
Abstract
Background
A role of the insulin-like growth factor-1 receptor (IGF-1R) in the pathogenesis of Graves’ orbitopathy (GO) has been proposed, but the existence and function of anti-IGF-1R-antibodies (IGF-1R-Abs) are debated.
Methods
We designed a cross-sectional investigation to measure serum IGF-1R-Abs by a commercial assay in consecutive patients with Graves’ disease (GD) compared with healthy subjects and patients with autoimmune thyroiditis (AT). A total of 134 subjects were screened including 27 healthy subjects, 80 GD patients (54 of whom with GO), and 27 AT patients. The main outcome measure was the prevalence of positive serum IGF-1R-Abs in GO, compared with GD without GO and with the other study groups.
Results
Having established a cut-off value at 55.2 ng/ml for positive tests, positive IGF-1R-Abs were more frequent in GD (25%), than in AT (3.7%, P = 0.003) and healthy subjects (0%, P = 0.006). Within GD, there was no difference between patients with or without GO. Serum levels of IGF-1R-Abs differed across the study population (P < 0.0001), reflecting their higher concentrations in GD (P < 0.0001 vs both AT and healthy subjects), but with no difference between patients with or without GO. In patients with GO, there was an inverse correlation between serum IGF-1R-Abs and CAS (R = − 0.376, 95% CI: from − 0.373 to − 0.631; P = 0.005), the significance of which remains to be investigated.
Conclusions
Serum autoantibodies against the IFG-1R are present in one-fourth of GD patients, regardless of the presence of GO. Further functional studies are needed to investigate the significance of their inverse correlation with GO activity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Graves’ orbitopathy (GO) is a disfiguring and disabling condition observed in ~ 25–30% of patients with Graves’ hyperthyroidism and rarely in patients with hypothyroid autoimmune thyroiditis or in the absence of thyroid dysfunction [1,2,3]. The current view on GO pathogenesis is that the syndrome follows autoimmunity against orbital fibroadipose tissue, where the major autoantigen is the thyrotropic hormone (TSH) receptor (TSHR) [4].
Recent studies have provided evidence for a role of the insulin-like growth factor-1 receptor (IGF-1R) in the pathogenesis of GO [5, 6]. IGF-1R, together with its ligand IGF-1, is involved at various levels in the development and maintenance of mammalian tissues [5,6,7]. Normal subjects and individuals with autoimmune diseases seem to differ in several aspects of the IGF-1 pathway, suggesting its role in the loss of immune tolerance [8]. The hypothesis that the IGF-1R may be involved in the pathogenesis of GO derives from initial observations in which serum immunoglobulins (Igs) from patients with Graves’ disease (GD) were found to displace the binding of IGF-1 to the membrane of orbital fibroblasts [9]. The existence of antibodies directed against the IGF-1R was supported by subsequent studies in which Igs from patients with GD were found to induce the expression of T-cell chemoattractants in autologous fibroblasts derived from the thyroid, the orbit and the skin [10]. These Igs were later demonstrated to target the IGF-1R [11]. Following those observations, several attempts of detecting functional autoantibodies against the IGF-1R (IGF-1RAbs) led to somehow conflicting results [12,13,14,15,16,17,18,19]. Nevertheless, solid evidence of an interplay between the IGF-1R and the TSHR was provided in thyroid epithelial cells, orbital fibroblasts, and bone marrow-derived fibrocytes infiltrating the orbital tissues of GO patients [5], supporting a role of IGF-1R in the pathogenesis of GO. In addition, functional IGF-1R was found to be present in professional immune-competent cells, including lymphocytes (both B and T cells) and monocytes, suggesting that IGF-1R may play a role in the pathogenesis of GO not only in orbital tissues, but also at the immune system level [5]. Strong support to a role of IGF-1R derives from a recent, multicenter, randomized, double-blind, drug vs placebo, clinical trial, showing an impressing beneficial effect of Teprotumumab, a blocking monoclonal antibody against the IGF-1R, in patients with GO [19, 20], thereby opening new perspectives for GO treatment in addition to the current, both established and experimental, modalities [1, 22,23,24,25].
As mentioned above, the existence and the significance of IGF-1RAbs have been questioned [12,13,14,15,16,17,18,19]. Taking advantage of the recent development of a commercial assay for IGF-1RAb detection, we conducted the present cross-sectional study to investigate the presence of serum IGF-1RAbs in GD and in particular in GO, being the primary end-point the prevalence of positive serum IGF-1RAbs compared with healthy subjects and another autoimmune thyroid disease, namely autoimmune thyroiditis (AT).
Methods
Study design
The study was aimed at assessing IGF-1R-Abs in patients with GD, with or without GO, compared with healthy subjects and patients with AT in a cross-sectional investigation. The research design entailed the inclusion of consecutive patients with the above mentioned conditions, up to the achievement of a minimum number of 25 patients per group and/or to completion of the recruitment period, which was planned to cover at least 3 months.
