
Abstract
Human cytochrome P450 (CYP) enzymes are composed of 57 individual enzymes that perform monooxygenase activities. They have diverse physiological roles in metabolizing xenobiotics and producing important endogenous compounds, such as steroid hormones and vitamins. At least seven CYP enzymes are involved in steroid biosynthesis. Steroidogenesis primarily occurs in the adrenal glands and gonads, connecting each reaction to substrates and products. Steroids are essential for maintaining life and significantly contribute to sexual differentiation and reproductive functions within the body. Disorders in steroid biosynthesis can frequently cause serious health problems and lead to the development of diseases, such as prostate cancer, breast cancer, and Cushing’s syndrome. In this review, we provide current updated knowledge on the major CYP enzymes involved in the biosynthetic process of steroids, with respect to their enzymatic mechanisms and clinical implications for the development of new drug candidates.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
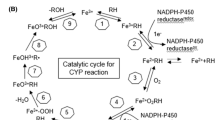
Cytochrome P450 (CYP, P450) enzymes are a superfamily of monooxygenases with heme as the prosthetic group [1]. They catalyze the metabolism of diverse xenobiotic and endogenous compounds including steroids, vitamins, and fatty acids [2]. These enzymes exist in the endoplasmic reticulum and mitochondria, and their catalytic activities are supported by NAD(P)H and redox partners such as P450 oxidoreductase (POR), adrenodoxin (ADX) and adrenodoxin reductase (ADR) [3]. The human genome contains 57 CYP genes, many of which are involved in steroid biosynthesis and metabolism [2, 4]. At least seven CYP enzymes are involved in steroid biosynthesis; CYP11A1, CYP17A1, CYP19A1, CYP11B1, CYP11B2, CYP21A2, and CYP51A1 (Fig. 1) [2]. Steroidogenesis primarily occurs in the adrenal glands and gonads, connecting each reaction to substrates and products. Steroids are critical for life and contribute significantly to sexual differentiation and reproductive functions within the body [5]. However, abnormal steroid levels can also cause diseases such as prostate cancer, breast cancer, and Cushing’s syndrome [6,7,8]. To treat these diseases, it is necessary to reduce steroid levels, and drugs targeting the key enzymes involved in each steroid biosynthesis step have been developed (Table 1). However, several shortcomings are associated with these drugs, particularly their selectivity and cross-inhibition. To date, various attempts have been made to address these issues. This review focuses on steroidogenic CYPs as potential drug targets for diseases treatment. Additionally, the efficacy and adverse effects of approved drugs and candidate compounds are explored.

Steroid biosynthesis pathway. FF-MAS (follicular fluid meiosis-activating sterol, 14-demethyl-14-dehydrolanosterol), DHEA (dehydroepiandrosterone), and DHT (dihydrotestosterone)
CYP11A1
CYP11A1 is involved in the initiation step of hormonal steroid biosynthesis from cholesterol (Fig. 1). It is located in the mitochondrial membrane and catalyzes the conversion of cholesterol to pregnenolone. Cholesterol is first transported into the mitochondria by translocator protein and steroidogenic acute regulatory protein. Subsequently, CYP11A1 performs two successive hydroxylations on C22 and C20 of cholesterol and cleaves the cholesterol side chain between C20 and C22 (Fig. 2). The activity of CYP11A1 requires two cofactor proteins in the mitochondrial membrane: ADX and ADR. Pregnenolone, a product of CYP11A1, is a precursor of all steroid hormones. Inhibiting this catalytic step can suppress subsequent steroidogenic reactions and induce a deficiency in steroid hormones [9]. There have been attempts to leverage steroid levels by co-treatment with a physiological dose of essential steroids to treat diseases [10]. ODM-208 was chosen as a candidate inhibitor after screening and utilizing the crystal structure of CYP11A1 bound to cholesterol (Fig. 3) [10]. ODM-208 inhibits pregnenolone biosynthesis and suppresses downstream of steroid biosynthesis, with IC50 values in the nanomolar range [10]. It has more potent efficacy than the other non-selective inhibitors. In patients with castration-resistant prostate cancer (CRPC) co-treated with dexamethasone and fludrocortisone, ODM-208 exhibited a reduction in the levels of pregnenolone and testosterone [10].

