
Abstract
Glioblastoma is highly aggressive and remains difficult to treat despite being the most common malignant primary brain tumor in adults. Current standard-of-care treatment calls for maximum resection of the tumor mass followed by concurrent chemotherapy and radiotherapy and further adjuvant chemotherapy if necessary. Despite this regimen, prognosis remains grim. Immunotherapy has shown promising success in a variety of solid tumor types, but efficacy in glioblastoma is yet to be demonstrated. Barriers to the success of immunotherapy in glioblastoma include: a heterogeneous tumor cell population, a highly immunosuppressive microenvironment, and the blood–brain barrier, to name a few. Several immunotherapeutic approaches are actively being investigated and developed to overcome these limitations. In this review, we present different classes of immunotherapy targeting glioblastoma, their most recent results, and potential future directions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Glioblastoma is a universally lethal brain tumor with an overall therapeutic failure. |
Glioblastoma encompasses several subtypes with different immune characteristics making them differentially susceptible to available and developed therapies. |
Immunotherapy is a promising therapeutic for glioblastoma and several approaches in this discipline are being developed and improved. |
Combining different therapies can be an interesting route to control glioblastoma from different angles. |
1 Introduction
Isocitrate dehydrogenase (IDH) wild-type diffuse and astrocytic grade IV glioma or glioblastoma is an aggressive and ultimately lethal primary malignancy of the brain for which the current treatment paradigm has advanced little over the past 15 years. Current standard-of-care treatment protocols for newly diagnosed glioblastoma consist of maximal surgical resection followed by cycles of radiation and alkylating chemotherapy (temozolomide [TMZ]). Despite this, median survival is less than 15 months [1].
Immunotherapy in the form of immune checkpoint inhibitors (ICIs) has achieved remarkable success in other aggressive cancers with previously poor prognoses such as melanoma and non-small cell lung cancer [2,3,4]. Unfortunately, similar results have been elusive in glioblastoma, with a multitude of failed trials [5, 6]. This reflects the multitude of challenges that limit immunotherapy efficacy, including the blood–brain barrier, intrinsic and acquired resistance to available therapies, antigen heterogeneity, and an immunosuppressive tumor microenvironment (TME). Efforts are ongoing to identify the optimal immunotherapy strategy that can overcome these challenges, using experiences from other difficult-to-treat malignancies [7]. This review outlines the current state of the glioblastoma immune landscape and immunotherapy, including each regimen’s strengths and weaknesses, and describes future directions for each immunotherapeutic regimen [8].
2 Molecular Heterogeneity and Immune Landscape of Glioblastoma
Various factors have led to the central nervous system (CNS) being viewed as an immune-privileged compartment, such as the tight blood–brain barrier encircling the CNS parenchyma preventing the entry of plasma inflammatory proteins and immune cells from the periphery. Additionally, the lack of lymphatic vessels and the mild reactivity to xenografts and bacterial and viral-related proteins after non-traumatic micro-injections into the CNS parenchyma further support this notion [9,10,11]. Despite this immune exclusion, the CNS hosts a diverse immune cell population, including microglia (which make up approximately 80% of the CNS immune cellularity), embryonically derived microglia-like macrophages (10%), innate immune cells [monocyte-derived cells, dendritic cells (DCs), and neutrophils] (3%), and adaptive immune cells [T and B cells] (1%) [12]. These immune cells are able to elicit an immune response similar to that observed peripherally.
In 2009, Verhaak et al. attempted to classify glioblastoma into subtypes based on their molecular signature, using 200 glioblastoma samples and two normal brain tissue samples. They proposed four subtypes: neural, proneural, mesenchymal, and classical. The neural subtype was clustered with normal brain tissue, while the other three were mainly defined by aberrations in PDGFRA/IDH1, NF1, and epidermal growth factor receptor (EGFR) respectively [13]. In 2016, the World Health Organization included molecular features in the diagnosis criteria of different adult gliomas, resulting in the division of glioblastoma (IDH wild-type), oligodendroglioma (IDHmut with 1p/19q co-deletion), and astrocytoma (IDHmut without codeletion) [14]. The recent 2021 World Health Organization classification maintained this general subdivision, with different astrocytic bifurcations grouped under a single diagnosis (astrocytoma with different grades 2, 3, or 4). Additionally, TERT promoter mutation, EGFR gene amplification, and chromosome 7/10 gain and deletion [+ 7/− 10] were included in the diagnosis of glioblastoma [15].
The immune landscape of glioblastoma is known to vary depending on the molecular subtype of the tumor [16, 17]. An increase in the gene signature of immune suppressive factors, chemokines, and signaling pathways was reported in mesenchymal glioblastoma compared with other subtypes (including interleukin (IL)-10, IL-23, transforming growth factor beta, programmed-death ligand 1 [PD-L1], CCL2, CCL22, and IL-6/STAT3) [16, 17]. These gene signatures are associated with an immunosuppressive phenotype of monocytes and macrophages [17]. CIBERSORT analysis reported that the mesenchymal subtype had a higher expression signature of tumor-associated macrophages, neutrophils, and CD4+ T cells, while the classical subtype exhibited an activated DC signature [16, 18]. In contrast, the proneural subset was found to be the least immunogenic, with a lower pool of B cells, CD3+ T cells, and CD163+ macrophages in the TME [19]. This heterogeneous immune landscape among the different glioblastoma subtypes should influence the choice of immunotherapy and may impact treatment outcomes. For instance, the proneural subtype is less likely to respond well to immunotherapy because of its cold TME, and has proven to be indifferent to aggressive chemotherapy and radiotherapy regimens.
3 Vaccine Therapies
3.1 Peptide Vaccine Trials
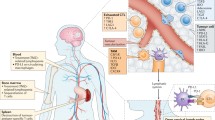
Peptide vaccines can be used to guide the immune system to neoplastic cells harboring peptide-corresponding tumor-specific antigens (TSAs) or tumor-associated antigens (TAAs) [20]. For TSA-derived peptide vaccines, epitope peptide-bearing mutations exclusively present in the tumor site are recognized by CD8+ and CD4+ T cells in a major histocompatibility complex 1 and 2 (MHC I and MHC II)-dependent mechanism. The same mechanism is applied for the TAA vaccine with a higher likelihood of systemic immune response because the antigen expression is not limited to tumor tissue [20] (Fig 1).

Glioblastoma vaccine mechanism of action: A different peptide vaccine groups developed: (1) dendritic cell (DC) vaccine loaded with different tumor-specific antigens/tumor-associated antigens; (2) peptide vaccines (epidermal growth factor receptor vIII [EGFRvIII], isocitrate dehydrogenase 1 [IDH1], Survivin, William’s tumor gene 1 [WT1]); (3) polypeptide vaccine. Pink-colored vaccines are injected intra-muscularly, Survivin intra-dermally, and EGFRvIII intravenously; B antigen presentation to naïve or memory T cells in the lymph nodes directly (DC vaccines) or after peptide processing (peptide vaccines); and (C) specific recognition of the target epitope of tumor cells by the cytotoxic CD8+ T cells and T-cell-mediated tumor killing. APC antigen-presenting cell, GSC glioma cancer stem cells, IFN interferon, IL interleukin, mRNA messenger RNA, TNF tumor necrosis factor. Figure designed on Biorender
However, glioblastoma frequently exhibits a low tumor mutational burden, and lacks a homogenously expressed TSA that can be used as a target [21]. Peptide vaccines that have been investigated in glioblastoma have variously targeted EGFRvIII (an EGFR mutant), isocitrate dehydrogenase 1 (IDH1), Survivin, and William’s tumor gene 1 (WT-1). However, no peptide vaccine is currently approved for the treatment of glioblastoma although studies remain ongoing. The failure of rindopepimut, a vaccine targeting EGFRvIII in phase III trials (NCT01480479), likely reflects the limitations of a treatment approach that targets a single TSA. While specific, this target is only expressed at varying degrees in a subset of patients with glioma [22]. Indeed, targeting EGFRvIII may only result in selective targeting of antigen-positive cells, with subsequent outgrowth by antigen-negative cells [23]. Other vaccine-based approaches have explored targeting IDH1, which is much more ubiquitously expressed in high-grade gliomas that have transformed from lower grades [24]. The arginine residue mutation R132H is the most frequent IDH1 mutation; tumorigenesis derives from the generation of oncometabolite 2-hydroxyglutarate, which increases genomic hyper-methylation and malignant transformation [20]. Preclinically, Schumacher et al. showed an anti-tumoral response in a transgenic mouse model bearing a mutant peptide derived from IDH1-R132H on a humanized MHC I and MHC II [25]. In a phase I safety trial, the injection of patients with R132H-positive glioma with an IDH1 peptide vaccine resulted in an enhanced immune response in 93.3% of patients bearing variable MHC alleles, along with 3-year progression-free survival (PFS) and overall survival (OS) rates of 0.63 and 0.84, respectively. However, immune responses were restricted to MHC-II, with no CD8 immune response being elicited. This was consistent with previously published results reporting a restricted CD4 antitumoral response to IDH1-R132H [25,26,27]. Further mechanistic studies are needed to elucidate this MHC-II restricted response. In this trial, vaccine-related side effects were mild and limited to grade 1 [28]. Although this approach may be suitable for patients with high-grade gliomas that have transformed, this does not address those patients with IDHwt high-grade glioma.
