
Abstract
Background
Fear of pain and movement is an important factor in the development of hypervigilance and avoidance behaviours.
Objective
We examined the effectiveness of exercise training on improving fear-avoidance beliefs.
Methods
A systematic review (data sources: MEDLINE, CINAHL, SPORTDiscus, EMBASE, CENTRAL) and metaanalysis of randomised controlled/clinical trials of exercise training in adults versus relevant nonexercise comparators that quantified fear-avoidance was conducted.
Results
After screening 4603 identified records, 17 (2014 participants) and 13 (1152 participants) studies were eligible for qualitative and quantitative synthesis, respectively. Pairwise meta-analysis showed exercise training was more effective than all non-exercise comparators (standardised mean difference (SMD) [95% CI] − 0.378 [− 0.623, − 0.133], P = 0.002, Grading of Recommendations Assessment, Development and Evaluation [GRADE]: very low) for reducing fear-avoidance. Exercise training was more effective than true control for reducing fear avoidance (− 0.407 [− 0.750, − 0.065], P = 0.020, GRADE: very low), however it was not more effective than other interventions (− 0.243 [− 0.614, 0.128], P = 0.199, GRADE: very low). In people with low back pain, exercise training was more effective than non-exercise comparator groups for reducing fear-avoidance (− 0.530 [− 0.755, − 0.304], P < 0.001, GRADE: very low). For individuals with neck pain, exercise training was not more effective than non-exercise comparator groups for reducing fear-avoidance (0.061 [− 0.360, 0.482], P = 0.777, GRADE: very low).
Conclusion
There is very low to low-quality evidence that exercise training is effective for reducing fear-avoidance, including in people with low back pain. Exercise training may be more effective than no intervention for reducing fear avoidance, but there is very low-quality evidence that non-exercise interventions are as effective as exercise for fear avoidance. Few studies with low risk of bias is a limitation.
Trail Registration
PROSPERO Registration Number: CRD42019139678.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Fear of pain and movement is an important factor in the development of pain syndromes. |
We found, via meta-analysis of 13 studies (1152 participants), that there is very low to low quality evidence that exercise training is effective for reducing fear-avoidance. |
This information can inform developing treatment programs for people with pain conditions. |
1 Introduction
Pain is a relevant driver in learning processes and informs an individual about potential or actual threat of bodily harm [1]. Fear of pain and movement may be an important factor in the development of hypervigilance and avoidance behaviours [2]. The fear-avoidance model provides a framework describing the pain experience for those who do and do not fear pain [3, 4]. The primary concept of the model describes fear of pain as a result of actual or perceived tissue damage, with two different responses to pain: confrontation or avoidance [3, 5]. According to the model, individuals who catastrophize pain may develop avoidance behaviours to prevent new injury or re-injury occurring (e.g. fear-avoidance behaviour) [5]. Kinesiophobia was introduced as a term to describe the excessive, irrational and debilitating fear of movement caused by feeling susceptible to painful injury or re-injury [6], and later defined as the fear of movement or (re)injury [7]. The Tampa Scale for Kinesiophobia (TSK) [6] and the Fear-Avoidance Beliefs Questionnaire (FABQ) [8], are both valid and reliable measures of fear-avoidance [7, 9, 10]. High levels of fear-avoidance have been found in up to 56% of patients with chronic musculoskeletal pain [11], and is associated with greater disability, greater pain intensity and lower quality of life in this population [12]. In people who do not have current musculoskeletal pain, there is evidence that kinesiophobia is a risk factor for the future development of pain [13]. As fear-avoidance beliefs are common in patients with chronic musculoskeletal pain, it may serve as a therapeutic target in conservative treatments to reduce the burden of disease associated with musculoskeletal conditions.
Exercise training is an important and effective treatment strategy for managing pain and disability for adults with low back pain [14, 15], with evidence in low back pain showing that participation in exercise-based treatment may encourage patients to confront their fear of completing movements or other activities of daily living [16]. It is well accepted that psychological and social factors mediate pain and impact clinical outcomes for patients with chronic musculoskeletal pain [17]; however, the effect of an exercise training approach alone specifically on fear-avoidance beliefs is not currently clear. A recent systematic review that investigated the effectiveness of conservative treatments for fear-avoidance beliefs concluded there was limited evidence for exercise training in reducing fear-avoidance beliefs in people with chronic low back pain [18]. However, this systematic review only examined studies that compared exercise training to other active treatment interventions, which reduced the ability to determine whether exercise itself is effective for reducing fear-avoidance beliefs [18].
