
Abstract
Purpose of Review
Sleep complaints are common in people with epilepsy (PWE). We aim to highlight the updated evidence regarding comorbid sleep disorders and epilepsy and the impact of epilepsy and its treatments on sleep.
Recent Findings
Up to two thirds of PWE report sleep disturbances which may signal presence of a comorbid sleep disorder, including insomnia, arousal parasomnias, excessive daytime sleepiness, obstructive sleep apnea, or restless legs syndrome. Uncontrolled seizures contribute to poor sleep quality, while presence of epilepsy (with or without seizures) and antiepileptic drugs is associated with changes in sleep architecture. Chronic intracranial EEG monitoring with implanted devices reveals a nocturnal peak for interictal epileptiform activity. Epilepsy surgery outcomes suggest better seizure control may improve sleep architecture and quality.
Summary
Screening for and treating sleep disorders may lead to improved seizure control and quality of life in PWE. Epilepsy surgery and implanted devices to treat refractory epilepsy provide new insights into the relationship between sleep and epilepsy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Epilepsy affects about 1% of the population and carries substantial global physical, social, and economic consequences, accounting for an estimated 0.5% of disease burden worldwide [1, 2]. Persons with epilepsy (PWE) tend to have poorer quality of life than the general population, with a greater degree of impairment in the presence of reported sleep disturbances [3, 4]. Sleep impairment in PWE is a multifaceted concern, owing to numerous factors including diurnal and nocturnal seizures and medication side effects as well as comorbid sleep disorders [5, 6]. One area gaining increasing attention is the presence of comorbid sleep disorders, as treatment of such underrecognized conditions may lead to improvements in seizure control and overall quality of life in PWE. This article reviews both pivotal and current research as pertains to sleep and epilepsy with an emphasis on sleep disorders.
Sleep Concerns in Epilepsy
Broad Sleep Concerns
According to the NIH Sleep Disorders Research Plan, an estimated 25–30% of the general adult population—and a comparable percentage of children and adolescents—suffer from diminution of sleep health [7]. Sleep disturbances have been reported in up to two thirds of PWE, with similar rates in people with focal and generalized onset epilepsies, and twice as often as the general population [1, 8,9,10,11]. Sleep-related concerns include insufficient sleep, increased nocturnal and early morning awakenings (sleep-maintenance insomnia), impaired initiation of sleep (sleep-onset insomnia), nonrestorative sleep, and excessive daytime sleepiness whether or not antiepileptic drugs (AEDs) are used [1, 5, 8, 10, 12, 13]. As a result, patients experience a detrimental impact on quality of life, work productivity, and overall health [1, 14]. Studies suggest comorbidities and intractable seizures are important causes of sleep disturbances [11]. Owing to the intricate relationship between sleep and epilepsy, the origins of these concerns are manifold.
Epilepsy and Sleep Architecture
Epilepsy produces changes in sleep macrostructure and microstructure. In general, patients with epilepsy experience increased wake after sleep onset (WASO) and frequency of stage shifts, prolonged sleep onset latency, increased time spent in light non-rapid eye movement (NREM) sleep (stages I (N1) and II (N2) sleep), and decreased percentage of rapid eye movement (REM) sleep [15]. Polysomnographic (PSG) findings vary slightly depending on the underlying type of epilepsy and the frequency of ictal or interictal activity. Patients with untreated nocturnal frontal lobe epilepsy showed increased WASO and slow wave sleep duration with reduced N2 sleep. They were also found to have a reduction in REM sleep (duration and percentage), prolonged REM sleep latency and increased cyclic alternating pattern (CAP) time and rate, a marker of sleep instability [16, 17]. In a population of 99 patients with Juvenile Myoclonic Epilepsy (JME), PSG showed poorer sleep quality as evidenced by decreased sleep efficiency and REM sleep, prolonged sleep latency, and increased WASO and N1 sleep compared with controls. Epileptiform discharges occurred more often during N1 sand N2 sleep. These trends were observed similarly between drug-naïve and treatment groups [18]. Findings are generally similar across several recent studies [19,20,21]. Diurnal seizures produce postictal daytime somnolence, whereas nocturnal seizures directly disrupt sleep. In addition, the sleep period following seizure activity is characterized by increase WASO, sleep fragmentation and suppression of REM sleep, with a greater degree of impairment if seizures occur during the sleep period [22, 23]. Zanzmera et al. documented an association between poor seizure control and sleep latency, REM sleep latency, frequency of arousals, sleep efficiency, and total sleep time [24], while Ismayilova and colleagues reported a correlation between seizure control, nocturnal seizures, and insomnia [10]. Interictal discharges may also increase sleep fragmentation, independently of seizures, by interfering with the physiologic coordination of sleep, which may in turn result in daytime somnolence and impaired learning [22, 25].
Mood Disorders and Sleep Hygiene
Maestri and colleagues did not observe a difference in daytime sleepiness (as measured by nocturnal polysomnography, visual reaction times, and Epworth Sleepiness Scale) between de novo untreated patients with epilepsy (PWE) who were without significant comorbidities or frequent seizures and the control group, leading to the suggestion that comorbid psychiatric or sleep disorders, nocturnal seizures, sleep fragmentation, and antiepileptic therapy may play a larger role than the physiologic factors related to epilepsy itself [6, 26, 27•]. Several additional studies have highlighted the potential impact of depression on sleep quality in PWE. Moser et al. conducted a retrospective and prospective study in a small population of PWE (N = 32) to find that depression scores were a strong predictor of poor sleep, independent of the number of antiepileptic medications [28]. Vendrame et al. suggested a similar correlation between depression, sleep impairment, and quality of life, whereas the work of Ismayilova et al. and Im et al. did not support this finding [6, 9, 10].
