medications continue to be below the therapeutic level. Any appreciable increase in bioavailability will lead to a reduction in the dose or the frequency of that specific drug's doses. The current global focus is on techniques designed to lower medication doses and, consequently, drug treatment costs [11]. Herbal bioenhancers are said to increase the bioavailability and bioefficacy of therapeutic medications or nutrients when coupled with them without having any usual pharmacological effect of their own at the dosage employed. The history of the idea of bioenhancers with botanical origins may be traced back to the ancient knowledge of the Indian medical system (Ayurveda). When long pepper was added to an Ayurvedic formula including vasaka (Adhatodavasica), Bose (1929) observed that the mixture's antiasthmatic effects were significantly boosted [12]. Bioenhancers work in a variety of ways. They have an impact on the drug target, drug metabolism, or the absorption process. The non-toxicity, effectiveness at low concentration levels, and ease of formulation procedures of bioenhancers are a few of the acknowledged justifications for their usage. When combined with other pharmacological classes including antibiotics, antituberculosis, antiviral, antifungal, and anticancer medicines, bioenhancers are successful. Bioenhancers also enhance the oral absorption of several nutrients, including vitamins, minerals, amino acids, and others [13]. Citrus trees, in particular, contain significant levels of flavonoids, and citrus fruits and juices are widely consumed across the world. Several of the most prominent biologically active flavonoid is naringenin, which is primarily present in several edible fruit species including those of the citrus genus and tomatoes [14]. Naringenin (7-[[2-O-(6-deoxy-α-L-mannopyranosyl)-β-D-glucopyranosyl]oxy]-2,3-dihydro-5-hydr-oxy-2-(4hydroxyphenyl)-4H-1-benzopyran-4-one), a flavanone glycoside (rutinoside), occurs naturally in the pericarp of citrus fruits and grapefruits (Citrus paradisi; Family: Rutaceae) [15]. Emerging research either from in vivo experiments findings has supported a number of naringenin's therapeutic potential use in conditions related to the neurological, liver, cardiovascular, digestive system, metabolic process, autoimmune dysfunction, pathogenic conditions, and neo-plastic condition [14]. Naringenin has the capacity to inhibit cytochrome P450, namely CYP3A4, as well as the P-gp export pump [16,17,18]. Drug and food interactions are becoming more widely acknowledged as great clinical occurrences, and other drugs can lead to unexpected, synergistic, additive, and antagonistic outcomes Medications may interfere with several bioactive molecules via altering drug-metabolizing enzymes that may inhibit or induce metabolism [19, 20]. Numerous medication interactions involving naringenin have been documented, including a reduction in pre-systemic metabolism by inhibition of the CYP3A4 enzyme, P-glycoprotein (P-gp), and multidrug resistance protein-2 (MRP2) [21, 22]. Ranolazine is quickly and severely processed in the liver and gastrointestinal tract by the CYP3A4 enzyme, and to a lesser extent by CYP2D6, with around 5% being removed renally unmodified [23].
Ranolazine has a bioavailability of around 30–55% [23]. The goal of the study was to raise the blood levels of ranolazine using the biological bio-enhancer naringenin. The cardiovascular system also appears to be protected by naringenin, and if ranolazine's bioavailability increases, the medication's dose and cost may be reduced. In light of these results, the current study's objective was to find out whether the flavonoid naringenin would alter the pharmacokinetics of ranolazine. For the detection of ranolazine in rat plasma, a simple and precise quantification method based on high-efficiency liquid chromatography was developed and assessed.
Methods
Working standards for naringenin and ranolazine were purchased from Sigma-Aldrich. HPLC-grade acetonitrile, methanol, water, and dimethyl sulfate were bought from Merck. All other materials and chemicals were of analytical reagent grade.
Animals used in the investigation
The animal ethics committee (IAEC/TRS/PT/22/26) authorized all animal research and ensured that they were carried out in accordance with the institution's policies for the care and use of laboratory animals. Six male Wistar rats (180–220 g) were confined in cages with unrestricted access to fresh water and food in typical controlled environments for a minimum of 7 days. The animals received a 12-h fast well before the program began, and they were denied access to food and drink while it was being conducted. The broiler chicks were bought from nearby farms and kept in carefully regulated circumstances.
