
Abstract
Purpose of Review
Cancer survivors represent the largest cohort of patients seeking specialty rehabilitative care. They carry a heavy burden of cardiopulmonary complications, but in the past have been excluded from many exercise studies, owing to perceived increased risk.
Recent Findings
Cardiopulmonary dysfunction in cancer survivors is a complex phenomenon that goes beyond lung volume loss, dilated cardiomyopathy, or accelerated coronary artery disease. All training modalities have been explored in cancer survivors before, during, and after active treatment, proving effective against aerobic capacity decline due to cancer.
Summary
We summarize common adverse treatment effects, particularly due to newer chemotherapeutic agents, and provide examples of exercise interventions, designed to mitigate cardiopulmonary decline in a cancer survivor. Carefully designed routines can be safely applied in most situations, where aerobic reconditioning is needed. Lastly, physiatrists may be the most effective advocates in overcoming systemic barriers, such as insurance regulations, that limit access to cardiopulmonary rehabilitation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The most common cause of death in the USA is cardiovascular disease (CVD) [1]. Cancer and CVD share risk factors, such as age and smoking exposure; thus, even without additional treatment-related morbidity, a cancer survivor is likely to have some form of underlying cardiopulmonary dysfunction (CPD). Owing to treatment advances, the overall 5-year survival for cancer survivors has improved from 49% in 1975–1977 to 69% in 2006–2012 and death rate decreased by 25% since 1991 [2]. Thus, the cancer survivor population, which already outnumbers other recipients of specialty rehabilitation services such as patients with stroke or traumatic brain injury, will continue to grow [1, 3]. The likelihood that a given cancer survivor has a CPD depends on several factors, including the treatment era, age at diagnosis, treatment modality, and the presence of pre-morbid conditions, such as hypertension (HTN), dyslipidemia (DL), abnormal glucose metabolism (AGM), or obesity. Classic cardiotoxic agents, such as anthracyclines, remain widely used due to their effectiveness, thus making it very likely that a cancer rehabilitation physiatrist will treat a patient with anthracycline cardiomyopathy. Typical course begins with the asymptomatic decline in ejection fraction, eventually manifesting as overt heart failure with fatal cardiac event hazard ratio of 3.46 and 50% mortality rate at 2 years [4]. The survivors of childhood cancers likely represent the cohort with the largest CPD burden. These patients suffer from cardiac mortality equivalent to that of the population 20 to 30 years older [5]. Childhood Hodgkin lymphoma (HL) survivors are twice as likely to have CPD as population controls (89% prevalence) and have at least one severe condition by 50 years of age, despite having the same prevalence of HTN and DL [6]. Childhood recipients of hematopoetic stem cell transplants (HSCT) carry higher burden of CPD than other cancer survivors, with up to 19.6% having a severe cardiovascular and 16.1% having a severe pulmonary disorder, along with higher prevalence of HTN, DL, AGM, and obesity [7]. Similarly, all children treated with high-dose carmustine in the 1980s and early 1990s developed upper zone pulmonary fibrosis with over 50% mortality [8]. In contrast, recently developed chemotherapeutics, e.g., small molecule tyrosine kinase inhibitors (TKIs, or “-inibs”), appear to have a much lower incidence of pulmonary fibrosis (around 1–4%), though also carry a 50–60% mortality rate, similar to the classic agents such as busulfan and nitrosureas [9]. It is important to remember that the global CPD in a cancer patient is more than the sum of individual treatment morbidities and that appropriate rehabilitative strategies along with lifestyle changes, such as weight control and smoking cessation, can mitigate some of the decline.
Overview of the Cardiopulmonary Function Decline Along the Survivorship Continuum
Direct echocardiographic measure of the left ventricular ejection fraction (LVEF) has long been accepted as a proxy of cardiac function and a marker of morbidity; however, it does not adequately describe one’s work reserve. Aerobic capacity, or the ability to make adenosine triphosphate (ATP) and use it for muscular work, is the underpinning of any sustained human activity. It can be directly measured via a cardiopulmonary exercise test (CPET), a tool that has been successfully employed in cancer survivors. Peak oxygen consumption (VO2peak) has been shown to decline with more treatment cycles [10, 11], which is not surprising, given that commonly used agents, such as cyclophosphamide, have been shown to decrease the amount of ATP generated [12]. However, at least one investigation suggests that the decline in VO2peak could be seen even before exposure to chemotherapy, and that despite having normal LVEF, up to one third of breast cancer patients have VO2peak below the independent living threshold [13]. One possible explanation for that observation could be the Warburg effect, the discovery that yielded the 1924 Nobel Prize in Medicine. Even when oxygen is available, cancer drives a shift toward a less efficient glycolytic pathway that increases the availability of lactate to the tumor cells and decreases a body’s ability to utilize oxygen [14]. One exciting therapeutic application of this phenomenon is the potential that aerobic conditioning which improves a person’s ability to clear lactate can have direct effect on cancer growth and spread.
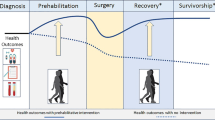
Detailed discussion of every possible reason behind CPD in a cancer survivor is beyond the scope of this text. In the broadest sense, cardiopulmonary capacity is the ability to effectively use oxygen for muscular contractions expressed as observable work. We believe that any decline in a survivor’s ability to move or take part in the activities of daily living is a manifestation of impaired oxygen utilization, unless the loss of function can be fully explained by other issues, such as uncontrolled pain, loss of limb, or psychologic factors. There are several events that have to take place so that an inhaled molecule of oxygen contributes to an externally apparent muscular effort. Figure 1 summarizes those steps, factors contributing to decreased aerobic capacity across the entire cancer care continuum, and lists corresponding corrective strategies. It is important to remember that there is an opportunity for effective rehabilitative intervention at every stage and that often there are systemic barriers, such as lack of insurance instruments that will demand creative solutions for a specific care scenario.

