
Abstract
Purpose
Evaluate the clinical performance of currently available dental bleaching technologies concerning their efficacy and safety features. This study aimed to evaluate the clinical outcome of a 940-nm diode laser-assisted in-office bleaching technique for vital teeth.
Methods
Subjects were assigned to treatments in a split-mouth study design. A 38% hydrogen peroxide gel photoactivated by 940 nm [400 μm fiber tip, 7 W; maximum energy of 210 J per tooth (smaller teeth received less energy than 210 J), maximum period of 30 s] (LaserWhite20, Biolase, USA) and a 38% hydrogen peroxide conventional gel (Power Whitening, WHITEsmile, Germany) were tested. The photoactivated system was evaluated on the right quadrants of upper and lower jaws, while the conventional hydrogen peroxide system was evaluated on the left quadrants. Gels were fixed in place for 10 min and then rinsed. The degree of color change was evaluated using a spectrophotometer based on VITAscale (Shade Star, Degudent, Germany) immediately after treatments. Data were analyzed using one-way ANOVA, followed by Tukey’s test or paired t test, setting a significance level of 5%.
Results
Both treatments were effective in promoting tooth whitening (p < 0.05). No differences among teeth and arches were observed within each treatment group (p > 0.05). The laser-assisted system resulted in lower shade values in both upper and lower jaws (p < 0.05). Few patients experienced tooth sensitivity in the treated areas upon completion of the treatment. The dental pulp viability of the treated teeth was maintained more than 1 year after the completion of the treatments.
Conclusions
The 940-nm diode laser-assisted tooth whitening has been shown to be effective in a short-term post-bleaching assessment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lightening teeth has become associated with health and beauty [1] and, as a result, desirable to modern dental patients. Tooth bleaching is an important component of esthetic dentistry since it is considered to be one of the most conservative alternatives for the treatment of tooth discoloration. Currently, two main bleaching approaches are widely used: at-home and in-office techniques. A recent systematic review comparing at-home and in-office bleaching has concluded that both techniques present equal effectiveness and similar risk/intensity of tooth sensitivity [2]. However, at-home bleaching is usually considered equally effective and less associated with tooth sensitivity than in-office modalities [3]. Despite the advantages of at-home whitening, in-office bleaching stands out because of the rigorous control of the dentist over the treatment process, preservation of the soft tissue health, prevention of swallowing material, discomfort from wearing trays, and expedited outcome. These benefits result in overall satisfaction of the patient and reduced treatment time [2, 4,5,6]. The in-office bleaching technique is also an appropriate alternative in cases of severe discoloration or single tooth discoloration [2, 7, 8].
Lasers, non-coherent light sources, and heat may be used for the activation of the bleaching agent to accelerate tooth whitening [9]. Accordingly, high-intensity light sources may increase the temperature of hydrogen peroxide (HP) gels [7], which, in turn, speed up the bleaching process by accelerating HP decomposition [10]. However, early methods of HP activation were associated with temperature increase and sensitivity [11]. To avoid or diminish adverse effects of light-activated bleaching, modern light sources [e.g., xenon–halogen lights, light-emitting diodes (LEDs), plasma arcs, and diode lasers] have been implemented to produce greater brightening results with less heat generation. In fact, bleaching with diode lasers has shown to result in less tooth and gingival sensitivity than the other bleaching systems [12]. Nevertheless, because the validity of adjunct lights in tooth bleaching is still controversial, rigorous studies are necessary to explore the advantages of these alternative systems.
Recently, a new bleaching system was introduced into the dental market, which combines an HP gel with irradiation with a diode laser at 940 nm or 810 nm using a bleaching hand piece attached to the trunk fiber (LaserWhite20, Biolase, USA). According to the manufacturer, this system was designed to lighten dark, yellowed, or discolored teeth with extrinsic and intrinsic staining. New dental bleaching technologies are being introduced daily into the market. The evaluation of their clinical performance in relation to both efficacy and safety aspects is of great relevance for the routine dental practice. This study aimed to evaluate the short-term clinical efficacy of this new in-office tooth bleaching system combined with 940-nm diode laser irradiation.