Setting
The study was carried in a tertiary referral center. Patients were not selected, but included by consecutive sampling. The inclusion criteria adopted are reported below. GRD, II, GL, DR, AS and BM collected the data and recorded them in a database. The study was not blinded. Database validation procedures included allowed character checks, batch totals, missing records check, cardinality check, digits check, consistency check, control totals, cross-system consistency check, data type check, hash totals, limit check, logic check, presence check, range check, spelling and grammar check, and uniqueness check.
Participants
Inclusion criteria were (1) for GD: a history of hyperthyroidism, associated with previous or present detectable serum autoantibodies against the TSHR (TRAbs), (2) for AT: the presence of at least two of the following: (a) primary hypothyroidism, (b) detectable serum autoantibodies against thyroglobulin (TgAbs) or thyroperoxidase (TPOAbs), and (c) a hypoechoic pattern of the thyroid by ultrasound examination [26], (3) for healthy subjects: (a) the absence of present or past evidence of hyper- or hypothyroidism, (b) undetectable TgAbs, TPOAbs and TRABs, and (c) a normal thyroid by ultrasound examination, (4) for all patients: written, signed informed consent. The only exclusion criterion was the lack of informed consent. A total of 134 subjects who satisfied the inclusion criteria and evaded the exclusion criterion were enrolled in the period reported above.
Outcomes
The primary outcome of the study was the prevalence of positive serum IGF-1R-Abs in patients with GO, compared with healthy subjects, patients with GD without a clinically relevant GO, and patients with AT.
The secondary outcomes of the study were
-
1.
The serum concentrations of positive IGF-1R-Abs in patients with GO, compared with healthy subjects, patients with GD without GO, and patients with autoimmune thyroiditis;
-
2.
The relationship between serum IGF-1R-Abs (both levels and prevalence) and the clinical features of GO, especially GO activity, evaluated by means of the Clinical Activity Score (CAS) [1], as well as the relationship between serum IGF-1R-Abs (both levels and prevalence) and the treatment of GO with intravenous glucocorticoids.
-
3.
The relationship between serum IGF-1R-Abs (both levels and prevalence) and TgAbs, TPOAbs and TRAbs.
As reported previously [27], the presence of GO in GD was established in any patient who had at least one of the following eye features: (i) exophthalmometry ≥ 17 mm in women and ≥ 19 mm in men, based on measurements conducted for the normal population [28,29,30,31,32]; (ii) eyelid aperture ≥ 9 mm [26, 32]; (iii) CAS ≥ 1/7; (iv) presence of diplopia; (v) presence of corneal alterations; (vi) presence of GO-related alterations of the fundi; (vii) reduction in visual acuity that could be attributed to GO.
Sources of data and measurements
An ophthalmological evaluation was performed in all patients with GD including (i) exophthalmometry, (ii) measurement of eyelid aperture, (iii) evaluation of CAS, (iv) assessment of diplopia, (v) assessment of the corneal status, (vi) examination of the fundi, and (vii) measurement of visual acuity.
The following blood tests were performed in all study subjects: FT4 and FT3 (Vitros Immunodiagnostics, Raritan, NJ); TSH (Immulite 2000, Siemens Healthcare, Gwynedd, UK); TgAbs and TPOAbs (AIA-Pack TgAbs, Tosoh Bioscience, San Francisco, CA); and TRAbs (Brahms, Berlin, Germany).
IGF-1R-Abs were measured using a commercial ELISA (MyBioSource, San Diego, CA). Details on the assay are reported below (see “Results”). Recombinant, human, soluble IGF-1R used in inhibition experiments was purchased from MyBioSource.
Potential bias
To our knowledge, no previous data were available on the IGF-1R-Ab assay used here. To overcome this limitation, we evaluated the inter- and intra-assay variations and, to assess the assay specificity, we performed inhibition experiments using recombinant, human, soluble IGF-1R as detailed in “Results”.
The levels and the prevalence of TgAbs, TPOAbs and TRAbs are well known to fluctuate across the clinical history of patients, depending on the stage and the treatment of the diseases they are affected with [33]. If similar fluctuations occurred with IGF-1RAb, these may lead to underestimations of their levels and prevalence, especially in patients with GO. To overcome this possible bias, concerning GO, we included both untreated patients and patients treated with intravenous glucocorticoids.
