
Abstract
Positive psychology interventions hold great promise as schools around the world look to increase the wellbeing of young people. To reach this aim, a program was developed to generate positive emotions, as well as improve life satisfaction, mental toughness and perceptions of school kindness in 538 expatriate students in Dubai, United Arab Emirates. Starting in September 2019, the program included a range of positive psychology interventions such as gratitude, acts of kindness and mental contrasting as examples. Life satisfaction and mental toughness at mid-year were sustained or grew by the end of the year. Positive affect, emotional wellbeing and social wellbeing increased at post-intervention 1, compared to baseline. However, this improvement reverted to baseline levels at post-intervention 2, when data were collected during the COVID-19 pandemic. Only psychological wellbeing, negative affect, perceptions of control, and school kindness were increased at post-intervention 2. During the lockdown, students moved less, but slept and scrolled more. Those who extended their sleep duration reported greater wellbeing. Boosting wellbeing through the use of positive psychology interventions works – even in a pandemic – and extended sleep duration appears to be a driving factor for this observation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Positive psychology has grown since its debut, bringing with it a demand for programming designed to nurture wellbeing. An outgrowth of this is positive education, which considers schools to be apt settings in which psychological skills can be taught for increasing wellbeing (White & Kern, 2018). One way to impart these skills has been through positive psychology programs where youth learn to capitalize on the positive and overcome the negative (Chodkiewicz & Boyle, 2017; White & Kern, 2018). Such programs are growing globally (Hendriks et al., 2019; Kim et al., 2018), including in the Middle East/North Africa (MENA) region. These developments are timely as reports show that youth wellbeing is a serious concern across many nations (Hawke et al., 2020; Huang & Zhao, 2020; Marques de Miranda et al., 2020), with studies already recording increases in youth depression, anxiety, and suicidality (Lai et al., 2018; Lawrence et al., 2015; Twenge et al., 2019; World Health Organization, 2017) as well as declines in life satisfaction globally (Marquez & Long, 2021).
The sleep habits of young people have also received much attention given the close connection they have to a wide range of health and wellbeing outcomes (Matos et al., 2017; Palmer & Alfano, 2017; Roberts & Duong, 2014), including depression, anxiety, emotional regulation and school performance (Marino et al., 2021; Orchard et al., 2020). Adolescents commonly experience delayed circadian rhythmicity resulting in a preference for eveningness (Hagenauer et al., 2009; Hummer & Lee, 2016); consequently, later sleep timings are common in this age group. In fact, much evidence suggests a high proportion of teens globally are sleep deprived (Hysing et al., 2020; Matricciani et al., 2012), and more so relative to early school starts, which do not take their biology into account. While sleep has gained notoriety in adolescent health research, it has not commonly been included in positive psychology studies or examined as a contributor to wellbeing.
Recently, the COVID-19 pandemic, a protracted global public health crisis with its widespread physical, psychological, social, economic, and societal toll has interrupted lives, families, and institutions. This context has had wide-ranging effects on young people; some experienced better mental health and wellbeing, while others experienced worse (e.g., Mitra et al., 2021). While the current study was not intended to study the effects of the pandemic, its unexpected presence offered an interesting opportunity to examine the effects of such a program within this context. This event also allowed us to determine who did better and why, particularly with respect to other less commonly examined factors affecting youth, like sleep, as well as social media use/time online and physical activity.
2 Positive Psychology: Valuing Wellbeing
As “wellbeing” is multidimensional and entails both feeling good and functioning well, it is often used as an umbrella term for a wide range of concepts. While we retain the term for ease of discussion, there are nonetheless major ways in which wellbeing is understood. With a focus on feeling good, hedonic wellbeing contributes to human flourishing (Huta & Ryan, 2010) and is often measured by the presence of positive emotions and an absence or low frequency of negative emotions. Equally important is eudaimonic wellbeing (Ryff & Singer, 2008), more concerned with purpose in life, relationships, goal strivings and personal growth. While both forms of wellbeing are distinct, complementary (Huta & Waterman, 2014; Ryan & Huta, 2009) and necessary for a good life (Joshanloo, 2016), an absence of poor functioning, i.e., mental health issues like depression and anxiety, is also vital. The presence of wellbeing and absence of illness are increasingly being integrated into a definition of mental health (Bohlmeijer & Westerhof, 2021). At last, a cognitive appraisal of how satisfied individuals are with their lives as a whole (Diener et al., 2009) is another facet of wellbeing.
Positive psychology has done much to explore the benefits of wellbeing. For example, individuals with more positive affect and higher life satisfaction have a greater likelihood of obtaining a college degree and being employed (DeNeve & Oswald, 2012; Haase et al., 2012; Longhi et al., 2018; Turban et al., 2013). With greater life satisfaction, academic performance tends to rise (Bücker et al., 2018; Durlak et al., 2011; Suldo et al., 2008, 2011; Zi Jia et al., 2015), as do perceptions of academic ability and social support (Danielsen et al., 2009; Suldo & Huebner, 2006; Suldo et al., 2008) and school engagement (Heffner & Antaramian, 2016; Lewis et al., 2011). Higher wellbeing protects against mental health issues and resulting academic declines (Lyons et al., 2013). In particular, youth who demonstrate more social competence and engagement tend to experience less depression, loneliness, and anxiety into their twenties (Kansky et al., 2016; Richards & Huppert, 2011). Associated socioemotional skills also boost labour market success and higher earnings (Anghel & Balart, 2017; Lundberg, 2019; Sørensen & Krassel, 2019; Walsh et al., 2018).
While the presence of wellbeing contributes to a range of positive outcomes, mental health issues and its contributors, tend to do the opposite. Sleep has been consistently related to adolescent mental health (Matos et al., 2017; Palmer & Alfano, 2017; Roberts & Duong, 2014). Specifically, disturbed sleep predicts depression and anxiety, as well as their severity (Marino et al., 2021; Orchard et al., 2020). Studies have shown difficulties in emotional regulation management in adolescents, with parents noting teens greater oppositionality after a few nights of poor sleep (Baum et al., 2014). Lower quality and duration of sleep has also been associated with worse learning outcomes and school performance (Chaput et al., 2016; Hayes & Bainton, 2020; Hysing et al., 2016). In contrast, longer sleep duration predicts subjective wellbeing and life satisfaction (Kalak et al., 2014; Lai & Ma, 2020; Ness & Saksvik-Lehouillier, 2018; Yang & Cha, 2018), with one cross-sectional analysis (Thumann et al., 2019) observing that higher wellbeing scores initially were associated with longer sleep duration and fewer odds of sleep disturbances, suggesting a bi-directional relationship between the two factors.
A contributor to poor sleep is also time spent online (i.e., smartphone use, video games, social media, etc.) (Arora et al., 2014; Hysing et al., 2015; Lund et al., 2021). Time-consuming, it generates psycho-physiological arousal due to its content and disrupts circadian rhythms (Illingworth, 2020). Studies suggest that online activity is fueling low levels of wellbeing and mental health (Kleszczewska et al., 2018; Marques et al., 2017; Rees, 2017; Twenge et al., 2018; Vannucci et al., 2020), although some studies show no, or positive effects (Clarke et al., 2018; Jensen et al., 2019; Kovess-Masfety et al., 2016; Orben & Przybylski, 2019). For instance, during the pandemic, adolescents reporting more gratitude turned to social media more frequently to have meaningful peer conversations (Maheux et al., 2021), while those who connected more often with their peers experienced less loneliness (Ellis et al., 2020). The consensus seems to be that the impact of social media is dependent on how it is used, to what degree, by whom and with what pre-existing factors (Appel et al., 2020).
During the pandemic, rates of physical activity were also impacted due to a variety of lockdown measures (e.g., Karageorghis et al., 2021); yet, studies show that those who maintained or increased their activity experienced better wellbeing (Chen et al., 2020; Nie et al., 2021; Tandon et al., 2021; Wright et al., 2021). These findings are important in light of evidence showing that physical activity is known to reduce symptoms of mental disorders and improve life satisfaction (Chekroud et al., 2018; Lees & Hopkins, 2013; McDowell et al., 2019; Schuch et al., 2018; White et al., 2017). The reverse is also true: suspending physical activity is associated with decreases in subjective wellbeing (Sokić et al., 2021; Weinstein et al., 2017). How young people use their time appears to be impactful for wellbeing (Rees, 2017; Rees & Main, 2015).
2.1 Positive Psychology Interventions
Positive psychology interventions (PPIs), are the behavioral and cognitive strategies designed to generate greater states of wellbeing, including positive emotions, as well as the actions and thoughts that underpin behaviors known to enhance it, including sleep. Examples of PPIs include acts of kindness (Kerr et al., 2015; Pressman et al., 2015) and self-compassion (Warren et al., 2016). A systematic review that specifically explored the effect of gratitude interventions upon physical health revealed that, of eight, five reported a significant improvement to sleep quality (Boggiss et al., 2020), with single studies showing the same (Alkozei et al., 2019; Jackowska et al., 2016). Meta-analyses in clinical and general population samples (Carr et al., 2020; Chakhssi et al., 2018; Hendriks et al., 2018, 2020; Hone et al., 2015; Weiss et al., 2016; White et al., 2019) have confirmed the efficacy of PPIs on both hedonic and eudaimonic measures of wellbeing, including appraisals of life satisfaction.
Yet, effect sizes of PPIs are generally small with inconsistent dose effects (Fischer et al., 2020). For instance, Sin and Lyubomirsky’s (2009) meta-analysis found PPIs to have moderate effects in decreasing symptoms of depression (r = .31) and enhancing wellbeing (r = .29). Bolier et al.’s (2013) meta-analysis found smaller effect sizes (r = .17; d = 0.34) for subjective wellbeing, for psychological wellbeing (r = .10; d = 0.20) and for depression (r = .11; d = 0.23). White et al. (2019) re-evaluated both, citing that these studies had small sample sizes, the bias of which was pronounced, and when taken into account, the effect size of PPIs on wellbeing were small but still significant (approximately r = .10). Fischer et al.’s (2020) meta-analysis of past reviews also compared the effectiveness of PPIs with other types of interventions such as CBT and mindfulness on anxiety, depression, wellbeing, and stress. They found that for anxiety, PPIs had comparable or slightly larger effects than CBT and others; for depression, some PPIs did more poorly than other interventions; for wellbeing, PPIs were comparable to others except for mindfulness which had stronger effects; and for stress, no differences across intervention types were found.
