
Abstract
Purpose
This study aims at identifying behavioural and psychological pretreatment predictors of 12- and 36-month weight loss in women with overweight/obesity enrolled in a behavioural weight management intervention.
Methods
A sample of 221 women participated in a randomized controlled trial on weight management (n12 month = 184; n36 month = 156). Multiple linear regressions were used to identify pretreatment predictors of successful weight loss, separately for intervention and control groups. Completers-only and baseline observation carried forward analyses were performed. This study is a secondary analysis of data from the ‘Promotion of Exercise and Health in Obesity’ randomized controlled trial.
Results
Fewer weight loss attempts in the last year positively predicted weight loss at 12 months in the intervention group, explaining 6% of the variance. At 36 months, in the intervention group, 20.2% of the variance in weight change was explained by lower eating disinhibition and higher weight-related quality of life in completers-only analyses, while baseline observation carried forward analyses explained only 9.8% of the variance in weight change via higher self-esteem and lower weight loss expectations. In the control group, higher exercise self-efficacy and a more internal weight locus of control predicted weight loss at 36 months, explaining 13.9% of the variance (completers-only analyses).
Conclusions
Previous weight loss attempts were identified as the most efficient pretreatment predictor of 12-month weight loss. Eating disinhibition, weight-related quality of life, self-esteem, weight loss expectations, exercise self-efficacy, and weight locus of control seem to be key factors for long-term success.
Level of evidence
Level I, randomized controlled trial.
Clinical trial registration
ClinicalTrials.gov identifier NCT00513084.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Overweight and obesity pose a major public health threat, due to their well-documented contribution to a wide range of chronic diseases [1]. Annually, 42% of adults worldwide try to lose weight and 23% try to maintain weight loss (WL) [2]. However, many of these individuals will not achieve success, in part due to the presence of certain unfavourable behavioural and psychological characteristics. A better understanding of which of these behavioural and psychological factors are more predictive of success, how they vary between individuals and how they can be overcome, can lead to the development of new strategies with better results [3].
Identifying pretreatment (i.e., baseline) characteristics that predict successful WL can give important clues toward more individualized interventions based on these characteristics, increasing individuals’ probabilities of success [4, 5]. Carraça et al. found that the previous WL attempts were the most consistent pretreatment predictor of WL; variables such as body image, self-esteem, or general quality of life were sometimes, but not consistently correlated with WL; and several other variables were consistently identified as non-predictors (e.g., eating disinhibition, cognitive eating restraint, and depression symptoms) [4]. In a recent systematic review on demographic, behavioural, psychological, social, and physical environmental determinants of WL maintenance, Varkevisser et al. found moderate evidence supporting the non-predictive effect of baseline physical activity level on WL maintenance, while all the other variables evaluated at baseline (e.g., initial BMI and cognitive eating restraint) showed inconsistent results, precluding firm conclusions regarding their predictive role [6]. Dalle Grave et al. found that novelty-seeking and self-directedness traits appear to be pretreatment predictors of short-term WL (≤ 6 months), and pretreatment persistence and novelty-seeking traits may be related to long-term WL maintenance (≥ 12 months) [7].
There is a dearth of studies assessing these variables as pretreatment predictors of 12-month WL and beyond. This study contributes to filling this gap by identifying behavioural and psychological pretreatment predictors of 12- and 36-month WL in women with overweight and obesity involved in a behavioural weight management intervention.
Methods
Study design and intervention
The present study is a secondary analysis of data obtained from the ‘Promotion of Exercise and Health in Obesity’ randomized controlled trial, which consisted of a 12-month behaviour change intervention and a 24-month follow-up with no intervention. Detailed information about the trial can be found elsewhere [8]. Briefly, the control group received a general health education curriculum including topics such as preventive nutrition, stress management, self-care, and effective communication skills, while the intervention group received a program based on self-determination theory [9], which included contents on physical activity, nutrition, and behaviour change, with a special focus on increasing autonomous regulation for exercise and weight control.