Sample size
To our knowledge, the prevalence of positive serum IGF-1R-Abs has not been established with certainty. Minich et al. found positive tests for IGF-1R-Abs in 14% of patients with GO and 11% in healthy subjects [13]. Based on this investigation, we estimated that at least ten patients per group would have been needed to detect at least one subject with IGF-R-Abs. Therefore, we arbitrarily decided to recruit a minimum number of 25 subjects per group, which would have exceeded the above estimate. As a matter of fact, the number of subjects recruited over the screening period was even greater. Thus, a total of 134 subjects were studied, including 27 untreated GO patients, 27 GO patients treated with intravenous glucocorticoids (ivGC), 26 patients with GD without a clinically relevant GO, 27 patients with autoimmune thyroiditis, and 27 healthy subjects. The number of healthy controls was established to match the patients’ groups.
Study registration and informed consent
The study was registered at ClinicalTrials.gov (registration number: NCT03498417) and it was approved by the local Ethic Committee (Comitato Etico Regionale per la Sperimentazione Clinica della Regione Toscana; approval number: 13354_MARINO’). Signed informed consent was obtained from all patients enrolled in the study.
Quantitative variables
Numerical data with a normal distribution, which was assessed using the Shapiro–Wilks test, are presented as mean ± SD. The remaining numerical data are presented as median and IQR.
Statistical analyses
When appropriate, the following tests were performed: (1) Shapiro–Wilks test, (2) ANOVA, (3) Wilcoxon–Kruskal–Wallis rank sum (equivalent to Mann–Whitney test), (4) Chi-square, (5) Wilcoxon signed rank and (6) linear regression.
Results
Participants
We measured IGF-1R-Abs in 134 subjects, whose demographical and clinical data are reported in Table 1. The study population included 107 patients and 27 healthy subjects. The patients’ groups did not differ for sex distribution, but they had a significantly different age (P = 0.001 by ANOVA). Notably, no relationship was observed between age and prevalence or levels of IGF-1R-Abs (not shown). Among patients with GD, 54 had GO, 27 of whom had been treated with ivGC. Most of GD patients were on methimazole, but a minority of them (all with GO) had been previously treated with I131, thyroidectomy or both [34, 35], and were on levothyroxine (LT4) treatment for hypothyroidism. Among patients with autoimmune thyroiditis, 16 were on LT4 for primary hypothyroidism. The majority of subjects were euthyroid, even though FT3, FT4 and TSH values had a significantly different distribution across the study population, reflecting the different underlying thyroid conditions and the variable control of thyroid function in patients with GD and AT. These differences did not affect IGF-1-R-Abs, which did not correlate with thyroid hormones and TSH across the study population (not shown). None of the healthy subjects had positive circulating TgAbs, TPOAbs or TRAbs. As expected [33], TgAbs and TPOAbs were variably positive in patients with GD and in nearly all patients with AT. TRAbs were positive in the majority of patients with GD. Reflecting the different underlying thyroid conditions [33], the levels and the prevalence of TgAbs, TPOAbs and TRAbs had a significantly different distribution across the study population.
As reported in Table 2, on average the 54 patients with GO had a moderately severe, active eye disease, as defined by the guidelines of the European Group On Graves Orbitopathy (EUGOGO) [1], namely having two or more of the following: (1) lid retraction ≥ 2 mm, (2) moderate or severe soft tissue involvement or exophthalmos ≥ 3 mm above normal for race and gender, and (3) inconstant or constant diplopia.
Preliminary data: establishment of normal values and serum IGF-1R-Ab assay validation
To measure serum IGF-1R-Abs, we used a commercial ELISA. The assay is based on microplates coated with human recombinant IGF-1R, onto which serum samples are incubated, followed by a horseradish peroxidase-labeled goat anti-human IgG. In spite of our request, the company that manufactured the assay would not disclose the following information, as it was considered proprietary: (1) amount of antigen used for coating and (2) source of the standard curve. The reference value suggested by the manufacturer is 0–58.3 ng/ml.
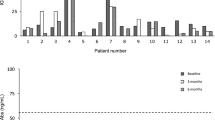
In our hands, the inter-assay variation was 4.3% and the intra-assay variation was 3.6%. As shown in Fig. 1a, in healthy subjects IGF-1R-Abs did not follow a normal distribution, as assessed by the Shapiro–Wilks test (P = 0.03 for likelihood of a non-normal distribution). Based on these findings, we established our own normal reference value below the 97th percentile, namely at 55.2 ng/ml. The use of the 97th percentile rather than of a lower percentile is based on the assumption that if IGF-1R-Abs were specific for GO, they would have been present in the normal population in not more than 1/1000 person, the estimated prevalence of GO in Europe [36].

Assay of serum antibodies against the insulin-like growth factor-1 receptor (IGF-1R-Abs): normal distribution and determination of the assay specificity. a Distribution of serum IGF-1R-Abs in 27 healthy subjects. P value was obtained by the Shapiro–Wilks test. b Effect of pre-incubation of serum samples with IGF-1R-Ab-free human serum, or with IGF-1R-Ab-free human serum plus recombinant human IGF-1R 50 μg/ml, on IGF-1R-Ab concentrations in eight serum samples with IGF-1R-Ab values above 55.2 ng/ml. Values presented as percent of the values above 55.2 ng/ml (the actual 0 concentration). P value was obtained by Wilcoxon signed rank
Of the 134 subjects tested, 21 had serum IGF-1R-Abs above the cut-off value of 55.2 ng/ml, all of whom with values also above the cut-off value of 58.3 ng/ml suggested by the assay manufacturer.