Multistep oxidation reactions of cholesterol by CYP11A1

Chemical structures of specific steroidogenic CYP inhibitors. CYP11A1 inhibitor, opevesostat; CYP17A1 inhibitor, abiraterone; CYP19A1 inhibitors, exemestane, letrozole, and anastrozole; CYP11B1 inhibitors, osilodrostat, and levoketoconazole; CYP11B2, baxdrostat and lorundrostat
As the protein crystal structure data of CYP11A1 is available, its analysis can provide clues for the development of new drug candidates [11]. The crystal structure of CYP11A1 revealed that C20 and C22 of cholesterol are positioned just above the heme, and that this interaction was facilitated by enzyme residues such as W87, L101, F202, and I461 (Fig. 4A). The two methyl groups on the β face of cholesterol interact with S352 and a water molecule, forming a hydrogen bond with S352. This interaction facilitates the positioning of the reactive site of cholesterol closer to heme. Additionally, various residues assist in binding cholesterol rings to the active site. The 3β hydroxyl of cholesterol forms hydrogen bonds with two water molecules, creating an extensive hydrogen bonding network with residues such as H39, Y61, N210, Q377, and other water molecules (Fig. 4A) [11]. Rational design targeting of these key residues could potentially aid in the development of novel inhibitors that more efficiently modulate the initial step of steroid synthesis.

Structural views of inhibitor binding in the active sites of steroidogenic CYP enzymes. a Binding of cholesterol to CYP11A1, b binding of abiraterone to CYP17A1, c binding of exemestane to CYP19A1
CYP17A1
CYP17A1 is primarily expressed in adrenal glands and gonads. It plays a crucial role in androgen synthesis by catalyzing the sequential 17α-hydroxylation of progesterone and pregnenolone, followed by a 17,20-lyase reaction. This reaction ultimately leads to the generation of androstenedione and dehydroepiandrosterone (DHEA) (Fig. 1). Androgens synthesized by CYP17A1 are essential for the differentiation and maturation of male reproductive organs. In addition, they are key factors in prostate cancer, promoting the survival and growth of prostate cancer cells. Therefore, androgen signaling is considered as an important therapeutic target for the treatment of prostate cancer [7]. Consequently, CYP17A1 has been considered as a drug target for suppressing androgen synthesis. The first drug approved as a CYP17A1 inhibitor was abiraterone (Fig. 3). Abiraterone is a pregnenolone analog with a pyridyl substituent at the 17th carbon atom that inhibits the 17-hydroxylase and 17,20-lyase activities of CYP17A1 [12]. CYP17A1 binds abiraterone through a type II inhibitory interaction with CYP enzyme [13]. Abiraterone binds more tightly to CYP17A1 than progesterone [13]. Inhibition assays with purified CYP17A1 and the H295R cell line demonstrated that abiraterone inhibits the 17-hydroxylase and 17,20-lyase activities of CYP17A1 with IC50 values in the nanomolar range [14]. In clinical trial, the serum levels of testosterone, DHEA, and androstenedione decreased significantly after treatment with abiraterone, and patients exhibited > 50% reduction in prostate-specific antigen [15]. In the crystal structure of CYP17A1 with abiraterone, structural folding characteristics of the CYP enzyme are evident, with the abiraterone structure showing tight interactions with residues in the active site of CYP17A1 through a hydrogen bond network, along with water molecules (Fig. 4B) [13]. These tight interactions result in the significant inhibition of CYP17A1 enzyme activity. However, there are some concerns with the use of abiraterone in relation to the steroid biosynthesis pathway; abiraterone inhibits not only the 17,20-lyase reaction but also the 17-hydroxylase reaction, leading to interference in cortisol production (Fig. 1) [16]. When treated with abiraterone, cortisol levels decrease and adrenocorticotropic hormone (ACTH) secretion increases [17]. Side effects such as hypertension and hypokalemia may occur due to increased mineralocorticoid activity. Co-administration of an appropriate dose of prednisone as a glucocorticoid replacement can reduce ACTH levels and mitigate adverse effects caused by mineralocorticoids [15, 17, 18]. Targeting the active site may be challenging because of the shared active site of both hydroxylase and lyase reactions. Therefore, it is necessary to target auxiliary proteins that interact with CYP17A1. Cytochrome b5 (b5) is a small hemeprotein that performs various functions in the body [19, 20]. In particular, the b5 protein shows selective