Analysis techniques
A modified version of the approach recently reported by Nalawade et al. (2010) was used to quantify the plasma levels of ranolazine. A pump (LC-20AD), C18 column (Zorbax, Agilent) 75*4.6 mm, 5 m particle size, and a dual-wavelength ultraviolet (UV)-visible detector made up of a Shimadzu HPLC system (Shimadzu, Tokyo, Japan) (SPD-10A). Data collection and processing were carried out using LC solution software (Tokyo, Japan). The mobile phase was composed of acetonitrile and water (80:20 v/v) and 0.2 percent acetic acid.
Plasma extraction of ranolazine
The plasma was removed by centrifugation at 4000 rpm after the blood was drawn into plastic tubes containing K2 EDTA as an anticoagulant. Around 0.4 mL of plasma was combined with 2 mL of ethyl acetate for 5 min before the mixture was centrifuged at 4000 rpm for 5 min at room temperature. The organic layer was then removed, and using a nitrogen stream, it was evaporated to dryness at 50 °C. In order to perform chromatographic analysis, the residue was concentrated with 0.150 mL of the mobile phase.
Ranolazine's pharmacokinetics in SDS and the impact of naringenin
Group I received ranolazine 14 mg/kg therapy, Group II received naringenin 25 mg/kg treatment, and Group III received ranolazine 14 mg/kg treatment followed by naringenin 25 mg/kg treatment after 30 min. Oral gavages were used to provide each medication to the appropriate group. Following treatment, blood samples were taken from the retro-orbital plexus at 0.0, 0.5, 1, 2, 3, 4, 4.5, 5, 6, 8, 12, and 18 h. The concentration of ranolazine in the plasma was then calculated using the RP-HPLC technique.
Ranolazine's pharmacokinetics in MDS and the impact of naringenin
Rats with MDS were given the same medications for 7 days. On the 8th day, the blood sample was collected from the retro-orbital plexus at 0.0, 0.5, 1, 2, 3, 4, 4.5, 5, 6, 8, 12, and 18 h. The ranolazine concentration in plasma was estimated by the RP-HPLC method.
Naringenin's impact on ranolazine intestinal absorption in rat-everted sac
The gastrointestinal P-gp transit of compounds from the mucosal to the serosal surface was investigated using the everted sac technique [24]. Pentobarbital was given to male Wistar rats (weight 180–220 g) at a dose of 30 mg/kg (s.c.). An abdominal incision was made midline. The rats were killed by puncturing their hearts. A glass rod was used to quickly remove and evert the small intestine, which had a length of 10–12 cm from the Treitz ligament to the ileocaecal junction. The 2 mL of a pH 7.4 Krebs–Henseleit bicarbonate buffer solution containing 0.4 percent glucose was added to the sacs. For sample collection, one end was ligated and the other end was ligated with a needle. The sac was incubated at 37 °C in a glass container with 25 mL of the same buffer solution and was gassed at a ratio of 95/5. Ranolazine (50 µM) solution was added to the glass jar after 5 min, and the preparation was then incubated once more. At 10, 20, 30, 40, 50, and 60 min, 0.5 mL of sample was taken from the sac and 0.5 mL of buffer was added. The process was repeated with more sacs. Verapamil (10, 50, 100, and 200 µM) and Naringenin (25, 50, 100, and 200 µM) were present. The RP-HPLC technique was used to measure the ranolazine transfer from the mucosal to the serosal side at 225 nm.
Naringenin's impact on the intestinal absorption of ranolazine from the chicken everted sac
Activity evaluation was done by the new P-gp model in the intestinal sac everted by a chick. For the study, we employed this model. To prepare and mount tissue, I strictly adhered to the process outlined in Tanaka K.et al. [25]. Animals were killed, and their intestines were harvested from the duodenal loop's proximal end to its distal end immediately (2 min); the caecal attachment was withdrawn, and ice-cold ringer solution was used for flushing. The intestine was everted, the sleeves were shortened to 1.5 cm, and by securing the tissue to stainless steel rods precisely one centimeter apart over grooves.
