
Key summary points
To identify risk factors for falling among acutely ill older patients aged ≥ 80 years, during hospitalization in acute geriatric ward.
AbstractSection FindingsThe strongest predictors of falling during hospitalization were dementia, CHF, hypertension and delirium.
AbstractSection MessageDetection of patients who are likely to fall during hospitalization, might enable the staff to better target hospital fall prevention and plan effective prevention strategies.
Abstract
Purpose
The study aims to identify risk factors for falling among acutely ill older patients, hospitalized in acute geriatric ward.
Methods
A retrospective study of 260 cases of patients who had fallen and 439 controls was conducted in a geriatric ward. We retrieved from the electronic hospital records data including patient demographics, medical diagnoses, and laboratory results, and drugs taken prior to the fall were reviewed. In addition, data on functional and cognitive status were recorded. Admission Morse Falls Scale for every patient was also retrieved.
Results
The following on-admission diagnoses were associated with a higher incidence of falls during hospitalization: hypertension (84% vs. 38%), congestive heart failure (CHF), 74% vs 16%, dementia (36% vs. 5%), and delirium (36% vs 5%). A higher percentage of fallers compared to controls consumed beta blockers (69% vs. 53%), benzodiazepines (46% vs. 32%), antidepressants (33% vs. 23%), oral diabetes drugs (20% vs. 11%) and opiates (8% vs. 4%). On-admission Morse Falls Scale score was found to be higher in the patients who fell (59 vs.53). The strongest predictors of falling during hospitalization were CHF, hypertension, dementia, delirium, assisted mobility and dependence.
Conclusion
A systematic screening of risk factors for falls and identification of them might contribute to reducing the risk associated with falls during hospitalization.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hospitalized patient falls are a worldwide problem. Hospitalization itself increases the risk of falls [1]. An acutely ill older person, hospitalized at an acute care facility, is at a higher risk of falling, both due to an increase in intrinsic factors, including acute illness and drugs used, and extrinsic factors in the hospital environment [2]. Patients find themselves in a strange environment, are ill, and undergoing a number of medical interventions, all of which increase the probability of a fall. Older patients over 65 years are a particularly vulnerable group, and have three times higher risk of falls in a hospital than in their home environment [1]. The complex interaction between individual vulnerabilities and those added by the hospital environment makes identification of a single, definitive causal link almost impossible [3].
Falls can be influenced by multiple factors [4]. The most consistently identified risk factors for falls in hospitalized patients are quite similar to those observed in community studies, including advanced age (> 85 years), male sex, a recent fall, gait instability, agitation and/or confusion, adverse drug reactions and neuro-cardiovascular instability (most notably orthostatic hypotension) [5].
Other risk factors for in-hospital falls, which were found, are arthritis, depression, visual disturbances, use of four or more drugs, hypoglycemia, Vitamin D deficiency, dementia, delirium, and time of day [3, 6,7,8].
Falls are the most commonly reported patient safety incident in the acute hospital setting, constituting up to 70% of inpatient accidents [2, 5, 9].
Risk of falls for hospitalized patients is monitored by scoring tools, such as the Morse Falls Scale (MFS) [10, 11], Falls Risk Assessment Tool (FRAT) and St. Thomas’s Risk Assessment Tool in Falling Elderly Inpatients (STRATIFY) [12]. The use of such scales allows the staff to prioritize at risk population in terms of placement, surveillance and physical therapy.
Common consequences of falls are serious physical and emotional injury, poor quality of life, increased length of hospital stay, discharge to a long-term care facility, increased health care cost [1, 2, 13], fear of further falls and delayed functional recovery [5]. Approximately 30% of hospital patient falls result in physical injury, with 4–6% causing serious injury, such as fractures, subdural hematomas, and even patient death [2, 5].
Although falls have been relatively well studied in community and nursing home settings, less is known about the epidemiology of falls in the hospital setting [2]. Previous studies suggested that 3–20% of hospitalized patients fall at least once during their stay [2, 14].