enhancement in the lyase reaction of CYP17A1 (not in 17-hydroxylation), with the lyase reaction being mainly dependent on the presence of b5 [21,22,23,24]. The b5 increases the coupling efficiency of NADPH consumption, suggesting that this is one of the reasons for the activation of the lyase reaction by b5 protein [25]. It has been suggested that b5 operates as an allosteric regulator of CYP17A1 [21, 26,27,28], functioning without directly transferring electrons [28]. Previous studies have shown that R347 and R358 of CYP17A1 play critical roles in binding to b5 [19, 21, 22]. An in vivo study showed that the loss of b5 function results in lyase deficiency, leading to a decrease in androgen levels [29]. Therefore, compounds targeting R347 and R358 of CYP17A1 to inhibit binding to b5 could be potential drug candidates for inhibiting the lyase reaction of CYP17A1 without interfering with the active site or hydroxylase reaction. Another concern regarding CYP17A1 inhibitors is their off-target effect that may inhibit several other CYP enzymes. Within the steroidogenic CYP family, abiraterone inhibits CYP21A2 at higher concentrations [30]. When CYP21A2 is inhibited, glucocorticoid and mineralocorticoid levels decrease, leading to increased ACTH secretion. This, in turn, can result in diseases such as adrenal hyperplasia and hyperkalemia [31, 32]. Therefore, various attempts have been made to develop new inhibitors with higher selectivity for CYP17A1 [32].
CYP19A1
CYP19A1 catalyzes the aromatase reaction to convert androstenedione and testosterone into estrone and estradiol, respectively, via a sequential reaction (Fig. 5). Estrogens, which are the products of the CYP19A1 reaction, are important hormones for reproductive development and growth in females. However, estrogen can cause breast cancer by inducing the division and proliferation of breast tissue [6]. Estrogen-dependent breast cancer can be treated by suppressing estrogen synthesis. Therefore, several approaches targeting CYP19A1, the key enzyme in estrogen synthesis, have been investigated and several clinical drugs have been developed. Exemestane, letrozole, and anastrozole are typical third generation CYP19A1 inhibitors (Fig. 3). They show high selectivity and potency in the suppression of CYP19A1 [33]. Exemestane, a steroidal inhibitor, inhibits CYP19A1 with IC50 values in the nanomolar range and high affinity [34]. In patients, exemestane caused a significant reduction in the levels of estrogen in both plasma and urine, demonstrating fast absorption [35]. The key factor in these inhibition reactions is the C6-methylidene group, which represents a crucial distinction between exemestane and androstenedione. Exemestane exhibits binding characteristics similar to those of androstenedione, a CYP19A1 substrate. The steroid nucleus is surrounded by hydrophobic residues, and the 3- and 17-keto oxygen atoms interact with 115R, 374 M, and 309D via hydrogen bonding. Several conformational changes in the access channel of CYP19A1 and additional hydrophobic interactions allow exemestane to bind to CYP19A1. These new interactions result in a higher affinity and more suitable structure for the CYP19A1 active site (Fig. 4C) [34]. Unlike exemestane, letrozole and anastrozole are non-steroidal inhibitors of CYP19A1. These inhibitors also decrease estrogen levels [36, 37]. The crystal structures of CYP19A1 with letrozole and anastrozole are not yet available. However, based on docking analysis, it has been speculated that the formation of a coordinate bond between the triazole structure of the two inhibitors and the heme iron of CYP19A1 contributes to their high-affinity inhibition [38]. One of the adverse effects of CYP19A1 inhibitors is related to bones. In premenopausal women, the ovaries are the main glands responsible for estrogen secretion. In postmenopausal women, these glands no longer function in estrogen synthesis; instead, several peripheral tissues produce estrogens, which function as paracrine and intracrine regulators, but not as endocrine regulators [39]. In particular, CYP19A1 is expressed in bone tissues, such as osteoblasts and can produce estrogen, which is responsible for the maintenance of bone formation [40, 41]. Therefore, exemestane-induced inhibition can cause estrogen reduction in the bone, thereby increasing bone resorption. In a clinical study, exemestane significantly reduced bone mineral density (BMD) and cortical thickness in various body parts [42]. Decreased BMD was also observed following treatment with letrozole, and anastrozole [43, 44].