Other peptide vaccine approaches have targeted Survivin and WT-1. Survivin is a member of a protein family acting on apoptosis inhibition and regulation of mitosis; it has been found to be upregulated in multiple cancer types, including glioblastoma [29,30,31]. Early Survivin peptide vaccine trials were found to promote ex-vivo human glioblastoma cell elimination via T-cell dependent cytotoxicity [32]. Combined administration of Survivin vaccine and granulocyte-macrophage colony-stimulating factor promoted survival and decreased tumor mass and progression in GL261 glioma mice [ 20, 33]. However, unlike human glioblastoma, GL261 is highly immunogenic [34]. Several trials were conducted based on these preclinical findings, including a concluded phase I trial (PFS and OS of 17.6 and 86.6, respectively) [32] (ClinicalTrials.gov identifier: NCT01250470) and an actively recruiting phase II trial of SVN53-67/M57-KLH and TMZ (NCT02455557). WT-1 and its downstream molecules modulate both proliferation and migration as well as cell fate decision and death. An alteration in the WT-1 signaling pathway has been reported in multiple cancers and studies have confirmed WT-1 expression in gliomas [35,36,37,38]. A recent preclinical study demonstrated integration of high-affinity, WT-1-specific T-cell receptors using CRISPR gene editing improves antitumor T-cell function in glioblastoma both in vivo and in vitro [39]. These findings have been used to support the development of WT-1 protein as a TAA that can be targeted by peptide vaccine therapy. In a phase I study, PFS of 15.2–49.1 months was observed in seven patients with newly diagnosed glioblastoma injected with a mixture of TMZ and a WT-1-based peptide vaccine as part of a safety phase I clinical trial [40]. In another phase I/II uncontrolled study, 27 patients with World Health Organization 2016 grade III and IV gliomas were intradermally injected with a mixture of WT-1 peptide and inactivated whole cell pertussis vaccine once a week for at least 12 weeks. Progression-free survival and OS were 12.7 and 21.9 months, respectively [41]. These results may attract more attention to the inclusion of WT-1-based peptides in glioma immunotherapy vaccines.
Several clinical trials involving peptide vaccines are currently ongoing or set to begin soon. These trials are exploring various combinations of conjugated peptides, either alone or in combination with other therapies. For example, there is a phase I clinical study (NCT04808245) that aims to evaluate the safety and immunogenicity of a H3K27M peptide vaccine for H3-mutated gliomas. Another trial (NCT04280848) is conducting an immunogenicity assessment study using telomerase-derived universal cancer peptides for glioblastoma, with an expected enrollment of 56 participants. Additionally, a phase Ib trial (NCT05283109) is studying the effects of P30-linked EphA2, CMV pp65, and Survivin vaccination (P30-EPS vaccine) in HLA-A*0201-positive patients with newly diagnosed unmethylated glioblastoma. The results from these trials are highly anticipated.
3.2 DC-Based Vaccine Trials
CD4+ and CD8+ T cells typically recognize peptides presented by DCs in an MHC-dependent manner after phagocytosis and intracellular processing to generate a peptide-specific immune response. During the dual dialogue, several proinflammatory cytokines are released by DCs, improving anti-tumoral T-cell efficacy [42]. Protocols for autologous DC vaccines call for cells to be extracted from the patient, cultured, and loaded with TSA/TAA ex vivo before administration to the patient to mediate a T-cell response [20]. Success in preclinical and clinical studies motivated investigators to load DCs with different molecules to identify those with the most robust glioblastoma-specific response: peptides, tumor lysates, messenger RNA (mRNA), viruses, and cancer stem cells. We summarize the work conducted to date with these different DC-based approaches. The first class of DC vaccines are tumor peptide-loaded DCs. Dendritic cell activation can be mediated through the same epitopes used in peptide vaccines, including EGFRvIII. A phase I study injected EGFRvIII-specific peptide-KLH pulsed DCs into 12 patients with newly diagnosed glioblastoma after surgical resection and radiotherapy [43]. Median PFS and OS were 6.8 and 18.7 months, respectively, and no life-threatening adverse reactions or toxicities were observed [43]. Another phase I trial injected WT-1-loaded DCs into seven patients with high-grade gliomas. Five patients exhibited stable clinical responses with OS after the first DC vaccine of 12.3 months [44, 45]. A third phase I trial showed OS of 20.6–47.3 months and PFS of 15.4–47.3 months in patients with newly diagnosed glioblastoma treated with CMV phosphoprotein 65 RNA-specific DCs [46]. Whereas the phosphoprotein 65 RNA-DC-induced CMV-specific T-cell expansion might be of higher functionality than ex vivo, the heterogenous CMV-peptide expression on tumor cells can limit the clinical benefits (12-month OS using autologous ex-vivo expanded CMV-specific T cells) [47].
A tumor lysate-loaded DC vaccine (DC-VaxL) has been tested as well. In this technique, patient tumor cells are broken down to generate cellular fragments that are eventually presented to DCs. This allows a larger tumor-specific response owing to the presentation of usually unrecognized TAAs, but it can also generate off-target immune reactions. Yu et al. presented impressive results in a phase I safety trial of autologous tumor lysate-based DC vaccines administered to patients with recurrent glioblastoma, reporting an OS of 133 weeks and a highly specific immune response [48]. The recently published results of the phase III clinical trial for DC-VaxL found that for patients with newly diagnosed glioblastoma, the median OS was 19.3 months when treated with DC-VaxL compared with 16.5 months for patients in the control group who received temozolomide. Similarly, for patients with recurrent glioblastoma, the median OS was 13.2 months with DC-VaxL versus 7.8 months with temozolomide. Furthermore, the survival benefit of DC-VaxL over the control population increased over time in the tails of the survival curves. At 60 months, the survival rate was 13.0% for patients with newly diagnosed glioblastoma treated with DC-VaxL and 5.7% for those treated with temozolomide. For patients with recurrent glioblastoma, the survival rate was 11.1% at 30 months with DC-VaxL and 5.1% with temozolomide. This clinically meaningful extension of the survival of patients with newly diagnosed or recurrent glioblastoma may lead to the approval of DC-VaxL as the first immunotherapy treatment for glioblastoma in the near future.
Tumor-derived mRNA is a newly emerging class of molecules that can be loaded to DCs. Interest was generated into identifying the optimal mRNA antigen to present to DCs [49,50,51]. Lin et al. evaluated the expression profile of glioblastoma antigens using the gene expression profiling interactive analysis to determine their influence on clinical prognosis [51]. Patient survival rate and infiltration of antigen-presenting cells were associated with six overexpressed and mutated tumor antigens (ARHGAP9, ARHGAP30, CLEC7A, MAN2B1, ARPC1B, and PLB1) in glioblastoma [51]. These promising targets will be the foundation of several clinical trials (ClinicalTrials.gov identifiers: NCT02649582, NCT02709616).
