
Abstract
There has been increasing interest in the identification of factors that promote resilience to suicidal thoughts and behaviors in high-risk youth. The present review summarizes and critiques the current literature on protective factors that promote resilience to suicidal thoughts and behaviors in those children and adolescents who are at high risk for these outcomes. In contrast to earlier work on this topic, which primarily focused on internal, psychological protective factors, the current review articulates an ecological model of resilience in youth that spans multiple domains, including the individual, parents, family, friends, peers, school, community, and culture. This model encompasses individual assets such as problem-solving ability and emotion regulation as well as ecological resources such as parent–child relationship quality, family functioning, peer acceptance, supportive school climate, and engagement in meaningful activities and interests. The present review suggests that future research on resilience to suicidality in youth may benefit from taking a multi-dimensional approach that is grounded in current theories on suicidal thoughts and behavior. The results also suggest that suicide prevention and intervention programs for youth may benefit from a domain-spanning approach that helps teens to enhance their connection to friends, family, and community while teaching them vital internal coping skills.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The past several decades of research on adolescent suicide has almost exclusively focused on risk factors for suicidal ideation and behavior while ignoring or failing to emphasize potential protective factors that may help to address this significant public health crisis. This lack of attention to protective factors in youth suicide is alarming given that we have not improved our ability to prevent youth suicide. In fact, rates of suicide have increased over the past 15 years (Curtin et al. 2016). Suicide is the second leading cause of death among individuals ages 10–24 (Heron 2016) and suicidal ideation and behavior is even more common (Kann et al. 2014). Notably absent from the suicide literature is research on factors that promote resilience to suicidal ideation and behavior (Luthar et al. 2000). In this article, we review and critically evaluate the current research available on protective factors within two broad categories: (1) individual assets such as problem-solving skills, self-esteem, and emotion regulation; and (2) ecological resources, including parents and family, peers and school, and the larger community and cultural context.
Although the focus of this review is on resilience factors, a brief discussion of the main risk factors in youth suicide is warranted. A history of prior suicide attempts is one of the best predictors of future suicidal ideation and behavior. Further, psychopathology increases risk, especially mood and depressive disorders, anxiety disorders, conduct disorder, and alcohol and substance abuse (Cash and Bridge 2009). Other individual differences linked to suicide risk include biological vulnerabilities, sexual orientation, socioeconomic status, hopelessness, low self-esteem, poor problem-solving skills, impulsivity, aggression, and negative life events such as physical and sexual abuse (Gould et al. 2003; King and Merchant 2008). Parent and family factors, including parental psychopathology, poor parent–child attachment, low parental or family support, a dysfunctional family environment, low family cohesion, and parent–child conflict, increase risk for suicidal ideation and behavior (Gould et al. 2003; King and Merchant 2008). Similarly, peer- and school-related risk factors include social isolation, interpersonal difficulty, peer victimization, low social competence, deviant peer group affiliation, recent moves/relocations, low school attachment, and academic difficulties (see King and Merchant 2008, for a review).
In the developmental literature, numerous terms have been applied to protective processes, including compensatory, promotive, and/or protective factors (Wright et al. 2013; Zimmerman et al. 2013). The term protective factors has been used to describe both main effects (i.e., predict a positive or more desirable outcome at both high and low levels of risk) and interaction effects (i.e., reduce the chance of negative outcomes particularly at high levels of risk). Here we use the language suggested by Wright and colleagues (2013), by describing variables that reduce negative outcomes across all risk levels (i.e., main effects) as compensatory factors and variables that reduce negative outcomes especially at high levels of risk (i.e., interaction effects) as protective factors. Research has identified an array of compensatory factors that reduce suicidal outcomes in youth regardless of initial risk. Many of these are individual capabilities: self-esteem and self-efficacy, coping efficacy, productive coping strategies, personal control, gratitude, religiosity/spirituality, self-discovery, and confidence in one’s emotions (Breton et al. 2015; Deeley and Love 2013; Lewinsohn et al. 1993; Li et al. 2012; Walsh and Eggert 2007). Meanwhile, family-related factors include parent and family connectedness and communication, parental expectations and presence, shared family activities, family alliance, cohesion, and harmony, and family support (Bearman and Moody 2004; Borowsky et al. 2001; Breton et al. 2015; DeWilde et al. 1993; Evans et al. 2004; Resnick et al. 1997; Rew et al. 2001; Walsh and Eggert 2007). Similarly, peer- and friend-related factors include a closely interconnected friend group, dense friendship networks, peer acceptance and support, and feelings of social connectedness (Bearman and Moody 2004; Breton et al. 2015; King and Merchant 2008; Rew et al. 2001). Finally, the literature points to compensatory factors related to school and the larger community: school safety and connectedness, school counseling services, caring adults at school, and engagement in meaningful activities such as sports teams or volunteering (Bearman and Moody 2004; Borowsky et al. 2001; Reisner et al. 2014; Resnick et al. 1997; Rew et al. 2001).
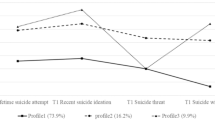
We know less about how protective factors promote resilience to suicidal ideation and behavior. In contrast to compensatory factors—which theorists view as having a direct effect on suicidal ideation and behavior, reducing suicidal outcomes at both high and low levels of risk or adversity (i.e., a main-effects model, as depicted in Fig. 1A)—protective factors have been described as factors that “…have particular importance for positive adaptation at high levels of risk or adversity…” (Wright et al. 2013, p. 19). Embedded in this conceptualization of resilience (vis a vis protective factors) are two primary elements: (1) the presence of risk factors or adverse life circumstances, such as childhood physical or sexual abuse or current life stress, that increases an individual’s risk for a negative outcome such as suicidal ideation or behaviors; and (2) the presence of protective factors, such as self-esteem or problem-solving ability, that buffer or protect the high-risk individual against the negative outcomes stemming from his or her elevated risk (Luthar et al. 2000). This conceptualization suggests that resilience results from the interaction of risk and protective factors (i.e., a moderation effect, as depicted in Fig. 1b–d).

Compensatory and protective effects models: a compensatory main effect, b protective–stabilizing interaction, c protective–reactive interaction, and d protective–enhancing interaction
Only one prior review has comprehensively examined protective factors related to suicidal ideation and behavior. Johnson and colleagues (2011) identified 77 studies that examined protective factors, and articulated a “buffering hypothesis” in which internal, psychological moderators like attributional style interact with risk factors such as physical abuse to buffer against suicidal outcomes (Johnson et al. 2011). Although the review found strong support for their hypothesis, it included both adults and youth, and did not interpret the 16 studies that used child/adolescent samples separately. Given that adolescence is a period of dynamic development with changing risk and protective factors (Wright et al. 2013), the applicability of the Johnson et al. (2011) study to adolescent suicide is limited. Further, the review by Johnson et al. (2011) focuses exclusively on psychological variables as protective factors. In focusing exclusively on psychological variables, the authors ignore key elements of a youth’s ecological context (e.g., family, peer, school, and neighborhood variables).
Current Study
Research on suicidal ideation and behavior in youth has begun to move beyond compensatory main effects to evaluate protective factors. Although a prior review summarized suicide-related protective factors (Johnson et al. 2011), the review combined research on adults and children/adolescents, and focused exclusively on internal, psychological protective factors. In this review, we provide a comprehensive summary of the research on child and adolescent suicide-related protective factors. Next, we evaluate resilience to suicidal ideation and behavior using an ecological framework that moves beyond an individual’s internal, psychological traits (e.g., problem-solving ability) to also include protective factors related to the family context, relationships with peers, and the school and community context. Finally, we critically interpret the existing literature and discuss implications for research and suicide prevention.
Methods
Relevant peer-reviewed research articles were identified via an electronic literature search. Inclusion criteria identified studies that: (i) reported data on interaction effects between one or more risk or protective factors; (ii) focused on a suicide-related outcome, such as suicidal ideation or attempts; and (iii) utilized a predominately child or adolescent sample. Searches were conducted across a variety of databases (e.g., PsycARTICLES, MEDLINE, Academic Search Premier) using the following search terms: (child* or adolescen* or youth) and (suicid* or ideat* or suicidal ideation or self-harm or self-injur* or suicide attempt) and (moderat* or interact* or resilien* or protective or buffer*). The most common reasons for study exclusion included: a sole focus on the main effects of compensatory factors instead of interaction effects; the use of an outcome other than suicidal ideation and behavior (e.g., depression); and the use of an adult (or predominately adult) sample. Once relevant research studies were identified for inclusion, full-text articles were retrieved and the author hand-searched each reference section as a secondary means of identifying relevant research studies.
Many risk and compensatory/protective variables are continuous and, therefore, can represent opposite ends of a bipolar spectrum (Wright et al. 2013). For instance, problem-solving ability can be viewed as “low problem-solving ability” or “high problem-solving ability” depending on the goals of the study. In the former case (i.e., low problem-solving ability), the variable might be viewed as a risk factor for suicidal outcomes. In the latter case (i.e., high problem-solving ability), it may be viewed as a compensatory/protective factor. To ensure a comprehensive summary of the literature, this review includes continuous bipolar moderator variables. We include studies examining suicidal ideation and plans (i.e., self-reported thoughts of killing oneself and specific plans regarding method, location and/or timing), nonfatal suicide attempts (i.e., a nonfatal self-inflicted act in which the individual has at least some intent to die), and death by suicide (Silverman et al. 2007). A small number of studies utilized high-school student samples that contained a minority of students who were technically of an age consistent with young adult status (oldest 18–21 years old).
Results
A total of 41 peer-reviewed research studies were identified for inclusion in the present review (see Table 1), with the vast majority (97.6%; N = 40) utilizing a cross-sectional design. Of these studies, two groups of researchers published more than one article on an overlapping sample. Due to differences in sample size, risk factors, and moderating variables, each of these articles is being considered as a separate study.
In terms of sample characteristics, over half of the studies used non-clinical school-based or epidemiological samples (61.0%; N = 25). An additional four studies used a psychiatric inpatient sample, while three studies included psychiatric outpatients in whole or part. A final grouping of nine studies used samples of clinically referred or at-risk youth. The majority of the studies used North American samples (65.9%; N = 27). The review also includes 14 studies with international samples (34.1%). Most studies (85.4%; N = 35) focused on samples of youth in the age range consistent with mid- to late-adolescence (approximately ages 11–13 through ages 17–19), with an additional six studies using samples consisting entirely of younger children or a broad age range from child to adolescent. Finally, of the studies that reported on biological sex (N = 38), most studies (60.5%; N = 23) included an even balance of males and females. Overall, the 38 studies included a mean of 52.9% female participants.
In the following sections, the research is reviewed using an ecological framework consistent with that of Fergus and Zimmerman (2005), who suggest a framework of assets and resources, as well as theoretical perspectives that suggest a more articulated breakdown of resilience domains that includes the adolescent, parents and family, peers and school, and the larger social community (e.g., Ayyash-Abdo 2002; Henry et al. 1993; Masten and Coatsworth 1998; Rew and Horner 2003; Wright et al. 2013). Figure 2 depicts the conceptual model guiding the present review.

Ecological model of resilience to suicidal outcomes in youth, with representative examples of protective factors that fall within the domains of individual assets and ecological resources
Individual Assets that Promote Resilience to Suicidal Ideation and Behaviors
Cognitive Factors
Problem-solving ability has been shown to be both a risk and compensatory factor against suicidal ideation and behavior in youth (e.g., Gould et al. 2003; Walsh and Eggert 2007). A total of four studies focused on problem solving as a potential protective factor. In one study, problem-solving ability was found to buffer the link between life stress and both suicidal ideation and attempts and to additionally moderate the relationship between chronic stress and ideation (but not attempts). Of note, although problem-solving ability buffered against suicidal outcomes at all levels of risk, it exerted the greatest effect at high levels of stress (Grover et al. 2009). In another study, social problem-solving ability did not buffer against suicidal ideation for those with high daily life stress (Chang 2002). Problem-solving confidence (i.e., a person’s confidence in and control of their problem-solving process) moderated the relationship between both physical and sexual abuse and suicidal ideation (Esposito and Clum 2002), while rational problem-solving (i.e., the systematic and deliberate use of effective problem-solving techniques) attenuated the effect of physical abuse on suicidal ideation, but only among female teens (Kwok et al. 2015).
Elements of an individual’s cognitive style—including the cognitive triad of pessimistic views about oneself, the world, and the future—also have been linked to suicidal ideation and behavior in youth as well as to depressive symptoms, a key risk factor for suicidal ideation and behavior (see Esposito-Smythers et al. 2014, for a review). A total of four studies focused on factors related to an individual’s cognitive style. Less negative interpretations of oneself, the world, and the future buffered the link between depressive symptoms and suicidal ideation (Chang et al. 2007), while lower levels of negative self-talk and cognitive errors moderated the relationship between peer victimization and suicidal ideation (Wolff et al. 2014), However, although the latter study found a buffering effect at both low and high levels of peer victimization, the buffering effect was greater at low levels of peer victimization. In contrast, Miller and Esposito-Smythers (2013) showed that neither cognitive errors nor the negative cognitive triad moderated the link between a history of child abuse and suicidal ideation. Further, Lee (2011) found no buffering effect of optimistic beliefs about the future on the link between depressive symptoms and suicidal ideation.
Although both problem-solving and cognitive style have been shown to be related to suicidal ideation and behavior in youth, the present review suggests that problem-solving may serve as a more consistent protective factor in buffering the impact of risk factors on suicidal ideation and behavior. Three of four studies suggested that general problem-solving, rational problem-solving, and problem-solving confidence are moderators of the relationship between suicidal outcomes and risk factors such as physical and sexual abuse and life event and chronic stress (Esposito and Clum 2002; Grover et al. 2009; Kwok et al. 2015). Of note, among the studies that included both suicidal ideation and suicide attempts as outcomes, results showed only one significant interaction predicting suicide attempts, indicating that problem-solving may play a greater role in buffering against suicidal ideation. It may be that enhanced problem-solving ability helps an individual to avoid the cognitive constriction hypothesized to play a role in suicidal thinking (Schneidman 1981), allowing a person to generate alternatives to “suicide as the only solution.” The role of cognitive style as a protective factor was less persuasive, with only two of four studies showing a significant interaction effect (Chang et al. 2007), including one study that found a greater buffering effect at lower levels of the risk factor (Wolff et al. 2014). It may be that cognitive errors and the negative cognitive triad play more of a role as a risk factor for suicidal ideation and behavior (Gould et al. 2003; Walsh and Eggert 2007) rather than as a protective factor. It should be noted, however, that researchers have not yet explored several cognitive factors that have been linked to suicidal outcomes, including hopelessness (Esposito-Smythers et al. 2014) and cognitive flexibility (Miranda et al. 2012).