Materials and methods
Participants
Young adults from 20 to 35 years of age, who were part of a convenience sample and volunteered to participate in the study, received an informed consent form containing information about the risks and benefits of the treatment.
Before being enrolled in the study, participants signed an informed consent form adhering to the ethical principle stated by the Declaration of Helsinki of the World Medical Association. Volunteers were required to be in good general and dental health. At the dental screening, participants who had optimum oral hygiene and vital teeth from the central incisor to the first premolar of all maxillary and mandibular quadrants were included in the study. Volunteers exhibiting active carious lesions or prosthetic restorations in the anterior teeth, tetracycline-stained teeth, gingival irritation or periodontal disease, or painful symptoms or tooth sensitivity in their anterior teeth were excluded. Participants who were smokers, who were pregnant or lactating, or who had used tooth whitening products within the preceding 3 years were also excluded from the study.
Experimental design
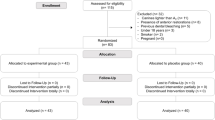
A split-mouth clinical study was designed with 20 subjects. Teeth in the maxillary and mandibular right quadrants were allocated to the laser-assisted bleaching technique with 38% HP (LaserWhite 20, Biolase, USA). For the left quadrants, a conventional bleaching gel with 38% HP (White Smile/Power Whitening, Germany), without laser irradiation, was applied.
The same trained evaluator recorded the initial (baseline) and final (post-bleaching) color of the evaluated teeth by using a spectrophotometer (Shade Star, Degudent, Germany). The colors were evaluated immediately after the bleaching process. To obtain reliable results, all volunteers were treated in the same room, lit with artificial light.
Bleaching procedure
Figure 1 illustrates the dental bleaching procedures. All teeth surfaces were initially cleaned using glycerin-free pumice and underwent thorough scaling, root planing, and cleaning to remove all the superficial stains and dental plaque. The teeth were not fluoridated after the cleaning procedure to avoid interference with penetration of the active components of the bleaching gel [8]. Lips were lubricated, and a cheek retractor was used to retract soft tissues. The gingival margins and all the embrasures were covered with gingival protector extending slightly on the tooth surface to assure adequate protection of the soft tissue.

Tooth bleaching procedures using the laser-assisted system (a) and the conventional treatment (b)
LaserWhite 20 system
The LaserWhite 20 gel is provided in two pastes (gel base and activator), which were mixed according to the manufacturer’s instructions. After placing a thin layer of the gel (approximately 1 mm) on the labial tooth surface, the InGaAsP diode laser (Ezlase, Biolase, USA) was used to activate the gel. The laser irradiation parameters were as follows: wavelength 940 nm, power 7 W, and maximum total energy delivered per tooth 210 J. The laser energy application was performed in scanning and non-contact mode, 1 mm away from the surface using a 400-μm fiber uninitiated tip (diameter 415 μm, length 21.17 mm, with calibration of 0.85), instead of the bleaching hand piece recommended by the manufacturer. This was done to control light exposure, particularly near the median line where the non-lased left quadrant was being assessed. A black cardboard bulkhead was placed in the median line to avoid light exposure in the left quadrants. The irradiation time was mostly based on the heat sensation reported by the patient, and when no heat was reported, the laser application was stopped when the maximum time of 30 s was reached. The gel remained in place for 10 min (Fig. 1a). Then, it was removed using high-volume suction followed by flushing with an air and water spray to remove any residual gel. This procedure was performed on each right quadrant (upper or lower), separately.
White smile/power whitening
The Power Whitening (WHITEsmile, Germany) is a red bleaching gel composed of a base and an activator contained within a double tube syringe that mixed them together in the nozzle. The 38% HP gel was placed on the labial teeth surface in each quadrant and rinsed after 10 min (Fig. 1b). This procedure was done for each quadrant on the left side separately. No light irradiation was performed.