Multi-component PPI (MPPI; Hendriks et al., 2020) programs offering a battery of PPIs administered over time with many measures collectively assessed, have also been examined. For instance, Shoshani and Steinmetz (2014) compared PPI use in a middle school, where optimism, gratitude, character strengths, positive emotions, and strengthening relationships were the aim. PPI groups showed less distress, depression and anxiety a year later and gains in optimism, self-esteem and self-efficacy, with controls showing the opposite. Similarly, Shoshani and Slone (2017) evaluated 32 weeks of positive education modules across 12 classes: relative to controls, treatment groups showed more prosocial behavior, subjective wellbeing, and empathy, but no change to mental health. Finally, in Kuwait (Lambert et al., 2019b) a program delivering weekly PPIs to almost 1,000 university and secondary students, showed that relative to controls three months later, wellbeing also rose.
Finally, the COVID-19 pandemic focused attention to the remediation of negative emotional experiences as emerging studies showed that loneliness, anxiety, stress, insomnia, fear and depression rose (Killgore et al., 2020; Kokou-Kpolou et al., 2020; Loades et al., 2020; Palgi et al., 2020; Shigemura et al., 2020). As PPI studies conducted during the pandemic are still forthcoming (i.e., Bono et al., 2020; Dominguez-Rodriguez et al., 2020; Prinzing et al., 2020), they too showed promise. For instance, Brouzos et al. (2021) evaluated a six-week online PPI program with Greek adults showing that positive outcomes persisted two weeks later. Moreover, these sustained outcomes resulted in greater positive emotion and resilience, as well as a reduction in levels of perceived loneliness, depression and anxiety. Dennis et al. (2020) explored the role of time orientation, examining which present-, past- or future-focused PPI had the largest effect on wellbeing during the pandemic, with the Best Possible Self (future-focused) exercise showing the strongest outcomes.
3 The Present Study
The purpose of this study, which incidentally occurred during the COVID-19 pandemic, was to determine whether the delivery of a MPPI program, developed by the primary author and components of which were previously tested in schools and universities (i.e., Lambert et al., 2019a, b), could impact satisfaction with life, positive and negative affect, indicators of mental health, perceptions of school kindness, and levels of mental toughness. PPIs included for example, positive reminiscing (Speer & Delgado, 2017), mental contrasting (Oettingen et al., 2015), and self-compassion (Neff & Pommier, 2013) (see Appendix for full content). Changes in physical activity, sleep duration, social media use and time playing video/online games were also explored.
3.1 Method
3.1.1 Participants
The MPPI program was delivered to 538 students (54.4% females) in grades 9 to 13 from a UAE private school. The breakdown was such: year 9 = 86 students (aged 13 to 14 years of age), year 10 = 118 (aged 14 to 15 years of age), year 11 = 109 (aged 15 to 16 years of age), year 12 = 115 (aged 16 to 17 years of age), year 13 = 101 (aged 17 to 18 years of age), and no response = 9. The school is host to mostly expatriate students, with the sample consisting of 18 Australians, 20 Canadians, six students from the Gulf Cooperation Council nations (GCC; Oman, Bahrain, Qatar, Saudi Arabia, UAE, or Kuwait), 99 Indians, 24 Pakistani nationals, 242 British, and 17 American students. An additional 127 students reported ‘Other’ nationalities, with nine reporting nothing. The sample sizes at post-intervention 1 (PO1) and post-intervention 2 (PO2) were 375 (55.6% females) and 265 (60.7% females), respectively. As there was neither control group, nor randomization, this sample comprised the total number of students taking part in the MPPI program.
3.1.2 Procedure
The MPPI program consisted of 15-to-20-minute weekly instruction. The program began in September 2019, when baseline measures were first taken, and were followed by post-test measures (PO1) at the end of December 2019, and a second set (PO2) at the end of June 2020. Measures were completed by students via a link provided by the counselling team, in which students provided their identification numbers to track scores over time. Identification numbers were removed at the end of the program and data were coded anonymously. No grades or incentives were given for participation. Ethical approval was granted by the primary author’s former institution and students and their parents provided informed written consent.
The weekly PPI program, the only programming being offered to students at this time, was delivered by teachers assigned to individual student groups with whom they met weekly for non-instructional contact time dedicated to catching up on classroom tasks, homework, guidance, etc. Approximately 15 to 20 minutes of this 60-minute time block was dedicated to the PPI program, where students were provided a short lesson on the topic at hand and engaged in either a writing, reflection, action, or discussion activity to be done in the class and with practice throughout the week. As the school shifted its instruction online at the start of the COVID-19 lockdown in the third week of March (2020), the same groups remained intact and program delivery continued online. Students did not return to the physical school for the remainder of the academic year from this point onwards.
3.1.3 Measures
Hedonic and eudaimonic measures were used showing acceptable internal consistency levels (Table 2).
The Positive & Negative Affect Schedule for Children-Short Form (PANAS-C-SF; Ebesutani et al., 2012) assesses positive and negative affect in children six to 18 years of age. There are ten items (i.e., joyful, cheerful, happy, lively, proud, miserable, mad, afraid, scared, sad) rated on a five-point Likert scale where higher ratings indicate a greater level of the given emotion based on the previous week.
The Mental Health Continuum Short Form (MHC-SF; Keyes, 2009) measures social wellbeing (social integration, contribution, growth, social acceptance, social interest), emotional wellbeing (positive emotion and life satisfaction, considered hedonic wellbeing), and psychological wellbeing (autonomy, personal growth, self-acceptance, environmental mastery, positive relations, and life purpose, considered eudaimonic wellbeing). The 14-item scale has been validated across cultural contexts (Joshanloo et al., 2013; Khumalo et al., 2012) and has good test-retest reliability (Lamers et al., 2012).
The Student Satisfaction with Life Scale (SSLS) (Huebner, 1991); This seven-item measure of life satisfaction in children as young as eight years has acceptable internal consistency, a unidimensional factor structure, and adequate temporal stability. An item example includes, “My life is better than most kids,” and “I have what I want in life.”
The School Kindness Scale (Binfet et al., 2016) is a five-item measure of school-based kindness using a five-point Likert type scale. Items include students’ perceptions of the frequency of classroom kindness (“Kindness happens regularly in my classroom”) and whether it is encouraged (“The adults in my school model kindness”).
The Mental Toughness Scale for Adolescents (MTS-A; McGeown et al., 2018) has 18 items measuring: (1) Control: feeling in control of one’s life and emotions; (2) Commitment: remaining steadfast in the face of goal pursuit despite difficulty; (3) Challenge: accepting threat as opportunities for growth; (4) Confidence: having faith in one’s personal and interpersonal abilities (Clough et al., 2002). Internal consistency (alpha) estimates range from 0.70 to 0.79 (Gerber et al., 2018; Lang et al., 2019; McGeown et al., 2018).
Time-use was measured using five-point Likert scales for a. physical activity (“In an average week, how many minutes of physical activity do you do? 1) 30 minutes or less; 2) 60 minutes or less; 3) 90 minutes or less; 4) 120 minutes or less; 5) More than 120 minutes”); b. hours of sleep (“How many hours of sleep, on average, do you get each night? 1) Less than 5; 2) Between 5 - 7; 3) Between 7 - 9; 4) More than 9”); c. social media use (“How much time do you spend on social media each day? 1) None; 2) Less than 1 hour; 3) Up to 3 hours: 4) Between 4 and 6: 5) More than 6”); and d. time playing video/online games (“How much time do you spend playing video or online games each day? 1) None; 2) Less than 1 hour; 3) Up to 3 hours; 4) Between 4 - 6; 5) More than 6”).
4 Statistical Methods
To examine if the intervention had a significant effect on the outcomes of the study at PO1, we performed paired-sample t-tests for all the variables of the study. Next, to examine if the intervention had a significant effect on the study’s variables at PO2 (compared to pre-intervention), we performed another set of paired-sample t-tests. To study changes in students’ daily activities as a consequence of the lockdown measures (i.e., between PO1 and PO2), we performed another set of paired-sample t-tests for variables reporting on daily activities. Finally, to study how changes in daily habits impacted the likelihood of experiencing increased wellbeing, we created a binary variable for each of the wellbeing items and scales studied (1= the score in the wellbeing item/scale increased; 0= the score in the wellbeing item/scale did not increase) and estimated logistic regression models. Data was analyzed using the SPSS 26 and JASP 0.12.2.0.
5 Results
Descriptive statistics for the variables of the study at the three time points are presented in Table 1, while Table 2 presents the intercorrelations between all study-related variables at the pre-intervention phase. All variables were positively correlated with each other, except for Negative Affect which showed an inverse relationship with all other variables (as expected).
Overall, the mean levels of the positive outcomes of the study increased as a result of the intervention, whereas negative affect declined post-intervention. The results (Table 3) suggest that the post-intervention increases in nine of the variables were statistically significant: MHC total, MHC emotional (hedonic), MHC social, Positive affect, MTS total, interpersonal confidence, emotional control, life control, and student life satisfaction. Effect sizes (Cohen's ds) ranged between 0.111 and 0.212. A Cohen’s d smaller than .20 is considered small, between .20 and .50 is considered medium, and greater than .80 is considered large (Valladares-Neto, 2018). Thus, these effect sizes are in the small range.
In Table 4, increases in nine of the variables were statistically significant when comparing baseline to PO2: MHC psychological (eudaimonic), Negative affect, MTS total, challenge, interpersonal confidence, emotional control, life control, student life satisfaction, and school kindness. Effect sizes (Cohen's ds) ranged between 0.139 and 0.289, and were bigger on average at PO2.
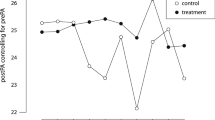
The results show that the increases in life satisfaction and four MTS variables (MTS total, interpersonal confidence, emotional control, and life control) at PO1 were sustained or grew at PO2. Positive affect and three of the MHC variables (MHC total, MHC emotional (hedonic), and MHC social) significantly increased at PO1 but reverted near to their pre-intervention levels at PO2. Interestingly, four of the variables did not increase significantly at PO1; yet, showed significant increases at PO2: MHC psychological (eudaimonic), PANAS negative affect, MTS challenge, and school kindness scale.
Further, , on average, the lockdown meant less physical activity, but more sleep, social media use, and playing video/online games. Out of those who responded both in PO1 and PO2, the numbers for these time-use variables were the following: sleep [Decreased: 21 (11.06%); Same: 130 (68.42%); Increased: 39 (20.52%)]; physical activity [Decreased: 50 (26.32%); Same: 113 (59.47%); Increased: 27 (14.21%)]; social media; [Decreased: 16 (8.42%); Same: 102 (53.68%); Increased: 72 (37.89%)]; videogames [Decreased: 16 (8.42%); Same: 115 (60.53%); Increased: 59 (31.05%)]. Further supporting these trends, Table 5 shows that, for the four time-use Likert scales (see more details about the scales in section 3.1.3 Measures), the effect sizes (Cohen's ds) were statistically significant and ranged between 0.118 and 0.472.