Studies aiming to identify risk factors of falls in hospitalized older patients have been conducted in different clinical settings, so that the results are comparable only to some extent. Most previous reports concerning falls in hospitals have been in rehabilitation wards. An understanding of the incidence and characteristics of falls in acute care wards is important for prevention of falls [15]. However, literature regarding specific risk factors associated with falls among oldest-old patients in acute geriatric departments is lacking. Thus, we retrospectively examined the characteristics of falls among oldest-old adults (aged ≥ 80 years old) hospitalized in acute geriatric ward. To our best knowledge very few studies focused on this age group of patients.
Methods
We conducted a retrospective study of falling cases in a large community-based hospital. We included patients aged ≥ 80 years, admitted between the years January 2012 and December 2017 from the emergency room to the acute geriatric ward at the Kaplan Medical Center (general hospital), Rehovot, Israel. The acute geriatric ward admits only patients from the emergency ward. This department is a unique facility providing acute care to patients 80 years old and above, suffering from a wide variety of acute medical conditions. The department has 36 beds and a high turnover (average stay length of less than 6 days). The department’s staff is utilizing the MFS in trying to identify patients at risk for fall.
Every fall event of any hospitalized patient in the geriatric ward is recorded on a fall report (a special dedicated form), regardless of whether it results in a harm to a patient or not. A fall is defined as an involuntary change of posture whereby a patient is ending up lying on the floor. The incident report is filled by the nurse in charge of the patient, and completed by a medical report filled by one of the department’s physicians after a physical examination of the patient.
A total of 260 cases of patients who had fallen were detected through the fall reports. A control group of 439 patients, who had not fallen, was selected randomly from a list of all the patients hospitalized in our department at the same time, excluding patients included in the study group.
We retrieved from the electronic hospital records data, including patient demographics, medical diagnoses and laboratory results. Records of drugs given prior to the fall were reviewed and divided into main pharmacological classes for every patient by a senior physician. The following drug types were retrieved: calcium blockers, β-blockers, ACE inhibitors, antidiabetics, anti-depressants, benzodiazepines, neuroleptics, antiaggregants, anticoagulants and diuretics. In addition, data on functional and cognitive status were also recorded. Admission MFS [10] score for every patient was also retrieved.
The study was approved by the Institutional Ethics Committee of the Kaplan Medical Center, Rehovot, Israel.
Statistical analysis
Data were analyzed using SPSS 25 software. Data are presented as means ± standard deviations or percentages. Continuous variables between the various study groups were tested for normality by Shapiro–Wilk test and when normal distribution was found, t-test was performed. Pearson Chi-Square Test was used for the relationship between two categorical variables. To model the probability of falls, logistic regression was used. P value < 0.05 was considered statistically significant.
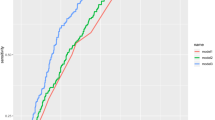
Two logistic regression models were done. The first included, as predictor variables, the MFS score, gender, age, hospital mortality, mobility and number of background conditions (model 1). In the presented model in the study (model 2) instead of the number of background conditions, we included the specific conditions found to have significant impact on the risk of falling. The model discrimination was evaluated with C-statistics, calculated from the ROC curve of the predicted probabilities of falls by model 1 and model 2. By ROC analysis, the model discrimination was high, with C-statistics of 0.94 (0.92–0.92), p value < 0.0001.
Results
Over the study period, approximately 3.5 falls for every 1000 patient days were recorded.
The selected characteristics of the 260 older patients (128 females, about 40%) and 439 controls (280 females, about 64%) are presented in Table 1. The mean age in both groups of patients was about 87 years. The percentage of men in the fallers group was significantly higher than in the controls. Among the fallers, overall hospital stay was longer (8 days vs 6 days), and mortality within a year of admission was higher (9% vs. 7.5%).
