
Abstract
Purpose of Review
Myofibroblasts represent matrix-producing effector cells which both produce and maintain the pro-fibrotic microenvironment in scleroderma and other fibrotic diseases. This review first explores the origins, function, regulators, interactions, and death of myofibroblasts in fibrotic tissue and then utilizes this information to guide understanding of current and future treatments which may target these cells.
Recent Findings.
Beyond existing immunomodulatory therapy for SSc, there are an increasing number of anti-fibrotic therapies which are either under clinical study or development which may be able to effectively target myofibroblasts.
Summary
The role of myofibroblast modulation in treatment of scleroderma is a promising field with data supporting multiple new agents which may modulate myofibroblasts as anti-fibrotic therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Systemic sclerosis (SSc, scleroderma) is a complex disease with a pathogenic triad of autoimmunity, vasculopathy, and fibrosis which can involve the skin and multiple internal organs [1•]. Fibrosis, a destructive scarring process, is the hallmark of SSc and frequently causes significant organ dysfunction and can lead to both disability and death [2]. Fibrosis is mediated by a variety of cellular and molecular processes, but the myofibroblast represents the cell which both promotes and maintains the fibrotic micro-environment and therefore is a critical mediator of SSc disease course and understanding and targeting the myofibroblast in SSc is a critical undertaking [3, 4••]. This review will focus on understanding myofibroblast biology with an emphasis on SSc disease relevance and emerging data on how current and future therapies may target these critical cells.
Myofibroblasts: definition, structure, origins, function
Myofibroblasts were first described in 1971 [5] as cells in wound beds having both the secretory features of fibroblasts and the contractile features of smooth muscle cells. Additional key factors defining these cells include their having a greater rate of extracellular matrix (ECM) secretion than fibroblasts, expression of alpha smooth muscle actin (ASMA), resistance to apoptosis, and constitutive expression of a variety of cytokines, chemokines, and cell surface receptors [6•].
The contractile properties of myofibroblasts come from their expression of microfilaments and particularly those expressing ASMA [7]. Normal wound healing probably represents the best evolutionarily defined myofibroblast function. In animal models of wound healing, ASMA expression is absent for up to 4 days after wound formation, increases from days 6 to 15, and then dissipates completely by day 30 [8]. During this process, fibroblasts in the wound bed undergo a two-stage differentiation. Two to 4 days after wound initiation, under mechanical stress, fibroblasts transition to intermediate proto-myofibroblasts which begin to express contractile cytoplasmic stress fibers which terminate in focal adhesion complexes [9]. A combination of mechanical and biochemical stresses promotes the differentiation of proto-myofibroblasts into myofibroblasts which then form more developed stress fibers and express ASMA and have organized fibronectin fibrils which allow them to generate greater contractile force, particularly via integrin-mediated focal adhesions and cadherin-mediated adherens junctions in which their actin cytoskeleton is anchored to the surrounding ECM [10].
Along with their contractile properties, myofibroblasts also produce extracellular matrix proteins including collagens I and III, and fibronectin [4••]. The organization of fibronectin (particularly the EDA isoform) is particularly important in promoting matrix stiffness [11]. Once activated, myofibroblasts also become very active secretory cells and produce cytokines like TGF-b, vascular endothelial growth factor (VEGF), endothelin-1, connective tissue growth factor (CTGF), MCP-1, IL-1, IL-6, IL-8, all of which help in promoting the wound healing process [6•].
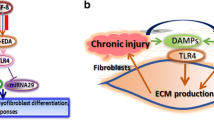
The origins of myofibroblasts are diverse and there is still controversy about the origins of some myofibroblasts [12]. As described earlier, the main source of myofibroblasts is tissue-resident fibroblasts which differentiate in response to pro-fibrotic stimuli. Other sources include pericytes [13], bone marrow–derived mesenchymal stem cells termed fibrocytes [14], adipocytes [15•], and epithelial and endothelial cells which may undergo epithelial-mesenchymal transition (EMT) [16•] and endothelial-mesenchymal transition (EndoMT) [17] respectively (Fig. 1).

source of myofibroblasts is tissue-resident fibroblasts which are activated to become proto-myofibroblasts and eventually evolve to a more contractile phenotype as myofibroblasts. Other sources of myofibroblasts include epithelial cells via epithelial-mesenchymal transition (EMT), endothelial cells via endothelial mesenchymal transition (EndoMT), adipocytes via adipocyte mesenchymal transition (AMT), and pericytes. Myofibroblasts produce and are associated with extracellular matrix (ECM, fibrillar lattice-like structure) and ECM interacts with proteins including integrins and TGF-β to lead to intracellular Rho/ROCK signaling and activation of the TGF-β/SMAD pathway. Other relevant intracellular pathways include the Wnt, YAP/TAZ, and PDGFR/AKT pathways. IL-6 and IL-4/13 represent key profibrotic cytokines which signal through JAK/STAT pathways to activate myofibroblasts. Figure made with Biorender
Myofibroblast origins and pathway activation during fibrosis. The primary
Pericytes play a central role in microvascular integrity and function, both regulating and being regulated by the endothelial cell. Pathologic changes in the endothelium can likely have profound influences on pericyte phenotype and function. It was shown that in the early stages of SSc, pericytes become activated and express PDGF receptors [18]. While direct lineage tracing studies have not been performed in skin as they have in kidney where it has been shown that pericytes give rise to myofibroblasts [19], the shared expression of surface markers between these cells in SSc has led to the suggestion that pericytes are a progenitor which transdifferentiate into myofibroblasts in SSc [13]. Another cell type which can give rise to myofibroblasts is the fibrocyte. Fibrocytes are a circulating cells of myeloid origin that rapidly invade wounds and, in contrast to other myeloid cells, produce ECM molecules [20]. After arrival, they are able to differentiate into a myofibroblast-like phenotype under the influence of factors including TGF-β. While many authors have described these cells as being important in wound healing and fibrosis, their relevance in vivo remains controversial [21]. In addition to the aforementioned cells, adipocytes are another potential source of myofibroblasts. Adipocyte mesenchymal transition, which we first described during skin fibrosis [15•], has now been described in a variety of fibrotic contexts [22] (Fig. 2).

Existing and emerging targets for myofibroblast-directed therapy. In addition to existing therapies which target cytokines such as IL-6, newer anti-fibrotic compounds such as nintedanib represent multi-potent growth factor inhibitors. In addition to these classes, emerging therapies are poised to target the myofibroblast by inducing apoptosis and phagocytosis, as well as blocking intracellular signaling. Figure made with Biorender
EMT is well described in lung fibrosis [23]. In this process, myofibroblasts arise when epithelial cells lose their intercellular adhesion molecules including E-cadherin and cytokeratin and differentiate into a mesenchymal phenotype with fibrogenic potential [24]. Repression of E-cadherin leads to the loss of the typical polygonal morphology of epithelial cells and causes them to acquire a spindle-shaped mesenchymal morphology and express markers that are associated with the mesenchymal cell state, including N-cadherin, vimentin, and fibronectin [16•]. EMT is regulated by EMT-inducing transcription factors (EMT-TFs), which induce gene expression to promote the mesenchymal cell state while repressing the epithelial state [25]. EndoMT is a similar trans-differentiation process in which endothelial cells lose the ability to express their phenotypic markers as well as their morphology and express mesenchymal cell markers [26], and has been better described in SSc [27,28,29].
Regulation of myofibroblast activation
Once formed, myofibroblast function is influenced by a variety of cellular, biochemical, and mechanical cues. Cellular interactions include direct interactions with endothelial cells, macrophages, lymphocytes, and epithelial cells which may activate or suppress matrix formation based on their context. This section will focus on biochemical factors which include paracrine and autocrine cytokines/chemokines/growth factors which can either promote or inhibit myofibroblast differentiation and activity.
Myofibroblast-inducing factors
Among the most important pro-fibrotic secreted factors include TGF-β, endothelin-1, connective tissue growth factor (CTGF), platelet-derived growth factor (PDGF), IL-6, IL-4, and IL-13 [4••].
TGF-β is the prototypic and probably most influential growth factor in its ability to induce myofibroblast differentiation [30]. There are three isoforms of TGF-β, and while all have effects of fibrotic processes, the TGF-β1 isoform has been most closely associated with fibrosis [31]. TGF-β1 is usually bound to latency-associated protein (LAP) which keeps it inactive. By binding cytokines [32] or myofibroblast contraction [33], LAP dissociates and TGF-β becomes active such that signal passes through the membrane and phosphorylates the intracellular SMAD2/3 proteins which subsequently enables transcription of pro-fibrotic genes. TGF-β’s role in fibrosis, SSc, and the myofibroblast phenotype is extensive and has been reviewed elsewhere [34, 35•].