Sequential enzyme reactions to produce estrogens by CYP19A
CYP11B1 and CYP11B2
The main activity of CYP11B1 in the adrenal cortex is the conversion of 11-deoxycortisol to cortisol and 11-deoxycorticosterone to corticosterone (Fig. 1). Excessive levels of cortisol, induced by various stimuli such as ACTH, can cause Cushing’s syndrome and a crucial factor in the treatment of Cushing’s syndrome is a reduction in cortisol levels [8]. Several candidate drug targeting CYP11B1 have been developed. Recently, osilodrostat and levoketoconazole have been approved as CYP11B1 inhibitors for the treatment of Cushing’s syndrome (Fig. 3). In a clinical study, these agents showed a significant reduction in the mean urinary free cortisol below upper limit of normal in patients with Cushing’s disease [45, 46]. Owing to the high similarity in amino acid sequences between CYP11B1 and CYP11B2, the simultaneous inhibition of CYP11B2 can be a serious issue because CYP11B2 is involved in the synthesis of aldosterone. In practice, osilodrostat has been reported to potently inhibit both CYP11B1 and CYP11B2 in several cell lines [47].
CYP11B2 plays a key role in aldosterone synthesis from corticosterone (Fig. 1). Elevated levels of aldosterone, resulting from excessive activation of CYP11B2, are a representative cause of secondary hypertension. Therefore, CYP11B2 is considered a potential drug target for the treatment of hypertension. There are currently no approved drugs that selectively target CYP11B2; however, several agents for this purpose are currently under development. To this end, baxdrostat (Fig. 3), a candidate drug for CYP11B2 inhibition, showed 100 times higher selectivity for CYP11B2 than for CYP11B1 in in vitro tests [48]. Additionally, it significantly decreased aldosterone levels and demonstrated a dose-dependent reduction in systolic blood pressure without affecting cortisol levels [49]. Lorundrostat (Fig. 3), another candidate drug, exhibited similar effects [50].
Conclusion
Several inhibitors of steroidogenic CYPs have been approved as clinical drugs and have demonstrated significant suppression of steroid biosynthesis. However, there remain unmet needs for the treatment of diseases involving steroid biosynthesis. A third-generation inhibitor of CYP19A1 showed a simultaneous decline in BMD in postmenopausal women with a decrease in estrogen levels. Abiraterone also showed high efficacy in the reduction of androgens by inhibiting CYP17A1; however, co-treatment with prednisone was required to replace glucocorticoids. In addition, osilodrostat and abiraterone inhibit off-target CYPs, leading to a deficiency in glucocorticoids and mineralocorticoids.
Numerous candidate agents are currently under development with the aim of improved efficacy. However, several challenges remain in the development of drugs targeting CYPs. First, each steroidogenic reaction is interconnected with its substrates and products, indicating that the inhibition of a particular CYP can lead to unexpected effects. Consequently, some CYP inhibitors may require co-administration with other drugs to mitigate their side effects. Another concern is the similarity between various CYPs, which may inadvertently lead to the inhibition of unintended CYPs. Achieving high selectivity for the target CYP is crucial for addressing this issue. Crystal structure data plays a pivotal role in the development of drugs with enhanced selectivity.
The crystal structures of several steroidogenic enzymes, including CYP11A1, CYP17A1, CYP19A1, CYP11B1, and CYP11B2, have been determined. By comparing the binding of enzyme with substrates or other inhibitors using these crystal structure, new drugs can be designed, and modifications to increase selectivity can be explored. Additionally, a new strategy for CYP inhibition beyond competitive enzyme inhibition is necessary. Targeting the proteinaceous cofactors of CYPs, such as b5, ADR, and POR, could offer promising avenues for inhibition. Identifying the residues responsible for binding between CYP and its cofactor could aid in the development of new drugs with heightened selectivity. By addressing these challenges and compensating for the related defects, CYP inhibitors with high efficacy and selectivity can be developed to treat various diseases caused by abnormal steroid levels.