Participants
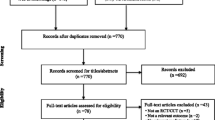
Participants were recruited from the community, mostly through media advertisements. A total of 258 women completed initial assessments and were randomized to either an intervention or control group. Thirty-seven women were excluded, because they (1) started pharmacological treatment susceptible of affecting weight (n = 13), (2) were diagnosed with severe illness/injury (n = 4), (3) entered menopause (n = 9), or (4) became pregnant (n = 11). Thus, 221 participants were eligible. There was an 83% overall retention at 12 months (n = 184) and 71% at 36 months (n = 156). For the 36-month analyses reported herein, 2 women without 36-month anthropometric data were excluded, leaving a final sample of 154 women. More detailed information on retention/dropouts can be found elsewhere [8].
Measurements
At baseline, participants completed a comprehensive battery of validated psychometric instruments [8, 10], herein categorized in the four groups outlined below. In general, higher scores represent higher manifestations of each psychometric variable except when specifically indicated.
Eating behaviour
Eating self-efficacy was assessed with the 20-item Weight Management Efficacy Questionnaire [11] (α = 0.94). External and emotional eating were assessed with the Portuguese validated version [12] of the 33-item Dutch Eating Behaviour Questionnaire [13] (10-items; α = 0.86 and 13-items; α = 0.95, respectively). The 51-item Three-Factor Eating Questionnaire [14, 15] assessed flexible cognitive restraint (7 items; α = 0.61), rigid cognitive restraint (7 items; α = 0.53), eating disinhibition (16 items; α = 0.79), and perceived hunger (14 items; α = 0.80).
General and exercise motivation
Exercise intrinsic motivation was assessed with the Intrinsic Motivation Inventory [16] (α = 0.86). Exercise self-efficacy was assessed with the Portuguese validated version [17] of the Self-Efficacy for Exercise Behaviours scale [18] (α = 0.83). Perceived barriers to exercise were assessed with an 11-item scale (α = 0.75) selected from the original 14-item Exercise Perceived Barriers scale [19]. General self-determination was assessed with the Portuguese validation [20] of the 10-item Self-determination Scale [21] (α = 0.83).
Psychological well-being and quality of life
Body shape concerns in terms of a dysfunctional investment in appearance were assessed using the 34-item Body Shape Questionnaire [22] (α = 0.94). The degree to which people become anxious when others observe or evaluate their physique was assessed using the 12-item Social Physique Anxiety Scale [23] (α = 0.85). Depression symptoms (cognitive, affective, and somatic) were assessed with the Portuguese validated version [24] of the 21-item Beck Depression Inventory I [25] (α = 0.87). Self-esteem was assessed using the Portuguese validated version [26] of the 10-item Rosenberg Questionnaire [27] (α = 0.86). Weight-related quality of life was assessed through the 31-item Portuguese validated version of the Impact of Weight on Quality of Life-Lite (α = 0.93) [28, 29]. Higher scores reflect lower perceived impact of weight on quality of life.
Weight-related
Weight locus of control was assessed with the Stotland and Zuroff scale [30]. Four items were excluded to improve internal consistency of the scale (α = 0.86). This instrument distinguishes more internal from more external locus of control. Previous WL attempts were assessed with the questions “How many times did you try to lose weight?” and “(…), during the last year?”. These two items were used as two independent variables and intended to assess how often participants engaged in WL attempts during their lifetime and in the last year. WL expectations were assessed using the question: “Realistically, considering everything (…) how many kg do you think you will be able to lose in the following year in the program?”. The percentage in relation to the baseline weight (before the beginning of the intervention phase) was calculated, with higher percentages reflecting lower outcome expectations.
Anthropometry
Body weight was measured twice at each assessment point (baseline, 12 and 36 months), using an electronic scale calibrated on site and accurate to 0.1 kg (SECA, Hamburg, Germany). Height was measured with a balance-mounted stadiometer to the nearest 0.1 cm. Initial BMI was calculated. Weight outcomes were expressed as weight change from baseline to 12 and 36 months. Negative values correspond to WL.