Dental pulp vitality
More than a year following treatments, the patients were recalled, and the pulp vitality was assessed using the heat and cold test.
Statistical analysis
Shade values were converted to scores as shown in Table 1, ranging from B1 (lowest value) to C4 (highest value). Means of shade scores within teeth, quadrants, and jaws were statistically compared by ANOVA complemented by the Tukey’s post hoc test. To compare shades before and after treatment, between both dental bleaching modalities, paired t tests were used. For all data analysis, the statistical significance level was set at 5%.
Results
Figure 2 presents one of the clinical cases to illustrate the outcomes of the treatments [e.g., conventional (left side) and laser-assisted (right side)]. The mean ± standard deviation age for the participants was 22.0 ± 1.4 years. Six participants were male, and 14 were female. Four participants experienced tooth sensitivity in the treated areas upon completion of the treatment. After 2 days, all patients were cleared, and no reports of sensitivity or discomfort were reported. The dental pulp viability of the treated teeth was maintained for more than 1 year after the completion of the treatments.

Clinical case: female, 34-year-old patient. a Baseline clinical condition, b post-bleaching clinical aspect, and c table showing in detail the differences in colors (Vita Classical shades) after bleaching of each treated tooth of this patient
Table 2 depicts the results for each tooth category in each quadrant. Data from each tooth category, both at baseline and post-bleaching, showed no significant difference between treatments in both arches. Canines presented significant decrease in shade in all groups and arches. For the overall treatment, i.e., when tooth categories were evaluated altogether, both treatments where effective in whitening tooth color in all quadrants (Table 3).
Comparing treatments, the laser-assisted system was found to improve color by more shade units than the conventional treatment in both arches (Fig. 3).

Comparison of dental bleaching efficacy between conventional and laser-assisted treatments
Discussion
The present study was conducted to compare and analyze the short-term efficacy of the laser-assisted dental bleaching with conventional treatment. Both treatments performed were effective in achieving whitening. Nevertheless, the laser-assisted system (38% HP + 940-nm diode laser) resulted in significantly lower shade values in both upper and lower arches compared to the conventional treatment (38% HP). In fact, it was observed that the laser-assisted system improved results more than the conventional system when it was applied once and for a period of only 10 min.
A number of tooth bleaching protocols have been described for both at-home and in-office treatments [2, 13, 14]. Highly concentrated HP protocols (35–38%), particularly, may be applied for variable periods of time in contact with the tooth surface, and in one or multiple cycles/sessions [2, 13,14,15]. However, adverse effects derived from these bleaching agents are widely described in the literature [13,14,15]. A recent study has shown that enamel slabs bleached with 38% HP may result in mild changes in enamel surface micromorphology [16], and others showed a decrease in the enamel mineral content [17]. As such, shorter contact times of 38% HP with the tooth surface, which allows satisfactory esthetic results, are preferable in the clinical setting. A previous study has shown that the 38% HP applied for 8 min in one cycle has achieved satisfactory bleaching results [15]. Thus, to compare with the LaserWhite20 system with the conventional method, the same time of application (10 min) and HP concentration was used.
The use of supplementary light on the effectiveness of vital bleaching treatments is still controversial, even for laser devices [18]. In spite of that, the Food and Drug Administration (FDA) has approved three types of lasers for laser-assisted bleaching: argon ion laser (488–514 nm), carbon dioxide laser (10,060 nm), and diode lasers (790–980 nm) [7]. Argon and CO2 lasers, however, are not used any more due to overheating. Significant shade changes using in-office bleaching systems and diode lasers were reported in the literature [12, 19,20,21,22,23]. However, other studies have not been able to confirm positive effects of light irradiation on the efficacy of tooth whitening agents [6, 13, 14, 18, 24, 25]. The lack of consensus may be due to the multiple methods used to analyze bleaching efficacy, such as variable protocols, laser exposure parameters, and methods of shade/color change assessment.