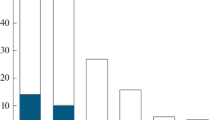
The number of comorbidities found on admission was higher in the fallers. The following on-admission diagnoses were associated with a higher incidence of falls: hypertension (84% vs. 38%), congestive heart failure (CHF), 74% vs. 16%, dementia (36% vs. 5%), and delirium (36% vs. 5%). Chronic obstructive pulmonary disease (COPD) was related to reduced incidence of falls (19% vs. 41%). A higher proportion of fallers compared to controls consumed beta blockers (69% vs. 53%), benzodiazepines (46% vs. 32%), antidepressants (33% vs. 23%), antipsychotics (22% vs. 15%), oral antidiabetics (20% vs. 11%) and opiates (8% vs. 4%). Z-drugs were also found to be associated with increased risk of falling, but were not included in the table due to small sample size, about 20 patients (data not shown). A lower percentage of fallers compared to controls used low molecular weight heparin (2.3% vs. 11.6%), direct oral anticoagulants (DOACs), 2% vs.8%, antiaggregants (8.5% vs. 37%), and corticosteroids (8% vs. 14%). Among the patients who fell there was a smaller percentage of smokers (15% vs. 84%). On-admission MFS score was found to be higher in the patients who fell (59 vs.53).
The incidence of falls was significantly higher (46.7%) during the night shift (from 23:00 to 07:00) (p = 0.0005) than on other shifts [morning (34.1%) and evening (19.2%)]. Weekends were not found to be significantly different in fall incidence from the other weekdays. Of the 260 fallers, 15 (5.8%) had a significant documented injury due to the fall (data not shown).
Multiple logistic regression analysis (Table 2) found that among comorbidities, the strongest predictors of falling during hospitalization were CHF, hypertension, dementia and delirium. Compared to independent patients, assisted patients with mobility and dependent patients were at higher risk for in-hospital falling, assisted patients being by 13.3 higher risk than the independent. The independent risk factors (CHF, hypertension, dementia, delirium,, assisted mobility and dependence) explain 72% (R2 = 0.720) of the difference in risk factors for in-hospital falling between the fallers and the controls.
Discussion
Our study focuses on falls in the oldest-old patients hospitalized in acute geriatric ward. The rates of falls among patients older than 80 are higher than among younger hospitalized adults [3]. The highest fall rates, with up to 11.7 falls per 1000 patient days, occur in geriatric departments [16]. During our study period, approximately 3.5 falls for every 1000 patient days were recorded. Falls rates in US hospitals range from 3.3 to 11.5 falls per 1000 patient days [17, 18].
The percentage of men in the fallers group was significantly higher, like in some other studies [13, 19]. However, there is no consensus in the literature on the association between gender and an increased risk for falls in hospitalized older patients [19]. Remor et al. has not found a difference in falls between genders [20]. However, in a Brazilian study, female subjects had twice as high a chance of being classified as having a high fall risk when compared to males [21].
Inpatient falls are the most commonly reported adverse hospital event and are associated with an increase in length of stay [13]. In the presented study, hospital stay was longer in the fallers than in the control patients, similarly to the findings of other studies [22,23,24].
During the first year after discharge from the hospital, the mortality rate, in our study, was higher among the fallers than among the non-fallers. To our best knowledge no study has focused on this outcome.
Typically, the times of the day, week, and year of the fall occurrence are not explored when investigating the epidemiology and etiology of hospital falls or when designing or evaluating preventive strategies and programs [25]. The most common time of falls was on the night shift, probably due to the combined impact of sundowning, dim lighting and reduced nursing staff. Falls occurrence at night is well-documented [15, 26].
In our study, like in two other studies [20, 27], the MFS score was higher among the fallers, but this tool was not found to be an independent risk factor for falling. The identified tools for predicting falls risk do not demonstrate predictive values as high as needed for identifying older inpatients at risk for falls [28]. It is difficult to predict with high predictive accuracy which patients are at risk of falls, because falls in the older individuals result from complex multifactorial etiologies [9].