References
Omura T (1999) Forty years of cytochrome P450. Biochem Biophys Res Commun 266:690–698. https://doi.org/10.1006/bbrc.1999.1887
Guengerich FP (2022) Roles of cytochrome P450 enzymes in pharmacology and toxicology: past, present, and future. Adv Pharmacol 95:1–47. https://doi.org/10.1016/bs.apha.2021.12.001
Guengerich FP (2004) Cytochrome P450: what have we learned and what are the future issues? Drug Metab Rev 36:159–197. https://doi.org/10.1081/dmr-120033996
Guengerich FP (2006) Cytochrome P450s and other enzymes in drug metabolism and toxicity. AAPS J 8:E101–E111. https://doi.org/10.1208/aapsj080112
Adhya D, Annuario E, Lancaster MA, Price J, Baron-Cohen S, Srivastava DP (2018) Understanding the role of steroids in typical and atypical brain development: advantages of using a “brain in a dish” approach. J Neuroendocrinol 3:e12547. https://doi.org/10.1111/jne.12547
Yaghjyan L, Colditz GA (2011) Estrogens in the breast tissue: a systematic review. Cancer Causes Control 22:529–540. https://doi.org/10.1007/s10552-011-9729-4
Basu S, Tindall DJ (2010) Androgen action in prostate cancer. Horm Cancer 1:223–228. https://doi.org/10.1007/s12672-010-0044-4
Lacroix A, Feelders RA, Stratakis CA, Nieman LK (2015) Cushing’s syndrome. Lancet 386:913–927. https://doi.org/10.1016/s0140-6736(14)61375-1
Miller WL, Auchus RJ (2011) The molecular biology, biochemistry, and physiology of human steroidogenesis and its disorders. Endocr Rev 32:81–151. https://doi.org/10.1210/er.2010-0013
Karimaa M, Riikonen R, Kettunen H, Taavitsainen P, Ramela M, Chrusciel M, Karlsson S, Rummakko P, Simola O, Wohlfahrt G, Hakulinen P, Vuorela A, Joensuu H, Utriainen T, Fizazi K, Oksala R (2022) First-in-class small molecule to inhibit CYP11A1 and steroid hormone biosynthesis. Mol Cancer Ther 21:1765–1776. https://doi.org/10.1158/1535-7163.Mct-22-0115
Strushkevich N, MacKenzie F, Cherkesova T, Grabovec I, Usanov S, Park HW (2011) Structural basis for pregnenolone biosynthesis by the mitochondrial monooxygenase system. Proc Natl Acad Sci U S A 108:10139–10143. https://doi.org/10.1073/pnas.1019441108
Potter GA, Barrie SE, Jarman M, Rowlands MG (1995) Novel steroidal inhibitors of human cytochrome P45017 alpha (17 alpha-hydroxylase-C17,20-lyase): potential agents for the treatment of prostatic cancer. J Med Chem 38:2463–2471. https://doi.org/10.1021/jm00013a022
DeVore NM, Scott EE (2012) Structures of cytochrome P450 17A1 with prostate cancer drugs abiraterone and TOK-001. Nature 482:116–119. https://doi.org/10.1038/nature10743
Bonomo S, Hansen CH, Petrunak EM, Scott EE, Styrishave B, Jørgensen FS, Olsen L (2016) Promising tools in prostate cancer research: selective non-steroidal cytochrome P450 17A1 inhibitors. Sci Rep 6:29468. https://doi.org/10.1038/srep29468
Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, Settatree S, Barrett M, Parker C, Martins V, Folkerd E, Clark J, Cooper CS, Kaye SB, Dearnaley D, Lee G, de Bono JS (2008) Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clin Oncol 26:4563–4571. https://doi.org/10.1200/jco.2007.15.9749
Guengerich FP (2023) Cytochrome P450 enzymes as drug targets in human disease. Drug Metab Dispos DMD-MR-2023-001431. https://doi.org/10.1124/dmd.123.001431 [Online ahead of print]
Auchus RJ, Yu MK, Nguyen S, Mundle SD (2014) Use of prednisone with abiraterone acetate in metastatic castration-resistant prostate cancer. Oncologist 19:1231–1240. https://doi.org/10.1634/theoncologist.2014-0167