Here, the proposed treatment showed to be more effective than the conventional one. This was observed for a minimal time of exposure on the dental surface for the 38% HP gel (10 min, one cycle) for both treatments. The mean change in shade for maxillary and mandibular quadrants using the laser-assisted system was at a minimum of one shade value lower than the conventional treatment. Although, previous works can be poorly correlated with the current study because this is the first time that this bleaching system (LaserWhite20) has been tested in vivo. In fact, it is already known that high concentrations (25–35%) of hydrogen peroxide (HP) itself can quickly produce enough radicals capable to react with tooth pigments [6]. However, we have demonstrated that at least immediately after tooth bleaching, the 38% HP for dental bleaching has shown improved results when combined with the 940-nm diode laser.
A few patients reported sensitivity in the treated areas upon completion of the treatment. After 48 h, all patients were cleared, and no reports of sensitivity or discomfort were reported. Moreover, even more than 1 year after the completion of the treatments, the pulp vitality of all teeth was preserved. In fact, it is claimed that the addition of dyes to the bleaching gels, as in the system studied here, results in improved absorption of light in the gel, i.e., superficially on the tooth surface, thus favoring teeth insulation and reducing the heating of the dental pulp due to photoactivation [26, 27]. Moreover, the photodynamic reaction triggered by laser interaction with the dye leads to the production of free radicals that might contribute to the improved bleaching process, as well [26].
The hazard to the dental structure is a great concern related to dental bleaching. Many studies were performed to verify the permeability of dental tissues to different concentrations of HP gels [28, 29]. The enamel behaves like a semi-permeable membrane, allowing the passage of water and other substances with small molecular size, such as oxygen ions present in the HP [2]. Accordingly, the Fick’s second law of diffusion states that diffusion is proportional to the surface, diffusion coefficient, and concentration and is inversely proportional to the diffusion distance [30]. A recent study has shown evidence that higher HP concentrations can reach dental pulp chambers more quickly than less concentrated products [31]. Nonetheless, light activation does not increase the average time for a 35% HP or 38% HP gel to reach the dental pulp chamber [14, 32,33,34]. In contrast, the main purpose of light application is to speed up the bleaching process and reduce the time of exposure of teeth surfaces to the HP. An in vitro study performed in human premolars with the same diode laser and parameters used in the current study has shown that the temperature rise in the pulp chamber is 2.73 °C when the tooth is photoactivated. While we have not measured the increase in the pulp chamber temperature when using the fiber tip, studies in the literature show that the pulp safety threshold is a temperature increase of 5.6 °C or less [35]. The laser-assisted treatment evaluated in the present study was well-tolerated by the patients, and the pulp vitality was preserved. The effect of light applied with no hand piece attached to the fiber should be better investigated in relation to cell viability, dental pulp temperature rise, and possible biological hazardous effects on this tissue and its surrounding.
A significant overall increase in whitening was observed for canines, irrespective of the treatment type. Similar results were previously reported when differences in color change between incisors and canines were investigated after dental bleaching [36, 37].
Conclusion
Within the limitations of this study, we conclude that the new protocol of 940-nm diode laser-assisted tooth whitening has shown effective in a short-term post-bleaching assessment. Future studies should be conducted to examine whether the above protocol is effective in a long-term trial.