Glioma stem cells were also loaded to DCs. Glioma stem cells are a cellular subtype known for self-renewal capability, resistance to chemoradiotherapies, and tumor recurrence [52,53,54]. Glioma stem cell elimination can allow a greater anti-tumor response. In a recently published preclinical study, Sy Do et al. used CD133 mRNA-loaded DCs targeting humanized mouse CD133-positive glioma stem cells, leading to a robust and long-lasting immune response along with inhibition of CD133-positive glioma stem cell propagation and tumor growth [55].
Finally, viral antigen-loaded DC cytomegalovirus nucleic acids and proteins are found in both primary and recurrent glioblastoma. Thus, pp65 was incorporated into DC vaccines as a potential novel immunotherapy [56]. A phase I trial evaluating pp65-specific DCs along with preconditioning with tetanus-diphtheria toxoid in patients with newly diagnosed glioblastoma showed an encouraging PFS of 15.4–47.3 months and an OS of 20.6–47.3 months [46]. A phase II randomized clinical trial in patients with glioblastoma who underwent resection and completed standard chemoradiation with CMV pp65-loaded autologous DC-tetanus-diphtheria toxoid pre-conditioning (ClinicalTrials.gov identifier: NCT02366728) has been completed and results are pending. Another randomized phase II trial involving a CMV pp65 DC vaccine is currently recruiting (ClinicalTrials.gov identifier: NCT02465268).
3.3 Early-Phase Development of Multi-Peptide Vaccines
Vaccine strategies using multiple fusion peptides have been developed to bypass the limitations of single-peptide vaccines. An example of limitation is the restriction to the HLA-A 02 haplotype and several glioblastoma subtypes, allowing only a small subgroup of patients with glioblastoma to benefit from targeting a single tumor antigen because of the heterogeneity of antigen expression in glioblastoma [20].
3.3.1 IMA950
IMA950 was developed from the fusion of 11 TAAs found in the majority of glioblastoma subtypes to activate multiple anti-tumor TUMAP-specific T-cell clones [20]. The TUMAP-derived poly-clonality increases the probability of a highly specific T-cell response against tumor cells, owing to the limited likelihood of poly-internalization of targeted antigens [20]. In a phase I trial, patients with glioblastoma who underwent tumor resection received an intradermal injection with IMA950 before or after starting chemoradiotherapy. The majority did not have remarkable survival results (PFS at 6 months of 74% and median OS of 15.3 months) [57].
3.3.2 ICT-107
ICT-107 is a glioblastoma-specific polypeptide vaccine [20]. Dendritic cells were loaded with six peptides selected based on a gene-overexpression comparison between glioblastoma cells and nonmalignant tissues: melanoma-associated antigen 1, HER2, interferon-inducible protein AIM2, I-dopachrome tautomerase, melanocyte protein (PMEL), and IL-13 receptor subunit-α2 (IL-13Rα2) [20]. In a phase I clinical trial, ICT-107 DC vaccines were administered to 15 patients with newly diagnosed glioblastoma. Median PFS was 16.9 months and median OS was 38.4 months. Six patients did not show any evidence of tumor recurrence after 40.1 months [58]. A randomized phase II trial in 124 patients with newly diagnosed glioblastoma (77 HLA A2-positive patients) reported encouraging results in the experimental group especially for HLA-A2-positive patients including a statistically significant elevation in the PFS by 2.2 months in the ICT-107 cohort with preservation of the quality of life in addition to a considerable therapeutic benefit with ICT-107 for MGMT methylated and unmethylated HLA-A2 patients [59]. The trial was as deemed to be underpowered because of insufficient participant numbers, which disabled weighty conclusions from subgroup analyses [59]. Financial difficulties disrupted the phase III trial of this vaccine, and progress in the ICT-107 program has stalled (ClinicalTrials.gov identifier: NCT02546102).
3.3.3 Heat Shock Proteins
Heat shock proteins (HSPs) are a member of the intracellular stress regulating chaperone family, inhibiting protein agglomeration and guiding misfolded proteins to proteasome degradation [60]. HSP70 and HSP90 have been reported to stimulate both innate and adaptive responses in addition to binding to some tumor antigens in glioblastoma [61]. A phase I clinical study vaccinated 12 patients with high-grade glioma with HSPPC-96. A tumor-specific peripheral immune response was observed in 11 patients [62]. The phase II multicenter clinical trial for patients with resectable glioblastoma treated with HSPPC-96-bind antigens reported median and 6-month OS to be 42.6 weeks and 29.3%, respectively [63]. Multiple subsequent trials are assessing combinations with radiation therapy, temozolomide, and pembrolizumab (an immune checkpoint inhibitor) with and without HSPPC-96 (NCT03018288). NCT01814813 is assessing HSPPC-96 with bevacizumab in recurrent glioblastoma.
4 ICIs
Cancer cells utilize several mechanisms to escape immune surveillance and demolition. One example is the “cold” microenvironment that promotes a state of immune tolerance and expression of immune cell inhibitory receptors (“immune checkpoints”) [64, 65]. Potential therapies could target these receptors using ICIs [66]. Promising results in many solid tumors have prompted study of ICIs such as anti-programmed cell death protein 1 (PD-1) and cytotoxic T-lymphocyte-associated protein 4 in glioblastoma.
4.1 Inhibitors Targeting PD-1, PD-L1, and/or Cytotoxic T-Lymphocyte-Associated Protein 4
Downstream effectors of the PD-1/PD-L1 pathway have a suppressive role on tumoral T cells [67]. Programmed-death ligand 1 is upregulated in multiple types of solid tumors. Usually, higher expression of PD-L1 predicts better clinical efficacy of PD-1/PD-L1 checkpoint blockades [68]. Nduom et al. reported that tumor cells with a PD-L1 expression of 1% or more were observed in 61% of patients with glioblastoma and 38% had at least 5% or greater PD-L1 expression [69]. The results of a phase I clinical trial called KEYNOTE-001, which investigated the effectiveness of pembrolizumab (anti-PD1) in treating advanced stage non-small cell lung carcinoma, showed that patients with non-small cell lung carcinoma who had PD-L1 expression on more than 50% of cells had a response rate of 45.2%. Patients with lower levels of PD-L1 expression had lower response rates, with 16.5% for those with 1–49% expression and 16.5% for those with less than 1% expression [70, 71]. These findings led to the accelerated Food and Drug Administration approval of pembrolizumab for patients with non-small cell lung carcinoma with PD-L1 expression greater than 1% [72]. Nevertheless, despite high levels of expression of PD-L1 on both tumor cell and immunosuppressive immune cells in the TME, a good infiltration of proinflammatory immune cells is required to obtain a clinical response with pembrolizumab [73]. The first clinical trial utilizing nivolumab (anti-PD1) therapy administered with or without ipilimumab (cytotoxic T-lymphocyte-associated protein 4) was CheckMate 143. Results from different trial phases demonstrated a higher clinical tolerance in the nivolumab-alone arm, and no significant survival difference between the two groups was reported [ 74, 75]. Two large phase III clinical trials were subsequently conducted (ClinicalTrials.gov identifier: NCT02617589 and NCT02667587). No survival benefit was observed for nivolumab when added to standard treatment in patients with glioblastoma and methylated MGMT or when compared to TMZ. Emphasizing the clinical and immunological relevance of the timing of anti-PD1 treatment, Cloughesy et al. reported that the time of initiation of the anti-PD1 treatment can be of considerable importance. According to their findings, neoadjuvant pembrolizumab can lead to longer patient survival in addition to a higher focal expression of PD-L1, compared with adjuvant pembrolizumab treatment [76].
In summary, three large phase III trials demonstrated that nivolumab does not produce a survival advantage when given to unselected patients with glioblastoma [6]. However, clinical trials of other PD-1 and PD-L1 inhibitors, combinations with other immunotherapies, and evaluating predictive biomarkers are ongoing (Table 1).
5 Oncolytic Viral Therapies
Oncolytic virus therapy is a promising new immunotherapy for cancer treatment. An oncolytic virus is a genetically engineered or naturally existing virus that can preferentially target and destabilize cancer cells without affecting normal tissues [77].