Self-esteem and Self-perception
An individual’s perception of oneself, including elements of self-esteem, self-worth, self-acceptance, and level of self-criticism, also has been linked to suicidal ideation and behavior in youth (e.g., Bearman and Moody 2004; Breton et al. 2015; Li et al. 2012; Walsh and Eggert 2007). Five studies focused on protective factors related to an individual’s level of self-esteem or self-acceptance. Research looking at self-esteem as a potential protective factor found that self-esteem buffered against suicidal ideation among students with depressive symptoms but did not do so for those with eating disorder symptoms (Brausch and Decker 2014). Similarly, self-esteem did not moderate the link between anxiety symptoms and either suicidal ideation or attempts (Yen et al. 2014), and self-image did not buffer the relationship between adopted child status and suicide attempts (Slap et al. 2001). Studies focused on self-acceptance as a protective factor also found null results suggesting that this factor does not buffer against suicidal ideation in the presence of depressive symptoms (Lee 2011) or against suicidal ideation and attempts in the presence of peer victimization in a sample of lesbian, gay, and bisexual teens (Hershberger and D’Augelli 1995).
Two studies focused on feelings of inferiority and self-criticism as potential moderating factors. Goodwin and Marušič (2003) found that feelings of inferiority moderated the link between a diagnosis of Panic Attack and suicidal ideation (but not suicide attempts), with trend-level findings suggesting that this factor also may play a role in buffering the impact of Social Phobia and Agoraphobia diagnoses on suicidal ideation (but not suicide attempts) and the impact of a Major Depressive Disorder diagnosis on suicide attempts (but not ideation). Meanwhile, Wedig and Nock (2007) showed that low levels of adolescent self-criticism attenuated the impact of parental expressed emotion on a composite variable representing suicidal ideation, plans, attempts, and non-suicidal self-injury.
Overall, the research examining the role of self-perception as a potential protective factor paints an inconsistent picture. Of five studies examining self-esteem or self-acceptance, only one showed a protective effect for self-esteem (Brausch and Decker 2014). Furthermore, although this study found that self-esteem moderated the relationship between depressive symptoms and suicidal ideation, a similar study found that self-acceptance did not moderate the relationship between depressive symptoms and suicidal ideation (Lee 2011). Additionally, self-esteem did not serve as a protective factor for individuals with high levels of either eating disorder symptoms (Brausch and Decker 2014) or anxiety symptoms (Yen et al. 2014). Given the inconsistent findings regarding self-esteem and self-acceptance, it is interesting that two studies found that variables representing the inverse of these constructs—low levels of self-criticism and feelings of inferiority—buffered against suicidal outcomes (Goodwin and Marušič 2003; Wedig and Nock 2007). It may be that reduced levels of negative self-perception, rather than heightened levels of positive self-perception, plays a more important role in providing resilience to suicidal ideation and behavior in children and adolescents. Alternatively, it may be that a more nuanced approach is needed in evaluating self-esteem as a protective factor given research that has identified specific domains of self-esteem related to appearance, athleticism, personal self, behavior, morals/ethics, and other domains (Gentile et al. 2009).
Emotion Regulation and Self-control
Also implicated in the development of suicidal ideation and behavior in youth are variables related to an individual’s ability to identify and regulate emotions (e.g., Deeley and Love 2013; Lewinsohn et al. 1993; Li et al. 2012; Walsh and Eggert 2007). Only four studies examined emotion regulation-related constructs as protective factors. Research found that overall emotional intelligence—defined as the ability to reason about emotions and use emotions to guide behavior—attenuated the impact of childhood sexual abuse on both suicidal ideation and attempts, with strategic emotional intelligence (i.e., the ability to understand and regulate emotions) also acting as a significant moderator while experiential emotional intelligence (i.e., the ability to perceive emotions in others) failed to do so (Cha and Nock 2009). Similarly, Tamás and colleagues (2007) found that adaptive emotion regulation moderated the relationship between both shyness and sociability and suicide attempts (but not suicidal ideation or planning). Emotion regulation buffered at low levels of sociability and at low levels of shyness, suggesting that emotion regulation may not be as relevant for highly introverted teens.
Two other studies evaluated emotional empathy and self-control as potential protective factors against suicidal ideation and behavior in youth. Kwok and colleagues (2015) found that emotional empathy attenuated the effect of physical abuse on suicidal ideation, an interaction effect that was trend-level in the total sample but significant for female (but not male) adolescents. Furthermore, the research pointed to a cross-over interaction such that low levels of empathy buffered for those with a history of physical abuse, while high empathy buffered for those without an abuse history (Kwok et al. 2015), a finding that is consistent with research suggesting that lower levels of emotional perception buffers against suicidal ideation in the presence of daily hassles (Ciarrochi et al. 2002). A final study found that high self-control (a variable representing a composite of low impulsivity and risk-taking) attenuated the impact of both traditional bullying (i.e., verbal or physical bullying) and cyberbullying on suicidal ideation (Hay and Meldrum 2010).
Taken together, the literature suggests that the ability of an adolescent to understand and cope with his or her own emotions may offer resilience to suicidal ideation and behavior. However, it should be noted that the current research in this area covers only a small fraction of the constructs associated with emotion regulation and personal control. Future research should focus on other aspects of emotion regulation and coping that have been shown to play a role in youth suicidal ideation and behavior, including emotion self-confidence, emotional adaptation and well-being, personal control, productive coping strategies, and coping self-efficacy (e.g., Borowsky et al. 2001; Breton et al. 2015; Deeley and Love 2013; Li et al. 2012; Walsh and Eggert 2007; Wang et al. 2011). The current research largely focuses on suicide risk factors related to interpersonal bullying or abuse. Future research on emotion regulation as a protective factor may wish to expand the range of risk factors to include consistent predictors of suicidal ideation and behavior like daily hassles, life or chronic stress, or psychopathology.
Other Individual Abilities, Beliefs, and Characteristics
A total of eight studies examined other individual abilities, beliefs, and characteristics as protective factors. A single study found that a higher grade point average (GPA) buffered the link between sexual abuse and suicidal ideation, although this effect was significant only for female students (Luster and Small 1997). Four studies examined the role of psychological symptoms as potential moderators of suicide-related outcomes. However, although Miller and Esposito-Smythers (2013) found that both fewer alcohol-related problems and fewer drug-related problems moderated the relationship between child maltreatment and suicidal ideation, other studies found null results. Neither depressive symptoms nor alcohol use moderated the link between anxiety symptoms and either suicidal ideation or attempts (Yen et al. 2014), depressive symptoms did not buffer the link between adopted child status and suicide attempts (Slap et al. 2001), and neither internalizing nor externalizing symptoms moderated the relationship between physical abuse and either suicidal ideation or attempts (Salzinger et al. 2007).
An additional three studies focused on personal beliefs and attitudes. Greening and Stoppelbein (2002) found that high levels of religious orthodoxy, defined as degree of belief and acceptance of traditional Christian doctrines, attenuated the effect of depressive symptoms on perceived suicide risk (i.e., one’s perceived likelihood of dying from 19 different lethal events). A second study found that self-reported reasons for living (i.e., total score on a scale that measures future optimism, self-acceptance, and other potential reasons for living) moderated the relationship between depressive symptoms and suicidal ideation (Lee 2011). Finally, a third study showed that higher levels of self-rated resilience (i.e., total score on a scale assessing personal competence, social competence, spiritual influences and other protective factors) buffered the link between a history of violent life events and suicide attempts (Nrugham et al. 2010).
On the whole, the research on individual beliefs and characteristics points to several research directions. Research on academic functioning (Luster and Small 1997; Borowsky et al. 2001; Lewinsohn et al. 1993) and aspects of religiosity (Sherman et al. 2014) as protective factors for suicidal ideation and behavior is warranted. The current research also suggests that psychological symptoms do not function as a protective factor, given generally null findings (Salzinger et al. 2007; Slap et al. 2001; Yen et al. 2014).
Ecological Resources that Promote Resilience to Suicidal Ideation and Behaviors
Parent–Child Relationship
A total of four studies focused on youth’s perception of parental support or factors that may impact the provision or perception of support. Parental support was shown to buffer the relationship between both sexual abuse and suicidal ideation (Luster and Small 1997) and depressive symptoms and suicidal ideation (Brausch and Decker 2014), although the latter study found that parental support did not buffer the link between eating disorders and suicidal ideation. Likewise, a separate study found that parental support did not moderate the relationship between homophobic teasing and depressive symptoms/suicidal ideation among lesbian, gay, bisexual, and sexually questioning teens (Espelage et al. 2008). With respect to factors that may impact a youth’s perception of parental support, one study found that both parental rejection and the presence of a parental internalizing disorder (i.e., an anxiety or depressive disorder) moderated the relationship between peer victimization and suicidal ideation. However, the researchers found that the presence of a parental externalizing disorder did not moderate this relationship (Herba et al. 2008).
An additional three studies examined specific aspects of the parent–child relationship. Kwok and Shek (2010) found that both mother– and father–adolescent communication attenuated the impact of feelings of hopelessness on suicidal ideation, with biological sex-specific analyses indicating that this buffering effect was present for male students only. Similarly, a second study revealed a cross-over interaction in which lower levels of emotional detachment from parents (i.e., hostile disengagement from parents rooted in distrust and alienation) buffered against suicidal ideation among youth with high levels of depressive symptoms, while higher levels of emotional detachment buffered against suicidal ideation for youth with low levels of depression (Pace and Zappulla 2010). This same study showed that emotional separation from parents (i.e., emotional individuation without negative feelings) was not a significant moderator. Similarly, Salzinger and colleagues (2007) found that attachment to parents—a construct that encompasses the enduring emotional bond between child and caregiver—did not buffer against either suicidal ideation or suicide attempts in youth with a history of physical abuse.
Five other studies focused on various aspects of parenting style. Authoritative parenting (i.e., setting limits, reasoning with children, and being responsive to their emotional needs) moderated the link between both traditional peer victimization (e.g., physical and verbal bullying) and cyberbullying victimization and suicidal ideation (Hay and Meldrum 2010). Meanwhile, authoritarian parenting (i.e., more restriction/rules, less flexibility, and a focus on obedience) was shown to buffer the link between depressive symptoms (but not aggression) and suicidal behavior, although further analyses found that this type of parenting buffered against suicidal behavior in two specific subgroups: older children aged 10–12 and African-American children (Greening et al. 2010). Studies focused on more specific elements of parenting style found that parental monitoring (i.e., awareness of a child’s activities) attenuated the impact of sexual abuse on suicidal ideation (Luster and Small 1997), while parental control (i.e., control over the child’s behavior through rules and limit-setting) moderated the relationship between hopelessness and suicidal ideation for female students only (Kwok and Shek 2008). Two studies examining parental concern (i.e., caring for and attending to the needs of the child) found inconsistent results. Parental concern buffered the link between hopelessness and suicidal ideation (Kwok and Shek 2008), but did not moderate the relationship between either physical abuse or psychological abuse and suicidal ideation (Kwok et al. 2013).
Taken together, research suggests that the parent–child relationship may play a role in conferring resilience to suicidal ideation and behavior in youth. Several studies indicated that high levels of parental support (or, conversely, low levels of parental rejection) offered resilience, although a risk factor-specific pattern was present: parental support buffered against suicidal outcomes for youth with a history of sexual abuse, depressive symptoms, and peer victimization, but did not do so for youth with a history of eating disorder symptoms or homophobic teasing (Brausch and Decker 2014; Espelage et al. 2008; Herba et al. 2008; Luster and Small 1997). Similarly, several studies pointed to a role for parenting style as a potential protective factor against suicidal ideation and behavior, including both authoritarian and authoritative parenting (Greening et al. 2010; Hay and Meldrum 2010) as well as aspects of parenting style such as parental control, concern, and monitoring (Kwok and Shek 2008; Luster and Small 1997). Across these parent-related variables, it should be noted that age-, biological sex-, and ethnicity-specific effects existed, such that parent–child communication may be more relevant for males (Kwok and Shek 2010), parental control may be more important for females (Kwok and Shek 2008), and authoritarian parenting may play more of a role for both older children and African–American children (Greening et al. 2010). Given that the majority of research in these parent domains focused on suicidal ideation (9 out of 12 total studies), future research should include a broader range of suicidal outcomes, including suicide attempts. In addition, research has not yet explored a number of important constructs related to both the parent–child relationship and parenting style, such as parent–child connectedness, parent–adolescent shared activities, and parental expectations for their child (Borowsky et al. 2001; Rew et al. 2001).
Family Functioning
Six studies have focused on either overall family functioning or family support as protective factors. High family functioning moderated the link between hopelessness and suicidal ideation in female students only (Kwok and Shek 2008), and buffered the relationship between poor social problem-solving ability and suicidal ideation in male students only (Kwok and Shek 2009). In contrast, family functioning did not moderate the link between anxiety symptoms and either suicidal ideation or suicide attempts (Yen et al. 2014). Similarly, studies focused on perceived family support as a potential protective factor found non-significant results. Family support showed a trend-level effect in moderating the link between depressive symptoms and a proxy measure of suicidal ideation and behavior (i.e., reasons for living) in a sample of African-American high-schoolers (Matlin et al. 2011), but family support did not buffer the link between peer victimization and suicidal ideation (Wolff et al. 2014) and did not attenuate the impact of peer victimization on suicidal ideation and behavior (i.e., suicidal ideation and behavior) in a sample of lesbian, gay, and bisexual teens (Hershberger and D’Augelli 1995).