Beyond TGF-β, developmental pathways like the Wnt/ β-catenin pathway are upregulated in fibrotic tissue and have found to promote fibroblast proliferation and myofibroblast differentiation through both TGF-dependent and TGF-independent mechanisms[36,37,38]. Other pathways like Hedgehog [39, 40] and Notch [40, 41] are also found to be over-expressed in systemic sclerosis fibroblasts and are thought to contribute to the myofibroblast phenotype. Another critical pro-fibrotic pathway is the YAP/TAZ signaling pathway which drives profibrotic signaling through matrix synthesis, contraction, and proliferation, particularly in the context of a stiff matrix [42, 43].
IL-4, IL-6, IL-11, IL-13, and IL-17 have all been deemed pro-fibrotic cytokines. IL-6 is a potent inducer of matrix production in fibroblasts by increasing TGF-β expression, TIMP-1 synthesis, and myofibroblast differentiation, resulting in collagen accumulation [44,45,46]. IL-4 has been demonstrated to be a pro-fibrotic cytokine participating in cutaneous, cardiac fibrosis, pulmonary fibrosis, and hepatic fibrosis, and has been shown to induce fibroblast proliferation, myofibroblast differentiation, and collagen production in vitro [47, 48]. IL-13 is increased in the serum and lesional tissue of patients with SSc, an in vitro stimulates fibroblasts both to proliferate and increase ECM synthesis [47, 49]. IL-17 levels are increased in the peripheral blood and tissue of SSc patients, and IL-17 treatment enhances the proliferation and differentiation of fibroblasts, although its influence is more nuanced and also has the potential to participate in protection from fibrosis depending on molecular and organ context [50, 51]. IL-11 has recently been described as a potent mediator of both inflammation and fibrosis [52], and has been found to be upregulated in SSc lung fibroblasts [53]. It is highly expressed on stromal, epithelial, and polarized cells, and non-canonical IL-11 signaling leads to myofibroblast activation and inhibition of tissue regeneration [53].
Connective tissue growth factor (CTGF) is a cysteine-rich secreted matricellular protein of the CCN family of extracellular matrix proteins which has several roles in wound repair and fibrosis and is induced by TGF-beta and endothelin-1 [54, 55]. Overexpression of CTGF in fibroblasts accelerates fibrosis in the skin, lung, kidney, and vasculature [56]. CTGF-deficient mice show resistance to bleomycin-induced fibrosis, primarily through a defect in myofibroblast recruitment [57].
Activation of PDGF/PDGFR signaling pathway has been observed in many fibrotic diseases[58]. In SSc fibroblasts, it was found that PDGF-a synthesis is driven by IL-1-α and PDGFR expression is upregulated in response to TGF-β thereby creating an autocrine loop leading to expansion of fibroblast matrix deposition. Blocking PDGF receptors inhibits myofibroblast formation and PDGF has induced myofibroblast activation while blocking its action inhibits myofibroblast activation [59].
Myofibroblast-inhibiting factors
There are fewer bonafide anti-fibrotic cytokines and growth factors than pro-fibrotic, which represents a challenge in targeting the myofibroblast therapeutically. A few of the described molecules that inhibit myofibroblast differentiation or function include TGF-β3, PPAR-γ FGF2, and interferon-γ.
While TGF-β1 and TGF-β2 are among the most important pro-fibrotic cytokines, TGF-β is often inhibitory as it has been shown to exert myofibroblast-suppressing and generally antifibrotic effects [60].
PPAR-gamma is a critical regulator of adipogenesis and is also a key anti-fibrotic regulator [61, 62]. Multiple studies have shown that PPAR-γ pathway expression is decreased in SSc and other fibrotic diseases, and that loss of PPAR-γ signaling is pro-fibrotic [63, 64].
Fibroblast growth factor 2 (FGF2) has also been implicated as a key suppressor of fibrosis; it reduces ASMA expression and antagonizes TGF-b1 signaling [65]. In fact, multiple FGF family members including FGF1, FGF2, and FGF9, and FGF10 can antagonize TGF-β1-induced myofibroblast differentiation and collagen production and thus may represent a class of anti-fibrotic molecules [66].
Interferon (IFN)-γ is an important pro-inflammatory cytokine produced by T cells and interestingly also has been shown to suppress ASMA expression in fibroblasts [67]. The myofibroblast-suppressing effect of IFN-γ appears to be mediated by activation of the repressor protein YB-1, which translocates to the nucleus and interferes with Smad3-mediated transcription of TGF-β1-induced genes [68].
Matrix stiffness effects on the myofibroblast
Matrix stiffness significantly contributes to myofibroblast differentiation and function: contraction of collagen into scar tissue is a primary function of myofibroblasts needed to maintain the mechanical integrity of damaged tissue. A mature scar is stiffer than the normal ECM and thus provides resistance to mechanical challenges. When fibroblasts move to a soft scaffold, their fibrils align, resulting in a denser ECM with increased stiffness [69]. Specifically, the mechanism of mechanotransduction in fibroblasts responds to matrix stiffening with changes in actin dynamics that favor filamentous actin polymerization, and this can be mediated by MKL1 a serum response factor coactivator which promotes the expression of ASMA [70].
The stiffness of the ECM also plays an important role in TGF-β activation. There is a requirement for ECM strain in order for TGF-β1 to be activated, and this serves as a mechanical checkpoint for the evolution of tissue repair. As ECM is slowly contracted by fibroblasts, it achieves a level of organization sufficient to activate latent TGF-β1. The available TGF-β1 can then further differentiate fibroblasts into myofibroblasts when remodeling of the strained and stiffened ECM requires increased force [71•].
A key molecular pathway related to mechano-signaling is the integrin family [72]. Integrins are upregulated in response to tissue stiffness and play an important role in regulating the fibroblast/mesenchymal cell-to-myofibroblast differentiation. The expression of both av and α1 integrins increases upon TGF-β1 treatment and blocking these integrins prevents TGF-β induced myofibroblast differentiation [73]. Mechanotransduction results in rapid changes in cellular mechanics by affecting gene expression, which requires integrin-dependent RhoA signaling and downstream actin dynamics. Mechanical stretch on integrins activates FAK and Src family kinases and induces cell stiffening. RhoA subsequently promotes stress fiber formation through the activation of Rho-associated coiled-coil containing protein kinase (ROCK) [72].
YAP (Yes-associated protein) and TAZ (transcriptional coactivator with PDZ-binding motif) are important transcription factors in the Hippo family that translocate to nucleus in response to matrix stiffening [74]. Increased ECM stiffness promotes nuclear localization of YAP and TAZ and upregulation of their target genes, with actin cytoskeleton tension resulting from manipulations of rigidity representing a link between ECM stiffness and YAP/TAZ activation. High ECM stiffness promotes cell spreading and subsequently leads to actin cytoskeleton tension, which in turn results in nuclear translocation of YAP/TAZ, at least partially through RhoA which functions as an ECM stiffness sensor [74].
Apoptosis in myofibroblasts
Apoptosis is the process by which cells undergo programmed death, and relative to fibroblasts, myofibroblasts have traditionally been viewed as resistant to this process. Myofibroblasts evade apoptosis by remaining activated after pro-survival biomechanical and growth factor signals from the fibrotic microenvironment. However, there is a growing literature that suggests that myofibroblasts are actually primed for apoptosis when survival pathways are inhibited and that they may therefore not need to be resistant to apoptosis [75•, 76•].
Apoptosis can be mediated by both an intrinsic and an extrinsic pathway [77]. The intrinsic pathway is triggered by stimuli such as DNA damage, oxidative stress, radiation, nutrient damage and induces apoptosis by promoting mitochondrial outer membrane permeabilization and cytochrome-c-dependent activation of caspases, and is regulated by BCL-2 proteins. The extrinsic pathway is activated by binding of extracellular death ligands such as FAS, TNF receptors, and other death receptors which then signal via caspases to initiate apoptosis by cleavage and activation of pro-caspase 3.
The expression of pro-apoptotic and pro-survival molecules determines mitochondrial priming, the degree to which mitochondria approach the apoptotic threshold [75•]. In myofibroblasts, TGF-b acts as a key regulator of apoptosis by inhibiting the intrinsic pathway by activation of ABL signaling which promotes pro-survival proteins and also by inhibiting the pro-apoptotic protein BCL-2 by FAK-P13K-AKT signaling. TGF-β also inhibits extrinsic pathway by inhibiting sphingomyelinase which thereby protects the cells from FASL-induced apoptosis. Biomechanical signaling also inhibits intrinsic pathway by signaling through the TGF-β, FAK, YAP-TAZ, BCL-XL and ROCK, MRTF, BCL-2 pathways [76•]. Matrix stiffness can also induce the expression of microRNAs miR-21 and miR-29a that promotes the survival of myofibroblasts by increasing expression of BCL-2 and reducing the expression of pro apoptotic BAX mRNA [78, 79].