Calibration curve standards and quality control (QC) sample preparation
Methanol was used to dissolve precisely weighted ranolazine, creating a standard primary solution with a 1 mg/mL concentration. By sequential diluting the primary solution with methanol: water (50:50), the secondary working solution with concentrations of 50, 100, 200, 1000, 5000, 10,000, 20,000, 30,000, 40,000, and 50,000 ng/mL was produced. 100 µL of blank rat plasma and 5 µL of each working solution were combined to create the calibrator standards, which had nominal values of 2.5, 5, 10, 50, 250, 500, 1000, 1500, 2000, and 2500 ng/mL. The same method was used to create the quality control (QC) samples from a separated stock solution at concentrations of 15, 80, 900, and 2100 ng/mL.
Statistic evaluation
The data were presented as mean SEM. Standard statistical procedures were used to determine the significance at p < 0.05 level using GraphPad Prism 8.0 (GraphPad Prism Software Inc., San Diego, USA).
Results
The body weight of different groups is represented in Fig. 1. Also, Fig. 1 illustrates that there were no significant (p > 0.05) changes in body weight among the different groups as determined by statistical analysis.

In the presence and absence of naringenin and verapamil, the transfer of ranolazine from the serosal to mucosal side of the chick-everted ileum (n = 6). R stands for ranolazine, N for naringenin, and MDS is for multidose study
Group-I received ranolazine 14 mg/kg therapy; Group-II received naringenin 25 mg/kg treatment; and Group-III received ranolazine 14 mg/kg treatment followed by naringenin 25 mg/kg treatment after 30 min.
Ranolazine pharmacokinetics in rats and the impact of naringenin
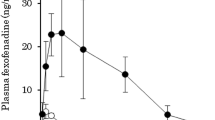
The pharmacokinetics (PK) parameters of ranolazine were computed in SDS and MDS (AUC, area under the curve; AUMC, area under the moment curve; t1/2, half-life; Cmax, maximum concentration; Tmax, the time required to reach maximum concentration; MRT, mean retention time). The PK characteristics of ranolazine were significantly changed by naringenin. In SDS and MDS, correspondingly, naringenin raised the peak rat plasma concentration of ranolazine from 231 ± 10.16 to 303.67 ± 9.46 and 325.67 ± 21.81 ng/mL. The naringenin-induced increase in ranolazine's AUC was also seen in SDS and MDS, where it went from 1293.54 ± 37.18 to 1505.38 ± 100.30 and 1575.42 ± 76.98 ng/mL/h, respectively. The outcomes are displayed in Table 1.
Naringenin impact upon ranolazine absorption from rat everted sacs during intestinal transit
The impact of naringenin on the intestinal transit of ranolazine was investigated using rat-everted intestinal sacs. Naringenin and verapamil, a common P-gp inhibitor, substantially (p < 0.01) enhanced the transfer of ranolazine from the mucosal side to the serosal side. Ranolazine's transport was boosted by naringenin (100 µM) from 20.95 ± 2.01 to 30.83 ± 20 at 60 min. But with Naringenin 100 and 200 µM, no appreciable transfer was seen. Ranolazine's transport was boosted by verapamil (100 µM) from 20.31 ± 1.56 to 36.47 ± 1.38 at 60 min. Tables 2 and 3 include the results.
Naringenin's impact on the intestinal absorption of ranolazine from chick-everted sacs
The impact of naringenin on the intestinal transit of ranolazine was also investigated using the gastrointestinal sacs of chicks. In the presence of 10, 50, 100, 200, and 300 µM naringenin, correspondingly, the transfer of ranolazine from the mucosal to serosal end accelerated from 2.68 ± 0.8 to 8.43 ± 1.69, 9.52 ± 1.56, 11.78 ± 1.59, and 12.98 ± 2.09 after 10 min of exposure. Following 10 min of exposure, the transfer of ranolazine from its mucosal to the serosal end improved from 2.97 ± 1.05 to 10.08 ± 1.8, 10.7 ± 1.88, 13.52 ± 2.87 and 17.65 ± 2.26 µg/ mL, correspondingly, inside the condition of 10, 50, 100, 200, and 300 µM verapamil (a prominent P-gp inhibitor). Figure 2 reports the outcomes.