A meta-analysis that had examined different tools for predicting falls risk, did not identify any tool which had an optimal balance between sensitivity and specificity, or which were clearly better than a simple clinical judgment of risk of falling [12]. NICE guidelines do not recommend the use of fall risk prediction tools to predict inpatients’ risk of falling in hospital [29].
Fallers, in our study, suffered from a quite high number of comorbidities. Multiple logistic regression analysis found that among comorbidities the strongest predictors of falling during hospitalization were CHF, hypertension dementia and. Delirium. Patients with comorbid CHF had an elevated risk of falls, as found by some other studies [30, 31]. Fall rates in heart failure (HF) patients are higher than average fall rates in older adults. Some studies reported that patients with HF had gray matter and axons alteration in sites of the brain, which may affect gait and balance. Also, heart failure patients receive multiple medications, that predispose them to falls [31].
In our study, patients, who suffered, from hypertension had about 10 times higher risk of falling during hospitalization. In a Brazilian study the patients with hypertension had a higher risk by about 38% of falling, but the Brazilian patients were younger than our patients, and only about 45% of them were older than 60 years [32]. Hypertension affects postural balance control in older adults unfavorably, which may result in falling [33]. The rapid changes in blood pressure seen in hypertension and the subsequent sudden reductions in blood flow can interfere with the mechanisms for controlling postural balance [34]. With increasing age, sensory and motor control of postural balance is often affected. Postural balance maintenance is one of the most important abilities required for the prevention of falls in the older population [33].
Hypertension in our study patients was primarily treated with either beta blockers, or calcium channel blockers, or ACE inhibitors, but only beta-blockers were associated with falls, and patients using beta blockers had a higher risk of falling. Beta-blockers due to their negative inotropic and chronotropic effect, may interfere with the compensatory responses to standing and predispose to an orthostatic blood pressure fall [35]. Multiple studies have reported central nervous system (CNS) side effects associated with use of beta-blockers, such as psychiatric conditions, sleep disturbances, delirium, psychosis, and visual hallucinations. The risk of beta-blocker CNS side effects is directly associated with the lipophilic properties of some beta-blockers (such as propranolol), which allow them to rapidly penetrate the blood–brain barrier [36].
Falls might also be an adverse effect of orthostatic hypotension (OH) caused by some other drugs. In the present study, a higher percentage of fallers compared to controls consumed benzodiazepines, antidepressants, antipsychotics and opiates. Correspondingly to the finding of Aryee et al. [13], psychotropic drugs, in our study, were associated with a higher risk of falling. It is well known that psychotropic drugs, like antipsychotics, antidepressants and benzodiazepines, that affect the CNS, may by themselves increase the risk of specific geriatric syndromes, including delirium and falls [37].
Benzodiazepines constitute the most frequently prescribed psychotropic medication class and are used as anxiolytics, sedatives, hypnotics, anticonvulsants, and skeletal muscle relaxants [38]. In our study, benzodiazepines were associated with a higher risk of falling. Several studies reported a significantly increased risk of falls by both short and long-acting benzodiazepines [16, 27, 38]. Long-term benzodiazepine use has been also associated with cognitive impairment, dependence, and withdrawal symptoms, which contribute to falls. American Geriatrics Society recommends avoiding benzodiazepines in older patients with a history or risk of falls, since these agents can cause ataxia, impaired psychomotor function, and syncope [38]. Z-drugs are sometimes considered to be advantageous compared with benzodiazepines, particularly concerning the development of tolerance and dependence, but several studies have reported similar adverse effects. Like benzodiazepines, Z-drugs have an impact on cognition, balance, and coordination—as main reasons for falls [16].
In our study, falls were associated with antipsychotic consumption. In Israel, the most used antipsychotic drugs in older patients are quetiapine and risperdone. Orthostatic hypotension, which might contribute to falls, develops in up to 40% of patients taking antipsychotics, with a higher incidence at advanced age [35]. Antipsychotic drugs have significant movement-related side effects, including ataxia and bradykinesia, which could lead to imbalance, inability to compensate, and falls [13]. Older people on psychotropic medications should have their medication reviewed, with specialist input if appropriate, and discontinued, if possible, to reduce their risk of falling [29].