Impact of immunomodulatory drugs used in SSc on myofibroblasts
In SSc, until the recent advent of antifibrotic agents, immunomodulation has been the mainstay of therapy for the treatment of organ fibrosis. While there not a lot of mechanistic studies which clearly identify the roles of immunomodulation in treating fibrosis, there are some data which suggest that immunomodulatory agents used in SSc may have some anti-fibrotic and therefore anti-myofibroblast properties.
Mycophenolate
Often, the first-line agent for skin and lung fibrosis, myophenolate mofetil (MMF), has some preclinical evidence of inhibition of myofibroblast function. In a rat model of renal injury after subtotal nephrectomy, mycophenolate treatment led to a significant reduction in myofibroblast infiltration and reduction in renal type III collagen deposition [80]. In vitro, mycophenolate was also found to decrease the expression of ASMA and decreasing the myofibroblast contractility and scar formation [81]. Moreover, MMF also exhibited a dose-dependent decrease in fibroblast proliferation.
Tocilizumab
Tocilizumab (TCZ) is an interleukin-6 (IL-6) receptor blocker. SSc patients were treated with tocilizumab for 24 weeks in the phase 2 faSScinate study [82••]. In this study, while the primary endpoint was not achieved, the subset of patients with interstitial lung disease (ILD) with elevated acute phase reactants showed a significant trend toward improvement, and this data has led to an FDA approval for tocilizumab for SSc-associated ILD [83]. A sub-study was performed in which skin biopsies from patients in the faSScinate trial were assessed [45], and dermal fibroblasts from patients treated with TCZ showed a variety of improvements suggesting that there was an anti-fibrotic effect. These included a decrease in migration and contractility, as well as a substantially altered the genomic phenotype with normalization of gene expression profiles dominated by TGFβ-regulated genes and molecular pathways including the interleukin 6/STAT3 cluster.
Cyclophosphamide
Cyclophosphamide (CYC) is an immunosuppressive agent that acts via its metabolite mustard to create DNA crosslinks and induce cell apoptosis which has efficacy in SSc-related interstitial lung disease. While mechanistic studies are lacking, a study assessed its role in skin fibrosis and showed that SSc patients treated with CYC had reduced myofibroblast numbers and reduced hyalinized collagen compared to placebo-treated patients [84].
Abatacept
Abatacept is a fusion protein of the extracellular domain of CTLA-4, a costimulatory T-cell co-stimulatory molecule, and an IgG1 Fc fragment. Pre-clinically, abatacept in reduced bleomycin induced dermal fibrosis in mice [85]. It was found that abatacept-treated mice had reduced T-cell activation, decreased resident fibroblast activation, decreased TGF-β signaling leading to reduction in myofibroblasts counts by 41%, dermal thickness by 48%, and hydroxyproline content of skin by 63% as compared to controls. A similar anti-fibrotic effect was seen in the chronic graft versus host disease–induced model of skin fibrosis [85]. In mice lacking T-cells, these effects were not observed suggesting that abatacept acts via T cells to exert its anti-fibrotic effects. The phase 2 ASSET trial [86] assessed the efficacy of abatacept in reducing skin fibrosis in patients; while the study did not meet its primary endpoint of changes in modified Rodnan skin score (MRSS) at 12 months, secondary outcome measures including gene expression studies which found that a subset of patients improved on abatcept, particularly those who had an inflammatory intrinsic gene subset.
Tofacitinib
Tofacitinib is an inhibitor of JAK1 and JAK3 which has been suggested as a potential treatment for SSc and is in clinical trials. In a study evaluating the JAK/STAT pathway in renal fibrosis, tofacitinib-treated mice exhibited fewer myofibroblasts and fewer fibrotic changes in mice after initiation of unilateral ureteral obstruction-induced kidney fibrosis [87].
Emerging anti-fibrotic therapy
Beyond immunomodulatory agents, there has been an increasing focus on trying to develop therapies which are truly anti-fibrotic. Data suggesting the efficacy of nintedanib [88••] and pirfenidone [89] for idiopathic pulmonary fibrosis (IPF) has ushered in a new class of agents and made anti-fibrotic therapy a potential primary or at least an adjunctive treatment strategy in SSc.
Pulmonary fibrosis and interstitial lung disease (ILD) in systemic sclerosis (SSc) are a major cause of morbidity and mortality. Increased numbers of smooth-muscle alpha-actin-positive myofibroblasts are found in the early fibrotic lung process and may be detected via bronchoalveolar lavage [90, 91]. These myofibroblasts produce significant extracellular matrix along alveoli, impairing gas exchange and damaging normal pulmonary architecture [4••]. They also may increase pulmonary arterial pressures directly by damaging arterioles and indirectly via release of endothelin-1, a potent vasoconstrictor [4••].
Nintedanib
Recently, nintedanib (a.k.a. BIBF 1120) has emerged as treatment for SS-associated ILD. Nintedanib inhibits the receptor tyrosine kinases fibroblast growth factor receptor (FGFR)-1, vascular endothelial growth factor receptor (VEGFR)-2, and platelet-derived growth factor receptor (PDGFR)-α and β [92]. In vitro studies of human pulmonary fibroblasts treated with nintedanib found it was antiproliferative, decreased TGF-β-induced transformation to myofibroblasts, and decreased TGF-β-induced collagen deposition [93]. It also may have in vitro anti-angiogenic properties [94].
The clinical efficacy of nintedanib was first demonstrated in idiopathic pulmonary fibrosis. In a phase II trial in patients with IPF, 52 weeks of nintedanib therapy resulted in a decreased reduction in forced vital capacity (FVC) decline and acute disease exacerbations [95]. Two phase III trials further studied nintedanib in IPF [96, 97]. The results confirmed that nintedanib therapy over 52 weeks decreased the decline in FVC in both phase III trials and decreased acute exacerbations in the second phase III trial [97]. A major side effect of nintedanib in the trials was diarrhea, which occurred in over 60% of users, but lead to discontinuation of the medication in less than 5% [97]. Following these trials, Nintedanib was studied in SSc-associated ILD. A phase III trial showed that 52 weeks of therapy with nintedanib resulted in a mild decrease in the rate of decline in FVC (− 52.4 ml per year vs − 93.3 ml per year in the placebo group), without improvement in the modified Rodnan skin score or St. George’s Respiratory Questionnaire [88••]. Nintedanib received US Food and Drug Administration (FDA) approval for SSc-associated ILD in September 2019.
Tyrosine kinase inhibitors
Inhibition of other tyrosine kinases have been potential targets for treatment of TGF-β induced fibrosis [98]. The pathophysiology of tyrosine kinases in SSc has recently been reviewed in detail, and there is good rationale for these agents as potentially anti-fibrotic [99]. Imatinib mesylate (a.k.a STI571) was noted to decrease bone marrow fibrosis when used for treatment chronic myelogenous leukemia (CML), suggesting it had an antifibrotic effect [100]. Early studies with imatinib demonstrated that it inhibited TGF-β-mediated c-Abl kinase in a mouse model of bleomycin-mediated lung fibrosis further suggesting it may have a therapeutic role in fibrotic lung disease [101]. In dermal fibroblast models of SSc, imatinib decreased TGF-β-mediated extracellular matrix protein deposition and myofibroblast transformation [102, 103]. Multiple small open-label trials of imatinib, testing various doses and durations of treatment, have been conducted in patients with SSc with varying results [104,105,106,107,108]. Significant edema and gastrointestinal side effects limited tolerability in many of these studies. Two small double-blind placebo-controlled trials have been conducted. One discontinued after enrollment of 10 patients due to medication intolerability without findings of improvement in skin disease [109]. The other enrolled 28 patients and failed to find improvement in skin or lung disease after 6 months of treatment [110].
Another tyrosine kinase inhibitor, dasatinib, also showed promise to have antifibrotic effects. It inhibits multiple proteins, including c-kit, BCR-Abl, PDGFR, ephrin-A receptor kinases, and Src, which is common to both PDGF and TGF-b pathways [99]. In an open-label trial of 31 SSc-associated ILD patients, there was no improvement overall in skin disease or pulmonary function tests, but lung fibrosis stabilized in about two-thirds of subjects as measured by high-resolution CT scan [111]. However, drug-induced pulmonary hypertension is a known complication of dasatinib, and this potential side effect limits its use in SSc patients who are already at risk for this manifestation [112].
