
Abstract
Post COVID-19 infections resulting in long COVID symptoms remain persistent yet neglected in healthcare priorities. Although long COVID symptoms are expected to decline after some time, many people continue to endure its debilitating effects affecting their daily lives. The diversity of characteristics amongst long COVID patients adds to the complexity of communicating personal health predicaments to healthcare providers. Recent research towards building an evidence base for long COVID with the aim of delivering responsive healthcare interventions for long COVID patients has utilised datasets generated from wearable devices. This paper examines the prospects presented by wearable devices for long COVID patients and physicians. It highlights distinct ethical and legal challenges arising from their use in practice. Several recommendations aiming to support their usage amongst long COVID patients are outlined for future research using wearable devices for long COVID treatment.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Characteristics and Prevalence of Long COVID: an Overview
Long COVID, a public health concern, affects approximately 225 million individuals globally, and spurred more than 90 long COVID patient groups advocating for support in long COVID research and clinical treatments (Payne 2022; Evans et al. 2021; Davis et al. 2023). Meanwhile, around 16 million Americans of working age have long COVID, with some affecting their employment prospects (Bach 2022). Long COVID broadly refers to physical or mental impairments experienced by individuals who contracted COVID-19 and continues to suffer from the debilitating effects post COVID-19 infection. Commonly reported symptoms ranged from respiratory difficulties (such as shortness of breath), prolonged lethargy, post exertional discomfort, heart palpitations, pain in chest and joints, ‘brain fog’, sleep disorders and other symptoms that are difficult to explain that last for weeks, months or years (Pinto et al. 2022; CDC 2022a; Baskett et al. 2023). Despite initial acceptance that COVID-19 is a respiratory infection, research has shown that it affects other body parts and organs, from the brains to limbs, muscles, reproductive tracts and other bodily tissues (Stein et al. 2022; NIAID 2022). This explains the constellation of symptoms experienced by long COVID patients.
Studies have reported substantial physical and mental health burdens in individuals due to persisting long COVID (Evans et al. 2021; Baskett et al. 2023; Hastie et al. 2022; Xu et al. 2023; Sellers 2022). Whilst long COVID is recognised as a disability in the USA (Office for Civil Rights 2021; CDC 2022b), this is not the case in other countries (Ministry of Health 2022). In a Scottish study, almost half of infected individuals recovered partially but continued to live with poorer quality of life and impairment across all daily activities (Hastie et al. 2022). Anecdotal accounts of long COVID patients revealed fatigue from daily activities such as walking, bathing, bending, lifting, communicating, struggling with work tasks and losing their memories (Pinto et al. 2022; Office for Civil Rights 2021; Wesley Ely 2023). Mental health effects include heightened risks of anxiety or depressive disorders, neurocognitive decline and sleep disorders (Xie et al. 2022).
There remains a lack of comprehensive understanding of long COVID (Lancet 2021; Lancet Neurology 2021; Lancet 2023; Ward et al. 2021). In the USA, the White House, through the National Institutes of Health, published its National Research Action Plan on Long COVID aimed at researching long COVID and finding a cure (DHHS 2022). The European Commissioner for Health and Food Safety similarly urged swift actions on long COVID in recognition of the impact on health systems (DGFHS 2022). WHO has similarly published guidance addressing support for long COVID patients whilst research continues (WHO 2021). Meanwhile, the effects of long COVID on individuals are continuously being identified, reported and mappedFootnote 1. Full recovery, however, remains a long process for millions of individuals suffering from the debilitating effects of long COVID.
Recent advances in wearable devices have shown early promising results that enable longitudinal mapping of the health status of long COVID patients (Evans 2021). This approach has the potential to enrich the evidence base for long COVID for future research. Whilst this is significant towards developing healthcare interventions for patients, there are important concerns affecting the users. Some studies have raised ethical implications in the use of wearable devices (Sui et al. 2023; Haroon et al. 2022; Southwick et al. 2021), but few have addressed specific concerns for long COVID patients. This paper aims to broaden the current discourse on public health strategies in addressing long COVID through health technologies such as wearable devices. This paper first examines the prospects presented by wearable devices in meeting the challenge of tracking the characteristics of long COVID and deepening an understanding of the seemingly ‘invisible’ effects plaguing long COVID patients. Next, it explores key ethical and legal challenges affecting its use. It highlights two distinct ethical concerns arising from its use—privacy and data security, followed by an assessment of key legal considerations governing its application and potential implications to policymakers. The paper concludes with recommendations in supporting their appropriate use amongst long COVID patients and future research in long COVID.