This systematic review and meta-analysis aimed to examine whether exercise interventions when used alone were effective in reducing fear-avoidance beliefs when compared to non-exercise training comparators in adults. Furthermore, we performed sub-group analyses to determine if exercise training was more effective compared to non-exercise comparator groups for: (a) fear-avoidance beliefs/kinesiophobia, (b) physical activity and work specific FABQ sub-scales, and (c) reducing fear-avoidance beliefs in patients with pain conditions (e.g. back pain or neck pain). These findings may provide insight into whether there is merit for the use of exercise to specifically address fear-avoidance beliefs.
2 Methods
This review was completed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [19]. The review was registered prospectively with PROSPERO (CRD42019139678).
2.1 Search Strategy
Five online databases (MEDLINE, CINAHL, SPORTDiscus, EMBASE and CENTRAL) were electronically used for research published from database inception to May 2019. The search terms and strategy can be found in Supplementary Table 1. The search had the following limits: MEDLINE (All Adult: 19+ years; Randomized Controlled Trial; Human), CINAHL (Exclude MEDLINE records; Human, Randomized Controlled Trials; Journal Article; All Adult), SPORTDiscus (Academic Journal), EMBASE (RCT; Not MEDLINE; Adult; Article) and CENTRAL (Trials). To locate additional references, we searched for previously published systematic reviews identified via the Cochrane Database of Systematic Reviews (search terms: kinesiophobia exercise; limits: none) and GoogleScholar (search terms: ‘systematic review’ kinesiophobia exercise; limits: previous 10 years). Both language and year of publication were not part of the exclusion criteria. All results of the search were screened by PJO to exclude duplicates. Additionally, relevant articles cited in included studies were entered into full-text screening. Independent screening of the titles and abstracts of the remaining studies was completed by JD and SH considering inclusion and exclusion criteria. Any disagreements were adjudicated by PJO.
2.2 Inclusion and Exclusion Criteria
Studies published in a peer-reviewed journal (i.e. grey literature excluded) with a parallel arm (individual- or cluster-designed) randomised controlled or clinical trial design comparing an exercise training intervention to a non-exercise training comparator were included. All other inclusion criteria followed the Participants, Interventions, Comparators, Outcomes and Study design (PICOS) framework [20]. There were no restrictions based on sex, race or disease state. Studies that included participants under the age of 18 years were excluded. Included interventions prescribed exercise training alone, without the addition of other treatments (e.g. massage, cognitive behavioural therapy, pain education). Non-exercise training comparator groups included true control (i.e. no intervention or wait-list control), therapist hands-on control (e.g. manual therapy, chiropractic, passive physiotherapy, osteopathic, massage or acupuncture) and therapist hands-off control (e.g. general practitioner management, education or psychological interventions). Studies were required to include the TSK or FABQ for the measurement of fear-avoidance beliefs. When both measures were available [21], the TSK was prioritised due to the greater prevalence of this measure within the included studies, which is in agreement with a previous systematic review which had a slightly higher number of studies using the TSK included compared to the FABQ [18].
2.3 Data Extraction
Data extraction was completed by two independent assessors (JH and SH). Extracted information included relevant publication information (i.e. author, title, year, journal), study design, number of participants, participant characteristics (e.g. age and sex), intervention details (e.g. duration, type) and outcome measures. Extracted outcome data were pre- and post-intervention mean and standard deviation (SD) for either the TSK or FABQ. When end of intervention data were presented as median (interquartile range) or alternate measures of variance, it was converted to mean and SD using established formulae [22]. If authors presented the follow-up data as mean (SD) change or alternate measures of variance, post-intervention SD was imputed using recommended formulae [22] and established test–retest correlations (i.e. 0.91 for TSK; 0.90 for FABQ) [23]. In order to include the FABQ results within the meta-analysis, the subscales (physical and work) were normalised to a scale from 0 to 100 and then pooled using established formulae [22]. In all instances where data required for meta-analysis were not available, authors were contacted a minimum of three times over a 4-week period to request the information. The authors of six studies were contacted [24,25,26,27,28,29], and three provided the requested data [25, 27, 28]. Similarity between extracted data from the two independent assessors (JH and SH) was evaluated through Covidence (Veritas Health Innovation, Melbourne, Australia; https://www.covidence.org). Any discrepancies were discussed by JH and SH with disagreements adjudicated by PJO. This method was piloted on ten studies chosen at random prior to commencing data extraction.