Nilotinib is another tyrosine kinase inhibitor of multiple proteins, including BCR-Abl, c-Kit, ephrin-A receptor kinases, and PDGF kinases [99]. In a small open-label trial in 10 early or active diffuse SSc patients, nilotinib treatment improved skin disease after 6 and 12 months of treatment; however, two patients discontinued the trial due to QTc prolongation on electrocardiogram and one discontinued due to worsening cardiac disease [113]. Future larger scale studies of nilotinib may be warranted but cardiac adverse events will need to be monitored closely.
Pirfenidone
Pirfenidone is another medication used to treat fibrotic lung disease. Its mechanism of action is not completely understood, but it is a derivate of pyridine [114]. It attenuates profibrotic pathways by decreasing expression of TGF-β1, downstream mediators of TGF-β1 (including SMAD3, α-SMA, tenascin-c, fibronectin, chaperone HSP47), TNF-α, PDGF, bFGF, collagen gene expression, MMP-9, TIMP1, and MMP-2 [114, 115]. Additionally, pirfenidone has anti-inflammatory effects with studies demonstrating that it decreases activation of dendric cells, macrophages, and T-lymphocytes, as well as reduces levels of proinflammatory cytokines TNF-α, IL-6, IL-10, and IFN-γ [114].
Clinical trials with pirfenidone as treatment for IPF found it to decrease the rate of decline in FVC and death related to IPF [89, 116]. Pirfenidone was approved by the US FDA in 2014 for treatment of IPF and in March 2020 received a breakthrough therapy designation for unclassifiable interstitial lung disease. However, its use in SSc-associated ILD trials has not demonstrated benefit to-date. A phase II trial assessing tolerability of pirfenidone in SSc-associated ILD did not find significant change from baseline in FVC, DLCO, or skin thickening at 16 weeks of treatment [117]. A recent small trial in SSc-associated ILD did not find an improvement in lung function or skin disease with pirfenidone treatment compared to placebo at 6 months, although 94% of SSc subjects had stabilization of FVC [118]. This study was limited by its small sample size and statistical power. Additional clinical trials are ongoing in SSc-associated ILD in China and the USA to assess if pirfenidone has role as an antifibrotic treatment (ClinicalTrials.gov Identifier: NCT03856853, NCT03221257).
Fresolimumab
Fresolimumab is a human IgG4 monoclonal antibody with the ability to neutralize all isoforms of TGF-β. In a trial looking at its effects on skin fibrosis in SSc [119], it was observed that treatment with fresolimumab led to decreased TGF-b-regulated gene expression of skin biomarker genes including NOX4, CTGF, and PAI-1. These changes correlated with decrease in skin thickness (MRSS) suggesting that this was a drug-induced anti-fibrotic effect. Beyond fresolimumab, other anti-TGF-β treatments are in the developmental pipeline.
CD47 blockade and fibroblast phagocytosis
c-Jun-mediated fibrosis has been shown to be an important pathway which maintains fibroblasts’ persistently activated state, and blockade of CD47, the so-called don’t eat me signal on myeloid cells, has been shown to reverse this process [120]. Recently, studies in both skin [121] and lung [122•] fibrosis have shown promising anti-fibrotic effects of combination therapy using both anti-IL-6 therapy and anti-CD47 antibodies to allow macrophages to phagocytose-activated fibroblasts/myofibroblasts. This approach therefore has the potential to address both immune and stromal components of SSc and target persistently activated myofibroblasts in diseased tissue. Given recent success with anti-CD47 antibodies in combination with biologics in lymphoma and other malignancies [123, 124], this approach has potential clinical utility.
Regulators of myofibroblast apoptosis
Another emerging mechanism to counter myofibroblast proliferation in SSc is the induction of apoptosis in these cells with multiple different agents being investigated. One compound is ABT-262 [76•]. This agent inhibits BCL-XL, an antiapoptotic protein continually expressed in myofibroblasts [76•]. Blockage of BCL-XL with ABT-262 results in myofibroblast apoptosis and improvement in dermal fibrosis in a mouse model of SSc [76•]. Another agent is TLY012. This compound is an engineered human TNF-related apoptosis-inducing ligand (TRAIL) and is able to induce apoptosis in cells expressing its cognate death receptors [125•]. In a mouse model of SSc, TLY012 was shown to induce apoptosis in myofibroblasts and reduce dermal fibrosis [125•]. Given the normal apoptosis resistance of fibrotic myofibroblasts, these therapies are thought to represent a novel targeted myofibroblast-specific therapy with better safety profiles than more non-specific anti-fibrotic agents like tyrosine kinase inhibitors.
Conclusion
Myofibroblasts are dynamic cells which both promote and maintain the fibrotic micro-environment in SSc. They are diverse in origin, have variable activation states driven by multiple canonical signaling pathways, are influenced by a variety of soluble factors and mechanical forces, and their persistence is critical to the progression or resolution of clinical disease. Moreover, increased understanding of the molecular pathways influencing myofibroblast biology has provided a number of new potential targets for treatment in SSc. Current immunomodulatory therapy has at least a secondary impact on myofibroblast function, and emerging anti-fibrotic therapies have shown that a variety of approaches that more specifically target myofibroblasts has the potential to create more targeted and effective therapies for SSc and other fibrotic illnesses.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
• Allanore Y, Simms R, Distler O, Trojanowska M, Pope J, Denton CP, Varga J. Systemic sclerosis Nat Rev Dis Primers. 2015;1:15002. https://doi.org/10.1038/nrdp.2015.2. (Overview of the pathogeneic basis of systemic sclerosis and its clincial and molecular hetorgeneity.)
Rockey DC, Bell PD, Hill JA. Fibrosis–a common pathway to organ injury and failure. N Engl J Med. 2015;372:1138–49. https://doi.org/10.1056/NEJMra1300575.
Garrett SM, Baker Frost D, Feghali-Bostwick C. The mighty fibroblast and its utility in scleroderma research. J Scleroderma Relat Disord. 2017;2:69–134. https://doi.org/10.5301/jsrd.5000240.
van Caam A, Vonk M, van den Hoogen F, van Lent P, van der Kraan P. Unraveling SSc Pathophysiology; The Myofibroblast. Front Immunol. 2018;9:2452. https://doi.org/10.3389/fimmu.2018.02452.
Gabbiani G, Ryan GB, Majne G. Presence of modified fibroblasts in granulation tissue and their possible role in wound contraction. Experientia. 1971;27:549–50. https://doi.org/10.1007/BF02147594.
Kendall RT, Feghali-Bostwick CA. Fibroblasts in fibrosis: novel roles and mediators. Front Pharmacol. 2014;5:123. https://doi.org/10.3389/fphar.2014.00123.
Schmitt-Graff A, Desmouliere A, Gabbiani G. Heterogeneity of myofibroblast phenotypic features: an example of fibroblastic cell plasticity. Virchows Arch. 1994;425:3–24. https://doi.org/10.1007/BF00193944.
Brown LF, Dubin D, Lavigne L, Logan B, Dvorak HF, Van de Water L. Macrophages and fibroblasts express embryonic fibronectins during cutaneous wound healing. Am J Pathol. 1993;142:793–801.
Gabbiani G. The myofibroblast in wound healing and fibrocontractive diseases. J Pathol. 2003;200:500–3. https://doi.org/10.1002/path.1427.
Hinz B, Dugina V, Ballestrem C, Wehrle-Haller B, Chaponnier C. Alpha-smooth muscle actin is crucial for focal adhesion maturation in myofibroblasts. Mol Biol Cell. 2003;14:2508–19. https://doi.org/10.1091/mbc.e02-11-0729.
Bhattacharyya, S., Tamaki, Z., Wang, W., Hinchcliff, M., Hoover, P., Getsios, S., . . . Varga, J. FibronectinEDA promotes chronic cutaneous fibrosis through Toll-like receptor signaling. Sci Transl Med (2014) 6 232ra250. https://doi.org/10.1126/scitranslmed.3008264.
Ebmeier S, Horsley V. Origin of fibrosing cells in systemic sclerosis. Curr Opin Rheumatol. 2015;27:555–62. https://doi.org/10.1097/BOR.0000000000000217.
Rajkumar VS, Howell K, Csiszar K, Denton CP, Black CM, Abraham DJ. Shared expression of phenotypic markers in systemic sclerosis indicates a convergence of pericytes and fibroblasts to a myofibroblast lineage in fibrosis. Arthritis Res Ther. 2005;7:R1113. https://doi.org/10.1186/ar1790.
Abu El-Asrar AM, Struyf S, Van Damme J, Geboes K. Circulating fibrocytes contribute to the myofibroblast population in proliferative vitreoretinopathy epiretinal membranes. Br J Ophthalmol. 2008;92:699–704. https://doi.org/10.1136/bjo.2007.134346.