References
Zekonis R, Matis BA, Cochran MA, Al Shetri SE, Eckert GJ, Carlson TJ (2003) Clinical evaluation of in-office and at-home bleaching treatments. Oper Dent 28:114–121
de Geus JL, Wambier LM, Kossatz S, Loguercio AD, Reis A (2016) At-home vs in-office bleaching: a systematic review and meta-analysis. Oper Dent 41:341–356
Haywood VB (1992) History, safety, and effectiveness of current bleaching techniques and applications of the nightguard vital bleaching technique. Quintessence Int 23:471–488
Hein DK, Ploeger BJ, Hartup JK, Wagstaff RS, Palmer TM, Hansen LD (2003) In-office vital tooth bleaching—what do lights add? Compend Contin Educ Dent 24:340–352
Tay LY, Kose C, Loguercio AD, Reis A (2009) Assessing the effect of a desensitizing agent used before in-office tooth bleaching. J Am Dent Assoc 140:1245–1251
Kossatz S, Dalanhol AP, Cunha T, Loguercio A, Reis A (2011) Effect of light activation on tooth sensitivity after in-office bleaching. Oper Dent 36:251–257
Marcondes M, Gandolfi Paranhos MP, Spohr AM, Mota EG, Lima da Silva IN, Souto AA, Burnett LH Jr (2008) The influence of Nd:YAG laser bleaching on physical and mechanical properties of the dental enamel. J Biomed Mater Res Part B: Appl Biomater 1:388–395
Strobl A, Gutknecht N, Franzen R, Hilgers RD, Lampert F, Meister J (2010) Laser-assisted in-office bleaching using a neodymium: yttrium-aluminium-garnet laser: an in vivo study. Laser Med Sci 25:503–509
Wetter NU, Walverde DA, Kato IT, Eduardo CDP (2004) Bleaching efficacy of whitening agents activated by xenon lamp and 960 nm diode radiation. Photomed Laser Surg 22:489–493
Dostalova T, Jelinkova H, Koranda P, Nemec M, Sulc J, Housova D, Miyagi M, Kokta MR (2003) Optical properties and surface structure comparison of tooth whitening using four laser systems and chemical action agents. Proc SPIE 4590:37–45
Cohen S, Parkins FM (1970) Bleaching tetracycline-stained vital teeth. Oral Surg Oral Med Oral Pathol 29:465–471
Gurgan S, Cakir FY, Yazici E (2010) Different light-activated in-office bleaching systems: a clinical evaluation. Lasers Med Sci 25:817–822
He LB, Shao MY, Tan K, Xu X, Li JY (2012) The effects of light on bleaching and tooth sensitivity during in-office vital bleaching: a systematic review and meta-analysis. J Dent 40:644653
Maran BM, Burey A, de Paris Matos T, Loguercio AD, Reis A (2017) In-office dental bleaching with light vs. without light: a systematic review and meta-analysis. J Dent S0300-5712(17)30283–X
Basting RT, Amaral FL, França FM, Flório FM (2012) Clinical comparative study of the effectiveness of and tooth sensitivity to 10% and 20% carbamide peroxide home-use and 35% and 38% hydrogen peroxide in-office bleaching materials containing desensitizing agents. Oper Dent 37(5):464–473
Fatima N (2016) In-vitro comparative study of in-office and home bleaching agents on surface micro-morphology of enamel. J Coll Physicians Pak 26(1):9–12
Paula S de S, Soares LE, do Espírito Santo AM, Martin AA, Cavalli V, Liporoni PC (2010) FT-Raman and energy dispersive X-ray fluorescence spectrometric analyses of enamel submitted to 38% hydrogen peroxide bleaching, an acidic beverage, and simulated brushing. Photomed Laser Surg 28(3):391–396
Buchalla W, Attin T (2007) External bleaching therapy with activation by heat, light or laser—a systematic review. Dent Mater 23:586–596
Tavares M, Stultz J, Newman M, Smith V, Kent R, Carpino E, Goodson JM (2003) Light augments tooth whitening with peroxide. J Am Dent Assoc 134:167–175
Goharkhay K, Schoop U, Wernisch J, Hartl S, De Moor R, Moritz A (2009) Frequency doubled neodymium: yttrium-aluminum-garnet and diode laser-activated power bleaching—pH, environmental scanning electron microscopy, and colorimetric in vitro evaluations. Laser Med Sci 24:339–346
Ontiveros JC, Paravina RD (2009) Color change of vital teeth exposed to bleaching performed with and without supplementary light. J Dent 37:840–847
Salem YM, Osman YI (2011) The effects of in-office vital bleaching and patient perception of the shade change. SADJ 66:72–76
Koçak S, Koçak MM, Sağlam BC (2014) Clinical comparison between the bleaching efficacy of light-emitting diode and diode laser with sodium perborate. Aust Endod J 40:17–20
Marson FC, Sensi LG, Vieira LC, Araújo E (2008) Clinical evaluation of in-office dental bleaching treatments with and without the use of light-activation sources. Oper Dent 33:15–22
Mondelli RF, Azevedo JF, Francisconi AC, Almeida CM, Ishikiriama SK (2012) Comparative clinical study of the effectiveness of different dental bleaching methods—two year follow-up. J Appl Oral Sci 20:435–443
De Moor RJ, Verheyen J, Diachuk A, Verheyen P, Meire MA, De Coster PJ, Keulemans F, De Bruyne M, Walsh LJ (2015) Insight in the chemistry of laser-activated dental bleaching. Sci World J 650492.