Sleep hygiene encompasses the habits, behaviors, and environment that impact the duration and quality of sleep. Optimizing sleep conditions requires maintenance of a regular sleep schedule, creation of a comfortable sleeping environment (generally dark, quiet, and of the appropriate temperature), avoidance of activities beyond sleep and sex in the bedroom (particularly use of electronic devices that emit blue light), limitation of strenuous or stimulating activity late in the day (including late evening heavy exercise, nicotine, caffeine), and elimination of alcohol prior to bed [23]. Much of our understanding of the impact of sleep hygiene on epilepsy is extrapolated from the awareness of the overall impact of sleep dysfunction on epilepsy with fewer data to support a direct relationship between sleep hygiene and seizure control [15]. Inadequate sleep hygiene is known to reduce sleep quality and duration, and as such has often been attributed to poor seizure control [8, 23, 29]. Manni et al. conducted a questionnaire-based survey of more than 200 epilepsy patients in attempt to measure sleep hygiene in this population. He evaluated habits including coffee drinking, smoking, irregular sleep-wake/sleep deprivation, upsetting activities at bedtime, evening napping, bedroom heating/humidity, bedroom brightness, bedroom noise, and alcohol intake at bedtime. He found overall sleep hygiene was better in epilepsy patients when compared to controls in all categories but that of smoking and coffee consumption. This observation is possibly attributed to habitual avoidance of practices known to exacerbate seizures. No significant relationship between degree of sleep hygiene practice and severity of epilepsy was observed within this limited population [29]. While evidence to support the direct impact of sleep habits on epilepsy may be lacking, there are data to suggest a distinct relationship between inadequate sleep hygiene and low quality of life in PWE [30].
Sleep Deprivation in Epilepsy
The clinical relevance of sleep deprivation in epilepsy is a controversial topic. Many studies have been performed; however, multiple different methodologies and outcomes were assessed making comparison between the studies difficult. It has been long accepted that sleep deprivation facilitates neuronal excitation and thus interictal and ictal epileptiform activity [31,32,33]. Several animal models as well as transcranial magnetic stimulation studies have supported this principle [34,35,36]. Badawy et al. suggest that the result is due to an imbalance between neuronal excitation and inhibition in the setting of sleep deprivation, which has been supported by his studies using transcranial magnetic stimulation to assess cortical excitability [34]. Giorgi and colleagues published an extensive review of sleep deprivation and EEG studies and concluded that standardized methods of sleep deprivation could enhance future studies on this topic [37••]. There has been additional research suggesting that, when controlled for other variables such as emotional stress and alcohol, acute sleep deprivation alone does not increase seizure activity when compared with a normal sleep condition [38, 39].
Sleep Disorders in Epilepsy
Arousal Parasomnias
Arousal parasomnias (somnambulism, sleep terrors, and confusional arousals) are common in patients with epilepsy [40, 41] and may manifest with behaviors similar to those observed in sleep-related frontal and temporal lobe seizures [42]. Tassanari et al. suggest that activation of central pattern generators in the brainstem may be responsible for the similar behavioral manifestations in nocturnal frontal lobe epilepsy and arousal parasomnias [43]. Provini and colleagues found arousal parasomnias commonly occur in patients with nocturnal frontal lobe epilepsy, or as it is now referred to, sleep-related hypermotor epilepsy, and their family members (N = 34 and 39/100, respectively) in a case-controlled family study [41]. Another case-controlled family study in patients with sleep-related hypermotor epilepsy and their families reported significantly greater lifetime prevalence of somnambulism compared to healthy controls [40]. This increased comorbid prevalence in patients and their family members suggests that genetic factors may influence the manifestation of these disorders.
Distinguishing between sleep-related hypermotor epilepsy and arousal parasomnias can be a diagnostic dilemma and lead to misdiagnoses. Benbir et al. reported CAP increases in arousal parasomnias and frontal and temporal lobe epilepsies compared to healthy controls. Different CAP features were observed in patients with NREM parasomnias compared to those with epilepsy [44]. Although scalp Video EEG may be normal during these seizures if associated with a deeper ictal focus, prolonged Video EEG or PSG should be considered to record hypermotor seizures or interictal epileptiform discharges (IEDs) to confirm sleep-related hypermotor epilepsy according to the diagnostic criteria outlined by Tinuper et al. [45•].
Insomnia
Insomnia and poor sleep are common in patients with epilepsy (PWE) and may adversely impact seizure control and quality of life. Prevalence of insomnia in PWE has been reported from 28.9 to 74.4%, based on different inclusion criteria and methodology between studies [46], and are more common than prevalence of insomnia in the generalized US population, which has been reported to range from 10 to 15% [47]. In one study by Vendrame et al., 51% of PWE surveyed had insomnia based on the Insomnia Severity Index and 72% were poor sleepers based on the Pittsburgh Sleep Quality Index; these factors significantly correlated with the number of antiepileptic medications, scores of depressive symptoms, and were significant predictors of lower quality of life on the Quality of Life in Epilepsy Inventory-31 [6]. A recent study by Im and colleagues found sleep disturbances were more common in PWE vs. healthy controls (53 vs. 25.5%, p < 0.001). Poor sleep quality, excessive daytime sleepiness, and insomnia were significantly associated with epilepsy; however, PWE who were seizure-free over the past year had lower rates of insomnia [9]. Another recent study by Quigg et al. confirmed findings that insomnia in PWE was associated with short-term poor seizure control and worse quality of life [48]. Although further studies are needed to determine the relationship between insomnia and seizure frequency, these findings suggest that the presence of insomnia may influence the manifestation of seizures.
Hypersomnia and Narcolepsy
Excessive daytime sleepiness is a common complaint in patients with epilepsy (PWE). Evidence suggests that uncontrolled seizures, comorbid sleep disorders, and mood disorders are major contributing factors [11, 14, 28, 49]. There are conflicting studies regarding the impact of AEDs on daytime sleepiness. A recent study by Maestri et al. demonstrated that newly diagnosed PWE not on AEDs had no difference from controls on Multiple Sleep Latency tests, reaction times, or Epworth Sleepiness Scale scores [26]. Another study demonstrated 11.1% of PWE had excessive daytime sleepiness, more frequently in the presence of obstructive sleep apnea and depression [49]. Although excessive daytime sleepiness is frequently reported, comorbid narcolepsy and epilepsy has been infrequently documented with only a few recent case series published [50, 51].
Medications used to treat hypersomnia and narcolepsy may lower seizure threshold; however, modafinil and sodium oxybate may not increase risk of seizures. Ozsoay et al. demonstrated a dose-dependent decrease in seizure frequency and duration with administration of modafinil in rats with pentylenetetrazol-induced convulsive epilepsy [52]. Although this benefit has not been reported in human studies, retrospective studies suggest modafinil does not exacerbate seizures [53, 54]. One case series of patients with Video EEG proven idiopathic generalized epilepsy and comorbid narcolepsy Type I demonstrated no increased seizure frequency after sodium oxybate was added to antiepileptic medications [51].