To our knowledge, no published data were available on the assay we used prior to this study. Therefore, to assess the assay’s specificity, we performed inhibition tests in eight positive samples. For this purpose, we used recombinant human IGF-1R at the arbitrary concentration of 50 μg/ml. Serum samples were pre-incubated for 1 h at 37 °C with IGF-1R diluted 1:2 in IGF-1R-Ab-free human serum, or with IGF-1R-Ab-free human serum without IGF-1R. As shown in Fig. 1b, IGF-1R-Ab values were reduced significantly (P = 0.03 by Wilcoxon signed rank) by pre-incubation with IgF1R, overall suggesting that the assay we used is specific for IGF-1R-Ab detection. Only in two samples there was no inhibition, presumably reflecting the relatively low concentration of the inhibitor.
Primary outcome data: prevalence of serum IGF-1R-Abs in the study population
Using the above mentioned cut-off value, positive tests for serum IGF-1R-Abs were found in 25% of patients with GD and in 3.7% of patients with AT (Fig. 2a). The distribution of IGF-1R-Ab positivity was significantly different across the three study groups (P = 0.0001 by Chi square), reflecting the greater prevalence of IGF-1R-Ab values above 55.2 ng/ml in patients with GD compared with healthy subjects (P = 0.003 by Chi square) and patients with AT (P = 0.006 by Chi square). Within patients with GD, the prevalence of positive serum IGF-1R-Abs was similar in those with a clinically relevant GO compared with those without GO. The prevalence of IGF-1R-Abs in patients with GO was greater than that of healthy subjects (P = 0.004 by Chi square) and of patients with AT (P = 0.007 by Chi square). None of the variables unrelated to diagnosis (age and sex) had any influence on the prevalence of positive serum IGF-1R-Abs (not shown).

Prevalence and levels of serum antibodies against the insulin-like growth factor-1 receptor (IGF-1R-Abs) in the study population. a Percentage prevalence of serum IGF-1R-Ab values ≥ 55.2 ng/ml in healthy subjects, patients with Graves’ disease, with or without Graves’ orbitopathy (GO), and patients with autoimmune thyroiditis. The number of positive samples is indicated. P values were obtained by Chi square. *P = 0.003 vs healthy subjects and P = 0.006 vs autoimmune thyroiditis; **P = 0.004 vs healthy subjects and P = 0.007 vs autoimmune thyroiditis; b concentrations (median and IQR) of serum IGF-1R-Abs in healthy subjects, patients with Graves’ disease, with or without GO, and patients with autoimmune thyroiditis. P values were obtained by Wilcoxon/Kruskal–Wallis. *P < 0.0001 vs healthy subjects and autoimmune thyroiditis; **P < 0.0001 vs healthy subjects and autoimmune thyroiditis
Secondary outcome data
1. Levels of serum IGF-1R-Abs in the study population.
As shown in Fig. 2b, serum concentrations of IGF-1R-Abs were significantly different across the study groups (P < 0.0001 by Wilcoxon/Kruskal–Wallis), reflecting higher concentrations in patients with GD (P < 0.0001 vs both healthy subjects and patients and AT, by Wilcoxon/Kruskal–Wallis). Within patients with GD, IGF-1R-Ab concentrations did not differ between those with or without a clinically relevant GO. IGF-1R-Ab serum levels in patients with GO were significantly greater than those of healthy subjects and patients with AT (P < 0.0001 in both cases, by Wilcoxon/Kruskal–Wallis)
2. Relationship between serum IGF-1R-Abs, the clinical features, and the treatment of GO.
Within patients with GO, there was no relationship between the percentage prevalence and the serum concentrations of IGF-1RAbs with GO duration, exophthalmometry, eyelid aperture, CAS, degree of diplopia, and visual acuity (not shown). However, as shown in Fig. 3, there was an inverse correlation between serum levels of IGF-1RAbs and CAS (R = − 0.376, 95% CI: from − 0.373 to − 0.631; P = 0.005 by linear regression, using Log10 for both parameters). There was no relationship between GO treatment and IGF-1RAb percentage prevalence and serum concentrations (not shown).

