
Abstract
Background
Survivin is involved in the regulation of cell division and survival, two key processes in cancer. The majority of studies on survivin in colorectal cancer (CRC) have focused on protein expression and less is known about the expression of survivin splicing variants or survivin gene polymorphisms in CRC. In the present study, the mRNA levels of the five known isoforms of survivin as well as survivin protein were assessed in matched normal and neoplastic colorectal tissue. Moreover, the 9386 C/T and -31 G/C polymorphisms were investigated.
Methods
Quantitative RT-PCR was used to assess mRNA levels in fresh/frozen tissue samples. Protein levels were immunohistochemically evaluated on formalin-fixed paraffin-embedded tissue sections. Individuals were genotyped using real time PCR
Results
Expression of all 5 survivin splice variants as well as survivin protein was elevated in colorectal carcinomas compared to normal tissue. Specific splice variant expression differentially correlated with clinicopathological parameters. Furthermore, both snps correlated with splice variant levels or their ratios in colorectal carcinomas while the -31 G/C snp may be related to CRC development and improved overall survival.
Conclusion
Our results support a role of survivin in colorectal carcinogenesis while the -31 G/C snp may constitute a marker of survival.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Survivin is a unique member of the family of the Inhibitors of Apoptosis Proteins (IAPs) as it carries a single baculoviral IAP repeat (BIR) domain. Survivin has lately drawn much attention due to its involvement in many cellular processes. It functions as a central regulator of cell division as it has been shown to promote mitotic progression and G1/S transition in cancer cells [1, 2]. Survivin also exerts significant anti-apoptotic functions via caspase-dependent and independent mechanisms [2]. Consistently, it is not expressed or is present at low levels in normal differentiated tissues, whereas it is highly expressed in many tumors including breast, lung and colon [3–6]. Survivin has also been correlated with chemoresistance [7].
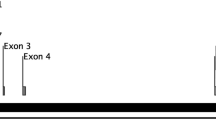
Five splice variants that give rise to distinct survivin protein isoforms have been characterized (Fig. 1). Survivin-2B has a 23 aminoacid insertion between exon 2 and 3 causing a markedly reduced anti apoptotic potential [8]. Survivin-ΔEx3 lacks exon 3 and has a different carboxy-terminal tail due to a frameshift in exon 4 but retains an anti-apoptotic activity [8]. In contrast, survivin-3B has an extra exon 3, derived from part of intron 3, that causes a frameshift resulting in a protein truncated by 22 amino acids that exerts cytoprotective functions [9, 10]. The recently characterized isoform, survivin-2α, contains the coding sequences from exon 1 and exon 2 and one additional amino acid before termination. This protein isoform contains a truncated BIR domain and lacks the carboxy-terminal coiled-coil domain. It is, therefore, assumed that survivin-2α does not exert anti-apoptotic activity [11]. Survivin is known to homodimerize in solution. Since survivin isoforms exert dinstinct apoptosis-related properties, heterodimer formation between survivin and its isoforms may be important in the regulation of survivin function with potential significant implications in carcinogenesis [1].

The exons of the 5 splice variants of survivin.BIR: baculoviral IAP repeat, BIR’: truncated BIR. UTR: Untranslated region. Horizontal arrows indicate primer positions. Perpendicular arrows indicated the site of the stop codon
A single nucleotide polymorphism (snp) was found in the promoter of the survivin gene [12]. It is located at position -31 within a cell cycle-dependent element (CDE) and a cell cycle homology region (CHR) repressor binding motif. Modification of this binding motif results in altered cell cycle-dependent transcription that characterizes survivin expression. The presence of -31 G/C snp may result in higher levels of survivin expression and it has previously been correlated with increased risk for lung cancer development. However, there was no correlation with cervical cancer suggesting that further investigation is required to clarify the significance of this polymorphism in human cancer [13, 14].
A second snp, 9386 C/T (rs2239680), located in the 3′ untranslated region (UTR) of the survivin gene was selected from the National Center for Biotechnology Information SNP database (http://www.ncbi.nlm.nih.gov/ snp). It is known that many regulatory events occur at the 3′UTR including mRNA stability and post-transcriptional regulation, often through binding of microRNAs [15].