In the present study, patients treated with antidepressants had a higher risk of falling than the controls. In Israel, the most used antidepressant drugs in older patients are escitalopram, mirtazapine and venlafaxine. Antidepressants have long been recognized as a contributory factor to falls, and many studies show an association between antidepressants and falls [39]. Antidepressants are thought to contribute to falls through several different mechanisms, including OH, hyponatremia, sedation and impaired reaction times and impaired balance [16, 39].
Our study patients treated with opiates were at higher risk of falling. Although there are few studies dealing with opiates and falls, opioids may be associated with increased risk of geriatric syndromes, including delirium, and can increase the risk of falls [37, 39, 40].
Similarly, to the findings of other studies [9, 24], our results showed that dementia was associated with the occurrence of falls and was an independent risk factor for falling. The information on the impact of dementia on falling among hospitalized older patients is scarce. Some studies did not find association between dementia and falls [1, 16]. Some other studies have suggested that dementia may adversely influence clinical outcomes in hospitalized patients [24]. Different types of cognitive impairment associated with problems in executive or visuospatial functions as well as apraxia, might explain increased risk of falling [41]
In our study, correspondingly to the Wedmann et al. finding [16], delirium was strongly associated with falls and was an independent risk factor for falling. Patients with more significant predisposing factors require fewer noxious insults to develop delirium, and vice versa. Known predisposing risk factors for delirium include dementia, functional impairment, sensory (visual and/or hearing) deprivation, depression, age over 75 years, and severity of comorbidities [42]. Hospital environment and the acute illness contribute to the development of delirium. Effective prevention strategies significantly reduced the risk of incident delirium by 53% and the risk of falls by 62% among hospitalized patients 65 years and older [43].
Other independent risk factors for falling in the presented study were assisted mobility and dependence. The risk of falling in patients with assisted mobility was higher than in independent patients. Walking aid is an indicator of impaired mobility most likely explaining the risk. Walkers are generally used to improve balance and mobility of older persons and to protect those persons from falling [44]. But, occasionally, like in our study, they may be associated with greater fall risk, because they can interfere with a person’s balance control [45]. Though dependence, as a risk factor for falling, was lower than that of patients with assisted mobility, yet it was about six times higher than that of the independent patients. Obviously, dependent patients almost do not walk, therefore their risk of falling is lower than that of patients with assisted mobility, but higher than that of independent patients, because there might be other causes of falling than walking.
Our study has all the disadvantages of a retrospective observational study. We did not have all the details that may have had an impact on falls in the oldest-old during hospitalization, because they were not found in the patients’ electronic data. Consequently, the independent variables—CHF, hypertension, dementia, delirium, assisted mobility and dependence—do not explain all of the risk factors for falls in hospitalized oldest-old patients, though a relatively high part of them they do explain (72%).
Our study strength lies in its population relatively large size. Since the study focuses on the risk factors for falls in the oldest-old patients in acute geriatric ward, we must point out that we have contributed to the medical knowledge regarding this population of inpatients, whose proportion in the geriatric population is recently significantly increasing.
Conclusion
The independent risk factors—comorbid CHF, hypertension, dementia, delirium and frailty and dependence—predicted falls in the oldest-old inpatients hospitalized in acute geriatric ward. It appears that comorbidities and functional status are the most predictive risk factors for falls. This fits well with the concept of frailty as a risk factor for many adverse outcomes. Putting attention on these frequent risk factors and medication often associated with them, might help us target intervention better and thus hopefully prevent more in-hospital falls.
Code availability
Not applicable.