Ranolazine plasma concentration levels in SDS and MDS with and without naringenin (n = 6). SDS single-dose study, MDS multi-dose study
Discussion
Kinetics and metabolic alterations are important because they can affect in vivo pharmacological action. The CYP450 enzyme system is crucial in the bio-transformation of a vast array of drugs with a wide range of chemical compositions. Due to restrictions or activation, several drugs interact dynamically with cellular enzymes [21]. P-glycoprotein (P-gp), an ATP-binding nucleotide shuttle that has been extensively studied, acts as a physiological barrier by expelling various compounds, including hazardous substances, from tissues. P-gp is critical for the absorption and elimination of medicines both in vivo and in vitro, according to several studies. Similar to CYP450 enzymes, P-gp restriction, and activation was also shown to be important factors in drug-drug interactions. Since many prototypical blockers and stimulators affect both CYP3A4 and P-gp, there are many pharmacological interactions. Medically, it can be quite difficult to tell the difference between P-gp and CYP3A4-driven drug effects. Ranolazine is effective for treating ischemia when taken by alone [26].
The most prevalent CYPs in the liver and intestine—specifically, CYPs 3A4 and 3A5—are responsible for metabolizing 45% of all therapeutic medicines. They are also a significant predictor of first-pass (hepatic and notably intestinal) metabolism and oral bioavailability of many medications. P-gp, an ATP-binding membrane transporter, serves as a biological barrier by driving toxicants and hazardous chemicals out of cells. P-gp is important for the uptake and elimination of drugs. P-gp inhibition and induction have both been identified as contributing factors to drug-drug interactions, just like CYP enzymes. Many medication interactions generated by these inhibitors and inducers include these two systems since many prototypical inhibitors and inducers impact both CYP3A4 and P-gp [27]. Due to (a) their co-existence in small intestine enterocytes, (b) the substantial overlap in their substrate specificities, and (c) the low oral bioavailability of medicines that are substrates for both CYP3A and P-gp, CYP3A and P-gp play a key role in restricting oral drug delivery [28]. Many of the same substances also activate or inhibit these enzyme and drug transporter proteins. P-gp facilitates recurrent drug cycling by diffusion and active efflux, increasing the exposure of pharmaceuticals to CYP3A4 in the gut [29]. Naringenin can inhibit cytochrome P450, namely CYP3A4, as well as the P-gp efflux pump [13, 30,31,32].
Ranolazine is mostly excreted in 5% unchanged via glomerular filtration after being processed to different degrees by cytochrome P450 (CYP3A4) and CYP2D6 processors. The piperidine ring is N-dealkylated, the methoxyphenyl moiety is o-de-arylated, the amide group is hydrolyzed, the mother molecule is oxygenated four times, and then it is conjugated with glucuronic acid to generate the primary metabolite. The systemic content of ranolazine was significantly raised in the proposed quantitative analysis by the addition of naringenin, going from 231 ± 10.16 to 303.67 ± 9.46 and 325.67 ± 21.81 in SDS and MDS, respectively. Additionally, naringenin raised the AUC in SDS and MDS from 1293.54 ± 37.18 to 1505.38 ± 100.30 and 1575.42 ± 76.98 ng/mL/h, correspondingly. The outcomes have all been displayed in Figs. 3 and 4. Hence from the obtained results it has been concluded that naringenin alters the pharmacokinetics of ranolazine in part through the inhibition of CYP3A4. The liver is typically thought to be the principal site of drug biotransformation due to its size and abundance of drug-metabolizing enzymes. In relation to the liver, the intestinal tract, and kidney may also significantly contribute to general biotransformation, which suppresses P-gp synthesis. P-gp and CYP3A4 both like a variety of targets. As a result, CYP3A4 and P-gp have a startling similarity in targets. Numerous medication conflicts may include both the enzymatic and exporter pathways since CYP3A4 and P-gp have similar targets, and several medications can impact both CYP3A4 and P-gp. Ranolazine is metabolized by the CYP3A pathway, and its levels are raised by ketoconazole, a CYP3A inhibitor that is given concurrently with ranolazine. Ranolazine quantities are unaffected by simvastatin, while ranolazine slightly enhances the initial levels and area under the curve of simvastatin. Digoxin abundances are around 1.5 times higher when ranolazine quantities are at their highest. Ranolazine's circulating systemic levels can rise 2.3 times as a result of verapamil, a mild CYP3A4 blocker, which can boost ranolazine's uptake. People with a history of QTc elongation, hepatic or renal dysfunction, all those who are receiving medications that extend the QTc, or those who are on strong CYP3 blockers should not use ranolazine. The findings of the current investigation indicated that naringenin strongly suppresses CYP3A4. Thus, it raises ranolazine's content and AUC.