• Marangoni, R. G., Korman, B. D., Wei, J., Wood, T. A., Graham, L. V., Whitfield, M. L., . . . Varga, J. Myofibroblasts in murine cutaneous fibrosis originate from adiponectin-positive intradermal progenitors. Arthritis Rheumatol (2015) 67, 1062–1073. https://doi.org/10.1002/art.38990. (Description of pathogenic role of adipose tissue in dermal fibrosis and SSc.)
Dongre A, Weinberg RA. New insights into the mechanisms of epithelial-mesenchymal transition and implications for cancer. Nat Rev Mol Cell Biol. 2019;20:69–84. https://doi.org/10.1038/s41580-018-0080-4.
Piera-Velazquez S, Li Z, Jimenez SA. Role of endothelial-mesenchymal transition (EndoMT) in the pathogenesis of fibrotic disorders. Am J Pathol. 2011;179:1074–80. https://doi.org/10.1016/j.ajpath.2011.06.001.
Gerhardt H, Betsholtz C. Endothelial-pericyte interactions in angiogenesis. Cell Tissue Res. 2003;314:15–23. https://doi.org/10.1007/s00441-003-0745-x.
Humphreys, B. D., Lin, S. L., Kobayashi, A., Hudson, T. E., Nowlin, B. T., Bonventre, J. V., . . . Duffield, J. S. Fate tracing reveals the pericyte and not epithelial origin of myofibroblasts in kidney fibrosis. Am J Pathol (2010) 176, 85–97. https://doi.org/10.2353/ajpath.2010.090517.
Reilkoff RA, Bucala R, Herzog EL. Fibrocytes: emerging effector cells in chronic inflammation. Nat Rev Immunol. 2011;11:427–35. https://doi.org/10.1038/nri2990.
Kleaveland KR, Moore BB, Kim KK. Paracrine functions of fibrocytes to promote lung fibrosis. Expert Rev Respir Med. 2014;8:163–72. https://doi.org/10.1586/17476348.2014.862154.
Marangoni RG, Korman B, Varga J. Adipocytic progenitor cells give rise to pathogenic myofibroblasts: adipocyte-to-mesenchymal transition and its emerging role in fibrosis in multiple organs. Curr Rheumatol Rep. 2020;22:79. https://doi.org/10.1007/s11926-020-00957-w.
Hewlett JC, Kropski JA, Blackwell TS. Idiopathic pulmonary fibrosis: Epithelial-mesenchymal interactions and emerging therapeutic targets. Matrix Biol. 2018;71–72:112–27. https://doi.org/10.1016/j.matbio.2018.03.021.
Guarino M, Tosoni A, Nebuloni M. Direct contribution of epithelium to organ fibrosis: epithelial-mesenchymal transition. Hum Pathol. 2009;40:1365–76. https://doi.org/10.1016/j.humpath.2009.02.020.
Stemmler MP, Eccles RL, Brabletz S, Brabletz T. Non-redundant functions of EMT transcription factors. Nat Cell Biol. 2019;21:102–12. https://doi.org/10.1038/s41556-018-0196-y.
Bischoff J. Endothelial-to-Mesenchymal Transition. Circ Res. 2019;124:1163–5. https://doi.org/10.1161/CIRCRESAHA.119.314813.
Cipriani, P., Di Benedetto, P., Ruscitti, P., Capece, D., Zazzeroni, F., Liakouli, V., . . . Giacomelli, R. The endothelial-mesenchymal transition in systemic sclerosis is induced by endothelin-1 and transforming growth factor-β and may be blocked by macitentan, a dual endothelin-1 receptor antagonist. J Rheumatol (2015) 42, 1808–1816. https://doi.org/10.3899/jrheum.150088
Serrati, S., Chilla, A., Laurenzana, A., Margheri, F., Giannoni, E., Magnelli, L., . . . Del Rosso, M. Systemic sclerosis endothelial cells recruit and activate dermal fibroblasts by induction of a connective tissue growth factor (CCN2)/transforming growth factor beta-dependent mesenchymal-to-mesenchymal transition. Arthritis Rheum (2013) 65, 258–269. https://doi.org/10.1002/art.37705.
Manetti M, Romano E, Rosa I, Guiducci S, Bellando-Randone S, De Paulis A, . . . Matucci-Cerinic M. Endothelial-to-mesenchymal transition contributes to endothelial dysfunction and dermal fibrosis in systemic sclerosis. Ann Rheum Dis (2017) 76, 924–934. https://doi.org/10.1136/annrheumdis-2016-210229.
Varga J, Pasche B. Transforming growth factor β as a therapeutic target in systemic sclerosis. Nat Rev Rheumatol. 2009;5:200–6. https://doi.org/10.1038/nrrheum.2009.26.
Gilbert RWD, Vickaryous MK, Viloria-Petit AM. Signalling by transforming growth factor beta isoforms in wound healing and tissue regeneration. J Dev Biol (2016) 4. https://doi.org/10.3390/jdb4020021.
Robertson IB, Rifkin DB. Unchaining the beast; insights from structural and evolutionary studies on TGFbeta secretion, sequestration, and activation. Cytokine Growth Factor Rev. 2013;24:355–72. https://doi.org/10.1016/j.cytogfr.2013.06.003.
Wipff PJ, Rifkin DB, Meister JJ, Hinz B. Myofibroblast contraction activates latent TGF-beta1 from the extracellular matrix. J Cell Biol. 2007;179:1311–23. https://doi.org/10.1083/jcb.200704042.
Frangogiannis N. Transforming growth factor-beta in tissue fibrosis. J Exp Med. 2020;217:e20190103. https://doi.org/10.1084/jem.20190103.
Lafyatis R. Transforming growth factor beta–at the centre of systemic sclerosis. Nat Rev Rheumatol. 2014;10:706–19. https://doi.org/10.1038/nrrheum.2014.137.
Wei J, Melichian D, Komura K, Hinchcliff M, Lam AP, Lafyatis R, . . . Varga J. Canonical Wnt signaling induces skin fibrosis and subcutaneous lipoatrophy: a novel mouse model for scleroderma? Arthritis Rheum (2011) 63, 1707–1717. https://doi.org/10.1002/art.30312.
Wei J, Fang F, Lam AP, Sargent JL, Hamburg E, Hinchcliff ME, . . . Varga J. Wnt/beta-catenin signaling is hyperactivated in systemic sclerosis and induces Smad-dependent fibrotic responses in mesenchymal cells. Arthritis Rheum (2012) 64, 2734–2745. https://doi.org/10.1002/art.34424.
Dees C, Schlottmann I, Funke R, Distler A, Palumbo-Zerr K, Zerr P, . . . Distler JH. The Wnt antagonists DKK1 and SFRP1 are downregulated by promoter hypermethylation in systemic sclerosis. Ann Rheum Dis (2014) 73, 1232–1239. https://doi.org/10.1136/annrheumdis-2012-203194.
Horn A, Palumbo K, Cordazzo C, Dees C, Akhmetshina A, Tomcik M, . . . Distler JH. Hedgehog signaling controls fibroblast activation and tissue fibrosis in systemic sclerosis. Arthritis Rheum (2012) 64, 2724–2733. https://doi.org/10.1002/art.34444.
Distler A, Lang V, Del Vecchio T, Huang J, Zhang Y, Beyer C, . . . Distler JH. Combined inhibition of morphogen pathways demonstrates additive antifibrotic effects and improved tolerability. Ann Rheum Dis (2014) 73, 1264–1268. https://doi.org/10.1136/annrheumdis-2013-204221.
Dees, C., Zerr, P., Tomcik, M., Beyer, C., Horn, A., Akhmetshina, A., . . . Distler, J. H. Inhibition of Notch signaling prevents experimental fibrosis and induces regression of established fibrosis. Arthritis Rheum (2011) 63, 1396–1404. https://doi.org/10.1002/art.30254.
Liu, F., Lagares, D., Choi, K. M., Stopfer, L., Marinković, A., Vrbanac, V., . . . Tschumperlin, D. J. Mechanosignaling through YAP and TAZ drives fibroblast activation and fibrosis. American Journal of Physiology-Lung Cellular and Molecular Physiology (2015) 308, L344-L357. https://doi.org/10.1152/ajplung.00300.2014.
Piersma B, Bank RA, Boersema M. Signaling in Fibrosis: TGF-beta, WNT, and YAP/TAZ Converge. Front Med (Lausanne). 2015;2:59. https://doi.org/10.3389/fmed.2015.00059.
Gallucci RM, Lee EG, Tomasek JJ. IL-6 modulates alpha-smooth muscle actin expression in dermal fibroblasts from IL-6-deficient mice. J Investig Dermatol. 2006;126:561–8. https://doi.org/10.1038/sj.jid.5700109.