References
Brabcová I, Hajduchová H, Tóthová V, Bártlová S, Filka J, Doseděl M et al (2019) Selected risk factors of falls in hospitalized patients: a case-control study. Neuro Endocrinol Lett 39:481–488
Anderson DC, Postler TS, Dam TT (2016) Epidemiology of hospital system patient falls: a retrospective analysis. Am J Med Qual 31:423–428. https://doi.org/10.1177/1062860615581199
Sillner AY, Holle CL, Rudolph JL (2019) The overlap between falls and delirium in hospitalized older adults: a systematic review. Clin Geriatr Med 35:221–236. https://doi.org/10.1016/j.cger.2019.01.004
Kalache A, Fu D, Yoshida S, Al-Faisal W, Beattie L, Chodzko-Zajko W, et al (2007) Ageing, Department Of (Ed.) & Course, Life (Ed.). World Health Organization global report on falls prevention in older age. Geneva. http://www.who.int/ageing/publications/Falls_prevention7March.pdf: World Health Organization, 2007. Geneva: WHO
Morris R, O’Riordan S (2017) Prevention of falls in hospital. Clin Med 17:360–362. https://doi.org/10.7861/clinmedicine.17-4-360
Uusi-Rasi K, Patil R, Karinkanta S, Tokola K, Kannus P, Lamberg-Allardt C et al (2019) Serum 25-hydroxyvitamin D levels and incident falls in older women. Osteoporos Int 30:93–101. https://doi.org/10.1007/s00198-018-4705-4
Berra C, De Fazio F, Azzolini E, Albini M, Zangrandi F, Mirani M et al (2019) Hypoglycemia and hyperglycemia are risk factors for falls in the hospital population. Acta Diabetol 56:931–938. https://doi.org/10.1007/s00592-019-01323-8
López-Soto PJ, Smolensky MH, Sackett-Lundeen LL, De Giorgi A, Rodríguez-Borrego MA, Manfredini R et al (2016) Temporal patterns of in-hospital falls of elderly patients. Nurs Res 65:435–445. https://doi.org/10.1097/NNR.0000000000000184
Beauchet O, Noublanche F, Simon R, Sekhon H, Chabot J, Levinoff EJ et al (2018) Falls risk prediction for older inpatients in acute care medical wards: is there an interest to combine an early nurse assessment and the artificial neural network analysis? J Nutr Health Aging 22:131–137. https://doi.org/10.1007/s12603-017-0950-z
Baek S, Piao J, Jin Y, Lee SM (2014) Validity of the Morse Fall Scale implemented in an electronic medical record system. J Clin Nurs 23:2434–2440. https://doi.org/10.1111/jocn.12359
Gringauz I, Shemesh Y, Dagan A, Israelov I, Feldman D, Pelz-Sinvani N et al (2017) Risk of falling among hospitalized patients with high modified Morse scores could be further Stratified. BMC Health Serv Res 17:721. https://doi.org/10.1186/s12913-017-2685-2
da Costa BR, Rutjes AW, Mendy A, Freund-Heritage R, Vieira ER (2012) Can falls risk prediction tools correctly identify fall-prone elderly rehabilitation inpatients? A systematic review and meta-analysis. PLoS ONE 7:e41061. https://doi.org/10.1371/journal.pone.0041061
Aryee E, James SL, Hunt GM, Ryder HF (2017) Identifying protective and risk factors for injurious falls in patients hospitalized for acute care: a retrospective case-control study. BMC Geriatr 17:260. https://doi.org/10.1186/s12877-017-0627-9
Chiu MH, Lee HD, Hwang HF, Wang SC, Lin MR (2015) Medication use and fall-risk assessment for falls in an acute care hospital. Geriatr Gerontol Int 15:856–863. https://doi.org/10.1111/ggi.12359
Sato N, Hase N, Osaka A, Sairyo K, Katoh S (2018) Falls among hospitalized patients in an acute care hospital: analyses of incident reports. J Med Invest 65:81–84. https://doi.org/10.2152/jmi.65.81
Wedmann F, Himmel W, Nau R (2019) Medication and medical diagnosis as risk factors for falls in older hospitalized patients. Eur J Clin Pharmacol 75:1117–1124. https://doi.org/10.1007/s00228-019-2668-3
