
Abstract
In recent years, the continuous development of innovative nanopharmaceuticals is expanding their biomedical and clinical applications. Nanomedicines are being revolutionized to circumvent the limitations of unbound therapeutic agents as well as overcome barriers posed by biological interfaces at the cellular, organ, system, and microenvironment levels. In many ways, the use of nanoconfigured delivery systems has eased challenges associated with patient differences, and in our opinion, this forms the foundation for their potential usefulness in developing innovative medicines and diagnostics for special patient populations. Here, we present a comprehensive review of nanomedicines specifically designed and evaluated for disease management in the pediatric population. Typically, the pediatric population has distinguishing needs relative to those of adults majorly because of their constantly growing bodies and age-related physiological changes, which often need specialized drug formulation interventions to provide desirable therapeutic effects and outcomes. Besides, child-centric drug carriers have unique delivery routes, dosing flexibility, organoleptic properties (e.g., taste, flavor), and caregiver requirements that are often not met by traditional formulations and can impact adherence to therapy. Engineering pediatric medicines as nanoconfigured structures can potentially resolve these limitations stemming from traditional drug carriers because of their unique capabilities. Consequently, researchers from different specialties relentlessly and creatively investigate the usefulness of nanomedicines for pediatric disease management as extensively captured in this compilation. Some examples of nanomedicines covered include nanoparticles, liposomes, and nanomicelles for cancer; solid lipid and lipid-based nanostructured carriers for hypertension; self-nanoemulsifying lipid-based systems and niosomes for infections; and nanocapsules for asthma pharmacotherapy.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the past decade, children’s medicines have been a major focus of attention and effort globally. As a result, the US Food and Drug Administration (US FDA) and European Medicines Agency (EMA) continued encouraging pharmaceutical companies to evaluate drugs for administration in pediatric patients [1,2,3]. The reason was related to the lack of pediatric drug research and developments, which have triggered serious problems such as under or overdosing and long-term adverse effects [4]. The pathophysiology of diseases in children and adolescents may differ from those of adults; hence, they are not “small adults,” and age-appropriate medicines are required for them [5, 6]. It is necessary to adapt biopharmaceutical methods to make sure that in vivo/in vitro predictions and drug development processes are relevant to pediatric patients because of the differences in their anatomy and physiology [7, 8].
Typically, pediatric doses are calculated by allometric scaling of adult doses based on the ratio of body weight and surface area. To determine an effective and safe pediatric dose, a simple proportional reduction of the adult dose may not be sufficient because of the remarkable differences in drug absorption, distribution, metabolism, and excretion patterns plus pharmacological effects [9, 10]. For instance, gastric pH may be changed from 1 to 8 between birth and the age of 3 years old, and intestinal transit time can be longer in neonates compared to adults due to their decreased intestinal motility. These differences can affect the overall drug absorption kinetics in children [11, 12]. Furthermore, drug distribution is continually influenced by other factors such as adipose tissue, total body water, and plasma protein binding during the first years of life. Extracellular water reduces from 40 to 20% during the first 4 months of life and the percentage of body fat grows in the same duration. Besides, a reduction in protein binding which is a result of a decline in plasma protein levels can have effects on the drug distribution [13, 14]. The pediatric population also has individual drug metabolism, which stems from the expression of some enzymes such as CYP3A5, CYP2B6, and CYP2C19 [15]. In children, the kidney’s processes of excretion (i.e., tubular secretion, reabsorption, and glomerular filtration) are generally influenced by renal blood and plasma flow, which rise with age as cardiac output increases and peripheral vascular resistance decreases [16, 17].
The development of modified-release drug delivery systems, such as nanomedicines for use by the pediatric population, is one of the age-appropriate formulation strategies, according to the European Pediatric Formulation Initiative (EuPFI). The use of nanotechnology-based platforms can be beneficial for preparing modified release formulations that can enhance pediatric biopharmaceutics [18, 19]. Relative to conventional drug products, nanomedicines have several potential advantages which can include, formulation stabilization, active or passive targeted drug delivery to specific tissues, controlled drug release and regulated encapsulation, improved solubility for hydrophobic drugs, reduced toxicity, limited exposure of drug molecules to potentially harmful physiological conditions (e.g., enzymatic degradation), and prevention of premature clearance [20, 21]. These can lead to better therapeutic effects and can improve drug target site accumulation and biodistribution plus diagnostic and therapeutic efficacy in vivo.
Additionally, nanostructured drug carriers may reduce the accumulation of drugs and imaging agents in healthy tissues, as well as decrease the frequency and seriousness of side effects, and extend circulation time by reducing renal excretion and hepatic degradation. There are several biological, chemical, physical, and clinical barriers related to the unsuccessful delivery of drugs to pathological sites that can be overcome using nanomedicines which are capable of enhancing the therapeutic index of low molecular weight agents in cancer, infections, inflammatory disorders, and other life-threatening diseases [21,22,23,24,25]. Therefore, nanomedicines can be used for the treatment, prevention, and diagnosis of several diseases, which can enhance the quality of a pediatric patient’s life [26]. Although nanomedicines have all the benefits mentioned earlier, they also have some demerits such as drug fusion and leakage from encapsulated nanoformulations, short half-life, low capacity for loading drugs, high water content in nanocarrier dispersions, burst release of encapsulated drugs, high production costs, lack of regulatory guidelines, and limited information on toxicity profiles [27, 28].
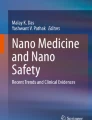
Considering what nanomedicines have to offer as it relates to effective pharmacotherapy, we believe they can serve as useful, specialized platforms for the delivery of bioactive agents in children. We therefore focused this review on reported applications of nanomedicines to manage varying diseases unique to the pediatric population. Different pediatric diseases treated by nanomedicines (e.g., cancers, infections, asthma, and human immunodeficiency virus) and different types of pediatric nanomedicines such as nanoparticles, micelles, and nanostructured lipid carriers were discussed. Besides, the advantages and disadvantages of these nanosystems were summarized. Research articles evaluated in this review were gathered by searching Google Scholar, Science Direct, Scopus, and PubMed using different relevant keywords, including “nanomedicines,” “nanoparticles,” pediatric/paediatric nanomedicine,” “pediatric nanoformulation,” “pediatric nanodrugs,” “pediatric nanodelivery.” The outline of this review manuscript is illustrated in Fig. 1.

A schematic displaying the different sections contained in this write-up
Pediatric nanomedicine — brief background and current trend
As already mentioned, pediatric organs and systems develop gradually after birth, and children differ from adults metabolically and biologically. Hence, when diseases affect both children and adults, nanomedicines need to be adjusted for pediatric use, demanding clinical trials in children to develop new pharmaceutical formulations. Additionally, specifically tailored nanomedicines need to be fabricated for diseases affecting children or causing greater harm to them. Nevertheless, both academic and industry researchers hesitate to study these age-specific nanodrug delivery systems because of the fragmented pediatric market complexities and the difficulty associated with conducting clinical trials in individuals within this age group [9, 29]. Therefore, there are limited nanotechnology-based commercialized pediatric drug formulations. Doxil®, known as liposomal doxorubicin, was the first US FDA-approved nanodrug and this occurred in 1995. This doxorubicin formulation is able to target tumors passively, and it could be combined with other drugs to treat Hodgkin lymphoma [30]. Further studies showed that the pharmacokinetics of Doxil® in the pediatric population differed from adults and its half-life was low in pediatric patients. Similarly, other liposomal formulations, which are US FDA-approved for adults, such as DaunoXome® (daunorubicin) and SPI-77 (liposomal cisplatin), were evaluated in the pediatric population and their pharmacokinetics were different from adults [19].
Although the application of nanomedicines for children is recommended by the EuPFI, there is a lack of research on how nanotechnology, which is effective for adults, can also be used for pediatric-specific drug delivery. The pediatric population is considered a smaller size market compared to adults and this presents challenges to nanotechnology researchers and innovators. Although around 27% of the global population consists of children, only 17% of all clinical trials registered with the World Health Organization (WHO) are dedicated to the pediatric population. Regarding the industry funding preference for adult diseases, regulatory limitations in the development of nanomedicines, and a tendency to use adult data, have led to the lack of new treatments and formulations for complex pediatric diseases [19]. In Table 1, some commercialized nanomedicines that have been evaluated for pediatric patients are summarized.
Commonly applied routes of administration in pediatric pharmacotherapy
Based on pediatric preferences, various routes of administration can be used for them, some of which are oral, nasal, ocular, otic, parenteral, dermal and transdermal, rectal, and pulmonary drug delivery with the most preferred being the oral channel [37].
The oral route of delivery is known as the most popular channel of drug administration for patients of all ages because of its great benefits, including the convenience of drug administration, patient compliance, and non-invasiveness [38,39,40]. However, swallowing difficulties (dysphagia) occur in children more than adults and this can influence dosage form suitability and choice [41, 42]. Even though dysphagia can affect healthy children at different ages, it is more likely to occur in children with prematurity, cardiopulmonary, neuromuscular, and gastrointestinal tract disorders, as well as anatomical anomalies of the upper aerodigestive tract [43, 44].
Pediatric patients typically have varied preferences when the need to consume medications arises and this could be due to their age, personality differences, specific physiology, and anatomy. As part of this administration route, pediatric formulations will have extra critical quality attributes (CQAs), including palatability, organoleptic characteristics, dosing flexibility, easy administration, safety, stability, and suitable pharmacokinetics [39, 45]. Solid dosage forms might be administered to school-aged children, but liquid dosage forms are preferable for children under 5 years old due to their comfortable dose adjustment and swallowing. Tablets and capsules, which have dose accuracy, are popular among pediatric populations over 6 years old owing to their taste masking [46].
It is believed that nanodrug delivery systems can carry drugs, both hydrophobic and hydrophilic, through the gastrointestinal tract (GIT). These systems not only can protect the therapeutic agents from harsh GIT environments, but they could also soar intestinal absorption of the drugs. Furthermore, controlled release or accumulation of drugs in certain cells can be achieved by employing these systems [21, 47, 48].
In 2020, cefpodoxime proxetil (CFP) was loaded into lyotropic liquid crystalline nanoparticles (LLCNs) system to mitigate the nasty taste of the drug and enhance the ease of administration for children [49]. Moreover, a liquid formulation of nanoparticles containing saquinavir, which is a liposoluble antiretroviral drug, was prepared to enhance stability and taste masking for the pediatrics [50]. In 2021, a 6-mercaptopurine-loaded oral nanoliquid formulation was prepared for acute lymphoblastic leukemia, which is known as the most common hematologic malignancy in the pediatric population [51]. In another study, nanoparticle-based orodispersible palatable formulations were developed as drug carriers for the combination of ritonavir (RTV) and lopinavir (LPV), which are unpalatable and low water-soluble drugs [52].
Potential limitations and challenges
Although nanotechnology benefits from great potential and may provide many new possibilities for pediatric medicines, it also increases concerns about their health risks. Since nanomedicines can affect pediatric health and wellbeing, assessing their safety profile is essential. Research investigations have revealed the need to exercise caution with the rapidly growing interests in the use of nanomedicines and examples include studies examining their neurotoxicity and effects on the health of children, indicating the need to understand their potential risks [53]. Pediatric drug development has been significantly influenced by numerous factors, including the inadequacy of approved active pharmaceutical ingredients and excipient safety data for this patient population. Excipient safety profile information is one of the obligatory requirements of regulatory organizations to avoid inappropriate or toxic ingredients for the pediatric population. Hence, excipients, which are approved as food grade, generally recognized as safe or as inactive ingredients are typically used in the preparation of pharmaceutical products. Furthermore, there is a limitation in the usage of organic solvents, particularly chlorinated solvents in the formulation method of drug products like this. For preventing the use of any potentially toxic or unsuitable additives for the formulation of pediatric medicines, it is one of the mandatory requirements of regulatory agencies to know the excipient safety profile. To ensure that prepared formulations are safe for use in children, all excipients used are either categorized as generally recognized as safe or are used as inactive ingredients [34].
Besides, the toxicity and adverse reactions of formulations can be challenging in pediatric drug development. More importantly, pediatric patients, depending on their age group, are unable to communicate effectively so verifying the onset of certain side effects may be challenging. Although pharmaceutical companies can access several regulatory documents that can guide them through the study design and conduct for adults, there are many unanswered questions regarding the development of pediatric drugs due to their complexity [54]. Furthermore, traditional animal models, such as mice and rats, have different organogenesis and physiology development from pediatrics and short life spans; thereby, they may not provide reliable preclinical pharmacokinetic/pharmacodynamic prediction or toxicity evaluations [55].
Children’s cancer is a particular concern because in vivo preclinical evidence is sometimes unable to replicate the disease or the age differences correctly, while late toxicities are not assessed [56]. In therapeutic areas such as rheumatology, oncology, allergy, and psychiatry where patients are being treated over the long term for chronic diseases or serious illnesses, this is especially significant. The long-term safety of drugs is difficult to evaluate because of the need for long follow-ups, and randomized controlled trials are probably not an appropriate method for studying long-term safety. In contrast, observational studies are more likely to produce results with uncertainty due to selection and recall biases. It can also be challenging to differentiate between drug-related and condition-related side effects when evaluating long-term safety [57].
Moreover, there are ethical issues in pediatric clinical trials, such as volunteers’ age and legal consent provided by their parents to participate, which make the process more difficult compared to adult clinical trials. For instance, liposome drug delivery systems biocompatibility in adults is recognized, and several nanoformulations, which are prepared for adult patients, have attained clinical trials. However, there is limited information on their safety in the pediatric population [58]. Besides, the pediatric population is heterogeneous, as it comprises various subgroups, including preterm newborns, term newborns, infants and toddlers, children, and adolescents. As a result, each developmental phase has its own physiologic factors and pharmacokinetic outcomes, which are discussed earlier, posing a challenge to pharmacological studies in pediatric clinical assessment [59]. Hence, the absence of regulatory clarity on quality and specification limits, small market value, shortage of appropriate in vivo models for different pediatric ages, and lack of pharmacokinetic data place limitations on nanoformulation development for minors [60].
Categories of nanomedicines explored for pediatric use
Nanoemulsion
Nanoemulsions are defined as stable dispersions of immiscible liquids (oil-in-water or water-in-oil) that are stabilized by surfactants. Their droplet sizes are typically smaller than 500 nm. These emulsions have applications in various dosage forms, such as creams, sprays, and gels, that can be administered through different routes, such as oral, pulmonary, transmucosal, transdermal, intravenous, and ocular. Nanoemulsions might enhance solubilization capacity and kinetic stability compared to traditional emulsions which are valuable in drug delivery. There are several advantages of using nanoemulsions, some of which are drug dissolution rate increase, bioavailability improvement, especially for hydrophobic drugs, target organ therapy, taste masking, and first-pass metabolism bypass [61, 62]. In 2022, an oil-in-water nanoemulsion of tadalafil, which is practically insoluble in water, was prepared for pediatric pulmonary hypertension treatment by using a nebulizer. This formulation not only improved drug solubility, but it was also safe in both in vitro (A549 cell line) and in vivo (male Sprague–Dawley rats) evaluations. The viscosity of liquid-optimized formulations was suitable, and they were stable after the nebulization [63]. In 2023, an oil-in-water nanoemulsion of coenzyme Q10 (CoQ10) was developed for the infant formula supplement to treat newborns suffering from CoQ10 deficiency. Playing a vital role in numerous essential cellular processes, CoQ10 is a crucial element of the mitochondrial respiratory chain. Apart from its primary function within this respiratory chain, CoQ10 is recognized as an exceptionally potent natural lipid antioxidant which can enable it to reduce the harmful effects of reactive oxygen species (ROS), regenerate other antioxidants like vitamins E and C, protect cellular membranes from lipid peroxidation, and ultimately prevent cell death. Neonates experiencing a deficiency in CoQ10 often exhibit severe hypotonia and hyporeactivity which might lead to difficulties in newborns’ proper sucking during feeding because of exhaustion. The study indicated that the CoQ10 nanoemulsion was stable for 90 days, and it showed no cytotoxicity in vitro using the macrophage-like RAW 264.7 cells. Moreover, the formula containing CoQ10 nanoemulsion led to quicker and enhanced absorption of coenzyme Q10 in comparison to the powder-enhanced formula [64].