Restless Legs Syndrome
Restless Legs Syndrome is a common disorder (5–15% US population) that manifests with an uncomfortable sensation in the limbs in the evenings at rest associated with an urge to move that improves with movement. It can be associated with iron deficiency, insomnia, and potentially, daytime impairment. Although primary Restless Legs Syndrome has been reported in 5.8% of an unselected Turkish epilepsy population [55] and 11% in a Nigerian epilepsy population [56], Geyer et al. found that 42% of patients with right temporal lobe epilepsy had primary Restless Legs Syndrome, 4.6 more likely than patients with left temporal lobe epilepsy, and some of those patients had Restless Legs Syndrome symptoms as a prodromal sign of seizures [57•]. Further studies into targeted epilepsy populations may lead to a better understanding about the relationship between epilepsy and Restless Legs Syndrome.
Sleep Apnea and Epilepsy
The prevalence of obstructive sleep apnea in patients with epilepsy (PWE) exceeds that of the general population and is associated with increased daytime somnolence, worsening quality of life, refractoriness of seizures, and potentially the risk of sudden unexpected death in epilepsy syndrome [23, 58,60,61,62,63,64,64]. Malow et al., in a study of 39 patients with refractory partial epilepsy, diagnosed obstructive sleep apnea (OSA; respiratory distress index > 5) in 33% of the population, with 13% having moderate to severe OSA (respiratory disturbance index > 10) [59]. More recently, Foldvary-Schaefer et al. demonstrated a similar prevalence of OSA in a retrospective study involving a population of 130 adults with epilepsy, 30% of whom had mild OSA and 16% of whom had more severe disease. The prevalence has been quoted as low as 9–10%, only slightly higher than the general population [58, 65], and as high as 80% [66], with variability depending on the population surveyed. The most consistent predictors of sleep apnea in PWE mirror risk factors for development of sleep apnea in the general population, including increasing age [58,60,60] and male gender [58, 59, 66]. There was less consistent data regarding association with higher body mass index [58, 67], neck circumference [67], increased seizure frequency [24, 58,60,60, 66, 68], nocturnal seizures [58, 59, 66], and dental problems [60].
While the reasons for increased prevalence of OSA among PWE are not fully elucidated, Foldvary-Schaefer et al. proposed one cause to be impairment of upper airway control related to extensive interictal discharges or seizures occurring from sleep [69]. Epilepsy treatments may also have an impact on the prevalence of sleep-disordered breathing. For instance, barbiturates and benzodiazepines may increase airway collapsibility, whereas valproic acid and carbamazepine may cause weight gain further increasing risk of obstructive apnea [33]. Vagus nerve stimulation is also known to worsen sleep-disordered breathing, including both obstructive and central sleep apneas, likely attributed to peripheral effects on upper airway musculature innervated by the Vagus nerve, alteration of central mechanisms responsible for airway patency and respiratory drive as well as increased vagal tone [33, 70, 71]. These deleterious effects may be reduced by decreasing Vagus nerve stimulation intensities and/or increasing signal off time as well as using continuous positive airway pressure therapy. These findings support the importance of screening patients for sleep apnea both before and after Vagus nerve stimulator implantation [72, 73].
Several studies have suggested worsening seizure control in patients with concomitant epilepsy and sleep apnea, suggesting a bi-directional relationship between OSA and epileptic seizures. This observation may be explained by chronic sleep deprivation, reduced sleep quality (i.e., fragmentation, frequent stage shifts, arousals, and sleep deprivation), acute and chronic paroxysmal hypoxia, and hypoxemia as well as sympathetic activation on epileptogenic brain regions [24, 33, 68, 74,76,76]. This conclusion is further reinforced by the numerous studies showing improvement in seizure control and reduction in interictal spike frequency with treatment of sleep apnea [61, 66, 77,79,80,80], highlighting the importance of diagnosis and treatment of sleep apnea in PWE as well as the need for further investigation into the potential pathogenic mechanisms.
Epilepsy Treatments and Sleep
Antiepileptic Drugs
AEDs have been reported to directly affect sleep architecture and indirectly contribute to various sleep disorders. An older review by Vaughn et al. reported drowsiness, increased sleep fragmentation, and reduced REM sleep with older AEDs including carbamazepine, phenobarbital, phenytoin and valproate, and increased slow wave sleep with pregabalin and gabapentin. Insomnia can be observed with felbamate, zonisamide, and high-dose lamotrigine [8]. A recent review by Jain and Glauser evaluated and rated the published evidence regarding the effects of AEDs on sleep architecture. Excessive daytime sleepiness was worsened with higher dosage levetiracetam, phenobarbital, and valproic acid but not with zonisamide or topiramate. Improved sleep efficiency and/or reduced sleep onset latency was observed with clobazam, carbamazepine, gabapentin, pregabalin, and tiagabine [27•]. Studies on chronopharmacology, adjusting AED amount and timing, show promise regarding strategies to tailor therapy and potentially improve seizure control in individuals, but further randomized studies are needed to determine which patients are likely to benefit [81•].
Epilepsy Surgery
Sleep stage has been shown to correlate with the expression of epilepsy with the most restricted fields manifesting during REM sleep. Okanari and colleagues demonstrated that children with generalized interictal epileptiform discharges (IEDs) on scalp Video EEG monitoring and normal/subtle changes on magnetic resonance imaging who underwent intracranial Video EEG for epilepsy surgery evaluation demonstrated both generalized and focal IEDs on intracranial Video EEG. Generalized IEDs occurred the least often during REM sleep (37%) and were more frequent during NREM sleep (67%, p < 0.001), and wakefulness (54%, p = 0.003). Lateralized IEDs were more frequent during REM sleep than NREM sleep. The hemisphere with lateralized IEDs during wakefulness, NREM, and REM sleep corresponded with the surgical side in 16 of 17 children. Multilobar resection was performed in 16 of 17 children, and 13 children were seizure-free after a mean 3.3 years postoperatively [82]. These findings suggest that IEDs recorded during REM sleep on intracranial Video EEG may help lateralize the epileptogenic zone in children with generalized IEDs and normal/subtle changes on magnetic resonance imaging.
