
Abstract
Background and Objective
The Oncomine Dx Target Test (ODxTT) has been used as a companion diagnostic test for lung cancer. Here, we evaluated whether the amount of nucleic acid and the degree of RNA degradation are related to the success of the ODxTT.
Methods
This study included 223 samples from 218 patients with lung cancer. For all samples, DNA and RNA concentrations were quantified using Qubit, and the degree of RNA degradation was evaluated using the Bioanalyzer.
Results
Of the 223 samples, 219 samples were successfully analyzed in the ODxTT and four were not. DNA analysis failed in two samples, which were attributed to low DNA concentrations and both were cytology specimens. Meanwhile, RNA analysis failed in the other two samples. These samples had sufficient amounts of RNA, but it was highly degraded with DV200 (the percentage of RNA fragments > 200 base pairs) less than 30. Compared with RNA samples with DV200 ≥ 30, analysis of RNA with DV200 < 30 yielded significantly fewer reads for the internal control genes. This test showed actionable mutations were identified in 38% (83/218) of all patients and in 46.6% (76/163) of patients with lung adenocarcinoma.
Conclusions
DNA concentration and degree of RNA degradation are key factors determining the success of diagnostic testing by the ODxTT.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Samples with low cell counts and low DNA yields were unsuitable for the Oncomine Dx Target Test (ODxTT). |
Samples with high RNA yields but highly degraded were unsuitable for the ODxTT. |
Nucleic acid concentrations and integrity are related to the success or failure of the ODxTT. |
1 Introduction
Lung cancer is the most common cancer type and has a poor prognosis [1]. Approximately 85% of patients with lung cancer have non-small-cell lung cancer (NSCLC), and 70% of NSCLC tumors are locally advanced or metastatic at diagnosis [2]. In addition to conventional chemotherapy and radiation therapy, molecularly targeted therapies have become effective treatment options for patients with advanced NSCLC. Clinical trials showed that molecularly targeted therapies have significantly improved progression-free survival or overall survival for patients who are positive for applicable genetic alterations such as epidermal growth factor receptor (EGFR), B-Raf proto-oncogene, serine/threonine kinase (BRAF), anaplastic lymphoma kinase (ALK) fusion, Ros1 proto-oncogene (ROS1) fusion, and ret proto-oncogene (RET) fusion [3,4,5,6,7,8]. Targeted therapies for these mutations have improved the clinical course of patients with advanced NSCLC. Therefore, it is essential to determine optimal therapy based on the driver gene mutation.
The Oncomine Dx Target Test (ODxTT) is a next-generation sequencing-based companion diagnostic test approved by the US Food and Drug Administration in 2017. In Japan, the ODxTT is approved as a companion diagnostic to identify mutations in five driver genes (EGFR, ALK, ROS1, BRAF, and RET) in lung cancer. In February 2022, it was also expanded and approved in Japan as a companion test to identify the RET fusion gene in thyroid cancer. Other mutations with effective molecularly targeted therapies, including met proto-oncogene (MET) exon 14 skipping and Kirsten rat sarcoma viral oncogene homolog (KRAS) G12C, are also analyzed with the test [9,10,11]. The ODxTT has become an important test in determining the treatment strategy.
The ODxTT analyzes a total of 46 genes, which including 35 genes in DNA analysis and 21 genes in RNA analysis. This test can detect multiple gene mutations simultaneously; however, if sufficient sequencing data are not acquired or the data criteria are not met, the test results are not available. Previous reports indicated that surgical specimens, the size of the tumor tissue, the number of tumor cells, and the tumor content are important factors determining whether the test is successful [12,13,14,15,16,17]. However, as the results on the success or failure of DNA and RNA analysis tests are output independently, it is necessary to evaluate these results separately. In particular, the degree of nucleic acid degradation effects on the success or failure of the test is not well understood. In this study, we aim to clarify the factors that determine the success or failure of the ODxTT with respect to the outputs of DNA and RNA analyses.
2 Materials and Methods
2.1 Patients and Outcomes
This study examined 223 samples from 218 patients with lung cancer who were tested with the ODxTT (Thermo Fisher Scientific, Waltham, MA, USA) from December 2019 to June 2022. All patients who underwent the ODxTT in our hospital were included in this study without any exclusion criteria. Samples were collected consecutively in this study. After analysis by this test, all extracted DNA and RNA samples were stored at − 80 °C until a subsequent analysis. The primary outcome of this study was to evaluate the effect of both the quantity and quality of nucleic acids utilized in the ODxTT on the test results. Secondary outcomes included the evaluation of the number of detectable actionable mutations detected by the ODxTT, and the relationship between these mutations and histopathological classification.