Statistics and data analysis
Statistical analyses were conducted using the IBM SPSS. The significance level was set at p < 0.05. Descriptive results are expressed in terms of [Mean ± SD (Min; Max)] for continuous variables and relative frequencies for categorical variables.
Analyses were performed separately for the intervention and control groups. This approach was taken because pretreatment predictors may act as moderators of the impact of the intervention phase on weight change and, therefore, have lower chances to emerge as significant if only analysed in the intervention group. It is important to note though that the term ‘pretreatment predictor’, especially when applied to the control group, should be interpreted as a baseline characteristic that was present before the beginning of the intervention study phase, independently of the random group allocation.
Analyses were performed for all participants who completed the 12-month and 36-month assessments (completers-only analyses). In addition, intention-to-treat analyses using the Baseline Observation Carried Forward (BOCF) method were performed, so that the identification of baseline predictors also took into account non-completers (which could have specific characteristics more prone to unfavourable results). BOCF was used because 46 (68%) non-completers did not report the reason why they quit the study; therefore, one may presume that their weight returned to the baseline observation. Moreover, BOCF increases the sample size and protects against type I and type II errors [31]. This method was previously used in other similar studies [32].
All variables were tested for normality using the Kolmogorov–Smirnov test, kurtosis, and skewness values. Pearson’s (for normally distributed variables) and Spearman’s (for non-normally distributed variables) correlations were used to examine associations between the independent variables and weight change at 12 and 36 months. Since Pearson correlations are robust against deviations from normal distribution in moderately large samples [31] and the differences between Pearson and Spearman correlation coefficients for the non-normally distributed variables were minimal, only the parametric results were reported.
Weight changes (i.e., the dependent variables) were expressed by baseline-residualized scores, where the 12- or 36-month value was regressed onto the baseline value, to remove the baseline weight effect from the weight difference outcome. This method protects against overcorrection of the post by the pre-score when using a subtraction score [33].
The independent variables examined were selected on the basis of theoretical considerations and systematic empirical reviews on weight control [4]. Significant correlates were included in multiple linear regression models (stepwise method) to determine the best possible predictive model in each group. Since age, education level, and marital status were not correlated with weight differences at 12 or 36 months, these variables were not included as potential confounding factors in the regression models. Only the most efficient models for both the intervention and control groups were reported.
Results
Women who entered the study (n = 221) had a mean age of 37.64 ± 6.98 years, a mean height of 1.61 ± 0.06 m, a mean weight of 81.90 ± 11.95 kg, and a mean BMI of 31.58 ± 4.13 kg/m2. There were no differences between intervention and control groups regarding baseline characteristics (p > 0.05; see supplementary material). The main effects of the intervention are described in detail elsewhere [5]. In brief, participants in the intervention group lost − 6.03 ± 5.3 kg vs. − 1.50 ± 4.1 kg in the control group (p < 0.001) at the end of the intervention phase; and − 3.06 ± 6.1 kg vs. − 1.00 ± 5.8 kg (p = 0.040) at the end of the follow-up phase.