Uncontrolled seizures have been reported to be a major cause of disrupted sleep in patients with epilepsy (PWE). Zanzmera and colleagues prospectively evaluated the effects of epilepsy surgery on subjective and objective measures of sleep in 17 PWE. Twelve (70.6%) patients had good surgical outcome (reduced seizure frequency), and these patients demonstrated improved subjective daytime sleepiness and objective arousal index and total sleep time suggesting improved sleep consolidation and sleep efficiency while three (25%) of these patients also demonstrated resolution of obstructive sleep apnea (apnea-hypopnea index improved from > 5 to < 5) [83••]. Serafini et al. evaluated the frequency of IEDs and effects on sleep macrostructure in 11 patients with refractory mesial temporal lobe epilepsy who became seizure-free for at least 2 years following epilepsy surgery. Reduction in IEDs was observed in all patients. A significant increase in total sleep time and REM sleep (p = 0.006) was observed after 1 year (p = 0.032 and 0.006, respectively) and REM sleep further increased after 2 years (p = 0.028) [84]. These findings suggest that only those patients with good postoperative seizure control (Engle classes I and II), but not those with persistent uncontrolled seizures, may show improvements in subjective and objective measures of sleep.
Deep Brain Stimulation
Deep brain stimulation of the bilateral anterior nuclei of the thalamus has been shown to improve seizure control in a large trial of people with refractory focal epilepsy [85]. Due to the importance of thalamic control of sleep-wake mechanisms, further understanding of the impact of thalamic deep brain stimulation on sleep is warranted. A recent study found that deep brain stimulation of the anterior nuclei of the thalamus was associated with sleep disruption. Increased arousals were observed during periods of stimulation appeared to be voltage-dependent [86]. Further studies are needed to characterize the impact of deep brain stimulation on sleep in patients with epilepsy.
Vagus Nerve Stimulation
As noted above, vagus nerve stimulation can worsen or induce sleep apnea at higher stimulus intensities. Additionally, vagus nerve stimulation is reported to have a voltage-dependent effect on daytime sleepiness and vigilance in patients with epilepsy (PWE) with lower stimulus intensities demonstrating improvements in subjective and objective sleep measures compared to pre-implantation, including in subjects without reductions in seizure frequency [87]. Lower stimulus intensities have been shown to improve daytime vigilance and quality of life in PWE as well [88]. Another study in children with vagus nerve stimulation for refractory epilepsy demonstrated decreased sleep latency and N1 sleep along with increased slow wave sleep during PSG. Increased arousals were observed, especially prior to stimulation; however, most children had reduced seizures, interictal epileptiform discharges, and improved quality of life [89].
Responsive Neurostimulation
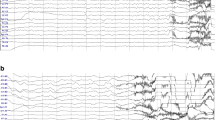
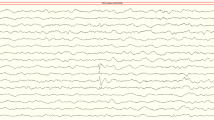
For patients with refractory epilepsy with two epileptogenic foci or a focus that overlaps eloquent cortex, implantation of a responsive neurostimulation device can detect and record seizure activity and then deliver therapeutic electrical stimulation to disrupt seizure activity. These devices provide ongoing electrocorticographical snapshots of short and long bursts of interictal epileptiform activity as well as seizures in the implanted brain areas. In some patients, the long bursts of interictal activity (i.e., long episodes) correlate with the individual patient’s electrographic and/or clinical seizures and can be used as a marker for ictal activity. Analysis of these long-term intracranial recordings is providing insights into circadian and ultradian patterns of focal seizure activity.
Previous studies utilizing scalp and intracranial Video EEG have demonstrated a nocturnal peak of interictal epileptiform discharges (IEDs) for most types of epilepsy and varying circadian patterns of seizures based on epileptogenic brain region [90,93,94,93] and also by age [91]. A recent study by Spencer and colleagues demonstrated that in people with a responsive neurostimulator implanted for refractory focal epilepsy, IEDs had a nocturnal peak frequency regardless of brain region while electrographic seizures had a circadian pattern that varied based on epileptogenic brain region. Neocortical seizures peaked during night and early morning hours while mesial temporal seizures had more complex, diurnal patterns [94••]. These findings confirm previously reported scalp and intracranial Video EEG studies and encourage further responsive neurostimulation studies to help characterize insights into the circadian and ultradian patterns of ictal and interictal epileptiform activity.
Conclusion
Sleep disturbances can affect a majority of patients with epilepsy (PWE) and often signal the presence of a comorbid sleep disorder, including excessive daytime sleepiness, insomnia, arousal parasomnias, obstructive sleep apnea, and restless legs syndrome. Thus, screening for and treating sleep disorders may lead to improved seizure control and quality of life in PWE. Antiepileptic drugs can alter sleep architecture and can be associated with daytime sleepiness, although further studies are needed to determine how amounts and timing of antiepileptic drugs affect sleep. Uncontrolled seizures contribute to poor sleep quality in PWE on subjective and objective sleep measures. The interictal expression of epilepsy is triggered by sleep with multiple scalp and intracranial EEG studies showing a nocturnal peak interictal epileptiform discharge frequency. The interictal epileptiform discharges observed during REM sleep may have lateralizing value in patients with intractable epilepsy undergoing epilepsy surgery evaluation. Epilepsy surgery outcomes suggest that improved seizure control is associated with improved sleep architecture. Although case reports suggest that epilepsy surgery may improve obstructive sleep apnea, further studies are needed to further define this association. Specific take-home points include the following:
Take-Home Points
-
Uncontrolled seizures and mood disorders contribute to poor quality sleep
-
Polysomnography data demonstrate poor sleep quality in patients with epilepsy (PWE), with prolonged latency of sleep onset and REM onset, reduced amounts of REM and slow wave sleep, and increased Non-REM stage 1 sleep and wake after sleep onset
-
Arousal parasomnias and epilepsy are common comorbidities and may share common central pattern generators and genetic factors
-
Video EEG or Polysomnography may help distinguish between arousal parasomnias and focal frontal and temporal lobe epilepsies
-
Insomnia is very common in PWE and is associated with uncontrolled seizures and poor quality of life
-
Obstructive sleep apnea occurs more frequently in PWE and can worsen seizure control if left untreated; treating OSA can improve seizure control
-
Restless legs syndrome may be more common in people with right temporal lobe epilepsy
-
Vagus nerve stimulation in PWE can induce/worsen obstructive and central sleep apnea; thus, consider polysomnographic evaluation and then vagus nerve stimulator adjustment and/or continuous positive airway pressure therapy if needed to mitigate these effects
-
Interictal epileptiform discharges during REM sleep may help lateralize the seizure onset zone in children with intractable epilepsy
-
Successful epilepsy surgery may improve objective sleep macrostructure, subjective sleepiness, and possibly obstructive sleep apnea
Abbreviations
- AEDs:
-
Antiepileptic drugs
- CAP:
-
Cyclic alternating pattern
- EEG:
-
Electroencephalography
- IED:
-
Interictal epileptiform discharge
- NREM:
-
Non-rapid eye movement sleep
- N1:
-
NREM stage 1 sleep
- N2:
-
NREM stage 2 sleep
- N3:
-
NREM stage 3 sleep
- OSA:
-
Obstructive sleep apnea
- PSG:
-
Polysomnography
- PWE:
-
People/patients with epilepsy
- REM:
-
Rapid eye movement sleep
- WASO:
-
Wake after sleep onset
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
De Weerd A, De Haas S, Otte A, Trenité DK-N, Van Erp G, Cohen A, et al. Subjective sleep disturbance in patients with partial epilepsy: a questionnaire-based study on prevalence and impact on quality of life. Epilepsia. 2004;45(11):1397–404. https://doi.org/10.1111/j.0013-9580.2004.46703.x.