Ryan CJ, Smith MR, Fong L, Rosenberg JE, Kantoff P, Raynaud F, Martins V, Lee G, Kheoh T, Kim J, Molina A, Small EJ (2010) Phase I clinical trial of the CYP17 inhibitor abiraterone acetate demonstrating clinical activity in patients with castration-resistant prostate cancer who received prior ketoconazole therapy. J Clin Oncol 28:1481–1488. https://doi.org/10.1200/jco.2009.24.1281
Bhatt MR, Khatri Y, Rodgers RJ, Martin LL (2017) Role of cytochrome b5 in the modulation of the enzymatic activities of cytochrome P450 17α-hydroxylase/17,20-lyase (P450 17A1). J Steroid Biochem Mol Biol 170:2–18. https://doi.org/10.1016/j.jsbmb.2016.02.033
Lee G-H, Kim V, Lee S-G, Jeong E, Kim C, Lee Y-B, Kim D (2024) Catalytic enhancements in cytochrome P450 2C19 by cytochrome b5. Toxicol Res 40:215–222. https://doi.org/10.1007/s43188-023-00219-8
Kim D, Kim V, McCarty KD, Guengerich FP (2021) Tight binding of cytochrome b(5) to cytochrome P450 17A1 is a critical feature of stimulation of C21 steroid lyase activity and androgen synthesis. J Biol Chem 296:100571. https://doi.org/10.1016/j.jbc.2021.100571
Geller DH, Auchus RJ, Miller WL (1999) P450c17 mutations R347H and R358Q selectively disrupt 17,20-lyase activity by disrupting interactions with P450 oxidoreductase and cytochrome b5. Mol Endocrinol 13:167–175. https://doi.org/10.1210/mend.13.1.0219
Gonzalez E, Guengerich FP (2017) Kinetic processivity of the two-step oxidations of progesterone and pregnenolone to androgens by human cytochrome P450 17A1. J Biol Chem 292:13168–13185. https://doi.org/10.1074/jbc.M117.794917
Katagiri M, Kagawa N, Waterman MR (1995) The role of cytochrome b5 in the biosynthesis of androgens by human P450c17. Arch Biochem Biophys 317:343–347. https://doi.org/10.1006/abbi.1995.1173
Peng HM, Im SC, Pearl NM, Turcu AF, Rege J, Waskell L, Auchus RJ (2016) Cytochrome b5 activates the 17,20-lyase activity of human cytochrome P450 17A1 by increasing the coupling of NADPH consumption to androgen production. Biochemistry 55:4356–4365. https://doi.org/10.1021/acs.biochem.6b00532
Estrada DF, Laurence JS, Scott EE (2013) Substrate-modulated cytochrome P450 17A1 and cytochrome b5 interactions revealed by NMR. J Biol Chem 288:17008–17018. https://doi.org/10.1074/jbc.M113.468926
Estrada DF, Skinner AL, Laurence JS, Scott EE (2014) Human cytochrome P450 17A1 conformational selection: modulation by ligand and cytochrome b5. J Biol Chem 289:14310–14320. https://doi.org/10.1074/jbc.M114.560144
Auchus RJ, Lee TC, Miller WL (1998) Cytochrome b5 augments the 17,20-lyase activity of human P450c17 without direct electron transfer. J Biol Chem 273:3158–3165. https://doi.org/10.1074/jbc.273.6.3158
Kok RC, Timmerman MA, Wolffenbuttel KP, Drop SL, de Jong FH (2010) Isolated 17,20-lyase deficiency due to the cytochrome b5 mutation W27X. J Clin Endocrinol Metab 95:994–999. https://doi.org/10.1210/jc.2008-1745
Malikova J, Brixius-Anderko S, Udhane SS, Parween S, Dick B, Bernhardt R, Pandey AV (2017) CYP17A1 inhibitor abiraterone, an anti-prostate cancer drug, also inhibits the 21-hydroxylase activity of CYP21A2. J Steroid Biochem Mol Biol 174:192–200. https://doi.org/10.1016/j.jsbmb.2017.09.007
Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, Meyer-Bahlburg HF, Miller WL, Montori VM, Oberfield SE, Ritzen M, White PC (2010) Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 95:4133–4160. https://doi.org/10.1210/jc.2009-2631