Table 1 shows bivariate correlations between baseline psychological and behavioural variables and 12- and 36-month weight change for all participants and for completers only. At the end of the intervention phase (12 months), fewer WL attempts in the past year [1.14 ± 1.27 (0; 6)] were positively correlated with WL in the intervention group, in both completers-only and BOCF analyses. At the end of the follow-up phase (36 months), several variables were significantly associated with weight change, in the expected direction. In the intervention group, lower levels of eating disinhibition [9.64 ± 3.59 (1; 16)], lower social physique anxiety [39.29 ± 7.57 (20; 59)], lower WL expectations [86.22 ± 6.33 (68; 98)], higher self-esteem [33.08 ± 4.52 (20; 40)], and higher weight-related quality of life [60.07 ± 16.40 (32; 105)] were positively associated with WL in both completers-only and BOCF analyses. Lower levels of perceived hunger [7.01 ± 3.30 (1; 14)] and fewer global WL attempts [4.97 ± 4.58 (1; 30)] were positively associated with 36-month WL only in completers. In the control group, higher levels of exercise self-efficacy [38.93 ± 4.94 (27; 50)], lower exercise perceived barriers [25.33 ± 6.39 (9; 41)], higher general self-determination [36.01 ± 5.77 (22; 50)], and a more internal weight locus of control [63.27 ± 6.44 (48; 79)] were positively associated with WL in the whole sample and in completers-only. Higher levels of exercise intrinsic motivation [56.51 ± 9.42 (30; 75)] were positively associated with 36-month WL in completers-only analyses.
Table 2 shows stepwise multiple regression results regarding the prediction of 12- and 36-month weight change for both intervention and control groups.
Regarding the predictive analyses in the intervention group, WL attempts in the past year explained about 6% of the 12-month weight change variance in both completers-only and BOCF analyses. A complementary (post hoc) comparison of previous attempts’ tertiles—0 attempts (n = 31), 1 attempt (n = 38), and ≥ 2 attempts (n = 24)—revealed significant differences in 12-month weight change, favouring fewer attempts (p = 0.05). The 36-month prediction model for completers-only was able to explain 20.2% of the variance in weight change, which was predicted by lower eating disinhibition and higher weight-related quality of life. When using the BOCF method, only 9.8% of the variance in weight change was explained by self-esteem and WL expectations.
In the control group, 36-month weight change was predicted by higher exercise self-efficacy and more internal weight locus of control in those participants completing the intervention phase (adjusted R2 = 13.9%). Using the BOCF method, only exercise self-efficacy emerged as a significant predictor, explaining 4.8% of the variance in weight change.
Discussion
This study sought to identify effective behavioural and psychological pretreatment predictors of 12- and 36-month WL. At the end of the intervention phase (12 months), fewer WL attempts in the past year predicted higher WL in the intervention group. At the end of the follow-up phase (36 months), lower eating disinhibition, higher weight-related quality of life, higher self-esteem, and lower WL expectations emerged as significant pretreatment predictors of WL in the intervention group. In the controls, higher exercise self-efficacy and more internal weight locus of control predicted more favourable weight outcomes. To our knowledge, this is the first study identifying pretreatment predictors of longer term WL (i.e., at the end of a 24-month follow-up with no intervention) among women with overweight and obesity enrolled in a behavioural weight management intervention, not only in completers, but also including non-completers. This study’s findings may, therefore, assume particular importance toward the improvement of intervention’s efficacy and clinical practice.
Fewer WL attempts in the past year emerged as a significant predictor of 12-month weight change in the intervention group. This is in line with prior research identifying fewer self-reported WL attempts as the most consistent pretreatment predictor of successful weight control [4]. A potential explanation on why more previous weight control efforts might impair future weight control include a history of recurrent dieting attempts that could be related to a psychological profile that is more vulnerable to failure because of a continuous increase in frustration regarding the failed attempts and a parallel decrease in effort and compliance with diet and physical activity. Other hypotheses might be related to a genetic or physiological predisposition toward weight gain, or with an obsession with food derived from repeated and restrictive dieting attempts [4]. Given that the previous WL attempts are an unchangeable pretreatment feature, which might reflect a “natural individual resistance” to WL and its maintenance, practitioners would do well to assess the previous WL attempts at the beginning of behavioural WL interventions, to identify individuals with lower likelihood of success, and be able to tailor the intervention program to their needs.
Lower eating disinhibition and higher weight-related quality of life positively predicted 36-month weight change in the intervention group for those completing the follow-up phase. However, these findings are not in line with the most recent systematic reviews identifying eating disinhibition as a consistent non-predictor of weight control. Regarding the predictive role of weight-related quality of life, prior research has shown contradictory results, preventing reliable conclusions due to the lack of consistent evidence [4, 6]. Considering that, presumably, no other long-term studies have explored this feature and that quality of life might play an important role in individuals’ compliance with their weight management process in the long term, further studies are needed.