2.2 Sample Preparation for the ODxTT
We made minor modifications to the standard protocol based on the package insert. As a criterion for performing the ODxTT, we set a threshold of 30% or more (n = 151, 67.7%) tumor content estimated by the pathologist (T.O.). However, even if the threshold was not met, samples with less than 30% tumor content (n = 72, 32.3%) were tested if requested by the physician. Two 5-μm-thick sections were prepared for specimens obtained by surgical resection, and 12 5-μm-thick sections were prepared for specimens obtained by methods other than surgery. We did not set any criteria for the number of tumor cells in the slides or the sample area. Macrodissection was performed on some formalin-fixed paraffin-embedded (FFPE) tumor tissues (n = 67) (Electronic Supplementary Material [ESM]).
2.3 Nucleic Acid Extraction and Quality Check
We prepared samples from cell block, cytology, and FFPE tissue (ESM). DNA and RNA were extracted using the Ion Torrent Dx Total Nucleic Acid Isolation Kit in accordance with the manufacturer’s instructions. In brief, FFPE tissue slices were treated with protease and the lysates were filtered through a filter cartridge. The filter cartridges were then washed with wash buffer, and RNA and DNA were extracted. RNA samples were treated with DNase prior to extraction. DNA and RNA concentrations were measured on Qubit 3.0 with the Ion Torrent Dx DNA Quantification Kit or the Ion Torrent Dx RNA Quantification Kit (Thermo Fisher Scientific). To determine the degree of RNA degradation, we used the Agilent 2100 Bioanalyzer with the Agilent RNA 6000 Pico Kit (Agilent Technologies, Santa Clara, CA, USA) and examined DV200 (the percentage of RNA fragments > 200 base pairs) values.
2.4 Library Preparation of the ODxTT
The ODxTT was performed in our institute at the Division of Genetics and Clinical Laboratory according to the manufacturer’s instructions (Thermo Fisher Scientific) with minor modifications. In brief, DNA samples were diluted to 0.83 ng/µL and RNA samples were diluted to 1.43 ng/µL with a dilution solution, in accordance with the recommended concentrations. Ten nanograms of DNA and RNA was used for the library synthesis as recommended in the standard protocol. If the extracted DNA or RNA concentration was less than the recommended concentration, we used the extracted samples with final input of less than 10 ng. Complementary DNA (cDNA) was synthesized using the Ion Torrent Dx cDNA Synthesis Kit. Target regions were amplified with DNA panel and RNA panel in the Ion PGM Dx Library Kit using extracted nucleic acids, DNA control, RNA control, and no template control [18]. Polymerase chain reaction amplicons were partially digested with FuPa reagent and then ligated with barcodes to generate a library. The library was purified and equalized with the Ion PGM Dx Library Equalizer Kit. Emulsion polymerase chain reaction and library enrichment were performed with the Ion OneTouch Dx Template Kit on the Ion OneTouch Dx instrument and the Ion OneTouch ES Dx instrument.
2.5 Sequencing of the ODxTT
Sequencing was conducted using the Ion PGM Dx sequencer (Thermo Fisher Scientific) with the Ion PGM Dx Sequencing Kit and the Ion PGM 318 Dx Chip in accordance with the manufacturer’s instructions. Data analysis was conducted with the Torrent Suite Dx software with an assay definition file. The data of all samples were passed to the control samples (DNA control, RNA control, and no template control, Control Fragment-1) of sequencing quality. In DNA analysis, “Failure” was defined as samples that did not meet (i) mean aliment quality 20 read length ≥ 90 bp or (ii) percent reads ≥ 0.7, or samples that resulted in “No Call” after variant call. In RNA analysis, “Failure” was defined as samples that did not meet mappable fusion reads ≥ 5000. “Success” was defined as samples that were (i) other than “Failure” and (ii) did not have “No Call” for mutations related to companion diagnostics, including EGFR, BRAF, ALK, ROS1, and RET genes. Five internal control genes in RNA analysis, including hydroxymethylbilane synthase (HMBS), integrin beta 7 (ITGB7), low density lipoprotein receptor-related protein 1 (LRP1), myelocytomatosis oncogene (MYC), and TATA box binding protein (TBP), were evaluated to assess RNA quality and the number of resulting sequencing reads.