Area under the curve of ranolazine alone and when naringenin was present in SDS and MDS (n = 6). SDS, single-dose study; MDS, multi-dose study

The movement of ranolazine from the serosal to the mucosal side of the rat-everted ileum (n = 6) in the presence and absence of naringenin. R, ranolazine; N, naringenin
To predict drug permeability and evaluate the effect of influx and efflux transporters, such as P-glycoprotein (P-gp), on drug absorption, several in-situ, in-vivo, ex-vivo, and in-vitro models have been created over time [33, 34]. The everted gut sac model has advantages since it is an easy, quick, and affordable procedure. Additionally, it has been demonstrated in earlier investigations that this method may be employed as a useful tool to evaluate P-function gp's in the intestinal absorption of many different therapeutic molecules [24, 35, 36]. In published data, the reliability of this in-vitro model by histological examinations was investigated [37,38,39]. In this study, naringenin and verapamil improved the transfer of ranolazine through the mucosal to the serosal portion of the rat and chick intestinal tract. Ranolazine's transit was boosted by naringenin (100 µM) from 20.95 ± 2.01 to 30.83 ± 20 at 60 min. However, no appreciable transit was seen with naringenin at 100 or 200 µM concentrations. Ranolazine's transit was boosted by verapamil (100 µM) from 20.31 ± 1.56 to 36.47 ± 1.38 at 60 min. The outcomes are displayed in Figs. 5 and 6. Following medication absorption, in vitro tests provided the first demonstration of the role of gastrointestinal P-gp in blood supply into the gut lumen (rat- and chick-everted intestinal sacs). The findings of the current investigation clearly showed that P-gp is important for ranolazine absorption. This may be due to naringenin compounds' inhibitory effects on the P-gp efflux transporter as well as naringenin's inhibitory effects on the intestinal cytochrome P450 (CYP) 3A4 isoenzyme activity [40,41,42,43].

The movement of ranolazine in the rat-everted ileum from the serosal to mucosal side in the presence and absence of verapamil (n = 6). R, ranolazine; V, verapamil

The movement of ranolazine in the rat-everted ileum from the serosal to mucosal side in the presence and absence of verapamil (n = 6). R, ranolazine; V, verapamil
A substance referred to as a bio-enhancer has the power to raise the drug's bioavailability or bio-efficacy when used in combination with a certain drug. There are many different pharmacological properties of the flavanone glycoside naringenin, which is present in citrus fruits. Previously, it was reported that naringenin's therapeutic potential was used in conditions related to the neurological, liver, cardiovascular, digestive system, metabolic process, autoimmune dysfunction, pathogenic conditions, and neo-plastic conditions [14]. The cytochrome P450 enzyme CYP3A4 and the P-gp efflux pump are both capable of being inhibited by naringenin. By blocking CYP-mediated metabolism and/or P-gp-mediated permeability. Naringenin is well-known for increasing the bioavailability of several structurally and therapeutically varied medications (verapamil, diltiazem, paclitaxel, tamoxifen) in rats by inhibiting CYP-mediated metabolism and/or P-gp-mediated permeability [13, 43,44,45]. Ranolazine, a specific inhibitor of belated sodium ion entry is likely to have a cardioprotective activity and illustrates potential benefits for ischemia, cardiac arrest, arrhythmias, and hyperglycemia [8,9,10]. Ranolazine oral bioavailability was restricted by P-gp and it is metabolized in the liver by cytochrome P450 CYP3A4. In the present study, naringenin alters the pharmacokinetics of ranolazine in part through the inhibition of CYP3A4 and P-gp.