5.1 Recombinant Oncolytic Poliovirus, PVSRIPO: Food and Drug Administration Breakthrough Therapy Designation
PVSRIPO is a live, weakened, poliovirus type 1 vaccine currently recognized as a promising cancer therapy (Fig. 2). It targets cells expressing the CD155/Necl5 poliovirus receptor, which is an onco-fetal cell adhesion molecule frequently expressed in glioblastoma. In the PVSRIPO vaccine, the adjacent internal ribosome entry site was substituted with human rhinovirus type 2 to prohibit neurovirulence and limit viral affinity to CNS cellularity [78].

Anti-glioblastoma immunotherapy approaches; A oncolytic virus vaccine; B immune checkpoint inhibitors; C bi-specific T-cell engagers; D chimeric antigen receptor (CAR) T-cell therapy; and E immunocytokines. CTLA4 cytotoxic T-lymphocyte-associated protein 4, EGFR epidermal growth factor receptor, GBM glioblastoma, IL interleukin, MHC major histocompatibility complex, PD1 programmed cell death protein 1, TCR T-cell receptor, TNF tumor necrosis factor. Figure designed on Biorenders
Desjardins et al. evaluated seven PVSRIPO doses, with a range between 107 and 1010 viral particles = 50% tissue-culture infectious doses injected intratumorally to 61 adult patients who had recurrent supratentorial glioblastoma. Survival rate reached a plateau of 21% at 24 months in the experimental group compared to historical controls and remained stable through 36 months [79]. According to a combined analysis of recent virotherapy trials for recurrent glioblastoma, the percentage of patients who survived for 24 months overall is estimated to be 15%, while the proportion who survived for 36 months is 9% [80], which makes the aforementioned results clinically significant. These results from a completed phase I clinical trial (ClinicalTrials.gov identifier: NCT01491893) motivated the Food and Drug Administration to approve a breakthrough therapy designation to the recombinant oncolytic poliovirus PVSRIPO in May 2016.
5.2 HSV-1, Adenovirus, Reovirus
Herpes virus simplex 1 (HVS-1) is the most commonly used and sole multi-generational engineered virus in oncolytic virus therapy. Different HSV-1 generations only differ in the number of added genes to the original HSV-1 genome. Todo et al. engineered G47Δ, a triple-mutated third-generation oncolytic HSV-1 expressing an additional deletion mutation to the second-generation HSV-1, G207 [81]. For human application, G47∆ is currently the only third-generation HSV‐1 available [82]. Following the successful conclusion of a Japanese phase I–IIa trial in patients with recurrent glioblastoma, a phase II single-arm safety study (UMIN-CTR Clinical Trial Registry UMIN000015995) focused on the efficacy of G47∆ in 19 adult patients with residual or recurrent supratentorial glioblastoma was conducted, and recently published its results [83]. The 1-year survival rate after G47∆ injection was 84.2%, median OS after G47∆ injection reached 20.2 and 28.8 months, respectively. In addition to fever, vomiting, nausea, lymphocytopenia, and leukopenia as G47∆-related common adverse events, increasing numbers of tumor-infiltrating CD4+/CD8+ lymphocytes and persistent low numbers of Foxp3+ cells were found upon biopsy [83]. In another recent study, the same group confirmed that G47∆ is safe for patients with progressive glioblastoma when administered intratumorally at doses of up to 1 × 10^9 plaque-forming units per dose for two doses within a 14-day period. Japan’s Ministry of Health, Labour and Welfare then approved Delytact® (commercial name for G47∆) for the treatment of malignant glioma. Efficacy findings were less exciting with a median OS of 7.3 months and a 1-year survival rate of 38.5%, both from the last G47∆ administration. According to the investigators, these results justified the foundation of the phase II clinical trial in patients with progressive glioblastoma [84].
Recombinant adenovirus is another promising oncolytic viral therapy. Adenovirus has a double-stranded DNA genome and infects human cells using the coxsackie and adenovirus receptor [77]. After endocytosis into tumor cells, adenoviruses remain episomal in the cytosol while expressing its genome. The genetically modified adenovirus ONYX-015 was the first to undergo a phase I clinical trial, where it resulted in no serious side effects being reported [85]. Adenovirus Delta-24 was designed to selectively replicate in cells deficient in the Rb/p16 tumor suppressor pathway [77]. Lang et al. reported objective and long-lasting biological and clinical responses from a phase I dose-escalation clinical trial in 37 patients with recurrent glioblastoma. For patients with a long-term response (> 3 years), evidence demonstrated immune infiltration (T cells and macrophages) into the TME with minimal toxicity especially when administrated with convection-enhanced delivery [86, 87]. Results from a phase II clinical trial evaluating the anti-tumor response of DNX-2401, a genetically modified oncolytic adenovirus, and intravenous pembrolizumab are eagerly awaited (NCT02798406).
A phase Ib study in 2018 conducted by Samson et al. demonstrated that intravenous administration of fnoncolytic human orthoreovirus (reovirus) lead to infection of both glioblastoma and brain metastases tumor cells, and increased cytotoxic T-cell tumor infiltration in comparison to patients not treated with the virus. They also found an upregulation of interferon-regulated gene expression and the PD-1/PD-L1 pathway in tumors via an interferon-related mechanism, and that supplementation of anti-PD-1 to the reovirus improves systemic efficiency of the therapy in a preclinical glioblastoma model [88]. These findings are worth further clinical investigation.
6 CAR T-Cell Therapy
Chimeric antigen receptor (CAR) T-cell therapy is another extensively investigated potential treatment, especially after the success reported with hematological malignancies [2,3,4]. A small number of patients with glioblastoma achieved complete response to CAR T cells [89]. Potential roadblocks challenging the therapeutic success of CAR T cells in solid tumors include: limited number of targetable antigens with a heterogenous antigen expression, serious off-target side effects due to the expression of the targeted antigen by non-malignant tissues, limited activation and expansion of injected T cells before reaching tumor sites, short-lasting local immune response, and the immunosuppressive TME [89]. Several techniques to overcome these challenges are currently in clinical and preclinical studies. This section focuses on completed clinical trials.
6.1 EGFRvIII
As EGFRvIII is expressed in around 30% of glioblastoma tumors, it was among the first targets of CAR T-cell therapy. In a phase I/II trial (ClinicalTrials.gov identifier: NCT01454596), patients with EGFRvIII-expressing glioblastoma were infused with EGFRvIII-targeting CAR T cells. No adverse events associated with the administration of up to 1 × 1010 CAR T cells were observed. Serious adverse events occurring in one patient receiving 3 × 1010 CAR T cells included dyspnea and hypoxia. Another patient who received an administration of 6 × 1010 CAR T cells experienced severe adverse effects. The patient developed acute dyspnea and oxygen desaturation 1 h after the CAR infusion, and these symptoms were not successfully managed by bilevel positive airway pressure and intubation. Tragically, the patient died 4 h post-infusion because of severe pulmonary edema [90]. The gravity of adverse events along with a low clinical success owing to the selection pressure and outgrowth of antigen-negative cells reduced the excitement for the use of this tumor antigen as a target for CAR T cells.
6.2 IL-13Rα2
IL-13Rα2 is an IL-13 receptor frequently overexpressed in adult and pediatric glioblastoma tumors, but under-expressed in non-malignant tissues, except the testes [91]. Chimeric antigen receptor T cells carrying a mutated form of IL-13 have been engineered to target IL-13Rα2-expressing tumors. Feasibility and safety of this CAR construct were confirmed in up to 12 intracranial injections (maximum dose 1 × 1018 CAR T cells) into three patients with recurrent glioblastoma [92]. Two phase I clinical trials are currently recruiting patients to investigate the anti-tumoral activity of IL-13Rα2 CAR T cells, the first with or without nivolumab and ipilimumab (ClinicalTrials.gov identifier: NCT04003649) and the other in different leptomeningeal disease-causing tumors including glioblastoma (ClinicalTrials.gov identifier: NCT04661384).
6.3 HER2
HER2 is an EGFR overexpressed in multiple cancer types (including approximately 80% of glioblastoma tumors) but normally expressed in non-malignant epidermal cells [93]. Work by Shen et al. has shown that third-generation HER2-specific CAR T cells can efficiently eradicate glioblastoma cells in vitro and can have enhanced immune activity if combined with PD-1 blockades [91, 94]. Additionally, no dose-limiting toxic effects were observed in patients intravenously injected with up to 1 × 108 HER2-specific CAR T cells, engineered with a CD28.ζ endodomain [95].
