
Abstract
Purpose of review
To highlight the role sleep plays in epilepsy and the importance for evaluating and treating sleep issues in patients with epilepsy.
Recent findings
Recent studies show that patients with epilepsy have a twofold greater prevalence of sleep complaints. These complaints can stem from the epilepsy or its treatment. The identification of sleep disorders may require further inquiry as some standard questionnaires are not as accurate in patients with less perceived symptoms. Further work suggests that discharges from the epileptic focus during sleep or wake may have differentiating effects on the physiological sleep processes. This offers new insights to the possible mechanisms contributing to the development of resistant epilepsies. Additional studies suggest treating sleep disorders, such as sleep apnea, benefits some patients, as does treating epilepsy may improve sleep.
Summary
Sleep disorders are prevalent in patients with epilepsy. Recognizing and treating comorbid sleep disorders affect patient quality of life and seizure freedom.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The relationship between sleep and epilepsy is bidirectional and remains complex despite recent gains in our understanding of both states. Historically, one of the first to describe this relationship was Aristotle who wrote “in many cases, epilepsy sets in during sleep” [1]. Later in the 1800s, Gowers estimated about 20% of epilepsy patients had seizures during sleep and that two-thirds of patients followed a diurnal pattern [2]. Further observations of the interaction of sleep, sleep deprivation, and sleep disorders in patients with epilepsy help us understand the window sleep provides to understanding epilepsy. Over the past 5 years, more research into epilepsy and sleep have contributed to understanding this relationship.
The epidemiology and characteristics of this relationship, pathophysiology of epilepsy in sleep, the ramifications of epilepsy on sleep, and the treatment sleep disorders in epilepsy patients are a small selection of topics in this complex link between epilepsy and sleep. Our aim is to highlight the importance of this bidirectional interaction.
Sleep Deprivation in Epilepsy
Traditionally, sleep deprivation has been cautioned against for patients with epilepsy [2]. Although epileptic seizures are precipitated by a variety of factors, the impact of sleep loss was found to be an important independent seizure trigger based on this prospective case crossover study [3]. In a prospective study of 104 patients (50 male and 54 female) from an outpatient epilepsy clinic, Ferlisi and Shorvon et al. found patients cited stress (82%) and sleep deprivation (70%) as the top two precipitants for seizures. They noted that sleep deprivation was noted more frequently to provoke seizures in patients with generalized epilepsy than in those with focal seizures [4].
Sleep Complaints and Sleep Disorders in Epilepsy
Analogous to sleep loss, perception of sleep disruption is traditionally noted to be two to three times more prevalent in patients with epilepsy. Several recent studies reemphasize the higher prevalence of sleep-related complaints. Ismayilova showed, using a series of questionnaires, a nearly twofold higher prevalence subjective complaints of insomnia, sleep apnea, and parasomnia in individuals with epilepsy than control subjects and that insomnia is more prevalent in those with nocturnal seizures and frequent epileptiform activity on EEG. They also reported that those who were seizure free for 2 years had much lower rates of insomnia [5]. Similar high prevalence of sleep complaints are noted in studies of patients with epilepsy in Poland [6] and Iran [7].
Many investigators stress the importance of screening for insomnia. Based on their cross-sectional case control study (n = 180; men 50% with a control group n = 2836; men 49.8%) Im found that epilepsy was significantly associated with poor sleep quality and insomnia after adjusting for depressive mood, anxiety, and other covariates such as alcohol use, tobacco use, insufficient sleep, BMI, age, and habitual snoring (Table 1) [8]. Other studies have attempted to evaluate the prevalence and impact of sleep complaints such as insomnia. Quigg found insomnia more common in those with refractory epilepsy and correlated with lower quality of life [9]. Yet the exact relationship of the insomnia to epilepsy remains controversial. Vendrame, using a retrospective review of cases, correlated insomnia with the number of antiepileptic medications and higher scores of depressive symptoms but contrary to others did not find a correlation between insomnia and poor seizure control [10]. This might be in part related to the method of analysis primarily comparing good to poor sleepers, and including patients who continued to have seizures, even at a low rate in the “good seizure control” group. Thus, the presence of seizures even at a low rate may influence the presence of insomnia.