Conclusions
The use of approaches helps to keep therapy costs low. The herbal bioenhancer is crucial in improving poorly accessible medications in order to lower healthcare costs by boosting therapeutic efficacy. Global attention is currently being paid to strategies for lowering medicine doses, which will lower the price of the therapy. Increasing medication bioavailability is one strategy to reduce drug dose and, as a result, drug toxicity and expense. Ranolazine has a low bioavailability. The recommended maximum dosage is 1000 mg. The findings of this investigation demonstrated that naringenin increases ranolazine's bioavailability. As a bioenhancer, naringenin works through a number of methods. A mechanism of action involves inhibiting drug efflux pumps and drug-metabolizing enzymes.
Availability of data and materials
All the data are present within the manuscript.
Abbreviations
- P-gp:
-
P-glycoprotein
- CYP3A4:
-
Cytochrome P4503A4
- SDS:
-
Single dose study
- MDS:
-
Multiple dose study
- MRP2:
-
Multiple resistance protein-2
- HPLC:
-
High-performance liquid chromatography
- K2EDTA:
-
Dipotassium ethylenediaminetetraacetic acid
- SCMC:
-
Sodium carboxymethyl cellulose
- s.c.:
-
Subcutaneous
- PK:
-
Pharmacokinetics
- AUC:
-
Area under the curve
- AUMC:
-
Area under the moment curve
- C max :
-
Maximum concentration
- T max :
-
Time to maximum plasma concentration
- MRT:
-
Maximum retention time
- QTc:
-
Corrected QT interval
References
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J (2005) Global burden of hypertension: analysis of worldwide data. Lancet 365(9455):217–223. https://doi.org/10.1016/S0140-6736(05)17741-1
Yusuf S, Hawken S, Ôunpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J (2004) Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 364(9438):937–952. https://doi.org/10.1016/S0140-6736(04)17018-9
Members WG, Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V (2008) Heart disease and stroke statistics—2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 117(4):e25–e146. https://doi.org/10.1161/CIRCULATIONAHA.107.187998
Association AH (2008) Heart disease and stroke statistics: biostatistical fact sheets. Circulation 117:4–12. https://doi.org/10.1161/CIR.0000000000001052
O’gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, De Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA (2013) 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 61(4):e78–e140. https://doi.org/10.1016/j.jacc.2012.11.019
O’gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, De Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA (2013) 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 127(4):529–555. https://doi.org/10.1161/CIR.0b013e3182742c84
Babu PR, Babu KN, Peter PH, Rajesh K, Babu PJ (2013) Influence of quercetin on the pharmacokinetics of ranolazine in rats and in vitro models. Drug Dev Ind Pharm 39(6):873–879. https://doi.org/10.3109/03639045.2012.707209
Nash DT, Nash SD (2008) Ranolazine for chronic stable angina. Lancet 372(9646):1335–1341. https://doi.org/10.1016/S0140-6736(08)61554-8
Tamargo J, Amorós I, Barana A, González M, Dolz P, Gómez R, Caballero R, Delpón E (2010) Farmacología clínica de la ranolazina, un nuevo fármaco en el tratamiento de la angina crónica estable. Rev Esp Cardiol Supl 10:41B-54B. https://doi.org/10.1016/S1131-3587(10)70014-5
Sossalla S, Maier LS (2012) Role of ranolazine in angina, heart failure, arrhythmias, and diabetes. Pharmacol Ther 133(3):311–323. https://doi.org/10.1016/j.pharmthera.2011.11.003
Atal N, Bedi K (2010) Bioenhancers: Revolutionary concept to market. J Ayurveda Integr Med 1(2):96. https://doi.org/10.4103/0975-9476.65073
Bose K (1929) Pharmacographia Indica. Bose Laboratories, Calcutta, India.[Google Scholar]