Colorectal cancer is a major cause of morbidity and mortality worldwide. Alterations in pathways regulating important biological processes including cell survival, cell proliferation, epithelial to mesenchymal transition and stroma production have been shown to contribute to colorectal carcinogenesis and tumor progression [16, 17]. Several lines of evidence suggest that survivin is implicated in the progression of dysplasia to neoplasia in the colon [18]. A significant role of survivin in colorectal carcinoma progression and recurrence of colon cancer liver metastases has been previously demonstrated [19, 20]. However, most studies have focused on protein expression, and the significance of specific splice variant expression or of survivin gene polymorphisms in CRC has not been fully addressed. We, therefore, quantified the mRNA expression of survivin, survivin-3B, survivin-2B, survivin-ΔEx3 and survivin-2α in matched normal and neoplastic colorectal tissue. We also assessed the presence of the snps 9386 C/T and -31 G/C of the survivin gene in blood samples and CRC tissues. Correlations between survivin splice variant mRNA expression, presence of survivin snps, survivin protein expression by immunohistochemistry and clinicopathological characteristics were evaluated. Moreover, the relationship between the -31 G/C snp and the risk for CRC development was assessed.
2 Materials and methods
2.1 Patients and samples
Peripheral blood and fresh-frozen colonic tissue were prospectively obtained from 45 consecutive patients who underwent therapeutic surgery at the University Hospital of Patras, Greece. Table 1 lists the clinicopathological characteristics of the patients for which fresh/frozen samples were available for this study. Moreover, 116 formalin fixed paraffin-embedded colorectal carcinoma samples were retrieved from the archives of the Department of Pathology at the University Hospital of Patras. In addition, blood samples from 132 healthy donors were obtained. For 95 (58.3%) patients information regarding relapse and survival was available. Of these, 53 (55.8 %) patients relapsed and the remaining (44.2%) remained disease free. Ethical approval for this study was obtained from the Institutional Review Board.
2.2 Primer design
The sequence of each splice variant was obtained either from the National Centre for Biotechnology Information (NCBI: http://www.ncbi.nlm.nih.gov/) or from published reports [9, 11]. Regarding the gene expression analysis, primers and Taqman probes (Table 2) were designed at areas that were unique for each variant (Fig. 1), using Primer3 [21] and then subjected to a BLAST (NCBI) analysis to ensure specificity. Similarly, for the -31 G/C snp genotyping, primers and Taqman LNA probes were designed, specific for each allele. The 9386 C/T snp was genotyped using allele-specific primers resulting in differentially sized products and thus allowing allele detection using sybr green in real time polymerase chain reactions (PCR) (Table 2). Primers were synthesized by the Foundation for Research and Technology-Hellas (Crete, Greece) or by Metabion International (Martinsried, Germany), Taqman probes by DNA Technology A/S (Aarhus C., Denmark) and LNA Taqman probes by Sigma-Proligo (The Woodlands, TX, USA).
2.3 Splice variant expression quantification
Total RNA was extracted from the fresh-frozen tissue samples using the Absolutely RNA ffpe kit (Stratagene, La Jolla, USA) and then quantified and reverse transcribed as previously described [22]. The expression of each splice variant was quantified by quantitative PCR using the variant-specific primers and Taqman probes (Table 1) as previously described [23]. Expression levels were normalized to Alu-Sq levels that were found to be stably expressed in normal and tumor tissue of different grades and stages.
2.4 Snp genotyping
DNA was extracted from whole blood samples of 47 patients with CRC and 132 healthy controls using the QIAamp DNA blood mini kit (QIAGEN, GmbH, Germany). Moreover, DNA was extracted from 116 formalin-fixed paraffin embedded tissue samples using a standard proteinase K, phenol/chloroform extraction procedure. The -31 G/C snp was genotyped using the primers and allele-specific Taqman LNA probes (Table 2) in real time PCR reactions using the Brilliant Quantitative PCR Core Reagents (Stratagene) and the MX3000p (Stratagene). The 9386 C/T snp was genotyped in 42 patients for which fresh-frozen tissue was also available using allele specific primers. A GC tail was added at the 5′ end of the C-specific primer so that different product sizes were obtained thus allowing genotyping using sybr green in real time PCR (sybr green master mix, PrimerDesign, UK) (Table 2).
2.5 Immunohistochemistry
Representative 4 μm tissue sections were de-paraffinized in xylene and rehydraded in graded ethanol solutions. Antigen retrieval was enhanced by microwaving the slides in 0.01 M citrate buffer (pH = 6). Endogenous peroxidase activity was blocked by treatment with 1% hydrogen peroxide for 15 min, followed by incubation with protein blocking solution (3% BSA in TBS). Sections were subsequently incubated with mouse monoclonal anti-survivin antibody (71G4B7E, Cell Signaling, Beverly, MA) in dilution 1:80 overnight at 4°C. Bound primary antibody was detected with the Envision detection kit (DAKO, Hamburg, Germany) following the manufacturer’s instructions. Slides were counterstained with haematoxylin, dehydraded and mounted. For negative controls, blocking solution was added instead of the primary antibody.