Nanosuspension
The liquid nanosuspension drug delivery system is a fluid colloidal dispersion of dissolution medium, stabilizers, and drug nanoparticles (smaller than 1000 nm). Since nanosuspensions can provide nanosized particles of drugs, they can improve the solubility and bioavailability of pharmaceutical agents. Likewise, formulation and scaling up of nanosuspension are straightforward [65]. Perween and colleagues developed an oral nanosuspension of mefenamic acid for pediatric administration by using hydroxypropyl methylcellulose (HPMC). Mefenamic acid (MA), which is known as a nonsteroidal anti-inflammatory drug (NSAID), has low water solubility and, consequently, poor oral bioavailability, which can lead to a challenging formulation. This study indicated that the more concentration of surfactant was used, the higher drug release was observed. Also, the drug’s solubility was increased, and the formulation was stable [66].
Dendrimers
Dendrimers, which are polymeric macromolecules, have the shape of spheres with central cores surrounded by multiple layers. Dendrimers benefit from the amphiphilic hollow structure which makes them ideal for incorporating therapeutic agents. Additionally, their surfaces are able to be modified by using biomolecules such as antibodies, targeting ligands, nucleic acids, and drugs. There are different types of dendrimers, one of which is polyamidoamine (PAMAM) dendrimers. They are generally spherical and highly branched polymers, and their size and surface can be regulated during synthesis. Dendrimers as drug carriers can enhance drug solubility and bioavailability, decline toxicity, and mitigate the unpleasant taste of drugs [67, 68]. In 2018, oral dosage forms of dendrimer-N-acetyl-l-cysteine conjugates (NAC) were developed to treat pediatric neuroinflammation. As NAC’s oral bioavailability is low, Capmul® MCM (glyceryl caprylate) was used in the formulation as a penetration enhancer. This study demonstrated that prepared formulation benefits from stability in gastrointestinal fluids, in vitro transepithelial permeability, and in vivo appropriate oral absorption [69].
Nanofibers
A collection of nanofibers, defined as fibers with 100 nm diameter or lower, is known sas a mat or a mesh. The mat could be formed of regular patterns of oriented fiber (woven) or randomly oriented fibers (non-woven). The nanofibers can have similar compositions, multi-component structures, or core/shell structures in the system. Nanofibers can be produced using several methods; for instance, electrospinning is one of the common and robust techniques [70]. Nanofibers can potentially protect the drug from decomposition within the body to reach the target site. Hence, they could be exploited to develop various dosage forms such as oral, transmucosal, ocular, topical, and transdermal [71]. Nanofibers can be composed of natural and synthetic polymers which may affect drug release properties [72]. Besides, they benefit from good stability and a high drug-loading capacity [73]. In 2015, ultra-rapidly dissolving orodispersible films containing iodine-loaded nanofibers were prepared for pediatrics to prevent or treat iodine deficiency which can cause mental impairment. The study revealed that the novel formulation had good mechanical properties and fast disintegration and dissolution rate in vitro [74]. In 2016, electrospun polymeric nanofibers of SN-38, known as an active metabolite of irinotecan and anti-solid tumor agent, were developed for pediatric uses after resection surgery. As SN-38 has poor water solubility and a short half-life due to hydrolysis in plasma, nanofibers could be an appropriate option for drug delivery. The experiment demonstrated enhanced survival, long-lasting therapeutic activity, sustained release in vitro, and, more importantly, tumor recurrence control in pediatric patient-derived xenograft in vivo models HSJD-ES-001 and HSJD-NB-005 [75].
Carbon nitride dots (CNDs)
A novel nanocarrier material, carbon nitride dots (CNDs), is a subclass of carbon dots. Their unique characteristics, including nanosized dimensions, high photoluminescence (PL), good water dispersion, nontoxicity, and suitable biocompatibility, make their application in biological and medical research possible [76, 77]. In an investigation, doxorubicin was delivered to pediatric brain tumor cells more efficiently and specifically via nontoxic water-soluble carbon dots conjugated with transferrin. Chemotherapeutic agents can be transported across the blood–brain barrier (BBB) and into the brain parenchyma by utilizing transferrin receptors on the BBB. Since brain tumor cells require a significant amount of iron, they express more transferrin receptors and can, therefore, take up more transferrin-bound chemotherapy than normal cells [78]. In 2020, it was shown that a conjugate system using carbon nitride dots (CNDs) as nanocarriers, coupled with a new glioma drug candidate, gemcitabine (GM), is capable of targeting cancerous cells while crossing the BBB, thereby resolving both major difficulties associated with glioblastoma chemotherapy of pediatrics [79].
Polymeric nanoparticles
Polymer-based nanoparticles (NPs), whose size/diameter is around 10–1000 nm, can be employed as a drug delivery system due to their ability to increase drugs’ half-life and solubility and provide controlled/sustained release characteristics. Moreover, controlled biodistribution and reduced toxicity of drugs can be achieved by employing stimuli-responsive nanoparticles [80]. Polymeric nanoparticles can improve drug bioavailability or targeted delivery at the site of action. Polymeric NPs have versatile applications in drug delivery, especially for oral administration. They may not only protect drugs from pH changes, efflux pumps, and enzymes but also improve stability in the gastrointestinal fluids. Benefiting from small-size particles, NPs may enhance contact with epithelial surfaces and improve drug uptake. Surfaces of polymer-based NPs can be modified by using various attachments such as ligands like antibodies. Besides, diverse therapeutic agents, including small molecules and nucleic acids, can be encapsulated in NPs [81, 82]. Polymeric nanoparticles have been broadly employed as viable templates for drug delivery systems intended for pediatric use (Table 2).
Solid lipid nanoparticles (SLNs)
Solid lipid nanoparticles, which are usually made from biodegradable lipidic ingredients, can be used as carriers for different types of therapeutic agents such as small and large drug molecules (whether hydrophilic or hydrophobic drugs), DNA or siRNA, and antigens. Although these nanoparticles may retain hydrophobic molecules in their core and provide a controlled release for drugs, they have limitations in terms of loaded drug capacity. Besides, SLNs can offer targeted drug delivery, appropriate physical stability, and drug protection in harsh environments [94]. In 2017, SLNs containing hydrochlorothiazide-in cyclodextrins were developed for pediatric hypertension treatment. As hydrochlorothiazide is known as a diuretic drug with low solubility and permeability, cyclodextrins can enhance their aqueous solubility, stability, and bioavailability. It was demonstrated that using cyclodextrins in this liquid oral formulation could improve drug entrapment efficiency in SLNs and in vitro drug release. More importantly, the novel formulation showed a higher diuretic therapeutic effect in male Sprague–Dawley rats (in vivo) [95].
Exosomes
Exosomes, classified as nanoparticles based on their size (30–100 nm), are known as extracellular vesicles containing proteins, bilayer lipids, and RNA/miRNAs. In contrast to nanoparticles prepared in vitro, exosomes are released endogenously from cells which are non-cytotoxic and can deliver substances to the target cells specifically based on their modifications. Exosomes have a wide range of advantages including improved permeability and retention (EPR) effect, passive targeting, and specific target therapy [96]. In 2020, an exosomal miR-181a inhibitor was prepared to suppress pediatric lymphatic leukemia growth. The study demonstrated that the novel formulation silenced the exosomal miR-181a, which derived from the serum of pediatric acute lymphocytic leukemia/conditioned medium of acute lymphocytic leukemia cell lines and induced the proliferation of leukemic cells in vitro [97].
Gold nanoparticles
Gold nanoparticles (Au NPs), whose sizes are between 1 and 150 nm, could be synthesized by using reducing agents to chemically reduce chloroauric acid. Their specific features such as nanosized particles, customizable surface, high X-ray absorption, and UV absorbance make them appropriate for drug delivery and imaging purposes. Modifying surfaces of Au NPs can enhance the selective targeting of tissue or cells through systemic delivery, leading to decreased antitumor drug treatment dosage, normal cell toxicity, and side effects. Moreover, biocompatible coatings of Au NPs can increase stability in physiological conditions [98, 99]. In 2019, an AuNP-based immunosensor was developed for detecting dehydroepiandrosterone sulfate (DHEAS), which is known as a biomarker of pediatric adrenocortical carcinoma, in blood plasma samples. The immunosensor was prepared by using a modified oxidized glassy carbon electrode with arginine-functionalized gold nanoparticles and anti-DHEA IgM antibodies. The experiment demonstrated that the novel formulation benefited from appropriate sensitivity, accuracy, stability, and DHEAS detection specificity. Besides, a statistical difference was not observed between the result of DHEAS quantification by using prepared formulation in real patient plasma samples and reference chemiluminescence assay [100].
Micelles
Micelles as nanostructures are composed of amphiphilic molecules within aqueous solutions. Micelles are self-assembled, and they have a core–shell structure consisting of both hydrophobic and hydrophilic sections. Their size is typically from 5 to 100 nm in diameter and can be varied based on the type of head groups and length of the alkyl chain. Micelles may have applications in drug delivery because of their ability to increase drug solubility, enhance circulation time, target drug delivery, and reduce toxicity. Moreover, they are capable of gene delivery and loading a wide range of insoluble therapeutic agents [101]. In 2018, glucosylated polymeric micelles containing dasatinib, which is a tyrosine kinase inhibitor and poorly water-soluble drug, were developed for targeted therapy in pediatric patient-derived sarcomas in murine models (in vivo). The study indicated that glucosylation of polymeric micelles increased the drug encapsulation and bioavailability in vitro (Rh30 cells). Besides, the formulation reduced cytotoxicity and enhanced survival in vivo [102]. In 2021, pitavastatin-loaded polymeric micelles coated by silica were prepared for targeted therapy in pediatric patient-derived glioblastoma. Pitavastatin, which is a hydrophobic drug, has an anti-glioblastoma multiforme effect. This drug was loaded in silica-coated mixed-polymeric micelles for targeting integrin in BBB and cancerous cells. The enhancement of drug uptake and the antiproliferative activity within pediatric patient-derived cells in vitro were shown in this study [103]. In 2023, anti-CD276 antibodies were conjugated on the polymeric micelles’ surface for the purpose of targeting brain tumor in pediatrics. In this study, ligand-installed micelles were employed due to their high stability. As CD276/B7-H3 expression could be high on the membrane of medulloblastoma (MB) cells, targeting them can increase ligand-installed micelles’ cellular uptake. The experiment showed that using an anti-CD276 antibody as a ligand increased intracellular delivery to MB cells with high CD276-expressing in vitro (DAOY (HTB-186) cell line). Besides, the more antibodies which micelles had on their surfaces, the higher cellular uptake was observed [104].
Nanostructured lipid carrier
Nanostructured lipid carriers (NLCs) consist of a solid lipid matrix composed of solid lipids and liquid lipids mix, plus surfactants as an aqueous phase. Mixing the liquid lipids and solid lipids can provide a matrix, whose crystal lattice is not perfect, and the imperfect core of solid matrix and amorphous matrix. There are three different types of NLCs, such as imperfect, amorphous, and multiple structures. This specific structure of NLCs leads to the solid form of NLCs at room temperature, physical stability enhancement, and drug leakage decrease over the storage time. Moreover, these carriers have a larger capacity for loading drugs despite SLNs having limited capacity [105,106,107]. In 2018, a hydrochlorothiazide (HCT)-cyclodextrin combination was loaded to NLCs to obtain an oral liquid dosage form for pediatrics. Cyclodextrin can improve the aqueous solubility of drugs such as HCT, whose solubility is low. The study showed that using cyclodextrin can enhance the entrapment efficiency of loaded drugs in NLCs and drug release. Moreover, the novel formulation had higher therapeutic effects rather than either HCT aqueous suspension or HCT-loaded NLC (without cyclodextrin) [108].
Nanocapsules
Nanocapsules consist of polymeric membranes (natural or synthetic) surrounding a core which can be aqueous or nonaqueous. This system is categorized as a submicroscopic colloidal drug carrier and its size ranges from 5 to 1000 nm. The core cavity incorporates therapeutic agents, which may be liquid or solid in nature and protects them from chemical or biological degradation. Nanocapsules are one of the most interesting drug delivery systems due to their controlled release and targeted drug delivery capabilities. Besides, they can potentially enhance drug stability and bioavailability significantly [109, 110]. In 2006, nanocapsules of spironolactone, a low-water solubility diuretic, were prepared by using polycaprolactone (PCL) polymer and oils for pediatric pharmacotherapy. It was reported that prepared formulations were stable for 6 months and drug release in simulated gastric medium was fast. Furthermore, this liquid formulation benefited from the high concentration of the drug which was suitable for pediatric administration [111]. In 2018, the reconstitutable powder of chitosan-coated nanocapsules of phenytoin (PHT) was prepared by using the spray drying method. PHT, which is practically insoluble in water, can be used as epilepsy treatment by blocking the voltage-dependent sodium channels. The experiment indicated that the chitosan-coated formulation enhanced the powder’s dispersibility in water. Besides, the formulation, after reconstitution, had good gastrointestinal stability. More importantly, the final oral liquid formulation showed a better anticonvulsant effect in mice which have induced seizures by pilocarpine [112]. Wirsching and colleagues developed ovalbumin nanocapsules of resiquimod (R848) coupled to polyethylene glycol (PEG) (OVA-PEG-R848) to stimulate neonatal dendritic cells. R848 is known as a toll-like receptor (TLR)7/8 agonist, which is capable of activating the innate immune system. The study demonstrated that ovalbumin nanocapsules simulation enhanced the activation marker expression and secretion of pro-inflammatory cytokines in neonatal dendritic cells [113].
Nanosponges
Nanosponges are porous, solid structures at the nanoscale (200–300 nm), consisting of crosslinked polymers, and have been extensively studied for targeted therapy and sustained drug release in cancer treatment. These structures are biocompatible, highly stable, and exhibit low cytotoxicity and side effects, which can make them suitable carriers for biomedical applications. They can be synthesized through various techniques, such as molecularly imprinted approaches, and can be functionalized by using silver nanowires and materials like carbon nanotubes. Moreover, they can improve drug penetration through the skin and enhance trans-epidermal drug delivery. However, pertinent factors related to the optimal performance of nanosponges such as pharmacokinetics, biocompatibility, bioavailability, histopathological changes, drug adsorption and encapsulation processes, and cytotoxicity should be evaluated systematically in clinical studies [114]. In 2015, a dried suspension of controlled-released gabapentin-loaded nanosponges was prepared for reconstitution for pediatric uses. Gabapentin has a bitter taste and a short half-life under biological conditions, and these were improved by using β-cyclodextrin nanosponge delivery systems. It was demonstrated that drug release was extended up to 12 h, and the nasty taste of the drug was masked. Furthermore, in vivo evaluation showed an increased bioavailability of the controlled-released delivery system in male Wistar rats [115]. In 2020, an oral liquid formulation of griseofulvin-loaded nanosponges, which is a poorly water-soluble drug with an unpleasant taste, was developed with the pediatric population in mind. The prepared β-cyclodextrin formulation had a masked taste, improved drug solubility, and was orally bioavailable as per evaluations conducted in rats [116].
Lipid-based nanovesicles
These nanovesicles are spherically shaped small vesicles that are characterized by a double-layered structure containing lipids. Small unilamellar vesicles or nanovesicles are comprised of a single bilayer structure and their size is typically below 200 nm. The surfaces of vesicles of this nature can be modified by attaching various ligands which can lead to the fabrication of multifunctional systems. Their physicochemical properties (e.g., size, shape/morphology, surface charge, density) significantly influence their functionality and are determined by the method of synthesis plus process variables [117].