Lower WL expectations and higher self-esteem positively predicted 36-month WL in the intervention group when non-completers were also considered in the analyses (BOCF). These results are somewhat contradicted by the most recent review on pretreatment predictors of weight control [4]. The fact that only 36-month WL (and not 12 months) was predicted by lower WL expectations and higher self-esteem may suggest that, in the short term, higher WL expectations and lower self-esteem do not represent a hazard to WL, while both can hinder the process in the long term. Subjects who have higher WL expectations or lower self-esteem may make more efforts to change their behaviours, and therefore, achieve a higher WL in the short term, which can be motivating. However, in the long run, this effort may not be sustainable and can even be deleterious and counterproductive. In addition, in fact, most studies reviewed by Carraça et al. that analysed the predictive role of WL expectations were short-term studies, and only one long-term study evaluated self-esteem [4]. For instance, Dalle Grave et al. identified higher WL expectations as a pretreatment predictor of dropout in an observational study with 36-month follow-up [34].
Higher exercise self-efficacy predicted 36-month WL in the control group; however, it was not predictive in the intervention group. This is in line with the findings of the most recent systematic review on pretreatment predictors of WL in individuals that have received a weight management intervention [4]. This is not surprising given that most interventions tend to produce improvements in individuals’ exercise self-efficacy.
A more internal weight locus of control also predicted 36-month weight change in the control group, but only in completers-only analyses. This finding is corroborated by previous studies using the same scale to assess this construct [35], although the use of different scales has generated mixed predictive effects [4].
Several variables were identified as non-significant predictors in the current study (e.g., emotional eating, external eating, and depressive symptoms). Some of them were also previously classified as non-significant predictors [4, 6, 36], while for others, evidence is mixed (e.g., eating self-efficacy and body shape concerns) or insufficient (e.g., bulimic symptoms) [4, 6]. Nevertheless, it is important to state that even if a variable is a consistent non-pretreatment predictor of weight control, it does not mean that the change in that same variable during the treatment phase cannot be a significant predictor of weight control (e.g., an increase in cognitive eating restraint has been shown to significantly predict weight loss) [37]. In addition, indeed, in the current trial, there was an improvement in many psychological and behavioural factors at 12 and 36 months [8, 38], which might explain the lack of significant baseline predictive effects for some of these variables.
Interestingly, long-term prediction models explained higher portions of variance in WL, which is uncommon because of the expected changes in behavioural and psychological variables throughout the treatment and/or maintenance phases, derived not only from the impact of the interventions and associated weight changes, but also from personal adaptations [36]. The higher explained variance may be due to the intervention program, which covered a wide range of topics, like increasing physical activity and energy expenditure, adopting a consistent diet with a moderate energy deficit, and integrating the regulation of these behaviours with one’s sense of self and one’s values and goals for supporting WL; all aspects that could have potentiated or inhibited the effect of the different baseline predictors. Moreover, the fact that the significant pretreatment predictors of 12- and 36-month WL differed may reflect distinct behavioural and psychological features in each study phase (intervention vs. follow-up with no intervention) and thus for short- and long-term weight control. These findings could inform the design of future WL and WL maintenance interventions. It is also important to highlight that the reasons for the differences found between the 12- and 36-month outcomes could result from the passage of time, or merely be due to the different study phase participants were in at the time of assessment (intervention phase vs. follow-up phase with no intervention).
Completers-only and BOCF analyses led to the identification of different pretreatment predictors, reinforcing the importance of performing both types of analyses. These findings suggest that non-completers might have been less responsive to treatment, and thus have dropped-out of the study, (potentially) because of their higher eating disinhibition levels and lower perceived weight-related quality of life; factors that were only predictive of success in completers (i.e., lower disinhibition and higher weight-related quality of life resulted in more favourable weight outcomes). This information is of great relevance to improve future interventions’ efficacy, highlighting that both these aspects should be enhanced in this type of intervention.