2.6 Immunohistological evaluation
Nuclear and cytoplasmic immunostaining for survivin was evaluated separately. Nuclear expression of survivin was semi-quantitatively evaluated based on the percentage of positive nuclei: 0: nuclear positivity in less than 10% of tumor cells, 1: nuclear expression in 10–30% of tumor cells, 2: nuclear expression in 30–80% of tumor cells and 3: nuclear expression in >80% of tumor cells. Cytoplasmic immunoreactivity was homogeneously distributed among the tumor cells and scored as follows: 0: negative staining, 1: weak staining, 2: moderate staining and 3: strong staining.
2.7 Statistical analysis
The data were analysed using SPSS (release 16, Chicago, IL, USA). Kruskal-Wallis and Mann-Whitney nonparametric tests were performed for intergroup comparisons of the expression levels of the survivin splice variants. Wilcoxon paired samples test was used for comparisons between related groups. Chi-square analysis was performed to detect associations between snps and clinicopathological data. The Kaplan-Meier analysis was used to compare survival curves. Logistic regression was used for cancer risk assessment. The level of significance was set at p value <0.05.
3 Results
3.1 Expression of survivin splice variants in normal and neoplastic tissue
Positive mRNA expression of all survivin isoforms was more frequently observed in neoplastic compared to normal tissue. In normal tissue, survivin, survivin-ΔEx3, survivin-2α, survivin-2B and survivin-3B were expressed in 80.8, 68.1, 100, 87.2 and 78.7 % of cases, respectively, whereas in neoplastic tissue, positive mRNA expression of theses variants was detected in 98.8, 89.4, 100, 97.8 and 95.7 % of cases, respectively. In addition, expression levels of the five survivin splice variants were significantly higher in neoplastic tissue compared to normal tissue (p ≤ 0.001), as shown in Tables 3 and 4 (Figs. 2 and 3).

Expression of survivin splice variants in normal and neoplastic tissue. N: normal tissue, CA: neoplastic tissue, S: survivin

Relationship between expression levels of survivin splice variants and -31 genotype. S: survivin. A: neoplastic tissue, B: normal tissue
No significant difference was observed in the expression levels between males and females and between patients with positive or negative lymph nodes. mRNA expression of survivin-2B significantly correlated with tumor grade with levels being higher in well differentiated compared to moderately and poorly differentiated tumors (Tables 3 and 4). A similar trend of higher expression in well differentiated tumors was also observed for survivin, survivin-ΔEx3 and survivin-2α but the differences failed to reach statistical significance (Tables 3 and 4).
Survivin splice variants were differentially expressed among different stages of the disease (Tables 3 and 4). Statistical analysis could safely be performed only for stages B and C due to the small sample number of in situ and stage A and D samples. Therefore, it should be noted that only differences between stages B and C can be stated with any confidence. Survivin, survivin-2B and -2α levels were lower in stage A than in B. The mRNA expression levels of all splice variants with the exception of survivin-3B were also higher in stage B tumors compared to stage C (statistical significance was reached only for survivin-ΔEx3, -2B and -2α with p = 0.008, 0.028 and 0.024, respectively), and in stage D tumors compared to stage C (p values for survivin, survivin-ΔEx3, -2B and -2α are 0.039, 0.010, 0.027 and 0.017, respectively).
3.2 Ratios of splice variant expression in normal and neoplastic tissue
The ratios of the expression of the different splice variants were then assessed. The expression ratio survivin to survivin-3B was significantly higher (p = 0.005) in neoplatic (median: 0.95; 0.31–1.93) compared to normal tissue (median: 0.72; 0–1.91) (Fig. 4a).

The change of ratios of expression of the different variants in normal and neoplastic tissue and according to degree of differentiation. ** indicate differences significant to the 0.05 level
Moreover, the ratio of survivin to survivin-ΔEx3 was significantly higher (p = 0.043) in the rectum samples (median: 1.48; 0.65–3.19) compared to left and right colonic tissue samples (median: 1.03; 0.45–1.78) although a similar difference was not noted for any other ratio. None of the ratios differed between lymph node positive or negative patients, or between different stages. However, the ratio of survivin to survivin-2B expression was significantly higher (p = 0.038) in moderately (median: 0.65; 0.49–1.16) compared to well differentiated tumors (median: 0.97; 0.44–2.31) (Fig. 4b).