Correlation between serum antibodies against the insulin-like growth factor-1 receptor (IGF-1R-Abs) and the clinical activity score (CAS) in patients with Graves’ orbitopathy. R and P values were obtained by linear regression analysis
3. Relationship between serum IGF-1R-Abs and TgAbs, TPOAbs and TRAbs.
There was no relationship between the percentage prevalence of positive tests or the serum concentrations of TgAbs and TPOAbs with the percentage prevalence of positive tests and the serum concentrations of IGF-1RAbs (not shown). As expected from the differences in serum IGF-1R-Abs in patients with GD compared with the other study groups, subjects with serum TRAbs above the upper limit of the normal range had a greater prevalence of serum IGF-1R-Abs ≥ 55.2 ng/ml (P = 0.003 by Chi square) compared with subjects with undetectable TRAbs (Fig. 4a). In addition, as shown in Fig. 4b, serum levels of IGF-1R-Abs were greater in TRAb-positive than in TRAb-negative subjects (P < 0.0001 by Wilcoxon/Kruskal–Wallis).

Prevalence and levels of serum antibodies against the insulin-like growth factor-1 receptor (IGF-1R-Abs) according to the presence or absence of detectable serum anti-TSH-receptor antibodies (TRAbs) in the study population. a Percentage prevalence of serum IGF-1R-Ab values above 55.2 ng/ml according to the presence of serum TRAb values ≥ 1.5 IU/ml. The number of positive samples is indicated. P values were obtained by Chi square, b concentrations (median and IQR) of serum IGF-1R-Abs according to the presence of serum TRAb values ≥ 1.5 IU/ml. P values were obtained by Wilcoxon/Kruskal–Wallis
Discussion
The present study stemmed from recent observations suggesting a major involvement of the IGF-1R and possibly of autoimmunity against it in GO [1, 2]. Taking advantage of a newly developed ELISA for IGF-1R-Abs, we measured Igs recognizing the IGF-1R in patients with GD and GO. Our findings suggest that IGF-1R-Abs are more frequent and their levels higher in patients with GD, regardless of the presence of GO, compared with healthy subjects and patients with AT.
In our hands, the assay used appeared to be precise (very low inter- and intra-assay variations) and specific, as shown by the inhibitory effect exerted by recombinant soluble IGF-1R on binding of human Igs to IGF-1R-coated ELISA plates. The concentrations of IGF-1R-Abs in healthy subjects did not follow a, normal, Gaussian distribution, because of which we arbitrary established normal values below the 97th percentile, namely 55.2 ng/ml. The prevalence of serum samples with IGF-1R-Ab concentrations equal or above the latter value was significantly greater in patients with GD than in healthy subjects or patients with AT. In line with this observation, the serum concentrations of IGF-1R-Abs were significantly higher in GD than in the other two study groups. About one-fourth of GD patients had detectable serum IGF-1R-Abs, but there were no differences between those with GO or without a clinically relevant GO. In accordance with the observation in patients with GD, serum IGF-1R-Ab values ≥ 55.2 ng/ml were observed more frequently and their concentrations were higher in subjects with serum TRAbs above the normal limit, compared with those with negative serum TRAbs, TRAbs being highly specific marker of GD [33].
In patients with GO, there was no relationship between GO severity and IGF-1R-Abs, which, however, correlated inversely with CAS. The interpretation of this surprising observation requires further investigations. A very speculative hypothesis is that this inverse correlation may reflect a protective role of IGF-1R-Abs in GO, thereby paralleling the action of the monoclonal, blocking anti-IGF-1R antibody Teprotumumab, which was recently shown to exert a remarkable beneficial effect in GO patients compared with placebo [20, 21]. Clearly, any considerations on a possible protective action of IGF-1R-Abs in GO are preliminary and require confirmation by functional assays.
TRAbs have been reported to correlate with the clinical features of GO, including CAS [37], although not all of the studies on the subject have confirmed firmly this observation [34, 35, 38]. Here we did not find any correlation between TRAbs and CAS (not shown), which is somehow consistent with the observation of a direct correlation between TRAbs and IGF-1R-Abs, and of an inverse correlation between CAS and IGF-1R-Abs.
Our study militates in favor of the specific presence of autoantibodies against the IGF-1R in patients with GD, regardless of the presence of GO. Following the initial observation that Igs from GD patients can bind to the IGF-1-R [9, 11], several attempts have been made to confirm their presence in the bloodstream of GD patients, as well as to define their function and their relation to GO. Some studies have indicated that anti-IGF-1R Igs exist, are specific for GD and GO, and can activate the IGF-1R in thyroid cells and in orbital fibroblasts [10]. In this regard, our observation of IGF-1R-Abs in patients with GD, but not, or to a much lower extent, in those with AT, suggests that IGF-1R-Abs may be involved in thyroid cell growth, although the lack of functional data (see below) in the present study does not allow firm conclusions.