Five additional studies focused on specific aspects of family functioning. Research focused on hopelessness as a risk factor showed that family mutuality was a moderator for females only, family communication was a moderator for males only, and low levels of conflict was a moderator for the entire sample (Kwok and Shek 2008). Similarly, a second study found that family mutuality and family communication attenuated the effect of physical abuse (but not psychological abuse) on suicidal ideation (Kwok et al. 2013). However, although mutuality and communication buffered against ideation at both low and high levels of physical abuse, the buffering effect was greater at low levels of physical abuse. Meanwhile, Lee (2011) showed that family alliance moderated the link between depressive symptoms and suicidal ideation for male students only, while Pisani and colleagues (2013) found that the presence of a trusted adult in the family buffered the link between poor emotion regulation and suicide attempts. In contrast, Kwok and colleagues (2013) showed that low levels of family conflict did not buffer the impact of physical or psychological abuse on suicidal ideation, while other research showed that family connectedness did not moderate the link between adopted child status and suicide attempts (Slap et al. 2001).
Overall, the current research indicates that a range of family-related variables may help to confer resilience to suicidal ideation and behavior in children and adolescents. However, the literature suggests that holistic indicators of family health (e.g., family support or family functioning) may be less useful indicators of resilience to suicidal ideation and behavior in youth, whereas more specific aspects of family functioning (e.g., family communication or family conflict) do function as protective factors. Many of these more specific protective effects were biological sex-linked, suggesting a more complex picture of how family interactions can impact suicide risk. Future research may wish to examine biological sex-specific effects in addition to overall effects in determining whether a given family-related factor provides resilience to suicidal ideation and behavior in youth.
Friends and Peers
Four studies have examined the role of peer support in buffering against suicidal outcomes in youth. Lee (2011) found that peer acceptance/support moderated the link between depressive symptoms and suicidal ideation but did so only for female students. Likewise, a second study showed that peer support attenuated the impact of depressive symptoms on a proxy measure of suicidal ideation and behavior (i.e., reasons for living) in a sample of African-American high-school students, although results indicated that peer support buffered against risk to a greater degree among youth with low to moderate levels of depression, suggesting that peer support may play a more limited resilience role in highly depressed teens (Matlin et al. 2011). A third study found disorder-specific effects: peer support moderated the link between eating disorder symptoms and suicidal ideation but did not buffer the relationship between depressive symptoms and suicidal ideation (Brausch and Decker 2014). Similarly, peer support did not buffer the link between peer victimization and suicidal ideation (Wolff et al. 2014).
Four additional studies focused on specific aspects of peer relationships. One study found that lower levels of homophobic teasing attenuated the effect of minority sexual orientation (i.e., self-identified lesbian, gay, bisexual, or sexually questioning) on depression/suicidal ideation (Birkett et al. 2009). Likewise, lower levels of peer victimization moderated the relationship between anxiety symptoms and suicidal ideation (but not suicide attempts) (Yen et al. 2014). However, the risk for suicidal ideation was higher among those students without a history of peer victimization. Other studies on potential peer-related protective factors found similarly inconclusive results. Youth’s social well-being among classmates did not buffer the relationship between peer victimization and suicidal ideation (Herba et al. 2008), while attachment to peers did not moderate the link between physical abuse and either suicidal ideation or attempts (Salzinger et al. 2007).
Taken as a whole, the current research yields an inconsistent picture of the role that peer relations plays in conferring resilience to suicidal ideation and behavior in youth. Although several studies found that peer support attenuated the impact of risk-related variables on suicidal ideation and behavior, results were inconsistent. Some studies show that peer support moderated the impact of depressive symptoms on ideation only in females (Lee 2011) or at lower levels of depression (Matlin et al. 2011), and other studies show that peer support moderated the impact of eating disorder symptoms (but not depressive symptoms) on ideation (Brausch and Decker 2014). The current research also is hampered by a focus on suicidal ideation, with only two of eight studies including suicide attempts as an outcome (Salzinger et al. 2007; Yen et al. 2014), as well as a focus on broader social dynamics such as peer support or peer victimization to the exclusion of friendship-related variables. Future research may wish to examine potential protective factors related to a youth’s closer friend circle, such as the availability of close friends, a dense friendship network, and more transitive friendships (Bearman and Moody 2004; King and Merchant 2008).
School Environment
Five studies focused on school-related protective factors. Three studies on school climate revealed consistent results. A positive school climate (i.e., perception that one is obtaining a good education and that there are caring adults at school) attenuated the impact of minority sexual orientation (i.e., lesbian, gay, bisexual, or sexually questioning) on depression/suicidal ideation (Birkett et al. 2009). Similarly, a positive school climate moderated the link between homophobic teasing and depression/suicidal ideation in a sample of lesbian, gay, bisexual, and sexually questioning students (Espelage et al. 2008). Likewise, a school climate supportive of minority sexual orientation (e.g., via staff trainings, a Gay-Straight Alliance) reduced risk for suicidal ideation—but not plans or attempts – in a sample of lesbian, gay, and bisexual students (Hatzenbuehler et al. 2014). Two other studies focused on the presence of trusted adults at school. Duong and Bradshaw (2014) found that the presence of an adult connection at school buffered the link between cyberbullying/school bullying and suicide attempts in a sample of lesbian, gay and bisexual high-school students. In contrast, the presence of a trusted adult at school did not buffer the link between emotion regulation deficits and suicide attempts (Pisani et al. 2013). Overall, research in the domain of a youth’s school environment suggests that variables such as school climate and the presence of caring, supportive adults at school may buffer against suicidal ideation and behavior.
Community and Culture
Four studies have focused on engagement in activities and community/cultural connectedness as protective factors. Armstrong and Manion (2015) found that engagement in meaningful activities (i.e., activities that promote success and challenge) buffered the link between a variety of risk factors—depressive symptoms, risky behavior, low self-esteem, and low social support—and suicidal ideation. However, the authors found that breadth of engagement (i.e., number of activities) attenuated only the impact of depressive symptoms and low self-esteem on ideation, while intensity (i.e., frequency) of activity engagement was not a significant moderator for any risk factor (Armstrong and Manion 2015). Cero and Sifers (2013) showed that both community service and participation in sports, clubs or other youth programs attenuated the effect of physical abuse on suicide attempts. With respect to cultural/community connection, Matlin and colleagues (2011) found that community connectedness (i.e., strength of the social cohesion and support, collective efficacy, and social capital within a person’s neighborhood) buffered the link between depressive symptoms and a proxy measure of suicidal ideation and behavior (i.e., reasons for living) in African-American students. A study focused on Asian-American teens found that higher levels of acculturation (as indexed by English-language proficiency, primary language at home, and proportion of life in the U.S.) moderated the relationship between parent–child conflict and suicidal ideation/attempts (Lau et al. 2002).
Overall Social Support
Six studies examined a range of variables related to a youth’s perception of overall social support. Esposito and Clum (2003) found that overall support (across family, peers, and teachers) attenuated the impact of comorbid internalizing/externalizing symptoms on suicidal ideation. Similarly, social support satisfaction (i.e., based on support received from up to nine individuals) moderated the link between sexual abuse—but not physical abuse—and both suicidal ideation and attempts (Esposito and Clum 2002). However, this study found that the number of social support sources was not a significant moderator. Similarly, Rigby and Slee (1999) showed that overall social support (across parents, friends, peers, and teachers) did not moderate the link between bullying experiences and suicidal ideation. Three additional studies focused on other aspects related to social support, including feelings of loneliness and community support. With respect to the former, lower levels of loneliness was shown to buffer the relationship between frequency of being bullied and both suicidal ideation and attempts (Cui et al. 2010). However, a second study found that feelings of loneliness did not moderate the link between physical abuse and suicidal ideation or suicide attempts (Salzinger et al. 2007). Likewise, Hatzenbuehler (2011) showed that a community climate supportive of minority sexual orientation (e.g., via a high proportion of same-sex couples in surrounding counties and a high proportion of schools with Gay-Straight Alliances) did not reduce risk for suicide attempts in lesbian, gay, and bisexual high-schoolers.
As a whole, the findings on protective factors related to community, cultural, and social engagement point to a need for additional research in this area. On the one hand, the literature suggests that meaningful engagement in the community can reduce risk for suicidal ideation and behavior associated with a variety of risk factors (e.g., Armstrong and Manion 2015; Cero and Sifers 2013). However, research focused on the role of general social support (i.e., support across all sources, including teachers, parents, peers, friends, and family) was mixed, with several studies suggesting that total social support can buffer against suicide risk in teens (Cui et al. 2010; Esposito and Clum 2002, 2003) and other studies finding no effect of overall social support (e.g., Hatzenbuehler 2011; Rigby and Slee 1999; Salzinger et al. 2007). These inconsistent findings mirror research focused on more specific sources of support, in which findings were shown to be either inconsistent (i.e., for peer support), disorder-specific (i.e., for parent support), or not significant (i.e., for family support). Future research may need to find a more articulated, multi-dimensional way of measuring social support that captures the amount and quality of social support received by a child/adolescent. Only two studies focused on cultural variables (e.g., acculturation) as potential protective factors (Lau et al. 2002; Matlin et al. 2011), pointing to a need for additional research in this area.
Discussion
This review summarized existing research on protective factors that buffer against suicide-related outcomes in children and adolescents, with a focus on resilience as conceptualized by Luthar and colleagues (2000): an array of factors that promote positive adaptation in the context of risk and adversity. In keeping with modern conceptualizations of resilience (e.g., Luthar et al. 2000; Wright et al. 2013), this review suggests that resilience is a multi-domain, multi-dimensional process encompassing a youth’s individual assets (e.g., problem-solving ability, emotion regulation) as well as ecological resources, which include: the parent–child relationship (e.g., parental support, parenting style), the family domain (e.g., facets of family functioning, such as alliance and conflict), the peer context (e.g., peer support and acceptance), the school domain (e.g., supportive school climate, connection to a caring adult), and the community and cultural context (e.g., community engagement, overall social support).
Although the current review provides evidence of multiple domains of resilience against suicidal outcomes in youth, the review also revealed weaknesses in the literature. A significant concern is the fact that most of the studies included in this article—while using a methodology consistent with Luthar and colleague’s (2000) conceptualization of resilience—were not explicitly designed to assess resilience. Thus, the body of literature as a whole is constrained, with separate and sometimes inconsistent findings that make it difficult to draw definitive conclusions about any given protective process. Below, we offer a critical examination of the existing literature and offer recommendations for future research. The following sections will provide a critical examination of the literature organized around four primary themes: (1) measurement-related issues, including the use of a limited range of risk factors, the use of single- or limited-item measure to represent key study variables, a disproportionate emphasis on suicidal ideation as the study outcome, and the use of composite outcome variables that conflate suicide-related constructs; (2) methodological and analytical issues, including an overreliance on cross-sectional designs, a lack of ethnic diversity within samples, an overreliance on non-clinical samples, a lack of research exploring biological sex differences in resilience, and inconsistency in how interaction effects were tested and how results were graphically presented; (3) suggestions for future research, with a focus on grounding resilience research in existing theoretical accounts of suicide and using comprehensive, multi-dimensional designs; (4) a discussion of clinical implications for suicide prevention efforts; and (5) a discussion of developmental contributions.
Measurement-Related Issues
Although the current review identified a number of protective factors that may play a role in resilience (e.g., problem-solving ability, parental support), evidence for other protective factors was less persuasive. While these inconsistent results may be valid, it is also possible that limitations in measurement may have played a role.
Narrow Range of Risk Factors
A weakness in the current literature is the narrow range of risk factors that have been used to explore suicide-related resilience. Of the 41 studies in the current review, only four risk factors were examined thoroughly enough to identify patterns or inconsistencies in the way that protective factors buffer against suicidal ideation and behavior in that area of risk: depressive symptoms, physical or sexual abuse, peer victimization, and sexual orientation. An initial focus on these risk domains in the resilience literature would make sense (Cash and Bridge 2009; King and Merchant 2008). However, the next step in resilience research will be to examine other common risk factors, such as psychopathology other than depressive symptoms. Research has shown that a range of mental health issues place youth at risk for suicidal ideation and behavior: bipolar disorder, anxiety disorders, eating disorders, post-traumatic stress disorder, conduct disorder, and oppositional defiant disorder (Goldston et al. 2009; Gould et al. 1998). Each psychiatric risk factor should be explored across the range of individual and sociocultural protective factors, given evidence that disorder-specific effects exist for protective factors, such as self-esteem and social support (e.g., Brausch and Decker 2014; Goodwin and Marušič 2003).
Another risk factor that has not yet been evaluated in the resilience literature is a history of alcohol or substance use. Alcohol and substance use has been implicated as both a distal risk factor (i.e., increasing stress and exacerbating psychopathology) and as a proximal trigger (i.e., increasing distress and impulsivity while lowering inhibition) for suicidal ideation and behavior in teens (Esposito-Smythers et al. 2014), and future research is needed to explore alcohol/substance use as both an individual risk factor and as a comorbid condition with depression or other psychiatric risk factors. Finally, although several studies provide initial evidence with respect to negative life events (Chang 2002; Grover et al. 2009; Nrugham et al. 2010), more research is needed to fully understand how protective factors can buffer against negative life events. In particular, research is needed to explore a broader range of difficult life events, including sources of episodic life stress (i.e., interpersonal conflict, parental divorce, academic troubles, or a move to a new geographic location) as well as sources of chronic life stress (i.e., living in a dysfunctional family environment, parent psychopathology, discrimination, or coping with a chronic illness).
Use of Single-item or Limited-item Measures
A second measurement-related issue revolves around the use of single- or limited-item measures of study constructs. Just over half of the studies in the current review (N = 24) used at least one single- or limited-item measure. The use of multi-item scales to measure a construct is considered to be psychometrically superior to the use of single items, with some recommending that a multi-item measure contain at least four items. Furthermore, single items reference only one conceptualization of a construct, making single items more vulnerable to respondent bias (Hoeppner et al. 2011). The issue of measurement error is especially important for moderation analysis. Measurement error in individual variables reduces the reliability of the interaction term built from those variables, resulting in an increased standard error of the interaction term and reduced power to detect statistically significant results (Frazier et al. 2004).
