
Abstract
Background
Wheeled walkers (WWs) are used to improve mobility and for fall prevention in older persons, but not all users are satisfied with the usability of WWs. Intelligent WWs are being developed to improve the usability.
Aims
The aim of this study was to support the development of intelligent WWs by investigating possible problems of using a WW.
Methods
This study investigated 22 geriatric in-patients (median age 82 years) with and without their WW while opening a door against the direction of walking and passing through. Other possible problems when using WWs were identified by interview.
Results
Walking through the door was faster without than with using the WW (8.71 versus 12.86 s, p < 0.001), while interference between door and WW was documented in 41 of 44 (93 %) cases. Backward walking performance was better when using a WW with regard to gait speed, step width and walk ratio (all p < 0.002). Most referred problems when using a WW were walking downhill (83 %) and uphill (77 %) and obstacle crossing in general (77 %).
Conclusions
Problems with opening a door against the direction of walking and the optimization of downhill and uphill walking as well as obstacle crossing should be regarded when developing an intelligent WW.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Physical performance, such as balance while walking or standing, decreases with age [1]. A wheeled walker (WW) is frequently used to improve balance and mobility of older persons [2, 3] and to protect those persons from falling [4]. However, those persons falling while using a WW are more likely to sustain a severe injury when falling, e.g., a hip fracture [5]. Furthermore, walking performance has been shown to decrease in a sub-population, i.e., Parkinson´s disease patients when using a WW [6]. In general, not all users are satisfied with the WW and usability and accessibility problems were identified as the main complaints [7]. With regard to accessibility, opening doors against the direction of walking and passing through is an obvious problem. In this situation, the interference of the WW with the door has to be managed while balance is challenged [8]. A side step could be an appropriate solution in this situation, but this has been shown to be associated with balance problems when using a walker, which has limited functionality for sideward movements [9]. To understand the effect of a WW on gait and balance an assessment of a daily activity, such as walking through a door, is recommended in combination with standard laboratory measures [10].
Another approach to prevent interference of the door with the WW is to walk backwards with the walking aid while opening the door. However, backwards navigation of most WWs is limited, due to fixed rear wheels. Only front wheels are 360° rotatable for convenient navigation. Backward walking without using an assistive device has been investigated in different cohorts of age and performance. A decrease in performance with age has been shown with more walking performance deficits in fallers than in non-fallers [11]. Although walking backwards with a WW seems to be a frequent daily activity of older persons with impaired walking performance. This phenomenon has not been investigated so far.
Today smart technology is able to improve usability of mechanical devices, such as a WW. Based on expert opinion and possible technical solutions, intelligent walkers are being developed focusing on obstacle avoiding, powered impulsion and navigation technology [12–14]. However, there was no identification of problems of the users in advance and there is no evidence that these technical solutions are relevant for older persons using a WW. Although smart walkers are probably the most studied aids in the field of robotic assistance designed for disabled individuals or persons at risk of disability, basic knowledge about how and where WWs are helpful or not is still lacking.
The aim of this study was to support the development of intelligent WWs by investigating possible problems of older adults while using a WW. We used typical real-life scenarios including walking through a door and walking backwards. We hypothesized that task difficulty increases when passing through a door while using a WW reflected by an increased ambulation time (versus without WW) and interferences between WW and door. Furthermore, we hypothesized that backward walking performance decreases while using a WW in comparison to walking without WW. The rationale for this hypothesis is that here the WW is not used according to the arrangement of the wheels. In addition, it was aimed to identify other possible problems when using a WW by conducting a semi-structured interview.
Methods
Subjects and design
For the experimental part of this cross-sectional study 22 patients (median age 82 years, inter-quartile range 79–86.3 years, 50 % men) were recruited from a geriatric rehabilitation clinic in the south–west of Germany. All participants used their own WWs with 4 wheels, of which the front wheels were 360° rotatable for navigation and the rear wheels were fixed. Most of the participants (n = 14; 64 %) were novice WW users and the mean duration of usage of the remaining participants (n = 8) was 33.1 months. They had to be able to walk forwards as well as backwards with and without the WW for at least 5 m. Exclusion criteria were unilateral functional impairment, such as stroke or recent hip replacement and inability to follow verbal instructions. The group is described in detail in Table 1. The study was approved by the ethical committee of the University of Tübingen. All participants gave written informed consent.