Table 6 results, reported in odds ratios (OR), shows that most of the statistically significant effects are observed for changes in hours of sleep. Compared to those who did not report sleeping more during the lockdown (i.e. PO2), those who did were three times more likely to report agreement with the statement 'My life is going well' compared to the pre-lockdown situation (i.e. PO1). They were three times more likely to report positive affect, twice less likely to report more negative affect and 4.45 times more likely to report greater emotional (hedonic) wellbeing. Statistically significant effects were absent for other activities, with a few exceptions for some specific items. For example, students who increased their physical activity in lockdown seemed more likely to report greater psychological (eudaimonic) and social wellbeing, although effects were statistically significant for three social wellbeing items only.
Out of those who responded both in PO1 and PO2, these are the numbers for the time-use variables:
-
Sleep [Decreased: 21 (11.06%); Same: 130 (68.42%); Increased: 39 (20.52%)]
-
Physical activity [Decreased: 50 (26.32%); Same: 113 (59.47%); Increased: 27 (14.21%)]
-
Social media [Decreased: 16 (8.42%); Same: 102 (53.68%); Increased: 72 (37.89%)]
-
Videogames [Decreased: 16 (8.42%); Same: 115 (60.53%); Increased: 59 (31.05%)]
6 Discussion
This study sought to determine the effects of a PPI program on student wellbeing, while also considering the impacts of sleep, physical activity and time spent online. The COVID-19 pandemic transpired during this time, but nonetheless allowed interesting insights to emerge. For instance, students reported greater life satisfaction and decreases to negative affect (from pre, PO1 to PO2) despite experiencing a pandemic, albeit with smaller effect sizes than those presented in prior studies (Chakhssi et al., 2018; Hendriks et al., 2018; Hendriks et al., 2020; Weiss et al., 2016; White et al., 2019). This suggests that PPIs may have counteracted at least some associated pandemic challenges. Scores on overall mental toughness and its sub-components (interpersonal confidence, emotional control, life control) increased over the two follow up time points, suggesting that coping with pandemic-related stressors may have equipped adolescents with necessary skills pertaining to resilience, which the intervention may also have reinforced. Gains in the areas of positive affect on the PANAS and MHC, overall mental health functioning and social wellbeing (i.e., social integration, contribution, growth, social acceptance, social interest) significantly increased by PO1 (prior to the pandemic). Yet, these were lost by PO2 (during the pandemic), with scores returning close to baseline.
At PO2 in June, three variables which had not increased at the first post-test did, including scores on psychological wellbeing (eudaimonic; autonomy, personal growth, self-acceptance, environmental mastery, positive relations with others, purpose in life), perceptions of school kindness, and feeling in control of challenge. It is likely that teachers showed more compassion to students, impacting their perceptions. Feeling in control of challenge may be explained by the fact that students adjusted to the lockdown and/or online learning conditions, or used the PPIs to a greater degree. It may also be that the impact of the PPIs took longer to emerge, or that students included in the pre-PO2 analyses (a subset of those in the pre-PO1 analysis) were more diligent in completing all three assessments.
While these factors may not have been affected by the pandemic, studies during this time suggest that adolescents were at high risk for low life satisfaction, symptoms of depression and anxiety, and loneliness and boredom (COVIDdatahub.com; Guessoum et al., 2020; Loades et al., 2020; Rodríguez-Rey et al., 2020), although other studies showed that anxiety decreased and wellbeing, as well as sleep, increased (Mitra et al., 2021; Widnall et al., 2020). As older students tend to score lower on measures of wellbeing, especially as their relationships with teachers weaken across adolescence and become strained during online learning (Danielsen et al., 2011; Diseth & Samdal, 2014; García-Moya et al., 2015; Moore et al., 2018; Newland et al., 2018; Rapee et al., 2019), our results raise interesting avenues of investigation.
Mental toughness (MT) was not an explicit part of the program; yet, the use of PPIs generated increases in its components. It is possible the skills underlying the PPIs overlapped with those used in MT, as it too, aims to enable psychological resources to support positive functioning (Drinkwater et al., 2019; Lin et al., 2017; Papageorgiou et al., 2019). As MT is correlated with life satisfaction, it may also tap onto perceptions relative to this factor (i.e., Crust & Clough, 2005; Dagnall et al., 2019; Gerber et al., 2013; Marchant et al., 2009). It is even possible that the pandemic, rather than our program, brought forward the skills of MT.
In the lockdown period, students spent less time doing physical activity and more time sleeping, using social media and playing video/online games. Our data show that more screen-based activity was not associated with wellbeing. While research suggests negative effects on wellbeing (Kleszczewska et al., 2018; Marques et al., 2017; Rees, 2017; Twenge et al., 2017, 2018), the extraordinary context may explain our results. In lockdown, the only way for students to connect with friends was through social media, which may have buffered against negative effects, as prior studies have shown (Magson et al., 2021). Conversely, students who increased their hours of sleep and physical activity were more likely to experience greater wellbeing, also in line with previous studies (Chen et al., 2020; Kalak et al., 2014; Lai & Ma, 2020; Ness & Saksvik-Lehouillier, 2018; Wright et al., 2021; Yang & Cha, 2018). For physical activity, effects were only found for increased psychological (eudaimonic) and social wellbeing.
Finally, our findings showed significant associations between increased sleep duration and several positive outcomes including one component of life satisfaction, as well as a significant decrease in the odds of negative affect (total score as well as sadness). The most striking observation was the association between extended sleep duration and positive mood, where the odds for the total positive affect was three-fold. The odds for all positive mood states assessed, except for one (proud), were significantly elevated where the ORs ranged from 2.30 (joyful) to 3.47 (happy). Increased sleep duration was also associated with a 2.66 odds of being good at managing the responsibilities of life and a 2.10 odds of having direction/meaning in life (components of psychological (eudaimonic) wellbeing). As previous research has identified positive effects on subjective sleep quality following engagement in gratitude interventions (i.e., Alkozei et al., 2019; Boggiss et al., 2020; Jackowska et al., 2016), it is possible that greater wellbeing derived from our PPIs may have contributed to enhanced sleep duration as Thumann et al. (2019) showed, although PPIs themselves may have contributed to greater sleep duration directly. Extra time in bed in the absence of a school commute may also have contributed.
7 Limitations, Future Directions and Implications
Our study was impacted by the global COVID-19 pandemic, which altered its delivery from in-person to online. Program gains after PO1 may have been influenced by the kindness of teachers or greater sleep; equally, better relationships with parents, and less pressure to excel academically. We cannot dismiss the possibility that our results were obtained solely due to students receiving positive attention during this time (Ciarrochi et al., 2016), particularly as good teacher-student relationships impact student wellbeing (García-Moya et al., 2015; Moore et al., 2018; Newland et al., 2018). Further, as is often the case with school-wide programs (i.e., Mackenzie & Williams, 2018), our lack of control group and randomization of participants make our results difficult to generalize. These are threats to the internal validity of our study, given that the switch to online learning and the pandemic also acted as confounding variables. We are still confident that the program was impactful as its outcomes were evident at PO1, although levels of missing data in PO1 and PO2 were high for most variables studied as less than half of all the participants (n= 538) responded to the questionnaire in both PO1 and PO2.
The restrictions imposed during the pandemic also significantly influenced the behavior of students; a total shutdown was experienced for several weeks whereby, as an example, electronic permissions were required to leave the home for 90 minutes per week and this was restricted to two household members for the purpose of grocery shopping only. Curfews were strictly enforced. While restrictions eased over time, the lack of ability to do anything but sleep, engage in social media and exercise should be kept in mind. The high socioeconomic status of students may also have buffered some of the negative effects generated by the restrictions and afforded them the ability to take part in more physical activity due to having a backyard or pool, for instance (i.e., Fegert et al., 2020).
MPPI programs contribute to wellbeing; however, in the case of our study, PPIs had small effect sizes for a range of reasons described and perhaps others still unknown. Nonetheless, greater wellbeing, given its positive impacts on educational, health and social outcomes as examples, remains a worthy endeavor for schools to consider. What was more surprising in our results was the significant impact of sleep and its potential as an inexpensive intervention. Adjusting school start times, 8:30am onwards, and introducing sleep hygiene programming are policy-driven solutions that have shown positive academic and mental health outcomes (Dunster et al., 2018; Gee et al., 2019; Gruber, 2017; Hayes & Bainton, 2020; Marino et al., 2021; Orchard et al., 2020; Scott et al., 2021; Troxel & Wolfson, 2017). We further echo findings recommending that teacher wellbeing be addressed (Lawler et al., 2017; Marquez & Main, 2021), given its links to student wellbeing and academic performance (Harding et al., 2019; Milkie & Warner, 2011; Oberle & Schonert-Reichl, 2016). Overall, a more systemic view of wellbeing must be promoted where MPPI programs are extended to improve the overall school climate so that the wellbeing of all stakeholders is supported (Marquez & Inchley, 2020).
8 Conclusion
The factors leading to wellbeing needed attention prior to the pandemic and for many students, schools continue to be the only place where wellbeing needs can be met (Golberstein et al., 2020). Our study indeed documented the effects of PPIs on student wellbeing in the UAE and given its timing, our results showed they can also be useful in trying times. However, for positive psychology to become globally relevant and locally useful, more research will contribute to the regional pool of data sorely needed and currently unavailable in Dubai (OECD, 2021), towards the development of school-based wellbeing policies. Yet, our study also highlights that schools need not make expensive interventions, attention to sleep is also compelling. As mental health concerns are set to outlive the pandemic (Brooks et al., 2020), wellbeing instruction through the use of PPIs in the classroom, as well as sleep-promoting programs, are essential for schools to adopt if students are to thrive, perform and be well going forward.