For some studies included in the present review, a single item may have been a logical choice given the construct, i.e., adoption status (e.g., Slap et al. 2001). In other cases, such as childhood sexual abuse (e.g., Luster and Small 1997), there may have been a lack of validated multi-item scales to assess the construct (see Walsh et al. 2004). However, for many studies, the inclusion of a multi-item scale would improve the quality of the research. Using such established, well-validated measures would allow researchers to more reliably compare resilience findings across studies. Similarly, future research would benefit from the use of well-established measures of suicidal ideation such as the Suicidal Ideation Questionnaire (Reynolds 1987) or the Modified Scale for Suicidal Ideation (Miller et al. 1986). Given that ideation is a multi-faceted construct that can be quantified by frequency, duration, severity, controllability, and level of intent, it is concerning that nearly half of the 41 studies used just one or two (often dichotomous) items to measure suicidal ideation.
Measurement Issues Related to Suicide Outcomes
Although suicide-related outcomes exist on a spectrum (not exclusively linear) from suicidal ideation to nonfatal suicide attempts to completed suicide (Silverman et al. 2007), this review suggests that the literature is overly reliant on studies using suicidal ideation as the outcome. Nearly half of the identified studies (N = 20) focused on suicidal ideation as the sole outcome, and no studies have as yet focused on death by suicide. Given that suicidal ideation is nearly twice as prevalent as attempts (CDC 2013b) and can be more readily assessed in community samples, ideation often is the outcome of choice in suicide research. However, while suicidal ideation is important as a unique outcome given its association with psychological distress and future suicidal behavior (Posner et al. 2014), it is vital that future research expand its focus to examine resilience to suicidal behaviors such as suicide attempts and death by suicide. In fact, the current review suggests that the effectiveness of protective factors may differ by suicide outcome, with variables such as problem-solving confidence and a supportive school climate buffering against ideation but not attempts (e.g., Esposito and Clum 2002; Hatzenbuehler et al. 2014), and variables such as adaptive emotion regulation reducing risk for attempts but not ideation or planning (e.g., Tamás et al. 2007). Part of this expansion should be a specific focus on the transition from suicidal ideation to attempts. Considering the fact that most teens with suicidal ideation do not go on to make an attempt, it is vital to identify sources of resilience that could help to buffer against eventual suicidal action in the presence of ideation.
A second concern is the use of measures that combine suicidal constructs or conflate suicidal ideation and behavior with other forms of psychological distress. The present review revealed a number of studies that used composite variables combining questions about suicidal ideation with questions about suicide attempts to create an index of “suicidality” (e.g., Hershberger and D’Augelli 1995; Lau et al. 2002; Matlin et al. 2011). Meanwhile, other studies further obscured the nature of the suicide-related outcome by using proxy variables to indirectly gauge suicide risk, e.g., “perceived suicide risk” (perceived risk of dying from 19 lethal events, including suicide) (Greening and Stoppelbein 2002). Finally, several studies used composite variables that combined suicidal ideation and/or behavior with other types of psychological distress, e.g., suicidal ideation and depressive symptoms (Birkett et al. 2009; Espelage et al. 2008) or suicidal ideation, plans, and attempts, and non-suicidal self-injury (Wedig and Nock 2007). As has been suggested in the literature (e.g., Posner et al. 2014), future research should attend to the importance of using clearly defined suicide constructs. In doing so, it is important that researchers dissociate suicidal ideation and behavior from related psychological constructs like depressive symptoms or non-suicidal self-injury, given that these latter constructs have been shown to be distinct from suicidal ideation and behavior, with differing presentations, risk factors, and sequelae (Butler and Malone 2013; Esposito-Smythers et al. 2014).
Issues with Study Design and Analysis
A Need for Longitudinal Research
Given that only one of the 41 studies included this review used a longitudinal design (Salzinger et al. 2007), there is a clear need for more longitudinal research examining resilience to suicidal ideation and behaviors in youth. Modern views on resilience view it as a dynamic process that unfolds over time, with resilience increasing or decreasing depending upon an individual’s current level of risk as well as changes in a person’s individual strengths and abilities or accessibility to social resources (Wright et al. 2013). In looking at only one point in time, cross-sectional designs limit researchers’ ability to examine when protective factors emerge and how they function over time to reduce suicide risk. Longitudinal research may be able to provide critical information about time periods that are crucial to the development of resilience, the temporal stability of protective factors, and the causal relationship between protective factors and reduced risk for future suicide.
Longitudinal research also would provide a needed developmental perspective, allowing researchers to account for intra-individual change as well as social and environmental change. The research to date focuses mostly on adolescents, with only five studies focused on children aged 11 or younger (Greening et al. 2010; Herba et al. 2008; Lau et al. 2002; Salzinger et al. 2007; Tamás et al. 2007). From a cross-sectional perspective, a focus on adolescents makes sense: suicidal ideation and behavior are far less prevalent prior to puberty, with steady increases across adolescence and into young adulthood (Esposito-Smythers et al. 2014). However, longitudinal studies spanning from childhood into adolescence would allow researchers to examine how risk and protective factors emerge and interact across the developmental timeline. For example, research may find that certain protective factors are influential in late childhood or early adolescence (e.g., parental support), while others become more important in mid- to late-adolescence (e.g., peer relationships and school context). The use of longitudinal studies would facilitate a more complex understanding of how risk and resilience interact over time, allowing for a richer account of how resilience emerges, develops, and functions to buffer youth against suicide risk.
A Need for More Diversity in Study Samples
The present review also revealed a need for research using more diverse and clinically distressed samples. With respect to racial and ethnic diversity, several concerns emerged. First, it should be noted that nearly one-third of the studies included in this review used an international sample (N = 14). Although this research provides support for the role of resilience in suicidal ideation and behavior, it also creates difficulties in integrating and interpreting findings. Perspectives on many key life domains are culturally mediated. For example, many Hispanic/Latino cultures place high importance on family closeness and unity (Ayón and Aisenberg 2010), and this value of familismo can influence Hispanic/Latino parenting practices as well as parent–child relationships (Guilamo-Ramos et al. 2007). Similarly, many East Asian cultures take an interdependent view of self that emphasizes collective welfare when engaging in social behavior. This collectivist view of self has implications for a person’s identity, self-esteem, relationships, communication style, parenting choices, and pursuit of life goals (Markus and Kitayama 1991). Thus, a given finding regarding self-esteem, parent–child communication, family support, or other protective factor may have drastically different implications depending on a participant’s culture of origin. In future research, scientists may wish to tease apart these cultural threads.
The current review also suggests a need for more racial/ethnic diversity within the subset of studies using North American samples. Of the 27 studies with U.S. or Canadian samples, only seven used diverse samples that were not predominately Caucasian. Such ethnically homogenous samples offer little insight as to how protective factors function across cultures. Such research is sorely needed, given ethnic differences in suicidal ideation and behavior. Although Caucasian youth typically show higher rates of suicide death, rates of serious suicidal ideation and medically serious attempts are higher in Hispanic/Latino youth (CDC 2013b). Meanwhile, suicidal ideation and behavior are highest among Alaskan Native/Native American youth (Esposito-Smythers et al. 2014), while African-American youth historically have had the lowest rates of suicidal ideation and behaviors (CDC 2013b; Esposito-Smythers et al. 2014). Further emphasizing the need to explore ethnic differences in protective factors is the fact that the effectiveness of many compensatory factors (i.e., main effects) differs by ethnicity (Borowsky et al. 2001). To date, only one study has examined ethnic differences in protective factors: Greening and colleagues (2010) found that authoritarian parenting buffered the link between depressive symptoms and suicidal ideation and behavior for African-American (but not Caucasian) youth, in keeping with research suggesting differences in the effectiveness of authoritarian and authoritative parenting in these groups (see Tamis-LeMonda et al. 2008, for a review).
Future research in this area also would benefit from research targeted to specific minority populations. Only five studies in the current review took such an approach, focusing on Asian–American (Lau et al. 2002), African–American (Matlin et al. 2011), and lesbian, gay, and bisexual youth (Duong and Bradshaw 2014; Espelage et al. 2008; Hershberger and D’Augelli 1995). The literature on culture-specific compensatory factors (i.e., main effects) suggests several future directions. With respect to Alaskan Native/Native American youth, studies have identified a number of cultural variables that could be explored within a resilience framework: cultural activities, tribal participation, relationships with community leaders, cultural continuity, strong cultural identity and tribal-based spirituality all have been shown to protect against suicidal outcomes in these teens (Allen et al. 2014; Cwik et al. 2015; Garroutte et al. 2003; Kral et al. 2009; LaFromboise et al. 2007). Similarly, the literature points to the value of examining family closeness and religion/spirituality as protective factors for Hispanic/Latino and African-American youth, given that these factors have been shown to reduce risk for suicidal ideation and behavior in both groups (O’Donnell et al. 2004; Sherman et al. 2014). Research especially is needed to evaluate which aspects of religion/spirituality are “active” in buffering against suicidal ideation and behavior, e.g., faith-based coping, the availability of support from the religious community, and/or adherence to religious proscriptions against suicide. Likewise, more research is needed to tease apart which specific aspects of social support help to buffer against suicidal outcomes in lesbian, gay, and bisexual youth, such as parental support related to the process of coming out as LGB, school safety, anti-LGB-bullying efforts, and larger community attitudes toward sexual minorities (Sherman et al. 2014).
A move toward research that focuses on specific minority populations, such as Native American or LGB youth, should be part of a larger goal of examining resilience to suicidal ideation and behavior in more clinically distressed individuals. Much of the current literature has been conducted using non-clinical school-based or epidemiological samples, with only 16 studies focused on psychiatric inpatients or outpatients or other at-risk youth (e.g., youth who are incarcerated, economically disadvantaged, homeless, or experiencing chronic stressors such as illness or disability). Although important to examine suicidal phenomena across settings, including within the school and community context, it is also vital that research be able to capture the full spectrum of suicidal ideation and behavior. The use of nonclinical populations may help to explain the literature’s heavy emphasis on suicidal ideation rather than suicide attempts, given that ideation is more prevalent than attempts and can be more easily examined in community samples. Future research in this area would benefit from more research with clinical populations, where researchers would be able to capture a greater range of suicidal ideation and behavior, including more severe and chronic suicidal ideation as well as recent suicide attempts.
A Need for Research that Considers Biological Sex
The results of the current review suggest a need for more biological sex-specific research into resilience. Only eight studies in the current review specifically tested for biological sex-related differences in resilience (Hatzenbuehler 2011; Kwok and Shek 2008, 2009, 2010; Kwok et al. 2015; Lee 2011; Luster and Small 1997; Pace and Zappulla 2010), a fact that is surprising given that biological sex differences exist for many suicide risk factors (e.g., depression, substance abuse, and aggressive and impulsive behavior) as well as for prevalence rates across the spectrum of suicidal ideation and behavior (Esposito-Smythers et al. 2014), including higher rates of completed suicide among males (CDC 2013a) and higher rates of ideation, planning, and attempts among females (CDC 2013b). Although half of the studies in the present review incorporated biological sex as a covariate, an argument can be made that the influence of biological sex on resilience should be directly examined. The eight studies that have so far probed for biological sex effects suggest that this may be a fruitful pursuit: six of the studies found biological sex differences suggesting that parental control, family mutuality, empathy, rational problem-solving, peer acceptance/support and academic achievement are particularly effective in promoting resilience for teenage girls, while parent/family communication and family alliance may be more important for teenage boys (Kwok and Shek 2008, 2009, 2010; Kwok et al. 2015; Lee 2011; Luster and Small 1997). In terms of future research, studies have revealed biological sex differences on an array of potential protective variables, including peer relationships (Rose and Rudolph 2006), cognitive style (Hankin and Abramson 2001), emotional expression and regulation (Kring and Gordon 1998; Zimmerman and Iwansi 2014), domains of self-esteem (Gentile et al. 2009), and traits such as inhibitory control and surgency (Else-Quest et al. 2006). Each of these possible protective factors is worth examining through the lens of biological sex.
Issues with Data Analysis and Presentation
The present review also revealed considerable variability in the analytic approach used to evaluate and present interaction effects. One key issue that arose is inconsistency in how multiple risk and/or protective factors were analyzed within a single study. Although a number of studies chose to reduce the number of separate analyses by including all risk and/or protective factors in the same model (e.g., Greening et al. 2010; Herba et al. 2008; Matlin et al. 2011; Tamás et al. 2007), others analyzed each protective factor or risk factor separately (i.e., separating models by protective factor or by risk factor), raising concerns about the possibility of an increased Type I error rate resulting from the large number of statistical analyses (Frazier et al. 2004). Although this is less problematic for studies resulting in only two or three total models (e.g., Birkett et al. 2009; Espelage et al. 2008), it is a more serious issue for studies resulting in six or eight total models (e.g., Kwok et al. 2015; Luster and Small 1997). Resilience research can only benefit from more complex studies that examine a given protective factor across different risk situations or that examine multiple protective factors in relation to a given source of risk. In doing so, however, researchers must attend to the potential for increased Type I errors by adjusting the significance level, as was done in some studies (e.g., Brausch and Decker 2014; Wolff et al. 2014), or by following recommendations to fold multiple moderators into a single model (Frazier et al. 2004).
A second concern involves inconsistency in the inclusion of covariates in statistical analyses. A surprising number of studies (N = 8) did not control for any covariates in their analyses, while others were inconsistent in their approach. Of particular concern was the failure to include covariates that are highly related to both study variables and suicidal outcomes. For instance, only 22 studies controlled for biological sex, 19 studies controlled for age, and 10 studies controlled for race/ethnicity, despite consistent research showing that these variables are associated with differences in youth suicidal ideation and behavior (Esposito-Smythers et al. 2014). Meanwhile, only three studies went beyond sociodemographic data to include variables that were theoretically meaningful to key study constructs, e.g., controlling for intrinsic and extrinsic religiosity in a study examining religious orthodoxy as a protective factor (Greening and Stoppelbein 2002). Similarly, only eight studies included covariates closely related to suicidal outcomes, such as depressive symptoms (e.g., Lau et al. 2002; Tamás et al. 2007) or feelings of hopelessness (Greening and Stoppelbein 2002; Grover et al. 2009). Including theoretically relevant covariates provides a stronger test of study relationships, and can ultimately influence results, as illustrated by Grover and colleagues (2009), who found that the buffering effect of problem-solving on the link between chronic and life stress and suicidal ideation and behavior was no longer present once depressive symptoms and hopelessness were added as covariates.