Outcome parameters and protocol
At a distance of 2.3 m, participants stood in front of a standard door without any automatic function and opening against the direction of walking. They were instructed to walk to the door, open it, walk through the door and close it all at their habitual pace. The task was performed with and without WW in random order. Time to perform this task was taken from a video and the faster of 2 trials was used as outcome parameter. The number of interferences between WW and door was recorded over all 44 trials. Interference was defined as an interruption of the opening of the door, caused by sideward or backward movement of the WW. Rating from video was performed by 2 independent investigators (UL, FK). After the experiment the participants were asked if passing through the door was easier with or without using the WW.
In addition, participants walked at their own pace forwards with their WW over an instrumented walkway (GAITRite®, CIR Systems, Haverton, USA) and thereafter they walked backwards with and without WW in random order. The mean of 2 trials was taken for analysis with gait speed, step width and walk ratio, i.e., step length divided by step frequency [15], as outcome parameters.
Descriptive parameters
Habitual gait speed (forward) and the number of sit-to-stand transfers over 30 s at maximum pace [16] were used as functional descriptive parameters. In the last named assessment the protocol was modified that the use of armrests was allowed. Furthermore, the older participants were screened for co-morbidities by questionnaire [17] in a standardized interview.
Statistics
Due to the small sample size median and inter-quartile range (IQR), as well as non-parametric tests (Wilcoxon rank-sum test) were used to describe parameters and differences between conditions, respectively. The significance level of all statistical procedures was set to α = 5 % (two-sided). All analyses were conducted using SPSS version 16 software (SPSS Inc., Chicago, IL, USA).
Interview
To identify possible problems when using a WW, a semi-structured interview was conducted with 60 patients (mean age 82.0 years, 67 % women) using a WW in the same geriatric rehabilitation clinic. The cohort included 29 (48 %) first-time users, starting usage during in-patient rehabilitation, and 31 (52 %) long-time users with a mean usage of 30 months. We asked if they ever had experienced a fall while using their WW. Problems were asked with regard to walking in different directions, indoors and outdoors, up- and downhill, in curves, through a door and on the spot, over obstacles and on uneven surface, and with regard to sitting on the WW and carrying things with the WW, using the WW during the sit-to-stand transfer and using the WW in different situations in the community, attending doctor’s appointment, visiting friends or using public transportation. An example of these questions is: “When you walk indoor with your WW, do you feel safe/the device is helpful or do you feel unconfident/the device is hindering?” If the participants opted unconfident/hindering, the question was “What is the problem?”
Results
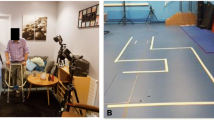
Walking through the door was faster without using the WW than with using the WW (8.71 s, IQR 7.81–10.19 versus 12.86 s, IQR 10.76–14.29; p < 0.001). Interference between door and WW was documented in 41 of 44 (93 %) cases with an example shown in Fig. 1. Directly after the experiment, 13 (59 %) older adults rated walking through the door without using the WW easier, for 6 patients (27 %) there was no difference and 3 patients (14 %) rated walking through the door with the use of their WW easier.

Interference of the wheeled walker with the door during opening against the direction of walking, showing not-rotatable back wheels (1), rotatable front wheels (2) and a back wheel with lost contact to the ground (3)
Walking forwards with the WW was performed faster, with smaller step width and with a higher walk ratio than walking backwards with WW. Walking backwards with WW was performed faster, with smaller step width and with a higher walk ratio than walking backwards without WW. With regard to walking performance, all differences between walking conditions were statistically significant (all p < 0.002) and are described in detail in Table 2.