Identifying the correct tool for diagnosing insomnia may be part of the challenge. Oliveria et al. in their review article noted that the prevalence of insomnia symptoms or disorder is widely varied from 36 to 74% using the International Classification of Sleep Disorders-2 (ICSD-2) criteria [11]. Epilepsy-related factors related to insomnia included characteristics such as post-traumatic epilepsy, focal epilepsy, nocturnal seizures, refractory epilepsy, and AED polytherapy in both adult and pediatric populations [11]. Yang showed, in their cohort of patients with epilepsy (n = 90), 29% had moderate to severe insomnia, as measured by the Insomnia Severity Index (ISI) score of > 8 [12]. However, the study compared the ISI and the ICSD-2 criteria for insomnia reporting that control group showed good agreement between the two methods but the epilepsy group had significant disagreement for those with low or intermediate levels of symptoms of insomnia. This raises the possibility that the standard questionnaires may misclassify some patients, due to either a difference in presentation or that the insomnia related to epilepsy may be distinct from previous categorizations of insomnia. The study population was controlled for OSA (with PSG), AED burden (standardized AED dose methodology by WHO), and modified Beck Depression Inventory (two questions related to evaluation of insomnia were removed) [12]. In their cohort, insomnia severity did correlate with AED polytherapy but not seizure type or seizure burden, although this would suggest that the degree of epilepsy may not play a role. However, seizure freedom was not specifically tested. These findings have led to speculation comorbid issues such as depression symptoms, sedative-hypnotic use, asthma/COPD, and head trauma may play a contributing role to the sleep disruption [12, 13]. These varied findings suggest that insomnia in patients with epilepsy is prevalent, may be multifactorial, and suggests the need for better tools to diagnose the insomnia and identify drivers.
Unfortunately, the dilemma of resolving whether epilepsy itself is associated with insomnia carries into studies in the pediatric epilepsy population. Saraswati et al. noted in their cross-sectional study (n = 120) that patient with JME (n = 40) or partial epilepsy (n = 40) had worse subjective sleep quality (ESS, PSQI) irrespective of AED monotherapy or drug naivety compared to controls (n = 40) [14]. Also using questionnaires in children and adolescents with epilepsy, a study in Norway found that psychiatric comorbidities were associated with reported sleep problems even after adjusting for relevant epilepsy factors [15].
One clue as to underlying mechanism may be from the patient perception and locus of control. Rizou’s study of illness perceptions among pediatric epilepsy patients found that those who believe that they had less personal control over their illness reported more sleep disturbance and higher levels of fatigue. This study excluded children with psychiatric comorbidities [16•]. Correspondingly, parental reports of sleep quality are often used in practice. However, Tsai, in a cross-sectional study using actigraphy and parental knowledge about childhood sleep, reported parents with children with epilepsy frequently gave inadequate information that was not supported by objective data [17••]. This highlights the importance of objective data in approaching these patient issues.
Similar to insomnia, the preponderance of evidence continues to suggest sleep-disordered breathing can be provocative and is prevalent in patients with epilepsy. The provocative nature of sleep apnea is highlighted in a case report of a patient whose repetitive apneas induced epileptiform discharges demonstrating the provocative nature of individual apneic events [18]. Overall, the prevalence of sleep apnea in patients with epilepsy appears to be elevated. Applying the STOP-BANG questionnaire to patients in an academic epilepsy clinic, Sharma identified 31% of patients as having significant risk of OSA and showed that application of the questionnaire in an epilepsy clinic improved the frequency of patient referral for formal sleep study [19]. Unfortunately, the study did not show the percentage of individuals who had apnea that had low scores on the questionnaire. In a recent meta-analysis of multiple polysomnographic studies, Lin estimated the prevalence of OSA to be 33% [20•]. This prevalence may be influenced by the refractory quality of the epilepsy or by age. Li found that both age and seizure frequency increased the risk of sleep apnea [21]. Maurousset also found that patients with late-onset epilepsy have a higher incidence of obstructive sleep apnea [22]. Although we have yet to clearly delineate the range of symptoms and the usefulness of our screening tools, these studies suggest that patients with recurrent seizures deserve further questioning regarding the possibility of sleep apnea (Table 2).
Circadian Rhythm in Epilepsy
A relatively growing area of interest is the influence of circadian rhythms in epilepsy. As a marker of circadian rhythms, Choi reported that sleep-wake patterns in patients with epilepsy are not much different from healthy control groups [23]. Although sleep-wake patterns may not be very different, another controlled study in patients with late-onset focal upset epilepsy found that patients with epilepsy were likely to be morning oriented even though this was not reflected in their dim light melatonin onset. The investigators speculated that lifestyle choices including a regular sleep schedule and an early bedtime, may induce a morning orientation and perception of being morning oriented [24].
The circadian influence may go beyond traditional circadian biomarkers. Spencer et al. conducted a retrospective review of 134 patients with RNS and found that epileptiform activity showed a strong circadian pattern irrespective of the location of the ictal-onset zone [25]. The study also agreed with prior studies of scalp EEG that mesial temporal epilepsy showed a diurnal pattern. Non-limbic areas with long episodes of epileptiform activity appear in a monophasic nocturnally prevalent daily rhythm. The timing of peak seizure occurrence varied according to this study. Mesial temporal patients were widely distributed with timing of events split evenly during the day. The temporal neocortical and frontal lobe groups showed peak seizure occurrences confined to the 00:00–05:00 timeframe. This study was limited to patients with focal epilepsy and the study did not have enough patients for analysis of occipital or parietal lobe epilepsies [25]. This study suggests that some epileptic discharges are under circadian influence and would add support to treating the epilepsy using a differential dosing plan to improve the seizure control and improve sleep quality.