Wearable Devices: Prospects for Long COVID Patients and Research
Research into long COVID has primarily utilised electronic health records to study reported symptoms and track their trajectories to understand the characteristics (Estiri et al. 2021; Huang et al. 2022; Ledford 2022). A growing number of researchers have turned to machine learning to examine long COVID by training large datasets from electronic health records databases (Palmer 2022; Nature Medicine 2023; Pfaff et al. 2022). Studies have shown that long COVID cases are underreported in medical records (Wise 2021), especially when patients were unable to obtain medical support or chose to recover at home without consulting any physicians, thus affecting data availability in their health records. Furthermore, these studies were often conducted using retrospective data, resulting in delays in symptoms reporting and delivering treatment in a timely way.
As studies into COVID-19 continue to progress, researchers have started utilising wearable devices such as smartwatches and wireless sensors by tracking respiratory and heart rates and bodily temperatures to predict the presence of COVID-19 in patients, with early results demonstrating greater accuracy compared to test-and-trace before symptoms appear (Channa et al. 2021; Quer et al. 2021; Morris 2020; Jayaraman et al. 2023). Wearable devices and sensors broadly refer to technologies that have sensing capabilities to record and transmit physiological or physical activity measurements to an interlinked network of patients, physicians and developers (Lu et al. 2020; Javaid et al. 2021). Examples of these wearable devices include smart glasses, headbands, smartwatches, rings and bracelets. They are designed to be worn on major parts of the body such as the head, limbs and chest for various health tracking purposes ranging from disease diagnosis and management to general health monitoring and rehabilitation (Lu et al. 2020; Panesar 2019). In COVID-19 infection detections, wearable-generated data were analysed by artificial intelligence to evaluate and interpret cough patterns (such as frequency, duration, amplitude with higher precision compared to traditional modes of monitoring such as clinical human judgement), respiration, heart rate and body temperature.
Research into detecting COVID-19 using wearable devices were subsequently applied in long COVID studies. A study using wearable devices revealed promising potential towards defining long COVID based on evidence that 14% of COVID-19 patients have elevated heart rates for months post infection (Economist 2021). Other studies used shortness of breath and oscillating heart rates to study and manage long COVID symptoms (Evans 2021; Radin et al. 2021). Wearable devices that collect biometric data were trialled to improve the quality of care for long COVID patients through symptom reduction (Weiss 2022) whilst immunological, proteomic, genetic and wearable data assist deep phenotyping of long COVID patterns to help better target therapies (Haroon et al. 2022).
Wearable devices hold potential in facilitating long COVID patient care and enriching the knowledge base of long COVID (Stewart et al. 2021; Suett 2020). They provide precise, continuous real-time mapping of specific aspects of individuals living with long COVID such as breathing, sleep patterns and physiological and physical activities (Southwick et al. 2021; Khondakar and Kaushik 2022; Corrado et al. 2022; Corman et al. 2022; Xue et al. 2022; Lua et al. 2021; Mekhael et al. 2022; Mahmood 2023). The longitudinal nature of data collection from wearable devices is valuable in identifying long COVID phases in patients from declining symptoms to recurring episodes and subsequent improvements. Current prevalence of long COVID is only recorded when individuals sought help from physicians or admitted into hospitals, hence the numbers are likely to be underreported. Long COVID patients often suffer from not being taken seriously in demonstrating the illness plaguing their daily lives, unlike physical wounds (Chew 2022). Consequently, they become hesitant in seeking medical attention until symptoms become unbearable. Data generated from wearable devices can substantiate their experiences and supplement existing data from electronic health records to enable a comprehensive recording of long COVID symptoms. Additionally, as long COVID affects individuals in different ways, wearable devices can detect distinct individual symptoms to enable tailored recovery interventions (Suett 2020). For instance, a study into sleep patterns using wearable wristbands has successfully identified individuals with sleep disruption, enabling physicians to have a summary of the individual’s autonomic system activity when read with biometrics data to design personalised symptom managements (Mekhael et al. 2022). Measurable data from directly activity-linked sensors offer proactive clinical care as physicians could address patients’ difficulties in performing daily tasks directly (Corman et al. 2022). Wearable devices present promising prospects in capturing the variegated lived experiences of long COVID patients which are then presented to physicians for care management (Suett 2020).
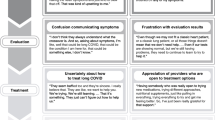
The CDC (2022b) for example, provides guidance for individuals in communicating their long COVID conditions to healthcare providers. These include documenting post COVID-19 infection experiences such as the presence, frequency and timing of symptoms, the ways in which the symptoms have affected the individual and medications. In severe cases, some individuals may not be able to recollect these details, and data from wearable devices can support these experiences and assist with clinical assessments. Additionally, these data can support individuals in starting their discussion with physicians regarding activity levels and routines that caused the worsening or improvements of symptoms. These preparations enable long COVID patients to effectively communicate their symptoms and the persistence of their illness. Physiological, physical and respiratory data generated from wearable devices play a supportive, evidence-based role to help initiate difficult conversations long COVID patients have to had when confronted with questions about their health status especially where their clinical test results did not show physical abnormalities. Data from wearable devices can therefore illuminate the ‘invisibility’ of the clinical symptoms and ‘validate’ long COVID symptoms in a tangible form.