Sama V, Pagilla B, Chiluka R, Alvala R, Pola RK, Mullangi R (2019) Bioenhancing effects of naringin on atorvastatin. ADMET DMPK 7(3):174–182. https://doi.org/10.5599/admet.647
Salehi B, Fokou PVT, Sharifi-Rad M, Zucca P, Pezzani R, Martins N, Sharifi-Rad J (2019) The therapeutic potential of naringenin: a review of clinical trials. Pharmaceuticals 12(1):11. https://doi.org/10.3390/ph12010011
Albach R, Redman G (1969) Composition and inheritance of flavanones in citrus fruit. Phytochemistry 8(1):127–143. https://doi.org/10.1016/S0031-9422(00)85805-7
Liu J, Liu H, Zeng Q (2019) The effect of naringenin on the pharmacokinetics of ibrutinib in rat: a drug–drug interaction study. Biomed Chromatogr 33(5):e4507. https://doi.org/10.1002/bmc.4507
Burkina V, Zlabek V, Halsne R, Ropstad E, Zamaratskaia G (2016) In vitro effects of the citrus flavonoids diosmin, naringenin and naringin on the hepatic drug-metabolizing CYP3A enzyme in human, pig, mouse and fish. Biochem Pharmacol 110:109–116. https://doi.org/10.1016/j.bcp.2016.04.011
Bailey DG, Arnold JMO, Munoz C, Spence JD (1993) Grapefruit juice–felodipine interaction: mechanism, predictability, and effect of naringin. Clin Pharmacol Ther 53(6):637–642. https://doi.org/10.1038/clpt.1993.84
Ameer B, Weintraub RA (1997) Drug interactions with grapefruit juice. Clin Pharmacokinet 33(2):103–121. https://doi.org/10.2165/00003088-199733020-00003
Bressler R (2006) Grapefruit juice and prescription drug interactions. Geriatrics 61(11)
Alvarez AI, Real R, Pérez M, Mendoza G, Prieto JG, Merino G (2010) Modulation of the activity of ABC transporters (P-glycoprotein, MRP2, BCRP) by flavonoids and drug response. J Pharm Sci 99(2):598–617. https://doi.org/10.1002/jps.21851
Diaconu CH, Cuciureanu M, Vlase L, Cuciureanu R (2011) Food-drug interactions: grapefruit juice. Rev Med Chir Soc Med Nat Iasi 115(1):245–250
Jerling M (2006) Clinical pharmacokinetics of ranolazine. Clin Pharmacokinet 45(5):469–491. https://doi.org/10.2165/00003088-200645050-00003
Barthe L, Bessouet M, Woodley J, Houin G (1998) The improved everted gut sac: a simple method to study intestinal P-glycoprotein. Int J Pharm 173(1–2):255–258. https://doi.org/10.1016/S0378-5173(98)00225-7
Tanaka K, Fujita T, Yamamoto Y, Murakami M, Yamamoto A, Muranishi S (1996) Enhancement of intestinal transport of thyrotropin-releasing hormone via a carrier-mediated transport system by chemical modification with lauric acid. Biochim Biophys Acta Biomembr 1283(1):119–126. https://doi.org/10.1016/0005-2736(96)00087-9
Calderón-Sánchez EM, Domínguez-Rodríguez A, Lopez-Haldon J, Jiménez-Navarro MF, Gomez AM, Smani T, Ordonez A (2016) Cardioprotective effect of ranolazine in the process of ischemia-reperfusion in adult rat cardiomyocytes. Rev esp cardiol 69(1):45–53. https://doi.org/10.3389/fphar.2020.593225
Lin JH (2003) Drug–drug interaction mediated by inhibition and induction of P-glycoprotein. Adv Drug Deliv Rev 55(1):53–81. https://doi.org/10.1016/s0169-409x(02)00171-0
Wacher VJ, Wu CY, Benet LZ (1995) Overlapping substrate specificities and tissue distribution of cytochrome P450 3A and P-glycoprotein: implications for drug delivery and activity in cancer chemotherapy. Mol Carcinog 13(3):129–134
Schuetz EG, Beck WT, Schuetz JD (1996) Modulators and substrates of P-glycoprotein and cytochrome P4503A coordinately up-regulate these proteins in human colon carcinoma cells. Mol Pharmacol 49(2):311–318
Hodek P, Trefil P, Stiborová M (2002) Flavonoids-potent and versatile biologically active compounds interacting with cytochromes P450. Chem Biol Interact 139(1):1–21. https://doi.org/10.1016/s0009-2797(01)00285-x
Doostdar H, Burke MD, Mayer RT (2000) Bioflavonoids: selective substrates and inhibitors for cytochrome P450 CYP1A and CYP1B1. Toxicology 144(1–3):31–38. https://doi.org/10.1016/s0300-483x(99)00215-2