The functional role of anti-IGF-1R Igs in orbital fibroblasts is debated [12,13,14,15,16,17,18,19]. On the one hand, they have been postulated to play a pathogenetic role; on the other hand, the interplay between the IGF-1R and the TSHR may be activated by autoimmunity against the TSHR, whereas autoimmunity against the IGF-1R would not play a major role [15]. It is, however, established that the blocking anti-IGF-1R monoclonal antibody Teprotumumab exerts an inhibitory function on IGF-1R in cultured orbital fibroblasts and a beneficial effect in patients with GO [20], which, as mentioned above, may be in line with our observation of an inverse correlation between CAS and IGF-1R-Abs in GO patients.
The existence of serum antibodies against the IGF-1R with inhibiting properties was suggested by Minich et al., who demonstrated that serum anti-IGF-1R reduced the IGF-1-induced signaling in hepatocarcinoma HepG2 cells [13]. In that study, detectable IGF-1R-Abs, measured with a different method, were observed in 14% of GO patients, a proportion slightly lower than that we observed here. In contrast with our findings, they found detectable serum IGF-1R-Abs in 11% of normal subjects [13]. In addition, unlike in our study, they did not observe any correlation between CAS and IGF-1R-Abs in patients with GO. The different methods for IGF-1R-Ab measurement, the lack of experimental standardization, and the different patients sampling may explain these discrepancies.
A limitation of our study is that we did not perform functional assays to determine whether the serum IGF-1R-Abs we detected exert activating or a blocking effects in thyroid cells and/or in orbital fibroblasts, to investigate which we are planning further studies. Another limitation is that we did not assess the possible interference of serum IGF-1 in binding of serum anti-IGF-1R antibodies to IGF-R-coated plates. Thus, serum IGF-1 may in theory inhibit binding of antibodies to IGF-1R if both IGF-1 and antibodies recognized overlapping binding sites. In this regard, Minich et al. reported that IGF-1 does not exert any interference in their IGF-1R-Ab assay, which is quite reassuring [13]. Another limitation of our study is that patients were variably treated for their thyroid diseases, which may have affected IGF-1R-Abs.
In conclusion, serum autoantibodies against the IFG-1R are present in 25% of patients with GD, regardless of the presence of GO. In GO they may exert a protective action, but further functional studies are needed to establish whether this is the case.
References
Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, Marcocci C, Perros P, Salvi M, Wiersinga WM, European Group on Graves’ Orbitopathy (EUGOGO) (2016) The 2016 European Thyroid Association/European Group on Graves’ orbitopathy guidelines for the management of Graves’ orbitopathy. Eur Thyroid J 5:9–26
Piantanida E, Tanda ML, Lai A, Sassi L, Bartalena L (2013) Prevalence and natural history of Graves’ orbitopathy in the XXI century. J Endocrinol Investig 36:444–449
Leo M, Menconi F, Rocchi R, Latrofa F, Sisti E, Profilo MA, Mazzi B, Albano E, Nardi M, Vitti P, Marcocci C, Marinò M (2015) Role of the underlying thyroid disease on the phenotype of Graves’ orbitopathy in a tertiary referral center. Thyroid 25:347–351
Bahn RS (2015) Current insights into the pathogenesis of Graves’ ophthalmopathy. Horm Metab Res 47:773–778
Mohyi M, Smith TJ (2018) IGF-I receptor and thyroid-associated ophthalmopathy. J Mol Endocrinol 61:T29–T43
Smith TJ, Hegedüs L, Douglas RS (2012) Role of insulin-like growth factor-1 (IGF-1) pathway in the pathogenesis of Graves’ orbitopathy. Best Pract Res Clin Endocrinol Metab 26:291–302
Tsui S, Naik V, Hoa N, Hwang CJ, Afifiyan NF, Sinha Hikim A, Gianoukakis AG, Douglas RS, Smith TJ (2008) Evidence for an association between thyroid-stimulating hormone and insulin-like growth factor 1 receptors: a tale of two antigens implicated in Graves’ disease. J Immunol 181:4397–4405
Smith TJ, Tsai CC, Shih MJ, Tsui S, Chen B, Han R, Naik V, King CS, Press C, Kamat S, Goldberg RA, Phipps RP, Douglas RS, Gianoukakis AG (2008) Unique attributes of orbital fibroblasts and global alterations in IGF-1 receptor signaling could explain thyroid-associated ophthalmopathy. Thyroid 18:983–988