Cycle of abnormal oxygen utilization in a cancer patient. It is a multi-step process that converts atmospheric oxygen into externally apparent work (mobility and activities of daily living). Gray boxes represent discrete stages with possible morbidities. Green boxes list corrective interventions that are within the scope of physiatric practice. Adapted from Bartels MN, Syrkin G: Cardiovascular Complications of Cancer and Their Treatment. In: Stubblefield, MD, editor. Cancer Rehabilitation, Principles and Practice, Second Edition. Demos Medical, 2018 (in print) [15]
Prehabilitation
It is well accepted that oxidative stress plays a large role in morbidity related to cancer treatment. Free radical formation happens as the result of exposure to radiotherapy and medications, most notably anthracyclines, such as doxorubicin, a classic cardiotoxic agent. While there has been increased interest in using the anti-oxidant effects of aerobic exercise to prevent treatment-related toxicity [16], the first studies on this subject are almost four decades old [17]. Murine data demonstrate beneficial effects on micro- and macroscopic levels, showing improved survival after the anthracycline administration. Unfortunately, at this time, there are no insurance regulations that would make it possible for patients to undergo supervised structured aerobic conditioning in preparation to cardiotoxic cancer treatment. One possible solution to this problem is utilizing existing principles of generalized aerobic conditioning, such as progressive aerobic loads with patient-specific training heart rate zones and providing patients with easily adopted self-directed exercise routine.
High-intensity training (HIIT) has been successfully employed in a variety of CPD scenarios. Owing to the short duration of intervention, HIIT is an appealing solution for situations when there is only a limited time window for rehabilitative intervention. As little as 7 days of intense training prior to planned pulmonary resection have been shown to reduce the incidence of immediate complications and the length of stay [18, 19] while longer programs helped mitigate the decline in VO2peak [20].
Exercise During Active Treatment and Hospitalization
Prevention of Hospital-Acquired Immobility
Risks of low mobility during hospital admission have been recognized in peer-reviewed literature since the 1940s [21] and have been associated with readmission, regardless of the presenting diagnosis [22,23,24]. Early mobilization has been shown to benefit even the critically ill [25]. This has particular relevance for cancer patients, especially those undergoing surgical procedures. Measures that promote early mobility, such as regional anesthesia, early enteral feeding, and careful fluid balance, have shown benefit in such high morbidity procedures as esophagectomies and lung lobectomies [26, 27]. Mobilizing patients out of bed to chair on postoperative day 1 in the thoracic unit at Memorial Sloan Kettering Cancer Center reduced the incidence of pulmonary complications from 14.4 to 2.9%, rate of ICU admission from 5.1 to 4.2%, and length of hospital stay from 9.3 to 8.2 days [28]. A cancer rehabilitation physiatrist serving as an acute care consultant can help prevent unnecessary immobilization by prescribing safe and effective exercise interventions in the immediate postoperative period.
Exercise During Active Treatment
Exercise has also been shown to be safe and beneficial even in such taxing circumstances as high-dose chemotherapy and HSCT in the management hematologic malignancies, where acute and 1-year mortality reaches 2.8–5.7% and 21% respectively [29, 30]. Approaches ranging from supine in-bed bicycling to multimodal resistance and endurance routines have been shown to positively affect cardiopulmonary fitness and reduce adverse effects of treatment [29, 31,32,33,34,35,36,37,38]. All studies utilized a baseline CPET to determine target heart rate and continuous pulse monitoring to ensure exercise efficacy. One of the more elegant investigations demonstrated that a 30-min daily intervention consisting of in-bed cycling intervals (1 min cycling at 50% cardiac reserve, followed by 1 min rest) can decrease length of stay, duration of neutropenia, thrombocytopenia, reduce diarrhea, pain, and limit the decline of physical function [31]. Newer studies employ psychologic counseling and relaxation for a more comprehensive approach [37, 38]. Similarly, exercise interventions have shown benefit in other diagnoses including lung, breast, prostate, and gastrointestinal cancers [39,40,41,42,43,44,45,46]. As with inpatients undergoing myeloablation, even simple exercise interventions, such as walking three times per week for 30 min at 50% of predicted cardiac reserve, significantly improved oxygen uptake and functional performance [43].
As in the prehabilitation period, properly designed and carefully administered high-intensity interval training (HIIT) is a promising training modality for cancer patients in active treatment, who often have low exercise tolerance. Due to the short session duration, work can be completed prior to the onset of debilitating fatigue. HIIT has been shown to be safe and effective in a variety of patient populations, including those with heart failure and recent cardiac surgery [47,48,49,50,51]. Repeated sit-to-stands (STS) have been validated as both a measure of frailty and a predictor of mortality in a variety of patient populations [52,53,54,55]. In our experience, STS can be easily administered to a hospitalized patient as the primary work load. Exercise safety is assured as the seating surface can be adjusted for height (controlling the muscular effort) and is directly behind the patient in case of lost balance. Finger pulse oximeter allows monitoring of heart rate in real time. For patients with congestive heart failure, exercise periods of 30 s and 60 s rest are recommended [50].
Role of Physiatry in the Post-acute Care
For those patients who are unable to function in the community as the result of their disease and its treatment, the importance of appropriate post-acute care cannot be overstated. Achieving functional status can often mean the difference between curative treatment and palliative care only. Inpatient and outpatient cardiopulmonary rehabilitation must be pursued for cancer patient who develops new heart failure and angina and suffers a myocardial infarction (MI), or significant lung volume loss. In our experience, it is often the consultant physiatrist who can most effectively advocate for the patients and overturn denials of rehabilitative care by insurance companies. As in general population, the primary barrier to structured cardiopulmonary rehabilitation is access and all members of the patient care team must be educated to ensure timely referrals.
Safety Considerations During Active Cancer Treatment
Acute coronary syndrome (ACS) remains an important cause of early chemotherapy-related cardiac disease. Classic agents, such as paclitaxel, cisplatin, and 5-fluorouracil, cause ACS in about 1% of chemotherapy recipients [56]. Some groups, such as African-Americans or patients with pre-existing cardiac risk factors, may be at a higher risk. Newer agents, such bevacizumab (Avastin), have been associated with a more than fourfold increase in cardiac ischemic events, including 0.6% incidence of MI [56, 57]. More alarmingly, up to one third of patients receiving anti-angiogenic tyrosine kinase inhibitors, such as sunitinib, sorafenib, and cediranib, have been reported to have an elevation in cardiac enzymes, EKG changes, or ACS symptoms [58]. Furthermore, uncontrolled hypertension due to high volumes of intravenous fluids, associated with classic chemotherapy agents, or renovascular dysregulation, caused by the newer medications, such as bevacizumab or TKIs, can result in ACS or acute congestive heart failure (CHF) [56, 58, 59]. Grade 3 HTN (systolic blood pressure > 180 mmHg, or diastolic pressure > 110 mmHg) can happen as early as the first 1–3 days, which may be found in up to 92% of patients with renal cell carcinoma receiving a combination of sunitinib and bevacizumab, or in 1 of every 17 patients receiving a single TKI [58, 60].