Several studies reported an increased anti-tumoral efficacy of CAR T cells boosted by cytokines including IL-12 and IL-23, against several systemic tumor models [96,97,98]. This motivated Agliardi et al. to intratumorally inject IL-12 alongside CAR T cells in a glioblastoma mouse model to test its enhancing effects [99]; results included enhanced cytotoxicity of CAR-T cells, modulation of TME, and increased infiltration of CD4+ T cells. Further incorporation of cytokines into the CAR T-cell construct for glioblastoma immunotherapy should be explored [99].
Several other tumor targets are currently in preclinical investigation including CAIX, CSPG4, CD70, EphA2, and TROP2 [91]. Nevertheless, the intensive investigation on CAR T cells encompasses other angles other than antigen specificity to surmount the abovementioned roadblocks. We believe the most challenging is the antigen dilemma; very few tumor-specific antigens are available as targets with only a small proportion of tumor cells expressing them, making high-efficiency CAR treatment targeting a single antigen of low likelihood. Neoantigens seem like a potential solution to this dilemma; however, most of them are derived from intracellular proteins and are patient specific, causing feasibility issues [89, 100]. An ideal route of delivery of CAR T cells would be systemically, if side effects could be prevented. Unfortunately, this is not the case, systemic and off-target toxicities were reported in several studies [101]. Localized administration of CARs [102, 103] and the inducible suicide genes developed [104] and continuously improved [105] are being used to enhance safety. Studies have shown that the CAR T-cell generation protocol, including initial activation with anti-CD3/anti-CD8 activation beads instead of traditional concavaline A and culture with hIL7/hIL15-supplemented media, plays a crucial role in the longevity and anti-tumor efficiency of the generated CARs [106, 107]. Therefore, small adjustments to the CAR generation protocol can be remarkably effective. Finally, despite the immunosuppressive TME being a significant obstacle to the anti-tumoral efficacy of CAR T cells, potential solutions are in the near future. For instance, cytokine-secreting CARs, such as IL-15-secreting CARs, can mitigate the immunosuppression of the regulatory T cells in the TME [108] and the use of cytokine switch receptors that convert inhibitory cytokine signals into survival-promoting signals [109].
7 Recent Immunotherapies
7.1 Immunocytokines
Cytokine administration is an emerging technique to convert the immunologically suppressive glioma microenvironment into a friendly environment, allowing for effective antitumor immunity. Multiple proinflammatory cytokine candidates (e.g., IL-2, IL-6, IL-12, tumor necrosis factor [TNF]-α) are currently being investigated for this type of therapy [110]. Different approaches are used to deliver cytokines to the TME including local administration, protein fusion, and inducible expression with different constructs (especially CARs) [110]. In an interesting study, Weiss et al. used three murine L19 targeting cytokine-fused antibodies (L19-mIL-2, L19-mIL-12, and L19-mTNF) to assess the efficacy of these cytokines in modeling the TME [110]. They discovered that L19 intravenous administration of L19-mIL-12 or L19-mTNF but not L19-mIL-2 cured a proportion of tumor-bearing mice before depletion of CD4 or CD8 T cells, suggesting adoptive immunity dependency of these cytokines [110]. A clinical trial evaluating the safety and efficacy of the L19-hTNF in patients with IDH-1wt glioblastoma is currently underway (ClinicalTrials.gov identifier: NCT03779230.)
7.2 BiTEs
Bi-specific T-cell engagers (BiTEs) are an innovative form of immunotherapy that hold promising potential for treating several types of tumors, including glioblastoma [111, 112]. Bi-specific T-cell engagers allow for the co-localization of cytotoxic T cells with heterogeneous T-cell receptors and tumor cells by utilizing two linked antigen-recognizing variable fragments without the Fc region of antibodies. This unique feature allows the BiTEs to penetrate the blood–brain barrier following intravenous administration [113, 114]. The bispecific fragment recognizes the CD3 protein on T cells and tumor-specific antigens present on tumor cells. EGFRvIII was the first target of BiTEs for glioblastoma. Choi et al. designed the first murine BiTES recognizing CD3 and EGFRvIII on glioblastoma, and reported a potent elimination of EGFRvIII-expressing tumor cells with a low dose of the drug (10 ng/mL) [112]. Subsequently, Gedeon et al. proposed fully humanized BiTEs that have proven high functionality [115]. Amgen conducted the first phase I clinical trial on humans using CD3-EGFRvIII BiTES (AMG 596). While this trial was completed in December 2021 (NCT03296696), official results are not yet published. However the interim analysis indicates that AMG 596 was tolerated and efficient for patients with recurrent glioblastoma [116]. Another phase I clinical trial was initiated (NCT04903795), this time targeting EGFRvIII and CD3 using a single-chain variable fragment 139 and 28F11, respectively. These two fragments are linked and were previously used in clinical settings [117, 118]. A more comprehensive review of BiTEs use in glioblastoma was previously published by our team [119].
8 Treatment Sequencing and Combination Approaches
As previously indicated, the current standard of care for glioblastoma proposes a maximum possible resection of the tumor, with concomitant radiotherapy and oral adjuvant chemotherapy (TMZ) without an official inclusion of any immunotherapy. Several preclinical and clinical studies explored the combinatorial benefits of multiple immunotherapies or the combination of classical and immunotherapy against glioblastoma [120]. Temozolomide with ICIs is the most studied combination for glioblastoma, TMZ is an alkylating agent that deposits methyl groups on the guanine base of the DNA, leading to a DNA double-stranded break and cell apoptosis of rapidly proliferating cells. The tumor lysates resulting from this mechanism and from the DNA double-stranded break induced by radiotherapy are phagocytized by the antigen-presenting cell and presented to the T cell, which, subsequently, promotes a polyclonal infiltration of T cells [121], and this made the rational foundation to investigate the combination of TMZ and ICIs.
Despite that the standard-dose TMZ might downregulate PD-L1 from the tumor surface and mitigate the efficacy of anti-PD1/PD-L1 [122], a metronomic or low dose of TMZ has been shown to maintain or increase the survival benefits of anti-PD1 therapy and increase the count of TILs in preclinical studies [123, 124]. The combination of radiotherapy alone or radio-chemotherapy with nivolumab (anti-PD1) was not successful in phase III clinical trials of CheckMate 498 and 548 [125, 126].
The combination of multiple checkpoint blockades was also assessed; anti-PD1 and anti-LAG3 together significantly increased survival in a cohort of mice in comparison to the no-treatment arm. However, the survival benefits and immune profile were similar to the mono-therapy groups (anti-PD-1 or anti-LAG3 alone) [127].
Anti-vascular endothelial growth factor inhibitors effect on glioblastoma is increasingly being investigated, Soubéran et al. [128] have reported increased innate immune cell infiltration between days 21 and 28 post-treatment with anti-vascular endothelial growth factor in GL261 glioma-bearing mice [128], which made it a rational combination therapy with sintilimab (anti-PD-1 approved in China) in a newly opened clinical trial (NCT05540275).
9 Conclusions/Future Research
Despite promising results of different immunotherapies in other cancer types, therapeutic success with immunotherapy in glioblastoma has been limited. Roadblocks include a limited number of targetable antigens with a heterogenous antigen expression, serious off-target side effects, limited activation and expansion of injected T cells before reaching tumor sites, and the immunosuppressive TME [89]. Additionally, the best murine models currently available are still insufficient in providing an accurate representation of human tumors because of poor recapitulation, which includes in vitro genetic deviation, changes in tumor cells, and poor recapitulation of the human TME. Furthermore, most syngeneic mouse models carry a higher mutational burden than human glioblastomas, making them less effective in mimicking the human condition. Further efforts dedicated to overcoming the challenges limiting the therapeutic success of immunotherapies in solid tumors are warranted, especially regarding the generation of more accurate preclinical mouse models. Preclinical efforts with emerging new treatment pathways allow a better understanding of immunobiological dynamics in glioblastoma and ultimately have the potential to have a meaningful impact on patient outcomes [7, 129]. Evidence suggests that mono-immunotherapy may not be sufficient to overcome potent immunosuppression present in glioblastoma, and attempts are being made to develop combinatorial approaches [130].