Weightman DR, Perros P, Sherif IH, Kendall-Taylor P (1993) Autoantibodies to IGF-1 binding sites in thyroid associated ophthalmopathy. Autoimmunity 16:251–577
Pritchard J, Horst N, Cruikshank W, Smith TJ (2002) Igs from patients with Graves’ disease induce the expression of T cell chemoattractants in their fibroblasts. J Immunol 168:942–950
Pritchard J, Han R, Horst N, Cruikshank WW, Smith TJ (2003) Immunoglobulin activation of T cell chemoattractant expression in fibroblasts from patients with Graves’ disease is mediated through the insulin-like growth factor I receptor pathway. J Immunol 170:6348–6354
Krieger CC, Place RF, Bevilacqua C, Marcus-Samuels B, Abel BS, Skarulis MC, Kahaly GJ, Neumann S, Gershengorn MC (2016) TSH/IGF-1 receptor cross talk in Graves’ ophthalmopathy pathogenesis. J Clin Endocrinol Metab 101:2340–2347
Minich WB, Dehina N, Welsink T, Schwiebert C, Morgenthaler NG, Köhrle J, Eckstein A, Schomburg L (2013) Autoantibodies to the IGF1 receptor in Graves’ orbitopathy. J Clin Endocrinol Metab 98:752–760
Wiersinga WM (2011) Autoimmunity in Graves’ ophthalmopathy: the result of an unfortunate marriage between TSH receptors and IGF-1 receptors? J Clin Endocrinol Metab 96:2386–2394
Krieger CC, Neumann S, Marcus-Samuels B, Gershengorn MC (2017) TSHR/IGF-1R cross-talk, not IGF-1R stimulating antibodies, mediates Graves’ ophthalmopathy pathogenesis. Thyroid 27:746–747
Smith TJ, Janssen JAMJL et al (2017) Response to Krieger et al. Re: “TSHR/IGF-1R cross-talk, not IGF-1R stimulating antibodies, mediates Graves’ ophthalmopathy pathogenesis” (Thyroid 2017;27:746–747). Thyroid 27:1458–1459
Neumann S, Gershengorn MC (2017) Rebuttal to Smith and Janssen. Thyroid 27:746–747. https://doi.org/10.1089/thy.2017.0281 (1459–1460)
Marcus-Samuels B, Krieger CC, Boutin A, Kahaly G, Neumann S, Gershengorn MC (2018) Evidence that Graves’ ophthalmopathy immunoglobulins do not directly activate IGF-1 receptors. Thyroid 28:650–655
Varewijck AJ, Boelen A, Lamberts SW, Fliers E, Hofland LJ, Wiersinga WM, Janssen JA (2013) Circulating IgGs may modulate IGF-I receptor stimulating activity in a subset of patients with Graves’ ophthalmopathy. J Clin Endocrinol Metab 98:769–776
Smith TJ, Kahaly GJ, Ezra DG, Fleming JC, Dailey RA, Tang RA, Harris GJ, Antonelli A, Salvi M, Goldberg RA, Gigantelli JW, Couch SM, Shriver EM, Hayek BR, Hink EM, Woodward RM, Gabriel K, Magni G, Douglas RS (2017) Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med 376:1748–1761
Piantanida E, Bartalena L (2017) Teprotumumab: a new avenue for the management of moderate-to-severe and active Graves’ orbitopathy? J Endocrinol Invest 40:885–887
Bartalena L, Veronesi G, Krassas GE, Wiersinga WM, Marcocci C, Marinò M, Salvi M, Daumerie C, Bournaud C, Stahl M, Sassi L, Azzolini C, Boboridis KG, Mourits MP, Soeters MR, Baldeschi L, Nardi M, Currò N, Boschi A, Bernard M, von Arx G, Perros P, Kahaly GJ (2017) Does early response to intravenous glucocorticoids predict the final outcome in patients with moderate-to-severe and active Graves’ orbitopathy? J Endocrinol Investig 40:547–553
Rotondo Dottore G, Torregrossa L, Caturegli P, Ionni I, Sframeli A, Sabini E, Menconi F, Piaggi P, Sellari-Franceschini S, Nardi M, Latrofa F, Vitti P, Marcocci C, Basolo F, Marinò M (2018) Association of T and B cells infiltrating orbital tissues in Graves orbitopathy with Graves orbitopathy activity. A possible explanation for GO response to immunosuppressive treatments. JAMA Ophthalmol 136:613–619
Sellari-Franceschini S, Rocchi R, Marinò M, Bajraktari A, Mazzi B, Fiacchini G, Lepri P, Dallan I, Vitti P, Marcocci C (2018) Rehabilitative orbital decompression for Graves’ orbitopathy: results of a randomized clinical trial. J Endocrinol Investig (in press)
Kahaly GJ, Riedl M, König J, Pitz S, Ponto K, Diana T, Kampmann E, Kolbe E, Eckstein A, Moeller LC, Führer D, Salvi M, Curro N, Campi I, Covelli D, Leo M, Marinò M, Menconi F, Marcocci C, Bartalena L, Perros P, Wiersinga WM, European Group on Graves’ Orbitopathy (EUGOGO) (2018) Combined mycophenolate + prednisolone therapy is more effective than prednisolone in active and moderate-to-severe Graves’ orbitopathy—a randomized, observer blind, multicenter trial. Lancet Diabetes Endocrinol 6:287–298