References
Alkozei, A., Smith, R., Kotzin, M. D., Waugaman, D. L., & Killgore, W. (2019). The association between trait gratitude and self-reported sleep quality is mediated by depressive mood state. Behavioral Sleep Medicine, 17(1), 41–48. https://doi.org/10.1080/15402002.2016.1276017
Anghel, B., & Balart, P. (2017). Non-cognitive skills and individual earnings: New evidence from PIAAC. SERIEs, 8(4), 417–473. https://doi.org/10.1007/s13209-017-0165-x
Appel, M., Marker, C., & Gnambs, T. (2020). Are social media ruining our lives? A review of meta-analytic evidence. Review of General Psychology, 24(1), 60–74. https://doi.org/10.1177/1089268019880891
Arora, T., Broglia, E., Thomas, G. N., & Taheri, S. (2014). Associations between specific technologies and adolescent sleep quantity, sleep quality, and parasomnias. Sleep Medicine, 15(2), 240–247. https://doi.org/10.1016/j.sleep.2013.08.799
Auyeung, L., & Mo, P. K. H. (2019). The efficacy and mechanism of online positive psychological intervention (PPI) on improving well-being among Chinese university students: A pilot study of the best possible self (BPS) intervention. Journal of Happiness Studies, 20, 2525–2550. https://doi.org/10.1007/s10902-018-0054-4
Baum, K. T., Desai, A., Field, J., Miller, L. E., Rausch, J., & Beebe, D. W. (2014). Sleep restriction worsens mood and emotion regulation in adolescents. Journal of Child Psychology and Psychiatry, 55(2), 180–190. https://doi.org/10.1111/jcpp.12125
Boggiss, A. L., Consedine, N. S., Brenton-Peters, J. M., Hofman, P. L., & Serlachius, A. S. (2020). A systematic review of gratitude interventions: Effects on physical health and health behaviors. Journal of Psychosomatic Research, 135, 110165. https://doi.org/10.1016/j.jpsychores.2020.110165
Bohlmeijer, E. T., & Westerhof, G. J. (2021). A new model for sustainable mental health: Integrating well-being into psychological treatment. In J. N. Kirby & P. Gilbert (Eds.), Making an impact on mental health: The applications of psychological research (pp. 153–188). Routledge/Taylor & Francis Group. https://doi.org/10.4324/9780429244551-7
Bolier, L., & Abello, K. M. (2014). Online positive psychological interventions: State of the art and future directions. In A. C. Parks & S. M. Schueller (Eds.), The Wiley Blackwell handbook of positive psychological interventions (pp. 286–309). Wiley Blackwell. https://doi.org/10.1002/9781118315927.ch16
Bolier, L., Haverman, M., Westerhof, G. J., Riper, H., Smit, F., & Bohlmeijer, E. (2013). Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health, 13, 119. https://doi.org/10.1186/1471-2458-13-119
Bono, G., Reil, K., & Hescox, J. (2020). Stress and wellbeing in college students during the COVID-19 pandemic: Can grit and gratitude help? International Journal of Wellbeing, 10(3), 39–57. https://doi.org/10.5502/ijw.v10i3.1331
Bowers, J. M., & Moyer, A. (2017). Effects of school start time on students’ sleep duration, daytime sleepiness, and attendance: A meta-analysis. Sleep Health, 3(6), 423–431. https://doi.org/10.1016/j.sleh.2017.08.004
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–920. https://doi.org/10.1016/S0140-6736(20)30460-8
Brouzos, A., Vassilopoulos, S. P., Baourda, V. C., Tassi, C., Stavrou, V., Moschou, K., & Brouzou, K. O. (2021). “Staying Home – Feeling Positive”: Effectiveness of an on-line positive psychology group intervention during the COVID-19 pandemic. Current Psychology. https://doi.org/10.1007/s12144-021-01613-x
Bücker, S., Nuraydin, S., Simonsmeier, B. A., Schneider, M., & Luhmann, M. (2018). Subjective well-being and academic achievement: A meta-analysis. Journal of Research in Personality, 74, 83–94. https://doi.org/10.1016/j.jrp.2018.02.007
Carr, A., Cullen, K., Keeney, C., Canning, C., Mooney, O., Chinseallaigh, E., & O’Dowd, A. (2021). Effectiveness of positive psychology interventions: A systematic review and meta-analysis. The Journal of Positive Psychology, 16(6),749–769. https://doi.org/10.1080/17439760.2020.1818807
Chakhssi, F., Kraiss, J. T., Sommers-Spijkerman, M., & Bohlmeijer, E. T. (2018). The effect of positive psychology interventions on well-being and distress in clinical samples with psychiatric or somatic disorders: A systematic review and meta-analysis. BMC Psychiatry, 18(1), 211. https://doi.org/10.1186/s12888-018-1739-2
Chan, C. S., Poon, C. Y. S., Leung, J. C. Y., Lau, K. N. T., & Lau, E. Y. Y. (2018). Delayed school start time is associated with better sleep, daytime functioning, and life satisfaction in residential high-school students. Journal of Adolescence, 66, 49–54. https://doi.org/10.1016/j.adolescence.2018.05.002
Chaput, J. P., Gray, C. E., Poitras, V. J., Carson, V., Gruber, R., Olds, T., Weiss, S. K., Connor Gorber, S., Kho, M. E., Sampson, M., Belanger, K., Eryuzlu, S., Callender, L., & Tremblay, M. S. (2016). Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Applied physiology, nutrition, and metabolism/Physiologie appliquee, nutrition et metabolisme, 41(6 Suppl 3), S266–S282. https://doi.org/10.1139/apnm-2015-0627
Chekroud, S. R., Gueorguieva, R., Zheutlin, A. B., Paulus, M., Krumholz, H. M., Krystal, J. H., & Chekroud, A. M. (2018). Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. The Lancet Psychiatry, 5(9), 739–746. https://doi.org/10.1016/s2215-0366(18)30227-x
Chen, F., Zheng, D., Liu, J., Gong, Y., Guan, Z., & Lou, D. (2020). Depression and anxiety among adolescents during COVID-19: A cross-sectional study. Brain, Behavior, and Immunity, 88, 36–38. https://doi.org/10.1016/j.bbi.2020.05.061
Chodkiewicz, A. R., & Boyle, C. (2017). Positive psychology school-based interventions: A reflection on current success and future directions. Review of Education, 5(1), 60–86. https://doi.org/10.1002/rev3.3080
Ciarrochi, J., Atkins, P. W. B., Hayes, L. L., Sahdra, B. K., & Parker, P. (2016). Contextual positive psychology: Policy recommendations for implementing positive psychology into schools. Frontiers in Psychology, 7, 1561. https://doi.org/10.3389/fpsyg.2016.01561
Clarke, J. L., Algoe, S. B., & Green, M. C. (2018). Social network sites and well-being: The role of social connection. Current Directions in Psychological Science, 27, 32–37. https://doi.org/10.1177/0963721417730833
COVIDdatahub.com (2020). Imperial College London/YouGov/Covid-19 Behaviour Tracker: Life Satisfaction Dashboard. https://ichpanalytics.imperialcollegehealthpartners.com/t/BDAU/views/YougovCovid-19TrackerLifeSatisfaction-20200622_15961947288210/LifeSatisfaction?:iid=4&:isGuestRedirectFromVizportal=y&:embed=y
Crust, L., & Clough, P. J. (2005). Relationship between mental toughness and physical endurance. Perceptual and Motor Skills, 100, 192–194. https://doi.org/10.2466/pms.100.1.192-194
Dagnall, N., Denovan, A., Papageorgiou, K. A., Clough, P. J., Parker, A., & Drinkwater, K. G. (2019). Psychometric assessment of Shortened Mental Toughness Questionnaires (MTQ): Factor structure of the MTQ-18 and the MTQ-10. Frontiers in Psychology, 10. https://doi.org/10.3389/fpsyg.2019.01933
Danielsen, A. G., Breivik, K., & Wold, B. (2011). Do perceived academic competence and school satisfaction mediate the relationships between perceived support provided by teachers and classmates, and academic initiative? Scandinavian Journal of Educational Research, 55(4), 379–401. https://doi.org/10.1080/00313831.2011.587322
Danielsen, A. G., Samdal, O., Hetland, J., & Wold, B. (2009). School-related social support and students' perceived life satisfaction. The Journal of Educational Research, 102(4), 303–318. https://doi.org/10.3200/JOER.102.4.303-320
DeNeve, J. E., & Oswald, A. (2012). Estimating the influence of life satisfaction and positive affect on later income using sibling fixed effects. Proceedings of the National Academy of Sciences of the USA, 109(49), 19953–19958. https://doi.org/10.1073/pnas.1211437109
Dennis, A., Ogden, J., & Hepper, E. G. (2022). Evaluating the impact of a time orientation intervention on well-being during the COVID-19 lockdown: Past, present or future? The Journal of Positive Psychology, 17(2), 419–429. https://doi.org/10.1080/17439760.2020.1858335
Diseth, Å., & Samdal, O. (2014). Autonomy support and achievement goals as predictors of perceived school performance and life satisfaction in the transition between lower and upper secondary school. Social Psychology of Education, 17(2), 269–291. https://doi.org/10.1007/s11218-013-9244-4
Dominguez-Rodriguez, A., De La Rosa-Gómez, A., Hernández Jiménez, M. J., Arenas-Landgrave, P., Martínez-Luna, S. C., Alvarez Silva, J., et al. (2020). A self-administered multicomponent Web-based mental health intervention for the Mexican population during the COVID-19 pandemic: Protocol for a randomized controlled trial. JMIR Research Protocols, 9(11), e23117. https://doi.org/10.2196/23117
Drinkwater, K., Dagnall, N., Denovan, A., & Parker, A. (2019). The moderating effect of mental toughness: Perception of risk and belief in the paranormal. Psychological Reports, 122, 268–287. https://doi.org/10.1177/0033294118756600
Dunster, G. P., de la Iglesia, L., Ben-Hamo, M., Nave, C., Fleischer, J. G., Panda, S., & Horacio, O. (2018). Sleepmore in Seattle: Later school start times are associated with more sleep and better performance in high school students. Science. Advances, 4(12), eaau6200. https://doi.org/10.1126/sciadv.aau6200
Durlak, J. A., Weissberg, R. P., Dymnicki, A. B., Taylor, R. D., & Schellinger, K. B. (2011). The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Development, 82(1), 405–432. https://doi.org/10.1111/j.1467-8624.2010.01564.x
Ebesutani, C., Regan, J., Smith, A., Reise, S., Higa-McMillan, C., & Chorpita, B. F. (2012). The 10-item positive and negative affect schedule for children, child and parent shortened versions: Application of item response theory for more efficient assessment. Journal of Psychopathology and Behavioral Assessment, 34, 191–203. https://doi.org/10.1007/s10862-011-9273-2
Ellis, W. E., Dumas, T. M., & Forbes, L. M. (2020). Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Canadian Journal of Behavioural Science, 52(3), 177–187. https://doi.org/10.1037/cbs0000215
Fegert, J. M., Vitiello, B., Plener, P. L., & Clemens, V. (2020). Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child and Adolescent Psychiatry and Mental Health, 14, 20. https://doi.org/10.1186/s13034-020-00329-3