Denton, C. P., Ong, V. H., Xu, S., Chen-Harris, H., Modrusan, Z., Lafyatis, R., . . . Sornasse, T. Therapeutic interleukin-6 blockade reverses transforming growth factor-beta pathway activation in dermal fibroblasts: insights from the faSScinate clinical trial in systemic sclerosis. Ann Rheum Dis (2018)77, 1362–1371. https://doi.org/10.1136/annrheumdis-2018-213031.
Kawaguchi Y. Contribution of interleukin-6 to the Pathogenesis of Systemic Sclerosis. Journal of Scleroderma and Related Disorders. 2017;2:S6–12. https://doi.org/10.5301/jsrd.5000258.
Gasparini G, Cozzani E, Parodi A. Interleukin-4 and interleukin-13 as possible therapeutic targets in systemic sclerosis. Cytokine. 2020;125:154799. https://doi.org/10.1016/j.cyto.2019.154799.
Salmon-Ehr, V., Serpier, H., Nawrocki, B., Gillery, P., Clavel, C., Kalis, B., . . . Maquart, F.-X. Expression of interleukin-4 in Scleroderma skin specimens and scleroderma fibroblast cultures: potential role in fibrosis. Archives of Dermatology (1996) 132, 802-806https://doi.org/10.1001/archderm.1996.03890310088013
Fuschiotti P, Larregina AT, Ho J, Feghali-Bostwick C, Medsger TA Jr. Interleukin-13-producing CD8+ T cells mediate dermal fibrosis in patients with systemic sclerosis. Arthritis Rheum. 2013;65:236–46. https://doi.org/10.1002/art.37706.
Chizzolini C, Dufour AM, Brembilla NC. Is there a role for IL-17 in the pathogenesis of systemic sclerosis? Immunol Lett. 2018;195:61–7. https://doi.org/10.1016/j.imlet.2017.09.007.
Ramani K, Biswas PS. Interleukin-17: Friend or foe in organ fibrosis. Cytokine. 2019;120:282–8. https://doi.org/10.1016/j.cyto.2018.11.003.
Ng, B., Dong, J., D'Agostino, G., Viswanathan, S., Widjaja, A. A., Lim, W. W., . . . Cook, S. A. Interleukin-11 is a therapeutic target in idiopathic pulmonary fibrosis. Sci Transl Med (2019) 11. https://doi.org/10.1126/scitranslmed.aaw1237.
Cook SA, Schafer S. Hiding in plain sight: interleukin-11 emerges as a master regulator of fibrosis, tissue integrity, and stromal inflammation. Annu Rev Med. 2020;71:263–76. https://doi.org/10.1146/annurev-med-041818-011649.
Ramazani Y, Knops N, Elmonem MA, Nguyen TQ, Arcolino FO, van den Heuvel L, . . . Goldschmeding R. Connective tissue growth factor (CTGF) from basics to clinics. Matrix Biology (2018) 68–69, 44–66. https://doi.org/10.1016/j.matbio.2018.03.007.
Abraham D. Connective tissue growth factor: growth factor, matricellular organizer, fibrotic biomarker or molecular target for anti-fibrotic therapy in SSc? Rheumatology (Oxford). 2008;47(Suppl 5):v8-9. https://doi.org/10.1093/rheumatology/ken278.
Chen Z, Zhang N, Chu HY, Yu Y, Zhang ZK, Zhang G, Zhang BT. Connective tissue growth factor: from molecular understandings to drug discovery. Front Cell Dev Biol. 2020;8:593269. https://doi.org/10.3389/fcell.2020.593269.
Liu S, Shi-wen X, Abraham DJ, Leask A. CCN2 is required for bleomycin-induced skin fibrosis in mice. Arthritis Rheum. 2011;63:239–46. https://doi.org/10.1002/art.30074.
Klinkhammer BM, Floege J, Boor P. PDGF in organ fibrosis. Mol Aspects Med. 2018;62:44–62. https://doi.org/10.1016/j.mam.2017.11.008.
Hinz B. Myofibroblasts. Exp Eye Res. 2016;142:56–70. https://doi.org/10.1016/j.exer.2015.07.009.
Fujio K, Komai T, Inoue M, Morita K, Okamura T, Yamamoto K. Revisiting the regulatory roles of the TGF-beta family of cytokines. Autoimmun Rev. 2016;15:917–22. https://doi.org/10.1016/j.autrev.2016.07.007.
Wei, J., Zhu, H., Komura, K., Lord, G., Tomcik, M., Wang, W., . . . Varga, J. A synthetic PPAR-gamma agonist triterpenoid ameliorates experimental fibrosis: PPAR-gamma-independent suppression of fibrotic responses. Ann Rheum Dis (2014) 73, 446-454https://doi.org/10.1136/annrheumdis-2012-202716
Wei, J., Ghosh, A. K., Sargent, J. L., Komura, K., Wu, M., Huang, Q. Q., . . . Varga, J. PPARgamma downregulation by TGFss in fibroblast and impaired expression and function in systemic sclerosis: a novel mechanism for progressive fibrogenesis. PLoS One (2010) 5, e13778. https://doi.org/10.1371/journal.pone.0013778.
Ruzehaji, N., Frantz, C., Ponsoye, M., Avouac, J., Pezet, S., Guilbert, T., . . . Allanore, Y. Pan PPAR agonist IVA337 is effective in prevention and treatment of experimental skin fibrosis. Ann Rheum Dis (2016) 75, 2175–2183. https://doi.org/10.1136/annrheumdis-2015-208029.
Korman B, Marangoni RG, Lord G, Olefsky J, Tourtellotte W, Varga J. Adipocyte-specific repression of PPAR-gamma by NCoR contributes to scleroderma skin fibrosis. Arthritis Res Ther. 2018;20:145. https://doi.org/10.1186/s13075-018-1630-z.
Dolivo DM, Larson SA, Dominko T. Fibroblast growth factor 2 as an antifibrotic: antagonism of myofibroblast differentiation and suppression of pro-fibrotic gene expression. Cytokine Growth Factor Rev. 2017;38:49–58. https://doi.org/10.1016/j.cytogfr.2017.09.003.
Xie, Y., Su, N., Yang, J., Tan, Q., Huang, S., Jin, M., . . . Chen, L. FGF/FGFR signaling in health and disease. Signal Transduct Target Ther (2020) 5, 181. https://doi.org/10.1038/s41392-020-00222-7.
Gu L, Zhu YJ, Guo ZJ, Xu XX, Xu WB. Effect of IFN-gamma and dexamethasone on TGF-beta1-induced human fetal lung fibroblast-myofibroblast differentiation. Acta Pharmacol Sin. 2004;25:1479–88.
Dooley S, Said HM, Gressner AM, Floege J, En-Nia A, Mertens PR. Y-box protein-1 is the crucial mediator of antifibrotic interferon-gamma effects. J Biol Chem. 2006;281:1784–95. https://doi.org/10.1074/jbc.M510215200.
Hinz B, McCulloch CA, Coelho NM. Mechanical regulation of myofibroblast phenoconversion and collagen contraction. Exp Cell Res. 2019;379:119–28. https://doi.org/10.1016/j.yexcr.2019.03.027.
Huang, X., Yang, N., Fiore, V. F., Barker, T. H., Sun, Y., Morris, S. W., . . . Zhou, Y. Matrix stiffness-induced myofibroblast differentiation is mediated by intrinsic mechanotransduction. Am J Respir Cell Mol Biol (2012) 47, 340–348. https://doi.org/10.1165/rcmb.2012-0050OC.
Hinz B. The extracellular matrix and transforming growth factor-β1: Tale of a strained relationship. Matrix Biol. 2015;47:54–65. https://doi.org/10.1016/j.matbio.2015.05.006.
Sun Z, Guo SS, Fassler R. Integrin-mediated mechanotransduction. J Cell Biol. 2016;215:445–56. https://doi.org/10.1083/jcb.201609037.
Schiller, H. B., Hermann, M. R., Polleux, J., Vignaud, T., Zanivan, S., Friedel, C. C., . . . Fassler, R. beta1- and alphav-class integrins cooperate to regulate myosin II during rigidity sensing of fibronectin-based microenvironments. Nat Cell Biol (2013) 15, 625–636. https://doi.org/10.1038/ncb2747.
Muppala S, Raghunathan VK, Jalilian I, Thomasy S, Murphy CJ. YAP and TAZ are distinct effectors of corneal myofibroblast transformation. Exp Eye Res. 2019;180:102–9. https://doi.org/10.1016/j.exer.2018.12.009.
Hinz B, Lagares D. Evasion of apoptosis by myofibroblasts: a hallmark of fibrotic diseases. Nat Rev Rheumatol. 2020;16:11–31. https://doi.org/10.1038/s41584-019-0324-5.