Table 1 summarizes frequently encountered cardiopulmonary toxicities of neoplastic agents.
Additionally, there may be other patient-specific barriers to exercise, such as impaired venous return, increased limb weight due to edema, pain, fever, anemia, and skeletal pain from metastatic bone lesions. Many of these factors can be effectively and safely addressed by appropriate national guidelines, such as venous thrombosis prophylaxis and timely mobilization [75, 76], while other may be helped by the modifying exercise program or employing adaptive equipment, orthoses, mobility aides, compression garments, or other tools of rehabilitation trade.
Table 2 summarizes various exercise exclusion criteria used in patients undergoing active cancer treatment.
Exercise After Active Treatment
Similarly, exercise in the post-treatment period showed numerous benefits for major cancer diagnoses [45, 77,78,79,80,81,82,83,84,85]. Typical resistance regimen is exemplified by a protocol outlined by Segal et al.: warm-up, followed by 2 sets of 8–12 repetitions of nine exercises targeting major muscle groups—leg extension, calf raises, leg curl, chest press, latissimus pulldown, overhead press, triceps extension, biceps curls, and modified curl-ups, performed at 60–70% of 1-repetition maximum 3 times weekly for 12 weeks [82]. Aerobic programs typically utilize a brief warm-up, followed by 30 min of cycling, walking, or jogging at 65–80% of cardiac reserve [83]. Even high-impact aerobic activity (soccer) in prostate cancer survivors with known asymptomatic bony metastases showed improved lean body mass and VO2max without observed pathologic fractures [86]. Simple, easily accessible eccentric exercise, such as descending stairs, has proven effective in decreasing heart rate and systolic blood pressure and increasing bone mineral density in healthy obese women [87], though it is yet to be validated in cancer survivors. Most recently, HIIT has been shown to reduce CVD risk factors in testicular cancer survivors by as much as 20% [88].
Exercise Adherence
Continued adoption of physical activity is a challenge in both general US population and cancer survivors, particularly those with lower baseline function [89]. Various approaches, such as group therapy [90,91,92,93,94], telephone follow-up [44], and team sport activities [86, 95], have proven to be helpful.
Early Recognition of Late Treatment Toxicity and Exercise Safety
Physiatrist taking care of a patient with remote history of cancer may be the person best positioned to detect early symptoms of CPD. Assessing treatment-related cardiopulmonary risk factors and communicating with cancer care providers can greatly facilitate timely diagnosis and safe rehabilitation. Another important role for a cancer rehabilitation physiatrist is ensuring exercise safety. When a survivor plans to engage in an exercise program that may include a high cardiac workload, physiatrist should elicit important historical risk factors, such as family history of sudden cardiac death, high left chest radiation exposures, anthracycline doses, or a combination of the two modalities. One trial (HF-ACTION) demonstrated higher all-cause mortality at 35 months (84 vs 66%) in the cancer survivors with heart failure, if they could not tolerate > 90 min of exercise per week, likely indicating that special attention is needed to guide aerobic exercise in such cases [96]. Indeed, a more recent report showed that women with heart failure due to the effects of breast cancer treatment demonstrate similar gains and same dropout rates as controls with ischemic cardiomyopathy [97].
Radiation therapy is a major contributor to the development or progression of coronary artery disease. While newer treatment modalities, such as breath holding and prone positioning, greatly reduce or eliminate cardiac irradiation, patients treated prior to the last decade are likely to have received more than the recommended maximum of 30–35 Gy to the cardiac region. The risk of events, such as MI, cardiac revascularization, or death from ischemic heart disease, increases by 7.4% for every 1 Gy delivered to the heart [98]. Similarly, radiation-induced valvular disease (RVD) is becoming less frequent—when calculated dose to valve is < 30 Gy, the increase in valvular disease risk is only about 1.4% at 30 years [99]. However, any modifiable risk factors (smoking, DL) must be managed as more than half of the patients with RVD will progress [99].
Stretching exercise, one of restorative therapy mainstays, has already been shown to benefit head and neck cancer patients before and during radiotherapy [100,101,102]. One mechanistic explanation for this is the stretch-induced production of nitric oxide (NO). It acts both as a free radical scavenger, protecting muscle stem cells [103], and as a signaling molecule, stimulating muscle repair [104]. Thus, there is good reason to counsel patient to engage in both general stretching routines and regular aerobic exercise to promote NO elaboration by cardiac muscle and surrounding tissues that happens in response to increased filling with activity.
Advanced Management of the End-Stage Cardiopulmonary Dysfunction
Ventricular Assist Devices in Cancer Patients
Physiatrist taking care of cancer survivor with cardiac disease can be an effective advocate in pursuit of advanced CPD management—ventricular assist devices (VADs) [105, 106]. Recent report from the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) suggests that patients with cancer treatment-related heart failure represent about 2% of VAD recipients. They are more likely to be younger and female and have fewer comorbidities, but higher incidence of right ventricular failure [107, 108]. Survival appears to be similar to that of VAD recipients without history of cancer (73, 63, and 47% respectively at 1, 2, and 3 years), although cancer patients often require more additional cardiac surgeries, such as tricuspid repair (approximately one-half vs one-third in other etiologies), and those with more severe restrictive cardiomyopathy may fare worse [106, 109]. Interestingly, in the cancer cohort recovery of cardiac function allowing explanation of the VAD has been reported in 4.1%, up to 21% of them show improvement of LVEF to greater than 40% [110].
Since VADs have been approved as a bridge to transplantation, two major scenarios have been described in oncologic population. There have been 32 new cancer diagnoses in VAD recipients, either during pre-transplant workup or while awaiting an organ, with at least 12 patients being able to undergo cancer treatment owing to VAD support [111,112,113,114]. Additionally, there are three cases of VADs implanted specifically to facilitate cancer treatment in patients with active disease [113, 115]. Furthermore, in several of the cases, VADs facilitated home discharge, which can be of great importance at the end-of-life [114, 116,117,118].