Matilde Leonardi TBU. The global burden of epilepsy. Epilepsia. 2002;43(s6):21–5. https://doi.org/10.1046/j.1528-1157.43.s.6.11.x.
Yazdi Z, Sadeghniiat-Haghighi K, Naimian S, Al Zohal M, Ghanin M. Prevalence of sleep disorders and their effects on sleep quality in epileptic patients. Basic Clin Neurosci. 2013;4(1):36–41.
Charitomeni Piperidou AK, Triantafyllou N, Terzoudi A, Constantinidis T, Vadikolias K, Heliopoulos I, et al. Influence of Sleep Disturbance on Quality of Life in Patients With Epilepsy. Seizure. 2008;17(7):588–94. https://doi.org/10.1016/j.seizure.2008.02.005.
Saraswati N, Nayak C, Sinha S, Nagappa M, Thennarasu K, Taly AB. Comparing sleep profiles between patients with juvenile myoclonic epilepsy and symptomatic partial epilepsy: sleep questionnaire-based study. Epilepsy Behav. 2017;66:34–8. https://doi.org/10.1016/j.yebeh.2016.10.009.
Vendrame M, Yang B, Jackson S, Auerbach SH. Insomnia and epilepsy: a questionnaire-based study. J Clin Sleep Med. 2013;9(2):141–6. https://doi.org/10.5664/jcsm.2410.
National Institutes of Health Sleep Disorders Research Plan. www.nhlbi.nih.gov: National Institutes of Health, Research NCoSD;2011.
Vaughn BV, Ali I. Sleep and epilepsy: opportunities for diagnosis and treatment. Neurol Clin. 2012;30(4):1249–74.
Im H-J, Park S-H, Baek S-H, Chu MK, Yang KI, Kim W-J, et al. Associations of impaired sleep quality, insomnia and sleepiness with epilepsy: A questionnaire-based case-control study. Epilepsy Behav. 2016;57(Part A):55–9. https://doi.org/10.1016/j.yebeh.2016.01.022.
Ismayilova VD, Ugur A, Tezer I. Subjective sleep disturbance in epilepsy patients at an outpatient clinic: a questionnaire-based study on prevalence. Epilepsy Res. 2015;115:119–25. https://doi.org/10.1016/j.eplepsyres.2015.06.009.
Unterberger I, Gabelia D, Prieschl M, Chea K, Hofer M, Hogl B, et al. Sleep disorders and circadian rhythm in epilepsy revisited: a prospective controlled study. Sleep Med. 2015;16(2):237–42. https://doi.org/10.1016/j.sleep.2014.09.021.
Watson NF, Viola-Saltzman M. Sleep and comorbid neurologic disorders. Continuum. 2013;19(1):148–69. https://doi.org/10.1212/01.CON.0000427208.13553.8c.
Staniszewska A, Mąka A, Religioni U, Olejniczak D. Sleep disturbances amont patients with epilepsy. Neuropsychiatr Dis Treat. 2017;Volume 13(13):1797–803. https://doi.org/10.2147/NDT.S136868.
Giorelli AS, Passos P, Carnaval T, Gomes M. Excessive daytime sleepiness and epilepsy: a systematic review Epilepsy Res Treat. 2013;2013(Article ID 629469):9 pages. https://doi.org/10.1155/2013/629469.
Foldvary N. Sleep and epilepsy. Curr Treat Options Neurol. 2002;4:129–35.
Parrino L, De Paolis F, Milioli G, Gioi G, Grassi A, Riccardi S, et al. Distinctive polysomnographic traits in nocturnal frontal lobe epilepsy. Epilepsia. 2012;57(7):1178–84. https://doi.org/10.1111/j.1528-1167.2012.03502.x.
Zucconi M, Oldani A, Smirne S, Ferini-Strambi L. The macrostructure and microstructure of sleep in patients with autosomal dominant nocturnal frontal lobe epilepsy. J Clin Neurophysiol. 2000;17(1):77–86.
Roshan S, Puri V, Chaudhry N, Gupta A, Rabi SK. Sleep abnormalities in juvenile myoclonic epilepsy—a sleep questionnaire and polysomnography based study. Seizure. 2017:194–201. https://doi.org/10.1016/j.seizure.2017.06.021.
Nayak CS, Sinha S, Nagappa M, Kandavel T, Taly AB. Effect of valproate on the sleep microstructure of juvenile myoclonic epilepsy patients – a cross-sectional CAP based study. Sleep Med. 2016;17(2016):129–33.
Krishnan P, Sinha S, Taly AB, Ramachandraiah CT, Rao S, Satishchandra P. Altered polysomnographic profile in juvenile myoclonic epilepsy. Epilepsy Res. 2014;108:459–67.
Ramachandraiah CT, Sinha S, Taly AB, Rao S, Satishchadra P. Interrelationship of sleep and juvenile myoclonic epilepsy (JME): a sleep questionnaire-, EEG-, and polysomnography (PSG)-based prospective case–control study. Epilepsy Behav. 2012;25:391–6.
Ju YS, Videnovic A, Vaughn BV. Comorbid Sleep Disturbances in Neurologic Disorders. Continuum: Lifelong Learn Neurol. 2017;23(4):1117–31. https://doi.org/10.1212/CON.0000000000000501.
Bazil CW. Epilepsy and sleep disturbance. Epilepsy Behav. 2003;4:39.
Zanzmera P, Shukla G, Gupta A, Singh H, Goyal V, Srivastava A, et al. Markedly disturbed sleep in medically refractory compared to controlled epilepsy- A clinical and polysomnography study. Seizure. 2012;21:487–90.
