
Abstract
Purpose
While there has been a great improvement in the treatment of adolescent idiopathic scoliosis, sagittal deformity correction has remained challenging. Increased rod stiffness has been shown to reduce thoracic flattening. We propose that the surgical technique can increase rod stiffness. A mechanical study was created to quantify the effect this has on construct stiffness.
Methods
The sagittal bending stiffness of a constrained over contoured rod was measured using four different commonly used instrumentation systems. Pedicle screws were secured into custom printed blocks. One block was completely immobilized, while the other block was subject to four levels of constraint. This includes no constraint, mild constraint, moderate constraint, and maximal constraint with both blocks immobilized. The rod apex was loaded until 1 cm of displacement occurred. The stiffness was then calculated and compared between groups.
Results
All four rod types showed increased bending stiffness as the construct became more constrained. The moderately constrained and the maximally constrained groups had a significantly higher stiffness compared to the unconstrained groups in all rod types (p < 0.05). The 6.0 mm titanium circular rods showed the highest increase in stiffness between maximal and no constraint, which became 3.02 × stiffer.
Conclusions
Rod stiffness is not only determined by size, shape, and metal alloy, but also by surgical technique. Constraining the spinal instrumentation by first locking the rod to the proximal and distal anchors significantly increases the sagittal bending stiffness. In a mechanical model this technique increases rod bending stiffness regardless of the material or shape.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Purpose
As instrumentation and surgical techniques have evolved, correction of deformity for adolescent idiopathic scoliosis (AIS) has improved. Initially the focus was on coronal deformity but more recently attention has been focused on sagittal deformity correction, which remains a challenge [1,2,3]. A recently published article reported that failure to restore normal thoracic kyphosis when performing selective thoracic fusions increases the risk of post-operative sagittal plane deterioration [4]. Literature has also shown that increased rod stiffness leads to an improved reduction with less thoracic flattening [5]. Rod stiffness is affected by rod diameter, rod material, and rod shape [6]. Surgical technique can also affect rod stiffness. This mechanical study seeks to evaluate how rod stiffness is affected by the surgical reduction sequence.
We hypothesize that rod stiffness can be increased during the surgical reduction sequence by initially securing an over contoured concave rod to the proximal and distal anchors prior to any reduction. We sought to quantify the amount of rod stiffness gained when constraining the rod by developing a mechanical model that simulates proximal and distal locking of the rod prior to reduction. We tested the relative stiffness of four different rods commonly used for posterior spinal instrumentation. In order to simulate variations in rod-spine stiffness during deformity correction, these rods were tested using four different levels of constraint placed between the proximal and distal fixation points.
Methods
Rod testing
The sagittal bending stiffness of a constrained, over-contoured rod was measured using four different levels of resistance to distraction between the proximal and distal ends of the rod (between the anchors). This was tested using four different commonly used instrumentation systems. These included: 5.5 mm ultra-high strength stainless steel circular rods [Depuy], 5.5 mm titanium rail rods [K2M], 6.0 mm titanium circular rods [Orthopediatrics], and 6.0 mm cobalt chromium circular rods [Orthopediatrics]. Five rods for each instrumentation system were tested under each of the four levels of constraint. Thus, a total of 20 rods were tested from each system for a total of 80 total rods.
Poly-axial pedicle screws 40–45 mm in length to be used with a corresponding brand of rod were secured into custom Makerbot 3D printed blocks using tough polylactic acid. All rods were cut to be 25 cm in length and contoured with a 75° bend. The rod was secured into the blocks representing proximal and distal anchors. One block was immobilized, while the other was placed onto an X–Y table and allowed to slide. The amount of constraint between the two blocks was varied by placing springs between the two anchors. Group 1 was unconstrained and the mobile anchor was allowed to move freely. Group 2 was mildly constrained, with one spring between the two blocks (spring constant = 26.4 N/mm). Group 3 was moderately constrained with two springs between the two blocks (spring constant = 52.8 N/mm). Group 4 was maximally constrained with both blocks immobilized. Five identical specimens of each of the 4 rod types were tested in each level of constraint.