Ethical and Legal Challenges: Concerns and Options
Ethical Considerations and Recommendations: Patient Privacy and Data Security
The use of wearable devices for long COVID patient monitoring is valuable; however, there are several ethical concerns arising from their tracking capabilities. Concerns preventing the widespread use of wearable devices in clinical settings include non-user-friendly options, security and privacy issues, lack of industry standards and technical complications (Lu et al. 2020). Important wide ranging ethical implications from the use of wearable devices include loss of autonomy, privacy, intrusiveness, stigma, medicalisation, reliability of devices, social isolation, patient safety and technological needs and concerns relating to informed consent, data mining and behavioural monitoring (Mittelstadt et al. 2014, 39; Resnick and Chircu 2017; Piwek et al. 2016). Other broader concerns include changes to physician-patient relationships where wearable devices are used outside of hospital settings, surveillance in private settings and over-reliance on wearable devices (Mittelstadt et al. 2014, 38, 45-46). A common recurring theme from these studies highlighted privacy, security and informed consent as important ethical considerations in using wearable devices for healthcare interventions.
Privacy and data security are most relevant given the nature of long COVID monitoring involving longitudinal data collection and potential cross-linkages with clinical and health records in tracking developing and declining symptoms in patients. Privacy concerns arise from the extent of intrusiveness in monitoring the individual’s health status and users’ ability to control who could have access to the transmitted data. Data generated from wearable devices are usually voluminous and stored in the cloud or servers for further analysis in identifying illness patterns for clinical interventions. Data security weaknesses could render these data vulnerable to unauthorised access and misuse; therefore, security infrastructure safeguards are essential. Additionally, commercially produced wearable devices (such as Apple and FitBit) have proprietary rights over the data collected. An option to address privacy and data security concerns is for healthcare providers to use clinician-designed devices instead of commercially produced wearable devices where users usually have limited control over the latter in terms of data use, privacy and security options. In the alternative, government healthcare providers could partner with trusted commercial developers to develop wearable devices that are tailored for this purpose with appropriate oversight from relevant ethics committee.
It is possible to include comprehensible privacy policies and consent forms supported by regulatory oversight and imposing penalties for misuse of health data collected by wearable devices (Anaya et al. 2018). Implementing informed consent processes and virtual walls to block the tracking of users’ digital footprints from sensor readings could help protect user privacy (ibid). However, true informed consent could be challenging in practice given prevailing formats of user acceptance such as fine prints and non-exhaustive exclusions of liabilities (Resnick and Chircu 2017). However, specifying controls to access to prevent data mining and disclosure of information from unauthorised parties such as cyber security attacks (denial of service, tampering) could potentially mediate data security risks (Anaya et al. 2018). For example, the US FDA guidelines stipulated wireless medical devices must include encryption protection for user security protection. A further option that could be implemented to mitigate the negative effects of wearable devices is adopting the policy of fair data use where participant consent is required for further use of their information. This will potentially minimise the risk of data misuse in the data collection and transmission processes.
Tracking individuals using wearable devices for longitudinal long COVID research to develop customised healthcare interventions for affected patients could strengthen the evidence base for long COVID. Research highlighted above have shown the promising potential of wearables in demonstrating symptoms experienced by long COVID patients; however, there are remaining concerns from longitudinal-type research that are closely related to privacy. An example is the psychosocial dimension associated with longitudinal use of wearables that could affect the mental wellbeing of individuals who use these devices. Familiarity with, and long-term usage of wearables could result in a shift in the user-device relationship. Where initially the purpose of using wearables is to substantiate their experiences with long COVID, yet it morphed into positioning these devices and data as the main instrument rather than the individual’s personal experiences, which may not be fully shown through numbers and metrics. The psychosocial effects may not be instantly recognisable, which adds to complexities in understanding their repercussions to individual mental health. It is therefore prudent not to overemphasise their credibility and accuracy, particularly where the metrics are yet to be verified by clinical evidence or having broad acceptance in medicine.
The emotional and psychological effects associated with longitudinal use might seem insignificant, yet they could evolve into other forms of mental health symptoms if users are unwary of them. For instance, long COVID and mental health symptoms arising from longitudinal monitoring may be unlikely to be distinguishable clearly. This is due to some long COVID symptoms that mirror mental health symptoms such as depressive moods or lethargy. Support and guidance from healthcare professionals are essential to ameliorate these effects, especially in situations where individuals have unsupervised use of these devices compared to patients who are formally enrolled on specialist long COVID research where follow-ups and monitoring check-ins are usually mandated. Use of wearable devices should, ideally be monitored and supported by healthcare professionals. Whilst wearables have potential, there are limitations given that the technologies that are driving these devices are still evolving. Consequently, a person-focused approach is preferable to prevent relegating those subjective experiences in favour of data and devices. The upshot is that wearable devices are treated as triangulation tools rather than primary diagnostic instruments.