2.4 Risk of Bias Assessment and GRADE
The Cochrane Collaboration Risk of Bias Tool was used to examine potential selection bias (random sequence generation and allocation concealment), performance bias (blinding of patients and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective outcome reporting) and other bias [22]. This assessment was completed independently by JH and SH. Studies were classified as having a low, high or unclear (when reporting was not adequate to rate a specific domain) risk for each type of bias. In line with our previous work [14], participant blinding is not feasible in exercise training studies and thus participant blinding was rated as having a high risk of bias for all studies. Any disagreements for the risk of bias were adjudicated by PJO. In addition, to assess the quality of the evidence for the ranking of treatments from meta-analysis, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used [30].
2.5 Statistical Analysis
Pairwise random-effects meta-analysis was conducted in Stata 15.0 (Stata Corp, College Station TX, USA). As all outcomes of interest were continuous, standardised mean difference (SMD) was used as the effect estimate. Data were pooled when a study investigated multiple groups defined as exercise training [22]. When there was more than one non-exercise intervention in a study, data for these groups were also pooled, as per our work prior [14]. The main analysis investigated pooled exercise training versus pooled non-exercise comparators in reducing fear-avoidance beliefs. Sub-group analyses were performed to consider: (a) exercise training versus true control for reducing fear avoidance, (b) exercise training versus non-exercise comparator groups (i.e. cognitive behavioural treatment, education, or general practitioner usual care), (c) exercise training versus comparator groups for reducing fear-avoidance beliefs in low back pain populations, (d) exercise training versus comparator groups for reducing fear-avoidance beliefs in neck pain populations (e) exercise training versus comparator groups for reducing kinesiophobia (TSK), (f) exercise training versus comparator groups for reducing fear avoidance beliefs (physical), (g) exercise training versus comparator groups for reducing fear avoidance beliefs (work) and (h) exercise training versus comparator groups for reducing fear-avoidance beliefs in chronic low back pain populations. Using the I2 statistic, heterogeneity was assessed for all pairwise comparisons and publication bias using the P value (significance P < 0.05) of Egger’s test and funnel plots.
3 Results
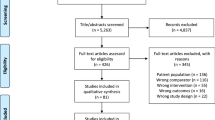
A summary of the systematic review process is shown in Fig. 1. There were 4603 studies (after removal of 207 duplicates) imported for initial title and abstract screening from the electronic database search. Two additional studies were found through a manual search of included studies reference lists [27, 31]. Following the completion of the title and abstract screening there were 381 studies included in the full-text screening. The examination of full-texts resulted in 17 studies being included for qualitative analysis (Table 1) [21, 24,25,26,27,28,29, 31,32,33,34,35,36,37,38,39,40], and of these included studies, 13 were deemed eligible for meta-analysis [21, 25, 27, 28, 31,32,33,34,35,36,37,38]. Reasons for exclusion from the meta-analysis included TSK only being measured at baseline [24, 29], and post-intervention data not available [26, 39].

Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) diagram of the study screening process for examining the effectiveness of exercise training for reducing fear avoidance beliefs
3.1 Study Characteristics
The details of each included study (n = 17; participants: n = 2014) [21, 24,25,26,27,28,29, 32,33,34,35,36,37,38,39,40] are shown in Table 1. The sample size of each study varied from 20 to 315 participants and mean age ranged from 27 to 69 years. The length of study (i.e. intervention) ranged from 4 to 24 weeks (one study did not specify intervention length [26]). There were 13 studies that included both males and females [21, 25,26,27, 29, 31,32,33,34, 37,38,39,40], while three studies included only females [24, 28, 36], and one study included only males [35]. Of the included studies, seven studies investigated chronic low back pain populations [21, 25, 29, 31, 33,34,35], two studies investigated low back pain lasting between 4 weeks and 6 months [27, 39], one study investigated failed back surgery syndrome [37], one study investigated sub-acute low back pain [40], two studies included patients with chronic neck pain [32, 38], one study included patients with either neck or back pain [26], one study included patients with osteoporosis [28], one study included post-menopausal women (no specific disease state) [24] and one study included participants from the general population (no specific disease state) [36]. A summary of the risk of bias assessment for each study is shown in Supplementary Table 2. When examining the studies overall, there was low risk of bias shown for random sequence generation (77%), blinding of outcome assessment (53%) and other sources of bias (100%), while low risk of bias was not common for blinding of patients and personnel (0%), allocation concealment (24%), incomplete outcome data (41%) and selective outcome reporting (35%; Fig. 2).