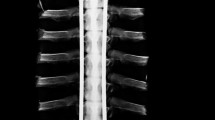
Using a universal biaxial materials testing machine (ElectroPuls E10000, Instron, Canton, MA), each rod was loaded at the apex until 1 cm of displacement of the apex occurred (Fig. 1). Stiffness was calculated as the slope of the load–displacement curve between initial and peak points. The mean bending stiffness was calculated for each rod type for each of the four constraint levels tested.

Biomechanical stiffness testing A unconstrained 5.5 mm Ti rail rod, B mildly constrained 6.0 mm Ti circular rod, C moderately constrained 5.5 mm UHSS circular rod, and D fully constrained 6.0 mm CoCr circular rod
Statistical Analysis
Each of the two semi-constrained and the maximally constrained groups were compared to the unconstrained group using paired T tests. P values < 0.05 were considered statistically significant.
Results
All four rod types showed increased bending stiffness as the construct became more constrained. The moderately constrained and the maximally constrained groups had a significantly higher stiffness compared to the unconstrained groups in all rod types (p < 0.05). The p value in comparison to the unconstrained group is shown in parentheses below each stiffness value (Table 1). The systems that showed the highest increase in stiffness between maximal constraint and no constraint were the 6.0 mm titanium circular rods and the 5.5 mm SS rods which became 3.02 × stiffer (170.1/56.2) and 2.99 × stiffer (164.6/55.1), respectively. The 6.0 mm CC rods became 2.73 × stiffer (228.3/83.5). The 5.5 mm titanium rail rod showed the highest amount of stiffness when not constrained, but it was least affected by constraint becoming 1.31 × stiffer (126/95.8) at maximal constraint.
Conclusion
Sagittal correction continues to gain more attention in the literature. Thoracic kyphosis is critical as it influences lumbar lordosis, increases thoracic volume, and may decrease the risk of proximal junctional kyphosis [4, 7,8,9]. However, restoring kyphosis in patients with adolescent idiopathic scoliosis remains challenging in spite of modern instrumentation systems and current reduction techniques.
Kyphosis restoration is likely affected by many factors. The literature has looked at use of ponte osteotomies, high screw density, as well as rod stiffness [10,11,12,13,14]. Many authors have found that using a larger diameter rod or a rod with a more stiff material allows for a better restoration of thoracic kyphosis [5, 15]. Newton et al. recently published an article showing that the greatest factor in kyphosis restoration was the surgeon, not the instrumentation system used or number of screws [16]. It appears that these findings are largely due to variability in surgical technique and effectiveness in maximizing mechanical advantage of the instrumentation system. Alterations in technique can have influence on rod/construct stiffness and other mechanical forces that affect deformity correction. This is analogous to differences in the amount of force that can be applied by holding a wrench or a mallet in different positions.
The results of this study demonstrate that amongst various instrumentation systems, stiffness of the rod is increased as constraint on the ends of the rod is increased. Increasing constraint on the rod during surgery occurs when the rod is locked both to proximal and distal anchors. In order for this to work properly the rod needs to be overcontoured on the concavity of a hypokyphotic spine. The over-contoured rod is locked into the proximal and distal pedicle screws creating an arch. As reduction proceeds, the rod will undergo some deformation and flattening which will result in distraction of the concave end vertebra. In vivo, the increasing resistance to distraction as the proximal and distal screws are distracted results in increasing constraint on the rod, which increases rod stiffness. Thus, when locked proximally and distally, rod stiffness increases as the reduction proceeds.
The more flexible rods in our study had a greater relative increase in stiffness when constraining the ends. Both the 5.5 mm stainless steel and 6.0 mm titanium circular rods had approximately a threefold increase in stiffness when fully constrained. While all of the rods had increased stiffness with increased constraint, the stiffer rods showed a relatively smaller increase in stiffness compared to the more flexible rods. This information is helpful to guide the reduction sequence in order to maximize rod stiffness using initial proximal and distal locking on the concave major thoracic curve. This technique is especially useful when using a more flexible rod. Using this technique can offer more options for rod choice by providing the benefits of some of the more flexible materials without sacrificing the benefits of a stiffer rod. Titanium has a higher yield strength compared to stainless steel or cobalt chromium, which is defined as the force required before there is permanent deformation [6]. The modulus of elasticity of titanium most closely approximates that of bone, which may decrease the risk of proximal junctional kyphosis [17]. In addition, there is some data that titanium decreases risk of hardware infection [18]. In spite of these potential advantages titanium rods are often avoided because of excessive flexibility and tends to flatten when attempting to reduce stiff spines. However, if a titanium rod is constrained proximally and distally, the rod stiffness can be greatly increased, and may even exceed an unconstrained cobalt chromium rod.