2.6 Statistical Analysis
Interquartile range (IQR) calculations, correlation analyses, and statistical analyses were performed in R (version 4.1.1) [http://www.r-project.org/]. Data visualization and analysis in R also made use of the ggplot2 (v3.3.5), ggpubr (v0.4.0), dplyr (v1.0.7), tidyr (v1.1.3), scales (v1.2.1), patchwork (v1.1.1), gtsummary (v1.5.2), and flextable (v.0.7.0) packages. Wilcoxon rank sum test, Fisher’s exact test, and Bonferroni correction for multiple testing were conducted. Statistical significance was defined as a p value < 0.05.
3 Results
3.1 Patient and Sampling Characteristics
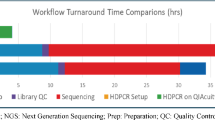
Patients included 77 female and 141 male individuals with a median age of 72 years (IQR 66–77 years) (Table S1 of the ESM). Sample sites were lung (n = 146, 65%), lymph node (n = 47, 21%), pleura (n = 10, 4%), pleural effusion (n = 9, 4%), bronchus (n = 3, 1%), and others (n = 8, 4%). Sample collection methods were surgery (n = 86, 39%), endobronchial ultrasonography with a guide sheath (n = 45, 20%), endobronchial ultrasound-guided transbronchial needle aspiration (n = 41, 18%), transbronchial biopsy (n = 23, 10%), aspiration (n = 9, 4%), thoracoscopy (n = 7, 3%), ultrasound-guided biopsy (n = 6, 2.7%), computed tomography-guided biopsy (n = 5, 2.2%), and endoscopic ultrasound-guided fine-needle aspiration (n = 1, 0.4%). Histology showed adenocarcinoma (n = 163, 73%), squamous cell carcinoma (n = 39, 17%), NSCLC (n = 14, 6%), and others (n = 7, 3%). Median turnaround time was 9 days (IQR 6–13 days).
3.2 Sample Type and Analysis of Test Success or Failure
We first analyzed the relationship between patient sample characteristics and sequencing success or failure. There were no significant differences based on collection site, collection method, tissue type, or microdissection, with success rates of over 98% in most categories (Table 1). Among the sample types, the success rates were high for cell block (100%, 7/7) and FFPE (99%, 204/206), but low for cytology (80%, 8/10) (Table 1, p = 0.015, Fisher’s exact test; q value = 0.2, Bonferroni correction for multiple testing). Although the number of samples evaluated was small, bronchus (67%, 2/3) also had a low success rate.
3.3 Analysis of Samples Below Recommended Nucleic Acid Concentrations
To determine the amount of nucleic acid obtained from the 223 samples subjected to the ODxTT, DNA and RNA concentrations were measured. The median amount of extracted DNA was 21.6 ng/µL (IQR 14.1–32.2 ng/µL) and the median amount of extracted RNA was 36.8 ng/µL (IQR 14.1–93.7 ng/µL) (Fig. 1A,B). The yield obtained for RNA was high compared to DNA, and DNA and RNA amounts were weakly correlated (R2 = 0.38, p < 0.001) (Fig. 1C).

Amounts of extracted DNA and RNA. A, B The histograms show the number of samples of each extracted amount of DNA (A) and RNA (B). The dashed line indicates the median concentration. C The scatter plot shows the correlated distribution of DNA and RNA concentrations. The red line indicates the recommended concentration for the analysis. The blue line indicates the regression line and the gray background indicates the 95% confidence interval
Of the 223 analyzed samples, 218 (97.8%) had nucleic acid concentrations above the recommended concentrations (DNA ≥ 0.83 ng/µL; RNA ≥ 1.43 ng/µL) and five (2.2%) did not (Table 2). DNA did not reach the specified concentration in one sample (#97, DNA: 0.24 ng/µL), RNA did not reach the specified concentration in three samples (#6, RNA: 1.3 ng/µL; #170, RNA: 1.3 ng/µL; #226, RNA: 1.1 ng/µL), and neither DNA nor RNA reached the specified amount in one sample (#88, DNA: 0.76 ng/µL, RNA: not measurable and below the detection limit) (Table 2). These five samples included two cytology samples and three FFPE samples. Although these samples did not reach the required concentrations, we analyzed these five samples by the ODxTT because no other samples were available. Notably, one sample (#88), for which DNA and RNA did not reach the required concentrations, could be analyzed for RNA but not for DNA (Table 2). Unexpectedly, the remaining four samples could be analyzed for DNA and RNA (#6, #97, #170, #226) [Table 2]. Although we only extracted low amounts of RNA samples (#6, #170, #226), the Bioanalyzer showed that these samples were less degraded and had RNA of more than 500 base pairs in length at high rates (Fig. S1 of the ESM). In two of four samples, we identified actionable mutations including MET exon 14 skipping (n = 1) and KRAS G12C (n = 1). Therefore, four of the five samples could be analyzed with the ODxTT, despite the nucleic acid amounts being less than the recommended concentration.