Fukuda K, Ohta T, Yamazoe Y (1997) Grapefruit component interacting with rat and human P450 CYP3A: possible involvement of non-flavonoid components in drug interaction. Biol Pharm Bull 20(5):560–564. https://doi.org/10.1248/bpb.20.560
Bohets H, Annaert P, Mannens G, Anciaux K, Verboven P, Meuldermans W, Lavrijsen K (2001) Strategies for absorption screening in drug discovery and development. Curr Top Med Chem 1(5):367–383. https://doi.org/10.2174/1568026013394886
Wang J, Urban L, Bojanic D (2007) Maximising use of in vitro ADMET tools to predict in vivo bioavailability and safety. Expert Opin Drug Metab Toxicol 3(5):641–665. https://doi.org/10.1517/17425255.3.5.641
Carreno-Gomez B, Duncan R (2000) Everted rat intestinal sacs: a new model for the quantitation of P-glycoprotein mediated-efflux of anticancer agents. Anticancer Res 20(5A):3157–3161
Arellano C, Philibert C, Vachoux C, Woodley J, Houin G (2007) The metabolism of midazolam and comparison with other CYP enzyme substrates during intestinal absorption: in vitro studies with rat everted gut sacs. J Pharm Pharm Sci 10(1):26–36
Khemiss F, Ahmadi S, Massoudi R, Ghoul-Mazgar S, Safta S, Moshtaghie AA, Saïdane D (2009) Effect of in vitro exposure to Vibrio vulnificus on hydroelectrolytic transport and structural changes of sea bream (Sparus aurata L.) intestine. Fish Physiol Biochem 35:541–549. https://doi.org/10.1007/s10695-008-9265-7
Khemiss F, Ghoul-Mazgar S, Moshtaghie A, Saidane D (2006) Study of the effect of aqueous extract of Grewia tenax fruit on iron absorption by everted gut sac. J Ethnopharmacol 103(1):90–98. https://doi.org/10.1016/j.jep.2005.07.017
Khemiss F, Massoudi R, Ahmadi S, Ghoul-Mazgar S, Safta S, Moshtaghie A, Saidane D (2008) Aeromonas hydrophila disturbs water and electrolyte transport in Mugil cephalus L. intestine. Afr J Biotechnol 7(4)
Taubert D, von Beckerath N, Grimberg G, Lazar A, Jung N, Goeser T, Kastrati A, Schömig A, Schömig E (2006) Impact of P-glycoprotein on clopidogrel absorption. Clin Pharmacol Ther 80(5):486–501. https://doi.org/10.1016/j.clpt.2006.07.007
Dahan A, Amidon GL (2009) Small intestinal efflux mediated by MRP2 and BCRP shifts sulfasalazine intestinal permeability from high to low, enabling its colonic targeting. Am J Physiol Gastrointest Liver Physiol 297(2):G371–G377. https://doi.org/10.1152/ajpgi.00102.2009
Föger F (2009) Strategies to overcome efflux pumps. Oral Delivery of Macromolecular Drugs: Barriers, Strategies and Future Trends:123–136
Choi J-S, Han H-K (2005) Enhanced oral exposure of diltiazem by the concomitant use of naringin in rats. Int J Pharm 305(1–2):122–128. https://doi.org/10.1016/j.ijpharm.2005.09.004
Kim HJ, Choi JS (2005) Effects of naringin on the pharmacokinetics of verapamil and one of its metabolites, norverapamil, in rabbits. Biopharm Drug Dispos 26(7):295–300. https://doi.org/10.1002/bdd.459
Choi J-S, Kang KW (2008) Enhanced tamoxifen bioavailability after oral administration of tamoxifen in rats pretreated with naringin. Arch Pharm Res 31:1631–1636. https://doi.org/10.1007/s12272-001-2161-7
Acknowledgements
Author would like to thank Shaqra University for providing facilities to carry out this work.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
The author read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
IAEC/TRS/PT/022/026.
Consent for publication
The work was completed by the corresponding author only; therefore, no need to take consent.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alotaibi, F. Naringenin alters the pharmacokinetics of ranolazine in part through the inhibition of cytochrome P450 (3A4) and P-glycoprotein. Futur J Pharm Sci 9, 23 (2023). https://doi.org/10.1186/s43094-023-00477-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-023-00477-1