A final issue emerged with respect to the presentation of findings, with a number of studies providing insufficient information to fully evaluate the analyses and/or results. First, several studies failed to provide enough information to determine how analyses were performed, i.e., if a single model or multiple models were used or—if more than one model was used—exactly how these models were structured (e.g., Armstrong and Manion 2015; Cero and Sifers 2013; Goodwin and Marušič 2003; Pisani et al. 2013). Similarly, several studies did not fully explain why certain risk and protective factors were measured but not included in the statistical analyses (Cui et al. 2010; Esposito and Clum 2003; Kwok et al. 2015). Perhaps most importantly, however, is the fact that one quarter of the studies did not include a plot of the interaction effect, i.e., did not plot predicted values of the outcome at key levels of the moderator, generally at the mean and at one standard deviation above and below the mean (e.g., Armstrong and Manion 2015; Esposito and Clum 2003), or only provided plots for a subset of the significant interactions (e.g., Kwok and Shek 2008; Miller and Esposito-Smythers 2013). It has been recommended that studies examining interaction effects provide a plot so that readers can examine the specific form of the interaction (Frazier et al. 2004). The importance of including such a plot is underscored by a number of studies in the current review that found significant interaction effects that either were contrary to prediction or took an unexpected form (e.g., Kwok et al. 2015; Lau et al. 2002; Matlin et al. 2011; Tamás et al. 2007; Wolff et al. 2014).
Need for Theory-Driven Research
The current review used an ecological lens to frame resilience as a multi-dimensional, multi-domain construct involving individual assets and abilities as well as ecological resources (see Fig. 2). In further exploring this model, a key direction for future research will be to move from an approach that pairs individual risk factors with individual protective factors to a complex, multi-dimensional strategy guided by existing theoretical accounts of suicidal ideation and behavior, such as Joiner’s Interpersonal-Psychological Theory of suicide (IPT; Joiner 2005) or Williams’ Cry of Pain model of suicide (CoP; Williams 2001).
Overlap with Existing Theories of Suicidal Ideation and Behavior
The protective factors identified in the current study overlap with two prominent theories of suicidal ideation and behavior: Joiner’s Interpersonal-Psychological Theory of suicide (IPT; Joiner 2005) and Williams’ Cry of Pain model (CoP; Williams 2001). The IPT model proposes three distinct constructs that contribute to suicidal ideation and behavior. Two of these constructs, thwarted belongingness and perceived burdensomeness, contribute to an individual’s desire for death by suicide. Thwarted belongingness refers to an individual’s perception that he or she does not have meaningful connections to those around him or her (i.e., a sense of social isolation and a belief that others do not care for the person or understand the person’s worldview or experiences), whereas perceived burdensomeness refers to an individual’s sense that he or she does not meaningfully contribute to the world such that the world (i.e., family, friends, community) would benefit more from the person’s death than his or her life (Anestis and Joiner 2011). Meanwhile, the third component of the IPT model suggests that an individual acquires a capacity for lethal self-harm through an accumulation of risky, dangerous life experiences; this acquired capability for suicide is thought to be related to suicide attempts and completed suicide (Anestis and Joiner 2011).
Many of the protective factors identified in the current review are theoretically linked to two of the core IPT components: thwarted belongingness and perceived burdensomeness. With respect to thwarted belongingness, the current review strongly suggests a protective role for acceptance by, connection to and social support from parents, family, peers, and trusted adults (e.g., Brausch and Decker 2014; Duong and Bradshaw 2014; Lee 2011). In addition, the review suggests that there may be parenting practices—such as authoritative or authoritarian parenting, parental control and monitoring, and parent–child communication—that help to increase a child’s perception of care and connection (e.g., Greening et al. 2010; Hay and Meldrum 2010; Kwok and Shek 2008, 2010; Luster and Small 1997). Similarly, the findings suggest that there are elements of family functioning, such as mutuality, communication, and harmony (e.g., Kwok and Shek 2008, 2010), as well as elements of the larger social context, such as a supportive school climate and community connectedness (e.g., Birkett et al. 2009; Hatzenbuehler et al. 2014; Matlin et al. 2011), that may augment a child’s sense of social inclusion. Each of these protective factors may help to decrease the perception of thwarted belongingness and, in turn, the desire for suicide.
There exists a more limited overlap between the current resilience research and the construct of perceived burdensomeness, suggesting a need for more research in this area. On the one hand, several studies identify protective factors that may facilitate a person’s perception of meaning in life, a factor that is inversely associated with perceived burdensomeness (Van Orden et al. 2012) and mediates the impact of perceived burdensomeness on suicidal ideation (Kleiman and Beaver 2013). Protective factors such as engagement in youth programs, sports teams, clubs, and community service (e.g., Armstrong and Manion 2015; Cero and Sifers 2013) may provide an individual with the chance to engage in meaningful activities. Similarly, religious or spiritual beliefs and practices (e.g., Greening and Stoppelbein 2002) may help adherents to feel as though their lives are part of a greater meaning and purpose (Pargament 2002). More research is needed, however, to identify other protective factors that generate meaning in life and thereby reduce feelings of perceived burdensomeness. The viability of this direction is supported by a compensatory main effects literature suggesting that feelings of competence, self-efficacy, self-discovery, and stable self-concept all reduce risk for suicidal ideation and behavior in teens (Breton et al. 2015; Cole 1989; DeWilde et al. 1993; Wichstrom 2009). Thus, future research may wish to examine variables such as: peer leadership or mentorship; academic or athletic achievement; or participation in activities that foster the development of a sense of self, identity, and purpose (e.g., exploring career, college, or other meaningful goals).
Although the IPT model offers a theoretical grounding for many socially oriented protective factors, it is less helpful when it comes to the individual assets and strengths (e.g., problem-solving ability) that are part of an ecological model of resilience. Thus, it may be helpful to draw from a second prominent theory of suicidal ideation and behavior. Williams’ Cry of Pain model suggests that suicidal ideation and behavior is a reactive response (a “cry”) to a situation in which three elements combine to create a feeling of entrapment (inescapable “pain”): (1) stressful life experiences such as rejection or loss; (2) a perception that there will be no rescue; and (3) a perception that there is no escape (CoP; Williams 2001). The initial element of the CoP model proposes that individuals at high risk of suicide experience stressful life events that prompt feelings of defeat, rejection, or loss; this component of the model accords with the many suicide risk factors that have been identified in the literature, from psychiatric disorders to physical or sexual abuse to peer victimization. The model further suggests that an individual then appraises his or her stressful situation in terms of entrapment/defeat. Guiding this appraisal are the two remaining elements of the CoP model: the individual assesses the availability of “rescue factors” such as social support, and evaluates the situation’s “escape potential.” The ability to identify “escape” routes is, in turn, heavily influenced by the individual’s own abilities and skills (e.g., problem-solving, coping skills, cognitive flexibility) (Bolton et al. 2007).
As with the IPT model, the socially oriented protective factors identified in this review align with the CoP model. It is possible that the social support, acceptance, and care provided by parents, families, peers, school, and the community help to reduce a youth’s suicide risk by, at least in part, providing an actual or perceived source of “rescue” from adverse life circumstances. Although this review identified an array of socially oriented protective factors, the literature on compensatory main effects suggests further research directions. First, the literature suggests that parental presence, parental expectations, parent–teen shared activities, and parental satisfaction with grades may be worthy of exploration within a resilience framework (Borowsky et al. 2001; Lewinsohn et al. 1993; Rew et al. 2001). Similarly, variables such as family cohesion, family recreation, and family support satisfaction should be explored as protective factors (DeWilde et al. 1993; McKeown et al. 1998; Walsh and Eggert 2007). Finally, the density and transitivity of friendship networks, school connectedness, school safety, and the presence of counseling services at school are potential research targets (Bearman and Moody 2004; Borowsky et al. 2001; Resnick et al. 1997). Exploring these additional social resource protective factors is supported by the present review as well as by the IPT and CoP models of suicidal ideation and behavior.
Examining Meaningful Risk-resilience Patterns Through an Ecological Lens
What is perhaps most important is that researchers begin to explore resilience to suicidal ideation and behavior in a programmatic way. Much of the research to date has examined pairings of one risk factor and one protective factor, often for research purposes unrelated to a resilience agenda. The present review suggests a need for more deliberate, theoretically driven research that explores resilience to the effects of any given risk factor from a multi-dimensional, multi-domain framework (i.e., individual, parent, family, peer, school, community). For instance, multiple independent studies suggest that resilience to depression-related suicide risk is multi-faceted, with resilience stemming from individual assets such as self-esteem, cognitive style, and religious beliefs, as well as ecological resources such as parental support, authoritarian parenting, family alliance, peer acceptance and support, community connectedness and engagement in meaningful activities (Armstrong and Manion 2015; Brausch and Decker 2014; Greening et al. 2010; Greening and Stoppelbein 2002; Lee 2011; Matlin et al. 2011). Multi-domain patterns of resilience also were found for risk factors such as peer victimization and childhood abuse. However, research has yet to evaluate these patterns in a comprehensive way, and it will be important for future studies to incorporate multiple protective factors in relation to any given source of risk.
The development and use of reliable, valid, multi-domain measures of resilience will help to facilitate this type of multi-dimensional research. Only one study in the current review used a resilience-oriented scale (Nrugham et al. 2010) and the scale in question—the Connor-Davidson Resilience Scale (Connor and Davidson 2003)—provided only a total resilience score. Future research in this area may wish to include a multi-domain resilience scale like the Resilience Scale for Adolescents (READ; Von Soest et al. 2010), which provides five domain-specific scores (Personal Competence, Social Competence, Structured Style, Family Cohesion, and Social Resources), or the Adolescent Resilience Questionnaire (ARQ; Gartland et al. 2011), which provides twelve domain-specific scores across five categories that align closely with an ecological model of resilience: individual, family, peer, school, and community factors. Alternatively, the Suicide Resilience Inventory-25 (SRI-25; Osman et al. 2004) measures a suicide-specific construct of resilience across three domains: Internal Protective Factors, Emotional Stability, and External Protective Factors. The adoption of measures such as the READ, ARQ, or SRI-25 would permit researchers to efficiently test multiple domains of resilience within a single study and would allow for robust, accurate interpretations when making cross-study comparisons.
As the literature moves toward a more multi-dimensional approach, it will be important to acknowledge that any given risk factor is likely to have a unique constellation of protective factors. For instance, this review suggests that individual qualities such as self-control and cognitive style are more effective than self-acceptance in buffering the suicide risk related to peer victimization. Similarly, social resources such as authoritative parenting and the presence of a caring school adult may be more effective than family support, peer support, or social well-being at buffering against peer victimization-related suicide risk (e.g., Duong and Bradshaw 2014; Hay and Meldrum 2010; Herba et al. 2008; Hershberger and D’Augelli 1995; Wolff et al. 2014). Given unique risk-resilience patterns like this, future research should incorporate existing theory on suicide risk factors to develop domain-spanning (e.g., individual, family, peer) hypotheses on which protective factors are most implicated for that specific risk factor.
In addition, as the resilience literature develops, researchers will need to move beyond simple interactional designs. More complex analyses, such as three-way moderation, would enable tests of biological sex or ethnic differences. Such analyses also would permit researchers to explore whether protective factors interact with each other in augmenting or decreasing resilience to suicide. Only one study has so far evaluated this, with Hershberger and D’Augelli (1995) finding null results when exploring a three-way interaction between peer victimization, family support, and self-acceptance. Future research may wish to include multiple risk factors in studies, or consider examining resilience from a framework of cumulative adversity, in which risk for suicide is evaluated in terms of lifetime experiences of adversity rather than any given risk factor. Recent research has suggested that the cumulative effect of lifetime adversity (e.g., childhood abuse, family violence, residential instability, community violence) strongly predicts past-year suicidal ideation in adolescents (Thompson et al. 2012).
Finally, once research converges on the sources of resilience—i.e., what confers resilience to suicidal ideation and behavior—it will be important for investigators to focus on identifying the mechanisms and processes that explain how these factors confer resilience (Luthar et al. 2000). Future studies using mediated moderation models are needed to explore the mechanisms underlying many of the relevant protective factors in the present review (Muller et al. 2005).
Clinical Implications for Suicide Prevention
A greater interface is needed between research into protective factors and the interventions that are used to prevent or manage outcomes such as suicidal ideation and behavior (Luthar et al. 2000). The findings from the current review have clear relevance to the design and implementation of suicide prevention efforts.
A move toward suicide prevention that focuses not just on risk reduction but on the promotion of resilience is aligned with prevention efforts directed at other risky behaviors like substance abuse. Theorists have suggested that, given the complex interaction of risk and resilience, prevention programs must take an approach that promotes the development of strengths and competencies even as it addresses risk (e.g., Jessor 1991; Olsson et al. 2003; Rew and Horner 2003). In keeping with an ecological approach to resilience, it has been suggested that this type of comprehensive prevention strategy address multiple domains of resilience, including the individual, family, peer, school, community, and social context (Jessor 1991; Rew and Horner 2003).
The present review suggests a number of protective factors that could be incorporated into a multi-domain, multi-level suicide prevention program. Skills-building elements focused on the individual could include decision-making and problem-solving, emotion regulation, self-esteem, cognitive appraisals, and engagement in service/volunteer/mastery activities. Peer- and school-related elements could include a focus on peer communication and relationships, conflict resolution, extracurricular involvement, peer mentoring, and coping with academic or interpersonal stress. Other school-based interventions could include the development of specific policies or clubs that increase school safety and connectedness, especially for marginalized groups (e.g., anti-bullying policies, Gay-Straight Alliance). The present review also suggests the importance of engaging parents and family in suicide prevention efforts. Elements could include helping parents and teens improve communication, process family conflict, improve parenting style and presence, develop warm and encouraging relationships, and engage in shared activities. Finally, multi-domain programs should reach outside the school to foster partnerships with community centers and youth programs that can provide students with external social support.