Fischer, R., Bortolini, T., Karl, J. A., Zilberberg, M., Robinson, K., Rabelo, A., et al. (2020). Rapid review and meta-meta-analysis of self-guided interventions to address anxiety, depression, and stress during COVID-19 social distancing. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.563876
García-Moya, I., Brooks, F., Morgan, A., & Moreno, C. (2015). Subjective well-being in adolescence and teacher connectedness: A health asset analysis. Health Education Journal, 74(6), 641–654. https://doi.org/10.1177/0017896914555039
Gee, B., Orchard, F., Clarke, E., Joy, A., Clarke, T., & Reynolds, S. (2019). The effect of non-pharmacological sleep interventions on depression symptoms: A meta-analysis of randomised controlled trials. Sleep Medicine Reviews, 43, 118–128. https://doi.org/10.1016/j.smrv.2018.09.004
Gerber, M., Best, S., Meerstetter, F., Walter, M., Ludyga, S., Brand, S., et al. (2018). Effects of stress and mental toughness on burnout and depressive symptoms: A prospective study with young elite athletes. Journal of Science and Medicine in Sport, 21(12), 1200–1205. https://doi.org/10.1016/j.jsams.2018.05.018
Gerber, M., Brand, S., Feldmeth, A. K., Lang, C., Elliot, C., Holsboer-Trachsler, E., & Pühse, U. (2013). Adolescents with high mental toughness adapt better to perceived stress: A longitudinal study with Swiss vocational students. Personality and Individual Differences, 54(7), 808–814. https://doi.org/10.1016/j.paid.2012.12.003
Golberstein, E., Wen, H., & Miller, B. F. (2020). Coronavirus disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatrics, 174(9), 19–820. https://doi.org/10.1001/jamapediatrics.2020.1456
Gruber, R. (2017). School-based sleep education programs: A knowledge-to-action perspective regarding barriers, proposed solutions, and future directions. Sleep Medicine Reviews, 36, 13–28. https://doi.org/10.1016/j.smrv.2016.10.001
Guessoum, S. B., Lachal, J., Radjack, R., Carretier, E., Minassian, S., Benoit, L., & Moro, M. R. (2020). Adolescent psychiatric disorders during the COVID-19 pandemic and lockdown. Psychiatry Research, 291, 113264. https://doi.org/10.1016/j.psychres.2020.113264
Haase, C. M., Poulin, M. J., & Heckhausen, J. (2012). Happiness as a motivator. Personality and Social Psychology Bulletin, 38, 1093–1104. https://doi.org/10.1177/0146167212444906
Hagenauer, M. H., Perryman, J. I., Lee, T. M., & Carskadon, M. A. (2009). Adolescent changes in the homeostatic and circadian regulation of sleep. Developmental Neuroscience, 31(4), 276–284. https://doi.org/10.1159/000216538
Harding, S., Morris, R., Gunnell, D., Ford, T., Hollingworth, W., Tilling, K., et al. (2019). Is teachers’ mental health and wellbeing associated with students’ mental health and wellbeing? Journal of Affective Disorders, 242, 180–187. https://doi.org/10.1016/j.jad.2018.08.080
Hawke, L. D., Barbic, S., Voineskos, A., Szatmari, P., Cleverley, K., Hayes, E., et al. (2020). Impacts of COVID-19 on youth mental health, substance use, and wellbeing: A rapid survey of clinical and community samples. Canadian Journal of Psychiatry, 65(10), 701–709. https://doi.org/10.1177/0706743720940562
Hayes, B., & Bainton, J. (2020). The impact of reduced sleep on school related outcomes for typically developing children aged 11–19: A systematic review. School Psychology International, 41(6), 569–594. https://doi.org/10.1177/0143034320961130
Heffner, A. L., & Antaramian, S. P. (2016). The role of life satisfaction in predicting student engagement and achievement. Journal of Happiness Studies, 17(4), 1681–1701. https://doi.org/10.1007/s10902-015-9665-1
Hendriks, T., Schotanus-Dijkstra, M., Hassankhan, A., de Jong, J., & Bohlmeijer, E. (2020). The efficacy of multi-component positive psychology interventions: A systematic review and meta-analysis of randomized controlled trials. Journal of Happiness Studies, 21, 357–390. https://doi.org/10.1007/s10902-019-00082-1
Hendriks, T., Schotanus-Dijkstra, M., Hassankhan, A., Graafsma, T., Bohlmeijer, E., & de Jong, J. (2018). The efficacy of positive psychology interventions from non-Western countries: A systematic review and meta-analysis. International Journal of Wellbeing, 8(1), 71–98. https://doi.org/10.5502/ijw.v8i1.711
Hendriks, T., Warren, M. A., Schotanus-Dijkstra, M., Hassankhan, A., Graafsma, T., Bohlmeijer, E., & de Jong, J. (2019). How WEIRD are positive psychology interventions? A bibliometric analysis of randomized controlled trials on the science of well-being. The Journal of Positive Psychology, 14(4), 489–501. https://doi.org/10.1080/17439760.2018.1484941
Hone, L. C., Jarden, A., & Schofield, G. M. (2015). An evaluation of positive psychology intervention effectiveness trials using the re-aim framework: A practice-friendly review. The Journal of Positive Psychology, 10(4), 303–322. https://doi.org/10.1080/17439760.2014.965267
Huang, Y., & Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Research, 288, 112954. https://doi.org/10.1016/j.psychres.2020.112954
Hummer, D. L., & Lee, T. M. (2016). Daily timing of the adolescent sleep phase: Insights from a cross-species comparison. Neuroscience and Biobehavioral Reviews, 70, 171–181. https://doi.org/10.1016/j.neubiorev.2016.07.023
Huta, V., & Ryan, R. M. (2010). Pursuing pleasure or virtue: The differential and overlapping well-being benefits of hedonic and eudaimonic motives. Journal of Happiness Studies, 11, 735–762. https://doi.org/10.1007/s10902-009-171-4
Huta, V., & Waterman, A. S. (2014). Eudaimonia and its distinction from hedonia: Developing a classification and terminology for understanding conceptual and operational definitions. Journal of Happiness Studies, 15, 1425-1456. 10.100/s10902-013-9485-0
Hysing, M., Harvey, A. G., Linton, S. J., Askeland, K. G., & Sivertsen, B. (2016). Sleep and academic performance in later adolescence: Results from a large population-based study. Journal of Sleep Research, 25(3), 318–324. https://doi.org/10.1111/jsr.12373
Hysing, M., Heradstveit, O., Harvey, A. G., Nilsen, S. A., Bøe, T., & Sivertsen, B. (2022). Sleep problems among adolescents within child and adolescent mental health services. An epidemiological study with registry linkage. European Child & Adolescent Psychiatry, 31(1), 121–131. https://doi.org/10.1007/s00787-020-01676-4
Hysing, M., Pallesen, S., Stormark, K. M., Jakobsen, R., Lundervold, A. J., & Sivertsen, B. (2015). Sleep and use of electronic devices in adolescence: Results from a large population-based study. BMJ Open, 5, e006748. https://doi.org/10.1136/bmjopen-2014-006748
Illingworth, G. (2020). The challenges of adolescent sleep. Interface Focus, 10, 20190080. https://doi.org/10.1098/rsfs.2019.0080
Jackowska, M., Brown, J., Ronaldson, A., & Steptoe, A. (2016). The impact of a brief gratitude intervention on subjective well-being, biology and sleep. Journal of Health Psychology, 21(10), 2207–2217. https://doi.org/10.1177/1359105315572455
Jensen, M., George, M., Russell, M., & Odgers, C. (2019). Young adolescents' digital technology use and mental health symptoms: Little evidence of longitudinal or daily linkages. Clinical Psychological Science, 7, 1416–1433. https://doi.org/10.1177/2167702619859336
Joshanloo, M. (2016). Revisiting the empirical distinction between hedonic and eudaimonic aspects of well-being using exploratory structural equation modeling. Journal of Happiness Studies, 17(5), 2023–2036. https://doi.org/10.1007/s10902-015-9683-z
Kalak, N., Lemola, S., Brand, S., Holsboer-Trachsler, E., & Grob, A. (2014). Sleep duration and subjective psychological well-being in adolescence: A longitudinal study in Switzerland and Norway. Neuropsychiatric Disease and Treatment, 10, 1199–1207. https://doi.org/10.2147/NDT.S62533
Kansky, J., Allen, J. P., & Diener, E. (2016). Early adolescent affect predicts later life outcomes. Applied Psychology, Health and Well-Being, 8(2), 192–212. https://doi.org/10.1111/aphw.12068
Karageorghis, C. I., Bird, J. M., Hutchinson, J. C., Hamer, M., Delevoye-Turrell, Y. N., Guérin, S., Mullin, E. M., Mellano, K. T., Parsons-Smith, R. L., Terry, V. R., & Terry, P. C. (2021). Physical activity and mental well-being under COVID-19 lockdown: A cross-sectional multination study. BMC Public Health, 21(1), 988. https://doi.org/10.1186/s12889-021-10931-5
Kern, M. L., Park, N., & Romer, D. (2005). The positive perspective on youth development. In D. L. Evans, E. B. Foa, R. E. Gur, H. Hendin, C. P. O' Brien, M. E. P. Seligman, & T. Walsh. (Eds.), Treating and preventing adolescent mental health disorders: What we know and what we don't know: A research agenda for improving the mental health of our youth (Chp. 27). Oxford University. https://oxfordmedicine.com/view/10.1093/9780195173642.001.0001/med-9780195173642-chapter-27
Kerr, S. L., O’Donovan, A., & Pepping, C. A. (2015). Can gratitude and kindness interventions enhance well-being in a clinical sample? Journal of Happiness Studies, 16(1), 17–36. https://doi.org/10.1007/s10902-013-9492-1
Killgore, W. D. S., Cloonan, S. A., Taylor, E. C., & Dailey, N. S. (2020). Loneliness: A signature mental health concern in the era of COVID-19. Psychiatry Research, 290, 113117. https://doi.org/10.1016/j.psychres.2020.113117
Kim, H., Doiron, K., Warren, M. A., & Donaldson, S. I. (2018). The international landscape of positive psychology research: A systematic review. International Journal of Wellbeing, 8(1), 50–70. https://doi.org/10.5502/ijw.v8i1.651
Kleszczewska, D., Dzielska, A., Salonna, S., & Mazur, J. (2018). The association between physical activity and general life satisfaction in lower secondary school students: The role of individual and family factors. Community Mental Health Journal, 54(8), 1245–1252. https://doi.org/10.1007/s10597-018-0309-x
Kokou-Kpolou, C. K., Megalakaki, O., Laimou, D., & Kousouri, M. (2020). Insomnia during COVID-19 pandemic and lockdown: Prevalence, severity, and associated risk factors in French population. Psychiatry Research, 290, 113128. https://doi.org/10.1016/j.psychres.2020.113128
Kovess-Masfety, V., Keyes, K., Hamilton, A., Hanson, G., Bitfoi, A., Golitz, D., et al. (2016). Is time spent playing video games associated with mental health, cognitive and social skills in young children? Social Psychiatry and Psychiatric Epidemiology, 51(3), 349–357. https://doi.org/10.1007/s00127-016-1179-6
Lai, C. C. W., & Ma, C. M. S. (2020). Sleep quality types and their influences on psychological and physical health in Chinese adolescents: A person-centered approach. The Journal of Early Adolescence, 40(2), 197–220. https://doi.org/10.1177/0272431619833481