Pathophysiology of Epilepsy in Sleep
Much of the pathophysiology research in sleep are in animal models. Rocha et al. used a rat model for pilocarpine-induced status epilepticus (SE). This group found an increase in melatonin (MT1 and MT2) receptors within a couple of hours after a seizure. There was a loss of these receptors in the chronic phase after SE which may in part explain some of the sleep disruption in epilepsy patients following large seizures [26]. This study gives clues as to the variable response to melatonin.
REM sleep has long been viewed to have anti-seizure properties and this has raised questions to the role substances that control REM sleep may play in epilepsy. In examining orexin, a neurotransmitter that influences REM sleep, Roundtree found Kcna1-null mice have an increased number of orexin-positive neurons compared to wild type which correlated to increased latency to REM sleep onset and blocking orexin binding with almorexant (a dual orexin receptor antagonist) reduced the seizure incidence and overall seizure burden. Also, a significant correlation between latency to REM onset and seizure burden was found [27].
The Effect of Epilepsy on Sleep
The long-term consequences of interictal discharges are far from being elucidated. The model of benign childhood epilepsy with centrotemporal spikes has long been debated as to their benign nature. The frequent interictal discharges in sleep make this disorder a classic to elucidate the effect of nocturnal discharges on brain function. One retrospective study noted no difference on cognition in those with > 50% spike wave index (SWI). However, there was a fine motor task deficit with more abundant spikes in sleep. Several limitations are noted by the authors including lack of overnight EEG data, exclusion of children with intellectual disability or autism, and an arbitrary dichotomy instead of a continuous variable for SWI [28]. However, a prospective study conducted by Galer et al. recruited patients with benign childhood epilepsy (n = 12) with centrotemporal spikes with no intellectual disability or other idiopathic focal epilepsies (n = 3) with no intellectual disability. Six of the 15 total patients were on valproate therapy. Patients were tested on non-verbal (2D object location task) and verbal declarative memory (word-pair learning task). The study was ultimately only able to include 9 patients with 8 age-matched controls for the non-verbal task. During regression analysis, only the non-verbal memory task showed significant effect of SWI on poorer memory score which represents a decrease from immediate to delayed recall performance. The EEG grade was excluded during the Spearman correlation analysis given a positive correlation between SWI and EEG grade. Although the neurophysiological processes involved in memory consolidation are still elusive, this study suggests that idiopathic focal epilepsy disrupts sleep-related memory consolidation processes [29].
Ictal and interictal discharges appear to influence the homeostatic drive of sleep. Boly et al. showed in an elegant series of experiments that daytime seizures and frequent daytime interictal discharges increase the drive for slow-wave sleep at night. Similarly, nighttime interictal discharges disrupted the slow-wave sleep and had a resulting deficit in daytime functioning [30••]. This in combination with the finding of synaptic pruning during sleep offers new insights into the role slow-wave sleep and the homeostatic mechanism may play in dendritic simplification and kindling. These studies also offer insight as to the potential sleep-related therapeutic targets to modulate epilepsy and the possible downstream effects of the process.
Nocturnal Seizures: Sleep-Related Hypermotor Epilepsy
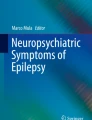
Although nocturnal seizures are noted in the differential of nocturnal events in the revised International League Against Epilepsy classification system, more recent guidelines are published outlining the newly defined sleep-related hypermotor epilepsy (SHE) (Table 3) [31]. This grouping includes epilepsies formally known as nocturnal frontal lobe epilepsy and autosomal dominant nocturnal frontal lobe epilepsy. The name change was prompted by the identification of cases showing the same semiology but emanating from foci outside the frontal lobes. SHE has an estimated minimum prevalence of 1.8 per 100,000 individuals and is characterized by “vigorous hyperkinetic features (complex body movements with kicking or cycling of limbs and rocking body movements), usually with vegetative signs, vocalization, and emotional facial expression” [31]. These events can be asymmetric tonic/dystonic seizures with or without head/eye deviation. Seizures are mostly during sleep and primarily in non-REM sleep. Video EEG may not demonstrate a clear epileptiform discharge, making the distinction from arousal parasomnias reliant upon the stereotypic semiology (Table 3 and Fig. 1) [31, 32]. Minor motor events are described in patients with SHE and they remain controversial as to whether they represent epileptic seizures [33]. These movements were mostly oroalimentary automatism, limb dystonia, straightening movements, and gestural automatisms [33]. Patients appear more likely to respond to carbamazepine; however, a significant portion remain intractable [34]. Two groups (Mangiardi, Samarasekera) found lacosamide to improve sleep and reduce seizures for patients who failed traditional medications such as carbamazepine or lamotrigine [35, 36]. However, some patients may benefit from surgical resection [34].