The fact that different pretreatment predictors of WL were found for the intervention and control groups supports the hypothesis that searching for universal pretreatment predictors of WL may not bring new insights on how to improve short- and long-term WL, given that the intervention itself can mask or attenuate the effect of potential pretreatment predictors, depending on whether they are addressed or not during the intervention. Perhaps, the main reason why previous WL attempts are the only consistent universal pretreatment predictor of weight control so far [4] is because it is an unmodifiable factor.
Limitations
The self-selected, homogeneous sample of women with overweight and obesity included in the current study may preclude generalization to other populations. For instance, men can display different predictors, as reported by Sasdelli et al. for variables as stress, anxiety, depression, and self-confidence [39]. Furthermore, most women participating in this study were overweight or class I obesity (79%), which may affect their psychological and behavioural characteristics. Results should also be interpreted, considering that the modest weight changes achieved by participants throughout the program. This study did not evaluate physiological features as predictors of short- and long-term WL, which can have important interactions with factors from the behavioural and psychological domains. In fact, interventions that include a strong focus on physical activity lead to a variety of individual responses, which can be explained by behavioural and physiological adaptations [40]. In addition, these kinds of WL programs are often searched by individuals who already tried to lose weight following a wide variety of commercial programs; thus, this sample may be composed of a large proportion of chronic dieters. It is also necessary to take into account that given this study’s sample size, the high number of variables explored, and the absence of multiple testing corrections, these results should be used and interpreted with caution due to the high risk of type I errors.
Conclusion
This study identified fewer previous WL attempts as a consistent predictor of short-term (12-month) WL, and several other variables as pretreatment predictors of long-term (36-month) WL, including eating disinhibition, weight-related quality of life, self-esteem, WL expectations, exercise self-efficacy, and weight locus of control. Due to the scarcity of long-term randomized controlled trials aiming at identifying long-term pretreatment predictors of WL among women with overweight and obesity, these findings are especially important, potentially posing a benchmark for future research and practice.
It would be important that all pretreatment predictors discussed in this paper continue to be tested, to generate new hypotheses and create better and more complete WL prediction models. This will not only help treatment-seeking populations with overweight/obesity (in particular women) be aware of more features that can be important in their personal weight control process, but also help practitioners select the most appropriate information to evaluate at the beginning of treatment, and subsequently allocate their patients to the best treatment option.
Data availability
The data sets generated during the current study are available from the corresponding author on reasonable request.
References
Kopelman P (2007) Health risks associated with overweight and obesity. Obes Rev 8:13–17. https://doi.org/10.1111/j.1467-789X.2007.00311.x
Santos I, Sniehotta FF, Marques MM, Carraça EV, Teixeira PJ (2017) Prevalence of personal weight control attempts in adults: a systematic review and meta-analysis. Obes Rev 18:32–50. https://doi.org/10.1111/obr.12466
MacLean PS, Wing RR, Davidson T, Epstein L, Goodpaster B, Hall KD et al (2015) NIH working group report: innovative research to improve maintenance of weight loss. Obesity 23:7–15. https://doi.org/10.1002/oby.20967