Chelly JE, Conroy L, Miller G, Elliott MN, Horne JL, Hudson ME (2008) Risk factors and injury associated with falls in elderly hospitalized patients in a community hospital. J Patient Saf 4:178–183. https://doi.org/10.1097/PTS.0b013e3181841802
Bouldin ELD, Andresen EM, Dunton NE, Simon M, Waters TM, Liu M et al (2013) Falls among adult patients hospitalized in the United States. J Patient Saf 1:13–17. https://doi.org/10.1097/pts.0b013e3182699b64
Severo IM, Kuchenbecker RS, Vieira DFVB, Lucena AF, Almeida MA (2018) Risk factors for fall occurrence in hospitalized adult patients: a case-control study. Rev Lat Am Enfermagem 26:e3016. https://doi.org/10.1590/1518-8345.2460.3016
Remor CP, Cruz CB, Urbanetto JS (2014) Análise dos fatores de risco para queda de adultos nas primeiras 48 horas de hospitalização [Analysis of fall risk factors in adults within the first 48 hours of hospitalization]. Rev Gaucha Enferm 35:28–34. https://doi.org/10.1590/1983-1447.2014.04.50716
Silva AKM, Costa DCMD, Reis AMM (2019) Risk factors associated with in-hospital falls reported to the Patient Safety Committee of a teaching hospital. Einstein (Sao Paulo) 17:eAO4432. https://doi.org/10.31744/einstein_journal/2019AO4432
Gettens S, Fulbrook P (2015) Fear of falling: association between the Modified Falls Efficacy Scale, in-hospital falls and hospital length of stay. J Eval Clin Pract 21:43–50. https://doi.org/10.1111/jep.12226
Bates DW, Pruess K, Souney P, Platt R (1995) Serious falls in hospitalized patients: correlates and resource utilization. Am J Med 99:137–143. https://doi.org/10.1016/s0002-9343(99)80133-8
Li F, Wang F, Jia J (2013) Evaluating the prevalence of dementia in hospitalized older adults and effects of comorbid dementia on patients’ hospital course. Aging Clin Exp Res 25:393–401. https://doi.org/10.1007/s40520-013-0068-z
López-Soto PJ, Manfredini R, Smolensky MH, Rodríguez-Borrego MA (2015) 24-hour pattern of falls in hospitalized and long-term care institutionalized elderly persons: a systematic review of the published literature. Chronobiol Int 32:548–556. https://doi.org/10.3109/07420528.2014.987295
Barbosa AS, Chaves EHB, Ribeiro RG, Quadros DV, Suzuki LM, Magalhaes AMM (2019) Characterization of the adult patients’ falling incidents in a university hospital. Rev Gaucha Enferm 40(esp):e20180303. https://doi.org/10.1590/1983-1447.2019.20180303
Noh HM, Song HJ, Park YS, Han J, Roh YK (2021) Fall predictors beyond fall risk assessment tool items for acute hospitalized older adults: a matched case–control study. Sci Rep 11:1–9. https://doi.org/10.1038/s41598-021-81034-9
Matarese M, Ivziku D, Bartolozzi F, Piredda M, De Marinis MG (2015) Systematic review of fall risk screening tools for older patients in acute hospitals. J Adv Nurs 71:1198–1209. https://doi.org/10.1111/jan.12542
National Institute for Health and Care Excellence. Falls in older people: assessing risk and prevention. Clinical guidline [CG161] (2013). https://www.nice.org.uk/guidance/cg161/chapter/Key-priorities-for-implementation#preventing-falls-in-older-people-during-a-hospital-stay
Manemann SM, Chamberlain AM, Boyd CM, Miller DM, Poe KL, Cheville A, Weston SA, Koepsell EE, Jiang R, Roger VL (2018) Fall risk and outcomes among patients hospitalized with cardiovascular disease in the community. Circ Cardiovasc Qual Outcomes 11:e004199. https://doi.org/10.1161/CIRCOUTCOMES.117.004199