Percentage of studies examining the efficacy of exercise training for reducing fear avoidance beliefs with low, unclear and high risk of bias for each aspect of the Cochrane Risk of Bias Tool. The use of exercise training makes it not possible to truly blind patients to treatment allocation; therefore, this was not considered in the overall risk of bias assessment of each study
3.2 All Exercise Versus All Non-exercise Comparator Groups
Pairwise meta-analysis demonstrated that exercise training (all) was more effective than all comparator groups (SMD [95% CI] − 0.378 [− 0.623, − 0.133], P = 0.002, I2 = 70.4%, studies: n = 13; Fig. 3) for reducing fear-avoidance/kinesiophobia (TSK or FABQ). There was evidence of publication bias within the comparison (P = 0.011; Supplementary Fig. 5). The overall GRADE quality was considered very low (Table 2). Meta-analyses for each different scale are presented in Supplemental Data A.

Forest plot for the meta-analysis investigating the effectiveness of exercise training versus non-exercise comparators for reducing fear-avoidance behaviour
3.3 Exercise Versus True Control for Reducing Fear Avoidance
Pairwise meta-analysis showed that exercise training (all) was more effective than true control for reducing fear avoidance (only TSK available; SMD [95% CI] − 0.407 [− 0.750, − 0.0.65], P = 0.020, I2 = 69.9%, studies: n = 7; Fig. 4). There was evidence of publication bias (P = 0.017; Supplementary Fig. 6). The overall GRADE quality was considered low (Table 2).

Forest plots (in order) for the meta-analysis investigating a exercise training versus true control for reducing fear avoidance, b exercise training versus non-exercise treatment groups, c exercise training versus comparator groups for reducing fear-avoidance beliefs in low back pain populations, and d exercise training versus comparator groups for reducing fear-avoidance beliefs in neck pain populations
3.4 Exercise Versus Other Interventions for Reducing Fear Avoidance
Pairwise meta-analysis showed that exercise training (all) was not more effective than non-exercise intervention groups (e.g. General Practitioner care as usual, psychological interventions) for reducing fear avoidance (TSK or FABQ; SMD [95% CI]: − 0.243 [− 0.614, 0.128], P = 0.199, I2 = 79.2%, studies: n = 7; Fig. 4). There was no evidence of publication bias (P = 0.296; Supplementary Fig. 7). The overall GRADE quality was considered very low (Table 2).
3.5 Exercise in Low Back Pain
In studies of patients with low back pain, pairwise meta-analysis revealed that exercise training (all) was more effective than all comparator groups (SMD [95% CI] − 0.530 [− 0.755, − 0.304], P < 0.001, I2 = 46.4%, studies: n = 9; Fig. 4) for reducing fear-avoidance/kinesiophobia (TSK or FABQ). There was evidence of publication bias within the comparison (P = 0.005; Supplementary Fig. 8). The overall GRADE quality was considered very low (Table 2). Similar findings existed for patients with chronic low back pain (see Supplemental Data A).
3.6 Exercise in Neck Pain
In studies of patients with neck pain, pairwise meta-analysis revealed that exercise training was not more effective than all comparator groups (SMD [95% CI] 0.061 [− 0.360, 0.482], P = 0.777, I2 = 0.0%, studies: n = 2; Fig. 4) for reducing fear-avoidance/kinesiophobia (TSK or FABQ). There was evidence of publication bias within the comparison (Assessment of potential publication bias, via Eggers test, was not possible with only two studies available; Supplementary Fig. 9). The overall GRADE quality was considered low (Table 2).
4 Discussion
This systematic review and meta-analysis found that exercise training may be effective for reducing fear-avoidance beliefs when compared to non-exercise training comparators. When compared to true control (i.e. no intervention or wait-list control), exercise training interventions alone were more effective in reducing fear-avoidance belief. However, when compared to non-exercise treatment comparator groups (i.e. cognitive behavioural treatment, education, or general practitioner usual care), exercise training alone was not more effective in reducing fear-avoidance beliefs. There were limited studies examining the effect of exercise in reducing fear-avoidance beliefs in pain-free populations. Notably, the evidence was very low quality overall, as assessed by the GRADE criteria.