A number of selective and universal suicide prevention programs have been developed that take this type of multi-dimensional, skills-building approach. Eggert and colleagues (2002) evaluated two programs in at-risk high school students: (1) a Counselors Care (C-CARE) program consisting of a 2-h motivational interviewing session, 2 h of counseling on topics such as problem-solving and help-seeking, and an intervention to connect teens with school staff and parents; and (2) a Coping and Support Training (CAST) program consisting of 12 1-h small group sessions focused on skills such as goal-setting and decision-making, self-esteem, family and peer support, and mood management. Studies showed that the C-CARE plus CAST program decreased suicidal ideation and behavior, depressive symptoms, and family distress, and increased self-efficacy, self-esteem, personal control, problem-solving coping, and family support (Eggert et al. 2002; Randell et al. 2001). Further testing of the C-CARE program with an added Parents Care component (P-CARE)—involving two home-based visits with parents to teach empathy, active listening, communication, and suicide risk identification and intervention skills—also was shown to reduce ideation and depression, while increasing coping, self-efficacy, and family support in at-risk high-schoolers (Hooven et al. 2010).
A Developmental Perspective on Resilience to Suicidal Ideation and Behaviors in Youth
To our knowledge, the current article is the first to comprehensively review the existing literature on resilience factors that buffer against suicidal ideation and behaviors in youth. Although a prior review by Johnson and colleagues (2011) had examined research on resilience to suicidal ideation and behaviors it was inclusive of all age groups. The current review takes a developmental approach to this topic by focusing exclusively on studies involving samples of children and adolescents. This focus is necessary given that while suicidal ideation and behavior occur in all age groups, it is developmentally mediated. Suicidal ideation, plans, attempts and completed suicide are extremely rare among prepubescent children, with rates sharply increasing after approximately age 12 (CDC 2013a; Nock et al. 2013). Research is needed to better understand this increase. However, it is possible that hormonal changes related to puberty, rapidly developing emotional areas of the brain and slower developing inhibitory regions of the brain (leading to impulsivity and risk-taking behaviors), and contextual challenges that include transitions to new school settings, an increased emphasis on peer relationships, sexual orientation and identity development, and the introduction of romantic relationships all contribute to the emergence of suicidal ideation and behavior during adolescence. At the same time, youth remain firmly embedded in a family system that can involve its own set of unique challenges related to the parent–child relationship, family dynamics, and renegotiation of boundaries and autonomy. Given the unique developmental context in which children and adolescents are embedded, this review of the resilience literature fills a vital role in focusing on this age group as a unique, and especially at-risk, population.
The model of resilience described in the current review takes this complex picture of adolescent development into account, expanding the conceptualization of resilience beyond that of prior reviews, which largely view resilience as involving internal, psychological constructs such as attributional style or problem-solving ability (Johnson et al. 2011). This review draws on ecological perspectives on child development (e.g., Bronfenbrenner 1977) and resilience (Fergus and Zimmerman 2005; Masten and Coatsworth 1998; Wright et al. 2013) to articulate a model of resilience to suicidal ideation and behaviors that focuses not only on internal psychological or personality traits but also on a youth’s developmental, ecological context: parents and family, friends and school, and neighborhood and culture (Wright et al. 2013). This ecological approach helps to avoid what has been described by some theorists as context minimization error, or the tendency to focus on individual differences as the sole cause of outcomes (Shinn and Toohey 2003). This minimization of developmental context not only results in impoverished theory that ignores transactional influences between child and environment, it also creates a false dichotomy: a child is made either resilient or not resilient based on the possession of a trait-like protective factor. The present review suggests that, given the many developmental contexts in which adolescents are embedded, there are a variety of ways that parents, providers, and the larger community can intervene to enhance a child’s internal resources or provide external support to buffer against suicidal ideation and behavior.
Although the present article moves the literature forward by reviewing the research on resilience to suicidal ideation and behaviors in youth, it should be acknowledged that most of the studies in this review involved simple, cross-sectional interaction analyses that do not fully account for the dynamic and transactional nature of adolescent development. As theorists have noted, what is needed is an ecological framework that permits a “…greater understanding of the adolescent suicide problem as [involving] complex relationships between personal, interpersonal, and sociocultural factors…” (Ayyash-Abdo 2002, p. 470). As individuals progress in age from childhood to adolescence to adulthood, different risk and protective factors may emerge in response to the changing developmental context (Wright et al. 2013). For example, young children may be particularly sensitive to the risks posed by physical abuse by caregivers and to protective variables such as parental warmth and support. As a child reaches school age, risk and protective factors relating to peer victimization and school safety and quality may increase in salience. Finally, as a child enters adolescence, risk and protective factors related to the adolescent’s peer and friendship network, activity engagement, and romantic relationships may become especially important. Given this developmental complexity, it is vital that future research move beyond simple interactional models. More advanced statistical models commonly employed in developmental research, such as growth curve modeling and trajectory analysis, may help researchers to more precisely map the development of resilience to suicidal ideation and behaviors in youth.
Conclusion
This review summarized the current literature on protective factors that confer resilience to suicidal ideation and behavior in youth. In contrast to earlier work in this area, which focused on internal, psychological protective factors in both adult and youth samples (Johnson et al. 2011), this review articulated an ecological model of resilience relevant to youth in which resilience occurs across multiple domains. In addition to integrating evidence suggesting that individual assets such as problem-solving, cognitive style, emotion regulation, and self-esteem buffer against suicidal ideation and behavior, this review also identified an array of protective ecological resources such as parent–child relationships, parenting style, family interactions, peer relationships, school climate, and engagement in meaningful activities. Future research is needed to explore protective factors in a more programmatic way, through the use of well-designed, longitudinal studies that assess multiple risk and protective factors across development, explore biological sex- and culture-based differences in how resilience manifests, and integrates existing theory on suicidal ideation and behavior. Finally, as resilience research moves forward, a greater interface between research and prevention will be needed to ensure that suicide prevention programs focus on developing individual strengths and social resources even as they function to reduce suicide risk factors.
References
Allen, J., Mohatt, G. V., Fok, C. C., Henry, D., Burkett, R., & Team, P. A. (2014). A protective factors model for alcohol abuse and suicide prevention among Alaska Native Youth. American Journal of Community Psychology, 54, 125–139.
Anestis, M. D., & Joiner, T. E. (2011). Examining the role of emotion in suicidality: Negative urgency as an amplifier of the relationship between components of the interpersonal–psychological theory of suicidal behavior and lifetime number of suicide attempts. Journal of Affective Disorders, 129, 261–269.
Armstrong, L. L. (2012). Initial development and validation of the checklist of risk behaviours for youth (CORBY). Psychology, Health & Medicine, 17(1), 116–124. 10.1080/13548506.2011.592842.
Armstrong, L. L., & Manion, I. G. (2015). Meaningful youth engagement as a protective factor for youth suicidal ideation. Journal of Research on Adolescence, 25, 20–27.
Ayón, C., & Aisenberg, E. (2010). Negotiating cultural values and expectations within the public child welfare system: A look at familismo and personalismo. Child & Family Social Work, 15, 335–344.
Ayyash-Abdo, H. (2002). Adolescent suicide: An ecological approach. Psychology in the Schools, 39, 459–475.
Barnes, H. L., & Olson, D. H. (1985). Parent-adolescent communication and the circumplex model. Child Development, 438–447.
Batson, C. D., Schoenrade, P., & Ventis, W. L. (1993). Religion and the individual: A social-psychological perspective. Oxford University Press.
Bearman, P. S., & Moody, J. (2004). Suicide and friendships among American adolescents. American Journal of Public Health, 94, 89–95.
Beck, A. T., Steer, R. A., Brown, G. K. et al. (1996). Manual for the beck depression inventory-II. San Antonio, TX: Psychological Corporation, 1, 82.
Bernstein, D. P., Ahluvalia, T., Pogge, D., & Handelsman, L. (1997). Validity of the childhood trauma questionnaire in an adolescent psychiatric population. Journal of the American Academy of Child & Adolescent Psychiatry, 36(3), 340–348.
Birkett, M., Espelage, D. L., & Koenig, B. (2009). LGB and questioning students in schools: The moderating effects of homophobic bullying and school climate on negative outcomes. Journal of Youth and Adolescence, 38, 989–1000.
Bolton, C., Gooding, P., Kapur, N., Barrowclough, C., & Tarrier, N. (2007). Developing psychological perspectives of suicidal behaviour and risk in people with a diagnosis of schizophrenia: We know they kill themselves but do we understand why? Clinical Psychology Review, 27, 511–536.
Borowsky, I. W., Ireland, M., & Resnick, M. D. (2001). Adolescent suicide attempts: Risks and protectors. Pediatrics, 107, 485–493.
Brausch, A. M., & Decker, K. (2014). Self-esteem and social support as moderators of depression, body image, and disordered eating for suicidal ideation in adolescents. Journal of Abnormal Child Psychology, 42, 779–789.
Breton, J. J., Labelle, R., Berthiaume, C., Royal, C., St. Georges, M., et al. (2015). Protective factors against depression and suicidal behaviour in adolescence. Canadian Journal of Psychiatry, 60, S5–S15.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32, 513–531. doi:10.1037/0003-066X.32.7.513.
Buss, A. H., & Plomin, R. (2014). Temperament (PLE: Emotion): Early developing personality traits (Vol. 3). London: Psychology Press.
Butler, A. M., & Malone, K. (2013). Attempted suicide v. non-suicidal self-injury: Behaviour, syndrome or diagnosis? The British Journal of Psychiatry, 202, 324–325.
Cash, S. J., & Bridge, J. A. (2009). Epidemiology of youth suicide and suicidal behavior. Current Opinion in Pediatrics, 21, 613–619.
Centers for Disease Control and Prevention (CDC). (2013a). National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS). http://www.cdc.gov/injury/wisqars/index.html. Accessed 11 Nov 2016.
Centers for Disease Control and Prevention (CDC). (2013b). Youth risk behavior surveillance—United States, 2013. MMWR, Surveillance Summaries, 63. http://www.cdc.gov/mmwr/pdf/ss/ss6304.pdf. Accessed 11 Nov 2016.
Cero, I., & Sifers, S. (2013). Moderating factors in the path from physical abuse to attempted suicide in adolescents: Application of the Interpersonal-Psychological Theory of suicide. Suicide and Life-Threatening Behavior, 43, 296–304.
Cha, C. B., & Nock, M. K. (2009). Emotional intelligence is a protective factor for suicidal behavior. Journal of the American Academy of Child & Adolescent Psychiatry, 48, 442–430.
Chan, D. W. (2003). Dimensions of emotional intelligence and their relationships with social coping among gifted adolescents in Hong Kong. Journal of Youth and Adolescence, 32(6), 409–418.
Chan, K. L. (2011). Children exposed to child maltreatment and intimate partner violence: A study of co-occurrence among Hong Kong Chinese families. Child Abuse & Neglect, 35(7), 532–542.
Chang, E. C. (2002). Predictingcia suicide ideation in an adolescent population: Examining the role of social problem solving as a moderator and a mediator. Personality and Individual Differences, 32, 1279–1291.
Chang, H. J., Lin, M. F., & Lin, K. C. (2007). The mediating and moderating roles of the cognitive triad on adolescent suicidal ideation. Nursing Research, 56, 252–259.
Chau, T. T., Hsiao, T. M., Huang, C. T., & Liu, H. W. (1991). A preliminary study of family Apgar index in the Chinese. Gaoxiong Yi Xue Ke Xue Za Zhi = The Kaohsiung Journal of Medical Sciences, 7(1), 27–31.
Ciarrochi, J., Dean, F. P., & Anderson, S. (2002). Emotional intelligence moderates the relationship between stress and mental health. Personality and Individual Differences, 32, 197–209.
Cole, D. A. (1989). Psychopathology of adolescent suicide: Hopelessness, coping beliefs, and depression. Journal of Abnormal Psychology, 98, 248–255.
Connor, K. M., & Davidson, J. R. T. (2003). Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18, 76–82.
Cui, S., Cheng, Y., Xu, Z., Chen, D., & Wang, Y. (2010). Peer relationships and suicide ideation and attempts among Chinese adolescents. Child: Care, Health and Development, 37, 692–702.
Curtin, S. C., Warner, M., & Hedegaard, H. (2016). Increase in suicide in the United States, 1999–2014. NCHS Data Brief, 241. http://www.cdc.gov/nchs/products/databriefs/db241.htm. Accessed 11 Nov 2016.
Cwik, M., Barlow, A., Tingey, L., Goklish, N., Larzelere-Hinton, F., Craig, M., & Walkup, J. T. (2015). Exploring risk and protective factors with a community sample of American Indian adolescents who attempted suicide. Archives of Suicide Research, 19, 172–189.
D’Zurilla, T. J., Nezu, A. M., & Maydeu-Olivares, A. (2002). Social Problem-solving Inventory–revised (SPSI-R). Tonawanda, NY: Multi-Health Systems.
Deeley, S. T., & Love, A. W. (2013). Longitudinal analysis of the emotion self-confidence model of suicidal ideation in adolescents. Advances in Mental Health, 12, 34–45.
DeWilde, E. J., Kienhorst, I. C., Diekstra, R. F., & Wolters, W. H. (1993). The specificity of psychological characteristics of adolescent suicide attempters. Journal of the American Academy of Child and Adolescent Psychiatry, 32, 51–59.
Dodge, K. A., & Coie, J. D. (1987). Social-information-processing factors in reactive and proactive aggression in children’s peer groups. Journal of Personality and Social Psychology, 53(6), 1146.
Dubow, E. F., & Ullman, D. G. (1989). Assessing social support in elementary school children: The survey of children’s social support. Journal of Clinical Child Psychology, 18(1), 52–64.
Duong, J., & Bradshaw, C. (2014). Associations between bullying and engaging in aggressive and suicidal behaviors among sexual minority youth: The moderating role of connectedness. Journal of School Health, 84, 636–645.
Eggert, L. L., Thompson, E. A., Randell, B. P., & Pike, K. C. (2002). Preliminary effects of brief school-based prevention approaches for reducing youth suicide-risk behaviors, depression, and drug involvement. Journal of Child and Adolescent Psychiatric Nursing, 15, 48–64.
Else-Quest, N. M., Hyde, J. S., Goldsmith, H. H., & Van Hulle, C. A. (2006). Gender differences in temperament: A meta-analysis. Psychological Bulletin, 132, 33–72.
Espelage, D. L., Aragon, S. R., Birkett, M., & Koenig, B. W. (2008). Homophobic teasing, psychological outcomes, and sexual orientation. School Psychology Review, 37, 202–216.