Legal Considerations and Regulatory Options
Privacy and data security remain important considerations in the regulatory spheres. Their ethical importance, when translated into practice, requires careful deliberations of how patient data is used in helping them navigate their long COVID recovery. From the patients’ perspectives, it is crucial for physicians to disclose potential risks associated with using wearable devices, including the scope and extent of data collection and monitoring use, which could include potentially sensitive information. Regulatory frameworks premised on proportionality could shed light on the proper collection and use of data from wearables for long COVID patients. For example, data should only be collected for a specific timeframe and proportional to the reported symptoms. The proportionality approach respects the persons’ interest from harm arising from undue intrusion into their private lives. This means collecting and using only data that relates to the health of the individual and subject to adjustments as the symptoms decline or recur. Hence, the person is treated as a ‘collaborator’ with their healthcare providers in their long COVID journey towards recovery rather than a subject under surveillance.
The distinctions between self-monitoring for long COVID symptoms to evidence individual experiences when seeking medical support from healthcare providers and monitoring for longitudinal research for systematically discovering solutions for patients and advancing research on long COVID attract different legal considerations. Self-monitoring poses risks of covert data commercialisation where third-party commercial devices are used. This is closely associated to the lack of user control highlighted above and surveillance risks to individuals for purposes that could be broader than originally accepted. The implication to users is clandestine use of their data through unauthorised sale or sharing to third parties such as insurers or pharmaceutical companies which may not necessarily benefit the users. This tendency leads to other forms of harm such as harassment (physical and emotional) or voyeurism. Stronger data protection enforcement is helpful to minimise such risks.
Monitoring for longitudinal research involves concerns that may not be immediately evident. For instance, it prompts questions about potential overlaps between research and treatment. There are benefits in advancing research and treatment, yet it could be difficult to demarcate the lines for patients, physicians and scientists. Individuals should not feel obliged to accept research enrolment and monitoring for fear of not receiving treatment; rather they should be made aware that their participation is voluntary and would not preclude any access to potential benefits derived from research into long COVID using wearable devices. The initial phases of long COVID patients are often disproportionately represented by frontline workers in the retail, consumer and essential services sectors who may have fewer opportunities to explore treatment options due to lower socio-economic and financial conditions. Research teams that recruit participants for long COVID research should account for this aspect in their investigations. Institutional and national research bodies could consider developing functional guidance to supplement existing guidelines surrounding research and treatment of long COVID patients to prevent unethical practices in the quest for advancing long COVID research.
Existing regulations and guidelines on data storage and security should be updated to reflect the distinct vulnerabilities affecting wearable devices, particularly in data transmission where weak coding or lack of encryption could render the data vulnerable to unauthorised access and interception. Wearable devices that are in prototype stages generally suffer from security and usability concerns, affecting user privacy and data security (Channa et al. 2021). User and physician awareness and knowledge regarding data security and privacy have been shown to be significant and necessary to change existing policy weaknesses, particularly the lack of transparency in data collection, storage and access control (Alvarez et al. 2021). Questions about privacy and risk of misuse are likely to be amplified where commercial devices are used, as users rarely have control over how their data are processed or shared with third parties. This in turn depends on the strength of regulatory protections in the users’ country.
A potential regulatory option is developing privacy checklists based on CIA and HIPAA frameworks premised on transparency, confidentiality, integrity and availability (Safavi and Shukur 2014). Furthermore, regulatory responses should be flexible and attend to the surrounding environments because privacy conceptions vary across societies and countries. (Resnick and Chircu 2017). An option is to clarify existing laws governing new technologies or create distinct laws to address distinct issues in policy (ibid), such as classifying wearable devices according to risk levels similar to the Food and Drug Administration rules (US) or Medicine and Healthcare products Regulatory Authority (UK). Lu et al. (2020) rightly proposed the need for common regulatory standards for data collection and processing, greater oversight of the wearables industry and clarification on the physician-patient relationship in addressing ethical concerns that arise. Alternatively, wearable devices developers could incorporate greater user choices in controlling their data in the design process, although this raises trade-off considerations between higher market costs through privacy enhancing technologies and balancing privacy interests (Baldini et al. 2018). Further considerations could be given to designing ethical governance throughout the data systems (Resnick and Chircu 2017).
Finally, it may be useful to use wearable devices that are developed specifically to measure common parameters of long COVID pending appropriate regulatory frameworks in place. An approach to mediate some of the ethical and practical concerns from commercially produced devices is for researchers developing wearable devices to partner with physicians and long COVID specialist clinics to customise devices that are appropriate for long COVID patient monitoring and research. Their use would be supported by ethics committee oversight in accordance with established research and data management protocols. This step could strengthen the safety and security of patients in so far as the collection, storage and use of their personal information and health data are concerned. Cultivating a responsible mindset amongst users could be helpful in pre-empting some of the concerns that emerged from using wearables for long COVID monitoring. Ideally, a greater awareness amongst the population about the benefits and risks of using commercially developed tracking devices is valuable in their societal participation in the broader digital health environment.