Three out of 60 (5 %) patients had ever experienced a fall while using their WW. Walking downhill (83 %) and uphill (77 %) and walking outdoors over uneven ground (73 %) were major problems identified by interview in the cohort of 60 patients using a WW. Obstacle crossing in general was a problem for 77 % of all interviewed patients. Here, stairs in the context of public transportation (70 %), leaving/entering the own apartment (60 %) and doctors surgeries, visiting pharmacies etc. (35 %) were a common problem. Also, walking indoors (25 %) and outdoors (10 %) and carrying objects indoors (7 %) and outdoors (10 %) while crossing obstacles were further problems. Walking backwards with their WW was a problem for 27 % of the patients. The problems during walking and obstacle crossing are also shown in Fig. 2.

Problems of older in-patients (n = 60) during walking and problems with obstacles when using the wheeled walker
A further problem identified by interview were the not-rotatable back wheels which limited navigation during walking sidewards (32 %), walking through a door (25 %) and turning on the spot (15 %). With regard to using the WW during the sit-to-stand transfer, 83 % of all patients indicated not fixing the brakes as a major problem.
Discussion
This study identified serious problems when using a WW during more complex walking tasks such as passing a door. In contrast to straight walking, where no interference of the WW with the environment occurs, motor performance declined substantially during a complex mobility task requiring sideward shifting. On the same note, this study shows that a WW provides advantages during straight backwards walking. Previous studies found similar results for forward walking [2]. Our study results demonstrate pros and cons of using a WW by combining the assessment of a daily task and standard laboratory testing [10].
The longer time to walk through the door in our study is likely an indicator of interference between WW and door. Given a higher stability of walking performance when using a WW [2], a longer time would be acceptable, but the high number of interferences between WW and door points out the incident of instability while opening and passing through the door. Although our experimental result was confirmed by the 59 % of patients, who rated walking through the door to be easier without using a WW, the awareness of this problem was less than half and likely underestimated in our interviewed cohort. In our experiment, the impossibility of a movement with the WW to the side because of not-rotatable rear wheels is comparable to the challenging situation when using a walker without wheels [9]. One potential solution could be the implementation of smart technology. An intelligent WW, which may be able to recognize its interference with a door caused by, could release the fixation of its back wheels. This way, the WW could be moved to the side, but still provide assistance during walking in this balance challenging situation.
In our study, the decrease of walking performance during backward walking was documented by slower gait speed, broader step width and a smaller walk ratio, which is associated with falls risk during forward walking [18]. Decreases in gait speed and step width are in line with another study with a cohort of 62 older adults showing a 68 % faster backward walking gait speed, but walking without an assistive device [11]. The limitation of visual control while walking backwards may have caused these changes in performance, which then can be regarded as a necessary adaptation. Since the difference between forwards and backwards walking performance is considerable in our study and in another study without using an assistive device [11], the calculation of a forward/backward performance ratio with and without WW may be helpful for assessment of walking performance in older adults.
The use of the WW while walking backwards improved walking performance, which is in line with the literature based on forward walking [2]. Findings are contradictory to our hypothesis. We expected that the WW would interfere with the subjects´ ability to ambulate backwards due to the reverse arrangement of the wheels. However, our results show that gait performance was better during backwards walking with WW reflected by a higher velocity and walk ratio and reduced step with as compared to waling without WW. Furthermore, our results indicate an overestimation of problems during backward walking in our interview cohort.
The results of our interview-based identification of problems when using a WW, which are partly confirmed by the result of our experimental study, may help to develop an intelligent WW. Here, the support and deceleration during uphill and downhill walking, respectively, a case sensitive release of the rear wheels and a support for obstacle crossing may be relevant issues. In addition, our results may help designing a test protocol to show the advantages of intelligent WWs during real-life situations which were identified as problematic in the present study. Another aspect of using intelligent WWs could be monitoring specific parameters related to mobility-related quality of life and health. For instance, the walking distance per day, an important marker of physical activity level, could be easily measured by adding simple technology. Furthermore, vertical force applied at the handle could be measured to estimate upper extremity weight bearing, which might be a parameter for monitoring rehabilitation progress. Also, detection of a WW in horizontal, i.e., lying position, could indicate a fall, which in turn could initiate an alarm call.
As a limitation of our study, the small sample size makes it hard to generalize our results. Nevertheless, a small sample size is rather expected to provide statistical trends than clear results, as in the experimental part of our study. Furthermore, only one of the several problems identified by our interviews was approached in the experimental part of our study. Future studies should investigate more of these problems to provide issues worth to be solved by an intelligent walker.