3.3 Assessment of survivin snps 9386 C/T and -31 G/C in CRC
Regarding the -31 G/G snp of the survivin gene, the G allele was noted more frequently than the C allele. Notably, 63 (38.6%) patients were GG, 16 (9.8%) were CC and 84 (51.6%) were heterozygotes. Moreover, in the healthy control group, 66 (50%) were GG, 16 (12.1%) were CC and 50 (37.9%) were heterozygotes. Neither allele was associated with the gender or the primary site. However, the C allele appears to be associated with CRC. In fact, 101 (61.9%) CRC patients carried the C allele, whereas in healthy controls, the percentage dropped to 50 (66 individuals) (p = 0.04). However, a larger number of cases is required to assess whether the C allele may predispose to CRC. Currently, the CC homozygotes may have a higher risk of developing cancer compared to GG individuals and the heterozygotes (odds ratio 1.587, 95% C.I: 0.997–2.526, p = 0.051).
Regarding the 9386 C/T snp, which was genotyped in 42 cases for which fresh/frozen tissue was available, 2 cases were CC (4.8%), 28 were CT (66.6%) and 12 were TT (28.6%).
3.4 Relationships between survivin snp genotypes and splice variant expression
Patients carrying the C allele at -31 had higher mRNA levels of the splice variants survivin, survivin-ΔEx3, survivin-2B and survivin-2α in neoplastic tissue compared to non-carriers (p = 0.056, 0.003, 0.022, 0.022, respectively) (Fig. 3). Interestingly, expression levels in normal tissue were independent of the -31 genotype (Fig. 3).
No association emerged between splice variant expression and the 9386 C/T snp genotype with the exception of the ratios survivin to survivin-2α and survivin to survivin-2B in neoplastic tissue. Notably, both of these ratios were lower in CC patients compared to CT and TT patients (survivin/survivin2α: p = 0.029, median: 0.38 [0.33–0.44]; 0.85 [0.41–1.02]; 0.60 [0.41–0.69], respectively and survivin/survivin-2B: p = 0.017, median: 0.48 [0.44–0.52]; 0.95 [0.54–1.26]; 0.65 [0.47–0.94], respectively).
3.5 Relationship between the -31 G/C snp, disease progression and patient survival
Since the C allele was more frequently observed in CRC patients and associated with higher levels of survivin expression in neoplastic tissue, the relationship between the -31 G/C snp and relapse and survival was assessed. Neither allele was associated with increased risk of relapse or with the time to disease progression (data not shown). Surprisingly, however, the C allele was associated with improved overall survival (95% CI; 95.074–118.126; p = 0.047) (Fig. 5).

Improved survival in the presence of the -31 C allele. Continuous and dotted lines represent the patients carrying the C allele and the GG homozygotes, respectively
3.6 Survivin protein expression and localization
In normal colorectal mucosa survivin protein expression was nuclear and mainly confined to the crypt epithelium (Fig. 6). A significantly higher survivin expression was found in neoplastic tissue compared to normal tissue (p < 0.001). Moreover, while in normal tissue samples protein expression was exclusively located in the nucleus, in carcinomas cytoplasmic expression of survivin was also noted in 7 of 43 cases (16.28%) (Table 5, Fig. 6). In carcinomas, nuclear survivin expression correlated with the primary site, with expression levels being higher in tumors of the right colon compared to tumors located in the left colon or the rectum (p = 0.004) (Table 5). There was no correlation between survivin mRNA and protein levels. Furthermore, survivin protein expression did not correlate either with the -31 G/C or the 9386 C/T snp genotype or with any of the clinicopathological parameters analyzed.