Heart and Lung Transplantation in Cancer Survivors
As with VAD use, physiatrist can serve as the interface between the oncology and solid organ transplant service for patients who may need heart and lung transplantation. Current guidelines no longer recommend the arbitrary 5-year waiting period following completion of cancer treatment. Indeed, there is at least one case report of a successful double-lung transplant for acute bleomycin toxicity 5 weeks following testicular cancer treatment [119]. The decision regarding the feasibility and timing of the transplantation in a cancer survivor should depend on the tumor type, treatment response, recurrence, and metastatic risk [120]. According to United Network for Organ Sharing (UNOS), cancer patients represent about 0.8% of those listed for an orthotopic heart transplant (OHT) and have comparable outcomes following the procedure without significant increase in secondary malignancies [105, 106]. Despite having more infections (22 vs 14%), fewer cancer patients had rejection at 1 year (28 vs 38%) and survival at 1, 3, and 5 years was similar to OHT recipients without oncologic history—86, 79, and 71% respectively [121].
Lifestyle Changes
Physiatrists often have close and lasting therapeutic relationships with their patients. In our opinion, that privilege makes it possible to successfully tackle such difficult problems as smoking cessation, weight control, and dietary changes. Since cancer survivors are prone to accelerated atherosclerosis due to effects of hormonal deprivation, radiation, and other forms of oxidative stress, risk-free interventions, such as plant-based diets, can provide same amount of CVD risk reduction as intense exercise and reduce risk of cancer by 8–15% [122,123,124]. Similarly, a physiatrist can also be more effective in helping patients quit smoking, citing immediate benefits and involvement during a pulmonary rehabilitation program while emphasizing benefits such as reduced pain and faster recovery following lung cancer surgery [125].
Conclusion
As physicians tasked with maintaining a person’s function across time and different settings, physiatrists are uniquely positioned to supplement the efforts of the oncology team and help patients tolerate some of the most morbid treatments. Physiatrists’ focus on interdisciplinary care and ability to navigate insurance barriers and social issues can help a cancer patient at any stage of the cancer journey, from prehabilitation to hospice. By taking into account co-existing diseases, anticipating adverse treatment effects, and utilizing adaptive equipment, physiatrists can help prepare patients for taxing cancer care, avoid unnecessary immobilization during hospitalization, guide appropriate post-acute care services, and provide sustainable restorative care until the very end. Regardless of the diagnosis or treatment phase, cardiopulmonary fitness of a cancer survivor can be improved through exercise [126], even to the point of being able to complete a full marathon during chemotherapy [127]. Additionally, by promoting healthy lifestyle changes, such as smoking cessation, weight control, and dietary interventions, physiatrists can literally alter the course of morbidity and mortality in a cancer survivor with cardiopulmonary dysfunction.
References
National Heart L, and Blood Disease Institute. Disease Statistics: US Department of Health and Human Services; [Available from: https://www.nhlbi.nih.gov/about/documents/factbook/2012/chapter4.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30.
de Moor JS, Mariotto AB, Parry C, Alfano CM, Padgett L, Kent EE, et al. Cancer survivors in the United States: prevalence across the survivorship trajectory and implications for care. Cancer Epidemiol Biomark Prev. 2013;22(4):561–70.
McGowan JV, Chung R, Maulik A, Piotrowska I, Walker JM, Yellon DM. Anthracycline chemotherapy and cardiotoxicity. Cardiovasc Drugs Ther. 2017;31(1):63–75.
Armstrong GT, Kawashima T, Leisenring W, Stratton K, Stovall M, Hudson MM, et al. Aging and risk of severe, disabling, life-threatening, and fatal events in the childhood cancer survivor study. J Clin Oncol. 2014;32(12):1218–27.
Bhakta N, Liu Q, Yeo F, Baassiri M, Ehrhardt MJ, Srivastava DK, et al. Cumulative burden of cardiovascular morbidity in paediatric, adolescent, and young adult survivors of Hodgkin’s lymphoma: an analysis from the St Jude Lifetime Cohort Study. Lancet Oncol. 2016;17(9):1325–34.
Eissa HM, Lu L, Baassiri M, Bhakta N, Ehrhardt MJ, Triplett BM, et al. Chronic disease burden and frailty in survivors of childhood HSCT: a report from the St. Jude Lifetime Cohort Study. Blood Adv. 2017;1(24):2243–6.
Lohani S, O'Driscoll BR, Woodcock AA. 25-year study of lung fibrosis following carmustine therapy for brain tumor in childhood. Chest. 2004;126(3):1007.
Shah RR. Tyrosine kinase inhibitor-induced interstitial lung disease: clinical features, diagnostic challenges, and therapeutic dilemmas. Drug Saf. 2016;39(11):1073–91.
Kim S, Song IC, Jee S. Cardiopulmonary exercise test in leukemia patients after chemotherapy: a feasibility study. Ann Rehabil Med. 2017;41(3):456–64.
Shallwani SM, Simmonds MJ, Kasymjanova G, Spahija J. Quality of life, symptom status and physical performance in patients with advanced non-small cell lung cancer undergoing chemotherapy: an exploratory analysis of secondary data. Lung Cancer. 2016;99:69–75.
Crouch ML, Knowels G, Stuppard R, Ericson NG, Bielas JH, Marcinek DJ, et al. Cyclophosphamide leads to persistent deficits in physical performance and in vivo mitochondria function in a mouse model of chemotherapy late effects. PLoS One. 2017;12(7):e0181086.
Jones LW, Courneya KS, Mackey JR, Muss HB, Pituskin EN, Scott JM, et al. Cardiopulmonary function and age-related decline across the breast cancer survivorship continuum. J Clin Oncol. 2012;30(20):2530–7.
San-Millán I, Brooks GA. Reexamining cancer metabolism: lactate production for carcinogenesis could be the purpose and explanation of the Warburg Effect. Carcinogenesis. 2017;38(2):119–33.
Bartels MN, Syrkin G. Cardiovascular complication of Cancer and their treatment. In: Stubblefield MD, editor. Cancer rehabilitation, principles and practice, Second Edition (in print). 2nd ed. New York: Demos Medical; 2018.
Marques-Aleixo I, Santos-Alves E, Mariani D, Rizo-Roca D, Padrão AI, Rocha-Rodrigues S, et al. Physical exercise prior and during treatment reduces sub-chronic doxorubicin-induced mitochondrial toxicity and oxidative stress. Mitochondrion. 2015;20:22–33.
Combs AB, Hudman SL, Bonner HW. Effect of exercise stress upon the acute toxicity of adriamycin in mice. Res Commun Chem Pathol Pharmacol. 1979;23(2):395–8.
Lai Y, Huang J, Yang M, Su J, Liu J, Che G. Seven-day intensive preoperative rehabilitation for elderly patients with lung cancer: a randomized controlled trial. J Surg Res. 2017;209:30–6.