a The seconds up to and the start of a sleep-related hypermotor seizure. Note the EEG demonstrates a subtle isolated rhythm in the left frontal region, the start designated by arrow and the rhythm by the solid line. Many times these events do not show a clear epileptiform change on EEG as demonstrated in the same patient’s second event shown in b. Note the muscle artifact on the right of the tracing but no clear EEG change prior to the muscle activity. Both events were behaviorally stereotypic. The line intervals are 1 s
Sudden Unexplained Death in Epilepsy and Sleep
Sudden unexplained death in epilepsy (SUDEP) is the leading cause of premature death in patients with epilepsy, and has long been known to occur more frequently at night. The Mortality in Epilepsy Monitoring Units Study (MORTEMUS) classified 16 reported cases of SUDEP and 9 cases of near SUDEP, with all assessable cases demonstrating a seizure immediately before the cardiorespiratory arrest [37]. Seventeen of these events occurred at night. Although the reason of the nocturnal predominance is unclear, Latreille found that nocturnal seizures were associated with more severe hypoxemia and generalized suppression of the EEG [38]. This raises the issue whether sleep apnea could play a role. Two small pilot studies, both (n = 35) using different methods to assess sleep apnea but both assessing SUDEP clinical risk using the SUDEP-7, suggest a higher rate of sleep apnea correlated with a higher clinical risk of SUDEP [39, 40]. The difficulty with these types of studies is that several of the risk factors for SUDEP inherently are risks for great sleep apnea and sleep disruption. Thus, the tool more likely points toward commonalities of intractable epilepsy as opposed to true risk drivers. Overall, the high prevalence of SUDEP events at night needs much further research to determine how sleep or the circadian rhythm may influence the events.
Treatment of Sleep Disorders in Epilepsy
As avoidance of sleep deprivation has long been recommended to patients with epilepsy, the treatment of sleep disorders offers an opportunity to reduce recurrent seizures. This is most notable in the realm of obstructive sleep apnea in patients with epilepsy. Several recent works support the growing body of evidence that reduction of sleep apnea can improve epilepsy markers, such as seizure frequency and interictal discharges. Lin’s 2017 meta-analysis of three studies of the treatment of obstructive sleep apnea in patients with epilepsy suggested a high odds ratio (5.26 OR) of improvement in seizure frequency with therapy [20•]. Looking at the night time effect, Pornsriniyom found that CPAP therapy reduces the interictal discharges in wake and sleep. Further examination showed an interesting pattern that the reduction of interictal discharges was in NREM sleep but not REM sleep [41]. This finding suggests that although the interictal discharges in REM sleep are less common, they do not appear to be influenced by the disruption created by OSA. This raises some interesting parallels with the effect of the homeostatic drive on interictal discharges in NREM sleep but not REM sleep. CPAP therapy is the most common therapy for OSA. However, Latreille reported in their experience in 23 patients with epilepsy receiving CPAP therapy showing lower adherence to therapy and more likely to have residual apneas despite therapy [42]. This study emphasizes the need for closer follow-up for these patients. In a case report, Shirani reports an individual who became seizure free after uvulopalatoplasty for OSA; however, little research has included alternative forms of therapies for OSA [43]. Overall, the preponderance of evidence continues to support the hypothesis that treatment of sleep apnea can improve seizure control in some patients.
Insomnia is a common feature in epilepsy but little research focuses on the therapy of insomnia in patients with epilepsy. Two studies shed some light in this area. Jain reported that in children sustained release melatonin reduced sleep latency and wake after sleep onset but did not decrease the seizure frequency [44]. This small study adds to the debate regarding if melatonin can improve sleep and seizure frequency in this population. A new treatment for insomnia, low frequency repetitive transcranial magnetic stimulation, acutely improved length and continuity of sleep and quality of life in patients with focal epilepsy [45]. This study did not include any data regarding seizure frequency nor longer-term sleep measures following therapy, and raises the need for more studies examining therapies of insomnia in epilepsy.
Treatment of Epilepsy on Sleep
As epilepsy may cause disruption of sleep, attention is needed on the influence the treatments of epilepsy may have on sleep (Table 4). Earlier works suggest that anticonvulsants have a direct effect on the mechanisms of sleep and some of these compounds may decrease epileptic discharges resulting in improved sleep. Several key elements of the effect of the treatment of epilepsy on sleep are revealed in recent publications. A review by Jain showed that nearly all therapies for epilepsy have some effect on subjective and objective sleep parameters. They concluded that gabapentin, tiagabine, pregabalin, clobazam, and carbamazepine improved sleep efficiency and/or reduce sleep latency and phenobarbital, valproic acid, and higher-dose levetiracetam aggravate daytime sleepiness [46]. In primary investigation, Toledo reported perampanel has little effect on subjective sleep issues (using the Pittsburgh Sleep Quality Index (PSQI) and Epworth Sleepiness Scale (ESS)) but no objective measures of sleep were obtained [47]. Foldvary examined lacosamide at 200 mg/day and 400 mg/day using subjective and objective measures of sleepiness and found no significant difference between placebo and controls. The authors also examined polysomnography findings with only minor differences in sleep architecture [48].