Profilo MA, Sisti E, Marcocci C, Vitti P, Pinchera A, Nardi M, Rocchi R, Latrofa F, Menconi F, Altea MA, Leo M, Rago T, Marinò M (2013) Thyroid volume and severity of Graves’ orbitopathy. Thyroid 23:97–102
Sabini E, Mazzi B, Profilo MA, Mautone T, Casini G, Rocchi R, Ionni I, Menconi F, Leo M, Nardi M, Vitti P, Marcocci C, Marinò M (2018) Serum high cholesterol is a novel risk factor for Graves’ orbitopathy (GO): results of a cross-sectional study. Thyroid 28:386–394
Mourits MP, Lombardo SH, van der Sluijs FA, Fenton S (2004) Reliability of exophthalmos measurement and the exophthalmometry value distribution in a healthy Dutch population and in Graves’ patients. An exploratory study. Orbit 23:161–168
Bilen H, Gullulu G, Akcay G (2007) Exophthalmometric values in a normal Turkish population living in the northeastern part of Turkey. Thyroid 17:525–528
Kashkouli MB, Nojomi M, Parvaresh MM, Sanjari MS, Modarres M, Noorani MM (2008) Normal values of Hertel exophthalmometry in children, teenagers, and adults from Tehran, Iran. Optom Vis Sci 85:1012–1017
Beden U, Ozarslan Y, Oztürk HE, Sönmez B, Erkan D, Oge I (2008) Exophthalmometry values of Turkish adult population and the effect of age, sex, refractive status, and Hertel base values on Hertel readings. Eur J Ophthalmol 18:165–171
Chan W, Madge SN, Senaratne T, Senanayake S, Edussuriya K, Selva D, Casson RJ (2009) Exophthalmometric values and their biometric correlates: the Kandy Eye Study. Clin Exp Ophthalmol 37:496–502
Marcocci C, Marinò M (2005) Thyroid directed antibodies. In: Braverman LE, Utiger RD (eds) Werner and Ingbar’s the thyroid: a fundamental and clinical text, 9th edn. Lippincott, Williams & Wilkins, Philadelphia, pp 360–372
Leo M, Marcocci C, Pinchera A, Nardi M, Megna L, Rocchi R, Latrofa F, Altea MA, Mazzi B, Sisti E, Profilo MA, Marinò M (2012) Outcome of Graves’ orbitopathy after total thyroid ablation and glucocorticoid treatment: follow-up of a randomized clinical trial. J Clin Endocrinol Metab 97:E44–48
Menconi F, Leo M, Vitti P, Marcocci C, Marinò M (2015) Thyroid ablation in Graves’ orbitopathy. J Endocrinol Investig 38:809–815
Perros P, Hegedüs L, Bartalena L, Marcocci C, Kahaly GJ, Baldeschi L, Salvi M, Lazarus JH, Eckstein A, Pitz S, Boboridis K, Anagnostis P, Ayvaz G, Boschi A, Brix TH, Currò N, Konuk O, Marinò M, Mitchell AL, Stankovic B, Törüner FB, von Arx G, Zarković M, Wiersinga WM (2017) Graves’ orbitopathy as a rare disease in Europe: a European Group On Graves’ Orbitopathy (EUGOGO) position statement. Orphanet J Rare Dis 12:72
Eckstein AK, Plicht M, Lax H, Neuhäuser M, Mann K, Lederbogen S, Heckmann C, Esser J, Morgenthaler NG (2006) Thyrotropin receptor autoantibodies are independent risk factors for Graves’ ophthalmopathy and help to predict severity and outcome of the disease. J Clin Endocrinol Metab 91:3464–3470
Sisti E, Menconi F, Leo M, Profilo MA, Mautone T, Mazzi B, Rocchi R, Latrofa F, Nardi M, Vitti P, Marcocci C, Marinò M (2015) Long-term outcome of Graves’ orbitopathy following high-dose intravenous glucocorticoids and orbital radiotherapy. J Endocrinol Investig 38:661–668
Acknowledgements
The study was funded by the University of Pisa (Fondi di Ateneo, to MM).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All diagnostic and therapeutic procedures performed in this study were in accordance with ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the local Ethic Committee (Comitato Etico Regionale per la Sperimentazione Clinica della Regione Toscana; approval number: 13354_MARINO’).
Informed consent
Informed consent was obtained from the individual participant included in the study.
Rights and permissions
About this article

Cite this article
Marinò, M., Rotondo Dottore, G., Ionni, I. et al. Serum antibodies against the insulin-like growth factor-1 receptor (IGF-1R) in Graves’ disease and Graves’ orbitopathy. J Endocrinol Invest 42, 471–480 (2019). https://doi.org/10.1007/s40618-018-0943-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-018-0943-8