Licker M, Karenovics W, Diaper J, Frésard I, Triponez F, Ellenberger C, et al. Short-term preoperative high-intensity interval training in patients awaiting lung cancer surgery: a randomized controlled trial. J Thorac Oncol. 2017;12(2):323–33.
Stefanelli F, Meoli I, Cobuccio R, Curcio C, Amore D, Casazza D, et al. High-intensity training and cardiopulmonary exercise testing in patients with chronic obstructive pulmonary disease and non-small-cell lung cancer undergoing lobectomy. Eur J Cardiothorac Surg. 2013;44(4):e260–5.
Asher RA. The dangers of going to bed. Br Med J. 1947;2(4536):967.
Krumholz HM. Post-hospital syndrome—an acquired, transient condition of generalized risk. N Engl J Med. 2013;368(2):100–2.
Hoyer EH, Needham DM, Miller J, Deutschendorf A, Friedman M, Brotman DJ. Functional status impairment is associated with unplanned readmissions. Arch Phys Med Rehabil. 2013;94(10):1951–8.
Hoyer EH, Needham DM, Atanelov L, Knox B, Friedman M, Brotman DJ. Association of impaired functional status at hospital discharge and subsequent rehospitalization. J Hosp Med. 2014;9(5):277–82.
Hashem MD, Parker AM, Needham DM. Early mobilization and rehabilitation of patients who are critically ill. Chest. 2016;150(3):722–31.
Cao S, Zhao G, Cui J, Dong Q, Qi S, Xin Y, et al. Fast-track rehabilitation program and conventional care after esophagectomy: a retrospective controlled cohort study. Support Care Cancer. 2013;21(3):707–14.
Scarci M, Solli P, Bedetti B. Enhanced recovery pathway for thoracic surgery in the UK. J Thorac Dis. 2016;8(Suppl 1):S78–83.
Syrkin G. Evidence Base for Exercise Interventions in Cancer Rehabilitation. 2nd Annual MSKCC Cancer Rehabilitation Symposium 2014.
Baumann FT, Zimmer P, Finkenberg K, Hallek M, Bloch W, Elter T. Influence of endurance exercise on the risk of pneumonia and fever in leukemia and lymphoma patients undergoing high dose chemotherapy. A pilot study. J Sports Sci Med. 2012;11(4):638–42.
Modi D, Deol A, Kim S, Ayash L, Alavi A, Ventimiglia M, et al. Age does not adversely influence outcomes among patients older than 60 years who undergo allogeneic hematopoietic stem cell transplant for AML and myelodysplastic syndrome. Bone Marrow Transplant. 2017;52:1530–6.
Dimeo F, Fetscher S, Lange W, Mertelsmann R, Keul J. Effects of aerobic exercise on the physical performance and incidence of treatment-related complications after high-dose chemotherapy. Blood. 1997;90(9):3390–4.
Dimeo FC, Stieglitz RD, Novelli-Fischer U, Fetscher S, Keul J. Effects of physical activity on the fatigue and psychologic status of cancer patients during chemotherapy. Cancer. 1999;85(10):2273–7.
Dimeo F, Schwartz S, Fietz T, Wanjura T, Böning D, Thiel E. Effects of endurance training on the physical performance of patients with hematological malignancies during chemotherapy. Support Care Cancer. 2003;11(10):623–8.
Baumann FT, Kraut L, Schüle K, Bloch W, Fauser AA. A controlled randomized study examining the effects of exercise therapy on patients undergoing haematopoietic stem cell transplantation. Bone Marrow Transplant. 2010;45(2):355–62.
Baumann FT, Zopf EM, Nykamp E, Kraut L, Schüle K, Elter T, et al. Physical activity for patients undergoing an allogeneic hematopoietic stem cell transplantation: benefits of a moderate exercise intervention. Eur J Haematol. 2011;87(2):148–56.
Streckmann F, Kneis S, Leifert JA, Baumann FT, Kleber M, Ihorst G, et al. Exercise program improves therapy-related side-effects and quality of life in lymphoma patients undergoing therapy. Ann Oncol. 2014;25(2):493–9.
Jarden M, Baadsgaard MT, Hovgaard DJ, Boesen E, Adamsen L. A randomized trial on the effect of a multimodal intervention on physical capacity, functional performance and quality of life in adult patients undergoing allogeneic SCT. Bone Marrow Transplant. 2009;43(9):725–37.
Oechsle K, Aslan Z, Suesse Y, Jensen W, Bokemeyer C, de Wit M. Multimodal exercise training during myeloablative chemotherapy: a prospective randomized pilot trial. Support Care Cancer. 2014;22(1):63–9.
Quist M, Rørth M, Langer S, Jones LW, Laursen JH, Pappot H, et al. Safety and feasibility of a combined exercise intervention for inoperable lung cancer patients undergoing chemotherapy: a pilot study. Lung Cancer. 2012;75(2):203–8.
Segal R, Evans W, Johnson D, Smith J, Colletta S, Gayton J, et al. Structured exercise improves physical functioning in women with stages I and II breast cancer: results of a randomized controlled trial. J Clin Oncol. 2001;19(3):657–65.
Courneya KS, McKenzie DC, Mackey JR, Gelmon K, Friedenreich CM, Yasui Y, et al. Effects of exercise dose and type during breast cancer chemotherapy: multicenter randomized trial. J Natl Cancer Inst. 2013;105(23):1821–32.
Courneya KS, Segal RJ, McKenzie DC, Dong H, Gelmon K, Friedenreich CM, et al. Effects of exercise during adjuvant chemotherapy on breast cancer outcomes. Med Sci Sports Exerc. 2014;46(9):1744–51.
Vincent F, Labourey JL, Leobon S, Antonini MT, Lavau-Denes S, Tubiana-Mathieu N. Effects of a home-based walking training program on cardiorespiratory fitness in breast cancer patients receiving adjuvant chemotherapy: a pilot study. Eur J Phys Rehabil Med. 2013;49(3):319–29.
Cornette T, Vincent F, Mandigout S, Antonini MT, Leobon S, Labrunie A, et al. Effects of home-based exercise training on VO2 in breast cancer patients under adjuvant or neoadjuvant chemotherapy (SAPA): a randomized controlled trial. Eur J Phys Rehabil Med. 2016;52(2):223–32.
Grabenbauer A, Grabenbauer AJ, Lengenfelder R, Grabenbauer GG, Distel LV. Feasibility of a 12-month-exercise intervention during and after radiation and chemotherapy in cancer patients: impact on quality of life, peak oxygen consumption, and body composition. Radiat Oncol. 2016;11:42.