Personalized treatment is another emerging therapeutic pathway [79]. The heterogenicity of glioblastoma makes it very difficult to develop a monotherapy that provides broad meaningful benefits. The Ivy Brain Tumor Center at the Barrow Neurological Institute tests new combination therapies for glioblastoma and other aggressive brain tumors and adjusts through a phase 0 clinical trial that matches new combination drug regimens to an individual’s unique tumor after advanced genetic testing within 10 days from surgery [131].
Immunotherapy restores hope in improving clinical outcomes for patients with glioblastoma, a devastating highly lethal disease. Despite the disappointing results of most of the concluded clinical trials, they have further developed our understanding of glioblastoma physiopathology. Exiting ongoing preclinical and clinical studies are relying on and building upon what was learned from previous experiences.
References
Tan AC, et al. Management of glioblastoma: state of the art and future directions. CA Cancer J Clin. 2020;70(4):299–312.
Maude SL, et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N Engl J Med. 2014;371(16):1507–17.
Grupp SA, et al. Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med. 2013;368(16):1509–18.
Porter DL, et al. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med. 2011;365(8):725–33.
Chuntova P, et al. Unique challenges for glioblastoma immunotherapy-discussions across neuro-oncology and non-neuro-oncology experts in cancer immunology. Meeting report from the 2019 SNO Immuno-Oncology Think Tank. Neuro Oncol. 2021;23(3):356–75.
Khasraw M, et al. PD-1 inhibitors: do they have a future in the treatment of glioblastoma? Clin Cancer Res. 2020;26(20):5287–96.
Miranda WY, Daniela FQ. Immunotherapy for glioblastoma: current progress and challenges. Front Immunol. 2021. https://doi.org/10.3389/fimmu.2021.78268.
Lim M, et al. Current state of immunotherapy for glioblastoma. Nat Rev Clin Oncol. 2018;15:422–42.
Medawar PB. Immunity to homologous grafted skin; the fate of skin homografts transplanted to the brain, to subcutaneous tissue, and to the anterior chamber of the eye. Br J Exp Pathol. 1948;29(1):58–69.
Andersson PB, Perry VH, Gordon S. The acute inflammatory response to lipopolysaccharide in CNS parenchyma differs from that in other body tissues. Neuroscience. 1992;48(1):169–86.
Locatelli G, et al. Primary oligodendrocyte death does not elicit anti-CNS immunity. Nat Neurosci. 2012;15(4):543–50.
Mrdjen D, et al. High-dimensional single-cell mapping of central nervous system immune cells reveals distinct myeloid subsets in health, aging, and disease. Immunity. 2018;48(2):380-95.e6.
Verhaak RG, et al. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell. 2010;17(1):98–110.
Louis DN, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–20.
Louis DN, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. 2021;23(8):1231–51.
Wang Q, et al. Tumor evolution of glioma-intrinsic gene expression subtypes associates with immunological changes in the microenvironment. Cancer Cell. 2017;32(1):42-56.e6.
Doucette T, et al. Immune heterogeneity of glioblastoma subtypes: extrapolation from the Cancer Genome Atlas. Cancer Immunol Res. 2013;1(2):112–22.
Newman AM, et al. Robust enumeration of cell subsets from tissue expression profiles. Nat Methods. 2015;12(5):453–7.
Martinez-Lage M, et al. Immune landscapes associated with different glioblastoma molecular subtypes. Acta Neuropathol Commun. 2019;7(1):203.
Visish MS, et al. Tumor vaccines for malignant gliomas. Neurotherapeutics. 2017;14:345–57.
Hodges TR, et al. Mutational burden, immune checkpoint expression, and mismatch repair in glioma: implications for immune checkpoint immunotherapy. Neuro Oncol. 2017;19:1047–57.
Weller M, et al. Assessment and prognostic significance of the epidermal growth factor receptor vIII mutation in glioblastoma patients treated with concurrent and adjuvant temozolomide radiochemotherapy. Int J Cancer. 2014;134:2437–47.
Weller M, et al. Rindopepimut with temozolomide for patients with newly diagnosed, EGFRvIII-expressing glioblastoma (ACT IV): a randomised, double-blind, international phase 3 trial. Lancet Oncol. 2017;18:1373–85.
Sanson M, et al. Isocitrate dehydrogenase 1 codon 132 mutation is an important prognostic biomarker in gliomas. J Clin Oncol. 2009;27:4150–4.
Schumacher T, et al. A vaccine targeting mutant IDH1 induces antitumour immunity. Nature. 2014;512:324–7.
Bunse L, et al. Proximity ligation assay evaluates IDH1R132H presentation in gliomas. J Clin Investig. 2015;125(2):593–606.
Bunse L, et al. Suppression of antitumor T cell immunity by the oncometabolite (R)-2-hydroxyglutarate. Nat Med. 2018;24(8):1192–203.
Platten M, et al. A vaccine targeting mutant IDH1 in newly diagnosed glioma. Nature. 2021;592:463–8.
Altieri DC. Survivin, versatile modulation of cell division and apoptosis in cancer. Oncogene. 2003;22:8581–9.
Garg H, et al. Survivin: a unique target for tumor therapy. Cancer Cell Int. 2016;16:49.
Kajiwara Y, et al. Expression of survivin in astrocytic tumors. Cancer. 2003;97:1077–83.
Fenstermaker RA, et al. Clinical study of a survivin long peptide vaccine (SurVaxM) in patients with recurrent malignant glioma. Cancer Immunol Immunother. 2016;65(11):1339–52.
Ciesielski MJ, et al. Antitumor cytotoxic T-cell response induced by a survivin peptide mimic. Cancer Immunol Immunother. 2010;59:1211–21.
Sanchez VE, et al. GL261 luciferase-expressing cells elicit an anti-tumor immune response: an evaluation of murine glioma models. Sci Rep. 2020;10(1):11003.
Kalani MYS, et al. Wnt-mediated self-renewal of neural stem/progenitor cells. Proc Nat Acad Sci. 2008;105:16970–5.
Holland EC. Gliomagenesis: genetic alterations and mouse models. Nat Rev Genet. 2001;2:120–9.
Clark AJ, et al. Wilms tumor 1 expression in malignant gliomas and correlation of +KTS isoforms with p53 status. J Neurosurg. 2007;107:586–92.
Rushing EJ, et al. High-grade astrocytomas show increased Nestin and Wilms’s Tumor Gene (WT1) protein expression. Int J Surg Pathol. 2010;18:255–9.
Ruggiero E, et al. CRISPR-based gene disruption and integration of high-avidity, WT1-specific T cell receptors improve antitumor T cell function. Sci Transl Med. 2022;14:eabg8027.
Hashimoto N, et al. Wilms tumor 1 peptide vaccination combined with temozolomide against newly diagnosed glioblastoma: safety and impact on immunological response. Cancer Immunol Immunother. 2015;64:707–16.
Kawanishi Y, et al. IMT-03 clinical trial for newly diagnosed malignant glioma with WT1-W10 vaccination. Neuro Oncol Adv. 2019;1(Suppl_2):ii17.
Steinman RM, et al. The induction of tolerance by dendritic cells that have captured apoptotic cells. J Exp Med. 2000;191:411–6.
Sampson JH, et al. An epidermal growth factor receptor variant III-targeted vaccine is safe and immunogenic in patients with glioblastoma multiforme. Mol Cancer Ther. 2009;8:2773–9.
Sakai K, et al. Dendritic cell-based immunotherapy targeting Wilms’ tumor 1 in patients with recurrent malignant glioma. J Neurosurg. 2015;123:989–97.
Huang B, et al. Current immunotherapies for glioblastoma multiforme. Front Immunol. 2021;11:603911.
Mitchell DA, et al. Tetanus toxoid and CCL3 improve dendritic cell vaccines in mice and glioblastoma patients. Nature. 2015;519:366–9.
Weathers SP, et al. Glioblastoma-mediated immune dysfunction limits CMV-specific T cells and therapeutic responses: results from a phase I/II trial. Clin Cancer Res. 2020;26(14):3565–77.