To the best of our knowledge, this is the first systematic review and meta-analysis that investigated the effectiveness of exercise training interventions alone compared to non-exercise comparators in adults with and without musculoskeletal pain disorders on fear-avoidance beliefs. The results of this study provide evidence that exercise training may be an effective tool in reducing fear-avoidance behaviour in the absence of a biopsychosocial and pain neuroscience education approach. Our findings are in line with a previous systematic review highlighting that exercise alone may reduce kinesiophobia (TSK) in adults with chronic low back pain, and also reported limited effectiveness for reducing fear avoidance beliefs (FABQ) [18]. Our meta-analysis combined all available evidence of self-reported outcome measures evaluating fear-avoidance beliefs to determine that overall, exercise training reduces fear-avoidance beliefs in patients with low back pain, and more specifically individuals with chronic low back pain. This is important as a large proportion (56%) of those with chronic musculoskeletal pain have been shown to have high levels of fear-avoidance beliefs [11]. The reduction of fear-avoidance beliefs is likely important as there is evidence of associations with pain intensity, disability and quality of life for patients with musculoskeletal pain disorders [12]. Therefore, this is further (low quality based on GRADE criteria) evidence that supports the use of exercise training for the management of chronic low back pain and its associated features (fear-avoidance beliefs) to mitigate the considerable burden of disease associated with this condition.
Fear-avoidance beliefs is a reported barrier for the participation in exercise training by those in pain, specifically in those with chronic low back pain [41]. It is believed that the brain can acquire long-term pain memory and associate threat to movements [42]. Therefore, those with chronic musculoskeletal pain may develop a protective pain memory [43]. This fear of movement may lead to altered motor control when completing movements deemed dangerous by the individual [44]. It is thought that the completion of painful therapeutic exercises could reduce threat perception of those movements [45, 46]. A potential mechanism for the effect of painful exercise is that it may alter the self-efficacy of an individual for completion of some physical activities [47]. This may be the result of a patient improving their response-outcome expectation and increasing their tolerance of more challenging exercises without prompting previous pain-related fear [48]. Another potential mechanism is alterations of brain function; for example one study showed that regular exercise reduces anxiety-related amygdala functional connectivity in young adults [49]. Due to these speculative mechanisms, exercise training may be an effective method for reducing fear-avoidance beliefs, yet further high-quality trials are warranted to confirm this notion.
A recent systematic review found limited strength of evidence for psychological interventions in decreasing kinesiophobia [18]. In the current study, due to the lack of studies that included a cognitive behavioural therapy intervention as a sole intervention compared to exercise, it was not feasible to examine the comparison between these interventions. Therefore, it is unknown whether exercise training is more effective in reducing fear-avoidance when compared to cognitive behavioural therapy. Future studies should examine the role of exercise training with and without the addition of cognitive behavioural therapy, ideally with a four-arm factorial RCT design, to determine the individual and synergistic effects of these treatments on fear avoidance behaviour.
Furthermore, although the effect size favoured exercise, we found very-low quality evidence for no difference between exercise and non-exercise interventions for reducing kinesiophobia. Seven studies were available for comparing exercise to non-exercise interventions and the comparators were general practitioner care as usual and psychological interventions. It remains open whether exercise per se, or any kind of ‘effective’ intervention, such as a well-designed psychological intervention, are better for reducing kinesiophobia.
It was not possible to investigate the effectiveness of exercise training in reducing fear-avoidance beliefs in healthy, pain-free, populations due to the lack of studies. Despite this, up to 30% of people without low back pain have been found to have kinesiophobia, and fear-avoidance behaviour may be a predictor of future LBP development [13, 50]. For example, Linton et al. showed that those with greater fear-avoidance beliefs were at twice the risk of developing back pain and 1.7 times more likely to have lowered physical function at the follow up [50]. Additionally, a 6-month study of 1571 people from the general population found that people without current LBP and greater kinesiophobia (TSK-17: ≥ 35 points) were 3.4 times more likely to develop low back pain with disability after 6 months [13]. Therefore, given that greater fear-avoidance beliefs in the general population may be a risk factor for low back pain development, it is important for future studies to investigate if exercise training interventions can reduce kinesiophobia in this population.