Segal RJ, Reid RD, Courneya KS, Sigal RJ, Kenny GP, Prud'Homme DG, et al. Randomized controlled trial of resistance or aerobic exercise in men receiving radiation therapy for prostate cancer. J Clin Oncol. 2009;27(3):344–51.
Meyer K, Lehmann M, Sünder G, Keul J, Weidemann H. Interval versus continuous exercise training after coronary bypass surgery: a comparison of training-induced acute reactions with respect to the effectiveness of the exercise methods. Clin Cardiol. 1990;13(12):851–61.
Meyer K, Foster C, Georgakopoulos N, Hajric R, Westbrook S, Ellestad A, et al. Comparison of left ventricular function during interval versus steady-state exercise training in patients with chronic congestive heart failure. Am J Cardiol. 1998;82(11):1382–7.
Foster C, Meyer K, Georgakopoulos N, Ellestad AJ, Fitzgerald DJ, Tilman K, et al. Left ventricular function during interval and steady state exercise. Med Sci Sports Exerc. 1999;31(8):1157–62.
Meyer K, Foster C. Non-traditional exercise training for patients with cardiovascular disease. Am J Med Sport. 2004;2:13.
Volterrani M, Iellamo F. Cardiac rehabilitation in patients with heart failure: new perspectives in exercise training. Card Fail Rev. 2016;2(1):63–8.
Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport. 1999;70(2):113–9.
Jones SE, Kon SS, Canavan JL, Patel MS, Clark AL, Nolan CM, et al. The five-repetition sit-to-stand test as a functional outcome measure in COPD. Thorax. 2013;68(11):1015–20.
De Buyser SL, Petrovic M, Taes YE, Toye KR, Kaufman JM, Goemaere S. Physical function measurements predict mortality in ambulatory older men. Eur J Clin Investig. 2013;43(4):379–86.
Puhan MA, Siebeling L, Zoller M, Muggensturm P, ter Riet G. Simple functional performance tests and mortality in COPD. Eur Respir J. 2013;42(4):956–63.
Di Lisi D, Madonna R, Zito C, Bronte E, Badalamenti G, Parrella P, et al. Anticancer therapy-induced vascular toxicity: VEGF inhibition and beyond. Int J Cardiol. 2017;227:11–7.
Totzeck M, Mincu RI, Rassaf T. Cardiovascular adverse events in patients with cancer treated with bevacizumab: a meta-analysis of more than 20 000 patients. J Am Heart Assoc. 2017;6(8):e006278.
Kruzliak P, Novák J, Novák M. Vascular endothelial growth factor inhibitor-induced hypertension: from pathophysiology to prevention and treatment based on long-acting nitric oxide donors. Am J Hypertens. 2014;27(1):3–13.
Arora N, Gupta A, Singh PP. Biological agents in gastrointestinal cancers: adverse effects and their management. J Gastrointest Oncol. 2017;8(3):485–98.
Abdel-Qadir H, Ethier JL, Lee DS, Thavendiranathan P, Amir E. Cardiovascular toxicity of angiogenesis inhibitors in treatment of malignancy: a systematic review and meta-analysis. Cancer Treat Rev. 2017;53:120–7.
Faruque LI, Lin M, Battistella M, Wiebe N, Reiman T, Hemmelgarn B, et al. Systematic review of the risk of adverse outcomes associated with vascular endothelial growth factor inhibitors for the treatment of cancer. PLoS One. 2014;9(7):e101145.
Yeh ET, Bickford CL. Cardiovascular complications of cancer therapy: incidence, pathogenesis, diagnosis, and management. J Am Coll Cardiol. 2009;53(24):2231–47.
Kroschinsky F, Stölzel F, von Bonin S, Beutel G, Kochanek M, Kiehl M, et al. New drugs, new toxicities: severe side effects of modern targeted and immunotherapy of cancer and their management. Crit Care. 2017;21(1):89.
Bendtsen MAF, Grimm D, Bauer J, Wehland M, Wise P, Magnusson NE, et al. Hypertension caused by lenvatinib and everolimus in the treatment of metastatic renal cell carcinoma. Int J Mol Sci. 2017;18(8):1736.
Garipagaoglu M, Munley MT, Hollis D, Poulson JM, Bentel GC, Sibley G, et al. The effect of patient-specific factors on radiation-induced regional lung injury. Int J Radiat Oncol Biol Phys. 1999;45(2):331–8.
Tomlinson J, Tighe M, Johnson S, Stone R, Nicholson AG, Rule S. Interstitial pneumonitis following mitozantrone, chlorambucil and prednisolone (MCP) chemotherapy. Clin Oncol. 1999;11(3):184–6.
Müller NL, White DA, Jiang H, Gemma A. Diagnosis and management of drug-associated interstitial lung disease. Br J Cancer. 2004;91(Suppl 2):S24–30.
Forghieri F, Luppi M, Morselli M, Potenza L. Cytarabine-related lung infiltrates on high resolution computerized tomography: a possible complication with benign outcome in leukemic patients. Haematologica. 2007;92(9):e85–90.
Gagnadoux F, Roiron C, Carrie E, Monnier-Cholley L, Lebeau B. Eosinophilic lung disease under chemotherapy with oxaliplatin for colorectal cancer. Am J Clin Oncol. 2002;25(4):388–90.
Vahid B, Marik PE. Infiltrative lung diseases: complications of novel antineoplastic agents in patients with hematological malignancies. Can Respir J. 2008;15(4):211–6.
Kirkbride P, Hatton M, Lorigan P, Joyce P, Fisher P. Fatal pulmonary fibrosis associated with induction chemotherapy with carboplatin and vinorelbine followed by CHART radiotherapy for locally advanced non-small cell lung cancer. Clin Oncol. 2002;14(5):361–6.
Koc M, Polat P, Suma S. Effects of tamoxifen on pulmonary fibrosis after cobalt-60 radiotherapy in breast cancer patients. Radiother Oncol. 2002;64(2):171–5.
Hay J, Shahzeidi S, Laurent G. Mechanisms of bleomycin-induced lung damage. Arch Toxicol. 1991;65(2):81–94.
Schmitz N, Diehl V. Carmustine and the lungs. Lancet. 1997;349(9067):1712–3.
Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315–52.