Nanoliposomes
Liposomes, which were discovered in the 1960s, comprise an aqueous core surrounded by phospholipid bilayers. Their ability to load hydrophilic and lipophilic therapeutic agents makes them appropriate choices for drug delivery. They also can be used for delivering gene medicines, anesthetics, anticancer, antifungal, antibiotics, and anti-inflammatory drugs. Nanoliposomes offer merits such as targeted therapy, surface modification, controlled release, cost-effectiveness, biocompatibility and biodegradability, and improved bioavailability, solubility, and stability during processing and digestion [118,119,120]. In 2009, MEPACT®, a liposomal form of mifamurtide, was approved by the European Commission for the market throughout the European Union for use as a safe and efficacious postoperative adjuvant to polychemotherapy of young patients, aged 2–30 years old, with non-metastatic, resectable high-grade osteosarcoma post “macroscopically complete surgical resection” [121].
In 2018, alpha lipoic acid (ALA) nanoliposomes of ceftriaxone (CTX) were developed for pediatric use. CTX is one of the cephalosporins, which are the most used antibiotics as initial empiric therapy in serious infection treatment. However, CTX can cause some severe side effects including bladder sludge, nephrolithiasis, and biliary pseudolithiasis, especially in pediatrics. The study demonstrated that alpha lipoic acid could provide a protective effect on ceftriaxone nephrotoxicity. Furthermore, the ALA nanoliposomes of CTX benefit from appropriate percentage entrapment efficiency and extended-release profile [122]. Stewart and colleagues prepared nanoliposomal irinotecan (nal-IRI) and carried out the pharmacokinetic studies on normal and tumor xenograft (derived from a solid tumor of the pediatric patient) mice model. Irinotecan is known as an antineoplastic enzyme inhibitor. The examination showed that using the single dose of nal-IRI maintained the active metabolite of irinotecan in tumors for several days compared to standard irinotecan which typically needs 5–10 days of administration. Therefore, this formulation had the potential to decrease side effects and hospital visits and could be a suitable treatment for pediatric patients [123].
Niosomes
Niosomes, which are the stable bi-layered structure of non-ionic surface-active agents, could be formed by mixing suitable proportions of surfactants and cholesterol together at a point that is higher than the gel liquid transition temperature. This bi-layered structure can encapsulate hydrophobic and/or hydrophilic drugs in their layers and centric hollow spaces, respectively. Besides, hydrophilic agents can be adsorbed to the bilayer surface of niosomes. Niosomes offer numerous advantages over conventional delivery systems, including greater chemical stability, longer shelf life, and enhanced osmotic activity compared to liposomes. The hydrophilic head’s functional group allows for easy surface formation and modification. They are less toxic and more biocompatible due to the absence of charges, are biodegradable without causing immunogenic reactions, and can encapsulate both hydrophilic and hydrophobic drugs. Niosomes can potentially enhance patient compliance, bioavailability, and drug stability and provide targeted, sustained, and controlled release delivery systems. They can be administered via various routes, such as oral, pulmonary, ocular, parenteral, and transdermal. However, the stability of niosomes in aqueous suspension may be challenging due to drug hydrolysis, drug leakage or aggregation [124]. In 2016, transdermal niosomal gel containing simvastatin, whose water solubility and GIT absorption are poor, was developed for treating pediatric dyslipidemia. The in vivo evaluation in rats showed that cholesterol and triglyceride were decreased and the bioavailability of transdermal niosomal simvastatin was higher than in oral suspension [125].
Virosomes
It is known that viruses have several characteristics that make them ideal for drug delivery, including their inherent ability to avoid being recognized by the immune system and their ability to penetrate cells to transfer their genes for self-replication. However, the safety and immunogenicity of viral vectors are being questioned, since they are pathogenic and originate from viruses that were previously encountered via infection [126, 127]. Virosomes are liposome-virus hybrid vesicles composed of lipid membranes and viral envelope proteins which allow cell penetration, escaping from the endosomes, and drug delivery to the cells’ cytoplasm. Virosomes can be used as a carrier for pharmaceutical and biopharmaceutical drugs, vaccines, and adjuvant systems, as they are able to produce long-term immunity against pathogens. However, their stability is low and there are safety concerns about their immunogenicity [117]. In 2009, the safety of Inflexal®V, known as an influenza vaccine, was evaluated in a post-marketing surveillance study in children aged 6 months to 6 years. Inflexal®V was marketed in 1997 for all ages of patients and it was found to be effective and safe in these young individuals [128]. The study showed low intensity localized and systemic adverse events with most symptoms reported being mild to moderate that disappeared after a few days [129]. In another investigation, the long-term immunogenicity effect of Epaxal® Junior, which is a safe and immunogenic virosomal hepatitis A pediatric vaccine, was evaluated in children aged 1–17. The reduction in antibody titers was more pronounced in younger children between 1 and 7 years old showing vaccine protection of at least 5.5 years after two doses, which was lower than the estimated duration of 25 years [130].
Cubosomes
Cubosomes, which are known as a loaded lyotropic liquid crystalline nanoparticles system, are formed from specific amphiphilic lipids and stabilizers. They could be administered through several drug delivery routes such as oral, transdermal, ocular, and chemotherapeutic methods. Cubosomes can provide a suitable delivery system for cancer therapy and other purposes, because of their acceptable biodegradability, targeted and controlled release, large surface area, straightforward manufacturing, and the ability to load diverse active compounds. Their preparation methods include sonication, emulsification, and homogenization, using both top-down and bottom-up techniques [131]. In 2020, cefpodoxime proxetil–loaded cubosomes were prepared for pediatric oral delivery. Cefpodoxime proxetil, which is a pro-drug for oral administration, is defined as a third-generation cephalosporin antibiotic and it has broad-spectrum activity against gram-positive and gram-negative microorganisms. However, the bitter taste of cefpodoxime proxetil can cause low pediatric compliance to marketed oral dosage forms such as tablets, capsules, and dry suspensions. The in vitro experiment demonstrated a sustained-release behavior in 24 h, and electronic tongue results indicated that cubosomes containing cefpodoxime proxetil masked the bitterness of the antibiotic [49].
State of the art in pediatric diseases managed with nanoconfigured drug carriers
Cancer
Nearly 90% of cancers in pediatric ages ranging from 0 to 19 years old occur in low- and middle-income countries (LMICs), where nearly 95% of the children live. The health systems of these countries are generally weaker, so cancers often go undetected and untreated. In terms of childhood cancers, acute lymphoblastic leukemia is the most common and accounts for 19% of all pediatric cancers. Non-Hodgkin lymphoma is next with 5%, followed by nephroblastoma and Burkitt lymphoma with 5% and retinoblastoma with 5%. Survival probabilities range from less than 30% in LMIC and low-income countries (LIC) to 50% in upper-middle-income countries and over 80% in high-income countries (HIC) [132].
Chemotherapy agents are mostly used for the control or prevention of metastatic disease. There are several major issues with present chemotherapy agents including their action against cancerous and normal cells without discrimination which can lead to killing normal cells, toxicities, and severe side effects. Using emerging technologies in nanomedical research can lead to targeted chemotherapy which can be administered specifically to tumor tissues to eradicate serious side effects and toxic effects associated with conventional chemotherapy [133]. A potential application of nanotechnology in this field is improving the therapeutic index of cytostatic agents by reducing their toxicity. Nanomedicines can deliver both chemotherapeutic and immunomodulating agents which can enhance immunogenic cell death inducement and immune response in tumors, respectively [134,135,136].
The usage of anticancer nanomedicines in pediatrics could, therefore, potentially be a major step in avoiding difficulties that stem from drug dose selection and chemotherapeutic toxicity [137]. It is believed that nanosized suspensions can escalate the therapeutic index of loaded therapeutic agents and raise tumor targeting; thereby, the tissue distribution and pharmacokinetics of these drugs could be modified [138]. Moreover, nanoparticles can overcome biological barriers (e.g., the blood–brain barrier) and they can be beneficial for treating brain tumors. Nanoparticles could be prepared by using organic or inorganic materials or a mix of them. Furthermore, they may be different in size, shape, and size, all of which can be tuned following the synthesis method used [139]. Several nanomedicines discussed herein, though fabricated as potentially effective therapies for childhood cancer, have also found substantial use in the management of adult carcinomas.
Brain cancer and tumors
Brain cancer is an uncontrolled cell growth disease in the brain which can spread to adjacent tissues in some cases. Brain cancers are of two kinds primary brain cancers, which originate in the brain, and secondary brain cancers, which start in the other parts of the body and spread to the brain [140, 141].
There are between 15 and 20% of all malignancies in children that arise from central nervous system (CNS) tumors [142]. Although brain tumors are rare in pediatrics, they are classified as the most prevalent solid tumors in this age population. It is believed that boys have a higher incidence of these tumors throughout their lives than girls. Each year, approximately 3700 pediatric CNS tumors are diagnosed in the USA between the ages of 0 and 14 [143]. A low-grade glioma, which is defined as an astrocytoma of WHO grades I and II, is the most common brain tumor in pediatrics, about 24% of all childhood brain cancers. Based on histological findings, they are categorized based on their location and histology [144].
Optimum drug delivery to tumors is the major challenge in all brain tumors treatments, especially pediatric brain tumors, due to the blood–brain barrier (BBB) and the brain-cerebrospinal fluid (CSF) barrier. The BBB, which is a vascular barrier, can provide brain protection by tightly regulating macromolecules, ions, and nutrient permeation [145, 146]. Nanoparticles are known as a non-invasive drug delivery system for passing through the BBB. Tumor-targeted delivery is another significant potential of nanoparticles for carrying a wide range of drugs to brain tumors in children. Additionally, fluorescent and magnetic molecules can be used to modulate nanoparticles [147,148,149]. Active or passive targeting might be achieved by using nanocarriers. An active targeting approach involves the attachment of targeting moieties to the nanoparticles’ surface, which may interact with overexpressed receptors on the brain tumor cells’ surface, while the enhanced permeability and retention (EPR) effect is attributed to passive targeting. Moreover, RNA therapeutic agents, such as miRNA and siRNA, can be employed as recent approaches for brain tumor treatment. Biocompatibility, high transfection capacity, preferable accumulation, and easy fabrication of liposomes make them one of the most effective nanocarriers for RNA molecules to be delivered to brain tumors [150, 151].
In 2014, liposomal nanoparticles comprising Evans blue were developed for targeting and imaging brainstem tumors in pediatric patients suffering from infiltrating brainstem gliomas (BSG). As nanoparticles were accumulated in brainstem tumors in the murine model, the investigation showed site-specific delivery of liposomal nanoparticles [152]. In 2015, chitosan-g-PEG copolymer (CP)-coated iron oxide nanoparticles were developed by using a co-precipitation method and siRNA was loaded into nanoparticles. This formulation delivered genes to brain cancer cells without in vivo (cell lines derived from pediatric MB and ependymoma) and in vitro cytotoxicity [153]. In 2017, gold nanoparticles were loaded with siRNA which was protected and carried to pediatric MB and ependymoma cells. Gold nanoparticles, which were coated with polyethylene glycol (PG), chitosan, and polyethyleneimine (Au-CP-PEI), decreased brain tumor resistance to radiation therapy in pediatrics [154]. In another study, high-density lipoprotein nanoparticles (HDL NPs) are investigated for their effect on Sonic hedgehog (SHH) subtype medulloblastomas, which make up about 25% of all malignancies. It was demonstrated that these nanoparticles bind and uptake in cells expressing HDL receptors and scavenger receptor type B-1 and have anti-neoplastic effects in MB cells [155].
In 2019, poly(beta-amino esters) (PBAEs) nanoparticles encapsulating plasmid DNA encoding the suicide gene herpes simplex virus I thymidine kinase (HSVtk) were developed for treating pediatric malignancies such as MB and atypical teratoid/rhabdoid tumors (AT/RT) which are the most common pediatric brain malignancies. PBAEs are cationic, biodegradable, and self-assembled polymers which could carry nucleic acids. This study indicated that genes of interest with significant therapeutic effects were delivered to MB and AT/RT tumors using PBAEs in mouse xenograft models in vivo via intracranial injection [88]. In 2021, gold nanoarchitecture containing doxorubicin was prepared as a treatment against diffuse intrinsic pontine glioma (DIPGs) which are the most aggressive high-grade gliomas in the pediatric population. These gliomas are difficult to treat because of their infiltrative nature in the brainstem. Doxorubicin-loaded nanoarchitectures were shown to be more effective than free doxorubicin in cytotoxicity against DIPG cells [156, 157]. Moreover, a novel N(3)-propargyl (N3P) derivative of temozolomide was loaded into nanoliposomes to enhance its solubility, sustained distribution, and stability for treating temozolomide-resistant pediatric diffuse midline glioma. In children, diffuse midline and diffuse intrinsic pontine gliomas (DIPG) are infiltrative malignant tumors of the ventral pons with no effective and currently available treatment. As a result, the combination of convection-enhanced delivery with the longer half-life of these therapeutic agents in the nanoparticles should be able to minimize systemic toxicities and administered doses. The experiment showed that the formulation benefited from a sustained-release profile and instant uptake during 1-h incubation in the DIPG model (in vitro), distribution, and penetration in vivo (rats) [158, 159].
Retinoblastoma
As the most prevalent intraocular malignancy in children, retinoblastoma (Rb), which is an aggressive eye cancer in infants and children, accounts for four percent of all pediatric cancers. It is estimated that 1 in 20,000 babies is born with retinoblastoma, and there are app) has been establisheroximately 200–300 new patients of retinoblastoma each year in the USA. The chance of survival and saving vision depends on the severity of the disease [160,161,162].
Several nanoformulations have been developed to overcome pediatric drug delivery obstacles; some of them are shown in Table 3.
Leukemia
Childhood acute lymphoblastic leukemia (ALL) is derived from B and T lymphoblasts in the thymus and bone marrow tissues. In the USA, about 40 patients per 1 million children aged 0–14 years suffer from ALL annually. Krishnan et al. prepared polymeric nanoparticles to encapsulate dexamethasone which is known as an anti-inflammatory and bone growth steroid. Dexamethasone is counted as one of the most effective chemotherapeutic agents for childhood ALL treatment. It can eradicate a large number of leukemic cells by inducing cell death of B and T lymphocytes. This study showed the nanoformulation of dexamethasone-induced leukemia apoptosis and enhanced survival with lower doses of dexamethasone [179]. In another study, zinc oxide nanoparticles (ZnO-NPs) were developed to treat pediatric leukemia. ZnO-NPs are one of the most popular drug carriers amongst all metal oxide nanoparticles due to their safety and lower toxicity. Since they benefit from the small particle size, the zinc could be absorbed easily in the body. Hence, they can be used as a cancer treatment and diagnosis agent [180, 181]. Liu et al. synthesized the ZnO-NPs by using a biological source. Besides, the dose-dependent cytotoxicity of these NPs against pediatric leukemia cells was evaluated and revealed. As discussed earlier, nanoparticles might be an efficient carrier to deliver small interfering RNA (siRNA) into the cancerous cells. In an investigation, a certain siRNA was loaded in lipid-based nanoparticles to treat acute myeloid leukemia (AML), which is characterized by the rapid proliferation of immature myeloid blast cells. This study showed that the prepared formulation did not affect normal cells due to its selective targeting of AML cells. Moreover, the potent uptake of nanoparticles by the pediatric AML cell line model and the inhibition of AML cell progression were revealed [182].
Osteosarcoma
The term sarcoma refers to malignant tumors derived from cartilage, bones, and muscle tissues. An osteosarcoma (OS) is characterized by mesenchymal malignancies which produce immature bones or osteoid. Generally, children under the age of 20 suffer from bone cancer infrequently and 650–700 new cases of bone cancer per year are estimated [183]. As part of the effort towards designing better therapeutic interventions for osteosarcoma management in the pediatric population, the effects of paclitaxel-loaded nanoparticle albumin-bound (nab-paclitaxel or Abraxane®) on 143.98.2 osteosarcoma cells were investigated in 2014. Five days of nab-paclitaxel treatment resulted in prolonged survival and inhibited the growth of OS [184]. In 2015, Ni and team developed a method of emulsion/solvent evaporation that was used to prepare salinomycin-loaded poly(lactic-co-glycolic acid) nanoparticles (NP) conjugated with CD133 aptamers (as an osteosarcoma marker) for targeting CD133+ osteosarcoma cancer stem cells. The aptamer is a molecule composed of an oligonucleic acid or peptide that binds to a particular target molecule. It has been proven that salinomycin, known as an antibiotic, can kill OS cancer stem cells. However, salinomycin is poorly soluble in water, inhibiting its clinical application. The study showed that compared to salinomycin-NP only or unbound salinomycin, the conjugated formulation had the best therapeutic effect on Saos-2 osteosarcoma xenograft mice. It was demonstrated that the prepared formulation killed OS cancer stem cells in vitro and in vivo [185].