• Lagares, D., Santos, A., Grasberger, P. E., Liu, F., Probst, C. K., Rahimi, R. A., . . . Tager, A. M. Targeted apoptosis of myofibroblasts with the BH3 mimetic ABT-263 reverses established fibrosis. Sci Transl Med (2017) 9. https://doi.org/10.1126/scitranslmed.aal3765. (Provides conceptual framework for targeting myofibroblast apoptosis as a treatment for fibrosis.)
Czabotar PE, Lessene G, Strasser A, Adams JM. Control of apoptosis by the BCL-2 protein family: implications for physiology and therapy. Nat Rev Mol Cell Biol. 2014;15:49–63. https://doi.org/10.1038/nrm3722.
Jafarinejad-Farsangi, S., Farazmand, A., Mahmoudi, M., Gharibdoost, F., Karimizadeh, E., Noorbakhsh, F., . . . Jamshidi, A. R. MicroRNA-29a induces apoptosis via increasing the Bax:Bcl-2 ratio in dermal fibroblasts of patients with systemic sclerosis. Autoimmunity (2015) 48, 369–378. https://doi.org/10.3109/08916934.2015.1030616.
Li, C. X., Talele, N. P., Boo, S., Koehler, A., Knee-Walden, E., Balestrini, J. L., . . . Hinz, B. MicroRNA-21 preserves the fibrotic mechanical memory of mesenchymal stem cells. Nat Mater (2017) 16, 379–389. https://doi.org/10.1038/nmat4780.
Badid, C., Vincent, M., McGregor, B., Melin, M., Hadj-Aissa, A., Veysseyre, C., . . . Laville, M. Mycophenolate mofetil reduces myofibroblast infiltration and collagen III deposition in rat remnant kidney. Kidney Int (2000) 58, 51–61. https://doi.org/10.1046/j.1523-1755.2000.00140.x.
Roos N, Poulalhon N, Farge D, Madelaine I, Mauviel A, Verrecchia F. In vitro evidence for a direct antifibrotic role of the immunosuppressive drug mycophenolate mofetil. J Pharmacol Exp Ther. 2007;321:583–9. https://doi.org/10.1124/jpet.106.117051.
•• Khanna D, Denton CP, Jahreis A, van Laar JM, Frech TM, Anderson ME, Baron M, Chung L, Fierlbeck G, Lakshminarayanan S, Allanore Y, Pope JE, Riemekasten G, Steen V, Müller-Ladner U, Lafyatis R, Stifano G, Spotswood H, Chen-Harris H, Dziadek S, Morimoto A, Sornasse T, Siegel J, Furst DE. Safety and efficacy of subcutaneous tocilizumab in adults with systemic sclerosis (faSScinate): a phase 2, randomised, controlled trial. Lancet. 2016 Jun 25;387(10038):2630-2640. https://doi.org/10.1016/S0140-6736(16)00232-4. Epub 2016 May 5. Erratum in: Lancet. 2018 Apr 7;391(10128):1356. (Clinical trial demonstrating efficacy of tocilizumab in systemic sclerosis.)
Roofeh D, Lescoat A, Khanna D. Treatment for systemic sclerosis-associated interstitial lung disease. Curr Opin Rheumatol. 2021;33:240–8. https://doi.org/10.1097/BOR.0000000000000795.
Kissin EY, Merkel PA, Lafyatis R. Myofibroblasts and hyalinized collagen as markers of skin disease in systemic sclerosis. Arthritis Rheum. 2006;54:3655–60. https://doi.org/10.1002/art.22186.
Ponsoye, M., Frantz, C., Ruzehaji, N., Nicco, C., Elhai, M., Ruiz, B., . . . Avouac, J. Treatment with abatacept prevents experimental dermal fibrosis and induces regression of established inflammation-driven fibrosis. Ann Rheum Dis (2016) 75, 2142–2149. https://doi.org/10.1136/annrheumdis-2015-208213.
Khanna, D., Spino, C., Johnson, S., Chung, L., Whitfield, M. L., Denton, C. P., . . . Furst, D. E. Abatacept in early diffuse cutaneous systemic sclerosis: results of a phase ii investigator-initiated, multicenter, double-blind, randomized, placebo-controlled trial. Arthritis Rheumatol (2020) 72, 125–136. https://doi.org/10.1002/art.41055.
Yan J, Zhang Z, Yang J, Mitch WE, Wang Y. JAK3/STAT6 stimulates bone marrow-derived fibroblast activation in renal fibrosis. J Am Soc Nephrol. 2015;26:3060–71. https://doi.org/10.1681/ASN.2014070717.
•• Distler, O., Highland, K. B., Gahlemann, M., Azuma, A., Fischer, A., Mayes, M. D., . . . Maher, T. M. Nintedanib for systemic sclerosis–associated interstitial lung disease. New England J Med (2019) 380, 2518–2528. https://doi.org/10.1056/NEJMoa1903076. (Large clinical trial providing evidence of efficacy of nintedanib for SSc-ILD.)
King, T. E., Jr., Bradford, W. Z., Castro-Bernardini, S., Fagan, E. A., Glaspole, I., Glassberg, M. K., . . . Group, A. S. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med (2014) 370, 2083–2092. https://doi.org/10.1056/NEJMoa1402582.
Beon M, Harley RA, Wessels A, Silver RM, Ludwicka-Bradley A. Myofibroblast induction and microvascular alteration in scleroderma lung fibrosis. Clin Exp Rheumatol. 2004;22:733–42.
Ludwicka, A., Trojanowska, M., Smith, E. A., Baumann, M., Strange, C., Korn, J. H., . . . Silver, R. M. Growth and characterization of fibroblasts obtained from bronchoalveolar lavage of patients with scleroderma. J Rheumatol (1992) 19, 1716–1723.
Wollin L, Wex E, Pautsch A, Schnapp G, Hostettler KE, Stowasser S, Kolb M. Mode of action of nintedanib in the treatment of idiopathic pulmonary fibrosis. Eur Respir J. 2015;45:1434–45. https://doi.org/10.1183/09031936.00174914.
Wollin L, Maillet I, Quesniaux V, Holweg A, Ryffel B. Antifibrotic and anti-inflammatory activity of the tyrosine kinase inhibitor nintedanib in experimental models of lung fibrosis. J Pharmacol Exp Ther. 2014;349:209–20. https://doi.org/10.1124/jpet.113.208223.
Hilberg, F., Roth, G. J., Krssak, M., Kautschitsch, S., Sommergruber, W., Tontsch-Grunt, U., . . . Rettig, W. J. BIBF 1120: triple angiokinase inhibitor with sustained receptor blockade and good antitumor efficacy. Cancer Res (2008) 68, 4774–4782. https://doi.org/10.1158/0008-5472.CAN-07-6307.
Richeldi, L., Costabel, U., Selman, M., Kim, D. S., Hansell, D. M., Nicholson, A. G., . . . du Bois, R. M. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. N Engl J Med (2011) 365, 1079–1087. https://doi.org/10.1056/NEJMoa1103690.
Richeldi, L., Cottin, V., Flaherty, K. R., Kolb, M., Inoue, Y., Raghu, G., . . . Collard, H. R. Design of the INPULSIS trials: two phase 3 trials of nintedanib in patients with idiopathic pulmonary fibrosis. Respir Med (2014) 108, 1023–1030. https://doi.org/10.1016/j.rmed.2014.04.011.
Richeldi, L., du Bois, R. M., Raghu, G., Azuma, A., Brown, K. K., Costabel, U., . . . Investigators, I. T. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med (2014) 370, 2071–2082. https://doi.org/10.1056/NEJMoa1402584.
Rosenbloom J, Jimenez SA. Molecular ablation of transforming growth factor beta signaling pathways by tyrosine kinase inhibition: the coming of a promising new era in the treatment of tissue fibrosis. Arthritis Rheum. 2008;58:2219–24. https://doi.org/10.1002/art.23634.
Mendoza FA, Piera-Velazquez S, Jimenez SA. Tyrosine kinases in the pathogenesis of tissue fibrosis in systemic sclerosis and potential therapeutic role of their inhibition. Transl Res. 2021;231:139–58. https://doi.org/10.1016/j.trsl.2021.01.001.
Beham-Schmid C, Apfelbeck U, Sill H, Tsybrovsky O, Hofler G, Haas OA, Linkesch W. Treatment of chronic myelogenous leukemia with the tyrosine kinase inhibitor STI571 results in marked regression of bone marrow fibrosis. Blood. 2002;99:381–3. https://doi.org/10.1182/blood.v99.1.381.
Daniels CE, Wilkes MC, Edens M, Kottom TJ, Murphy SJ, Limper AH, Leof EB. Imatinib mesylate inhibits the profibrogenic activity of TGF-beta and prevents bleomycin-mediated lung fibrosis. J Clin Invest. 2004;114:1308–16. https://doi.org/10.1172/JCI19603.