Yu JS, et al. Vaccination with tumor lysate-pulsed dendritic cells elicits antigen-specific, cytotoxic T-cells in patients with malignant glioma. Cancer Res. 2004;64:4973–9.
Ye L, et al. Identification of tumor antigens and immune landscape in glioblastoma for mRNA vaccine development. Front Genet. 2021;12:701065.
Wu C, et al. Tumor antigens and immune subtypes of glioblastoma: the fundamentals of mRNA vaccine and individualized immunotherapy development. J Big Data. 2022;9:92.
Lin H, et al. Identification of tumor antigens and immune subtypes of glioblastoma for mRNA vaccine development. Front Immunol. 2022;13:249.
Chen R, et al. A hierarchy of self-renewing tumor-initiating cell types in glioblastoma. Cancer Cell. 2010;17:362–75.
Bao S, et al. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature. 2006;444:756–60.
Fidoamore A, et al. Glioblastoma stem cells microenvironment: the paracrine roles of the niche in drug and radioresistance. Stem Cells Int. 2016;2016:1–17.
Do ASS, et al. CD133 mRNA-loaded dendritic cell vaccination abrogates glioma stem cell propagation in humanized glioblastoma mouse model. Mol Ther Oncolytics. 2020;18:295–303.
Nair SK, et al. Immunological targeting of cytomegalovirus for glioblastoma therapy. OncoImmunology. 2014;3: e29289.
Rampling R, et al. A Cancer Research UK first time in human phase I trial of IMA950 (novel multipeptide therapeutic vaccine) in patients with newly diagnosed glioblastoma. Clin Cancer Res. 2016;22:4776–85.
Phuphanich S, et al. Phase I trial of a multi-epitope-pulsed dendritic cell vaccine for patients with newly diagnosed glioblastoma. Cancer Immunol Immunother. 2013;62:125–35.
Wen PY, et al. A randomized double-blind placebo-controlled phase II trial of dendritic cell vaccine ICT-107 in newly diagnosed patients with glioblastoma. Clin Cancer Res. 2019;25:5799–807.
Craig EA, et al. Heat shock proteins and molecular chaperones: mediators of protein conformation and turnover in the cell. Cell. 1994;78:365–72.
Graner MW, Bigner DD. Chaperone proteins and brain tumors: Potential targets and possible therapeutics. Neuro Oncol. 2005;7:260–8.
Crane CA, et al. Individual patient-specific immunity against high-grade glioma after vaccination with autologous tumor derived peptides bound to the 96 KD chaperone protein. Clin Cancer Res. 2013;19:205–14.
Bloch O, et al. Heat-shock protein peptide complex–96 vaccination for recurrent glioblastoma: a phase II, single-arm trial. Neuro Oncol. 2014;16:274–9.
Drake CG, Jaffee E, Pardoll DM. Mechanisms of immune evasion by tumors. Adv Immunol. 2006;90:51–81.
Armand P. Immune checkpoint blockade in hematologic malignancies. Blood. 2015;125:3393–400.
Sharma P, Allison JP. Dissecting the mechanisms of immune checkpoint therapy. Nat Rev Immunol. 2020;20:75–6.
Dai S, et al. The PD-1/PD-Ls pathway and autoimmune diseases. Cell Immunol. 2014;290:72–9.
Weber JS, et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015;16:375–84.
Nduom EK, et al. PD-L1 expression and prognostic impact in glioblastoma. Neuro Oncol. 2016;18(2):195–205.
Garon EB, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372(21):2018–28.
Doroshow DB, et al. PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nat Rev Clin Oncol. 2021;18(6):345–62.
Sul J, et al. FDA approval summary: pembrolizumab for the treatment of patients with metastatic non-small cell lung cancer whose tumors express programmed death-ligand 1. Oncologist. 2016;21(5):643–50.
de Groot J, et al. Window-of-opportunity clinical trial of pembrolizumab in patients with recurrent glioblastoma reveals predominance of immune-suppressive macrophages. Neuro Oncol. 2020;22(4):539–49.
Omuro A, et al. Nivolumab with or without ipilimumab in patients with recurrent glioblastoma: results from exploratory phase I cohorts of CheckMate 143. Neuro Oncol. 2018;20:674–86.
Reardon DA, et al. Effect of nivolumab vs bevacizumab in patients with recurrent glioblastoma. JAMA Oncol. 2020;6:1003.
Cloughesy TF, Mochizuki AY, Orpilla JR, et al. Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma. Nat Med. 2019;25:477–86. https://doi.org/10.1038/s41591-018-0337-7.
Fukuhara H, Ino Y, Todo T. Oncolytic virus therapy: a new era of cancer treatment at dawn. Cancer Sci. 2016;107:1373–9.
Gromeier M, Alexander L, Wimmer E. Internal ribosomal entry site substitution eliminates neurovirulence in intergeneric poliovirus recombinants. Proc Natl Acad Sci. 1996;93:2370–5.
Desjardins A, et al. Recurrent glioblastoma treated with recombinant poliovirus. N Engl J Med. 2018;379:150–61.
Chiocca EA, et al. Viral and other therapies for recurrent glioblastoma: is a 24-month durable response unusual? Neuro Oncol. 2018;21(1):14–25.
Todo T, et al. Oncolytic herpes simplex virus vector with enhanced MHC class I presentation and tumor cell killing. Proc Natl Acad Sci USA. 2001;98(11):6396-6401. https://doi.org/10.1073/pnas.101136398
Ino Y, Todo T. Clinical development of a third-generation oncolytic Hsv-1 (G47Δ) for malignant glioma. Gene Ther Regul. 2010;05:101–11.
Todo T, et al. Intratumoral oncolytic herpes virus G47∆ for residual or recurrent glioblastoma: a phase 2 trial. Nat Med. 2022;28:1630–9.
Todo T, et al. A phase I/II study of triple-mutated oncolytic herpes virus G47∆ in patients with progressive glioblastoma. Nat Commun. 2022;13:4119.
Chiocca EA, et al. A phase I open-label, dose-escalation, multi-institutional trial of injection with an E1B-attenuated adenovirus, ONYX-015, into the peritumoral region of recurrent malignant gliomas, in the adjuvant setting. Mol Ther. 2004;10:958–66.
Lang FF, et al. Phase I study of DNX-2401 (delta-24-RGD) oncolytic adenovirus: replication and immunotherapeutic effects in recurrent malignant glioma. J Clin Oncol. 2018;36:1419–27.
van Putten EHP, et al. Convection enhanced delivery of the oncolytic adenovirus delta24-RGD in patients with recurrent GBM: a phase I clinical trial including correlative studies. Clin Cancer Res. 2022;28:1572–85.
Samson A, et al. Intravenous delivery of oncolytic reovirus to brain tumor patients immunologically primes for subsequent checkpoint blockade. Sci Transl Med. 2018;10:eaam7577.
Wagner J, et al. CAR T cell therapy for solid tumors: bright future or dark reality? Mol Ther. 2020;28:2320–39.
Goff SL, et al. Pilot trial of adoptive transfer of chimeric antigen receptor-transduced T cells targeting EGFRvIII in patients with glioblastoma. J Immunother. 2019;42:126–35.
Maggs L, et al. CAR T cell-based immunotherapy for the treatment of glioblastoma. Front Neurosci. 2021;15:662064.
Brown CE, et al. Bioactivity and safety of IL13Rα2-redirected chimeric antigen receptor CD8+ T cells in patients with recurrent glioblastoma. Clin Cancer Res. 2015;21:4062–72.
Mineo JF, et al. Low HER2-expressing glioblastomas are more often secondary to anaplastic transformation of low-grade glioma. J Neuro Oncol. 2007;85:281–7.
Shen L , et al. The efficacy of third generation anti-HER2 chimeric antigen receptor T cells in combination with PD1 blockade against malignant glioblastoma cells. Oncol Rep. 2019;42(4):1549-1557. https://pubmed.ncbi.nlm.nih.gov/31524276/. Epub 2019 Aug 5.
Ahmed N, et al. HER2-specific chimeric antigen receptor-modified virus-specific T cells for progressive glioblastoma. JAMA Oncol. 2017;3:1094.
Pegram HJ, et al. Tumor-targeted T cells modified to secrete IL-12 eradicate systemic tumors without need for prior conditioning. Blood. 2012;119(18):4133–41.