Verheyen P, Walsh LJ, Wernish J, Schoop U, Moritz A (2006) Laser-assisted bleaching. In Oral laser application, Quintessenz Verlags-Gmbh, Berlin, Germany, pp 407–448.
Camps J, De Franceschi H, Idir F, Roland C, About I (2007) Time-course diffusion of hydrogen peroxide through human dentin: clinical significance for young tooth internal bleaching. J Endod 33:455–459
Kwon SR, Oyoyo U, Li Y (2013) Effect of light activation on tooth whitening efficacy and hydrogen peroxide penetration: an in vitro study. J Dent 41:e39–e45
Pashley DH (1985) Dentin–predentin complex and its permeability: physiologic overview. J Dent Res 64:613–620
Torres CR, Souza CS, Borges AB, Huhtala MF, Caneppele TM (2013) Influence of concentration and activation on hydrogen peroxide diffusion through dental tissues in vitro. Sci World J 193241
Camargo SE, Valera MC, Camargo CH, Gasparoto Mancini MN, Menezes MM (2007) Penetration of 38% hydrogen peroxide into the pulp chamber in bovine and human teeth submitted to office bleach technique. J Endod 33(9):1074–1077
Coelho RA, Oliveira AG, Souza-Gabriel AE, Silva SR, Silva-Sousa YT, Silva RG (2011) Ex-vivo evaluation of the intrapulpal temperature variation and fracture strength in teeth subjected to different external bleaching protocols. Braz Dent J 22(1):32–36
Moncada G, Sepúlveda D, Elphick K, Contente M, Estay J, Bahamondes V, Fernandez E, Oliveira OB, Martin J (2013) Effects of light activation, agent concentration, and tooth thickness on dental sensitivity after bleaching. Oper Dent 38(5):467–476
Zach L, Cohen G (1965) Pulp response to externally applied heat. Oral Surg Oral Med Oral Pathol 19:515–530
Wetter NU, Branco EP, Deana AM, Pelino JE (2009) Color differences of canines and incisors in a comparative long-term clinical trial of three bleaching systems. Lasers Med Sci 24:941–947
Al-Karadaghi TS, Al-Saedi AA, Al-Maliky MA, Mahmood AS (2016) The effect of bleaching gel and (940 nm and 980 nm) diode lasers photoactivation on intrapulpal temperature and teeth whitening efficiency. Aust Endod J 42:112–118
Funding
MMM is supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico grants CNPq number 307874/2014-1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Ardekani, Y.T., Marques, M.M., Franzen, R. et al. Immediate clinical evaluation of a 940-nm diode laser-assisted in-office bleaching technique. Laser Dent Sci 2, 239–245 (2018). https://doi.org/10.1007/s41547-018-0042-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41547-018-0042-3