Lai, M. K., Leung, C., Kwok, S. Y. C., Hui, A. N. N., Lo, H. H. M., Leung, J. T. Y., & Tam, C. H. L. (2018). A multidimensional PERMA-H positive education model, general satisfaction of school life, and character strengths use in Hong Kong senior primary school students: Confirmatory factor analysis and path analysis using the APASO-II. Frontiers in Psychology, 9. https://doi.org/10.3389/fpsyg.2018.01090
Lambert, L., Passmore, H.-A., & Joshanloo, M. (2019a). A positive psychology intervention program in a culturally-diverse university: Boosting happiness and reducing fear. Journal of Happiness Studies, 20(4), 1141–1162. https://doi.org/10.1007/s10902-018-9993-z
Lambert, L., Passmore, H.-A., Scull, N., Al Sabah, I., & Hussain, R. (2019b). Wellbeing matters in Kuwait: The Alnowair’s Bareec education initiative. Social Indicators Research, 143(2), 741–763. https://doi.org/10.1007/s11205-018-1987-z
Lambert, N. M., Gwinn, M., Baumeister, R. F., Strachman, A., Washburn, I. J., Gable, S. L., & Fincham, F. D. (2013). A boost of positive affect: The perks of sharing positive experiences. Journal of Social and Personal Relationships, 30, 24–43. https://doi.org/10.1177/0265407512449400
Lang, C., Brand, S., Colledge, F., Ludyga, S., Pühse, U., & Gerber, M. (2019). Adolescents personal beliefs about sufficient physical activity are more closely related to sleep and psychological functioning than self-reported physical activity: A prospective study. Journal of Sports Health Sciences, 8, 280–288. https://doi.org/10.1016/j.jshs.2018.03.002
Lawler, M. J., Newland, L. A., Giger, J. T., Roh, S., & Brockevelt, B. L. (2017). Ecological, relationship-based model of children’s subjective well-being: Perspectives of 10-year-old children in the United States and 10 other countries. Child Indicators Research, 10(1), 1–18. https://doi.org/10.1007/s12187-016-9376-0
Lawrence, D., Johnson, S., Hafekost, J., Hann, K. B. D., Sawyer, M., Ainley, J., & Zubrick, S. (2015). The mental health of children and adolescents: Report on the second Australian Child and Adolescent Survey of Mental Health and Wellbeing. https://www.health.gov.au/internet/main/publishing.nsf/Content/9DA8CA21306-FE6EDCA257E2700016945/File/child2.pdf
Lees, C., & Hopkins, J. (2013). Effect of aerobic exercise on cognition, academic achievement, and psychosocial function in children: A systematic review of randomized control trials. Preventing Chronic Disease, 10, E174. https://doi.org/10.5888/pcd10.130010
Lewis, A. D., Huebner, E. S., Malone, P. S., & Valois, R. F. (2011). Life satisfaction and student engagement in adolescents. Journal of Youth and Adolescence, 40(3), 249–262. https://doi.org/10.1007/s10964-010-9517-6
Lin, Y., Mutz, J., Clough, P. J., & Papageorgiou, K. A. (2017). Mental toughness and individual differences in learning, educational and work performance, psychological well-being, and personality: A systematic review. Frontiers in Psychology, 8. https://doi.org/10.3389/fpsyg.2017.01345
Lo, J. C., Lee, S. M., Lee, X. K., Sasmita, K., Chee, N. Y. I. N., Tandi, J., et al. (2018). Sustained benefits of delaying school start time on adolescent sleep and well-being. Sleep, 41(6), zsy052. https://doi.org/10.1093/sleep/zsy052
Loades, M. E., Chatburn, E., Higson-Sweeney, N., Reynolds, S., Shafran, R., Brigden, A., … Crawley, E. (2020). Rapid systematic review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. Journal of the American Academy of Child and Adolescent Psychiatry, 59(11), 1218–1239. https://doi.org/10.1016/j.jaac.2020.05.009
Longhi, S., Nandi, A., Bryan, M., Connolly, S., & Gedikli, C. (2018). Transitions form full-time education into employment: The role of wellbeing. What Works Centre for Wellbeing, UK. https://editorialexpress.com/cgi-bin/conference/download.cgi?db_name=ESPE2018&paper_id=350
Lund, L., Sølvhøj, I. N., Danielsen, D., & Andersen, S. (2021). Electronic media use and sleep in children and adolescents in Western countries: A systematic review. BMC Public Health, 21, 1598. https://doi.org/10.1186/s12889-021-11640-9
Lundberg, S. (2019). Non-cognitive skills as human capital. In C. Hulten & V. Ramey (Eds.), Education, skills, and technical change: Implications for future U.S. GDP growth (pg. 219-243). National Bureau of Economic Research. https://sjlundberg.weebly.com/uploads/1/1/0/0/110062333/lundberg_nbercriw_2018.pdf
Lyons, M. D., Huebner, E. S., & Hills, K. J. (2013). The dual-factor model of mental health: A short-term longitudinal study of school-related outcomes. Social Indicators Research, 114(2), 549–565. https://doi.org/10.1007/s11205-012-0161-2
Mackenzie, K., & Williams, C. (2018). Universal, school-based interventions to promote mental and emotional well-being: What is being done in the UK and does it work? A systematic review. BMJ Open, 8, e022560. https://doi.org/10.1136/bmjopen-2018-02256
Magson, N. R., Freeman, J. Y. A., Rapee, R. M., Richardson, C. E., Oar, E. L., & Fardouly, J. (2021). Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. Journal of Youth and Adolescence, 50(1), 44–57. https://doi.org/10.1007/s10964-020-01332-9
Maheux, A. J., Nesi, J., Galla, B. M., Roberts, S. R., & Choukas-Bradley, S. (2021). #Grateful: Longitudinal associations between adolescents' social media use and gratitude during the COVID-19 pandemic. Journal of Research on Adolescence, 31(3), 734–747. https://doi.org/10.1111/jora.12650
Marchant, D. C., Polman, R. C. J., Clough, P. J., Jackson, J. G., Levy, A. R., & Nicholls, A. R. (2009). Mental toughness: Managerial and age differences. Journal of Managerial Psychology, 24(5), 428–437. https://doi.org/10.1108/02683940910959753
Marino, C., Andrade, B., Campisi, S. C., Wong, M., Zhao, H., Jing, X., Aitken, M., Bonato, S., Haltigan, J., Wang, W., & Szatmari, P. (2021). Association between disturbed sleep and depression in children and youths: A systematic review and meta-analysis of cohort studies. JAMA Network Open, 4(3), e212373. https://doi.org/10.1001/jamanetworkopen.2021.2373
Marques, A., Mota, J., Gaspar, T., & de Matos, M. G. (2017). Associations between self-reported fitness and self-rated health, life-satisfaction and health-related quality of life among adolescents. Journal of Exercise Science & Fitness, 15(1), 8–11. https://doi.org/10.1016/j.jesf.2017.03.001
Marques de Miranda, D., da Silva Athanasio, B., Sena Oliveira, A. C., & Simoes-E-Silva, A. C. (2020). How is COVID-19 pandemic impacting mental health of children and adolescents? International Journal of Disaster Risk Reduction: IJDRR, 51, 101845. https://doi.org/10.1016/j.ijdrr.2020.101845
Marquez, J. M., & Inchley, J. (2020, October 18). A comparative study of factors explaining declining levels in adolescents’ life satisfaction: The importance of school well-being. https://doi.org/10.31235/osf.io/42sd8
Marquez, J. M., & Long, E. (2021). A global decline in adolescents’ subjective well-being: A comparative study exploring patterns of change in the life satisfaction of 15-year-old students in 46 countries. Child Indicators Research, 14, 1251–1292. https://doi.org/10.1007/s12187-020-09788-8
Marquez, J. M., & Main, G. (2021). Can schools and education policy make children happier? A comparative study in 33 countries. Child Indicators Research, 14, 283–339. https://doi.org/10.1007/s12187-020-09758-0
Matricciani, L., Olds, T., & Petkov, J. (2012). In search of lost sleep: Secular trends in the sleep time of school-aged children and adolescents. Sleep Medicine Reviews, 6(3), 203–211. https://doi.org/10.1016/j.smrv.2011.03.005
Matos, M. G., Marques, A., Gaspar, T., & Paiva, T. (2017). Perception of quantity and quality of sleep and their association with health related quality of life and life satisfaction during adolescence. Health Education Care, 2(2), 1-6. https://doi.org/10.15761/HEC.1000117
McDowell, C. P., Dishman, R. K., Gordon, B. R., & Herring, M. P. (2019). Physical activity and anxiety: A systematic review and meta-analysis of prospective cohort studies. American Journal of Preventive Medicine, 57(4), 545–556. https://doi.org/10.1016/j.amepre.2019.05.012
McGeown, S., St. Clair-Thompson, H., & Putwain, D. W. (2018). The development and validation of a mental toughness scale for adolescents. Journal of Psychoeducational Assessment, 36(2), 148–161. https://doi.org/10.1177/0734282916673512
Milkie, M. A., & Warner, C. H. (2011). Classroom learning environments and the mental health of first grade children. Journal of Health and Social Behavior, 52(1), 4–22. https://doi.org/10.1177/0022146510394952
Mitra, R., Waygood, E. O. D., & Fullan, J. (2021). Subjective well-being of Canadian children and youth during the COVID-19 pandemic: The role of the social and physical environment and healthy movement behaviours. Preventive Medicine Reports, 23, 101404. https://doi.org/10.1016/j.pmedr.2021.101404
Moore, G. F., Cox, R., Evans, R. E., Hallingberg, B., Hawkins, J., Littlecott, H. J., et al. (2018). School, peer and family relationships and adolescent substance use, subjective wellbeing and mental health symptoms in Wales: A cross sectional study. Child Indicators Research, 11(6), 1951–1965. https://doi.org/10.1007/s12187-017-9524-1
Neff, K. D., & Pommier, E. (2013). The relationship between self-compassion and other-focused concern among college undergraduates, community adults, and practicing meditators. Self and Identity, 12(2), 160–176. https://doi.org/10.1080/15298868.2011.649546
Ness, T. E. B., & Saksvik-Lehouillier, I. (2018). The relationships between life satisfaction and sleep quality, sleep duration and variability of sleep in university students. Journal of European Psychology Students, 9(1), 28–39. https://doi.org/10.5334/jeps.434
Newland, L. A., Lawler, M. J., Giger, J. T., Roh, S., & Carr, E. R. (2018). Multilevel analysis of child and adolescent subjective well-being across 14 countries: Child- and country-level predictors. Child Development, 90(2), 395–413. https://doi.org/10.1111/cdev.13134
Nie, Y., Ma, Y., Wu, Y., Li, J., Liu, T., Zhang, C., Lv, C., & Zhu, J. (2021). Association between physical exercise and mental health during the COVID-19 outbreak in China: A nationwide cross-sectional study. Frontiers in Psychiatry, 12, 722448. https://doi.org/10.3389/fpsyt.2021.722448
Oberle, E., & Schonert-Reichl, K. A. (2016). Stress contagion in the classroom? The link between classroom teacher burnout and morning cortisol in elementary school students. Social Science & Medicine, 159, 30–37. https://doi.org/10.1016/j.socscimed.2016.04.031