In another investigation, doxorubicin-loaded PEGylated liposomes were developed using the pH gradient hydration method. The study demonstrated that liposomal doxorubicin increased toxicity in MG-63, U2-OS, SaOS-2, SaOS-LM7 cell lines, and human primary osteoblasts cells compared to free doxorubicin. Besides, the permeability of doxorubicin into the cell was enhanced due to nanoparticle encapsulation [186]. González-Fernández and colleagues prepared edelfosine-loaded lipid nanoparticles (EF-LN) for primary tumor targeting and metastases elimination. The antitumor effect of edelfosine (EF) has been established in vitro and in vivo; however, low oral bioavailability and severe side effects of EF lead to therapeutic use prevention in clinical practice. In vivo evaluations showed that EF-LN reduced the progression of the primary tumor growth in MNNG-HOS and 143 B-orthotopic OS mice models. Furthermore, EF-LN prevented the metastatic spread of 143B OS cells from the primary tumor to the lung [187]. Also, the surface of the cancer cell membrane derived from 143B cells was modified using silica nanoparticles to target homogenous 143B cells. Furthermore, indocyanine green as a photothermal agent was encapsulated into the nanoparticles to provide tumor-targeted photothermal therapy of osteosarcoma cells. In vitro and in vivo studies showed that the novel formulation benefited from higher targeting ability and anticancer efficacy compared to free drug and unmodified silica nanoparticles. Moreover, the encapsulated indocyanine green was delivered to isogenous 143B cells specifically by the prepared nanosystem and it has pH-dependent release [188].
Furthermore, the 50-nm nanoassemblies (NAs) were formed by co-assembling alkyl-lysophospholipid edelfosine (EF) and squalenoyl-gemcitabine (SQ-Gem). Gemcitabine is known as a second-line antineoplastic therapeutic drug for pediatric OS treatment. EF, which is a pro-apoptotic drug, is believed to modify SQ-Gem pharmacokinetics and increase its tolerability. It was demonstrated that EF enhanced SQ-Gem exposure after intravenous administration. This experiment showed that not only was the toxicity, after administering the novel formulation several times, in mice (in vivo OS model) decreased, but the tolerability was also improved. Besides, the developed formulation reduced the kinetic of primary tumor growth without causing adverse effects [189]. Xu and colleagues also explored the novel nanosystem of zoledronic acid–loaded nanoparticles that was prepared by using hyaluronic acid, polyethylene glycol, and nanohydroxyapatite for targeted therapy of osteosarcoma cells. Zoledronic acid, an approved bisphosphonate for treating metastatic bone diseases, has been shown to be safe and tolerable. The results demonstrated that a series of human osteosarcoma cell lines, including 143b, HOS, and MG63, were effectively inhibited by the NPs, while there was no significant cytotoxic effect on normal cells. Moreover, the injection of NPs locally in vivo showed the stimulation of tumor apoptosis and necrosis and infiltration of granulocytes in blood vessels [190].
Neuroblastoma
Neuroblastoma (NB), which is an extracranial pediatric malignancy, represents about 13% of all pediatric cancer mortality and is the main cause of death in children aged 1 to 5 years. NB stems from neuronal crest progenitor cells and affects infants younger than one year of age more commonly than other cancers. NB is characterized by noticeable biological and genetic diversity, as well as clinical heterogeneity. It is associated with spontaneous remission, resistance treatment, and a low rate of survival [191]. In 2018, doxorubicin-loaded nanocells were developed for pediatric aggressive NB. The in vitro results showed that tumor growth and volume were reduced in mice with orthotopic xenografts of human neuroblastoma after 28 days [192].
Hypertension
Pediatric hypertension (HTN), which can happen because of obesity, is a growing health concern. Hydrochlorothiazide (HCT), categorized as a diuretic drug, is mostly used for pediatric hypertension treatment because of its safety and effectiveness. Besides, HCT benefits from high-level patient compliance because it is easy to administer (i.e., once daily). Nevertheless, HCT is a BCS class IV drug indicating that it has low solubility and permeability that can result in poor bioavailability. Mura and colleagues prepared two different types of hydrochlorothiazide nanocarriers, solid lipid nanoparticles (SLNs) and nanostructured lipid carriers (NLCs), for pediatric therapies in the form of oral liquid formulations to resolve the solubility and stability problems of HCT. Both SLNs and NLCs were stable after 6 months, and they did not show cytotoxicity on cells. However, the drug release and entrapment efficiency of NLCs were higher than SLNs [107].
Infections
Infectious diseases, including malaria, diarrhea, and acute respiratory infections in countries with high mortality, are the major cause of death in post-neonatal children who are less than 5. The deadliest communicable disease impacting the pediatric population relative to other infectious diseases is acute respiratory infection (ARI) [193]. As some of these infectious diseases require long-duration or even lifelong therapies, prolonged and fixed-dose combination formulations can be beneficial to improve patients’ compliance and treatment efficiency. Achieving these goals can be made possible using nanoconfigured technologies which have distinguishing merits, such as targeted delivery to the bacteria, improvement of stability, solubility, and bioavailability of anti-infective agents, and thus reduce the development of drug resistance [194, 195].
Parasitic infections
Parasites can cause chronic diseases in general, and their symptoms usually are not noticeable in contrast to bacterial infections. Most anti-parasitic agents such as benzimidazoles have low water solubility and stability leading to insufficient bioavailability and therapeutic effect which can be resolved by using nanoformulations [196, 197]
Malaria
Malaria, which is a life-threatening disease, is typically transmitted to humans, when bitten, by an infective female Anopheles mosquito. Globally, half of the world’s population lives in malaria-endemic territories, and imports of malaria disease are common in almost every country. Children aged 6 months to 5 years are the most affected, and malaria may account for up to 10% of all child deaths in regions where it is endemic [198]. Nanomedicines have found some potential applications in the management of malaria. For instance, Dandagi and co-workers employed solid lipid nanoparticles (SLN) as novel carriers for the delivery of quinine sulfate, a key antimalarial drug, used in children and even adults. The developed nanostructured system effectively masked the bitter taste of quinine and provided a flexible dose adjustment system based on body weight which are useful for improving acceptance, compliance, and therapeutic efficacy in the pediatric population [199].
In 2017, a fast dissolvable oral formulation containing mefloquine-loaded liposomes was developed for pediatrics. Mefloquine, used as a prophylaxis or treatment of malaria, has low water solubility and bitter taste causing low adherence in children. The research depicted that drug solubility was elevated, and the unpleasant taste was masked. Besides, the prepared liquid formulation was stable for more than 3 months in a refrigerator (4 °C) and the lyophilized powder of liposomal formulation was stable for more than 3 months at room temperature. The result of the in vivo evaluation showed that drug absorption was significantly increased in mice [200].
Schistosomiasis
Schistosomiasis is an acute and chronic neglected tropical parasitic disease caused by trematode worms. It affects about 240 million people, of which some of them are preschool-age children accounting for 28 million cases. Although praziquantel (PZQ) is the first choice of treatment for schistosomiasis, its nasty and metallic taste can reduce children’s compliance. Besides, the low aqueous solubility of PZQ could significantly affect the drug’s dissolution and bioavailability [201, 202]. In 2019, dried PZQ-loaded nanoparticles were fabricated and investigations showed not only taste improvement but also better aqueous solubility [203].
Chagas disease
Trypanosoma cruzi is the causative organism for Chagas disease, which affects approximately 6–7 million people around the world, and it particularly affects children who are chronically infected. Benznidazole (BNZ) is the first-line treatment for Chagas disease, while the USFDA recently approved it for treating patients aged 2–12. BNZ is practically insoluble in water [204, 205]. The powder form of polymeric nanoparticles containing BNZ was developed by using the freeze-drying method. This nanoformulation increased drug dissolution and provided dose flexibility to meet the needs of children of all age groups [206].
Fascioliasis
Fascioliasis is a parasitic infection affecting the hepatobiliary system especially observed among pediatric patients in countries with unhealthy water resources. As a first-line therapy, triclabendazole (TBZ) has been recommended to treat this disease. However, its poor water solubility limits the dissolution rate [207]. Considering that many patients suffering from fascioliasis are children, a dosage form tailored to pediatrics is essential. In 2022, the self-nanoemulsifying lipid-based system of TBZ (TBZ SNEDDS) was prepared to enhance its aqueous solubility and bioavailability. Moreover, solid TBZ SNEDDS in dispersible colored tablet form was developed which was able to customize pediatric weight-based doses to avoid toxicity and side effects. Hence, the prepared tablet was a suitable formulation for use in pediatric treatment [208].
Cutaneous leishmaniasis
Leishmaniasis is a parasitic disease spread by female sandfly bites. Globally, 350 million people are at risk of contracting leishmaniasis in 98 countries and children constitute an important number of cases [209, 210]. Cutaneous leishmaniasis is the most prevalent form of the disease, which causes long-lasting atrophic scarring and nodule-ulcerative lesions. Amphotericin B, as a liposomal preparation (L-AmB) marketed as AmBisome®, is an effective and preferred bioactive molecule that is commonly used in the treatment of cutaneous leishmaniasis in persons of all ages. Specifically, the efficacy of intravenous L-AmB for treating cutaneous leishmaniasis in pediatric patients was investigated. In the study, intravenous L-AmB was administered in six doses (3 mg/kg/day) for five successive days, and on day 10, slow infusion of L-AmB over 60 min was administered. Systemic antihistamine, methylprednisolone, and paracetamol were given before L-AmB administration, and less than 50% of the pediatric patients treated showed complete clinical recovery [210].
Sepsis
Sepsis is the life-threatening response of the body to infections which causes organ dysfunction. There is a high rate of child mortality due to pediatric sepsis around the world [211]. Although metronidazole is usually utilized for treating bacterial infections, its short half-life limits its usage. In 2023, a pH-responsive system containing metronidazole nanocarriers was prepared by using the hydrothermal method to provide a controlled release of the drug. In this system, metronidazole was encapsulated in zeolitic imidazole frameworks-90 (ZIF-90) to be protected from decomposition in acidic conditions. It was demonstrated that the developed formulation can enhance immunity while eliminating microbial infections [212].
Viral infections
Viral infections, which stem from viral pathogens, could have no symptoms or severe presentations. Although many pediatric viral infections can be prevented by using vaccines, very few of them might be treated by antiviral drugs. Although children may be infected during pregnancy or at birth due to maternal infections, they can be impacted by viruses at older ages [213, 214].
Human immunodeficiency virus (HIV)
The human immunodeficiency virus (HIV) targets T-helper lymphocytes and attacks the immune system. In most infected children, the human immunodeficiency virus type 1 (HIV-1) is transferred from mother to child during pregnancy, delivery, or breastfeeding. According to the recent World Health Organization (WHO) reports, 1.5 million children aged between 0 and 14 years are living with HIV [215, 216]. Chiappetta and colleagues loaded efavirenz (EFV) into the core of polymeric micelles for pediatric uses. EFV, known to be poorly soluble in water, is known as a first-choice antiretroviral drug for pediatric treatment. This experiment illustrated that encapsulating EFV in polymeric micelles improved the water solubility and bioavailability of the drug [217]. In 2011, a pediatric oral formulation of tenofovir-loaded niosomes was prepared by using high-pressure homogenization technology. Tenofovir is a nucleotide antiretroviral drug that is used against (HIV-1), and its bioavailability is insufficient. The effects of physical process and compositional variables on formulation features such as vesicle size and drug release were evaluated. The significant effects of compositional variables, such as drug amount, level of cholesterol, and length of surfactant chain, on drug release profile were shown in this study [218]. Furthermore, a group of investigators prepared D-α-tocopheryl polyethylene glycol 1000 succinate (TPGS) micelles containing nelfinavir mesylate (NFV) was prepared as an HIV treatment in the pediatric population. NFV is the first non-peptidic HIV-1 protease inhibitor recommended for pediatric use. Based on the Biopharmaceutical Classification System (BCS), NFV is a class IV biomolecule (i.e., low aqueous solubility and permeability). However, polymeric micelles are known to improve drug stability and water solubility, so NFV was incorporated into their hydrophobic cores. The experiment showed that NFV-loaded TPGS micelles were solubilized in an aqueous formulation which could provide ease of administration and dose adjustment for children. Overall, the oral bioavailability of NFV was enhanced [219]. In another study, chitosan nanoparticles of dolutegravir were prepared by using the spray drying method as a food or milk admixture for infected pediatrics. Dolutegravir (DTG), classified as a BCS class II, is an integrase strand transfer inhibitor. This study demonstrated that the administration of DTG nanoformulation with milk is feasible, and in vivo study in Balb-C mice was done for validation. Moreover, the nanoformulated drug biodistribution in plasma and organs was more than the pure drug [220]. In 2023, a lipid-based nanostructured oral liquid formulation of lamivudine and zidovudine was developed based on green chemistry principles. The lamivudine and zidovudine combination are known as the first-line treatment of nucleoside reverse transcriptase inhibitor (NRTI) backbone for pediatrics. The novel formulation provided a controlled release of the drugs and protected them from degradation in the acidic gastric environment. Also, they were suitable for children because they were taste-masked and offered flexible dosing for dose adjustment purposes [221].
Asthma
Asthma is defined as airways chronic inflammatory disease, known by recurrent airflow obstruction which arises from the edematous and bronchospastic airways, and increasing mucus production. According to the Centers for Disease Control and Prevention (CDC) reports, more than 6 million of the pediatric population in the USA suffer from asthma. In general, asthma is a chronic disease with a high morbidity rate and a low mortality rate [222]. In 2015, prednisolone-loaded nanoparticles in oral dispersible tablets dosage form were developed. Prednisolone (PDS), which is a synthetic glucocorticoid and immunosuppressive drug, is a good choice for pediatric treatment of asthma. However, available dosage forms can cause swallowing difficulties in children. Besides, PDS’s solubility in water is low which can be improved by using nanoencapsulation. Therefore, Chen and colleagues prepared fast-disintegrating tablets containing PDS-loaded chitosan nanoparticles with the overall goal of enhancing patient compliance and overcoming swallowing problems [223]. Also, in 2021, the suspension of zafirlukast (ZFR)-loaded nanoparticles was prepared for children. ZFR, which has a low solubility in water can control and reduce asthma-induced symptoms, including wheezing and shortness of breath. Using chitosan to prepare nanoparticles in this formulation improved both drug solubility and drug release from suspension [224].