3.4 Characteristics of Samples for Which Analysis Failed
Of the 223 samples analyzed, 219 samples (98.2%) were successfully analyzed, while for four samples (1.8%) the analysis failed (Table 3). The two specimens for which DNA analysis failed were cytology specimens collected by endobronchial ultrasound-guided transbronchial needle aspiration or endobronchial ultrasonography with a guide sheath, which showed low numbers of cells (#88, #204) (Table 3 and Fig. S2 of the ESM) [19]. Meanwhile, the two specimens that failed in RNA analysis were both FFPE tissues from surgical specimens (#49, #174) (Table 3).
To examine the factors determining the success or failure of the analysis, nucleic acid amounts were compared. Compared with the successful samples, the two samples with failures in DNA analysis had significantly lower DNA concentrations (Fig. 2A, p = 0.017, Wilcoxon rank sum test). Meanwhile, the two failed samples in RNA analysis did not have lower RNA concentrations than the successful samples, but rather tended to have higher concentrations (Fig. 2B, p = 0.18, Wilcoxon rank sum test).

Nucleic acid concentration and degree of RNA degradation in the analyzed samples. A The boxplot shows DNA concentrations for samples for which DNA analysis was successful and failed. B The boxplot shows RNA concentrations for samples for which RNA analysis was successful and failed. C The histogram shows the number of samples of each DV200 value measured by the Bioanalyzer. The dashed line indicates the median DV200 value. D The scatter plot shows the correlation distribution between RNA concentration and DV200 values. The blue line indicates the regression line and the gray background indicates the 95% confidence interval. E The boxplot shows the total number of reads obtained when samples with DV200 values below and above 30 were analyzed for RNA in the ODxTT
To assess the degree of RNA degradation, DV200 was calculated on the Bioanalyzer. Samples that failed in RNA analysis had highly degraded RNA (#49, #174) (Fig. S1 of the ESM). Out of 223 samples, 222 were evaluable and 1 was not; the median value of DV200 was 66 (IQR 56–72) (Fig. 2C). There was no correlation between RNA amount and DV200 (R2 < 0.01, p = 0.51) (Fig. 2D). When we divided the data into four categories by DV200 value (<30 [n = 11], 30–50 [n = 30], 50–70 [n = 101], ≥ 70 [n = 80]) [20], RNA analysis failed in the DV200 < 30 (success: 9/11, fail: 2/11), and always succeeded at DV200 ≥ 30 (Table 4). Furthermore, the total number of reads obtained by RNA analysis was significantly lower for samples with DV200 < 30 compared with that for samples with DV200 ≥ 30 (Fig. 2E, p = 0.013, Wilcoxon rank sum test). Similarly, for the five internal control genes (HMBS, ITGB7, LRP1, MYC and TBP) measured in RNA analysis, the number of reads tended to be lower in samples with DV200 < 30 (Fig. S3 of the ESM). Thus, RNA analysis showed that the degree of RNA degradation, rather than the amount of RNA, affected the success or failure of the test.
3.5 Actionable Mutations Detected by the ODxTT
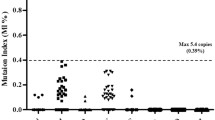
We next analyzed the extent to which the ODxTT could detect actionable mutations. In 83 out of 218 patients (38%), actionable mutations were identified (Table 5). The mutations identified were in EGFR (22.4%, n = 49), BRAF V600E (0.5%, n = 1), KRAS G12C (4.1%, n = 9), MET exon 14 skipping (7.3%, n = 16), ALK fusion (1.8%, n = 4), ROS1 fusion (1.4%, n = 3), and RET fusion (0.5%, n = 1) (Table 5). EGFR p.E746_A750del (8.7%, n = 19) and EGFR L858R (8.7%, n = 19) were more frequent. In addition, EGFR E746_A750del + T790M and single T790M resistance mutations against tyrosine kinase inhibitors were identified in each patient (n = 2).