Liu Y, et al. Armored inducible expression of IL-12 enhances antitumor activity of glypican-3-targeted chimeric antigen receptor-engineered T cells in hepatocellular carcinoma. J Immunol. 2019;203(1):198–207.
Ma X, et al. Interleukin-23 engineering improves CAR T cell function in solid tumors. Nat Biotechnol. 2020;38(4):448–59.
Agliardi G, et al. Intratumoral IL-12 delivery empowers CAR-T cell immunotherapy in a pre-clinical model of glioblastoma. Nat Commun. 2021;12(1):444.
Wang Z, Cao YJ. Adoptive cell therapy targeting neoantigens: a frontier for cancer research. Front Immunol. 2020;11:176.
Brudno JN, Kochenderfer JN. Toxicities of chimeric antigen receptor T cells: recognition and management. Blood. 2016;127(26):3321–30.
Tchou J, et al. Safety and efficacy of intratumoral injections of chimeric antigen receptor (CAR) T cells in metastatic breast cancer. Cancer Immunol Res. 2017;5(12):1152–61.
Priceman SJ, et al. Regional delivery of chimeric antigen receptor-engineered T cells effectively targets HER2(+) breast cancer metastasis to the brain. Clin Cancer Res. 2018;24(1):95–105.
Guercio M, et al. Inclusion of the inducible caspase 9 suicide gene in CAR construct increases safety of CAR.CD19 T cell therapy in B-cell malignancies. Front Immunol. 2021;12:755639.
Liu Y, et al. Inducible caspase-9 suicide gene under control of endogenous oct4 to safeguard mouse and human pluripotent stem cell therapy. Mol Ther. 2022;24:332–41.
Xu Y, et al. Closely related T-memory stem cells correlate with in vivo expansion of CAR.CD19-T cells and are preserved by IL-7 and IL-15. Blood. 2014;123(24):3750–9.
Lanitis E, et al. Optimized gene engineering of murine CAR-T cells reveals the beneficial effects of IL-15 coexpression. J Exp Med. 2020;218(2):e20192203.
Perna SK, et al. Interleukin 15 provides relief to CTLs from regulatory T cell-mediated inhibition: implications for adoptive T cell-based therapies for lymphoma. Clin Cancer Res. 2013;19(1):106–17.
Wang Y, et al. An IL-4/21 inverted cytokine receptor improving CAR-T cell potency in immunosuppressive solid-tumor microenvironment. Front Immunol. 2019;10:1691.
Weiss T, et al. Immunocytokines are a promising immunotherapeutic approach against glioblastoma. Sci Transl Med. 2020;12(564):eabb2311.
Offner S, et al. Induction of regular cytolytic T cell synapses by bispecific single-chain antibody constructs on MHC class I-negative tumor cells. Mol Immunol. 2006;43(6):763–71.
Choi BD, et al. Systemic administration of a bispecific antibody targeting EGFRvIII successfully treats intracerebral glioma. Proc Natl Acad Sci. 2013;110(1):270–5.
Brinkmann U, Kontermann RE. The making of bispecific antibodies. MAbs. 2017;9(2):182–212.
Spiess C, Zhai Q, Carter PJ. Alternative molecular formats and therapeutic applications for bispecific antibodies. Mol Immunol. 2015;67(2 Pt A):95–106.
Gedeon PC, et al. A rationally designed fully human EGFRvIII:CD3-targeted bispecific antibody redirects human T cells to treat patient-derived intracerebral malignant glioma. Clin Cancer Res. 2018;24(15):3611–31.
Rosenthal MA, et al. ATIM-49 (LTBK-01). AMG 596, a novel anti-EGFRVIII bispecific T cell engager (BITE®) molecule for the treatment of glioblastoma (GBM): planned interim analysis in recurrent GBM(RGBM). Neuro Oncol. 2019;21(Suppl_6):vi283.
van der Woude JC, et al. Phase I, double-blind, randomized, placebo-controlled, dose-escalation study of NI-0401 (a fully human anti-CD3 monoclonal antibody) in patients with moderate to severe active Crohn’s disease. Inflamm Bowel Dis. 2010;16(10):1708–16.
Su, R.W.F.F.G.M.G.K.L.R.R.D.Y.C.F.-C.J.S.K.T.K.L.K.J. Antibodies directed to the deletion mutants of epidermal growth factor receptor and uses thereof, in Google Patents, I. ABGENIX, editor. 2004.
Singh K, et al. For whom the T cells troll? Bispecific T-cell engagers in glioblastoma. J Immunother Cancer. 2021;9(11): e003679.
Bausart M, Préat V, Malfanti A. Immunotherapy for glioblastoma: the promise of combination strategies. J Exp Clin Cancer Res. 2022;41(1): s35.
Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39(1):1–10.
Heynckes S, et al. Crosslink between temozolomide and PD-L1 immune-checkpoint inhibition in glioblastoma multiforme. BMC Cancer. 2019;19(1):117.
Karachi A, et al. Modulation of temozolomide dose differentially affects T-cell response to immune checkpoint inhibition. Neuro Oncol. 2019;21(6):730–41.
Dai B, et al. Temozolomide combined with PD-1 antibody therapy for mouse orthotopic glioma model. Biochem Biophys Res Commun. 2018;501(4):871–6.
Lim M, et al. Phase III trial of chemoradiotherapy with temozolomide plus nivolumab or placebo for newly diagnosed glioblastoma with methylated MGMT promoter. Neuro Oncol. 2022;24(11):1935–49.
Omuro A, et al. Radiotherapy combined with nivolumab or temozolomide for newly diagnosed glioblastoma with unmethylated MGMT promoter: an international randomized phase III trial. Neuro Oncol. 2022;25(1):123–34.
Harris-Bookman S, et al. Expression of LAG-3 and efficacy of combination treatment with anti-LAG-3 and anti-PD-1 monoclonal antibodies in glioblastoma. Int J Cancer. 2018;143(12):3201–8.
Soubéran A, et al. Effects of VEGF blockade on the dynamics of the inflammatory landscape in glioblastoma-bearing mice. J Neuroinflamm. 2019;16(1):191.
Ravi M, et al. A review of glioblastoma immunotherapy. J Neuro Oncol. 2021;151:41–53.
Singh K, et al. Designing clinical trials for combination immunotherapy: a framework for glioblastoma. Clin Cancer Res. 2021;28(4):585–93.
Barrow Neurological, Institute., phase 0 clinical trial, including GBM. 2020. https://www.ivybraintumorcenter.org/phase-0-clinical-trials/why-phase-0-trials/. Accessed 17 Apr 2023.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for the preparation of this article.
Conflict of interest
JHS has an equity interest in Istari Oncology, which has licensed intellectual property from Duke related to the use of poliovirus and D2C7 in the treatment of glioblastoma. JHS is an inventor on patents related to the PEP-CMV DC vaccine with tetanus, as well as the poliovirus vaccine and D2C7 in the treatment of glioblastoma. JHS has an equity interest in Annias Immunotherapeutics, which has licensed intellectual property from Duke related to the use of the pepCMV vaccine in the treatment of glioblastoma. MK reports research funding from the institutions: BMS, AbbVie, Daiichi Sankyo, BioNTech, Celldex, Astellas, and CNS Pharmaceuticals and honoraria from JAX lab for genomic research, Johnson and Johnson, Voyager Therapeutics, and George Clinical. SEZ, EM, KS, AM, MS, MAS, KH, SS, and WL have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
Not applicable.
Code availability
Not applicable.
Authors’ contributions
MK and WL conceptualized and designed the work, SEZ wrote the original draft and revised it, MK, EM, and KS edited and improved the first version of the manuscript, and AM, MS, MAS, KH, SS, WL, JHS, and MK subsequently revised the manuscript. SEZ and AM developed the figures, which were revised with input from all authors. MK supervised and proposed methodology, all authors contributed to the article and approved the submitted version.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zaidi, S.E., Moelker, E., Singh, K. et al. Novel Immunotherapeutic Approaches for the Treatment of Glioblastoma. BioDrugs 37, 489–503 (2023). https://doi.org/10.1007/s40259-023-00598-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40259-023-00598-2