Distler, J. H., Jungel, A., Huber, L. C., Schulze-Horsel, U., Zwerina, J., Gay, R. E., . . . Distler, O. Imatinib mesylate reduces production of extracellular matrix and prevents development of experimental dermal fibrosis. Arthritis Rheum (2007) 56, 311–322. https://doi.org/10.1002/art.22314.
Akhmetshina, A., Venalis, P., Dees, C., Busch, N., Zwerina, J., Schett, G., . . . Distler, J. H. Treatment with imatinib prevents fibrosis in different preclinical models of systemic sclerosis and induces regression of established fibrosis. Arthritis Rheum (2009) 60, 219–224. https://doi.org/10.1002/art.24186.
Spiera, R. F., Gordon, J. K., Mersten, J. N., Magro, C. M., Mehta, M., Wildman, H. F., . . . Crow, M. K. Imatinib mesylate (Gleevec) in the treatment of diffuse cutaneous systemic sclerosis: results of a 1-year, phase IIa, single-arm, open-label clinical trial. Ann Rheum Dis (2011) 70, 1003–1009. https://doi.org/10.1136/ard.2010.143974.
Khanna, D., Saggar, R., Mayes, M. D., Abtin, F., Clements, P. J., Maranian, P., . . . Furst, D. E. A one-year, phase I/IIa, open-label pilot trial of imatinib mesylate in the treatment of systemic sclerosis-associated active interstitial lung disease. Arthritis Rheum 63 (2011), 3540–3546. https://doi.org/10.1002/art.30548.
Guo L, Chen XX, Gu YY, Zou HJ, Ye S. Low-dose imatinib in the treatment of severe systemic sclerosis: a case series of six Chinese patients and literature review. Clin Rheumatol. 2012;31:1395–400. https://doi.org/10.1007/s10067-012-2032-2.
Tamaki, Z., Asano, Y., Hatano, M., Yao, A., Kawashima, T., Tomita, M., . . . Sato, S. Efficacy of low-dose imatinib mesylate for cutaneous involvement in systemic sclerosis: a preliminary report of three cases. Mod Rheumatol (2012) 22, 94–99. https://doi.org/10.1007/s10165-011-0472-1.
Gordon, J., Udeh, U., Doobay, K., Magro, C., Wildman, H., Davids, M., . . . Spiera, R. F. Imatinib mesylate (Gleevec) in the treatment of diffuse cutaneous systemic sclerosis: results of a 24-month open label, extension phase, single-centre trial. Clin Exp Rheumatol (2014) 32, S-189–193.
Pope, J., McBain, D., Petrlich, L., Watson, S., Vanderhoek, L., de Leon, F., . . . Summers, K. Imatinib in active diffuse cutaneous systemic sclerosis: results of a six-month, randomized, double-blind, placebo-controlled, proof-of-concept pilot study at a single center. Arthritis Rheum (2011) 63, 3547–3551. https://doi.org/10.1002/art.30549.
Prey, S., Ezzedine, K., Doussau, A., Grandoulier, A. S., Barcat, D., Chatelus, E., . . . Taieb, A. Imatinib mesylate in scleroderma-associated diffuse skin fibrosis: a phase II multicentre randomized double-blinded controlled trial. Br J Dermatol (2012) 167, 1138–1144. https://doi.org/10.1111/j.1365-2133.2012.11186.x.
Martyanov, V., Kim, G. J., Hayes, W., Du, S., Ganguly, B. J., Sy, O., . . . Varga, J. Novel lung imaging biomarkers and skin gene expression subsetting in dasatinib treatment of systemic sclerosis-associated interstitial lung disease. PLoS One (2017) 12, e0187580. https://doi.org/10.1371/journal.pone.0187580.
OzgurYurttas N, Eskazan AE. Dasatinib-induced pulmonary arterial hypertension. Br J Clin Pharmacol. 2018;84:835–45. https://doi.org/10.1111/bcp.13508.
Gordon, J. K., Martyanov, V., Magro, C., Wildman, H. F., Wood, T. A., Huang, W. T., . . . Spiera, R. F. Nilotinib (Tasigna) in the treatment of early diffuse systemic sclerosis: an open-label, pilot clinical trial. Arthritis Res Ther (2015) 17, 213. https://doi.org/10.1186/s13075-015-0721-3.
Ruwanpura SM, Thomas BJ, Bardin PG. Pirfenidone: molecular mechanisms and potential clinical applications in lung disease. Am J Respir Cell Mol Biol. 2020;62:413–22. https://doi.org/10.1165/rcmb.2019-0328TR.
Lopez-de la Mora, D. A., Sanchez-Roque, C., Montoya-Buelna, M., Sanchez-Enriquez, S., Lucano-Landeros, S., Macias-Barragan, J. & Armendariz-Borunda, J. Role and new insights of pirfenidone in fibrotic diseases. Int J Med Sci (2015) 12 840–847. https://doi.org/10.7150/ijms.11579.
Noble, P. W., Albera, C., Bradford, W. Z., Costabel, U., Glassberg, M. K., Kardatzke, D., . . . Group, C. S. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet (2011) 377, 1760-1769. https://doi.org/10.1016/S0140-6736(11)60405-4
Khanna, D., Albera, C., Fischer, A., Khalidi, N., Raghu, G., Chung, L., . . . Gorina, E. An open-label, phase II study of the safety and tolerability of pirfenidone in patients with scleroderma-associated interstitial lung disease: the LOTUSS Trial. J Rheumatol (2016) 43, 1672-1679https://doi.org/10.3899/jrheum.151322
Acharya N, Sharma SK, Mishra D, Dhooria S, Dhir V, Jain S. Efficacy and safety of pirfenidone in systemic sclerosis-related interstitial lung disease-a randomised controlled trial. Rheumatol Int. 2020;40:703–10. https://doi.org/10.1007/s00296-020-04565-w.
Rice, L. M., Padilla, C. M., McLaughlin, S. R., Mathes, A., Ziemek, J., Goummih, S., . . . Lafyatis, R. Fresolimumab treatment decreases biomarkers and improves clinical symptoms in systemic sclerosis patients. J Clin Invest (2015) 125, 2795–2807. https://doi.org/10.1172/JCI77958.
Wernig, G., Chen, S. Y., Cui, L., Van Neste, C., Tsai, J. M., Kambham, N., . . . Weissman, I. L. Unifying mechanism for different fibrotic diseases. Proc Natl Acad Sci U S A (2017) 114, 4757–4762. https://doi.org/10.1073/pnas.1621375114.
Lerbs, T., Cui, L., King, M. E., Chai, T., Muscat, C., Chung, L., . . . Wernig, G. CD47 prevents the elimination of diseased fibroblasts in scleroderma. JCI Insight (2020) 5. https://doi.org/10.1172/jci.insight.140458.
• Cui, L., Chen, S. Y., Lerbs, T., Lee, J. W., Domizi, P., Gordon, S., . . . Wernig, G. Activation of JUN in fibroblasts promotes pro-fibrotic programme and modulates protective immunity. Nat Commun (2020) 11, 2795. https://doi.org/10.1038/s41467-020-16466-4. (Provides evidence for a novel role of role of modulating Jun and CD47 in treating lung fibrosis.)
Advani, R., Flinn, I., Popplewell, L., Forero, A., Bartlett, N. L., Ghosh, N., . . . Smith, S. M. CD47 Blockade by Hu5F9-G4 and rituximab in non-Hodgkin’s lymphoma. N Engl J Med (2018) 379, 1711–1721. https://doi.org/10.1056/NEJMoa1807315.
Zhang, W., Huang, Q., Xiao, W., Zhao, Y., Pi, J., Xu, H., . . . Jin, H. Advances in anti-tumor treatments targeting the CD47/SIRPalpha axis. Front Immunol (2020) 11, 18. https://doi.org/10.3389/fimmu.2020.00018.
• Park, J. S., Oh, Y., Park, Y. J., Park, O., Yang, H., Slania, S., . . . Lee, S. Targeting of dermal myofibroblasts through death receptor 5 arrests fibrosis in mouse models of scleroderma. Nat Commun (2019) 10, 1128. https://doi.org/10.1038/s41467-019-09101-4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Anthony Ocon declares that he has no conflict of interest. Sravani Lokineni declares that she has no conflict of interest. Benjamin Korman declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Scleroderma
Rights and permissions
About this article

Cite this article
Ocon, A., Lokineni, S. & Korman, B. Understanding and Therapeutically Targeting the Scleroderma Myofibroblast. Curr Treat Options in Rheum 8, 1–18 (2022). https://doi.org/10.1007/s40674-021-00189-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40674-021-00189-8