Glennon JM, Weiss-Croft L, Harrison S, Cross JH, Boyd SG, Baldeweg T. Interictal epileptiform discharges have an independent association with cognitive impairment in children with lesional epilepsy. Epilepsia. 2016;57(9):1436–42. https://doi.org/10.1111/epi.13479.
Maestri M, Giorgi FS, Pizzanelli C, Fabbrini M, Di Coscio E, Carnicelli L, et al. Daytime sleepiness in de novo untreated patients with epilepsy. Epilepsy Behav. 2013;29(2):344–8. https://doi.org/10.1016/j.yebeh.2013.07.025.
• Jain SVG, Tracy A. Effects of epilepsy treatments on sleep architecture and daytime sleepiness: an evidence-based review of objective sleep metrics. Epilepsia. 2013;55(1):26–37. https://doi.org/10.1111/epi.12478. This is an extensive review which critically evaluates the literature evaluating the effects of AEDs on objective sleep measures.
Moser D, Pablik E, Aull-Watschinger S, Pataraia E, Wöber C, Seidel S. Depressive symptoms predict the quality of sleep in patients with partial epilepsy — a combined retrospective and prospective study. Epilepsy Behav. 2015;47:104–10. https://doi.org/10.1016/j.yebeh.2015.04.021.
Manni RPL, Ratti MT, Marchioni E, Sartori I, Galimberti CA, Tartara A. Sleep hygiene in adult epilepsy patients: a question naire-based survey. Acta Neurol Scand. 2000;101:301–4.
Lee S-A, Han S-H, No Y-J, Jo K-D, Kwon J-H, Kim JY, et al. Sleep hygeine and its association with mood and quality of life in people with epilepsy. Epilepsy Behav. 2015;52(Part A):225–9. https://doi.org/10.1016/j.yebeh.2015.09.011.
Malow BA. Sleep deprivation and epilepsy. Epilepsy Curr. 2004;4(5):193–5.
Diaz-Negrillo A. Influence of sleep and sleep deprivation on ictal and Interictal epileptiform activity. Epilepsy Res Treat. 2013;2013:1–7. https://doi.org/10.1155/2013/492524.
van Golde EG, Gutter T, de Weerd AW. Sleep disturbances in people with epilepsy; prevalence, impact and treatment. Sleep Med Rev. 2011;15(6):357–68. https://doi.org/10.1016/j.smrv.2011.01.002.
Badaway RA, Curatolo JM, Newton M, Berkovich SF, Macdonell RAL. Sleep deprivation increases cortical excitability in epilepsy: syndrome-specific effects. Neurology. 2006;67(6):1018–22. https://doi.org/10.1212/01.wnl.0000237392.64230.f7.
Hrnčić D, Rasić-Marković A, Bjekić-Macut J, Šušić V, Djuric D, Stanojlović O. Paradoxical sleep deprivation potentiates epilepsy induced by homocysteine thiolactone in adult rats. SAGE J. 2013;238(1):77–83. https://doi.org/10.1258/ebm.2012.012154.
Anderson ML, Matos G, Martins RCS, Tufik S. Sleep deprivation increases seizures induced by cocaine in rats. Sleep Sci. 2010;3(4):131–5.
•• Giorgi FS, Guida M, Caciagli L, Maestri M, Carnicelli L, Bonanni E, et al. What is the role for EEG after sleep deprivation in the diagnosis of epilepsy? Issues, controversies, and future directions. Neurosci Biobehav Rev. 2014;47:533–48. https://doi.org/10.1016/j.neubiorev.2014.10.005. This study provides an extensive review on sleep deprivation and EEG with suggestions on standardized methods that can improve future studies.
Malow BA, Passaro E, Milling C, Minecan DN, Levy K. Sleep deprivation does not affect seizure frequency during inpatient video-EEG monitoring. Neurology. 2002;59(9):1371–4. https://doi.org/10.1212/01.WNL.0000031810.15811.9E.
Malow BA, Passaro EA, Hall JH, et al. Sleep deprivation does not increase seizure frequency during long term monitoring. Epilepsia. 1999;40(Suppl 7):99–100.
Bisulli F, Vignatelli L, Naldi I, Licchetta L, Provini F, Plazzi G, et al. Increased frequency of arousal parasomnias in families with nocturnal frontal lobe epilepsy: a common mechanism? Epilepsia. 2010;51(9):1852–60. https://doi.org/10.1111/j.1528-1167.2010.02581.x.
Provini F, Plazzi G, Tinuper P, Vandi S, Lugaresi E, Montagna P. Nocturnal frontal lobe epilepsy. A clinical and polygraphic overview of 100 consecutive cases. Brain. 1999;122(Pt 6):1017–31.
Schenck CH. The far side of sleep: Towards a deeper understanding of parasomnias and nocturnal seizures. Sleep Sci. 2014;7(3):129–34. https://doi.org/10.1016/j.slsci.2014.11.006.
Tassinari CA, Rubboli G, Gardella E, Cantalupo G, Calandra-Buonaura G, Vedovello M, et al. Central pattern generators for a common semiology in fronto-limbic seizures and in parasomnias. A neuroethologic approach. Neurol Sci. 2005;26(Suppl 3):s225–32. https://doi.org/10.1007/s10072-005-0492-8.
Benbir G, Kutlu A, Gozubatik-Celik G, Karadeniz DCAP. Characteristics differ in patients with arousal parasomnias and frontal and temporal epilepsies. J Clin Neurophysiol. 2013;30(4):396–402. https://doi.org/10.1097/WNP.0b013e31829dda86.
• Tinuper P, Bisulli F, Cross JH, Hesdorffer D, Kahane P, Nobili L, et al. Definition and diagnostic criteria of sleep-related hypermotor epilepsy. Neurology. 2016;86(19):1834–42. https://doi.org/10.1212/wnl.0000000000002666. This is an important study which defines criteria that renames and defines diagnostic criteria for sleep-related hypermotor epilepsy.
Macedo P, Oliveira PS, Foldvary-Schaefer N, Gomes MDM. Insomnia in people with epilepsy: a review of insomnia prevalence, risk factors and associations with epilepsy-related factors. Epilepsy Res. 2017;135:158–67. https://doi.org/10.1016/j.eplepsyres.2017.05.014.
Kraus SS, Rabin LA. Sleep America: managing the crisis of adult chronic insomnia and associated conditions. J Affect Disord. 2012;138(3):192–212. https://doi.org/10.1016/j.jad.2011.05.014.