Esposito, C. L., & Clum, G. A. (2002). Social support and problem-solving as moderators of the relationship between childhood abuse and suicidality: Applications to a delinquent population. Journal of Traumatic Stress, 15, 137–146.
Esposito, C. L., & Clum, G. A. (2003). The relative contribution of diagnostic and psychosocial factors in the prediction of adolescent suicidal ideation. Journal of Clinical Child and Adolescent Psychology, 32, 386–395.
Esposito-Smythers, C., Weismoore, J., Zimmerman, R. P., & Spirito, A. (2014). Suicidal behaviors among children and adolescents. In M. K. Nock (Ed.), The Oxford handbook of suicide and self-injury (pp. 61–81). New York, NY: Oxford University Press.
Evans, E., Hawton, K., & Rodham, K. (2004). Factors associated with suicidal phenomena in adolescents: A systematic review of population-based studies. Clinical Psychology Review, 24, 957–979.
Fergus, S., & Zimmerman, M. A. (2005). Adolescent resilience: A framework for understanding healthy development in the face of risk. Annual Review of Public Health, 26, 399–419.
Frazier, P. A., Tix, A. P., & Barron, K. E. (2004). Testing moderator and mediator effects in counseling psychology research. Journal of Counseling Psychology, 51, 115–134.
Garner, D. M., & Garfinkel, P. E. (1979). The eating attitudes test: An index of the symptoms of anorexia nervosa. Psychological Medicine, 9(2), 273–279.
Garroutte, E. M., Goldberg, J., Beals, J., Herrell, R., & Manson, S. M. & AI–SUPERPFP Team. (2003). Spirituality and attempted suicide among American Indians.. Social Science & Medicine, 56, 1571–1579.
Gartland, D., Bond, L., Olsson, C. A., Buzwell, S., & Sawyer, S. M. (2011). Development of a multi-dimensional measure of resilience in adolescents: the Adolescent Resilience Questionnaire. BMC Medical Research Methodology, 11, 134.
Gentile, B., Grabe, S., Dolan-Pascoe, B. D., Twenge, J. M., Wells, B. E., & Maitino, A. (2009). Gender differences in domain-specific self-esteem: A meta-analysis. Review of General Psychology, 13, 34–45.
Goldston, D. B., Daniel, S. S., Erkanli, A., Reboussin, B. A., Mayfield, A., Frazier, P. H., & Treadway, S. L. (2009). Psychiatric diagnoses as contemporaneous risk factors for suicide. Journal of Consulting and Clinical Psychology, 77, 281–290.
Goodwin, R. D., & Marušič, A. (2003). Feelings of inferiority and suicide ideation and suicide attempt among youth. Croatian Medical Journal, 44, 553–557.
Gould, M. S., Greenberg, T., Velting, D. M., & Shaffer, D. S. (2003). Youth suicide risk and preventive interventions: A review of the past 10 years. Journal of the American Academy of Child & Adolescent Psychiatry, 42, 386–405.
Gould, M. S., King, R., Greenwald, S., Fisher, P., Schwab-Stone, M., et al. (1998). Psychopathology associated with suicidal ideation and attempts among children and adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 37, 915–923.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54.
Greening, L., & Dollinger, S. J. (1993). Rural adolescents’ perceived personal risks for suicide. Journal of Youth and Adolescence, 22(2), 211–217.
Greening, L., & Stoppelbein, L. (2002). Religiosity, attributional style, and social support as psychosocial buffers for African American and White adolescents’ perceived risk for suicide. Suicide and Life-Threatening Behavior, 32, 404–417.
Greening, L., Stoppelbein, L., & Luebbe, A. (2010). The moderating effects of parenting styles on African-American and Caucasian children’s suicidal behaviors. Journal of Youth and Adolescence, 39, 357–369.
Grover, K. E., Green, K. L., Pettit, J. W., Monteith, L. L., Garza, M. J., & Venta, A. (2009). Problem solving moderates the effects of life event stress and chronic stress on suicidal behaviors in adolescence. Journal of Clinical Psychology, 65, 1281–1290.
Guilamo-Ramos, V., Dittus, P., Jaccard, J., Johansson, M., Bouris, A., & Acosta, N. (2007). Parenting practices among Dominican and Puerto Rican mothers. Social Work, 52, 17–30.
Hammen, C., Brennan, P. A., & Shih, J. H. (2004). Family discord and stress predictors of depression and other disorders in adolescent children of depressed and nondepressed women. Journal of the American Academy of Child & Adolescent Psychiatry, 43(8), 994–1002.
Hankin, B. L., & Abramson, L. Y. (2001). Development of gender differences in depression: An elaborated cognitive vulnerability-transactional stress theory. Psychological Bulletin, 127, 773–796.
Harrell, A. V., & Wirtz, P. W. (1989). Screening for adolescent problem drinking: Validation of a multidimensional instrument for case identification. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 1(1), 61.
Hatzenbuehler, M. L. (2011). The social environment and suicide attempts in lesbian, gay, and bisexual youth. Pediatrics, 127, 896–903.
Hatzenbuehler, M. L., Birkett, M., Van Wagenen, A., & Meyer, I. H. (2014). Protective school climates and reduced risk for suicide ideation in sexual minority youths. American Journal of Public Health, 104, 279–286.
Hay, C., & Meldrum, R. (2010). Bullying victimization and adolescent self-harm: Testing hypotheses from General Strain Theory. Journal of Youth and Adolescence, 39, 446–459.
Henry, C. S., Stephenson, A. L., Hanson, M. F., & Hargett, W. (1993). Adolescent suicide and families: An ecological approach. Adolescence, 28, 291–308.
Heppner, P. (1988). The problem solving inventory. Palo Alto, CA: Consulting Psychologists Press.
Herba, C. M., Ferdinand, R. F., Stijnen, T., Veenstra, R., Oldehinkel, A. J., Ormel, J., & Verhulst, F. C. (2008). Victimisation and suicide ideation in the TRAILS study: Specific vulnerabilities of victims. Journal of Child Psychology and Psychiatry, 49, 867–876.
Heron, M. (2016). Deaths: Leading causes for 2013. National Vital Statistics Reports, 65(2). https://www.cdc.gov/nchs/data/databriefs/db241.pdf. Accessed 11 Nov 2016.
Hershberger, S. L., & D’Augelli, A. R. (1995). The impact of victimization on the mental health and suicidality of lesbian, gay, and bisexual youths. Developmental Psychology, 31, 65–74.
Hoeppner, B. B., Kelly, J. F., Urbanoski, K. A., & Slaymaker, V. (2011). Comparative utility of a single-item vs. multiple-item measure of self-efficacy in predicting relapse among young adults. Journal of Substance Abuse Treatment, 41, 305–312.
Hooven, C., Herting, J. R., & Snedker, K. A. (2010). Long-term outcomes for the Promoting CARE suicide prevention program. American Journal of Health Behavior, 34, 721–736.
Horowitz, L. M., Wang, P. S., Koocher, G. P., Burr, B. H., Smith, M. F., Klavon, S., & Cleary, P. D. (2001). Detecting suicide risk in a pediatric emergency department: Development of a brief screening tool. Pediatrics, 107(5), 1133–1137.
Jessor, R. (1991). Risk behavior in adolescence: A psychosocial framework for understanding and action. Journal of Adolescent Health, 12, 597–605.
Johnson, J., Wood, A. M., Gooding, P., Taylor, P. J., & Tarrier, N. (2011). Resilience to suicidality: The buffering hypothesis. Clinical Psychology Review, 31, 563–591.
Joiner, T. E. (2005). Why people die by suicide. Cambridge, MA: Harvard University Press.
Kann, L., Kinchen, S., Shanklin, S. L., Flint, K. H., Hawkins, J., et al. (2014). Youth Risk Behavior Surveillance – United States, 2013. Morbidity and Mortality Weekly Report, 63(SS04), 1–68. https://www.cdc.gov/mmwr/preview/mmwrhtml/ss6304a1.htm. Accessed 11 Nov 2016.
Kaslow, N. J., Stark, K. D., Printz, B., Livingston, R., & Ling Tsai, S. (1992). Cognitive triad inventory for children: Development and relation to depression and anxiety. Journal of Clinical Child Psychology, 21(4), 339–347.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., et al. (1997). Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. Journal of the American Academy of Child & Adolescent Psychiatry, 36(7), 980–988.
King, C. A., & Merchant, C. R. (2008). Social and interpersonal factors relating to adolescent suicidality: A review of the literature. Archives of Suicide Research, 12, 181–196.
Kleiman, E. M., & Beaver, J. K. (2013). A meaningful life is worth living: Meaning in life as a suicide resiliency factor. Psychiatry Research, 210, 934–939.
Knight, J. R., Sherritt, L., Harris, S. K., Gates, E. C., & Chang, G. (2003). Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcoholism: Clinical and Experimental Research, 27(1), 67–73.
Kohn, P. M., & Milrose, J. A. (1993). The inventory of high-school students’ recent life experiences: A decontaminated measure of adolescents’ hassles. Journal of Youth and Adolescence, 22(1), 43–55. doi:10.1007/BF01537903.
Kovacs, M. (1992). Children’s depression inventory: manual. Cheektowaga, NY: Multi-Health Systems.
Kovacs, M. (2000). The “Feelings and Me” emotion regulatory strategy utilization questionnaires. Pittsburgh, PA: University of Pittsburgh School of Medicine.
Kral, M. J., Wiebe, P. K., Nisbet, K., Dallas, C., Okalik, L., Enuaraq, N., & Cinotta, J. (2009). Canadian Inuit community engagement in suicide prevention. International Journal of Circumpolar Health, 68, 292–308.
Kring, A. M., & Gordon, A. H. (1998). Sex differences in emotion: Expression, experience, and physiology. Journal of Personality and Social Psychology, 74, 686–703.
Kwok, S. Y., Chai, W., & He, X. (2013). Child abuse and suicidal ideation among adolescents in China. Child Abuse & Neglect, 37, 986–996.
Kwok, S. Y., & Shek, D. T. (2008). Hopelessness, family functioning and suicidal ideation among Chinese adolescents in Hong Kong. Open Family Studies Journal, 1, 49–55.
Kwok, S. Y., & Shek, D. T. (2009). Social problem solving, family functioning, and suicidal ideation among Chinese adolescents in Hong Kong. Adolescence, 44, 391–406.
Kwok, S. Y., & Shek, D. T. (2010). Hopelessness, parent-adolescent communication, and suicidal ideation among Chinese adolescents in Hong Kong. Suicide and Life-Threatening Behavior, 40, 224–233.
Kwok, S. Y., Yeung, J. W., Low, A. Y., Lo, H. H., & Tam, C. H. (2015). The roles of emotional competence and social problem-solving in the relationship between physical abuse and adolescent suicidal ideation in China. Child Abuse & Neglect, 44, 117–129.
LaFromboise, T. D., Medoff, L., Harris, A., & Lee, C. (2007). Psychosocial and cultural correlates of suicidal ideation among American Indian early adolescents on a Northern Plains reservation. Research in Human Behavior, 41, 119–143.
Lau, A. S., Jernewall, N. M., Zane, N., & Myers, H. F. (2002). Correlates of suicidal behaviors among Asian-American outpatient youths. Cultural Diversity and Ethnic Minority Psychology, 8, 199–213.
Lee, S. Y. (2011). Reasons for living and their moderating effects on Korean adolescents’ suicidal ideation. Death Studies, 35, 711–728.
Leitenberg, H., Yost, L. W., & Carroll-Wilson, M. (1986). Negative cognitive errors in children: Questionnaire development, normative data, and comparisons between children with and without self-reported symptoms of depression, low self-esteem, and evaluation anxiety. Journal of Consulting and Clinical Psychology, 54(4), 528–536. doi:10.1037/0022-006X.54.4.528.
Lewinsohn, P. M., Rohde, P., & Seeley, J. R. (1993). Psychosocial characteristics of adolescents with a history of a suicide attempt. Journal of the American Academy of Child and Adolescent Psychiatry, 32, 60–68.
Li, D., Zhang, W., Li, X., Li, N., & Ye, B. (2012). Gratitude and suicidal ideation and suicide attempts among Chinese adolescents: Direct, mediated, and moderated effects. Journal of Adolescence, 35, 55–56.
Luster, T., & Small, S. A. (1997). Sexual abuse history and problems in adolescence: Exploring the effects of moderating variables. Journal of Marriage and the Family, 59, 131–142.
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71, 543–562.
Malecki, C. K., & Demaray, M. K. (2002). Measuring perceived social support: Development of the child and adolescent social support scale (CASSS). Psychology in the Schools, 39(1), 1–18.
Markus, H. R., & Kitayama, S. (1991). Culture and the self: Implications for cognition, emotion, and motivation. Psychological Review, 98, 224–253.
Masten, A. S., & Coatsworth, J. D. (1998). The development of competence in favorable and unfavorable environments: Lessons from research on successful children. American Psychologist, 53, 205–220.
Matlin, S. L., Molock, S. D., & Tebes, J. K. (2011). Suicidality and depression among African American adolescents: The role of family and peer support and community connectedness. American Journal of Orthopsychiatry, 81, 108–117.
Markus, M. T., Lindhout, I. E., Boer, F., Hoogendijk, T. H., & Arrindell, W. A. (2003). Factors of perceived parental rearing styles: The EMBU-C examined in a sample of Dutch primary school children. Personality and Individual Differences, 34(3), 503–519.
Mayer, J. D., & Salovey, P. (2007). Mayer-Salovery-Caruso emotional intelligence test. Cheektowaga, NY: Multi-Health Systems Incorporated.
McKeown, R. E., Garrison, C. Z., Cuffe, S. P., Waller, J. L., Jackson, K. L., & Addy, C. L. (1998). Incidence and predictors of suicidal behavior in a longitudinal sample of young adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 37, 612–619.
Miller, A. B., & Esposito-Smythers, C. (2013). How do cognitive distortions and substance-related problems affect the relationship between child maltreatment and adolescent suicidal ideation? Psychology of Violence, 3, 340–353.
Miller, F. G., Lazowski, L. E. (2001). The adolescent SASSI-A2 manual: Identifying substance use disorders. Springville, IN: The SASSI Institute.
Miller, I. W., Norman, W. H., Bishop, S. B., & Dow, M. G. (1986). The Modified Scale for Suicidal Ideation: Reliability and validity. Journal of Consulting and Clinical Psychology, 54, 724–725.