For non-pharmacological therapies, Jain’s (2014) showed these therapies likewise influence sleep. Ketogenic diet increased mildly the degree of slow-wave sleep and epilepsy surgery only improved nocturnal sleep in a subgroup of patients with improved seizure frequency. However, not all non-pharmacological therapies improve sleep [46]. Vagus nerve stimulation may reduce daytime sleepiness, but can cause stimulation-related hypopneas [49]. These hypopneas typically do not appear to improve with positive airway pressure but are abated with reducing stimulation intensity. Similarly, Voges found that deep brain stimulation of anterior nucleus thalami causes more arousals and fragments sleep in patients with epilepsy [50]. These non-pharmacological therapies raise important avenues to question their effects on sleep, given they may directly disrupt the epileptic focus or have significant downstream influences on the sleep mechanisms. Similarly, research is needed to investigate if those patients who are not responding to these therapies are incurring great sleep disruption than those benefiting from seizure reduction.
The finding of improvement in select cases with epilepsy surgery also supports the hypothesis that diminishing the disrupting output from the seizure focus may improve sleep. Other evidence that this may be at work exists in studies of primary generalized epilepsies. Sleep architecture was also found to improve with treatment in both juvenile myoclonic epilepsy (JME) and childhood absence epilepsy. Three independent groups (Mekky, Roshan, and Nayak) found valproate to decrease nocturnal discharges, improve sleep continuity, and reduce arousals in subjects with JME [51,52,53]. Likewise, Dinopoulos found that children who responded medication (valproate, ethosuximide or lamotrigine monotherapy or in combination), compared to their drug-naive state, had significant reduction in arousals and epileptic discharges, compared to those who did not respond to medication [54]. These studies suggest that by reducing the epileptic discharges also may improve sleep architecture, at least in primary generalized epilepsies.
Additionally, identifying chronotype may aid in treating epilepsy and identify individuals vulnerable to side effects of medication. Taneja examined the prevalence of mood issues in individuals taking levetiracetam based upon their subjective chronotype [55]. The author found that individuals with morning chronotype were more likely to have mood issues with the medication than those with intermediate or evening chronotypes. In their sample of 110 adults, no subjects with self-report of evening chronotype developed mood issues with levetiracetam, and that depression, as measured by the Beck Depression Inventory-II, did not correlate with the drug-induced mood issues [55]. This raises a new area of inquiry to use the chronotype as a mechanism to predict medication side effects.
Conclusion
The relationship between sleep and epilepsy continues to be complex and bidirectional (Fig. 2). Research into different models has yielded some interesting findings regarding how sleep influences epilepsy ultimately revealing possible avenues for treatment in patients with epilepsy. Sleep issues remain a significant quality of life issue for patients and deserve attention and screening during routine clinic visits. Improved seizure monitoring has enabled researchers to study the chronotype of certain epilepsies providing us a possible way to treat epilepsy more effectively with differential dosing. Testing epilepsy therapies using a sleep model has given us new insights into identifying which patients may experience side effects. Perhaps one of the most influential developments is a study investigating the effect of ictal and interictal discharges on sleep-related physiology and subsequent downstream outcomes such as learning and memory. This work also gives a new insight into synaptic pruning and the kindling model for epilepsy. Sleep remains an important marker for epilepsy patients and offers an opportunity to further understand the pathophysiological mechanisms that drive our daytime and nighttime sequela of epilepsy as well as potential for novel biomarkers and therapeutic targets to improve the lives of our patients.

This figure demonstrates the complex interaction of epileptic seizures, their treatment, and sleep disturbance
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Jain SV, Kothare SV. Sleep and epilepsy. Semin Pediatr Neurol. 2015;22(2):86–92. https://doi.org/10.1016/j.spen.2015.03.005.
Kataria L, Vaughn BV. Sleep and epilepsy. Sleep Med Clin. 2016;11(1):25–38. https://doi.org/10.1016/j.jsmc.2015.10.008.
Samsonsen C, Sand T, Bråthen G, Helde G, Brodtkorb E. The impact of sleep loss on the facilitation of seizures: a prospective case-crossover study. Epilepsy Res. 2016;127:260–6. https://doi.org/10.1016/j.eplepsyres.2016.09.014.
Ferlisi M, Shorvon S. Seizure precipitants (triggering factors) in patients with epilepsy. Epilepsy Behav. 2014;33:101–5. https://doi.org/10.1016/j.yebeh.2014.02.019.
Ismayilova V, Demir AU, Tezer FI. Subjective sleep disturbance in epilepsy patients at an outpatient clinic: a questionnaire-based study on prevalence. Epilepsy Res. 2015;115:119–25. https://doi.org/10.1016/j.eplepsyres.2015.06.009.
Staniszewska A, Mąka A, Religioni U, Olejniczak D. Sleep disturbances among patients with epilepsy. Neuropsychiatr Dis Treat. 2017;13:1797–803. https://doi.org/10.2147/NDT.S136868.
Yazdi Z, Sadeghniiat-Haghighi K, Naimian S, Zohal MA, Ghaniri M. Prevalence of sleep disorders and their effects on sleep quality in epileptic patients. Basic Clin Neurosci. 2013;4(1):36–41.