Oettingen, G., Kappes, H. B., Guttenberg, K. B., & Gollwitzer, P. M. (2015). Self-regulation of time management: Mental contrasting with implementation intentions. European Journal of Social Psychology, 45, 218–229. https://doi.org/10.1002/ejsp.2090
Office for National Statistics. (2020). Coronavirus and the social impacts on young people in Great Britain: 3 April to 10 May 2020. Indicators from the Opinions and Lifestyle Survey on the impact of the coronavirus (COVID-19) pandemic on young people in Great Britain. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/coronavirusandthesocialimpactsonyoungpeopleingreatbritain/3aprilto10may2020#toc
Orben, A., & Przybylski, A. K. (2019). The association between adolescent well-being and digital technology use. Nature Human Behaviour, 3, 173–182. https://doi.org/10.1038/s41562-018-0506-1
Orchard, F., Gregory, A. M., Gradisar, M., & Reynolds, S. (2020). Self-reported sleep patterns and quality amongst adolescents: Cross-sectional and prospective associations with anxiety and depression. Journal of Child Psychology and Psychiatry, 61(10), 1126–1137. https://doi.org/10.1111/jcpp.13288
Organization for Economic Cooperation and Development (OECD). (2021). OECD review of well-being policies and practices in Dubai’s private school sector. OECD Publishing. https://doi.org/10.1787/0e9aa172-en. https://www.oecd-ilibrary.org/education/oecd-review-of-well-being-policies-and-practices-in-dubai-s-private-school-sector_0e9aa172-en
Palgi, Y., Shrira, A., Ring, L., Bodner, E., Avidor, S., Bergman, Y., Cohen-Fridel, S., Keisari, S., & Hoffman, Y. (2020). The loneliness pandemic: Loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. Journal of Affective Disorders, 275, 109–111. https://doi.org/10.1016/j.jad.2020.06.036
Palmer, C. A., & Alfano, C. A. (2017). Sleep and emotion regulation: An organizing, integrative review. Sleep Medicine Reviews, 31, 6–16. https://doi.org/10.1016/j.smrv.2015.12.006
Papageorgiou, K. A., Denovan, A., & Dagnall, N. (2019). The positive effect of narcissism on depressive symptoms through mental toughness: Narcissism may be a dark trait but it does help with seeing the world less grey. European Psychiatry, 55, 74–79. https://doi.org/10.1016/j.eurpsy.2018.10.002
Pressman, S. D., Kraft, T. L., & Cross, M. P. (2015). It’s good to do good and receive good: The impact of a ‘pay it forward’ style kindness intervention on giver and receiver well-being. Journal of Positive Psychology, 10(4), 293–302. https://doi.org/10.1080/17439760.2014.965269
Prinzing, M. M., Zhou, J., West, T. N., Le Nguyen, K. D., Wells, J. L., & Fredrickson, B. L. (2022). Staying “in sync” with others during COVID-19: Perceived positivity resonance mediates cross-sectional and longitudinal links between trait resilience and mental health. The Journal of Positive Psychology, 17(3), 40–455. https://doi.org/10.1080/17439760.2020.1858336
Rapee, R. M., Oar, E. L., Johnco, C. J., Forbes, M. K., Fardouly, J., Magson, N. R., & Richardson, C. E. (2019). Adolescent development and risk for the onset of social-emotional disorders: A review and conceptual model. Behaviour Research and Therapy, 123, 103501. https://doi.org/10.1016/j.brat.2019.103501
Rees, G. (2017). Children’s activities and time use: Variations between and within 16 countries. Children and Youth Services Review, 80, 78–87. https://doi.org/10.1016/j.childyouth.2017.06.057
Rees, G., & Main, G. (Eds.). (2015). Children’s views on their lives and subjective well-being in 15 countries: An initial report on the Children’s Worlds survey, 2013-14. Children’s Worlds Project (ISCWeB).
Richards, M., & Huppert, F. A. (2011). Do positive children become positive adults? Evidence from a longitudinal birth cohort study. The Journal of Positive Psychology, 6(1), 75–87. https://doi.org/10.1080/17439760.2011.536655
Roberts, R. E., & Duong, H. T. (2014). The prospective association between sleep deprivation and depression among adolescents. Sleep, 37(2), 239–244. https://doi.org/10.5665/sleep.3388
Rodríguez-Rey, R., Garrido-Hernansaiz, H., & Collado, S. (2020). Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.01540
Ryan, R. M., & Huta, V. (2009). Wellness as healthy functioning or wellness as happiness: the importance of eudaimonic thinking (response to the Kashdan et al. and Waterman discussion). The Journal of Positive Psychology, 4, 202-204. https://doi.org/10.1080/17439760902844285
Ryff, C. D., & Singer, B. H. (2008). Know thyself and become what you are: A eudaimonic approach to psychological well-being. Journal of Happiness Studies, 9(1), 13–39. https://doi.org/10.1007/s10902-006-9019-0
Schuch, F. B., Vancampfort, D., Firth, J., Rosenbaum, S., Ward, P. B., Silva, E. S., et al. (2018). Physical activity and incident depression: A meta-analysis of prospective cohort studies. American Journal of Psychiatry, 175(7), 631–648. https://doi.org/10.1176/appi.ajp.2018.17111194
Scott, J. F., Webb, T. L., Martyn-St James, M., Rowse, G., & Weich, S. (2021). Improving sleep quality leads to better mental health: A meta-analysis of randomised controlled trials. Sleep Medicine Reviews, 60, 101556. https://doi.org/10.1016/j.smrv.2021.101556
Shigemura, J., Ursano, R. J., Morganstein, J. C., Kurosawa, M., & Benedek, D. M. (2020). Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry and Clinical Neurosciences, 74(4), 281–282. https://doi.org/10.1111/pcn.12988
Shoshani, A., & Slone, M. (2017). Positive education for young children: Effects of a positive psychology intervention for preschool children on subjective wellbeing and learning behaviors. Frontiers in Psychology, 8, 1866. https://doi.org/10.3389/fpsyg.2017.01866
Shoshani, A., & Steinmetz, S. (2014). Positive psychology at school: A school-based intervention to promote adolescents’ mental health and well-being. Journal of Happiness Studies, 15(6), 1289–1311. https://doi.org/10.1007/s10902-013-9476-1
Sin, N., & Lyubomirsky, S. (2009). Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. Journal of Clinical Psychology, 65, 467–487. https://doi.org/10.1002/jclp.20593
Smith, M. M., Saklofske, D. H., Keefer, K. V., & Tremblay, P. F. (2016). Coping strategies and psychological outcomes: The moderating effects of personal resiliency. The Journal of Psychology: Interdisciplinary and Applied, 150(3), 318–332. https://doi.org/10.1080/00223980.2015.1036828
Sokić, J., Popov, S., Dinić, B. M., & Rastović, J. (2021). Effects of physical activity and training routine on mental health during the COVID-19 pandemic and curfew. Frontiers in Psychology, 12, 624035. https://doi.org/10.3389/fpsyg.2021.624035
Sørensen, K. L., & Krassel, K. F. (2019). Childhood and adulthood skill acquisition: Importance for labor market outcomes. Journal of Economics and Economic Education Research, 20(1), https://www.abacademies.org/articles/childhood-and-adulthood-skill-acquisition%2D%2Dimportance-for-labor-market-outcomes-7842.html
Speer, M. E., & Delgado, M. R. (2017). Reminiscing about positive memories buffers acute stress responses. Nature Human Behaviour, 1(5), 0093. https://doi.org/10.1038/s41562-017-0093
IBM Corp. (2018). IBM SPSS Statistics for Windows, Version 26.0. IBM Corp.
Suldo, S. M., Shaffer, E. J., & Riley, K. N. (2008). A social-cognitive-behavioral model of academic predictors of adolescents' life satisfaction. School Psychology Quarterly, 3(1), 56–69. https://doi.org/10.1037/1045-3830.23.1.56
Suldo, S., Thalji, A., & Ferron, J. (2011). Longitudinal academic outcomes predicted by early adolescents' subjective well-being, psychopathology, and mental health status yielded from a dual factor model. The Journal of Positive Psychology, 6(1), 17–30. https://doi.org/10.1080/17439760.2010.536774
Tandon, P. S., Zhou, C., Johnson, A. M., Gonzalez, E. S., & Kroshus, E. (2021). Association of children’s physical activity and screen time with mental health during the COVID-19 pandemic. JAMA Network Open, 4(10), e2127892. https://doi.org/10.1001/jamanetworkopen.2021.27892
Thumann, B. F., Börnhorst, C., Michels, N., Veidebaum, T., Solea, A., Reisch, L., Moreno, L. A., Lauria, F., Kaprio, J., Hunsberger, M., Felső, R., Gwozdz, W., De Henauw, S., Ahrens, W., & IDEFICS and Family Consortia. (2019). Cross-sectional and longitudinal associations between psychosocial well-being and sleep in European children and adolescents. Journal of Sleep Research, 28(2), e12783. https://doi.org/10.1111/jsr.12783
Troxel, W. M., & Wolfson, A. R. (2017). The intersection between sleep science and policy: Introduction to the special issue on school start times. Sleep Health, 3(6), 419–422. https://doi.org/10.1016/j.sleh.2017.10.001
Turban, D. B., Lee, F. K., Veiga, S. P. D. M., Haggard, D. L., & Wu, S. Y. (2013). Be happy, don’t wait: The role of trait affect in job search. Personnel Psychology, 66, 483–514. https://doi.org/10.1111/peps.12027
Twenge, J. M., Cooper, A. B., Joiner, T. E., Duffy, M. E., & Binau, S. G. (2019). Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 2005–2017. Journal of Abnormal Psychology, 128(3), 185–199. https://doi.org/10.1037/abn0000410
Twenge, J. M., Joiner, T. E., Rogers, M. L., & Martin, G. N. (2017). Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clinical Psychological Science, 6, 3–17. https://doi.org/10.1177/2167702617723376
Twenge, J. M., Martin, G. N., & Campbell, W. K. (2018). Decreases in psychological well-being among American adolescents after 2012 and links to screen time during the rise of smartphone technology. Emotion, 18(6), 765–780. https://doi.org/10.1037/emo0000403
Valladares-Neto, J. (2018). Effect size: A statistical basis for clinical practice. Revista Odonto Ciência, 33(1), 84-90. https://doi.org/10.15448/1980-6523.2018.1.29437
Vannucci, A., Simpson, E. G., Gagnon, S., & Ohannessian, C. M. (2020). Social media use and risky behaviors in adolescents: A meta-analysis. Journal of Adolescence, 79, 258–274. https://doi.org/10.1016/j.adolescence.2020.01.014
Walsh, L. C., Boehm, J. K., & Lyubomirsky, S. (2018). Does happiness promote career success? Revisiting the evidence. Journal of Career Assessment, 26(2), 199–219. https://doi.org/10.1177/1069072717751441
Warren, R., Smeets, E., & Neff, K. (2016). Risk and resilience: Being compassionate to oneself is associated with emotional resilience and psychological well-being. Current Psychiatry, 15(2), 19–33.