Carraça EV, Santos I, Mata J, Teixeira PJ (2018) Psychosocial pretreatment predictors of weight control: a systematic review update. Obes Facts 11:67–82. https://doi.org/10.1159/000485838
Elfhag K, Rossner S (2005) Who succeeds in maintaining weight loss? A conceptual review of factors associated with weight loss maintenance of weight loss. Obes Rev 6:67–85. https://doi.org/10.1111/j.1467-789X.2005.00170.x
Varkevisser RD, van Stralen MM, Kroeze W, Ket JC, Steenhuis IH (2019) Determinants of weight loss maintenance: a systematic review. Obes Rev 20:171–211. https://doi.org/10.1111/obr.12772
Dalle Grave R, Calugi S, El Ghoch M (2018) Are personality characteristics as measured by the Temperament and Character Inventory (TCI) associated with obesity treatment outcomes? A systematic review. Curr Obes Rep 7:27–36. https://doi.org/10.1007/s13679-018-0294-y
Silva MN, Vieira NV, Coutinho SR, Minderico CS, Matos MG, Sardinha LB et al (2010) Using self-determination theory to promote physical activity and weight control: a randomized controlled trial in women. J Behav Med 33:110–122. https://doi.org/10.1007/s10865-009-9239-y
Ryan RM, Deci EL (2017) Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness, 1st edn. Guilford Press, New York
Silva MN, Teixeira PJ, Vieira PN, Minderico CS, Castro M, Coutinho S et al (2007) Programa P.E.S.O—Promoção do Exercício e Saúde na Obesidade: Metodologia e descrição da intervenção. ENDO—Endocrinologia. Diabetes Obes 16:17–28
Machado P, Gonçalves S, Martins C, Soares I (2001) The Portuguese version of the eating disorders inventory: evaluation of its psychometric properties. Eur Eat Disord Rev 9:43–52. https://doi.org/10.1002/erv.359
Viana V, Sinde S (2003) Estilo Alimentar: adaptação e validação do questionário holandês do comportamento alimentar. Psicologia Teoria Investigação e Prática 8:59–71
van Strien T, Frjiters E, Bergers P, Defares P (1986) The Dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int J Eat Disord 5:295–315
Stunkard AJ, Messick S (1985) The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J Psychosom Res 29:71–83
Westenhoefer J, Stunkard AJ, Pudel V (1999) Validation of the flexible and rigid control dimensions of dietary restraint. Int J Eat Disord 26:53–64
McAuley E, Duncan T, Tammen VV (1989) Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: a confirmatory factor analysis. Res Q Exerc Sport 60:48–58
Sousa H, Rosa J (2002) Validação preliminar da escala de auto-eficácia para o exercício. Psicologia do Desporto e Atividades Físicas ULHT, Lisbon
Sallis JF, Pinski MA, Grossman RB, Patterson TL, Nader PR (1988) The development of self-efficacy scales for health-related diet exercise behaviors. Health Educ Res 3:283–292
Steinhardt MA, Dishman RH (1989) Reliability and validity of expected outcomes and barriers for habitual physical activity. J Occup Med 31:536–546
Silva MN, Vieira PN, Minderico CS, Castro MM, Coutinho SR, Santos TC, Teixeira PJ (2007) Testing a Portuguese self-determination theory-based psychometric battery. In: International society for behavioral nutrition and physical activity annual meeting, Oslo, Norway
Sheldon G, Williams G, Joiner T (2003) Self-Determination Theory on the clinic: Motivation physical and mental health. Yale University Press, New Haven
Rosen JC, Jones A, Ramirez E, Waxman S (1996) Body shape questionnaire: studies of validity and reliability. Int J Eat Disord 20:315–319
Hart EA, Leary MR, Rejeski WJ (1989) The measurement of social physique anxiety. J Sport Exerc Psychol 11:94–104
Cunha JA (2001) Manual da versão em português das escalas de Beck. Psychological Corporation, São Paulo
Beck A, Steer R, Brown K (1996) Manual for the beck depression inventory-II. Psychological Corporation, San Antonio
Antunes P, Palmeira A (2003) Motivation for physical education classes: its relations with physical self-perceptions and body mass index. In: XI conference of the European federation of sport psychology, Copenhagen, Denmark
Rosenberg M (1965) Society and the adolescent self-image. Princeton University Press, Princeton