Fehl C, Vogt CD, Yadav R, Li K, Scott EE, Aubé J (2018) Structure-based design of inhibitors with improved selectivity for steroidogenic cytochrome P450 17A1 over cytochrome P450 21A2. J Med Chem 61:4946–4960. https://doi.org/10.1021/acs.jmedchem.8b00419
Bhatnagar AS (2007) The discovery and mechanism of action of letrozole. Breast Cancer Res Treat 105(Suppl 1):7–17. https://doi.org/10.1007/s10549-007-9696-3
Ghosh D, Lo J, Morton D, Valette D, Xi J, Griswold J, Hubbell S, Egbuta C, Jiang W, An J, Davies HM (2012) Novel aromatase inhibitors by structure-guided design. J Med Chem 55:8464–8476. https://doi.org/10.1021/jm300930n
Evans TR, Di Salle E, Ornati G, Lassus M, Benedetti MS, Pianezzola E, Coombes RC (1992) Phase I and endocrine study of exemestane (FCE 24304), a new aromatase inhibitor, in postmenopausal women. Cancer Res 52:5933–5939
Lipton A, Demers LM, Harvey HA, Kambic KB, Grossberg H, Brady C, Adlercruetz H, Trunet PF, Santen RJ (1995) Letrozole (CGS 20267). A phase I study of a new potent oral aromatase inhibitor of breast cancer. Cancer 75:2132–2138. https://doi.org/10.1002/1097-0142(19950415)75:8%3c2132::aid-cncr2820750816%3e3.0.co;2-u
Plourde PV, Dyroff M, Dowsett M, Demers L, Yates R, Webster A (1995) ARIMIDEX: a new oral, once-a-day aromatase inhibitor. J Steroid Biochem Mol Biol 53:175–179. https://doi.org/10.1016/0960-0760(95)00045-2
Mojaddami A, Sakhteman A, Fereidoonnezhad M, Faghih Z, Najdian A, Khabnadideh S, Sadeghpour H, Rezaei Z (2017) Binding mode of triazole derivatives as aromatase inhibitors based on docking, protein ligand interaction fingerprinting, and molecular dynamics simulation studies. Res Pharm Sci 12:21–30. https://doi.org/10.4103/1735-5362.199043
Simpson ER (2003) Sources of estrogen and their importance. J Steroid Biochem Mol Biol 86:225–230. https://doi.org/10.1016/s0960-0760(03)00360-1
Sasano H, Uzuki M, Sawai T, Nagura H, Matsunaga G, Kashimoto O, Harada N (1997) Aromatase in human bone tissue. J Bone Miner Res 12:1416–1423. https://doi.org/10.1359/jbmr.1997.12.9.1416
Khosla S, Oursler MJ, Monroe DG (2012) Estrogen and the skeleton. Trends Endocrinol Metab 23:576–581. https://doi.org/10.1016/j.tem.2012.03.008
Cheung AM, Tile L, Cardew S, Pruthi S, Robbins J, Tomlinson G, Kapral MK, Khosla S, Majumdar S, Erlandson M, Scher J, Hu H, Demaras A, Lickley L, Bordeleau L, Elser C, Ingle J, Richardson H, Goss PE (2012) Bone density and structure in healthy postmenopausal women treated with exemestane for the primary prevention of breast cancer: a nested substudy of the MAP.3 randomised controlled trial. Lancet Oncol 13:275–284. https://doi.org/10.1016/s1470-2045(11)70389-8
Perez EA, Josse RG, Pritchard KI, Ingle JN, Martino S, Findlay BP, Shenkier TN, Tozer RG, Palmer MJ, Shepherd LE, Liu S, Tu D, Goss PE (2006) Effect of letrozole versus placebo on bone mineral density in women with primary breast cancer completing 5 or more years of adjuvant tamoxifen: a companion study to NCIC CTG MA.17. J Clin Oncol 24:3629–3635. https://doi.org/10.1200/jco.2005.05.4882
Eastell R, Adams JE, Coleman RE, Howell A, Hannon RA, Cuzick J, Mackey JR, Beckmann MW, Clack G (2008) Effect of anastrozole on bone mineral density: 5-year results from the anastrozole, tamoxifen, alone or in combination trial 18233230. J Clin Oncol 26:1051–1057. https://doi.org/10.1200/jco.2007.11.0726