Concluding remarks
Here, we have discussed a wide range of nanomedicines fabricated to circumvent possible impediments to successful pediatric-specific disease management. Interestingly, the use of these diversified bioactive molecules containing nanosystems displayed the capacity to meet the unique needs of the pediatric population that can make desired therapeutic outcomes achievable. Generally, nanosystems offer a variety of characteristic features (such as shape/morphology, surface charge and properties, size) that are adaptable to provide a range of properties that can aid and/or optimize drug delivery for specific purposes and diverse patient categories. This customization potential makes them incredibly attractive for use as innovative drug carriers for various patient-specific biomedical/clinical applications, along with potential opportunities for precision/personalized medicines that can significantly enhance therapeutic efficacy and minimize adverse effects. Additionally, nanomedicines function as encapsulating structures that can increase the aqueous solubility of hydrophobic drugs thus facilitating bioavailability. They can also provide targeted therapy, especially for anti-cancer agents, which can negatively impact normal cells and increase the cellular uptake of drugs raising their biological effectiveness. These novel systems also provide differing drug release kinetics (e.g., sustained, extended, controlled release) which make them versatile delivery matrices that can cater for a variety of pediatric therapeutic needs. Furthermore, nanomedicines may escalate drug delivery through the blood brain barriers for tumor shrinking or imaging or even for specific gene delivery applications or on the other hand shield encapsulated ribonucleic acids during delivery to tumors. All these make up useful applications for the pediatric population. Besides, nanomedicines have good flexibility and potential as effective pediatric drug delivery systems because they have been shown to provide the benefits that are critical for developing child-friendly formulations such as improving palatability and other organoleptic characteristics, aiding dosing and administration flexibility, reducing dosing frequency, enhancing safety and in vitro/in vivo stability, alleviating swallowing difficulties, and augmenting in vivo performance (i.e., pharmacokinetics and pharmacodynamics).
Expert opinion
Undoubtedly, a huge global need for innovative pediatric medicines exists and the use of nanomedicines is a potentially viable solution to this lingering challenge considering their flexibility. Therefore, intensifying research and development efforts centered on designing effective nanoconfigured drug carriers can serve as a major contribution to scientific knowledge and the innovation of marketable child-friendly medicines that can aid disease management and clinical outcomes. From our perspective, the nanoemulsion, nanosuspension, nanoparticle (polymer, polymer-lipid, lipid-based), and liposomal technologies would be good options to continue pursuing and expand on for commercialization purposes majorly because these delivery systems have shown repeated promise for further development of child-friendly dosage forms and appear to be easily scalable options for pharmaceutical manufacturing purposes. Besides, a closer look at their toxicity profiles, the most suitable animal model for preclinical in vivo studies, excipients, and active drug selection, as well as identifying key quality parameters and specification limits that can strengthen current regulatory measures, particularly for this patient population, will go a long way in making these sustainable.
Data availability
Not applicable.
References
Lehmann B. Regulation (EC) No 1901/2006 on medicinal products for paediatric use & clinical research in vulnerable populations. Child Adolesc Psychiatry Ment Health. 2008;2:37. https://doi.org/10.1186/1753-2000-2-37.
Abdel-Rahman SM, Amidon GL, Kaul A, Lukacova V, Vinks AA, Knipp GT. Summary of the National Institute of Child Health and Human Development-Best Pharmaceuticals for Children Act Pediatric Formulation Initiatives Workshop-Pediatric Biopharmaceutics Classification System Working Group. Clin Ther. 2012;34:S11–24. https://doi.org/10.1016/j.clinthera.2012.09.014.
Avant D, Wharton GT, Murphy D. Characteristics and changes of pediatric therapeutic trials under the Best Pharmaceuticals for Children Act. J Pediatr. 2018;192:8–12. https://doi.org/10.1016/j.jpeds.2017.08.048.
Ren Z, Zajicek A. Review of the Best Pharmaceuticals for Children Act and the Pediatric Research Equity Act: what can the obstetric community learn from the pediatric experience? Semin Perinatol. 2015;39:530–1. https://doi.org/10.1053/j.semperi.2015.08.006.
Turner MA, Catapano M, Hirschfeld S, Giaquinto C. Paediatric drug development: the impact of evolving regulations. Adv Drug Deliv Rev. 2014;73:2–13. https://doi.org/10.1016/j.addr.2014.02.003.
Maphalle LNF, Michniak-Kohn BB, Ogunrombi MO, Adeleke OA. Pediatric tuberculosis management: a global challenge or breakthrough? Children. 2022;9:1120. https://doi.org/10.3390/children9081120.
Batchelor HK, Kendall R, Desset-Brethes S, Alex R, Ernest TB. Application of in vitro biopharmaceutical methods in development of immediate release oral dosage forms intended for paediatric patients. Eur J Pharm Biopharm. 2013;85:833–42. https://doi.org/10.1016/j.ejpb.2013.04.015.
Batchelor H. Paediatric biopharmaceutics classification system: current status and future decisions. Int J Pharm. 2014;469:251–3. https://doi.org/10.1016/j.ijpharm.2014.02.046.
Rose K. The challenges of pediatric drug development. Curr Ther Res. 2019;90:128–34. https://doi.org/10.1016/j.curtheres.2019.01.007.
Katzung BG, Trevor AJ. Basic and clinical pharmacology 15e. McGraw-Hill Education. 2020.
Fernandez E, Perez R, Hernandez A, Tejada P, Arteta M, Ramos JT. Factors and mechanisms for pharmacokinetic differences between pediatric population and adults. Pharmaceutics. 2011;3:53–72. https://doi.org/10.3390/pharmaceutics3010053.
Yu G, Zheng Q-S, Li G-F. Similarities and differences in gastrointestinal physiology between neonates and adults: a physiologically based pharmacokinetic modeling perspective. AAPS J. 2014;16:1162–6. https://doi.org/10.1208/s12248-014-9652-1.
Lu H, Rosenbaum S. Developmental pharmacokinetics in pediatric populations, The. J Pediatr Pharmacol Ther. 2014;19:262–76. https://doi.org/10.5863/1551-6776-19.4.262.
Sage DP, Kulczar C, Roth W, Liu W, Knipp GT. Persistent pharmacokinetic challenges to pediatric drug development. Front Genet 5. 2014. https://www.frontiersin.org/articles/10.3389/fgene.2014.00281 (accessed June 5, 2023).
Job KM, Gamalo M, Ward RM. Pediatric age groups and approach to studies. Drug Inf J. 2019;53:584–9. https://doi.org/10.1177/2168479019856572.
Mian AN, Schwartz GJ. Measurement and estimation of glomerular filtration rate in children. Adv Chronic Kidney Dis. 2017;24:348–56. https://doi.org/10.1053/j.ackd.2017.09.011.
Muhari-Stark E, Burckart GJ. Glomerular filtration rate estimation formulas for pediatric and neonatal use, The. J Pediatr Pharmacol Ther. 2018;23:424–31. https://doi.org/10.5863/1551-6776-23.6.424.
Krekels EH, Rower JE, Constance JE, Knibbe CA, Sherwin CM. Chapter 8 - Hepatic drug metabolism in pediatric patients, in: W. Xie (Ed.). Drug metabolism in diseases. Academic Press, Boston, 2017: pp. 181–206. https://doi.org/10.1016/B978-0-12-802949-7.00008-0.
Yellepeddi VK, Joseph A, Nance E. Pharmacokinetics of nanotechnology-based formulations in pediatric populations. Adv Drug Deliv Rev. 2019;151–152:44–55. https://doi.org/10.1016/j.addr.2019.08.008.
Giacoia GP, Taylor-Zapata P, Zajicek A. Eunice Kennedy Shriver National Institute of Child Health and Human Development Pediatrics Formulation Initiative: Proceedings from the Second Workshop on Pediatric Formulations. Clin Ther. 2012;34:S1–10. https://doi.org/10.1016/j.clinthera.2012.09.013.
ADELEKE O.A. Method for encapsulating pharmaceutical actives (European Patent No. EP3291795B1), EP3291795B1. 2019. https://patents.google.com/patent/EP3291795B1/en (accessed November 10, 2023).
Duncan R, Gaspar R. Nanomedicine(s) under the microscope. Mol Pharmaceutics. 2011;8:2101–41. https://doi.org/10.1021/mp200394t.
Rizzo LY, Theek B, Storm G, Kiessling F, Lammers T. Recent progress in nanomedicine: therapeutic, diagnostic and theranostic applications. Curr Opin Biotechnol. 2013;24:1159–66. https://doi.org/10.1016/j.copbio.2013.02.020.
Kunjachan S, Ehling J, Storm G, Kiessling F, Lammers T. Noninvasive imaging of nanomedicines and nanotheranostics: principles, progress, and prospects. Chem Rev. 2015;115:10907–37. https://doi.org/10.1021/cr500314d.
Lammers TL, Kiessling F, Hennink WE, Storm G. Gert, Drug targeting to tumors: principles, pitfalls and (pre-) clinical progress, in: Nano-enabled medical applications, Jenny Stanford Publishing, 2020.
Kreyling W. Nanomedicine : an ESF-European Medical Councils (EMRC) forword look report 2005. 2005.
Moghimi SM, Hunter AC, Murray JC. Nanomedicine: current status and future prospects. FASEB J. 2005;19:311–30. https://doi.org/10.1096/fj.04-2747rev.
Chavda VP. Chapter 4 - Nanobased nano drug delivery: a comprehensive review, in: S.S. Mohapatra, S. Ranjan, N. Dasgupta, R.K. Mishra, S. Thomas (Eds.). Applications of targeted nano drugs and delivery systems. Elsevier. 2019: pp. 69–92. https://doi.org/10.1016/B978-0-12-814029-1.00004-1.
Sosnik A, Carcaboso AM. Nanomedicines in the future of pediatric therapy. Adv Drug Deliv Rev. 2014;73:140–61. https://doi.org/10.1016/j.addr.2014.05.004.
Barenholz YC. Doxil® — the first FDA-approved nano-drug: lessons learned. J Control Release. 2012;160:117–34. https://doi.org/10.1016/j.jconrel.2012.03.020.
Swank Kimberley. Harinstein, Lisa, Muñoz, Monica, Pediatric postmarketing pharmacovigilance review. Food and Drug Administration. 2017. https://www.fda.gov/files/advisory%20committees/published/Emend-%28aprepitant%29-Capsule-and-Oral-Suspension-Pediatric-Postmarketing-Pharmacovigilance-Review.pdf .
Office of the Commissioner. Pediatric Oncology Drug Approval. FDA 2023. https://www.fda.gov/about-fda/oncology-center-excellence/pediatric-oncology-drug-approvals (accessed August 15, 2023).
Stone NR, Bicanic T, Salim R, Hope W. Liposomal amphotericin B (AmBisome®): a review of the pharmacokinetics, pharmacodynamics, clinical experience and future directions. Drugs. 2016;76:485–500. https://doi.org/10.1007/s40265-016-0538-7.
N. Nieto González, A. Obinu, G. Rassu, P. Giunchedi, E. Gavini, Polymeric and lipid nanoparticles: which applications in pediatrics?, Pharmaceutics 13 (2021) 670. https://doi.org/10.3390/pharmaceutics13050670.
Shah NN, Merchant MS, Cole DE, Jayaprakash N, Bernstein D, Delbrook C, Richards K, Widemann BC, Wayne AS. Vincristine sulfate liposomes injection (VSLI, Marqibo®): results from a phase I study in children, adolescents, and young adults with refractory solid tumors or leukemias. Pediatr Blood Cancer. 2016;63:997–1005. https://doi.org/10.1002/pbc.25937.
Peyrl A, Sauermann R, Chocholous M, Azizi AA, Jäger W, Höferl M, Slavc I. Pharmacokinetics and toxicity of intrathecal liposomal cytarabine in children and adolescents following age-adapted dosing. Clin Pharmacokinet. 2014;53:165–73. https://doi.org/10.1007/s40262-013-0106-1.
Batchelor HK, Marriott JF. Formulations for children: problems and solutions. Br J Clin Pharmacol. 2015;79:405–18. https://doi.org/10.1111/bcp.12268.
M.S. Alqahtani, M. Kazi, M.A. Alsenaidy, M.Z. Ahmad, Advances in oral drug delivery, Frontiers in Pharmacology 12 (2021). https://www.frontiersin.org/articles/https://doi.org/10.3389/fphar.2021.618411 (accessed May 22, 2023).
Rampedi PN, Ogunrombi MO, Wesley-Smith J, Adeleke OA. A micro-configured multiparticulate reconstitutable suspension powder of fixed dose rifampicin and pyrazinamide: optimal fabrication and in vitro quality evaluation. Pharmaceutics. 2022;15:64. https://doi.org/10.3390/pharmaceutics15010064.
Kean EA, Adeleke OA. Orally disintegrating drug carriers for paediatric pharmacotherapy. Eur J Pharm Sci. 2023;182: 106377. https://doi.org/10.1016/j.ejps.2023.106377.
Kakodkar K, Schroeder JW. Pediatric dysphagia. Pediatr Clin. 2013;60:969–77. https://doi.org/10.1016/j.pcl.2013.04.010.
E. Umay, S. Eyigor, E. Giray, E. Karadag Saygi, B. Karadag, N. Durmus Kocaaslan, D. Yuksel, A.M. Demir, E. Tutar, C. Tikiz, E. Gurcay, Z. Unlu, P. Celik, E. Unlu Akyuz, G. Mengu, S. Bengisu, S. Alicura, N. Unver, N. Yekteusaklari, C. Uz, M. Cikili Uytun, F. Bagcier, E. Tarihci, M.S. Akaltun, I. Ayranci Sucakli, D. Cankurtaran, Z. Aykın, R. Aydın, F. Nazli, Pediatric dysphagia overview: best practice recommendation study by multidisciplinary experts, World J Pediatr 18 (2022) 715–724. https://doi.org/10.1007/s12519-022-00584-8.
Dodrill P, Gosa MM. Pediatric dysphagia: physiology, assessment, and management. Ann Nutr Metab. 2015;66:24–31. https://doi.org/10.1159/000381372.
Lawlor CM, Choi S. Diagnosis and management of pediatric dysphagia: a review. JAMA Otolaryngology-Head & Neck Surgery. 2020;146:183–91. https://doi.org/10.1001/jamaoto.2019.3622.
Preis M, Breitkreutz J. Pediatric drug development and dosage form design. AAPS PharmSciTech. 2017;18:239–40. https://doi.org/10.1208/s12249-016-0705-x.
Ali AA, Charoo NA, Abdallah DB. Pediatric drug development: formulation considerations. Drug Dev Ind Pharm. 2014;40:1283–99. https://doi.org/10.3109/03639045.2013.850713.
Reinholz J, Landfester K, Mailänder V. The challenges of oral drug delivery via nanocarriers. Drug Delivery. 2018;25:1694–705. https://doi.org/10.1080/10717544.2018.1501119.
D. Sahoo, R. Bandaru, S.K. Samal, R. Naik, P. Kumar, P. Kesharwani, R. Dandela, Chapter 9 - Oral drug delivery of nanomedicine, in: P. Kesharwani, S. Taurin, K. Greish (Eds.), Theory and applications of nonparenteral nanomedicines, Academic Press, 2021: pp. 181–207. https://doi.org/10.1016/B978-0-12-820466-5.00009-0.
Fan Y, Chen H, Huang Z, Zhu J, Wan F, Peng T, Pan X, Huang Y, Wu C. Taste-masking and colloidal-stable cubosomes loaded with Cefpodoxime proxetil for pediatric oral delivery. Int J Pharm. 2020;575: 118875. https://doi.org/10.1016/j.ijpharm.2019.118875.
Krieser K, Emanuelli J, Daudt RM, Bilatto S, Willig JB, Guterres SS, Pohlmann AR, Buffon A, Correa DS, Külkamp-Guerreiro IC. Taste-masked nanoparticles containing Saquinavir for pediatric oral administration. Mater Sci Eng, C. 2020;117: 111315. https://doi.org/10.1016/j.msec.2020.111315.
Zou Y, Mei D, Yuan J, Han J, Xu J, Sun N, He H, Yang C, Zhao L. Preparation, characterization, pharmacokinetic, and therapeutic potential of novel 6-mercaptopurine-loaded oral nanomedicines for acute lymphoblastic leukemia. Int J Nanomedicine. 2021;16:1127–41. https://doi.org/10.2147/IJN.S290466.
Deng Y, Shen L, Yang Y, Shen J. Development of nanoparticle-based orodispersible palatable pediatric formulations. Int J Pharm. 2021;596: 120206. https://doi.org/10.1016/j.ijpharm.2021.120206.
Omidian H, Mfoafo K. Exploring the potential of nanotechnology in pediatric healthcare: advances, challenges, and future directions. Pharmaceutics. 2023;15:1583. https://doi.org/10.3390/pharmaceutics15061583.