3.6 Histology and Actionable Mutations
In lung cancer, genetic mutations are known to be detected at different rates depending on the histology. We next examined the relationship between histological types and actionable mutations. In the case of lung adenocarcinoma (n = 163), actionable mutations were identified in at least 46.6% of cases (n = 76) and included EGFR (28.8%, n = 47), KRAS G12C (5.5%, n = 9), MET exon 14 skipping (7.4%, n = 12), ALK fusion (2.5%, n = 4), ROS1 fusion (1.8%, n = 3), and RET fusion (0.6%, n = 1) by the ODxTT (Table 2 of the ESM). EGFR (n = 1), BRAF V600E (n = 1), and MET exon 14 skipping (n = 2) mutations were detected in 28.6% of NSCLC (4/14); and EGFR (n = 2) and MET exon 14 skipping (n = 3) mutations were detected in 12.8% of squamous cell carcinoma (5/39) (Fig. 3). No therapeutic gene mutations were detected in other histological types including adenosquamous carcinoma, large-cell carcinoma, large-cell neuroendocrine carcinoma, neuroendocrine carcinoma, and pleomorphic carcinoma (Fig. 3).

Lung cancer histology and actionable mutations. A–G Bar plots indicate the number of samples detected in each histological category. Actionable mutations refer to those in epidermal growth factor receptor (EGFR) (A), B-Raf proto-oncogene, serine/threonine kinase (BRAF) V600E (B), anaplastic lymphoma kinase (ALK) fusion (C), Ros1 proto-oncogene (ROS1) fusion (D), met proto-oncogene (MET) exon 14 skipping (E), Kirsten rat sarcoma viral oncogene homolog (KRAS) G12C (F), and ret proto-oncogene (RET) fusion (G). Orange indicates positive, cyan indicates negative, and yellow indicates samples with no results (failure)
4 Discussion
In this study, we analyzed the factors that determine the success or failure of DNA and RNA analyses by the ODxTT, which is approved as a companion diagnostic test for lung cancer. Interestingly, RNA analysis showed that, even if the amount of RNA was sufficient, the analysis failed for samples with advanced RNA degradation. Therefore, it is clear that different factors affect the test results for DNA and RNA analyses. It is important to scrutinize both the quantity and the quality of the extracted nucleic acids before testing to improve the success rate of the ODxTT.
Previous studies showed that the success rate of the ODxTT is higher for surgical specimen tissue than for biopsy tissue [14]. Furthermore, it has been shown that success rates are higher when larger forceps devices are used to perform biopsies [13]. These reports are consistent with our results regarding the success or failure of DNA analysis. For example, DNA analysis failed for two cytological samples, which may have resulted from lower DNA yields. Therefore, the DNA yield is considered to be an important factor in determining the success or failure of DNA analysis.
For RNA analysis, few studies have been performed on the success or failure of the results. A previous study showed that surgical samples (i.e., lobectomy sample) were prone to poor RNA quality because of the delay until the beginning of formalin fixation and inadequate formalin fixation [21]. Our findings also demonstrated that the ODxTT failed in analyzing RNA from two surgical specimens, likely attributable to significant RNA degradation resulting from inadequate fixation procedures. Thus, this study indicates that the degree of degradation (quality), rather than the amount of RNA, is more important for the success of RNA analysis. Although there is no mention of assessing RNA degradation in the standard protocol based on the package insert, we demonstrated the DV200 value is utilized for determining the success rate of RNA analysis in the ODxTT. As the degree of RNA degradation does not correlate with the amount of RNA, it is necessary to evaluate whether degradation is occuring by other methods, and not just relying on the quantification of nucleic acid concentration. The test is considered to fail for highly degraded RNA samples because the total number of reads is lower and does not meet the criteria for the analysis. To our knowledge, such findings regarding the evaluation of RNA degradation in the ODxTT have not been previously presented. Thus, this study provides evidence of the value of incorporating RNA degradation assessment into the analysis process, thereby increasing the success rate of testing procedures.