A limitation of this study is the use of pooled data for all exercise types, which precludes the ability to determine which specific type of exercise training may be most effective in reducing fear-avoidance behaviour. A recent network meta-analysis found that active therapies such as Pilates, resistance training, aerobic exercise and motor control training were effective in reducing pain intensity and increasing function in those with chronic low back pain, and therefore suggests a single type of exercise training may not be better than another for treatment [14]. This may be the case for reducing fear-avoidance beliefs, but further research should investigate this before conclusions may be drawn. When estimating the mean change in TSK value, the calculated value was − 3.5 points (pooled SD for TSK for all included studies 9.27 × − 0.378 SMD). A clinically meaningful change in TSK score has previously been found to be 8 points [51]. The effect size in people with back pain was larger, but still less than the threshold for clinical significance, which suggests that exercise training may not result in clinically meaningful changes in fear avoidance. Two studies [25, 34] showed very large effect sizes, which seemed unusual. We double-checked the measures of spread and reported means for these papers and the effect size estimates did not change. Another important factor not addressed within this review is the intensity of training. One of the included studies in this systematic review utilised both high- and low-intensity lumbar extensor strengthening programs, which resulted in 2- and 5-point reduction in TSK scores, respectively [35]. However, both training intensities in this study did not result in a clinically meaningful difference [35]. This may suggest that the intensity of exercise is not an important factor in the reduction of fear-avoidance beliefs. Further research should aim to investigate whether the intensity of exercise is important for an exercise training intervention to reduce fear-avoidance beliefs.
5 Conclusion
The results of this systematic review and meta-analysis provided low to very low quality evidence that exercise training alone may be an effective treatment for reducing fear-avoidance beliefs. For patients with back pain, and more specifically chronic low back pain, exercise training may be effective for reducing fear-avoidance behaviour. This review provides further evidence that exercise training may be a suitable conservative treatment for managing features, such as fear avoidance beliefs, which are commonly experienced in adults with chronic musculoskeletal pain. However, further high-quality studies are warranted to extend the observations found in this review, as they are currently limited by the low quality of evidence.
References
Vlaeyen JW, Linton SJ. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain. 2012;153(6):1144–7.
Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–32. https://doi.org/10.1016/S0304-3959(99)00242-0.
Lethem J, Slade P, Troup J, Bentley G. Outline of a fear-avoidance model of exaggerated pain perception—I. Behav Res Ther. 1983;21(4):401–8.
Crombez G, Eccleston C, Van Damme S, Vlaeyen JWS, Karoly P. Fear-avoidance model of chronic pain: the next generation. Clin J Pain. 2012;28(6):475–83. https://doi.org/10.1097/AJP.0b013e3182385392.
Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K, Vlaeyen JW. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30(1):77–94.
Kori S. Kinesiophobia: a new view of chronic pain behavior. Pain Manag. 1990;35–43.
Vlaeyen JW, Kole-Snijders AM, Boeren RG, Van Eek H. Fear of movement/(re) injury in chronic low back pain and its relation to behavioral performance. Pain. 1995;62(3):363–72.
Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–68.
Pfingsten M, Kröner-Herwig B, Leibing E, Kronshage U. Validation of the German version of the fear-avoidance beliefs questionnaire (FABQ). Eur J Pain. 2000;4(3):259–66.
Lee K-C, Chiu TT, Lam T-H. Psychometric properties of the Fear-Avoidance Beliefs Questionnaire in patients with neck pain. Clin Rehabil. 2006;20(10):909–20.
Bränström H, Fahlström M. Kinesiophobia in patients with chronic musculoskeletal pain: differences between men and women. J Rehabil Med. 2008;40(5):375–80.
Luque-Suarez A, Martinez-Calderon J, Falla D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: a systematic review. Br J Sports Med. 2019;53(9):554–9.
Picavet HSJ, Vlaeyen JWS, Schouten JSAG. Pain catastrophizing and kinesiophobia: predictors of chronic low back pain. Am J Epidemiol. 2002;156(11):1028–34. https://doi.org/10.1093/aje/kwf136.
Owen PJ, Miller CT, Mundell NL, Verswijveren SJ, Tagliaferri SD, Brisby H et al. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. 2019.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–47.
Kernan T, Rainville J. Observed outcomes associated with a quota-based exercise approach on measures of kinesiophobia in patients with chronic low back pain. J Orthop Sports Phys Ther. 2007;37(11):679–87.