Survivin protein expression by immunohistochemistry in colorectal carcinomas. a. Significantly higher nuclear expression of survivin in cancerous tissue (upper part) compared to adjacent normal colonic crypts (lower part) (x20), b. Strong nuclear expression of survivin in a case of colorectal carcinoma (x40) and c. A representative case showing both cytoplasmic and nuclear localization of survivin (x40)
4 Discussion
Survivin has attracted much attention in cancer research due to its involvement in the regulation of cell division and survival. Most studies of survivin in CRC have focused on protein expression and less is known about the expression of survivin splicing variants or survivin gene polymorphisms in CRC. In the present study, the mRNA expression levels of the five known isoforms of survivin were assessed in matched normal and neoplastic colorectal tissue. Also survivin protein levels and survivin 9386 C/T and -31 G/C genetic polymorphisms were analysed. Our study provides evidence on the distinct significance of survivin splice variant expression and gene polymorphisms in human colorectal carcinogenesis
In agreement with previous reports, we have shown that mRNA expression of survivin splice variants was more frequent and significantly higher in neoplastic compared to normal tissue suggesting survivin involvement in colorectal carcinogenesis [24, 25]. To the best of our knowledge this is the first report of splice variants survivin-2α and survivin-3B expression in human CRC. Similarly to the findings of Suga et al, survivin expression did not correlate with gender and lymph node metastasis. However, survivin-2B mRNA levels were significantly higher in well differentiated tumors and survivin-ΔEx3, -2B and -2α mRNA expression was significantly higher in stage B than in stage C patients indicating a correlation of specific splice variant expression with a less aggressive CRC phenotype. These findings are in agreement with the lack of an anti-apoptotic activity that characterize survivin-2B and survivin-2α isoforms but are unexpected for survivin-ΔEx3 that is known to promote cell survival [8, 11]. It would be of interest to assess the expression of the survivin variants in the corresponding metastases and the circulating blood cells. It has been shown that in both cases, expression of molecules in key pathways including EGFR and TGFβ are often different between the primary tumor, the metastases and the circulating blood cells [16, 26].
To further address the significance of the specific survivin splice variant expression in CRC we assessed their ratio relative to survivin, since the relative abundance of these isofoms may be more significant than the presence of each isoform alone. In contrast to the mRNA levels, survivin to survivin-ΔEx3 and survivin-2α ratios showed no significant correlation with any of the clinicopathological parameters analyzed. However, survivin-2B levels were significantly higher relatively to survivin in well differentiated tumors. The later finding is consistent with the reduced anti-apoptotic activity of this isoform and also indicates that among the different splice variants survivin-2B is more likely to associate with favorable features of CRC. Unfortunately, the cohort of patients for whom fresh/frozen tissue was available for splice variant analysis had no sufficient time of follow up to allow survival analysis so as to assess the prognostic significance of the survivin isoforms. However, in further agreement with our findings, distinct significance of survivin specific splice variant expression has been reported in several tumor types [27]. It has been shown that survivin isoforms dimerize and this could partly constitute a control mechanism for the end action of survivin. Given the differential expression of splice variants, it appears to be more prudent to take into account ratios of expression rather than each isoform alone.
Of interest is the finding that both snps of the survivin gene correlated with survivin isoform mRNA expression levels or ratios in neoplastic but not in normal tissue, suggesting that these snps may influence the differential expression of survivin splice variants in colorectal carcinogenesis. Regarding the better studied -31 G/C snp, this finding may suggest that repression through binding to the CDE/CHR element gains importance as a control mechanism of survivin expression in cancer, since other mechanisms involved in the regulation of survivin expression such as APC and P53 are often inactivated in neoplasia due to mutations [28, 29]. In agreement with the findings of Gazouli et al we also showed a significantly higher frequency of the C allele in CRC patients compared to healthy controls suggesting a role of the -31 G/C snp in colorectal carcinogenesis [30]. Nevertheless, it is possible that the -31 G/C snp does not have a causative role but may simply feature a marker.
Notably we provided evidence that the presence of the C allele in -31 G/C snp was associated with improved overall survival of CRC patients. Although an association of survivin -31 G/C snp with increased risk of cancer development has been suggested by other reports, its prognostic significance in human CRC has not previously been addressed. Considering that the -31 G/C snp correlated with splice variant expression in our tumor samples, this finding agrees with the association we found between isoform expression and favorable pathologic features, further indicating a complex most likely favorable prognostic role of survivin in human CRC. Although many reports state that increased levels of survivin correlate with colorectal cancer progression, liver metastasis [19, 20] and decreased survival, contradictory observations are also available [31]. In some studies different splice variants appear to correlate differently to survival while in others survivin levels were unrelated to survival in CRC cases [31, 32]. However, it is also likely that the -31 G/C snp may simply be a favorable prognostic marker in CRC irrespectively of its possible effect on survivin expression.
Contrary to mRNA levels, protein levels were unrelated to any of the clinicopathological parameters with the exception of the primary site. This may reflect the genetic differences noted in the different anatomical sites which may be accounted for by their different embryological origin [33]. The antibody used in the immunohistochemical analysis was not able to differentiate between different isoforms and, therefore, it is not clear whether the differences observed at the mRNA levels between stages and grades are reflected on the protein level or not. However, the contribution of post-transcriptional regulatory mechanisms in the regulation of survivin expression may account for the lack of correlation between protein and mRNA expression and is in agreement with the findings of Kannangai et al although contradictory reports have also been published [1, 34, 35].