In patients with advanced lung cancer, it is sometimes not possible to reobtain tissue specimens, and we may face the situation that leftover specimens are tested. If no results are obtained, it is not possible to provide patients with an optimal strategy for lung cancer treatment. Therefore, in this study, we analyzed samples with DNA or RNA amounts less than the recommended amount; interestingly, one of the two samples with DNA amounts less than the recommended amount underwent a successful DNA analysis, and all four of the samples with RNA amounts less than the recommended amount underwent a successful RNA analysis. Furthermore, two samples harbored actionable mutations including MET exon 14 skipping and KRAS G12C. Although such an analysis is not recommended according to the standard protocol, when it is difficult to reobtain another tumor tissue, the ODxTT could be successful even if the nucleic acid content was less than the specified amount in some cases. Perhaps, even in the case of low nucleic acid concentrations, the ODxTT is an amplicon-based assay and could analyze the target region. We previously compared genetic abnormalities in tissue and cytology specimens by the ODxTT and showed that the genetic mutations to be treated were consistent [18]. The use of cytological specimens is effective not only in lung cancer but also in gynecologic and cholangiopancreatic cancers [19, 22, 23]. In actual clinical practice, there are cases in which only cytological specimens are obtained, without obtaining tissue specimens. When a large tumor tissue cannot be obtained, the amount of nucleic acids obtained from cytology specimens is expected to be small, but the use of cytology specimens can be of great benefit to patients.
In routine clinical molecular tests, nucleic acid evaluation is important before testing. In a cancer tissue examination, FFPE tissue is archived in hospitals, providing the advantage of easy accessibility. However, unlike samples such as blood in which nucleic acids are not so degraded, FFPE samples undergo nucleic acid degradation and crosslinking due to formalin fixation [24]. To predict the success or failure in subsequent molecular tests, it is necessary to evaluate the quantity (amount of extracted nucleic acid) and quality (degree of degradation) of the extracted nucleic acid. The nucleic acid quantity can be quantitatively measured by spectrophotometry or intercalators of fluorescent dyes. In addition, the degree of degradation can be evaluated by gel electrophoresis and real-time polymerase chain reaction. In this study, we emphasize the importance of understanding the characteristics of nucleic acids required for each molecular test using these methods.
This study has several limitations. First, it was conducted at a single institution, and the number of samples was limited. In particular, we examined a few samples with lower nucleic acid concentrations that did not meet the recommended criteria. Therefore, more data are needed to generalize the conclusions. Second, we tested 32.3% of samples (n = 72) with less than 30% of tumor content; therefore, the detection rate of actionable mutations may be somewhat low.
The ODxTT identified corresponding drugs in 38% (88/218) of all patients and in 46.6% (76/163) of patients with lung adenocarcinoma exclusively. This test is considered to be very important for first-line drug decisions. Osimertinib as adjuvant therapy was shown to significantly prolong disease-free survival in patients with stage IB–IIIA EGFR-positive NSCLC [25]. Therefore, in the future, testing will be necessary not only for patients with advanced cancer but also for patients with operable lung cancer.
5 Conclusions
In summary, we conducted a study to evaluate the success rate of the ODxTT in detecting genomic alterations in patients with NSCLC. We analyzed 223 samples and found a high success rate of 98.2%, with no significant differences in success rates based on collection site, collection method, tissue type, or microdissection. However, we observed a lower success rate for cytology samples (80%, 8/10) and bronchus samples (67%, 2/3). Our results showed that the success of this test is largely determined by DNA concentration and the degree of RNA degradation. This study has provided novel data demonstrating the importance of assessing RNA quality for determining the success of RNA analysis, and that in some cases, analysis results can still be obtained even when the amount of nucleic acid is insufficient for the ODxTT. We recommend that the collection of high-quality tissue samples should be prioritized to ensure a successful analysis.
References
Dela Cruz CS, Tanoue LT, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clin Chest Med. 2011;32(4):605–44. https://doi.org/10.1016/j.ccm.2011.09.001.
Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584–94. https://doi.org/10.4065/83.5.584.
Soria J-C, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2017;378(2):113–25. https://doi.org/10.1056/NEJMoa1713137.
Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–8. https://doi.org/10.1016/S1470-2045(09)70364-X.
Shaw AT, Ou S-HI, Bang Y-J, Camidge DR, Solomon BJ, Salgia R, et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N Engl J Med. 2014;371(21):1963–71. https://doi.org/10.1056/NEJMoa1406766.
Peters S, Camidge DR, Shaw AT, Gadgeel S, Ahn JS, Kim D-W, et al. Alectinib versus crizotinib in untreated ALK-positive non-small-cell lung cancer. N Engl J Med. 2017;377(9):829–38. https://doi.org/10.1056/NEJMoa1704795.