Conclusion
Existing ‘illness framework’ implies long COVID patients are neither too ill to be admitted for ‘treatment’, yet unwell enough compared to their pre-COVID selves. Wearable devices are designed to provide continuous monitoring, and hence particularly useful for tracking the developments of long COVID in individuals to assist in recovery and symptom interventions. Lifestyle and health data from wearable devices provide a rich collection of symptoms and longitudinal information in mapping the trajectories of long COVID symptoms. Data from wearable devices are valuable in linking existing disparate evidence on long COVID towards better informing physicians and healthcare services in providing patient care. Patient monitoring through wearable devices potentially eases physicians’ burdens whilst providing accurate and timely catalogues of health data for customised symptoms management.
Despite their promising features, there remain limitations in technologies that are still developing. Greater attention to implementing security infrastructure is essential towards protecting patient privacy and safeguarding data integrity. Current regulatory frameworks that are protective of user privacy and safety could be utilised to address immediate gaps in governing the use of wearable devices for long COVID patients. Future research could include greater assurance in wearable devices use, incorporating user insights and demonstrating better accountability by companies that develop, manufacture and market these devices. Meanwhile, the psychological, social and emotional effects from using wearable devices for longitudinal long COVID research and monitoring should be more widely recognised to enable efforts to address any adverse effects to individual mental health. Support from healthcare providers would be helpful in identifying risks to mental health in the early stages of using wearables in their long COVID journey.
References
Alvarez, Sarah L., Stephanie L. Baller, and Anthony Walton. 2021. Who owns your health data? Two interventions addressing data of wearable health devices among young adults and future health clinicians. Journal of Consumer Health on the Internet 25 (1): 35–49. https://doi.org/10.1080/15398285.2020.1852386.
Bach, Katie. 2022. New data shows long COVID is keeping as many as 4 million people out of work. Brookings, 24 August 2022. https://www.brookings.edu/research/new-data-shows-long-covid-is-keeping-as-many-as-4-million-people-out-of-work/. Accessed 14 Sept 2022.
Baldini, Gianmarco, Maarten Botterman, Ricardo Neisse, and Mariachiara Tallacchini. 2018. Ethical design in the internet of things. Science and Engineering Ethics 24: 905–925. https://doi.org/10.1007/s11948-016-9754-5.
Baskett, William I., Adnan I. Qureshi, Daniel Shyu, Jane M. Armer, and Chi-Ren Shyu. 2023. COVID-specific long-term sequelae in comparison to common viral respiratory infections: an analysis of 17 487 infected adult patients. Open Forum Infectious Diseases 10 (1): ofac683. https://doi.org/10.1093/ofid/ofac683.
CDC. 2022a. Long COVID or post-COVID conditions. Centers for Disease Control and Prevention, 16 December 2022. https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html.
CDC. 2022b. Patient tips: healthcare provider appointments for post-COVID conditions. Centers for Disease Control and Prevention, 11 July 2022. https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/post-covid-appointment/index.html.
Channa, A., N. Popescu, J. Skibinska, and R. Burget. 2021. The rise of wearable devices during the COVID-19 pandemic: a systematic review. Sensors 21: 5787. https://doi.org/10.3390/s21175787.
Chew, Hui Min. 2022. Breathlessness, fatigue, persistent cough: doctors see more cases of ‘long COVID’ in Singapore. Channel NewsAsia, 23 March 2022. https://www.channelnewsasia.com/singapore/long-covid-coronavirus-breathless-cough-fatigue-doctors-therapy-2578961.
Corman, B.H.P., S. Rajupet, F. Ye, and E.R. Schoenfeld. 2022. The role of unobtrusive home-based continuous sensing in the management of postacute sequelae of SARS CoV-2. Journal of Medical Internet Research 24 (1): e32713–e32713. https://doi.org/10.2196/32713.
Corrado, J., S. Halpin, N. Preston, D. Whiteside, R. Tarrant, J. Davison, A.D. Simms, R.J. O’Connor, A. Casson, and M. Sivan. 2022. HEART rate variability biofeedback for long COVID symptoms (HEARTLOC): protocol for a feasibility study. BMJ Open 12 (11): e066044–e066044. https://doi.org/10.1136/bmjopen-2022-066044.
Davis, H.E., L. McCorkell, J.M. Vogel, et al. 2023. Long COVID: major findings, mechanisms and recommendations. Nature Reviews Microbiology 21: 133–146. https://doi.org/10.1038/s41579-022-00846-2.
DHHS. 2022. National research action plan on long COVID. Department of Health and Human Services, August 2022. https://www.covid.gov/assets/files/National-Research-Action-Plan-on-Long-COVID-08012022.pdf.