Im HJ, Park SH, Baek SH, Chu MK, Yang KI, Kim WJ, et al. Associations of impaired sleep quality, insomnia, and sleepiness with epilepsy: a questionnaire-based case-control study. Epilepsy Behav. 2016;57(Pt A):55–9. https://doi.org/10.1016/j.yebeh.2016.01.022.
Quigg M, Gharai S, Ruland J, Schroeder C, Hodges M, Ingersoll KS, et al. Insomnia in epilepsy is associated with continuing seizures and worse quality of life. Epilepsy Res. 2016;122:91–6. https://doi.org/10.1016/j.eplepsyres.2016.02.014.
Vendrame M, Yang B, Jackson S, Auerbach SH. Insomnia and epilepsy: a questionnaire-based study. J Clin Sleep Med. 2013;9(02):141–6. https://doi.org/10.5664/jcsm.2410.
Oliveria P, Oliveria PS, Foldvary-Schaefer N, Gomes M. Insomnia in people with epilepsy. Epilepsy Res. 2017;135:158–67. https://doi.org/10.1016/j.eplepsyres.2017.05.014.
Yang KI, Grigg-Damberger M, Andrews N, O’Rourke C, Bena J, Foldvary-Schaefer N. Severity of self-reported insomnia in adults with epilepsy is related to comorbid medical disorders and depressive symptoms. Epilepsy Behav. 2016;60:27–32. https://doi.org/10.1016/j.yebeh.2016.03.023.
Shen Y, Zhang M, Wang Y, Wang L, Xu X, Xiao G, et al. Subjective sleep disturbance in Chinese adults with epilepsy: associations with affective symptoms. Epilepsy Res. 2017;135:150–7. https://doi.org/10.1016/j.eplepsyres.2017.06.014.
Saraswati N, Nayak C, Sinha S, Nagappa M, Thennarasu K, Taly AB. Comparing sleep profiles between patients with juvenile myoclonic epilepsy and symptomatic partial epilepsy: sleep questionnaire-based study. Epilepsy Behav. 2017;66:34–8. https://doi.org/10.1016/j.yebeh.2016.10.009.
Hansen BH, Alfstad KÅ, van Roy B, Henning O, Lossius MI. Sleep problems in children and adolescents with epilepsy: associations with psychiatric comorbidity. Epilepsy Behav. 2016;62:14–9. https://doi.org/10.1016/j.yebeh.2016.06.015.
• Rizou I, De Gucht V, Papavasiliou A, Maes S. The contribution of illness perceptions to fatigue and sleep problems in youngsters with epilepsy. Eur J Paediatr Neurol. 2016;20(1):93–9. https://doi.org/10.1016/j.ejpn.2015.10.001. One of the few studies looking at illness perception in children with epilepsy.
•• Tsai SY, Lee WT, Lee CC, Jeng SF, Weng WC. Sleep in children with epilepsy: the role of maternal knowledge of childhood sleep. Sleep. 2018. https://doi.org/10.1093/sleep/zsy157. First study to look at parental knowledge about sleep in children with epilepsy.
Nguyen-Michel VH, Pallanca O, Navarro V, Dupont S, Baulac M, Claude A. How are epileptic events linked to obstructive sleep apneas in epilepsy? Seizure. 2015;24:121–3. https://doi.org/10.1016/j.seizure.2014.09.004.
Sharma A, Molano J, Moseley BD. The STOP-BANG questionnaire improves the detection of epilepsy patients at risk for obstructive sleep apnea. Epilepsy Res. 2017;129:37–40. https://doi.org/10.1016/j.eplepsyres.2016.11.009.
• Lin Z, Si Q, Xiaoyi Z. Obstructive sleep apnoea in patients with epilepsy: a meta-analysis. Sleep Breath. 2017;21(2):263–70. https://doi.org/10.1007/s11325-016-1391-3. This meta-analysis provides further insight into improving seizure frequency with OSA therapy.
Li P, Ghadersohi S, Jafari B, Teter B, Sazgar M. Characteristics of refractory vs. medically controlled epilepsy patients with obstructive sleep apnea and their response to CPAP treatment. Seizure. 2012;21(9):717–21. https://doi.org/10.1016/j.seizure.2012.07.016.
Maurousset A, De Toffol B, Praline J, Biberon J, Limousin N. High incidence of obstructive sleep apnea syndrome in patients with late-onset epilepsy. Neurophysiol Clin. 2017;47(1):55–61. https://doi.org/10.1016/j.neucli.2016.11.002.
Choi SJ, Joo EY, Hong SB. Sleep-wake pattern, chronotype and seizures in patients with epilepsy. Epilepsy Res. 2016;120:19–24. https://doi.org/10.1016/j.eplepsyres.2015.11.010.
Manni R, Cremascoli R, De Icco R, Terzaghi M. Chronotype in patients with epilepsy: a controlled study in 60 subjects with late-onset focal epilepsy. Epilepsy Behav. 2015;50:1–6. https://doi.org/10.1016/j.yebeh.2015.05.031.