Physiologic resistance to distraction varies significantly in different patients. Even within the same patient the amount of resistance to distraction often increases as the reduction proceeds. With this in mind there is no single level of constraint that could be truly representative of physiologic loads. In our mechanical model we chose to test our implants using no constraint, which shows the amount of intrinsic stiffness of unconstrained implants. Two intermediate levels of constraint were used which were intended to represent points within the range of physiologic stiffness. The senior author tested the amount of resistance to distraction created by the springs using a spinal distractor to confirm that they were similar to distraction forces seen during routine scoliosis surgery. The maximal constraint was tested with the two blocks in fixed positions. This point likely is beyond the typical amount of constraint encountered in vivo. It was studied for two reasons: The range of increased stiffness between group 3 and group 4 gives us an idea of the effect of a constrained rod in a stiff spine. Second, it allows us to understand, where failure occurs when maximally constraining the ends of the rod. We were interested to know if the screw would fail, if the rod would deform, if there would be failure at the screw rod interface, or if there would be deformation of the polylactic acid blocks.
Titanium rail rods were shown to be the stiffest of all of the unconstrained rods. Due to its unique shape, the titanium rail maintains the benefits of titanium without sacrificing stiffness. This is advantageous for correcting thoracic kyphosis. Interestingly, when maximally constrained, the titanium rail rod actually was less stiff than any of the other rods. Some screw–rod slippage occurred when tested at maximal constraint allowing the implant to flatten. This appears to be due to the fact that the screw–rod interface is not designed for such high loads which are likely beyond what is encountered in surgery. The other three instrumentation systems failed with loads well above typical loads in various ways including: rod bending at the apex, slight screw–rod interface motion, and pedicle screw-block motion.
Limitations
During the reduction of scoliosis, the stress on the spine and instrumentation is not incremental or stagnant, but a dynamic continuous variable. This biomechanical model uses incremental changes in constraint on spinal instrumentation to simulate a range of scenarios. It is uncertain how any given spine at any given point in reduction would actually compare to the in-situ levels of constraint chosen for this study. Nonetheless, the trends seen in our model offer valuable information when comparing implants and the potential benefits of over contoured rods with initial proximal and distal locking. Finally, this biomechanical study could also have been performed using a digital modeling approach.
Constraining the spinal instrumentation by first locking the rod to the proximal and distal anchors significantly increases the sagittal bending stiffness. In a mechanical model this technique increases rod bending stiffness regardless of the material or shape. This study explains how small variations in technique can significantly alter the mechanical properties of the instrumentation construct. By maximizing the mechanical advantage of the instrumentation system, rod stiffness can be significantly increased, mitigating some of the limitations of smaller or more flexible instrumentation systems. It is our hope that improved understanding of the mechanical properties of the instrumentation system as well as surgeon ability to alter the rod stiffness will allow for improved deformity correction especially in the sagittal plane.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Code availability
Not applicable.