Quigg M, Gharai S, Ruland J, Schroeder C, Hodges M, Ingersoll KS, et al. Insomnia in epilepsy is associated with continuing seizures and worse quality of life. Epilepsy Res. 2016;122:91–6. https://doi.org/10.1016/j.eplepsyres.2016.02.014.
Gammino M, Zummo L, Bue AL, Urso L, Terruso V, Marrone O, et al. Excessive daytime sleepiness and sleep disorders in a population of patients with epilepsy: a case-control study. J Epilepsy Res. 2016;6(2):79–86. https://doi.org/10.14581/jer.16015.
Joshi PA, Poduri A, Kothare SV. Juvenile myoclonic epilepsy and narcolepsy: a series of three cases. Epilepsy Behav. 2015;51:163–5. https://doi.org/10.1016/j.yebeh.2015.07.030.
Baiardi S, Vandi S, Pizza F, Alvisi L, Toscani L, Zambrelli E, et al. Narcolepsy type 1 and idiopathic generalized epilepsy: diagnostic and therapeutic challenges in dual cases. J Clin Sleep Med. 2015;11(11):1257–62. https://doi.org/10.5664/jcsm.5180.
Ozsoy S, Aydin D, Ekici F. Effects of modafinil on pentylenetetrazol-induced convulsive epilepsy. Bratisl Lek Listy. 2015;116(3):162–6.
Andrade C. A method for deciding about the possible safety of modafinil and armodafinil in patients with seizure disorder. J Clin Psychiatry. 2016;77(1):e25–8. https://doi.org/10.4088/JCP.15f10580.
Artsy E, McCarthy DC, Hurwitz S, Pavlova MK, Dworetzky BA, Lee JW. Use of modafinil in patients with epilepsy. Epilepsy Behav. 2012;23(4):405–8. https://doi.org/10.1016/j.yebeh.2012.02.011.
Ozturk I, Aslan K, Bozdemir H, Foldvary-Schaefer N. Frequency of Restless Legs Syndrome in adults with epilepsy in Turkey. Epilepsy Behav. 2016;57(Pt A):192–5. https://doi.org/10.1016/j.yebeh.2016.02.013.
Komolafe MA, Sunmonu TA, Ogunrin OA, Disu JO, Ezeala BA, Abubakar SA, et al. Sleep disturbances among patients with epilepsy in Nigeria. Ann Afr Med. 2015;14(2):103–8. https://doi.org/10.4103/1596-3519.149880.
• Geyer JD, Geyer EE, Fetterman Z, Carney PR. Epilepsy and restless legs syndrome. Epilepsy Behav. 2017;68:41–4. https://doi.org/10.1016/j.yebeh.2016.12.010. This is the first study to demonstrate that restless legs syndrome may be associated with a lateralized focal epilepsy (right temporal lobe).
Manni R, Terzaghi M, Arbasino C, Sartori I, Calimberti CA, Tartara A. Obstructive sleep apnea in a clinical series of adult epilepsy patients: frequency and features of the comorbidity. Epilepsia. 2003;44(6):836–40. https://doi.org/10.1046/j.1528-1157.2003.55702.x.
Malow BL, Levy K, Maturen K, Bowes R. Obstructive sleep apnea is common in medically refractory epilepsy patients. Neurology. 2000;55(7):1002–7.
Foldvary-Schaefer N, Andrews ND, Pornsriniyom D, Moul DE, Sun Z, Bena J. Sleep apnea and epilepsy: Who’s at risk? Epilepsy Behav. 2012;25:363–7.
Li P, Ghadersohi S, Jafari B, Teter B, Sazgar M. Characteristics of refractory vs. medically controlled epilepsy patients with obstructive sleep apnea and their response to CPAP treatment. Seizure. 2012;21(9):717–21. https://doi.org/10.1016/j.seizure.2012.07.016.
Park JG, Ramar K, Olson EJ. Updates on definition, consequences, and Management of Obstructive Sleep Apnea. Mayo Clin Proc. 2011;86(60):549–55.
Klobucnikova K, Siarnik P, Sivakova M, Kollar B. Sleep-disordered breathing and excessive daytime sleepiness in patients with epilepsy - a polysomnographic study. Neuroendocrinol Lett. 2016;37(4):313–7.
Derry CP, Duncan S. Sleep and Epilepsy. Epilepsy Behav. 2013;26(3):394–404. https://doi.org/10.1016/j.yebeh.2012.10.033.
Khatami R, Zutter D, Siegel A, Mathis J, Donati F, Bassetti CL. Sleep-wake habits and disorders in a series of 100 adult epilepsy patients--a prospective study. Seizure. 2006;15:299–306.
Malow B, Foldvary-Schaefer N, Vaughn BV, Selwa LM, Chervin RD, Weatherwax KJ, et al. Treating obstructive sleep apnea in adults with epilepsy: a randomized pilot trial. Neurology. 2008;71(8):572–7. https://doi.org/10.1212/01.wnl.0000323927.13250.54.
Venturi M, Neves GS, Pontes IM, Valois A, de Mota Gomes M. Risk and determinant factors for obstructive sleep apnea in patients with epilepsy. Arq Neuropsiquiatr. 2011;69(6):924–7.
Chihorek AM, Abou-Khalil B, Malow BA. Obstructive sleep apnea is associated with seizure occurrence in older adults with epilepsy. Neurology. 2007;69(19):1823–7. https://doi.org/10.1212/01.wnl.0000279334.78298.d5.
Foldvary-Schaefer N, Stephenson L, Bingaman W. Resolution of obstructive sleep apnea with epilepsy surgery? Expanding the relationship between sleep and epilepsy. Epilepsia. 2008;49(8):1457–9.
Marzec M, Edwards J, Sagher O, Fromes G, Malow BA. Effects of vagus nerve stimulation on sleep-related breathing in epilepsy patients. Epilepsia. 2003;44(7):930–5.
Salvadé A, Ryvlin P, Rossetti AO. Impact of vagus nerve stimulation on sleep-related breathing disorders in adults with epilepsy. Epilepsy Behav. 2017;79:126–9.
Parhizgar F, Nugent K, Raj R. Obstructive sleep apnea and respiratory complications associated with Vagus nerve stimulators. J Clin Sleep Med. 2011;7(4):401–7. https://doi.org/10.5664/JCSM.1204.