DGHFS. 2022. Facing the impact of post COVID-19 condition (long COVID) on health systems. Director General for Health and Food Safety, 13 December 2022. https://health.ec.europa.eu/publications/facing-impact-post-covid-19-condition-long-covid-health-systems_en.
Economist. 2021. A new study using wearable devices could help to define long COVID. Economist, 17 July 2021. https://www.economist.com/graphic-detail/2021/07/17/a-new-study-using-wearable-devices-could-help-to-define-long-covid. Accessed 15 Sept 2022.
Estiri, H., Z.H. Strasser, G.A. Brat, Y.R. Semenov, Consortium for Characterization of COVID-19 by EHR, C.J. Patel, and S.N. Murphy. 2021. Evolving phenotypes of non-hospitalized patients that indicate long COVID. BMC Medicine 19:249. https://doi.org/10.1186/s12916-021-02115-0.
Evans, Jonny. 2021. Can an Apple Watch help manage ‘long COVID’? Computerworld, 12 July 2021. https://www.computerworld.com/article/3624617/can-an-apple-watch-help-manage-long-covid.html. Accessed 15 Sept 2022.
Evans, Rachael A., Hamish McAuley, Ewen M. Harrison, Aarti Shikotra, Amisha Singapuri, and Marco Sereno. 2021. Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): a UK multicentre, prospective cohort study. The Lancet: Respiratory Medicine 9 (11): 1275–1287. https://doi.org/10.1016/S2213-2600(21)00383-0.
Haroon, S., K. Nirantharakumar, S.E. Hughes, et al. 2022. Therapies for long COVID in nonhospitalised individuals: from symptoms, patient-reported outcomes and immunology to targeted therapies (The TLC Study). BMJ Open 12: e060413. https://doi.org/10.1136/bmjopen-2021-060413.
Hastie, Claire E., David J. Lowe, Andrew McAuley, Andrew J. Winter, Nicholas L. Mills, Corri Black, Janet T. Scott, Catherine A. O’Donnell, David N. Blane, Susan Browne, Tracy R. Ibbotson, and P. Jill. 2022. Pell Outcomes among confirmed cases and a matched comparison group in the long COVID in Scotland study. Nature Communications 13: 5663. https://doi.org/10.1038/s41467-022-33415-5.
Huang, Y., M.D. Pinto, J.L. Borelli, M. Asgari Mehrabadi, H.L. Abrahim, N. Dutt, N. Lambert, E.L. Nurmi, R. Chakraborty, A.M. Rahmani, and C.A. Downs. 2022. COVID symptoms, symptom clusters, and predictors for becoming a long-hauler looking for clarity in the haze of the pandemic. Clinical Nursing Research 31 (8): 1390–1398. https://doi.org/10.1177/10547738221125632.
Javaid, Mohd, Abid Haleem, Shanay Rab, Ravi Pratap Singh, and Rajiv Suman. 2021. Sensors for daily life: a review. Sensors International 2:100121. https://doi.org/10.1016/j.sintl.2021.100121.
Jayaraman, Arun, Shirley Ryan, and AbilityLab. 2023. Wearable sensor to monitor COVID-19 like signs and symptoms. ClinicalTrials.gov, 13 January 2023. https://clinicaltrials.gov/ct2/show/NCT04393558.
Khondakar, K.R., and A. Kaushik. 2023. Role of wearable sensing technology to manage long COVID. Biosensors (Basel) 13 (1): 62. https://doi.org/10.3390/bios13010062.
Lancet. 2021. Understanding long COVID: a modern medical challenge. Lancet 398 (10302): 725. https://doi.org/10.1016/S0140-6736(21)01900-0.
Lancet Neurology. 2021. Long COVID: understanding the neurological effects. Lancet Neurology 20 (4): 247–247. https://doi.org/10.1016/s1474-4422(21)00059-4.
Lancet. 2023. Long COVID: 3 years in. Lancet 401 (10379): 795. https://doi.org/10.1016/S0140-6736(23)00493-2
Ledford, Heidi. 2022. How common is long COVID? Why there’s still no answer. Nature 606 (7916): 852–853.
Lu, Lin, Jiayao Zhang, Yi Xie, Fei Gao, Xu Song, Wu Xinghuo, and Zhewei Ye. 2020. Wearable health devices in health care: narrative systematic review. JMIR mHealth and uHealth 8 (11): e18907. https://doi.org/10.2196/18907.
Lua, S.B.H., D. Lowe, A. Taylor, M. Sim, B. Henderson, C. Trueman, O. Meredith, S. Burns, P. McGuinness, and C. Carlin. 2021. P24 COVID-19 advanced respiratory physiology (CARP) wearable respiratory monitoring: early insights. Thorax 76 (Suppl 2): A78–A79. https://thorax.bmj.com/content/76/Suppl_2/A78.2. Accessed 10 Jan 2024.
Mahmood, A. 2023. A package of smartphone and sensor-based objective measurement tools for physical and social exertional activities for patients with illness-limiting capacities. PhD Thesis, Marquette University.