Spencer DC, Sun FT, Brown SN, Jobst BC, Fountain NB, Wong VS, et al. Circadian and ultradian patterns of epileptiform discharges differ by seizure-onset location during long-term ambulatory intracranial monitoring. Epilepsia. 2016;57(9):1495–502. https://doi.org/10.1111/epi.13455.
Rocha AKAA, de Lima E, Amaral F, Peres R, Cipolla-Neto J, Amado D. Altered MT1 and MT2 melatonin receptors expression in the hippocampus of pilocarpine-induced epileptic rats. Epilepsy Behav. 2017;71(Pt A):23–34. https://doi.org/10.1016/j.yebeh.2017.01.020.
Roundtree HM, Simeone TA, Johnson C, Matthews SA, Samson KK, Simeone KA. Orexin receptor antagonism improves sleep and reduces seizures in Kcna1-null mice. Sleep. 2016;39(2):357–68. https://doi.org/10.5665/sleep.5444.
Nissenkorn A, Pappo A, Feldmann Y, Heimer G, Bar-Yosef O, Tzadok M, et al. Influence of epileptic activity during sleep on cognitive performance in benign childhood epilepsy with centrotemporal spikes. Eur J Paediatr Neurol. 2017;21(6):858–63. https://doi.org/10.1016/j.ejpn.2017.07.001.
Galer S, Urbain C, De Tiège X, Emeriau M, Leproult R, Deliens G, et al. Impaired sleep-related consolidation of declarative memories in idiopathic focal epilepsies of childhood. Epilepsy Behav. 2015;43:16–23. https://doi.org/10.1016/j.yebeh.2014.11.032.
•• Boly M, Jones B, Findlay G, Plumley E, Mensen A, Hermann A, et al. Altered sleep homeostasis correlates with cognitive impairment in patients with focal epilepsy. Brain. 2017;140(4):1026–40. https://doi.org/10.1093/brain/awx017. This study associates epileptiform discharges during slow-wave sleep with decreased learning and memory.
Tinuper P, Bisulli F, Cross JH, Hesdorffer D, Kahane P, Nobili L, et al. Definition and diagnostic criteria of sleep-related hypermotor epilepsy. Neurology. 2016;86(19):1834–42. https://doi.org/10.1212/WNL.0000000000002666.
Vignatelli L, Bisulli F, Giovannini G, Licchetta L, Naldi I, Mostacci B, et al. Prevalence of nocturnal frontal lobe epilepsy in the adult population of Bologna and Modena, Emilia-Romagna region, Italy. Sleep. 2015;38(3):479–85. https://doi.org/10.5665/sleep.4514.
Giuliano L, Uccello D, Fatuzzo D, Mainieri G, Zappia M, Sofia V. Electroclinical findings of minor motor events during sleep in temporal lobe epilepsy. Epilepsia. 2017;58(7):1261–7. https://doi.org/10.1111/epi.13770.
Veronica M, Bisulli F, Tinuper P, Nobili L. Sleep-related hypermotor epilepsy: prevalence, impact and management strategies. Nat Sci Sleep. 2018;10:317–26. https://doi.org/10.2147/NSS.S152624.
Mangiardi M, Alfano G. A clinical efficacy experience of Lacosamide on sleep quality in patients with Nocturnal Frontal Lobe Epilepsy (NFLE). Acta Biomed. 2018;89(3):397–9. https://doi.org/10.23750/abm.v89i3.6956.
Samarasekera SR, Berkovic SF, Scheffer IE. A case series of lacosamide as adjunctive therapy in refractory sleep-related hypermotor epilepsy (previously nocturnal frontal lobe epilepsy). J Sleep Res. 2018;27(5):e12669. https://doi.org/10.1111/jsr.12669.
Ryvlin P, Nashef L, Lhatoo SD, Bateman LM, Bird J, Bleasel A. Incidence and mechanisms of cardiorespiratory arrests in epilepsy monitoring units (MORTEMUS): a retrospective study. Lancet Neurol. 2013;12(10):966–77. https://doi.org/10.1016/S1474-4422(13)70214-X.
Latreille V, Abdennadher M, Dworetzky BA, Ramel J, White D, Katz E, et al. Nocturnal seizures are associated with more severe hypoxemia and increased risk of postictal generalized EEG suppression. Epilepsia. 2017;58(9):e127–31. https://doi.org/10.1111/epi.13841.
McCarter AR, Timm PC, Shepard PW, Sandness DJ, Luu T, McCarter SJ, et al. Obstructive sleep apnea in refractory epilepsy: a pilot study investigating frequency, clinical features, and association with risk of sudden unexpected death in epilepsy. Epilepsia. 2018;59(10):1973–81. https://doi.org/10.1111/epi.14548.
Billakota S, Odom N, Westwood AJ, Hanna E, Pack A, Bateman LM. Sleep disordered breathing, neuroendocrine function and clinical SUDEP risk in patients with epilepsy. Epilepsy Behav. 2018;87:78–82. https://doi.org/10.1016/j.yebeh.2018.07.011.