Lee K, Pressler SJ, Titler M (2016) Falls in patients with heart failure: a systematic review. J Cardiovasc Nurs 31:555–561. https://doi.org/10.1097/JCN.0000000000000292
Bittencourt VLL, Graube SL, Stumm EMF, Battisti IDE, Loro MM, Winkelmann ER (2017) Factors associated with the risk of falls in hospitalized adult patients. Rev Esc Enferm USP 51:e03237. https://doi.org/10.1590/s1980-220x2016037403237
Acar S, Demırbüken İ, Algun C, Malkoç M, Tekın N (2015) Is hypertension a risk factor for poor balance control in elderly adults? J Phys Ther Sci 27:901–904. https://doi.org/10.1589/jpts.27.901
Abate M, Di Iorio A, Pini B et al (2009) Effects of hypertension on balance assessed by computerized posturography in the elderly. Arch Gerontol Geriatr 49:113–117
Rivasi G, Rafanelli M, Mossello E, Brignole M, Ungar A (2020) Drug-related orthostatic hypotension: beyond anti-hypertensive medications. Drugs Aging 37:725–738. https://doi.org/10.1007/s40266-020-00796-5
Shah R, Babar A, Patel A, Dortonne R, Jordan J (2020) Metoprolol-associated central nervous system complications. Cureus 22(12):e8236. https://doi.org/10.7759/cureus.8236
Peron EP, Gray SL, Hanlon JT (2011) Medication use and functional status decline in older adults: a narrative review. Am J Geriatr Pharmacother 9:378–391. https://doi.org/10.1016/j.amjopharm.2011.10.002
Picton JD, Marino AB, Nealy KL (2018) Benzodiazepine use and cognitive decline in the elderly. Am J Health Syst Pharm 75:e6–e12. https://doi.org/10.2146/ajhp160381
Darowski A, Chambers SA, Chambers DJ (2009) Antidepressants and falls in the elderly. Drugs Aging 26:381–394. https://doi.org/10.2165/00002512-200926050-00002
Zazzara MB, Palmer K, Vetrano DL, Carfì A, Graziano O (2021) Adverse drug reactions in older adults: a narrative review of the literature. Eur Geriatr Med 12:463–473. https://doi.org/10.1007/s41999-021-00481-9
Zhang W, Low LF, Schwenk M, Mills N, Gwynn JD, Clemson L (2019) Review of gait, cognition, and fall risks with implications for fall prevention in older adults with dementia. Dement Geriatr Cogn Disord 48:17–29. https://doi.org/10.1159/000504340
Rieck K, Pagali S, Miller DM (2020) Delirium in hospitalized older adults. Hosp Pract 48(sup1):3–16. https://doi.org/10.1080/21548331.2019.1709359
Oh ES, Fong TG, Hshieh TT, Inouye SK (2017) Delirium in older persons. Adv Diagn Treat JAMA 318:1161–1174. https://doi.org/10.1001/jama.2017.12067
Lindemann U, Schwenk M, Klenk J, Kessler M, Weyrich M, Kurz F et al (2016) Problems of older persons using a wheeled walker. Aging Clin Exp Res 28:215–220. https://doi.org/10.1007/s40520-015-0410-8
Bateni H, Heung E, Zettel J, McLlroy WE, Maki BE (2004) Can use of walkers or canes impede lateral compensatory stepping movements? Gait Posture 20:74–83. https://doi.org/10.1016/S0966-6362(03)00098-5
Acknowledgements
I would like to thank Felicia Stern, Ph.D., RD for her assistance in the preparation and editing of this manuscript.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
ST and GO each equally contributed to writing the manuscript. SJ retrieved the data from the electronic hospital health records.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
The study was approved by the Institutional Ethics Committee of the Kaplan Medical Center, Rehovot, Israel.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Oren, G., Jolkovsky, S. & Tal, S. Falls in oldest-old adults hospitalized in acute geriatric ward. Eur Geriatr Med 13, 859–866 (2022). https://doi.org/10.1007/s41999-022-00660-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41999-022-00660-2