Protein expression was detected exclusively in the nucleus in normal tissue, whereas both nuclear and cytoplasmic expression, with the predominance of nuclear staining, was noted in CRCs. A cytoplasmic expression of survivin has previously been demonstrated for colorectal carcinomas [6, 19]. The difference in localization patterns between studies may be due to the different antibodies used for the detection of survivin, targeting different areas of the protein and therefore reacting with different isoforms. It is known that survivin exists in two subcellular pools consistent with its function in cell division (nucleus) and cell viability (cytoplasm) as well as the presence of the different isoforms which have distinct cellular localizations [36]. The nuclear immunoreactivity has been associated with significantly higher proliferating index in hepatocellular carcinomas suggesting a predominant role of survivin in promoting cell division in these tumors [37, 38]. The cellular localization pattern of survivin in our tumor samples suggests that survivin probably exerts both cell division-promoting and anti-apoptotic functions in colorectal carcinogenesis.
In conclusion, mRNA expression of all 5 survivin splice variants as well as survivin protein expression was elevated in colorectal carcinomas compared to normal tissue supporting a role of survivin in colorectal carcinogenesis. Specific survivin splice variant expression differentially correlated with pathologic tumor parameters. Furthermore, both the -31 G/C snp and the 9386 C/T snp correlated with splice variant levels or their ratios in colorectal carcinomas while the -31 G/C snp may be related to CRC development and overall survival.
References
F. Li, Survivin study: what is the next wave? J. Cell. Physiol. 197, 8–29 (2003)
F. Li, G. Ambrosini, E.Y. Chu, J. Plescia, S. Tognin, P.C. Marchisio, D.C. Altieri, Control of apoptosis and mitotic spindle checkpoint by survivin. Nature 396, 580–584 (1998)
G. Ambrosini, C. Adida, D.C. Altieri, A novel anti-apoptosis gene, survivin, expressed in cancer and lymphoma. Nat. Med. 3, 917–921 (1997)
K. Tanaka, S. Iwamoto, G. Gon, T. Nohara, M. Iwamoto, N. Tanigawa, Expression of survivin and its relationship to loss of apoptosis in breast carcinomas. Clin. Cancer Res. 6, 127–134 (2000)
M. Monzo, R. Rosell, E. Felip, J. Astudillo, J.J. Sanchez, J. Maestre, C. Martin, A. Font, A. Barnadas, A. Abad, A novel anti-apoptosis gene: re-expression of survivin messenger RNA as a prognosis marker in non-small-cell lung cancers. J. Clin. Oncol. 17, 2100–2104 (1999)
H. Kawasaki, D.C. Altieri, C.D. Lu, M. Toyoda, T. Tenjo, N. Tanigawa, Inhibition of apoptosis by survivin predicts shorter survival rates in colorectal cancer. Cancer Res. 58, 5071–5074 (1998)
F. Li, X. Ling, Survivin study: an update of “what is the next wave”? J. Cell. Physiol. 208, 476–486 (2006)
C. Mahotka, M. Wenzel, E. Springer, H.E. Gabbert, C.D. Gerharz, Survivin-deltaEx3 and survivin-2B: two novel splice variants of the apoptosis inhibitor survivin with different antiapoptotic properties. Cancer Res. 59, 6097–6102 (1999)
A. Badran, A. Yoshida, K. Ishikawa, T. Goi, A. Yamaguchi, T. Ueda, M. Inuzuka, Identification of a novel splice variant of the human anti-apoptopsis gene survivin. Biochem. Biophys. Res. Commun. 314, 902–907 (2004)
S.K. Knauer, C. Bier, P. Schlag, J. Fritzmann, W. Dietmaier, F. Rodel, L. Klein-Hitpass, A.F. Kovacs, C. Doring, M.L. Hansmann, W.K. Hofmann, M. Kunkel, C. Brochhausen, K. Engels, B.M. Lippert, W. Mann, R.H. Stauber, The survivin isoform survivin-3B is cytoprotective and can function as a chromosomal passenger complex protein. Cell Cycle 6, 1502–1509 (2007)