Hillegass E, Puthoff M, Frese EM, Thigpen M, Sobush DC, Auten B, et al. Role of physical therapists in the management of individuals at risk for or diagnosed with venous thromboembolism: evidence-based clinical practice guideline. Phys Ther. 2016;96(2):143–66.
Dimeo F, Bertz H, Finke J, Fetscher S, Mertelsmann R, Keul J. An aerobic exercise program for patients with haematological malignancies after bone marrow transplantation. Bone Marrow Transplant. 1996;18(6):1157–60.
Dimeo FC, Tilmann MH, Bertz H, Kanz L, Mertelsmann R, Keul J. Aerobic exercise in the rehabilitation of cancer patients after high dose chemotherapy and autologous peripheral stem cell transplantation. Cancer. 1997;79(9):1717–22.
Dimeo F, Rumberger BG, Keul J. Aerobic exercise as therapy for cancer fatigue. Med Sci Sports Exerc. 1998;30(4):475–8.
Dimeo FC, Thomas F, Raabe-Menssen C, Pröpper F, Mathias M. Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery. A randomised controlled trial. Support Care Cancer. 2004;12(11):774–9.
Dimeo F, Schwartz S, Wesel N, Voigt A, Thiel E. Effects of an endurance and resistance exercise program on persistent cancer-related fatigue after treatment. Ann Oncol. 2008;19(8):1495–9.
Segal RJ, Reid RD, Courneya KS, Malone SC, Parliament MB, Scott CG, et al. Resistance exercise in men receiving androgen deprivation therapy for prostate cancer. J Clin Oncol. 2003;21(9):1653–9.
Galvão DA, Taaffe DR, Spry N, Joseph D, Newton RU. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: a randomized controlled trial. J Clin Oncol. 2010;28(2):340–7.
Courneya KS, Mackey JR, Bell GJ, Jones LW, Field CJ, Fairey AS. Randomized controlled trial of exercise training in postmenopausal breast cancer survivors: cardiopulmonary and quality of life outcomes. J Clin Oncol. 2003;21(9):1660–8.
Cavalheri V, Jenkins S, Cecins N, Gain K, Phillips MJ, Sanders LH, et al. Exercise training for people following curative intent treatment for non-small cell lung cancer: a randomized controlled trial. Braz J Phys Ther. 2017;21(1):58–68.
Uth J, Schmidt JF, Christensen JF, Hornstrup T, Andersen LJ, Hansen PR, et al. Effects of recreational soccer in men with prostate cancer undergoing androgen deprivation therapy: study protocol for the ‘FC Prostate’ randomized controlled trial. BMC Cancer. 2013;13:595.
Chen TC, Hsieh CC, Tseng KW, Ho CC, Nosaka K. Effects of descending stair walking on health and fitness of elderly obese women. Med Sci Sports Exerc. 2017;49(8):1614–22.
Adams SC, DeLorey DS, Davenport MH, Stickland MK, Fairey AS, North S, et al. Effects of high-intensity aerobic interval training on cardiovascular disease risk in testicular cancer survivors: a phase 2 randomized controlled trial. Cancer. 2017;123(20):4057–65.
Fazzino TL, Klemp J, Befort C. Late breast cancer treatment-related symptoms and functioning: associations with physical activity adoption and maintenance during a lifestyle intervention for rural survivors. Breast Cancer Res Treat. 2018;168(3):755–61.
Midtgaard J, Rorth M, Stelter R, Adamsen L. The group matters: an explorative study of group cohesion and quality of life in cancer patients participating in physical exercise intervention during treatment. Eur J Cancer Care (Engl). 2006;15(1):25–33.
May AM, Duivenvoorden HJ, Korstjens I, van Weert E, Hoekstra-Weebers JE, van den Borne B, et al. The effect of group cohesion on rehabilitation outcome in cancer survivors. Psychooncology. 2008;17(9):917–25.
Losito J, Murphy S, Thomas M. The effects of group exercise on fatigue and quality of life during cancer treatment. Oncol Nurs Forum. 2006;33(4):821–5.
Mutrie N, Campbell AM, Whyte F, McConnachie A, Emslie C, Lee L, et al. Benefits of supervised group exercise programme for women being treated for early stage breast cancer: pragmatic randomised controlled trial. BMJ. 2007;334(7592):517.
Adamsen L, Quist M, Andersen C, Møller T, Herrstedt J, Kronborg D, et al. Effect of a multimodal high intensity exercise intervention in cancer patients undergoing chemotherapy: randomised controlled trial. BMJ. 2009;339:b3410.
Ray HA, Verhoef MJ. Dragon boat racing and health-related quality of life of breast cancer survivors: a mixed methods evaluation. BMC Complement Altern Med. 2013;13:205.
Jones LW, Douglas PS, Khouri MG, Mackey JR, Wojdyla D, Kraus WE, et al. Safety and efficacy of aerobic training in patients with cancer who have heart failure: an analysis of the HF-ACTION randomized trial. J Clin Oncol. 2014;32(23):2496–502.
Bonsignore A, Marzolini S, Oh P. Cardiac rehabilitation for women with breast cancer and treatment-related heart failure compared with coronary artery disease: a retrospective study. J Rehabil Med. 2017;49(3):277–81.
Darby SC, Ewertz M, McGale P, Bennet AM, Blom-Goldman U, Brønnum D, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987–98.
Cutter DJ, Schaapveld M, Darby SC, Hauptmann M, van Nimwegen FA, Krol AD, et al. Risk of valvular heart disease after treatment for Hodgkin lymphoma. J Natl Cancer Inst. 2015;107(4). https://doi.org/10.1093/jnci/djv008.
Retèl VP, van der Molen L, Hilgers FJ, Rasch CR, L'Ortye AA, Steuten LM, et al. A cost-effectiveness analysis of a preventive exercise program for patients with advanced head and neck cancer treated with concomitant chemo-radiotherapy. BMC Cancer. 2011;11:475.
van der Molen L, Heemsbergen WD, de Jong R, van Rossum MA, Smeele LE, Rasch CR, et al. Dysphagia and trismus after concomitant chemo-Intensity-Modulated Radiation Therapy (chemo-IMRT) in advanced head and neck cancer; dose-effect relationships for swallowing and mastication structures. Radiother Oncol. 2013;106(3):364–9.
van der Molen L, van Rossum MA, Rasch CR, Smeele LE, Hilgers FJ. Two-year results of a prospective preventive swallowing rehabilitation trial in patients treated with chemoradiation for advanced head and neck cancer. Eur Arch Otorhinolaryngol. 2014;271(5):1257–70.