Zisowsky J, Krause A, Dingemanse J. Drug development for pediatric populations: regulatory aspects. Pharmaceutics. 2010;2:364–88. https://doi.org/10.3390/pharmaceutics2040364.
Lavan M, Byrn SR, Knipp G. Pediatric formulations: knowledge gaps limiting the expedited preclinical to clinical translation in children. AAPS PharmSciTech. 2019;20:73. https://doi.org/10.1208/s12249-018-1253-3.
Rodríguez-Nogales C, González-Fernández Y, Aldaz A, Couvreur P, Blanco-Prieto MJ. Nanomedicines for pediatric cancers. ACS Nano. 2018;12:7482–96. https://doi.org/10.1021/acsnano.8b03684.
Lagler FB, Hirschfeld S, Kindblom JM. Challenges in clinical trials for children and young people. Arch Dis Child. 2021;106:321–5. https://doi.org/10.1136/archdischild-2019-318676.
Yang S, Wallach M, Krishna A, Kurmasheva R, Sridhar S. Recent developments in nanomedicine for pediatric cancer. J Clin Med. 2021;10:1437. https://doi.org/10.3390/jcm10071437.
M.S. Marques, L.A. Lima, F. Poletto, R.V. Contri, I.C. Kulkamp Guerreiro, Nanotechnology for the treatment of paediatric diseases: a review, Journal of Drug Delivery Science and Technology 75 (2022) 103628. https://doi.org/10.1016/j.jddst.2022.103628.
Domingues C, Jarak I, Veiga F, Dourado M, Figueiras A. Pediatric drug development: reviewing challenges and opportunities by tracking innovative therapies. Pharmaceutics. 2023;15:2431. https://doi.org/10.3390/pharmaceutics15102431.
Singh Y, Meher JG, Raval K, Khan FA, Chaurasia M, Jain NK, Chourasia MK. Nanoemulsion: concepts, development and applications in drug delivery. J Control Release. 2017;252:28–49. https://doi.org/10.1016/j.jconrel.2017.03.008.
Kumar M, Bishnoi RS, Shukla AK, Jain CP. Techniques for formulation of nanoemulsion drug delivery system: a review. Prev Nutr Food Sci. 2019;24:225–34. https://doi.org/10.3746/pnf.2019.24.3.225.
Elbardisy B, Boraie N, Galal S. Tadalafil nanoemulsion mists for treatment of pediatric pulmonary hypertension via nebulization. Pharmaceutics. 2022;14:2717. https://doi.org/10.3390/pharmaceutics14122717.
Garcia-Becerra C, Rojas A, Höcht C, Bernabeu E, Chiappetta D, Tevez S, Lucangioli S, Flor S, Tripodi V. Characterization and bioavailability of a novel coenzyme Q10 nanoemulsion used as an infant formula supplement. Int J Pharm. 2023;634: 122656. https://doi.org/10.1016/j.ijpharm.2023.122656.
J. Zhang, Z. Xie, N. Zhang, J. Zhong, Chapter 13 - Nanosuspension drug delivery system: preparation, characterization, postproduction processing, dosage form, and application, in: E. Andronescu, A.M. Grumezescu (Eds.), Nanostructures for drug delivery, Elsevier, 2017: pp. 413–443. https://doi.org/10.1016/B978-0-323-46143-6.00013-0.
Perween N, Alshehri S, Easwari TS, Verma V, Faiyazuddin M, Alanazi A, Shakeel F. Investigating the feasibility of mefenamic acid nanosuspension for pediatric delivery: preparation, characterization, and role of excipients. Processes. 2021;9:574. https://doi.org/10.3390/pr9040574.
Wang J, Li B, Qiu L, Qiao X, Yang H. Dendrimer-based drug delivery systems: history, challenges, and latest developments. J Biol Eng. 2022;16:18. https://doi.org/10.1186/s13036-022-00298-5.
Zenze M, Daniels A, Singh M. Dendrimers as modifiers of inorganic nanoparticles for therapeutic delivery in cancer. Pharmaceutics. 2023;15:398. https://doi.org/10.3390/pharmaceutics15020398.
Yellepeddi VK, Mohammadpour R, Kambhampati SP, Sayre C, Mishra MK, Kannan RM, Ghandehari H. Pediatric oral formulation of dendrimer-N-acetyl-l-cysteine conjugates for the treatment of neuroinflammation. Int J Pharm. 2018;545:113–6. https://doi.org/10.1016/j.ijpharm.2018.04.040.
G.R. Williams, B.T. Raimi-Abraham, C.J. Luo, Nanofibres in drug delivery, UCL Press, 2018.
Farhaj S, Conway BR, Ghori MU. Nanofibres in drug delivery applications. Fibers. 2023;11:21. https://doi.org/10.3390/fib11020021.
Kajdič S, Planinšek O, Gašperlin M, Kocbek P. Electrospun nanofibers for customized drug-delivery systems. Journal of Drug Delivery Science and Technology. 2019;51:672–81. https://doi.org/10.1016/j.jddst.2019.03.038.
Ghosal K, Augustine R, Zaszczynska A, Barman M, Jain A, Hasan A, Kalarikkal N, Sajkiewicz P, Thomas S. Novel drug delivery systems based on triaxial electrospinning based nanofibers. React Funct Polym. 2021;163: 104895. https://doi.org/10.1016/j.reactfunctpolym.2021.104895.
Rustemkyzy C, Belton P, Qi S. Preparation and characterization of ultrarapidly dissolving orodispersible films for treating and preventing iodine deficiency in the pediatric population. J Agric Food Chem. 2015;63:9831–8. https://doi.org/10.1021/acs.jafc.5b03953.
Monterrubio C, Pascual-Pasto G, Cano F, Vila-Ubach M, Manzanares A, Schaiquevich P, Tornero JA, Sosnik A, Mora J, Carcaboso AM. SN-38-loaded nanofiber matrices for local control of pediatric solid tumors after subtotal resection surgery. Biomaterials. 2016;79:69–78. https://doi.org/10.1016/j.biomaterials.2015.11.055.
Zhou J, Yang Y, Zhang C. A low-temperature solid-phase method to synthesize highly fluorescent carbon nitride dots with tunable emission. Chem Commun. 2013;49:8605–7. https://doi.org/10.1039/C3CC42266F.
Wang W, Lu Y-C, Huang H, Feng J-J, Chen J-R, Wang A-J. Facile synthesis of water-soluble and biocompatible fluorescent nitrogen-doped carbon dots for cell imaging. Analyst. 2014;139:1692–6. https://doi.org/10.1039/C3AN02098C.
Li S, Amat D, Peng Z, Vanni S, Raskin S, Angulo GD, Othman AM, Graham RM, Leblanc RM. Transferrin conjugated nontoxic carbon dots for doxorubicin delivery to target pediatric brain tumor cells. Nanoscale. 2016;8:16662–9. https://doi.org/10.1039/C6NR05055G.
Liyanage P, Zhou Y, Al-Youbi AO, Bashammakh AS, El-Shahawi MS, Vanni S, Graham RM, Leblanc RM. Pediatric glioblastoma target-specific efficient delivery of gemcitabine across the blood–brain barrier via carbon nitride dots. Nanoscale. 2020;12:7927–38. https://doi.org/10.1039/D0NR01647K.
Dang Y, Guan J. Nanoparticle-based drug delivery systems for cancer therapy. Smart Materials in Medicine. 2020;1:10–9. https://doi.org/10.1016/j.smaim.2020.04.001.
Pridgen EM, Alexis F, Farokhzad OC. Polymeric nanoparticle drug delivery technologies for oral delivery applications. Expert Opin Drug Deliv. 2015;12:1459–73. https://doi.org/10.1517/17425247.2015.1018175.
Begines B, Ortiz T, Pérez-Aranda M, Martínez G, Merinero M, Argüelles-Arias F, Alcudia A. Polymeric nanoparticles for drug delivery: recent developments and future prospects. Nanomaterials. 2020;10:1403. https://doi.org/10.3390/nano10071403.
Gil ES, Wu L, Xu L, Lowe TL. β-cyclodextrin-poly(β-amino ester) nanoparticles for sustained drug delivery across the blood–brain barrier. Biomacromol. 2012;13:3533–41. https://doi.org/10.1021/bm3008633.
Pham K, Li D, Guo S, Penzak S, Dong X. Development and in vivo evaluation of child-friendly lopinavir/ritonavir pediatric granules utilizing novel in situ self-assembly nanoparticles. J Control Release. 2016;226:88–97. https://doi.org/10.1016/j.jconrel.2016.02.001.
Islam MS, Reineke J, Kaushik R, Woyengo T, Baride A, Alqahtani MS, Perumal O. Bioadhesive food protein nanoparticles as pediatric oral drug delivery system. ACS Appl Mater Interfaces. 2019;11:18062–73. https://doi.org/10.1021/acsami.9b00152.
Liu G, Li D-C, Li P-P, Li R-R, Chen S-Y. Methotrexate nanoparticle delivery system for treatment of inflammatory bowel disease in pediatric patients. Trop J Pharm Res. 2016;15:1361–8. https://doi.org/10.4314/tjpr.v15i7.2.
Zhang T, Ma J, Li C, Lin K, Lou F, Jiang H, Gao Y, Yang Y, Ming C, Ruan B. Core-shell lipid polymer nanoparticles for combined chemo and gene therapy of childhood head and neck cancers. Oncol Rep. 2017;37:1653–61. https://doi.org/10.3892/or.2017.5365.
Choi J, Rui Y, Kim J, Gorelick N, Wilson DR, Kozielski K, Mangraviti A, Sankey E, Brem H, Tyler B, Green JJ, Jackson EM. Nonviral polymeric nanoparticles for gene therapy in pediatric CNS malignancies, Nanomedicine: Nanotechnology. Biology and Medicine. 2020;23: 102115. https://doi.org/10.1016/j.nano.2019.102115.
S. Attias Cohen, P.S. Kingma, J.A. Whitsett, R. Goldbart, T. Traitel, J. Kost, SP-D loaded PLGA nanoparticles as drug delivery system for prevention and treatment of premature infant’s lung diseases, International Journal of Pharmaceutics 585 (2020) 119387. https://doi.org/10.1016/j.ijpharm.2020.119387.
Diefenthaeler HS, Bianchin MD, Marques MS, Nonnenmacher JL, Bender ET, Bender JG, Nery SF, Cichota LC, Külkamp-Guerreiro IC. Omeprazole nanoparticles suspension: development of a stable liquid formulation with a view to pediatric administration. Int J Pharm. 2020;589: 119818. https://doi.org/10.1016/j.ijpharm.2020.119818.
Chen G, Jin D, Jiang X, Qiu Y. Preparation of dopamine nanoparticles and its application in the treatment of neonatal scleredema. Sci Adv Mater. 2021;13:1048–57. https://doi.org/10.1166/sam.2021.4029.
N. Nieto González, G. Cerri, J. Molpeceres, M. Cossu, G. Rassu, P. Giunchedi, E. Gavini, Surfactant-free chitosan/cellulose acetate phthalate nanoparticles: an attempt to solve the needs of captopril administration in paediatrics, Pharmaceuticals 15 (2022) 662. https://doi.org/10.3390/ph15060662.
Nerli G, Gonçalves LMD, Cirri M, Almeida AJ, Maestrelli F, Mennini N, Mura PA. Design, evaluation and comparison of nanostructured lipid carriers and chitosan nanoparticles as carriers of poorly soluble drugs to develop oral liquid formulations suitable for pediatric use. Pharmaceutics. 2023;15:1305. https://doi.org/10.3390/pharmaceutics15041305.
Paliwal R, Paliwal SR, Kenwat R, Kurmi BD, Sahu MK. Solid lipid nanoparticles: a review on recent perspectives and patents. Expert Opin Ther Pat. 2020;30:179–94. https://doi.org/10.1080/13543776.2020.1720649.
M. Cirri, N. Mennini, F. Maestrelli, P. Mura, C. Ghelardini, L. Di Cesare Mannelli, Development and in vivo evaluation of an innovative “hydrochlorothiazide-in cyclodextrins-in solid lipid nanoparticles” formulation with sustained release and enhanced oral bioavailability for potential hypertension treatment in pediatrics, International Journal of Pharmaceutics 521 (2017) 73–83. https://doi.org/10.1016/j.ijpharm.2017.02.022.
Sun D, Zhuang X, Zhang S, Deng Z-B, Grizzle W, Miller D, Zhang H-G. Exosomes are endogenous nanoparticles that can deliver biological information between cells. Adv Drug Deliv Rev. 2013;65:342–7. https://doi.org/10.1016/j.addr.2012.07.002.
Haque S, Vaiselbuh SR. Silencing of exosomal miR-181a reverses pediatric acute lymphocytic leukemia cell proliferation. Pharmaceuticals. 2020;13:241. https://doi.org/10.3390/ph13090241.
Ajnai G, Chiu A, Kan T, Cheng C-C, Tsai T-H, Chang J. Trends of gold nanoparticle-based drug delivery system in cancer therapy. Journal of Experimental & Clinical Medicine. 2014;6:172–8. https://doi.org/10.1016/j.jecm.2014.10.015.
Siddique S, Chow JCL. Gold nanoparticles for drug delivery and cancer therapy. Appl Sci. 2020;10:3824. https://doi.org/10.3390/app10113824.
D. Lima, J. Inaba, L. Clarindo Lopes, G.N. Calaça, P. Los Weinert, R. Lenzi Fogaça, J. Ferreira de Moura, L. Magalhães Alvarenga, B. Cavalcante de Figueiredo, K. Wohnrath, C. Andrade Pessôa, Label-free impedimetric immunosensor based on arginine-functionalized gold nanoparticles for detection of DHEAS, a biomarker of pediatric adrenocortical carcinoma, Biosensors and Bioelectronics 133 (2019) 86–93. https://doi.org/10.1016/j.bios.2019.02.063.
Hanafy NAN, El-Kemary M, Leporatti S. Micelles structure development as a strategy to improve smart cancer therapy. Cancers. 2018;10:238. https://doi.org/10.3390/cancers10070238.
Bukchin A, Pascual-Pasto G, Cuadrado-Vilanova M, Castillo-Ecija H, Monterrubio C, Olaciregui NG, Vila-Ubach M, Ordeix L, Mora J, Carcaboso AM, Sosnik A. Glucosylated nanomicelles target glucose-avid pediatric patient-derived sarcomas. J Control Release. 2018;276:59–71. https://doi.org/10.1016/j.jconrel.2018.02.034.
Chauhan PS, Kumarasamy M, Carcaboso AM, Sosnik A, Danino D. Multifunctional silica-coated mixed polymeric micelles for integrin-targeted therapy of pediatric patient-derived glioblastoma. Mater Sci Eng, C. 2021;128: 112261. https://doi.org/10.1016/j.msec.2021.112261.
Watanabe T, Mizuno HL, Norimatsu J, Obara T, Cabral H, Tsumoto K, Nakakido M, Kawauchi D, Anraku Y. Ligand installation to polymeric micelles for pediatric brain tumor targeting. Polymers. 2023;15:1808. https://doi.org/10.3390/polym15071808.
Khosa A, Reddi S, Saha RN. Nanostructured lipid carriers for site-specific drug delivery. Biomed Pharmacother. 2018;103:598–613. https://doi.org/10.1016/j.biopha.2018.04.055.
Haider M, Abdin SM, Kamal L, Orive G. Nanostructured lipid carriers for delivery of chemotherapeutics: a review. Pharmaceutics. 2020;12:288. https://doi.org/10.3390/pharmaceutics12030288.
Mura P, Maestrelli F, D’Ambrosio M, Luceri C, Cirri M. Evaluation and comparison of solid lipid nanoparticles (SLNs) and nanostructured lipid carriers (NLCs) as vectors to develop hydrochlorothiazide effective and safe pediatric oral liquid formulations. Pharmaceutics. 2021;13:437. https://doi.org/10.3390/pharmaceutics13040437.