Booth J, Moseley GL, Schiltenwolf M, Cashin A, Davies M, Hübscher M. Exercise for chronic musculoskeletal pain: a biopsychosocial approach. Musculoskelet Care. 2017;15(4):413–21.
Martinez-Calderon J, Flores-Cortés M, Morales-Asencio JM, Luque-Suarez A. Conservative interventions reduce fear in individuals with chronic low back pain: a systematic review. Arch Phys Med Rehabil. 2019;101:329.
Moher D, Liberati A, Tetzlaff J, Altman D, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. PLoS Med. 2009;6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Vincent HK, George SZ, Seay AN, Vincent KR, Hurley RW. Resistance exercise, disability, and pain catastrophizing in obese adults with back pain. Med Sci Sports Exerc. 2014;46(9):1693.
Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.0 Cochrane. 2019. https://www.training.cochrane.org/handbook.
Tagliaferri SD, Miller CT, Owen PJ, Mitchell UH, Brisby H, Fitzgibbon B, et al. Domains of chronic low back pain and assessing treatment effectiveness: a clinical perspective. Pain Pract. 2020;2:211. https://doi.org/10.1111/papr.12846.
Bernard P, Ninot G, Bernard P, Picot M, Jaussent A, Tallon G, et al. Effects of a 6-month walking intervention on depression in inactive post-menopausal women: a randomized controlled trial. Aging Ment Health. 2015;19(6):485–92.
Keane LG. Comparing AquaStretch with supervised land based stretching for chronic lower back pain. J Bodyw Move Ther. 2017;21(2):297–305.
Klaber Moffett J, Jackson DA, Gardiner E, Torgerson DJ, Coulton S, Eaton S, et al. Randomized trial of two physiotherapy interventions for primary care neck and back pain patients: ‘McKenzie’ vs brief physiotherapy pain management. Rheumatology. 2006;45(12):1514–21.
Klaber Moffett JA, Torgerson D, Bell-Syer S, Jackson D, Llewlyn-Phillips H, Farrin A, et al. Randomised controlled trial of exercise for low back pain: clinical outcomes, costs, and preferences. BMJ. 1999;319(7205):279–83.
Oksuz S, Unal E. The effect of the clinical pilates exercises on kinesiophobia and other symptoms related to osteoporosis: randomised controlled trial. Complement Ther Clin Pract. 2017;26:68–72.
Smeets RJ, Vlaeyen JW, Hidding A, Kester AD, van der Heijden GJ, van Geel AC, et al. Active rehabilitation for chronic low back pain: cognitive-behavioral, physical, or both? First direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;7(1):5.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Zadro JR, Shirley D, Simic M, Mousavi SJ, Ceprnja D, Maka K, et al. Video-game–based exercises for older people with chronic low back pain: a randomized controlled table trial (GAMEBACK). Phys Ther. 2018;99(1):14–27.
Bahat HS, Croft K, Carter C, Hoddinott A, Sprecher E, Treleaven J. Remote kinematic training for patients with chronic neck pain: a randomised controlled trial. Eur Spine J. 2018;27(6):1309–23.
Cruz-Díaz D, Bergamin M, Gobbo S, Martínez-Amat A, Hita-Contreras F. Comparative effects of 12 weeks of equipment based and mat Pilates in patients with chronic low back pain on pain, function and transversus abdominis activation. A randomized controlled trial. Complement Ther Med. 2017;33:72–7.
Cruz-Díaz D, Romeu M, Velasco-González C, Martínez-Amat A, Hita-Contreras F. The effectiveness of 12 weeks of Pilates intervention on disability, pain and kinesiophobia in patients with chronic low back pain: a randomized controlled trial. Clin Rehabil. 2018;32(9):1249–57.
Harts CC, Helmhout PH, de Bie RA, Staal JB. A high-intensity lumbar extensor strengthening program is little better than a low-intensity program or a waiting list control group for chronic low back pain: a randomised clinical trial. Aust J Physiother. 2008;54(1):23–31.
Jørgensen MB, Ektor-Andersen J, Sjøgaard G, Holtermann A, Søgaard K. A randomised controlled trial among cleaners-effects on strength, balance and kinesiophobia. BMC Public Health. 2011;11(1):776.
Karahan AY, Sahin N, Baskent A. Comparison of effectiveness of different exercise programs in treatment of failed back surgery syndrome: a randomized controlled trial. J Back Musculoskelet Rehabil. 2017;30(1):109–20.