Caiozzo VJ, Giedzinski E, Baker M, Suarez T, Izadi A, Lan M, et al. The radiosensitivity of satellite cells: cell cycle regulation, apoptosis and oxidative stress. Radiat Res. 2010;174(5):582–9.
Wozniak AC, Anderson JE. The dynamics of the nitric oxide release-transient from stretched muscle cells. Int J Biochem Cell Biol. 2009;41(3):625–31.
Deo SV, Al-Kindi SG, Oliveira GH. Management of advanced heart failure due to cancer therapy: the present role of mechanical circulatory support and cardiac transplantation. Curr Treat Options Cardiovasc Med. 2015;17(6):388.
Bianco CM, Al-Kindi SG, Oliveira GH. Advanced heart failure therapies for cancer therapeutics-related cardiac dysfunction. Heart Fail Clin. 2017;13(2):327–36.
Oliveira GH, Matthias D, Naftel DC, Yuan Y, Meyers SL, Schmuhl D, et al. 111 outcomes of patients with anthracycline cardiomyopathy treated with mechanical circulatory support: data from the INTERMACS Registry. J Heart Lung Transplant. 31(4):S46.
Oliveira GH, Dupont M, Naftel D, Myers SL, Yuan Y, Tang WH, et al. Increased need for right ventricular support in patients with chemotherapy-induced cardiomyopathy undergoing mechanical circulatory support: outcomes from the INTERMACS Registry (Interagency Registry for Mechanically Assisted Circulatory Support). J Am Coll Cardiol. 2014;63(3):240–8.
Patel SR, Saeed O, Naftel D, Myers S, Kirklin J, Jorde UP, et al. Outcomes of restrictive and hypertrophic cardiomyopathies after LVAD: an INTERMACS analysis. J Card Fail. 2017;23:859–67.
Topkara VK, Garan AR, Fine B, Godier-Furnémont AF, Breskin A, Cagliostro B, et al. Myocardial recovery in patients receiving contemporary left ventricular assist devices: results from the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS). Circ Heart Fail. 2016;9(7):e003157.
Murakawa T, Murayama T, Nakajima J, Ono M. Lung lobectomy in a patient with an implantable left ventricular assist device. Interact Cardiovasc Thorac Surg. 2011;13(6):676–8.
Loyaga-Rendon RY, Inampudi C, Tallaj JA, Acharya D, Pamboukian SV. Cancer in end-stage heart failure patients supported by left ventricular assist devices. ASAIO J. 2014;60(5):609–12.
Smail H, Pfister C, Baste JM, Nafeh-Bizet C, Gay A, Barbay V, et al. A difficult decision: what should we do when malignant tumours are diagnosed in patients supported by left ventricular assist devices? Eur J Cardiothorac Surg. 2015;48(3):e30–6.
Khan M, Wasim A, Mirrakhimov AE, McMahon BA, Judge DP, Chu LC, et al. Case report of a patient with left ventricular assistance device undergoing chemotherapy for a new diagnosis of lung cancer. Case Rep Oncol Med. 2015;2015:163727.
Netuka I, Stepankova P, Urban M, Maly J, Szarszoi O, Dorazilova Z, et al. Is severe cardiac dysfunction a contraindication for complex combined oncotherapy of Hodgkin’s lymphoma? Not any more. ASAIO J. 2013;59(3):320–1.
Swartz MF, Fink GW, Carhart RL. Use of a biventricular assist device in the treatment of acute doxorubicin-induced cardiotoxicity. Congest Heart Fail. 2004;10(4):197–9.
Simsir SA, Lin SS, Blue LJ, Gockerman JP, Russell SD, Milano CA. Left ventricular assist device as destination therapy in doxorubicin-induced cardiomyopathy. Ann Thorac Surg. 2005;80(2):717–9.
Schweiger M, Dave H, Lemme F, Cavigelli-Brunner A, Romanchenko O, Heineking B, et al. Acute chemotherapy-induced cardiomyopathy treated with intracorporeal left ventricular assist device in an 8-year-old child. ASAIO J. 2013;59(5):520–2.
Narayan V, Deshpande C, Bermudez CA, Golato JM, Lee JC, Diamond J, et al. Bilateral lung transplantation for bleomycin-associated lung injury. Oncologist. 2017;22(5):620–2.
Mehra MR, Canter CE, Hannan MM, Semigran MJ, Uber PA, Baran DA, et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: a 10-year update. J Heart Lung Transplant. 2016;35(1):1–23.
Oliveira GH, Hardaway BW, Kucheryavaya AY, Stehlik J, Edwards LB, Taylor DO. Characteristics and survival of patients with chemotherapy-induced cardiomyopathy undergoing heart transplantation. J Heart Lung Transplant. 2012;31(8):805–10.
Dinu M, Abbate R, Gensini GF, Casini A, Sofi F. Vegetarian, vegan diets and multiple health outcomes: a systematic review with meta-analysis of observational studies. Crit Rev Food Sci Nutr. 2017;57(17):3640–9.
Kahleova H, Levin S, Barnard N. Cardio-metabolic benefits of plant-based diets. Nutrients. 2017;9(8). https://doi.org/10.3390/nu9080848.
Patel H, Chandra S, Alexander S, Soble J, Williams KA. Plant-based nutrition: an essential component of cardiovascular disease prevention and management. Curr Cardiol Rep. 2017;19(10):104.
Balduyck B, Sardari Nia P, Cogen A, Dockx Y, Lauwers P, Hendriks J, et al. The effect of smoking cessation on quality of life after lung cancer surgery. Eur J Cardiothorac Surg. 2011;40(6):1432–7. discussion 7-8
Jones LW, Liang Y, Pituskin EN, Battaglini CL, Scott JM, Hornsby WE, et al. Effect of exercise training on peak oxygen consumption in patients with cancer: a meta-analysis. Oncologist. 2011;16(1):112–20.
Bernhörster M, Rosenhagen A, Vogt L, Thiel C, Jäger E, Banzer W. Marathon run under chemotherapy: is it possible? Onkologie. 2011;34(5):259–61.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Cancer Rehabilitation
Rights and permissions
About this article

Cite this article
Syrkin, G., Bartels, M.N. The Role of Rehabilitation Medicine in Managing Cardiopulmonary Complications of Cancer. Curr Phys Med Rehabil Rep 6, 121–130 (2018). https://doi.org/10.1007/s40141-018-0183-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40141-018-0183-z