Weinstein, A. A., Koehmstedt, C., & Kop, W. J. (2017). Mental health consequences of exercise withdrawal: A systematic review. General Hospital Psychiatry, 49, 11–18. https://doi.org/10.1016/j.genhosppsych.2017.06.001
Weiss, L. A., Westerhof, G. J., & Bohlmeijer, E. T. (2016). Can we increase psychological well-being? The effects of interventions on psychological well-being: A meta-analysis of randomized controlled trials. PLoS ONE, 11(6), e0158092. https://doi.org/10.1371/journal.pone.0158092
White, C. A., Uttl, B., & Holder, M. D. (2019). Meta-analyses of positive psychology interventions: The effects are much smaller than previously reported. PLOS ONE, 14(5), e0216588. https://doi.org/10.1371/journal.pone.0216588
White, M. A., & Kern, M. L. (2018). Positive education: Learning and teaching for wellbeing and academic mastery. International Journal of Wellbeing, 8(1), 1–17. https://doi.org/10.5502/ijw.v8i1.588
White, R. L., Babic, M. J., Parker, P. D., Lubans, D. R., Astell-Burt, T., & Lonsdale, C. (2017). Domain-specific physical activity and mental health: A meta-analysis. American Journal of Preventive Medicine, 52(5), 653–666. https://doi.org/10.1016/j.amepre.2016.12.008
Widnall, E., Winstone, L., Mars, B., Haworth, C., & Kidger, J. (2020). Young people's mental health during the COVID-19 pandemic: Initial findings from a secondary school survey study in South West England. NIHR: School for Public Health Research. https://sphr.nihr.ac.uk/wp-content/uploads/2020/08/Young-Peoples-Mental-Health-during-the-COVID-19-Pandemic-Report-Final.pdf
Woodworth, R. J., O'Brien-Malone, A., Diamond, M. R., & Schüz, B. (2017). Web-based positive psychology interventions: A reexamination of effectiveness. Journal of Clinical Psychology, 73(3), 218–232. https://doi.org/10.1002/jclp.22328
World Health Organization. (2017). Depression and other common mental disorders: Global health estimates. http://www.who.int/mental_health/management/depression/prevalence_global_health_estimates/en/
Wright, L. J., Williams, S. E., & Veldhuijzen van Zanten, J. J. C. S. (2021). Physical activity protects against the negative impact of coronavirus fear on adolescent mental health and well-being during the COVID-19 pandemic. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2021.580511
Yang, S. J., & Cha, H. S. (2018). Retrospective cohort study on Korean adolescents’ sleep, depression, school adjustment, and life satisfaction. Nursing & Health Sciences, 20, 422–430. https://doi.org/10.1111/nhs.12425
Zi Jia, N. G., Huebner, S. E., & Hills, K. J. (2015). Life satisfaction and academic performance in early adolescents: Evidence for reciprocal association. Journal of School Psychology, 53(6), 479–491. https://doi.org/10.1016/J.JSP.2015.09.004
Acknowledgments
We wish to thank Dubai College for its full support and collaboration in implementing this wellbeing program. Support from school leadership, teachers, parents as well as students themselves made it a success. The program was financially supported by the College, with the primary author (LL) financially remunerated for developing the program in collaboration with MS and ST. All other co-authors were instrumental in the statistical analysis and writing of the paper and have no conflicts of interest to declare.
Data availability
We are happy to share any data upon reasonable request. This request can be made to the first author.
Code availability (software application or custom code)
Not applicable
Funding
The first author received a fee from the school noted in the study to develop the PPI program.
Author information
Authors and Affiliations
Contributions
Material preparation, program development and data collection were done by Dr. Louise Lambert. Analysis was completed by Dr. Mohsen Joshanloo, Dr. Jose Marquez, and Dr. Brettjet Cody. The first draft of the manuscript was written by Dr. Louise Lambert and all remaining authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest/Competing interests
The first author was commissioned to develop the PPI program in collaboration with the last two authors, who worked at the school where the study was conducted.
Humans and/or animals
Not applicable
Ethics approval
Ethics approval was granted by the United Arab Emirates University Ethics Committee, Approval number: ERS_2019_5948
Consent to participate
Participants – as well as their parents – gave their written informed consent to participate in the program and for the primary author to use their data towards the publication of this paper.
Consent for publication
Participants and the school itself were aware of, agreed to and provided their written consent for this study to be published.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Week | Title | Description of PPI |
|---|---|---|
1 | Introduction | Introduction to program and its aims. What does happiness mean to you? Self-reflection and use of positive reminiscing. Share a happier moment with another student (building classroom relationships). Notice when you are happier this week and what you are doing during that time. |
2 | Place your order | Establishing norms for a happier classroom. What do you need to be happy in this class? (i.e., fewer interruptions, more kindness, no gossip). Place your order on a sticky tab on the wall. Consider what you can do in light of others orders to make it better for others? Choose an action and pledge to meet it, e.g., “I will listen when others speak…” |
3 | The do good marathon | Developing more kindness; Noticing others more often In the next 7 minutes, do as many kind acts as you can. Notice how you feel, notice the response in others. Want a challenge? Can you do 25 kind acts this week to improve your mood and that of others? Note them all down. |
4 | I wish this place was more… | Creating a more humane school culture; taking responsibility for school climates How do students experience the school, other students? Are they welcomed, judged? Is it a nice place to be? What can you do as a person and class to make this place better for everyone? [Share and commit] |
5 | Think you know your family? | Making meaningful family connections; Elicit collective character strengths What strengths does your family show? Are you all hard workers, creative, funny, brave, kind? Share examples of where you use the same strengths. What other strengths does your family have? Interview them this week to find out. |
6 | Conversation stations | Authentic conversations lead to greater social trust and connections Ask the person next to you, “What’s your greatest life joy?” It’s deep, but helps to know people. What other meaningful positive questions have you wanted to ask? This week, we’ll set up conversation stations to have more of these talks. |
7 | Mid-term report | Awareness of personal positive qualities; Commit to using them more often What qualities are you using these days? From a list including honesty, kindness, persistence, etc., rate yourself from 1-10. Can you use those in other places, with other people, and more often? Are there any you would like to improve? How? |
8 | Make it as bad as you can | Use mental contrasting to increase realistic optimism and readiness for difficulty Stress & assignments go together. What’s the worst scenario for you in this time? Exaggerate it much as you can; imagine it happens. What actions (and thoughts) could you take to fix it? If it came to this situation, would your plan work? Could you handle it? Add real solutions until you feel confident that you could. |
9 | Bad to better | Normalizing negative emotions; Gaining control over negative moods Feeling low happens but there are things we can do to lessen how negative moments feel. List three things you do to go from a bad mood to better on the board. Once you’ve written yours, read the strategies of others and rate them to see which might work for you too. Try a new one this week as an experiment. |
10 | What’s in a name? | Self-identity and choosing a positive self-narrative Do you know what your name means? Look it up! While you do, find three famous people with the same name. What characteristics do you share? What extra value do you have that they might not? How does the meaning of your name show in your actions? |
11 | The worry bin | Develop self-efficacy and self-compassion; Build classroom social supports Still got worries? Write out as many as you have and choose three to note on slips of paper. Add them to the bin and exchange them for three more. Write concrete supportive advice on the back of each. We’ll tape them to the wall after to see what others had to say. Find yours and correct the advice to suit you better. |
12 | Say thanks, already! | Expressing gratitude to a sibling; Strengthening relationships It’s weird, but saying thanks is a way to be happier. If you have siblings, think of a time when one really helped you. It could have been with homework, an issue, or defending your actions. Write them a letter of thanks for it; add more to share what they mean to you. You can do it with a friend too. Done? Send it! |
13 | Grades (don’t fully) matter | Identifying character strengths and their use Grades matter, but so does character: it’s what will help you get friends and jobs. If you were to write a CV based on your strengths (not grades), what would it say? Write a 1-page CV outlining your strengths and experiences that shaped them. Ask your peers for endorsements and/or take the VIA for more. |
14 | See others | Affirming others We all know someone who could use a boost, but get so busy we forget to send a “hello, I see you” message. Yet, being seen is a powerful validation. Who needs you to see them? Send a note to that person saying, I’m thinking of you, I see you, or whatever would make them feel they matter. Note how you feel doing it. |
15 | Strengths Spotting | Finding the goodness in others; Developing awareness that others see us Remember the positive qualities list? Here’s your chance to see them in others. As you move from desk to desk, where you can, comment on other’s positive qualities on the list by using an example of where you saw them use it. Be real, specific and kind. |
16 | Be the weirdo | Acknowledge others to boost one’s sense of self; Talking to strangers We worry that strangers are well, strange. We also worry they’ll think we are too. But most people are open to being talked with and pleased someone did. Go on, say hello, strike up a conversation and see whether you can make a connection and boost your networking and social skills. Was it as bad as you thought? |
Rights and permissions
About this article

Cite this article
Lambert, L., Joshanloo, M., Marquez, J.M. et al. Boosting Student Wellbeing Despite a Pandemic: Positive Psychology Interventions and the Impact of Sleep in the United Arab Emirates. Int J Appl Posit Psychol 7, 271–300 (2022). https://doi.org/10.1007/s41042-022-00066-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41042-022-00066-2