Hyman DM, Puzanov I, Subbiah V, Faris JE, Chau I, Blay J-Y, et al. Vemurafenib in multiple nonmelanoma cancers with BRAF V600 mutations. N Engl J Med. 2015;373(8):726–36. https://doi.org/10.1056/NEJMoa1502309.
Yoh K, Seto T, Satouchi M, Nishio M, Yamamoto N, Murakami H, et al. Vandetanib in patients with previously treated RET-rearranged advanced non-small-cell lung cancer (LURET): an open-label, multicentre phase 2 trial. Lancet Respir Med. 2017;5(1):42–50. https://doi.org/10.1016/S2213-2600(16)30322-8.
Paik PK, Felip E, Veillon R, Sakai H, Cortot AB, Garassino MC, et al. Tepotinib in non-small-cell lung cancer with MET exon 14 skipping mutations. N Engl J Med. 2020;383(10):931–43. https://doi.org/10.1056/NEJMoa2004407.
Wolf J, Seto T, Han J-Y, Reguart N, Garon EB, Groen HJM, et al. Capmatinib in MET exon 14-mutated or MET-amplified non-small-cell lung cancer. N Engl J Med. 2020;383(10):944–57. https://doi.org/10.1056/NEJMoa2002787.
Skoulidis F, Li BT, Dy GK, Price TJ, Falchook GS, Wolf J, et al. Sotorasib for lung cancers with KRAS p.G12C mutation. N Engl J Med. 2021;384(25):2371–81. https://doi.org/10.1056/NEJMoa2103695.
Takeyasu Y, Yoshida T, Motoi N, Teishikata T, Tanaka M, Matsumoto Y, et al. Feasibility of next-generation sequencing (Oncomine™ DX Target Test) for the screening of oncogenic mutations in advanced non-small-cell lung cancer patients. Jpn J Clin Oncol. 2021;51(7):1114–22. https://doi.org/10.1093/jjco/hyab059.
Sakaguchi T, Iketani A, Furuhashi K, Nakamura Y, Suzuki Y, Ito K, et al. Comparison of the analytical performance between the Oncomine Dx Target Test and a conventional single gene test for epidermal growth factor receptor mutation in non-small cell lung cancer. Thorac Cancer. 2021;12(4):462–7. https://doi.org/10.1111/1759-7714.13767.
Sakata S, Otsubo K, Yoshida H, Ito K, Nakamura A, Teraoka S, et al. Real-world data on NGS using the Oncomine DxTT for detecting genetic alterations in non-small-cell lung cancer: WJOG13019L. Cancer Sci. 2022;113(1):221–8. https://doi.org/10.1111/cas.15176.
Nemoto D, Yokose T, Katayama K, Murakami S, Kato T, Saito H, et al. Tissue surface area and tumor cell count affect the success rate of the Oncomine Dx Target Test in the analysis of biopsy tissue samples. Thorac Cancer. 2021;12(2):194–200. https://doi.org/10.1111/1759-7714.13743.
Mizote S, Matsumura M, Sekiya M, Sugiyama M, Sekine A, Kobayashi N, et al. Pathological criteria for multiplex gene-panel testing using next-generation sequencing in non-small cell lung cancer. Cancer Treat Res Commun. 2022;32: 100614. https://doi.org/10.1016/j.ctarc.2022.100614.
Murakami S, Yokose T, Nemoto D, Suzuki M, Usui R, Nakahara Y, et al. Suitability of bronchoscopic biopsy tissue samples for next-generation sequencing. Diagnostics. 2021;11(3):391. https://doi.org/10.3390/diagnostics11030391.
Amemiya MSK, Hirotsu PhDY, Nagakubo MSY, Mochizuki MDH, Higuchi MDR, Tsutsui MDT, et al. Actionable driver DNA variants and fusion genes can be detected in archived cytological specimens with the Oncomine Dx Target Test Multi-CDx system in lung cancer. Cancer Cytopathol. 2021;129(9):729–38. https://doi.org/10.1002/cncy.22434.
Kunimasa K, Hirotsu Y, Amemiya K, Nagakubo Y, Goto T, Miyashita Y, et al. Genome analysis of peeling archival cytology samples detects driver mutations in lung cancer. Cancer Med. 2020;9(13):4501–11. https://doi.org/10.1002/cam4.3089.