Pivonello R, Fleseriu M, Newell-Price J, Bertagna X, Findling J, Shimatsu A, Gu F, Auchus R, Leelawattana R, Lee EJ, Kim JH, Lacroix A, Laplanche A, O’Connell P, Tauchmanova L, Pedroncelli AM, Biller BMK (2020) Efficacy and safety of osilodrostat in patients with Cushing’s disease (LINC 3): a multicentre phase III study with a double-blind, randomised withdrawal phase. Lancet Diabetes Endocrinol 8:748–761. https://doi.org/10.1016/s2213-8587(20)30240-0
Fleseriu M, Pivonello R, Elenkova A, Salvatori R, Auchus RJ, Feelders RA, Geer EB, Greenman Y, Witek P, Cohen F, Biller BMK (2019) Efficacy and safety of levoketoconazole in the treatment of endogenous Cushing’s syndrome (SONICS): a phase 3, multicentre, open-label, single-arm trial. Lancet Diabetes Endocrinol 7:855–865. https://doi.org/10.1016/s2213-8587(19)30313-4
Valentín-Goyco J, Liu J, Peng HM, Oommen J, Auchus RJ (2023) Selectivity of osilodrostat as an inhibitor of human steroidogenic cytochromes P450. J Steroid Biochem Mol Biol 231:106316. https://doi.org/10.1016/j.jsbmb.2023.106316
Bogman K, Schwab D, Delporte ML, Palermo G, Amrein K, Mohr S, De Vera Mudry MC, Brown MJ, Ferber P (2017) Preclinical and early clinical profile of a highly selective and potent oral inhibitor of aldosterone synthase (CYP11B2). Hypertension 69:189–196. https://doi.org/10.1161/hypertensionaha.116.07716
Freeman MW, Halvorsen YD, Marshall W, Pater M, Isaacsohn J, Pearce C, Murphy B, Alp N, Srivastava A, Bhatt DL, Brown MJ (2023) Phase 2 trial of baxdrostat for treatment-resistant hypertension. N Engl J Med 388:395–405. https://doi.org/10.1056/NEJMoa2213169
Laffin LJ, Rodman D, Luther JM, Vaidya A, Weir MR, Rajicic N, Slingsby BT, Nissen SE (2023) Aldosterone synthase inhibition with lorundrostat for uncontrolled hypertension: the target-HTN randomized clinical trial. JAMA 330:1140–1150. https://doi.org/10.1001/jama.2023.16029
Amaral C, Varela C, Azevedo M, da Silva ET, Roleira FM, Chen S, Correia-da-Silva G, Teixeira N (2013) Effects of steroidal aromatase inhibitors on sensitive and resistant breast cancer cells: aromatase inhibition and autophagy. J Steroid Biochem Mol Biol 135:51–59. https://doi.org/10.1016/j.jsbmb.2012.12.017
Lu Q, Liu Y, Long BJ, Grigoryev D, Gimbel M, Brodie A (1999) The effect of combining aromatase inhibitors with antiestrogens on tumor growth in a nude mouse model for breast cancer. Breast Cancer Res Treat 57:183–192. https://doi.org/10.1023/a:1006225601046
Creemers SG, Feelders RA, de Jong FH, Franssen GJH, de Rijke YB, van Koetsveld PM, Hofland LJ (2019) Osilodrostat is a potential novel steroidogenesis inhibitor for the treatment of cushing syndrome: an in vitro study. J Clin Endocrinol Metab 104:3437–3449. https://doi.org/10.1210/jc.2019-00217
Creemers SG, Feelders RA, de Jong FH, Franssen GJH, de Rijke YB, van Koetsveld PM, Hofland LJ (2021) Levoketoconazole, the 2S,4R enantiomer of ketoconazole, a new steroidogenesis inhibitor for cushing’s syndrome treatment. J Clin Endocrinol Metab 106:e1618–e1630. https://doi.org/10.1210/clinem/dgaa989
Funding
The authors have not disclosed any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest regarding the content of this article.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kim, C., Jeong, E., Lee, Yb. et al. Steroidogenic cytochrome P450 enzymes as drug target. Toxicol Res. 40, 325–333 (2024). https://doi.org/10.1007/s43188-024-00237-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43188-024-00237-0