In conclusion, opening a door against the direction of walking caused interference between WW and, door and was identified as one problem when using a WW. Developing an intelligent WW, this possible safety problem should be regarded. In contrast, backward walking performance was improved by using a WW. For evaluation of future intelligent WWs, a combination of task specific tests and standard laboratory tests is recommended.
References
Steffen TM, Hacker TA, Mollinger L (2002) Age- and gender-related test performance in community-dwelling elderly people: 6-min walk test, Berg Balance Scale, Timed Up and Go Test, and gait speeds. Phys Ther 82:128–137
Bateni H, Maki BE (2005) Assistive devices for balance and mobility: benefits, demands, and adverse consequences. Arch Phys Med Rehabil 86:134–145
Salminen AL, Brandt A, Samuelsson K et al (2009) Mobility devices to promote activity and participation: a systematic review. J Rehabil Med 41:697–706
Graafmans WC, Lips P, Wijlhuizen GJ et al (2003) Daily physical activity and the use of a walking aid in relation to falls in elderly people in a residential care setting. Zeitschrift Für Gerontologie Und Geriatrie 36:23–28
Van Riel KMM, Hartholt KA, Panneman MJM et al (2014) Four-wheeled walker related injuries in older adults in the Netherlands. Inj Prev 20:11–15
Bryant MS, Pourmoghaddam A, Thrasher A (2012) Gait changes with walking devices in persons with Parkinson’s disease. Disabil Rehabil Assist Technol 7:149–152
Brandt A, Iwarsson S, Stahl A (2003) Satisfaction with rollators among community-living users: a follow-up study. Disabil Rehabil 25:343–353
Simoneau M, Teasdale N, Bourdin C et al (1999) Aging and postural control: postural perturbations caused by changing the visual anchor. J Am Geriatr Soc 47:235–240
Bateni H, Heung E, Zettel J et al (2004) Can use of walkers or canes impede lateral compensatory stepping movements? Gait Posture 20:74–83
Tung JY, Chee JN, Zabjek KF et al (2014) Combining ambulatory and laboratory assessment of rollator use for balance and mobility in neurologic rehabilitation in-patients. Disabil Rehabil Assist Technol. doi:10.3109/17483107.2014.908243
Fritz NE, Worstell AM, Kloos AD et al (2013) Backward walking measures are sensitive to age-related changes in mobility and balance. Gait Posture 37:593–597
Rentschler AJ, Cooper RA, Blasch B et al (2003) Intelligent walkers for the elderly: performance and safety testing of VA-PAMAID robotic walker. J Rehabil Res Dev 40:423–431
Umea University (2014) Biotech Umeå—developing an intelligent rollator. http://www.biotechumea.se/developing-an-intelligent-rollator. Accessed 22 July 2014
University of Stuttgart (2014) Institut für Automatisierungs- und Softwaretechnik. http://www.ias.uni-stuttgart.de/?page_id=46&demo_id=18. Accessed 17 July 2014
Sekiya N, Nagasaki H (1998) Reproducibility of the walking patterns of normal young adults: test-retest reliability of the walk ratio (step-length/step-rate). Gait Posture 7:225–227
Jones CJ, Rikli RE, Beam WC (1999) A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport 70:113–119
Groll DL, To T, Bombardier C et al (2005) The development of a comorbidity index with physical function as the outcome. J Clin Epidemiol 58:595–602
Callisaya ML, Blizzard L, McGinley JL et al (2012) Risk of falls in older people during fast-walking–the TASCOG study. Gait Posture 36:510–515
Acknowledgments
The authors thank Aaron Haslbauer, Karin Kampe and Elisabeth Petrias for data collection and technical support and the authors thank Aileen Currie for proofreading the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This work was supported by the Robert Bosch Foundation as the owner of the Robert-Bosch-Hospital where the study was conducted. The authors declare that they have no conflict of interest.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lindemann, U., Schwenk, M., Klenk, J. et al. Problems of older persons using a wheeled walker. Aging Clin Exp Res 28, 215–220 (2016). https://doi.org/10.1007/s40520-015-0410-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-015-0410-8