Hatanaka Y, Kuwata T, Morii E, Kanai Y, Ichikawa H, Kubo T, et al. The Japanese Society of Pathology practical guidelines on the handling of pathological tissue samples for cancer genomic medicine. Pathol Int. 2021;71(11):725–40. https://doi.org/10.1111/pin.13170.
Sakaguchi T, Iketani A, Furuhashi K, Nakamura Y, Suzuki Y, Ito K, et al. A method to improve genetic analysis of lung cancer samples. Respirology. 2021;26(9):887–90. https://doi.org/10.1111/resp.14114.
Nozaki T, Sakamoto I, Kagami K, Amemiya K, Hirotsu Y, Mochizuki H, et al. Molecular analysis of ascitic fluid cytology reflects genetic changes of malignancies of the ovary equivalent to surgically resected specimens. Cancer Cytopathol. 2022;130(8):640–9. https://doi.org/10.1002/cncy.22596.
Ohyama H, Hirotsu Y, Amemiya K, Amano H, Hirose S, Hosoda K, et al. Detection of actionable mutations in cytological specimens obtained by endoscopic ultrasound-guided fine needle aspiration with rapid onsite evaluation in pancreatic cancer. Ann Diagn Pathol. 2022;60: 152008. https://doi.org/10.1016/j.anndiagpath.2022.152008.
Amemiya K, Hirotsu Y, Oyama T, Omata M. Relationship between formalin reagent and success rate of targeted sequencing analysis using formalin fixed paraffin embedded tissues. Clin Chim Acta. 2019;488:129–34. https://doi.org/10.1016/j.cca.2018.11.002.
Wu Y-L, Tsuboi M, He J, John T, Grohe C, Majem M, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383(18):1711–23. https://doi.org/10.1056/NEJMoa2027071.
Acknowledgements
We thank all of the medical and ancillary hospital staff at the Department of Pathology, Yamanashi Central Hospital, and the patients for their participation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was supported by a Grant-in-Aid for the Genome Research Project from Yamanashi Prefecture (to M.O. and Y.H.), the Japan Society for the Promotion of Science KAKENHI Early-Career Scientists JP18K16292 (to Y.H.), a Grant-in-Aid for Scientific Research (B) 20H03668 and 23H02955 (to Y.H.), a Research Grant for Young Scholars (to Y.H.), the YASUDA Medical Foundation (to Y.H.), the Uehara Memorial Foundation (to Y.H.), Medical Research Grants from the Takeda Science Foundation (to Y.H.), and Kato Memorial Bioscience Foundation (to Y.H.).
Conflict of interest
Yuki Nagakubo, Yosuke Hirotsu, Kenji Amemiya, Hitoshi Mochizuki, Toshiharu Tsutsui, Yumiko Kakizaki, Yoshihiro Miyashita, Rumi Higuchi, Takahiro Nakagomi, Taichiro Goto, Toshio Oyama, and Masao Omata have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
The Institutional Review Board of the Clinical Research and Genome Research Committee at Yamanashi Central Hospital approved this study and the use of an opt-out consent method (approval number: G 2018-4). This study was performed in accordance with the Declaration of Helsinki.
Consent to participate
The requirement for written informed consent was waived by The Institutional Review Board of the Clinical Research and Genome Research Committee at Yamanashi Central Hospital because of the retrospective nature of the study.
Consent for publication
Not applicable.
Availability of data and material
All data generated or analyzed during this study are included in this published article.
Code availability
Not applicable.
Authors’ contributions
Y.N. performed the Oncomine Dx Target Test, data analysis, data collection, and manuscript preparation. Y.H. drafted the manuscript, and performed the data collection, data visualization, data interpretation, and statistical analyses. K.A. performed the Oncomine Dx Target Test and data collection. H.M. supervised and organized this study. T.T., Y.K., Y.M., R.H., T.N., and T.G. collected samples and interpreted the clinical data. T.O. assessed the diagnosis, pathologic classification and tumor content of lung cancer. M.O. conceptualized the study design and revised the manuscript. All authors reviewed and approved the manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Nagakubo, Y., Hirotsu, Y., Amemiya, K. et al. Nucleic Acid Quality Assessment is Critical to the Success of the Oncomine Dx Target Test for Lung Cancer. Mol Diagn Ther 27, 513–523 (2023). https://doi.org/10.1007/s40291-023-00653-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40291-023-00653-2