Lee J, Lee M, Lim T, Kim T, Kim S, Suh D, et al. Effectiveness of an application-based neck exercise as a pain management tool for office workers with chronic neck pain and functional disability: a pilot randomized trial. Eur J Integr Med. 2017;12:87–92.
Klaber Moffett JA, Carr J, Howarth E. High fear-avoiders of physical activity benefit from an exercise program for patients with back pain. Spine J. 2004;29(11):1167–72.
Storheim K, Brox JI, Holm I, Koller AK, Bo K. Intensive group training versus cognitive intervention in sub-acute low back pain: short-term results of a single-blind randomized controlled trial. J Rehabil Med. 2003;35(3):132–40.
Boutevillain L, Dupeyron A, Rouch C, Richard E, Coudeyre E. Facilitators and barriers to physical activity in people with chronic low back pain: a qualitative study. PLoS ONE. 2017;12(7):e0179826.
Nijs J, Girbés EL, Lundberg M, Malfliet A, Sterling M. Exercise therapy for chronic musculoskeletal pain: innovation by altering pain memories. Man Ther. 2015;20(1):216–20.
Zusman M. Mechanisms of musculoskeletal physiotherapy. Phys Ther Rev. 2004;9(1):39–49.
Tucker K, Larsson A-K, Oknelid S, Hodges P. Similar alteration of motor unit recruitment strategies during the anticipation and experience of pain. Pain. 2012;153(3):636–43.
Smith BE, Hendrick P, Bateman M, Holden S, Littlewood C, Smith TO, et al. Musculoskeletal pain and exercise—challenging existing paradigms and introducing new. Br J Sports Med. 2019;53(14):907–12.
Tagliaferri SD, Miller CT, Ford JJ, Hahne AJ, Main LC, Rantalainen T, et al. Randomized trial of general strength and conditioning versus motor control and manual therapy for chronic low back pain on physical and self-report outcomes. J Clin Med. 2020;9(6):1726.
Tryon WW. Possible mechanisms for why desensitization and exposure therapy work. Clin Psychol Rev. 2005;25(1):67–95.
Petruzzello SJ, Landers DM, Hatfield BD, Kubitz KA, Salazar W. A meta-analysis on the anxiety-reducing effects of acute and chronic exercise. Sports Med. 1991;11(3):143–82.
Chen Y-C, Chen C, Martínez RM, Etnier JL, Cheng Y. Habitual physical activity mediates the acute exercise-induced modulation of anxiety-related amygdala functional connectivity. Sci Rep. 2019;9(1):1–12.
Linton SJ, Buer N, Vlaeyen J, Hellsing A-L. Are fear-avoidance beliefs related to the inception of an episode of back pain? A prospective study. Psychol Health. 2000;14(6):1051–9. https://doi.org/10.1080/08870440008407366.
Lüning Bergsten C, Lundberg M, Lindberg P, Elfving B. Change in kinesiophobia and its relation to activity limitation after multidisciplinary rehabilitation in patients with chronic back pain. Disabil Rehabil. 2012;34(10):852–8. https://doi.org/10.3109/09638288.2011.624247.
Acknowledgements
The authors thank Josh Defazio for his assistance in the project in screening of the titles/abstracts and full-texts. Scott Tagliaferri is supported by an Australian Government Research Training Program (RTP) Scholarship.
Author information
Authors and Affiliations
Contributions
Secured funding: NA; Study conception: Belavy, Donath, Owen, Miller; Screening: Held, Defazio; Extraction: Hanel, Held; Statistical analyses: Hanel, Owen, Tagliaferri; Drafted manuscript: Hanel; Revised manuscript for intellectually important content: Owen, Held, Tagliaferri, Miller, Donath, Belavy; Approved final manuscript: All.
Corresponding author
Ethics declarations
Funding
No funding was received for the performance of this work.
Conflict of interest
The authors declare no conflicts of interest.
Availability of Data and Material
The data extracted as part of this systematic review and used in subsequent analysis is made available in Table 1.
Code Availability (Software Application or Custom Code)
Not applicable.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hanel, J., Owen, P.J., Held, S. et al. Effects of Exercise Training on Fear-Avoidance in Pain and Pain-Free Populations: Systematic Review and Meta-analysis. Sports Med 50, 2193–2207 (2020). https://doi.org/10.1007/s40279-020-01345-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-020-01345-1