Engel SG, Kolotkin RL, Teixeira PJ, Sardinha LB, Vieira PN, Crosby RD (2005) Psychometric and cross-national evaluation of a Portuguese version of the impact of weight on quality of life-lite (IWQOL-Lite) questionnaire. Eur Eat Disord Rev 13:133–143. https://doi.org/10.1002/erv.614
Kolotkin RL, Head S, Hamilton M, Tse CK (1995) Assessing impact of weight on quality of life. Obes Res 3:49–56
Stotland S, Zuroff DC (1990) A new measure of weight locus of control: the dieting beliefs scale. J Pers Assess 54:191–203
Field AP (2009) Discovering statistics using SPSS, 3rd edn. Sage Publications, London
Teixeira PJ, Palmeira AL, Branco TL, Martins SS, Minderico CS, Barata JT et al (2004) Who will lose weight? A reexamination of predictors of weight loss in women. Int J of Behav Nutr Phys Act 1:12. https://doi.org/10.1186/1479-5868-1-12
Cohen J, Cohen P, West S, Aiken L (2003) Applied multiple regression/correlation analysis for the behavioral sciences, 3rd edn. Lawrence Erlbaum Associates, Mahwah
Dalle Grave R, Melchionda N, Calugi S, Centis S, Tufano A, Fatati G et al (2005) Continuous care in treatment of obesity: an observational multicentre study. J Intern Med 258:265–273. https://doi.org/10.1111/j.1365-2796.2005.01524.x
Nir Z, Neumann L (1995) Relationship among self-esteem, internal-external locus of control, and weight change after participation in a weight reduction program. J Clin Psychol 51:482–490
Teixeira P, Going S, Sardinha L, Lohman T (2005) A review of psychosocial pre-treatment predictors of weight control. Obes Rev 6:43–65. https://doi.org/10.1111/j.1467-789X.2005.00166.x
Urbanek JK, Metzgar CJ, Hsiao PY, Piehowski KE, Nickols-Richardson SM (2015) Increase in cognitive eating restraint predicts weight loss and change in other anthropometric measurements in overweight/obese premenopausal women. Appetite 87:244–250. https://doi.org/10.1016/j.appet.2014.12.230
Silva MN, Markland D, Carraça EV, Vieira PN, Coutinho SR, Minderico CS et al (2011) Exercise autonomous motivation predicts 3-year weight loss in women. Med Sci Sports Exerc 43:728–737. https://doi.org/10.1249/MSS.0b013e3181f3818f
Sasdelli AS, Petroni ML, Paoli AD, Collini G, Calugi S, Dalle Grave R et al (2018) Expected benefits and motivation to weight loss in relation to treatment outcomes in group-based cognitive-behavior therapy of obesity. Eat Weight Disord 23:205–214. https://doi.org/10.1007/s40519-017-0475-9
Foright RM, Presby DM, Sherk VD, Kahn D, Checkley LA, Giles ED et al (2018) Is regular exercise an effective strategy for weight loss maintenance? Physiol Behav 188:86–93. https://doi.org/10.1016/j.physbeh.2018.01.025
Funding
This study was funded by grants from the Portuguese Science and Technology Foundation (FCT-POCI/DES/57705/2004) and the Calouste Gulbenkian Foundation (grant number 65565/2004). The authors are grateful to the Oeiras City Council and Nestlé Portugal for their additional financial support.
Author information
Authors and Affiliations
Contributions
Rui Jorge and Inês Santos made substantial contributions to the analysis, interpretation of data, and took the lead on drafting and revising the manuscript for important intellectual content; Rita Tomás, Marlene N. Silva, Eliana V. Carraça, Vitor H. Teixeira, and Pedro J. Teixeira were involved in revising the manuscript for important intellectual content. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
All procedures of this study were approved by the Institutional Review Board of the Faculty of Human Kinetics, Technical University of Lisbon and are in accordance with the 1964 Helsinki declaration and its later amendments.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Jorge, R., Santos, I., Tomás, R. et al. Behavioural and psychological pretreatment predictors of short- and long-term weight loss among women with overweight and obesity. Eat Weight Disord 25, 1377–1385 (2020). https://doi.org/10.1007/s40519-019-00775-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-019-00775-9