Miranda, R., Gallagher, M., Bauchner, B., Vaysman, R., & Marroquin, B. (2012). Cognitive inflexibility as a prospective predictor of suicidal ideation among young adults with a suicide attempt history. Depression and Anxiety, 29, 180–186.
Muller, D., Judd, C. M., & Yzerbyt, V. Y. (2005). When moderation is mediated and mediation is moderated. Journal of Personality and Social Psychology, 89, 852–863.
Nieboer, A., Lindenberg, S., Boomsma, A., & Bruggen, A. C. V. (2005). Dimensions of well-being and their measurement: The SPF-IL scale. Social Indicators Research, 73(3), 313–353.
Nock, M. K., Green, J. G., Hwang, I., McLaughlin, K. A., Sampson, N. A., Zaslavsky, A. M., & Kessler, R. C. (2013). Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry, 70(3), 300–310.
Nock, M. K., Holmberg, E. B., Photos, V. I., & Michel, B. D. (2007). Self-injurious thoughts and behaviors interview: Development, reliability, and validity in an adolescent sample. Psychological Assessment, 19(3), 309–317. doi:10.1037/1040-3590.19.3.309.
Nrugham, L., Holen, A., & Sund, A. M. (2010). Associations between attempted suicide, violent life events, depressive symptoms, and resilience in adolescents and young adults. Journal of Nervous and Mental Disease, 198, 131–136.
O’Donnell, L., O’Donnell, C., Wardlaw, D. W., & Stueve, A. (2004). Risk and resiliency factors influencing suicidality among urban African American and Latino youth. American Journal of Community Psychology, 33, 37–49.
Olsson, C. A., Bond, L., Burns, J. M., Vella-Brodrick, D. A., & Sawyer, S. M. (2003). Adolescent resilience: A concept analysis. Journal of Adolescence, 26, 1–11.
Ormel, J., Oldehinkel, A. J., Ferdinand, R. F., Hartman, C. A., De Winter, A. F., et al. (2005). Internalizing and externalizing problems in adolescence: General and dimension-specific effects of familial loadings and preadolescent temperament traits. Psychological Medicine, 35(12), 1825–1835.
Osman, A., Downs, W. R., Kopper, B. A., Barrios, F. X., Baker, M. T., et al. (1998). The reasons for living inventory for adolescents (RFL-A): Development and psychometric properties. Journal of Clinical Psychology, 54(8), 1063–1078.
Osman, A., Gutierrez, P. M., Muehlenkamp, J. J., Dix-Richardson, F., Barrios, F. X., & Kopper, B. A. (2004). Suicide Resilience Inventory–25: Development and preliminary psychometric properties. Psychological Reports, 94, 1349–1360.
Pace, U., & Zappulla, C. (2010). Relations between suicidal ideation, depression, and emotional autonomy from parents in adolescence. Journal of Child and Family Studies, 19, 747–756.
Pargament, K. I. (2002). The bitter and the sweet: An evaluation of the costs and benefits of religiousness. Psychological Inquiry, 13, 168–181.
Pisani, A. R., Wyman, P. A., Petrova, M., Schmeelk-Cone, K., Goldston, D. B., Xia, Y., & Gould, M. S. (2013). Emotion regulation difficulties, youth-adult relationships, and suicide attempts among high school students in underserved communities. Journal of Youth and Adolescence, 42, 807–820.
Posner, K., Brodsky, B., Yershova, K., Buchanan, J., & Mann, J. (2014). The classification of suicidal behavior. In M. K. Nock (Ed.), The Oxford handbook of suicide and self-injury (pp. 7–22). New York, NY: Oxford University Press.
Radloff, L. S. (1977). The CES-D scale. Applied Psychological Measurement, 1(3), 385–401.
Randell, B. P., Eggert, L. L., & Pike, K. C. (2001). Immediate post intervention effects of two brief youth suicide prevention interventions. Suicide & Life-Threatening Behavior, 31, 41–61.
Reisner, S. L., Biello, K., Perry, N. S., Gamarel, K. E., & Mimiaga, M. J. (2014). A compensatory model of risk and resilience applied to adolescent sexual orientation disparities in nonsuicidal self-injury and suicide attempts. American Journal of Orthopsychiatry, 84, 545–556.
Reitman, D., Rhode, P. C., Hupp, S. D., & Altobello, C. (2002). Development and validation of the parental authority questionnaire–revised. Journal of Psychopathology and Behavioral Assessment, 24(2), 119–127.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., et al. (1997). Protecting adolescents from harm: Results from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association, 278, 823–832.
Rew, L., & Horner, S. D. (2003). Youth resilience framework for reducing health-risk behaviors in adolescents. Journal of Pediatric Nursing, 18, 379–388.
Rew, L., Thomas, N., Horner, S. D., Resnick, M. D., & Beuhring, T. (2001). Correlates of recent suicide attempts in a triethnic group of adolescents. Journal of Nursing Scholarship, 33, 361–367.
Reynolds, W. M. (1987). Suicidal Ideation Questionnaire. Odessa: Psychological Assessment Resources.
Reynolds, W. M. (1988). SIQ, Suicidal ideation questionnaire: Professional manual. Psychological Assessment Resources.
Reynolds, W. M. (2002). Reynolds Adolescent Depression Scale–Second Edition: Professional manual. Odessa, FL: Psychological Assessment Resources.
Rigby, K., & Slee, P. (1999). Suicidal ideation among adolescent school children, involvement in bully-victim problems, and perceived social support. Suicide and Life-Threatening Behavior, 29, 119–130.
Rigby, K., & Slee, P. T. (1993). Dimensions of interpersonal relation among Australian children and implications for psychological well-being. The Journal of Social Psychology, 133(1), 33–42.
Ronan, K. R., Kendall, P. C., & Rowe, M. (1994). Negative affectivity in children: Development and validation of a self-statement questionnaire. Cognitive Therapy and Research, 18(6), 509–528.
Rose, A. J., & Rudolph, K. D. (2006). A review of sex differences in peer relationship processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin, 132, 98–131.
Rosen, R. (1981). Perception of support inventory. Washington, DC: Children’s National Medical Center, (unpublished manuscript).
Rosenberg, M. (1965). Rosenberg self-esteem scale (RSE). Acceptance and Commitment Therapy. Measures Package, 61, 52.
Russell, D. W. (1996). UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. Journal of Personality Assessment, 66(1), 20–40.
Salzinger, S., Rosario, M., Feldman, R. S., & Ng-Mak, D. S. (2007). Adolescent suicidal behavior: Associations with preadolescent physical abuse and selected risk and protective factors. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 859–866.
Sampson, R. J., Raudenbush, S. W., & Earls, F. (1997). Neighborhoods and violent crime: A multilevel study of collective efficacy. Science, 277(5328), 918–924.
Sarason, I. G., Sarason, B. R., Shearin, E. N., & Pierce, G. R. (1987). A brief measure of social support: Practical and theoretical implications. Journal of Social and Personal Relationships, 4(4), 497–510.
Schneidman, E. (1981). A psychological theory of suicide. Suicide and Life-Threatening Behavior, 11, 221–231.
Shek, D. T. (1993). Measurement of pessimism in Chinese adolescents: the Chinese Hopelessness Scale. Social Behavior and Personality: an International Journal, 21(2), 107–119.
Shek, D. T., & Ma, C. M. (2010). The Chinese family assessment instrument (C-FAI) hierarchical confirmatory factor analyses and factorial invariance. Research on Social Work Practice, 20(1), 112–123.
Sherman, R. M., D’Orio, B., Rhodes, M. N., Johnson, S. G., & Kaslow, N. J. (2014). Racial/ethnic, spiritual/religious, and sexual orientation influences on suicidal behaviors. In M. K. Nock (Ed.), The Oxford handbook of suicide and self-injury (pp. 265–285). New York, NY: Oxford University Press.
Shinn, M., & Toohey, S. M. (2003). Community contexts of human welfare. Annual Review of Psychology, 54(1), 427–459.
Silverman, M. M., Berman, A. L., Sanddal, N. D., O’Carroll, P. W., & Joiner, T. E. (2007). Rebuilding the Tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors part 2: Suicide-related ideations, communications, and behaviors. Suicide and Life-Threatening Behavior, 37, 264–277.
Siu, A. M., & Shek, D. T. (2005). The Chinese version of the social problem-solving inventory: Some initial results on reliability and validity. Journal of Clinical Psychology, 61(3), 347–360.
Slap, G., Goodman, E., & Huang, B. (2001). Adoption as a risk factor for attempted suicide during adolescence. Pediatrics, 108, 859–866.
Steinberg, L., & Silverberg, S. B. (1986). The vicissitudes of autonomy in early adolescence. Child Development, 841–851.
Tamás, Z., Kovacs, M., Gentzler, A. L., Tepper, P., Gádoros, J., et al. (2007). The relations of temperament and emotion self-regulation with suicidal behaviors in a clinical sample of depressed children in Hungary. Journal of Abnormal Child Psychology, 35, 640–652.
Tamis-LeMonda, C. S., Briggs, R. D., McClowry, S. G., & Snow, D. L. (2008). Challenges to the study of African American parenting: Conceptualization, sampling, research approaches, measurement, and design. Parenting: Science and Practice, 8, 319–358.
Thompson, R., Litrownik, A. J., Isbell, P., Everson, M. D., English, D. J., et al. (2012). Adverse experiences and suicidal ideation in adolescence: Exploring the link using the LONGSCAN samples. Psychology of Violence, 2, 211–225.
Tse, J. W., Bagley, C., & Muk-Leung Yau, A. (2002). The suicidal risk scale for Hong Kong students. https://eprints.soton.ac.uk/33581/. Accessed 13 Mar 2017.
Van Orden, K. A., Bamonti, P. M., King, D. A., & Duberstein, P. R. (2012). Does perceived burdensomeness erode meaning in life among older adults? Aging & Mental Health, 16, 855–860.
Vernberg, E. M., Jacobs, A. K., & Hershberger, S. L. (1999). Peer victimization and attitudes about violence during early adolescence. Journal of Clinical Child Psychology, 28(3), 386–395.
Von Soest, T., Mossige, S., Stefansen, K., & Hjemdal, O. (2010). A validation study of the Resilience Scale for Adolescents (READ). Journal of Psychopathology and Behavioral Assessment, 32, 215–225.
Walsh, C., Jamieson, E., MacMillan, H., & Trocmé, N. (2004). Measuring child sexual abuse in children and youth. Journal of Child Sexual Abuse, 13, 39–67.
Walsh, E., & Eggert, L. L. (2007). Suicide risk and protective factors among youth experiencing school difficulties. International Journal of Mental Health Nursing, 16, 349–359.
Wang, R. H., Lai, H. J., Hsu, H. Y., & Hsu, M. T. (2011). Risk and protective factors for suicidal ideation among Taiwanese adolescents. Nursing Research, 60, 413–421.
Wedig, M. M., & Nock, M. K. (2007). Parental expressed emotion and adolescent self-injury. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 1171–1178.
Wichstrom, L. (2009). Predictors of non-suicidal self-injury versus attempted suicide: Similar or different? Archives of Suicide Research, 13, 105–122.
Williams, J. M. G. (2001). The Cry of Pain. London: Penguin.
Wolff, J., Esposito-Smythers, C., Becker, S., Seaboyer, L., Rizzo, C., Lichtenstein, D., & Spirito, A. (2014). Social-cognitive moderators of the relationship between peer victimization and suicidal ideation among psychiatrically hospitalized adolescents. Journal of Aggression, Maltreatment & Trauma, 23, 268–285.
World Health Organization (WHO). (1993). Composite international diagnostic interview (CIDI), version 1.1. Composite International Diagnostic Interview (CIDI), Version 1.1.
Wright, M. O., Masten, A. S., & Narayen, A. J. (2013). Resilience processes in development: Four waves of research on positive adaptation in the context of adversity. In Handbook of resilience in children (pp. 15–37). New York, NY: Springer Science + Business Media.
Yang, B., & Clum, G. A. (2000). Childhood Stress Leads to Later Suicidality via Its Effect on Cognitive Functioning. Suicide and Life-Threatening Behavior, 30(3), 183–198. doi:10.1111/j.1943-278X.2000.tb00985.x.
Yen, C. F., Lai, C. Y., Ko, C. H., Liu, T. L., Tang, T. C., Wu, Y. Y., & Yang, P. (2014). The associations between suicidal ideation and attempt and anxiety symptoms and the demographic, psychological, and social moderators in Taiwanese adolescents. Archives of Suicide Research, 18, 104–116.
Yen, C.-F., Kim, Y.-S., Tang, T.-C., Wu, Y.-Y., & Cheng, C.-P. (2012). Factor structure, reliability, and validity of the Chinese version of the School Bullying Experience Questionnaire. The Kaohsiung Journal of Medical Sciences, 28(9), 500–505. 10.1016/j.kjms.2012.04.008.
Zimmerman, M. A., Stoddard, S. A., Eisman, A. B., Caldwell, C. H., Aiyer, S. M., & Miller, A. (2013). Adolescent resilience: Promotive factors that inform resilience. Child Developmental Perspectives, 7, 1–9.
Zimmerman, P., & Iwansi, A. (2014). Emotion regulation from early adolescence to emerging adulthood and middle adulthood: Age differences, gender differences, and emotion-specific developmental variations. International Journal of Behavioral Development, 38, 182–194.
Acknowledgements
Mitchell J. Prinstein, Deborah J. Jones, and Eric A. Youngstrom (University of North Carolina at Chapel Hill) for consultation regarding the design and implementation of the review, and for the provision of comments on the initial manuscript. Support was provided by National Institutes of Mental Health (NIH) Grant F32MH108238 awarded to Adam Bryant Miller.
Author information
Authors and Affiliations
Contributions
MG conceived of the review, participated in its design and coordination, and drafted the initial manuscript. ABM contributed to data interpretation and to the writing and editing of the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Gallagher, M.L., Miller, A.B. Suicidal Thoughts and Behavior in Children and Adolescents: An Ecological Model of Resilience. Adolescent Res Rev 3, 123–154 (2018). https://doi.org/10.1007/s40894-017-0066-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40894-017-0066-z