H. Caldas, L.E. Honsey, R.A. Altura, Survivin 2alpha: a novel Survivin splice variant expressed in human malignancies. Mol. Cancer 4, 11 (2005)
Y. Xu, F. Fang, G. Ludewig, G. Jones, D. Jones, A mutation found in the promoter region of the human survivin gene is correlated to overexpression of survivin in cancer cells. DNA Cell Biol. 23, 527–537 (2004)
J.S. Jang, K.M. Kim, K.H. Kang, J.E. Choi, W.K. Lee, C.H. Kim, Y.M. Kang, S. Kam, I.S. Kim, J.E. Jun, T.H. Jung, J.Y. Park, Polymorphisms in the survivin gene and the risk of lung cancer. Lung Cancer 60, 31–39 (2008)
A.A. Borbely, M. Murvai, K. Szarka, J. Konya, L. Gergely, Z. Hernadi, G. Veress, Survivin promoter polymorphism and cervical carcinogenesis. J. Clin. Pathol. 60, 303–306 (2007)
W.H. Majoros, U. Ohler, Spatial preferences of microRNA targets in 3′ untranslated regions. BMC Genomics 8, 152 (2007)
L.M. Veenendaal, O. Kranenburg, N. Smakman, A. Klomp, I.H. Borel Rinkes, P.J. van Diest, Differential Notch and TGFbeta signaling in primary colorectal tumors and their corresponding metastases. Cell. Oncol. 30, 1–11 (2008)
W.E. Mesker, G.J. Liefers, J.M. Junggeburt, G.W. van Pelt, P. Alberici, P.J. Kuppen, N.F. Miranda, K.A. van Leeuwen, H. Morreau, K. Szuhai, R.A. Tollenaar, H.J. Tanke, Presence of a high amount of stroma and downregulation of SMAD4 predict for worse survival for stage I-II colon cancer patients. Cell. Oncol. 31, 169–178 (2009)
H. Kawasaki, M. Toyoda, H. Shinohara, J. Okuda, I. Watanabe, T. Yamamoto, K. Tanaka, T. Tenjo, N. Tanigawa, Expression of survivin correlates with apoptosis, proliferation, and angiogenesis during human colorectal tumorigenesis. Cancer 91, 2026–2032 (2001)
L.F. Fan, W.G. Dong, C.Q. Jiang, Q. Qian, Q.F. Yu, Role of Hypoxia-inducible factor-1 alpha and Survivin in colorectal carcinoma progression. Int. J. Colorectal Dis. 23, 1057–1064 (2008)
S. Lassmann, L. Tang, M. Capanu, T. Brabletz, A. Schopflin, A. Zur Hausen, M. Gonen, N. Kemeny, J. Shia, D. Klimstra, M. Werner, Predictive molecular markers for colorectal cancer patients with resected liver metastasis and adjuvant chemotherapy. Gastroenterology 133, 1831–1839 (2007)
S. Rozen, H. Skaletsky, Primer3 on the WWW for general users and for biologist programmers. Methods Mol. Biol. 132, 365–386 (2000)
A.G. Antonacopoulou, P.D. Grivas, L. Skarlas, M. Kalofonos, C.D. Scopa, H.P. Kalofonos, POLR2F, ATP6V0A1 and PRNP expression in colorectal cancer: new molecules with prognostic significance? Anticancer Res. 28, 1221–1227 (2008)
P.D. Grivas, A. Antonacopoulou, V. Tzelepi, G. Sotiropoulou-Bonikou, Z. Kefalopoulou, A.G. Papavassiliou, H. Kalofonos, HER-3 in colorectal tumourigenesis: from mRNA levels through protein status to clinicopathologic relationships. Eur. J. Cancer 43, 2602–2611 (2007)
K. Suga, T. Yamamoto, Y. Yamada, S. Miyatake, T. Nakagawa, N. Tanigawa, Correlation between transcriptional expression of survivin isoforms and clinicopathological findings in human colorectal carcinomas. Oncol. Rep. 13, 891–897 (2005)
F. Vegran, R. Boidot, C. Oudin, J.M. Riedinger, S. Lizard-Nacol, Distinct expression of Survivin splice variants in breast carcinomas. Int. J. Oncol. 27, 1151–1157 (2005)
S. Lankiewicz, E. Rother, S. Zimmermann, C. Hollmann, F. Korangy, T.F. Greten, Tumour-associated transcripts and EGFR deletion variants in colorectal cancer in primary tumour, metastases and circulating tumour cells. Cell. Oncol. 30, 463–471 (2008)
S. De Maria, G. Pannone, P. Bufo, A. Santoro, R. Serpico, S. Metafora, C. Rubini, D. Pasquali, S.M. Papagerakis, S. Staibano, G. De Rosa, E. Farina, M. Emanuelli, A. Santarelli, M.A. Mariggio, L. Lo Russo, L. Lo Muzio, Survivin gene-expression and splicing isoforms in oral squamous cell carcinoma. J. Cancer Res. Clin. Oncol. 135, 107–116 (2009)