M. Cirri, F. Maestrelli, P. Mura, C. Ghelardini, L. Di Cesare Mannelli, Combined approach of cyclodextrin complexationand nanostructured lipid carriers for the development of a pediatric liquid oral dosage form of hydrochlorothiazide, Pharmaceutics 10 (2018) 287. https://doi.org/10.3390/pharmaceutics10040287.
C. Pathak, F.U. Vaidya, S.M. Pandey, Chapter 3 - Mechanism for development of nanobased drug delivery system, in: S.S. Mohapatra, S. Ranjan, N. Dasgupta, R.K. Mishra, S. Thomas (Eds.), Applications of targeted nano drugs and delivery systems, Elsevier, 2019: pp. 35–67. https://doi.org/10.1016/B978-0-12-814029-1.00003-X.
Deng S, Gigliobianco MR, Censi R, Di Martino P. Polymeric nanocapsules as nanotechnological alternative for drug delivery system: current status, challenges and opportunities. Nanomaterials. 2020;10:847. https://doi.org/10.3390/nano10050847.
I. Limayem Blouza, C. Charcosset, S. Sfar, H. Fessi, Preparation and characterization of spironolactone-loaded nanocapsules for paediatric use, International Journal of Pharmaceutics 325 (2006) 124–131. https://doi.org/10.1016/j.ijpharm.2006.06.022.
de Oliveira EG, Cardoso AM, Paese K, Coradini K, de Oliveira CV, Pohlmann AR, Oliveira MS, Guterres SS, Beck RCR. Reconstituted spray-dried phenytoin-loaded nanocapsules improve the in vivo phenytoin anticonvulsant effect and the survival time in mice. Int J Pharm. 2018;551:121–32. https://doi.org/10.1016/j.ijpharm.2018.09.023.
S. Wirsching, M. Machtakova, F. Borgans, L. Pretsch, M. Fichter, M.L. Cacicedo, H. Thérien-Aubin, K. Landfester, S. Gehring, OVA-PEG-R848 nanocapsules stimulate neonatal conventional and plasmacytoid dendritic cells, Frontiers in Pediatrics 10 (2022). https://www.frontiersin.org/articles/https://doi.org/10.3389/fped.2022.966113 (accessed July 31, 2023).
Iravani S, Varma RS. Nanosponges for drug delivery and cancer therapy: recent advances. Nanomaterials. 2022;12:2440. https://doi.org/10.3390/nano12142440.
Rao MRP, Bhingole RC. Nanosponge-based pediatric-controlled release dry suspension of gabapentin for reconstitution. Drug Dev Ind Pharm. 2015;41:2029–36. https://doi.org/10.3109/03639045.2015.1044903.
Omar SM, Ibrahim F, Ismail A. Formulation and evaluation of cyclodextrin-based nanosponges of griseofulvin as pediatric oral liquid dosage form for enhancing bioavailability and masking bitter taste. Saudi Pharmaceutical Journal. 2020;28:349–61. https://doi.org/10.1016/j.jsps.2020.01.016.
Grimaldi N, Andrade F, Segovia N, Ferrer-Tasies L, Sala S, Veciana J, Ventosa N. Lipid-based nanovesicles for nanomedicine. Chem Soc Rev. 2016;45:6520–45. https://doi.org/10.1039/C6CS00409A.
M. Demirci, M.Y. Caglar, B. Cakir, İ. Gülseren, 3 - Encapsulation by nanoliposomes, in: S.M. Jafari (Ed.), Nanoencapsulation technologies for the food and nutraceutical industries, Academic Press, 2017: pp. 74–113. https://doi.org/10.1016/B978-0-12-809436-5.00003-3.
K.M. Aguilar-Pérez, J.I. Avilés-Castrillo, D.I. Medina, R. Parra-Saldivar, H.M.N. Iqbal, Insight into nanoliposomes as smart nanocarriers for greening the twenty-first century biomedical settings, Frontiers in Bioengineering and Biotechnology 8 (2020). https://www.frontiersin.org/articles/https://doi.org/10.3389/fbioe.2020.579536 (accessed August 7, 2023).
Taléns-Visconti R, Díez-Sales O, de Julián-Ortiz JV, Nácher A. Nanoliposomes in cancer therapy: marketed products and current clinical trials. Int J Mol Sci. 2022;23:4249. https://doi.org/10.3390/ijms23084249.
L. Kager, U. Pötschger, S. Bielack, Review of mifamurtide in the treatment of patients with osteosarcoma, Ther Clin Risk Manag 6 (2010) 279–286. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2893760/ (accessed July 22, 2023).
U.A. Fahmy, H. Aldawsari, Combined ceftriaxone sodium with alpha lipoic acid nanoliposomes for more stable, and less nephrotoxic formula in pediatrics, 13 (2018) 245–252. https://www.chalcogen.ro/245_FahmiUA.pdf.
Stewart E, Blankenship K, Freeman B, Federico S, Dyer M. Abstract 6716: Preclinical evaluation of nano-liposomal irinotecan in pediatric solid tumor patient-derived xenografts. Can Res. 2023;83:6716. https://doi.org/10.1158/1538-7445.AM2023-6716.
Bhardwaj P, Tripathi P, Gupta R, Pandey S. Niosomes: a review on niosomal research in the last decade. Journal of Drug Delivery Science and Technology. 2020;56: 101581. https://doi.org/10.1016/j.jddst.2020.101581.
Zidan AS, Hosny KM, Ahmed OAA, Fahmy UA. Assessment of simvastatin niosomes for pediatric transdermal drug delivery. Drug Delivery. 2016;23:1536–49. https://doi.org/10.3109/10717544.2014.980896.
Nayak S, Herzog RW. Progress and prospects: immune responses to viral vectors. Gene Ther. 2010;17:295–304. https://doi.org/10.1038/gt.2009.148.
Parodi A, Molinaro R, Sushnitha M, Evangelopoulos M, Martinez JO, Arrighetti N, Corbo C, Tasciotti E. Bio-inspired engineering of cell- and virus-like nanoparticles for drug delivery. Biomaterials. 2017;147:155–68. https://doi.org/10.1016/j.biomaterials.2017.09.020.
Kanra G, Marchisio P, Feiterna-Sperling C, Gaedicke G, Lazar H, Durrer P, Kürsteiner O, Herzog C, Kara A, Principi N. Comparison of immunogenicity and tolerability of a virosome-adjuvanted and a split influenza vaccine in children. Pediatr Infect Dis J. 2004;23:300. https://doi.org/10.1097/00006454-200404000-00005.
Künzi V, Dornseiff M, Horwath J, Hartmann K. Safe vaccination of children with a virosomal adjuvanted influenza vaccine. Vaccine. 2009;27:1261–5. https://doi.org/10.1016/j.vaccine.2008.12.008.
Van Herck K, Hens A, De Coster I, Vertruyen A, Tolboom J, Sarnecki M, Van Damme P. Long-term antibody persistence in children after vaccination with the pediatric formulation of an aluminum-free virosomal hepatitis A vaccine. Pediatr Infect Dis J. 2015;34: e85. https://doi.org/10.1097/INF.0000000000000616.
Sivadasan D, Sultan MH, Alqahtani SS, Javed S. Cubosomes in drug delivery—a comprehensive review on its structural components, preparation techniques and therapeutic applications. Biomedicines. 2023;11:1114. https://doi.org/10.3390/biomedicines11041114.
World Health Organization, CureAll framework: WHO global initiative for childhood cancer: increasing access, advancing quality, saving lives, World Health Organization, 2021. https://apps.who.int/iris/handle/10665/347370 (accessed June 1, 2023).
Aleassa EM, Xing M, Keijzer R. Nanomedicine as an innovative therapeutic strategy for pediatric cancer. Pediatr Surg Int. 2015;31:611–6. https://doi.org/10.1007/s00383-015-3683-2.
Galluzzi L, Buqué A, Kepp O, Zitvogel L, Kroemer G. Immunogenic cell death in cancer and infectious disease. Nat Rev Immunol. 2017;17:97–111. https://doi.org/10.1038/nri.2016.107.
Cabral H, Kinoh H, Kataoka K. Tumor-targeted nanomedicine for immunotherapy. Acc Chem Res. 2020;53:2765–76. https://doi.org/10.1021/acs.accounts.0c00518.
Quader S, Kataoka K, Cabral H. Nanomedicine for brain cancer. Adv Drug Deliv Rev. 2022;182: 114115. https://doi.org/10.1016/j.addr.2022.114115.
Rosenblum D, Joshi N, Tao W, Karp JM, Peer D. Progress and challenges towards targeted delivery of cancer therapeutics. Nat Commun. 2018;9:1410. https://doi.org/10.1038/s41467-018-03705-y.
Shi J, Kantoff PW, Wooster R, Farokhzad OC. Cancer nanomedicine: progress, challenges and opportunities. Nat Rev Cancer. 2017;17:20–37. https://doi.org/10.1038/nrc.2016.108.
Abballe L, Spinello Z, Antonacci C, Coppola L, Miele E, Catanzaro G, Miele E. Nanoparticles for drug and gene delivery in pediatric brain tumors’ cancer stem cells: current knowledge and future perspectives. Pharmaceutics. 2023;15:505. https://doi.org/10.3390/pharmaceutics15020505.
Cerna T, Stiborova M, Adam V, Kizek R, Eckschlager T. Nanocarrier drugs in the treatment of brain tumors. J Cancer Metastasis Treat. 2016;2:407–16.
Naki T, Aderibigbe BA. Efficacy of polymer-based nanomedicine for the treatment of brain cancer. Pharmaceutics. 2022;14:1048. https://doi.org/10.3390/pharmaceutics14051048.
Udaka YT, Packer RJ. Pediatric brain tumors. Neurol Clin. 2018;36:533–56. https://doi.org/10.1016/j.ncl.2018.04.009.
S. Partap, M. Monje, Pediatric brain tumors, CONTINUUM: Lifelong Learning in Neurology 26 (2020) 1553. https://doi.org/10.1212/CON.0000000000000955.
Segal D, Karajannis MA. Pediatric brain tumors: an update. Curr Probl Pediatr Adolesc Health Care. 2016;46:242–50. https://doi.org/10.1016/j.cppeds.2016.04.004.
Obermeier B, Daneman R, Ransohoff RM. Development, maintenance and disruption of the blood-brain barrier. Nat Med. 2013;19:1584–96. https://doi.org/10.1038/nm.3407.
Guido C, Baldari C, Maiorano G, Mastronuzzi A, Carai A, Quintarelli C, De Angelis B, Cortese B, Gigli G, Palamà IE. Nanoparticles for diagnosis and target therapy in pediatric brain cancers. Diagnostics. 2022;12:173. https://doi.org/10.3390/diagnostics12010173.
M. Alavi, M. Hamidi, Passive and active targeting in cancer therapy by liposomes and lipid nanoparticles, Drug Metabolism and Personalized Therapy 34 (2019). https://doi.org/10.1515/dmpt-2018-0032.
Sharma HS, Muresanu DF, Nozari A, Lafuente JV, Tian ZR, S. Sahib, I. Bryukhovetskiy, A. Bryukhovetskiy, A.D. Buzoianu, R. Patnaik, L. Wiklund, A. Sharma, Chapter one - Pathophysiology of blood-brain barrier in brain tumor. Novel therapeutic advances using nanomedicine, in: I. Bryukhovetskiy, A. Sharma, Z. Zhang, H.S. Sharma (Eds.), International review of neurobiology, Academic Press, 2020: pp. 1–66. https://doi.org/10.1016/bs.irn.2020.03.001.
Power EA, Rechberger JS, Gupta S, Schwartz JD, Daniels DJ, Khatua S. Drug delivery across the blood-brain barrier for the treatment of pediatric brain tumors – an update. Adv Drug Deliv Rev. 2022;185: 114303. https://doi.org/10.1016/j.addr.2022.114303.
El-Shafie S, Fahmy SA, Ziko L, Elzahed N, Shoeib T, Kakarougkas A. Encapsulation of nedaplatin in novel PEGylated liposomes increases its cytotoxicity and genotoxicity against A549 and U2OS human cancer cells. Pharmaceutics. 2020;12:863. https://doi.org/10.3390/pharmaceutics12090863.
Fahmy SA, Dawoud A, Zeinelabdeen YA, Kiriacos CJ, Daniel KA, Eltahtawy O, Abdelhalim MM, Braoudaki M, Youness RA. Molecular engines, therapeutic targets, and challenges in pediatric brain tumors: a special emphasis on hydrogen sulfide and RNA-based nano-delivery. Cancers. 2022;14:5244. https://doi.org/10.3390/cancers14215244.
Kambhampati M, Yadavilli S, McNeeley KM, Pai SB, Yu Q, Bellamkonda R, Fernandes R, Packer RJ, Nazarian J. NI-44liposomal nanoparticles for targeting and imaging of pediatric brain tumors. Neuro Oncol. 2014;16:v147–8. https://doi.org/10.1093/neuonc/nou264.42.
Kievit FM, Stephen ZR, Wang K, Dayringer CJ, Sham JG, Ellenbogen RG, Silber JR, Zhang M. Nanoparticle mediated silencing of DNA repair sensitizes pediatric brain tumor cells to γ-irradiation. Mol Oncol. 2015;9:1071–80. https://doi.org/10.1016/j.molonc.2015.01.006.
Liu Z, Yan H, Li H. Silencing of DNA repair sensitizes pediatric brain tumor cells to γ-irradiation using gold nanoparticles. Environ Toxicol Pharmacol. 2017;53:40–5. https://doi.org/10.1016/j.etap.2017.04.017.
Bell JB, Rink JS, Eckerdt F, Clymer J, Goldman S, Thaxton CS, Platanias LC. HDL nanoparticles targeting sonic hedgehog subtype medulloblastoma. Sci Rep. 2018;8:1211. https://doi.org/10.1038/s41598-017-18100-8.
Buczkowicz P, Hawkins C. Pathology, molecular genetics, and epigenetics of diffuse intrinsic pontine glioma, Frontiers in Oncology 2015;5. https://www.frontiersin.org/articles/10.3389/fonc.2015.00147 (accessed July 16, 2023).
Ung C, Tsoli M, Liu J, Cassano D, Pocoví-Martínez S, Upton DH, Ehteda A, Mansfeld FM, Failes TW, Farfalla A, Katsinas C, Kavallaris M, Arndt GM, Vittorio O, Cirillo G, Voliani V, Ziegler DS. Doxorubicin-loaded gold nanoarchitectures as a therapeutic strategy against diffuse intrinsic pontine glioma. Cancers. 2021;13:1278. https://doi.org/10.3390/cancers13061278.
Cooney TM, Lubanszky E, Prasad R, Hawkins C, Mueller S. Diffuse midline glioma: review of epigenetics. J Neurooncol. 2020;150:27–34. https://doi.org/10.1007/s11060-020-03553-1.
Heravi Shargh V, Luckett J, Bouzinab K, Paisey S, Turyanska L, Singleton WG, Lowis S, Gershkovich P, Bradshaw TD, Stevens MF, Bienemann A. Coyle, Chemosensitization of temozolomide-resistant pediatric diffuse midline glioma using potent nanoencapsulated forms of a N(3)-propargyl analogue. ACS Appl Mater Interfaces. 2021;13:35266–35280. https://doi.org/10.1021/acsami.1c04164.
Shields CL, Shields JA. Basic understanding of current classification and management of retinoblastoma. Curr Opin Ophthalmol. 2006;17:228. https://doi.org/10.1097/01.icu.0000193079.55240.18.
Dimaras H, Kimani K, Dimba EA, Gronsdahl P, White A, Chan HS, Gallie BL. Retinoblastoma. The Lancet. 2012;379:1436–46. https://doi.org/10.1016/S0140-6736(11)61137-9.
Grossniklaus HE. Retinoblastoma. Fifty Years of Progress. The LXXI Edward Jackson Memorial Lecture. Am J Ophthalmol. 2014;158:875–891e1. https://doi.org/10.1016/j.ajo.2014.07.025.