Pornsriniyom D, Shinlapawittayatorn K, Fong J, Andrews ND, Foldvary-Schaefer N. Continuous positive airway pressure therapy for obstructive sleep apnea reduces interictal epileptiform discharges in adults with epilepsy. Epilepsy Behav. 2014;37:171–4. https://doi.org/10.1016/j.yebeh.2014.06.025.
Latreille V, Bubrick EJ, Pavlova M. Positive airway pressure therapy is challenging for patients with epilepsy. J Clin Sleep Med. 2018;14(7):1153–9. https://doi.org/10.5664/jcsm.7214.
Shirani G, Arshad M, Mahmoudi X, Azarians S. Effect of treatment of obstructive sleep apnea by uvulopalatoplasty on seizure outcomes: a case report. J Dent (Tehran). 2017;14(6):361–5.
Jain SV, Horn PS, Simakajornboon N, Beebe DW, Holland K, Byars AW, et al. Melatonin improves sleep in children with epilepsy: a randomized, double-blind, crossover study. Sleep Med. 2015;16(5):637–44. https://doi.org/10.1016/j.sleep.2015.01.005.
Sánchez-Escandón O, Arana-Lechuga Y, Terán-Pérez G, Ruiz-Chow A, González-Robles R, Shkurovich-Bialik P, et al. Effect of low-frequency repetitive transcranial magnetic stimulation on sleep pattern and quality of life in patients with focal epilepsy. Sleep Med. 2016;20:37–40. https://doi.org/10.1016/j.sleep.2015.11.022.
Jain SV, Glauser TA. Effects of epilepsy treatments on sleep architecture and daytime sleepiness: an evidence-based review of objective sleep metrics. Epilepsia. 2014;55(1):26–37. https://doi.org/10.1111/epi.12478.
Toledo M, Gonzalez-Cuevas M, Miró-Lladó J, Molins-Albanell A, Falip M, Martinez AB, et al. Sleep quality and daytime sleepiness in patients treated with adjunctive perampanel for focal seizures. Epilepsy Behav. 2016;63:57–62. https://doi.org/10.1016/j.yebeh.2016.08.004.
Foldvary-Schaefer N, Neme-Mercante S, Andrews N, Bruton M, Wang L, Morrison S, et al. Wake up to sleep: the effects of lacosamide on daytime sleepiness in adults with epilepsy. Epilepsy Behav. 2017;75:176–82. https://doi.org/10.1016/j.yebeh.2017.08.002.
Salvadé A, Ryvlin P, Rossetti AO. Impact of vagus nerve stimulation on sleep-related breathing disorders in adults with epilepsy. Epilepsy Behav. 2018;79:126–9. https://doi.org/10.1016/j.yebeh.2017.10.040.
Voges BR, Schmitt FC, Hamel W, House PM, Kluge C, Moll CK, et al. Deep brain stimulation of anterior nucleus thalami disrupts sleep in epilepsy patients. Epilepsia. 2015;56(8):e99–e103. https://doi.org/10.1111/epi.13045.
Mekky JF, Elbhrawy SM, Boraey MF, Omar HM. Sleep architecture in patients with Juvenile Myoclonic Epilepsy. Sleep Med. 2017;38:116–21. https://doi.org/10.1016/j.sleep.2017.02.013.
Roshan S, Puri V, Chaudhry N, Gupta A, Rabi SK. Sleep abnormalities in juvenile myoclonic epilepsy-a sleep questionnaire and polysomnography based study. Seizure. 2017;50:194–201. https://doi.org/10.1016/j.seizure.2017.06.021.
Nayak CS, Sinha S, Nagappa M, Kandavel T, Taly AB. Effect of valproate on the sleep microstructure of juvenile myoclonic epilepsy patients - a cross-sectional CAP based study. Sleep Med. 2016;17:129–33. https://doi.org/10.1016/j.sleep.2015.11.006.
Dinopoulos A, Tsirouda MA, Bonakis A, Pons R, Pavlopoulou ID, Tsoumakas K. Sleep architecture and epileptic characteristics of drug naïve patients in childhood absence epilepsy spectrum. A prospective study. Seizure. 2018;59:99–107. https://doi.org/10.1016/j.seizure.2018.04.021.
Taneja R, Hunter K, Burakgazi-Dalkilic E, Carran M. Effect of sleep patterns on levetiracetam induced mood changes. Epilepsy Behav. 2017;75:237–40. https://doi.org/10.1016/j.yebeh.2017.07.038.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Ethan S. Yun and Bradley V. Vaughn each declare no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Sleep and Neurological Conditions
Rights and permissions
About this article

Cite this article
Yun, E.S., Vaughn, B.V. The Interface Between Sleep and Epilepsy. Curr Sleep Medicine Rep 5, 61–70 (2019). https://doi.org/10.1007/s40675-019-00139-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40675-019-00139-w