Upadhyay H, Bhat S, Gupta D, Mulvey M, Ming S. The therapeutic dilemma of vagus nerve stimulatorinduced sleep disordered breathing. Ann Thorac Med. 2016;11(2):151–4. https://doi.org/10.4103/1817-1737.180025.
Brunetti V, Ferilli MAN, Vollono C, Della Marca G. Sleep apneas trigger epilepsy. Sleep Med. 2017;39:23–4.
Manni RT, Comorbidity M. between epilepsy and sleep disorders. Epilepsy Res. 2010;90:171–7.
Sonka K, Juklícková M, Pretl M, Dostálová S, Horínek D, Nevsímalová S. Seizures in sleep apnea patients: occurrence and time distribution. Sb Lek. 2000;101(3):229–32.
Wyler AR, Weymuller EA Jr. Epilepsy complicated by sleep apnea. Ann Neurol. 1981;9(4):403–4. https://doi.org/10.1002/ana.410090415.
Devinsky O, Ehrenberg B, Barthlen GM, Abramson HS, Luciano D. Epilepsy and sleep apnea syndrome. Neurology. 1994;44(11):2060–4.
Vendrame M, Auerbach S, Loddenkemper T, Kothare S, Montouris G. Effect of continuous positive airway pressure treatment on seizure control in patients with obstructive sleep apnea and epilepsy. Epilepsia. 2011;52(11):168–71.
Pornsriniyom D, Kim HW, Bena J, Andrews ND, Moul D, Foldvary-Schaefer N. Effect of positive airway pressure therapy on seizure control in patients with epilepsy and obstructive sleep apnea. Epilepsy Behav. 2014;37:270–5. https://doi.org/10.1016/j.yebeh.2014.07.005.
• Ramgopal S, Thome-Souza S, Loddenkemper T. Chronopharmacology of anti-convulsive therapy. Curr Neurol Neurosci Rep. 2013;13(4):339. https://doi.org/10.1007/s11910-013-0339-2. This review evaluates studies regarding the factors that may affect the chronopharmacology of AEDs.
Okanari K, Baba S, Otsubo H, Widjaja E, Sakuma S, Go CY, et al. Rapid eye movement sleep reveals epileptogenic spikes for resective surgery in children with generalized interictal discharges. Epilepsia. 2015;56(9):1445–53. https://doi.org/10.1111/epi.13081.
•• Zanzmera P, Shukla G, Gupta A, Goyal V, Srivastava A, Garg A, et al. Effect of successful epilepsy surgery on subjective and objective sleep parameters--a prospective study. Sleep Med. 2013;14(4):333–8. https://doi.org/10.1016/j.sleep.2012.11.017. This is the first study to prospectively measure objective and subjective parameters before and after temporal lobectomy.
Serafini A, Kuate C, Gelisse P, Velizarova R, Gigli GL, Coubes P, et al. Sleep before and after temporal lobe epilepsy surgery. Seizure. 2012;21(4):260–5. https://doi.org/10.1016/j.seizure.2012.01.007.
Fisher R, Salanova V, Witt T, Worth R, Henry T, Gross R, et al. Electrical stimulation of the anterior nucleus of thalamus for treatment of refractory epilepsy. Epilepsia. 2010;51(5):899–908. https://doi.org/10.1111/j.1528-1167.2010.02536.x.
Voges BR, Schmitt FC, Hamel W, House PM, Kluge C, Moll CK, et al. Deep brain stimulation of anterior nucleus thalami disrupts sleep in epilepsy patients. Epilepsia. 2015;56(8):e99–e103. https://doi.org/10.1111/epi.13045.
Malow BA, Edwards J, Marzec M, Sagher O, Ross D, Fromes G. Vagus nerve stimulation reduces daytime sleepiness in epilepsy patients. Neurology. 2001;57(5):879–84.
Galli R, Bonanni E, Pizzanelli C, Maestri M, Lutzemberger L, Giorgi FS, et al. Daytime vigilance and quality of life in epileptic patients treated with vagus nerve stimulation. Epilepsy Behav. 2003;4(2):185–91.
Hallbook T, Lundgren J, Kohler S, Blennow G, Stromblad LG, Rosen I. Beneficial effects on sleep of vagus nerve stimulation in children with therapy resistant epilepsy. Eur J Paediatr Neurol. 2005;9(6):399–407. https://doi.org/10.1016/j.ejpn.2005.08.004.
Karafin M, St Louis EK, Zimmerman MB, Sparks JD, Granner MA. Bimodal ultradian seizure periodicity in human mesial temporal lobe epilepsy. Seizure. 2010;19(6):347–51. https://doi.org/10.1016/j.seizure.2010.05.005.
Passarelli V, Castro LH. Gender and age influence in daytime and nighttime seizure occurrence in epilepsy associated with mesial temporal sclerosis. Epilepsy Behav. 2015;50:14–7. https://doi.org/10.1016/j.yebeh.2015.05.028.
Durazzo TS, Spencer SS, Duckrow RB, Novotny EJ, Spencer DD, Zaveri HP. Temporal distributions of seizure occurrence from various epileptogenic regions. Neurology. 2008;70(15):1265–71. https://doi.org/10.1212/01.wnl.0000308938.84918.3f.
Hofstra WA, Grootemarsink BE, Dieker R, van der Palen J, de Weerd AW. Temporal distribution of clinical seizures over the 24-h day: a retrospective observational study in a tertiary epilepsy clinic. Epilepsia. 2009;50(9):2019–26. https://doi.org/10.1111/j.1528-1167.2009.02044.x.
•• Spencer DC, Sun FT, Brown SN, Jobst BC, Fountain NB, Wong VS, et al. Circadian and ultradian patterns of epileptiform discharges differ by seizure-onset location during long-term ambulatory intracranial monitoring. Epilepsia. 2016;57(9):1495–502. https://doi.org/10.1111/epi.13455. This large study carefully characterizes circadian patterns of interictal epileptiform discharges and timing of seizures based on long-term intracranial data from patients with implanted RNS for refractory epilepsy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Leslie P. Grayson declares no conflicts of interest.
Jennifer L. DeWolfe reports grants from Marinus Pharmaceuticals, outside the submitted work.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Sleep and Neurological Disorders
Rights and permissions
About this article

Cite this article
Grayson, L.P., DeWolfe, J.L. Sleep Disorders in Epilepsy: Current Trends and Future Perspectives. Curr Sleep Medicine Rep 4, 125–133 (2018). https://doi.org/10.1007/s40675-018-0110-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40675-018-0110-y