Mekhael, M., C.H. Lim, A.H. El Hajjar, C. Noujaim, C. Pottle, N. Makan, L. Dagher, Y. Zhang, N. Chouman, D.L. Li, T. Ayoub, and N. Marrouche. 2022. Studying the effect of long COVID-19 infection on sleep quality using wearable health devices: observational study. Journal of Medical Internet Research 24 (7): e38000–e38000. https://doi.org/10.2196/38000.
Ministry of Health. 2022. Incidence of long COVID amidst recovered Singaporeans. Ministry of Health, 4 April 2022. https://www.moh.gov.sg/news-highlights/details/incidence-of-long-covid-amidst-recovered-singaporeans/.
Mittelstadt, Brent, Ben Fairweather, Mark Shaw, and Neil McBride. 2014. The ethical implications of personal health monitoring. International Journal of Technoethics 5 (2): 37–60. https://doi.org/10.4018/ijt.2014070104.
Morris, Amanda 2020. Monitoring COVID-19 from hospital to home: first wearable device continuously tracks key symptoms. Northwestern, 4 May 2020. https://news.northwestern.edu/stories/2020/04/monitoring-covid-19-from-hospital-to-home-first-wearable-device-continuously-tracks-key-symptoms/. Accessed 15 Aug 2022.
National Institute of Allergy and Infectious Diseases. 2022. NIAID pandemic autopsy study fosters long COVID treatment trial. NIAID Now, 14 December 2022. https://www.niaid.nih.gov/news-events/covid-autopsy-study.
Nature Medicine. 2023. Machine learning identifies long COVID patterns from electronic health records. Nature Medicine 29 (1): 47–48. https://doi.org/10.1038/s41591-022-02130-5.
Office for Civil Rights. 2021. Guidance on “Long COVID” as a disability under the ADA, Section 504, and Section 1557. Department of Health and Human Services, 26 July 2021. https://www.hhs.gov/civil-rights/for-providers/civil-rights-covid19/guidance-long-covid-disability/index.html
Palmer, Katie. 2022. Researchers test the power of machine learning to unravel long COVID’s mysteries. STAT, 29 April 2022. https://www.statnews.com/2022/04/29/long-covid-machine-learning-n3c/.
Panesar, Arjun. 2019. Future of Healthcare. In machine learning and ai for healthcare: big data for improved health outcomes, 255–304. New York, NY: Apress. https://doi.org/10.1007/978-1-4842-3799-1_7.
Payne, Daniel. 2022. ‘Left to rot’: the lonely plight of long COVID sufferers. Politico, 14 August 2022. https://www.politico.com/news/2022/08/14/left-to-rot-long-covid-patients-around-the-world-call-for-more-government-action-00051161. Accessed 28 Aug 2022.
Pfaff, Emily R., Andrew T. Girvin, Tellen D. Bennett, Abhishek Bhatia, Ian M. Brooks, Rachel R. Deer, Jonathan P. Dekermanjian, et al. 2022. Identifying who has long COVID in the USA: a machine learning approach using N3C data. Lancet Digital Health 4 (7): e532–e541. https://doi.org/10.1016/s2589-7500(22)00048-6.
Pinto, M.D., C.A. Downs, Y. Huang, S.A. El-Azab, N.S. Ramrakhiani, A. Barisano, L. Yu, K. Taylor, A. Esperanca, H.L. Abrahim, T. Hughes, M.G. Herrera, A.M. Rahamani, N. Dutt, R. Chakraborty, C. Mendiola, and N. Lambert. 2022. A distinct symptom pattern emerges for COVID-19 long-haul: a nationwide study. Scientific Reports 12 (1): 15905. https://doi.org/10.1038/s41598-022-20214-7.
Piwek, L., D.A. Ellis, S. Andrews, and A. Joinson. 2016. The rise of consumer health wearables: promises and barriers. PLoS Medicine 13 (2): e1001953. https://doi.org/10.1371/journal.pmed.1001953.
Quer, Giorgio, Jennifer M. Radin, Matteo Gadaleta, Katie Baca-Motes, Lauren Ariniello, Edward Ramos, Vik Kheterpal, Eric J. Topol, and R. Steven. 2021. Steinhubl Wearable sensor data and self-reported symptoms for COVID-19 detection. Nature Medicine 27: 73–77. https://doi.org/10.1038/s41591-020-1123-x.
Radin, Jennifer M., Giorgio Quer, Edward Ramos, Katie Baca-Motes, Matteo Gadaleta, Eric J. Topol, and R. Steven. 2021. Steinhubl Assessment of prolonged physiological and behavioral changes associated with COVID-19 infection. JAMA Network Open 4 (7): e2115959. https://doi.org/10.1001/jamanetworkopen.2021.15959.
Resnick, Marc L., and Alina M. Chircu. 2017. Wearable devices: ethical challenges and solutions. In Managing security issues and the hidden dangers of wearable technologies, ed. Andrew Marrington, Don Kerr, and John Gammac, 182–205. Hershey, PA: IGI Global.