References
de Jonge T, Dubousset JF, Illes T (2002) Sagittal plane correction in idiopathic scoliosis. Spine (Phila Pa 1976) 27:754–760
Bridwell KH, Betz R, Capelli AM et al (1990) Sagittal plane analysis in idiopathic scoliosis patients treated with Cotrel-Dubousset instrumentation. Spine (Phila Pa 1976) 15:644–649
Clement JL, Chau E, Vallade MJ et al (2011) Simultaneous translation on two rods is an effective method for correction of hypokyphosis in AIS: radiographic results of 24 hypokyphotic thoracic scoliosis with 2 years minimum follow-up. Eur Spine J 20:1149–1156
Rothenfluh DA, Stratton A, Nnadi C et al (2019) A critical thoracic kyphosis is required to prevent sagittal plane deterioration in selective thoracic fusions in Lenke I and II AIS. Eur Spine J 28:3066–3075
Abul-Kasim K, Karlsson MK, Ohlin A (2011) Increased rod stiffness improves the degree of deformity correction by segmental pedicle screw fixation in adolescent idiopathic scoliosis. Scoliosis 6:13
Ohrt-Nissen S, Dahl B, Gehrchen M (2018) Choice of rods in surgical treatment of adolescent idiopathic scoliosis: what are the clinical implications of biomechanical properties? A review of the literature. Neurospine 15:123–130
Ogilvie JW, Schendel MJ (1988) Calculated thoracic volume as related to parameters of scoliosis correction. Spine (Phila Pa 1976) 13:39–42
Clement JL, Pelletier Y, Solla F et al (2019) Surgical increase in thoracic kyphosis increases unfused lumbar lordosis in selective fusion for thoracic adolescent idiopathic scoliosis. Eur Spine J 28:581–589
Yaszay B, Bastrom TP, Bartley CE et al (2017) The effects of the three-dimensional deformity of adolescent idiopathic scoliosis on pulmonary function. Eur Spine J 26:1658–1664
Clements DH, Betz RR, Newton PO et al (2009) Correlation of scoliosis curve correction with the number and type of fixation anchors. Spine (Phila Pa 1976) 34:2147–2150
Larson AN, Aubin CE, Polly DW Jr et al (2013) Are more screws better? A systematic review of anchor density and curve correction in adolescent idiopathic scoliosis. Spine Deform 1:237–247
Lonner BS, Lazar-Antman MA, Sponseller PD et al (2012) Multivariate analysis of factors associated with kyphosis maintenance in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 37:1297–1302
Halanski MA, Cassidy JA (2013) Do multilevel Ponte osteotomies in thoracic idiopathic scoliosis surgery improve curve correction and restore thoracic kyphosis? J Spinal Disord Tech 26:252–255
Shah SA, Dhawale AA, Oda JE et al (2013) Ponte osteotomies with pedicle screw instrumentation in the treatment of adolescent idiopathic scoliosis. Spine Deform 1:196–204
Liu H, Li Z, Li S et al (2015) Main thoracic curve adolescent idiopathic scoliosis: association of higher rod stiffness and concave-side pedicle screw density with improvement in sagittal thoracic kyphosis restoration. J Neurosurg Spine 22:259–266
Newton PO, Wu KW, Bastrom TP et al (2019) What factors are associated with kyphosis restoration in lordotic adolescent idiopathic scoliosis patients? Spine Deform 7:596–601
Han S, Hyun SJ, Kim KJ et al (2017) Rod stiffness as a risk factor of proximal junctional kyphosis after adult spinal deformity surgery: comparative study between cobalt chrome multiple-rod constructs and titanium alloy two-rod constructs. Spine J 17:962–968
Di Silvestre M, Bakaloudis G, Lolli F et al (2011) Late-developing infection following posterior fusion for adolescent idiopathic scoliosis. Eur Spine J 20(Suppl 1):S121-127
Funding
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
Substantial contribution to the work: CB, JS, SN. Draft the work/revised the work: CB, JS, SN. Approved the version to be published: CB, JS, SN. Agree to be accountable: CB, JS, SN.
Corresponding author
Ethics declarations
Conflict of interest
Dr. Burke and Dr. Speirs declare that they have no conflict of interest. Dr. Scott Nelson has received consulting fees and honorarium not associated with this work from K2M, NuVasive, OrthoSpine, and Orthofix.
Ethics approval
This biomechanical study followed all ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB) of Loma Linda University approved this study (IRB# 5160178).
Consent to participate
Not applicable.
Rights and permissions
About this article

Cite this article
Burke, C.A., Speirs, J.N. & Nelson, S.C. Maximizing mechanical advantage: surgical technique increases stiffness in spinal instrumentation. Spine Deform 10, 295–299 (2022). https://doi.org/10.1007/s43390-021-00425-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43390-021-00425-0