T. Zhang, T. Otevrel, Z. Gao, Z. Gao, S.M. Ehrlich, J.Z. Fields, B.M. Boman, Evidence that APC regulates survivin expression: a possible mechanism contributing to the stem cell origin of colon cancer. Cancer Res. 61, 8664–8667 (2001)
N. Zhu, L. Gu, H.W. Findley, F. Li, M. Zhou, An alternatively spliced survivin variant is positively regulated by p53 and sensitizes leukemia cells to chemotherapy. Oncogene 23, 7545–7551 (2004)
M. Gazouli, N. Tzanakis, G. Rallis, G. Theodoropoulos, I. Papaconstantinou, A. Kostakis, N.P. Anagnou, N. Nikiteas, Survivin -31 G/C promoter polymorphism and sporadic colorectal cancer. Int. J. Colorectal Dis. 24, 145–150 (2009)
J.G. Kalliakmanis, C. Kouvidou, C. Latoufis, G. Kouvatseas, D. Anagnostakis, G. Papatheodoridis, J. Koskinas, A. Archimandritis, Survivin expression in colorectal carcinomas: correlations with clinicopathological parameters and survival. Dig. Dis. Sci. 55, 2958–2964 (2009)
P.N. Span, V.C. Tjan-Heijnen, J.J. Heuvel, J.B. de Kok, J.A. Foekens, F.C. Sweep, Do the survivin (BIRC5) splice variants modulate or add to the prognostic value of total survivin in breast cancer? Clin. Chem. 52, 1693–1700 (2006)
K. Komuro, M. Tada, E. Tamoto, A. Kawakami, A. Matsunaga, K. Teramoto, G. Shindoh, M. Takada, K. Murakawa, M. Kanai, N. Kobayashi, Y. Fujiwara, N. Nishimura, J. Hamada, A. Ishizu, H. Ikeda, S. Kondo, H. Katoh, T. Moriuchi, T. Yoshiki, Right- and left-sided colorectal cancers display distinct expression profiles and the anatomical stratification allows a high accuracy prediction of lymph node metastasis. J. Surg. Res. 124, 216–224 (2005)
R. Kannangai, J. Wang, Q.Z. Liu, F. Sahin, M. Torbenson, Survivin overexpression in hepatocellular carcinoma is associated with p53 dysregulation. Int. J. Gastrointest. Cancer 35, 53–60 (2005)
B. Ryan, N. O’Donovan, B. Browne, C. O’Shea, J. Crown, A.D. Hill, E. McDermott, N. O’Higgins, M.J. Duffy, Expression of survivin and its splice variants survivin-2B and survivin-DeltaEx3 in breast cancer. Br. J. Cancer 92, 120–124 (2005)
F. Li, J. Yang, N. Ramnath, M.M. Javle, D. Tan, Nuclear or cytoplasmic expression of survivin: what is the significance? Int. J. Cancer 114, 509–512 (2005)
W.S. Moon, A.S. Tarnawski, Nuclear translocation of survivin in hepatocellular carcinoma: a key to cancer cell growth? Hum. Pathol. 34, 1119–1126 (2003)
S. Peroukides, V. Bravou, A. Alexopoulos, J. Varakis, H. Kalofonos, H. Papadaki, Survivin overexpression in HCC and liver cirrhosis differentially correlates with p-STAT3 and E-cadherin. Histol. Histopathol. 25, 299–307 (2010)
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper is a reprint from ‘The survivin -31 snp in human colorectal cancer correlates with survivin splice variant expression and improved overall survival, Anna G Antonacopoulou, Konstantina Floratou, Vasiliki Bravou, Anastasia Kottorou, Fotinos-Ioannis Dimitrakopoulos, Stella Marousi, Michalis Stavropoulos, Agelos K Koutras, Chrisoula D Scopa, Haralabos P Kalofonos’ originally published in Analytical Cellular Pathology/Cellular Oncology, Volume 33, number 5–6, 2010, pp. 177–189, IOS Press.
An erratum to this article can be found at http://dx.doi.org/10.1007/s13402-011-0057-1
Rights and permissions
About this article
Cite this article
Antonacopoulou, A.G., Floratou, K., Bravou, V. et al. The survivin -31 snp in human colorectal cancer correlates with survivin splice variant expression and improved overall survival. Cell Oncol. 34, 381–391 (2011). https://doi.org/10.1007/s13402-011-0038-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13402-011-0038-4