Safavi, S., and Z. Shukur. 2014. Conceptual privacy framework for health information on wearable device. PLoS ONE 9 (12): e114306. https://doi.org/10.1371/journal.pone.0114306.
Segura Anaya, L.H., Abeer Alsadoon, Nectar Costadopoulos, and P.W.C. Prasad. 2018. Ethical implications of user perceptions of wearable devices. Science and engineering ethics 24: 1–28. https://doi.org/10.1007/s11948-017-9872-8.
Sellers, Frances Stead. 2022. ‘We are in trouble’: Study raises alarm about impacts of long COVID’. Washington Post, 13 October 2022. https://www.washingtonpost.com/health/2022/10/12/long-covid-study-scotland/.
Southwick, L., S.C. Guntuku, E.V. Klinger, A. Pelullo, H. McCalpin, and R.M. Merchant. 2021. The role of digital health technologies in COVID-19 surveillance and recovery: a specific case of long haulers. International Review of Psychiatry 33 (4): 412–423. https://doi.org/10.1080/09540261.2020.1854195.
Stein, Sydney R., Sabrina C. Ramelli, Alison Grazioli, Joon-Yong. Chung, Manmeet Singh, Claude Kwe Yinda, et al. 2022. SARS-CoV-2 infection and persistence throughout the human body and brain at autopsy. Nature 612 (7941): 758–763. https://doi.org/10.1038/s41586-022-05542-y.
Stewart, C., Y. Ranjan, P. Conde, Z. Rashid, H. Sankesara, X. Bai, R.J.B. Dobson, and A.A. Folarin. 2021. Investigating the use of digital health technology to monitor COVID-19 and its effects: protocol for an observational study (COVID Collab Study). JMIR Research Protocols 10 (12): e32587–e32587. https://doi.org/10.2196/32587.
Suett, C., Nisreen A. Alwan, Emily Attree, Jennifer Mary Blair, Debby Bogaert, Mary-Ann Bowen, et al. 2020. Rapid response: from doctors as patients: a manifesto for tackling persisting symptoms of COVID-19. BMJ 370: m3026. https://doi.org/10.1136/bmj.m3026.
Sui, A., W. Sui, S. Liu, and R. Rhodes. 2023. Ethical considerations for the use of consumer wearables in health research. Digital Health 9: 20552076231153740. https://doi.org/10.1177/20552076231153740.
Ward, H., B. Flower, P.J. Garcia, S.W.X. Ong, D.M. Altmann, B. Delaney, N. Smith, P. Elliott, and G. Cooke. 2021. Global surveillance, research, and collaboration needed to improve understanding and management of long COVID. Lancet 398 (10316): 2057–2059. https://doi.org/10.1016/s0140-6736(21)02444-2.
Weiss, Eric. 2022. RTHM and Stella leverage wearable biometrics to help treat long COVID. FindBiometics, 6 June 2022. https://findbiometrics.com/rthm-stella-leverage-wearable-biometrics-help-treat-long-covid-060608/ Accessed 15 Sept 2022.
Wesley Ely, E. 2023. The haunting brain science of long COVID. STAT, 16 February 2023. https://www.statnews.com/2023/02/16/the-haunting-brain-science-of-long-covid/.
WHO. 2021. Support for rehabilitation: self-management after COVID-19-related illness, second edition. Health Workforce and Service Delivery, World Health Organization, 27 September 2021. https://www.who.int/europe/publications/i/item/WHO-EURO-2021-855-40590-59892.
Wise, J. 2021. COVID-19: long COVID cases are underreported in GP records, research suggests. BMJ 374: n1685. https://doi.org/10.1136/bmj.n1685.
Xie, Y., E. Xu, and Z. Al-Aly. 2022. Risks of mental health outcomes in people with COVID-19: cohort study. BMJ 376: e068993. https://doi.org/10.1136/bmj-2021-068993.
Xu, E., Y. Xie, and Z. Al-Aly. 2023. Long-term gastrointestinal outcomes of COVID-19. Nature Communications 14: 983. https://doi.org/10.1038/s41467-023-36223-7.
Xue, F., A. Monaghan, G. Jennings, L. Byrne, T. Foran, E. Duggan, and R. Romero-Ortuno. 2022. A novel methodology for the synchronous collection and multimodal visualization of continuous neurocardiovascular and neuromuscular physiological data in adults with long COVID. Sensors (Basel) 22 (5): 1758. https://doi.org/10.3390/s22051758.
Funding
This research is supported by the National Research Foundation, Singapore under its Campus for Research Excellence and Technological Enterprise (CREATE) programme.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Not required.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chan, H.Y. Wearable Devices for Long COVID: Prospects, Challenges and Options. ABR (2024). https://doi.org/10.1007/s41649-023-00272-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41649-023-00272-3