Gary-Bobo M, Mir Y, Rouxel C, Brevet D, Hocine O, Maynadier M, Gallud A, Da Silva A, Mongin O, Blanchard-Desce M, Richeter S, Loock B, Maillard P, Morère A, Garcia M, Raehm L, Durand J-O. Multifunctionalized mesoporous silica nanoparticles for the in vitro treatment of retinoblastoma: drug delivery, one and two-photon photodynamic therapy. Int J Pharm. 2012;432:99–104. https://doi.org/10.1016/j.ijpharm.2012.04.056.
Mitra M, Kandalam M, Rangasamy J, Shankar B, Maheswari UK, Swaminathan S, Krishnakumar S. Novel epithelial cell adhesion molecule antibody conjugated polyethyleneimine-capped gold nanoparticles for enhanced and targeted small interfering RNA delivery to retinoblastoma cells. Mol Vis. 2013;19:1029–1038. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3654846/ (accessed August 2, 2023).
Ahmed F, Ali MJ, Kondapi AK. Carboplatin loaded protein nanoparticles exhibit improve anti-proliferative activity in retinoblastoma cells. Int J Biol Macromol. 2014;70:572–82. https://doi.org/10.1016/j.ijbiomac.2014.07.041.
Gallud A, Warther D, Maynadier M, Sefta M, Poyer F, Thomas CD, Rouxel C, Mongin O, Blanchard-Desce M, Morère A, Raehm L, Maillard P, Durand JO, Garcia M, Gary-Bobo M. Identification of MRC2 and CD209 receptors as targets for photodynamic therapy of retinoblastoma using mesoporous silica nanoparticles. RSC Adv. 2015;5:75167–72. https://doi.org/10.1039/C5RA14640B.
Kalmodia S, Parameswaran S, Ganapathy K, Yang W, Barrow CJ, Kanwar JR, Roy K, Vasudevan M, Kulkarni K, Elchuri SV, Krishnakumar S. Characterization and molecular mechanism of peptide-conjugated gold nanoparticle inhibiting p53-HDM2 interaction in retinoblastoma. Molecular Therapy - Nucleic Acids. 2017;9:349–64. https://doi.org/10.1016/j.omtn.2017.10.012.
Tabatabaei SN, Derbali RM, Yang C, Superstein R, Hamel P, Chain JL, Hardy P. Co-delivery of miR-181a and melphalan by lipid nanoparticles for treatment of seeded retinoblastoma. J Control Release. 2019;298:177–85. https://doi.org/10.1016/j.jconrel.2019.02.014.
N’Diaye M, Vergnaud-Gauduchon J, Nicolas V, Faure V, Denis S, Abreu S, Chaminade P, Rosilio V. Hybrid lipid polymer nanoparticles for combined chemo- and photodynamic therapy. Mol Pharmaceutics. 2019;16:4045–58. https://doi.org/10.1021/acs.molpharmaceut.9b00797.
Sims LB, Tyo KM, Stocke S, Mahmoud MY, Ramasubramanian A, Steinbach-Rankins JM. Surface-modified melphalan nanoparticles for intravitreal chemotherapy of retinoblastoma. Invest Ophthalmol Vis Sci. 2019;60:1696–705. https://doi.org/10.1167/iovs.18-26251.
Li Z, Guo Z, Chu D, Feng H, Zhang J, Zhu L, Li J. Effectively suppressed angiogenesis-mediated retinoblastoma growth using celastrol nanomicelles. Drug Delivery. 2020;27:358–66. https://doi.org/10.1080/10717544.2020.1730522.
Moradi S, Mokhtari-Dizaji M, Ghassemi F, Sheibani S, Amoli FA. The effect of ultrasound hyperthermia with gold nanoparticles on retinoblastoma Y79 cells. Gold Bull. 2020;53:111–20. https://doi.org/10.1007/s13404-020-00279-w.
Godse R, Rathod M, De A, Shinde U. Intravitreal galactose conjugated polymeric nanoparticles of etoposide for retinoblastoma. Journal of Drug Delivery Science and Technology. 2021;61: 102259. https://doi.org/10.1016/j.jddst.2020.102259.
Guo Z, Shi L, Feng H, Yang F, Li Z, Zhang J, Jin L, Li J. Reduction-sensitive nanomicelles: delivery celastrol for retinoblastoma cells effective apoptosis. Chin Chem Lett. 2021;32:1046–50. https://doi.org/10.1016/j.cclet.2020.03.066.
Delrish E, Jabbarvand M, Ghassemi F, Amoli FA, Atyabi F, Lashay A, Soleimani M, Aghajanpour L, Dinarvand R. Efficacy of topotecan nanoparticles for intravitreal chemotherapy of retinoblastoma. Exp Eye Res. 2021;204: 108423. https://doi.org/10.1016/j.exer.2020.108423.
Narayana RVL, Jana P, Tomar N, Prabhu V, Nair RM, Manukonda R, Kaliki S, Coupland SE, Alexander J, Kalirai H, Kondapi AK, Vemuganti GK. Carboplatin- and etoposide-loaded lactoferrin protein nanoparticles for targeting cancer stem cells in retinoblastoma in vitro. Invest Ophthalmol Vis Sci. 2021;62:13. https://doi.org/10.1167/iovs.62.14.13.
Mudigunda SV, Pemmaraju DB, Paradkar S, Puppala ER, Gawali B, Upadhyayula SM, Vegi Gangamodi N, Rengan AK. Multifunctional polymeric nanoparticles for chemo/phototheranostics of retinoblastoma. ACS Biomater Sci Eng 2022;8:151–160. https://doi.org/10.1021/acsbiomaterials.1c01234.
Kartha B, Thanikachalam K, Vijayakumar N, Alharbi NS, Kadaikunnan S, Khaled JM, Gopinath K, Govindarajan M. Synthesis and characterization of Ce-doped TiO2 nanoparticles and their enhanced anticancer activity in Y79 retinoblastoma cancer cells. Green Processing and Synthesis. 2022;11:143–9. https://doi.org/10.1515/gps-2022-0011.
Krishnan V, Xu X, Barwe SP, Yang X, Czymmek K, Waldman SA, Mason RW, Jia X, Rajasekaran AK. Dexamethasone-loaded block copolymer nanoparticles induce leukemia cell death and enhance therapeutic efficacy: a novel application in pediatric nanomedicine. Mol Pharmaceutics. 2013;10:2199–210. https://doi.org/10.1021/mp300350e.
Wiesmann N, Tremel W, Brieger J. Zinc oxide nanoparticles for therapeutic purposes in cancer medicine. J Mater Chem B. 2020;8:4973–89. https://doi.org/10.1039/D0TB00739K.
Anjum S, Hashim M, Malik SA, Khan M, Lorenzo JM, Abbasi BH, Hano C. Recent advances in zinc oxide nanoparticles (ZnO NPs) for cancer diagnosis, target drug delivery, and treatment. Cancers. 2021;13:4570. https://doi.org/10.3390/cancers13184570.
Connerty P, Moles E, de Bock CE, Jayatilleke N, Smith JL, Meshinchi S, Mayoh C, Kavallaris M, Lock RB. Development of siRNA-loaded lipid nanoparticles targeting long non-coding RNA LINC01257 as a novel and safe therapeutic approach for t(8;21) pediatric acute myeloid leukemia. Pharmaceutics. 2021;13:1681. https://doi.org/10.3390/pharmaceutics13101681.
Taran SJ, Taran R, Malipatil NB. Pediatric osteosarcoma: an updated review, Indian J Med Paediatr. Oncol. 2017;38:33–43. https://doi.org/10.4103/0971-5851.203513.
Wagner LM, Yin H, Eaves D, Currier M, Cripe TP. Preclinical evaluation of nanoparticle albumin-bound paclitaxel for treatment of pediatric bone sarcoma. Pediatr Blood Cancer. 2014;61:2096–8. https://doi.org/10.1002/pbc.25062.
Ni M, Xiong M, Zhang X, Cai G, Chen H, Zeng Q, Yu Z. Poly(lactic-co-glycolic acid) nanoparticles conjugated with CD133 aptamers for targeted salinomycin delivery to CD133+ osteosarcoma cancer stem cells. Int J Nanomed. 2015;10:2537–54. https://doi.org/10.2147/IJN.S78498.
Haghiralsadat F, Amoabediny G, Sheikhha MH, Forouzanfar T, Helder MN, Zandieh-Doulabi B. A novel approach on drug delivery: investigation of a new nano-formulation of liposomal doxorubicin and biological evaluation of entrapped doxorubicin on various osteosarcoma cell lines. Cell J. 2017;19:55–65. https://doi.org/10.22074/cellj.2017.4502.
González-Fernández Y, Brown HK, Patiño-García A, Heymann D, Blanco-Prieto MJ. Oral administration of edelfosine encapsulated lipid nanoparticles causes regression of lung metastases in pre-clinical models of osteosarcoma. Cancer Lett. 2018;430:193–200. https://doi.org/10.1016/j.canlet.2018.05.030.
Zhang J, Miao Y, Ni W, Xiao H, Zhang J. Cancer cell membrane coated silica nanoparticles loaded with ICG for tumour specific photothermal therapy of osteosarcoma. Artificial Cells, Nanomedicine, and Biotechnology. 2019;47:2298–305. https://doi.org/10.1080/21691401.2019.1622554.
Rodríguez-Nogales C, Moreno H, Zandueta C, Desmaële D, Lecanda F, Couvreur P, Blanco-Prieto MJ. Combinatorial nanomedicine made of squalenoyl-gemcitabine and edelfosine for the treatment of osteosarcoma. Cancers. 2020;12:1895. https://doi.org/10.3390/cancers12071895.
Xu Y, Qi J, Sun W, Zhong W, Wu H. Therapeutic effects of zoledronic acid-loaded hyaluronic acid/polyethylene glycol/nano-hydroxyapatite nanoparticles on osteosarcoma. Front bioeng biotechnol. 2022;10. https://www.frontiersin.org/articles/10.3389/fbioe.2022.897641 (accessed January 12, 2024).
Katta SS, Nagati V, Paturi ASV, Murakonda SP, Murakonda AB, Pandey MK, Gupta SC, Pasupulati AK, Challagundla KB. Neuroblastoma: emerging trends in pathogenesis, diagnosis, and therapeutic targets. J Control Release. 2023;357:444–59. https://doi.org/10.1016/j.jconrel.2023.04.001.
Sagnella SM, Trieu J, Brahmbhatt H, MacDiarmid JA, MacMillan A, Whan RM, Fife CM, McCarroll JA, Gifford AJ, Ziegler DS, Kavallaris M. Targeted doxorubicin-loaded bacterially derived nano-cells for the treatment of neuroblastoma. Mol Cancer Ther. 2018;17:1012–23. https://doi.org/10.1158/1535-7163.MCT-17-0738.
WHO, World health statistics 2023: monitoring health for the SDGs, sustainable development goals, World Health Organization (2023). https://www.who.int/publications-detail-redirect/9789240074323 (accessed July 28, 2023).
Yeh YC, Huang TH, Yang SC, Chen CC, Fang JY. Nano-based drug delivery or targeting to eradicate bacteria for infection mitigation: a review of recent advances, Front Chem. 2020;8. https://www.frontiersin.org/articles/10.3389/fchem.2020.00286 (accessed July 28, 2023).
Kirtane AR, Verma M, Karandikar P, Furin J, Langer R, Traverso G. Nanotechnology approaches for global infectious diseases. Nat Nanotechnol. 2021;16:369–84. https://doi.org/10.1038/s41565-021-00866-8.
Sun Y, Chen D, Pan Y, Qu W, Hao H, Wang X, Liu Z, Xie S. Nanoparticles for antiparasitic drug delivery. Drug Delivery. 2019;26:1206–21. https://doi.org/10.1080/10717544.2019.1692968.
Bajwa HU, Khan MK, Abbas Z, Riaz R, Rehman TU, Abbas RZ, Aleem MT, Abbas A, Almutairi MM, Alshammari FA, Alraey Y. Nanoparticles: synthesis and their role as potential drug candidates for the treatment of parasitic diseases. Life. 2022;12:750. https://doi.org/10.3390/life12050750.
Pediatric malaria: background, etiology. epidemiology. 2022. https://emedicine.medscape.com/article/998942-overview?form=fpf (accessed January 11, 2024).
Dandagi PM, Rath SP, Gadad AP, Mastiholimath VS. Taste masked quinine sulphate loaded solid lipid nanoparticles for flexible pediatric dosing. Indian Journal of Pharmaceutical Education and Research. 2014;48:93–9.
Tang W-L, Tang W-H, Chen WC, Diako C, Ross CF, Li S-D. Development of a rapidly dissolvable oral pediatric formulation for mefloquine using liposomes. Mol Pharmaceutics. 2017;14:1969–79. https://doi.org/10.1021/acs.molpharmaceut.7b00077.
Münster M, Mohamed-Ahmed AHA, Immohr LI, Schoch C, Schmidt C, Tuleu C, Breitkreutz J. Comparative in vitro and in vivo taste assessment of liquid praziquantel formulations. Int J Pharm. 2017;529:310–8. https://doi.org/10.1016/j.ijpharm.2017.06.084.
Kokaliaris C, Garba A, Matuska M, Bronzan RN, Colley DG, Dorkenoo AM, Ekpo UF, Fleming FM, French MD, Kabore A, Mbonigaba JB, Midzi N, Mwinzi PNM, N’Goran EK, Polo MR, Sacko M, Tchuenté L-AT, Tukahebwa EM, Uvon PA, Yang G, Wiesner L, Zhang Y, Utzinger J, Vounatsou P. Effect of preventive chemotherapy with praziquantel on schistosomiasis among school-aged children in sub-Saharan Africa: a spatiotemporal modelling study. Lancet Infect Dis. 2022;22:136–49. https://doi.org/10.1016/S1473-3099(21)00090-6.
Gonzalez MA, Ramírez Rigo MV, González Vidal NL. Orphan formulations in pediatric schistosomiasis treatment: development and characterization of praziquantel nanoparticle—loaded powders for reconstitution. AAPS Pharm Sci Tech. 2019;20:318. https://doi.org/10.1208/s12249-019-1548-z.
Traynor K. Benznidazole approved for Chagas disease in children. Am J Health Syst Pharm. 2017;74:1519. https://doi.org/10.2146/news170065.
Lidani KC, Andrade FA, Bavia L, Damasceno FS, Beltrame MH, Messias-Reason IJ, Sandri TL. Chagas disease: from discovery to a worldwide health problem. Front Public Health. 2019;7. https://www.frontiersin.org/articles/10.3389/fpubh.2019.00166 (accessed July 23, 2023).
Seremeta KP, Arrúa EC, Okulik NB, Salomon CJ. Development and characterization of benznidazole nano- and microparticles: a new tool for pediatric treatment of Chagas disease? Colloids Surf, B. 2019;177:169–77. https://doi.org/10.1016/j.colsurfb.2019.01.039.
Good R, Scherbak D. Fascioliasis in: StatPearls StatPearls. Publishing Treasure Island (FL). 2023. http://www.ncbi.nlm.nih.gov/books/NBK537032/ (accessed July 23, 2023).
Daware S, Patki M, Saraswat A, Palekar S, Patel K. Development of a safe pediatric liquisolid self-nanoemulsifying system of triclabendazole for the treatment of fascioliasis. Int J Pharm. 2022;626: 122163. https://doi.org/10.1016/j.ijpharm.2022.122163.
Uribe-Restrepo A, Cossio A, Desai MM, Dávalos D, del Castro MM. Interventions to treat cutaneous leishmaniasis in children: a systematic review. PLoS Negl Trop Dis. 2018;12: e0006986. https://doi.org/10.1371/journal.pntd.0006986.
Erat T, An I. Treatment of pediatric cutaneous leishmaniasis with liposomal amphotericin B. Dermatol Ther. 2022;35: e15706. https://doi.org/10.1111/dth.15706.
Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, Colombara DV, Ikuta KS, Kissoon N, Finfer S, Fleischmann-Struzek C, Machado FR, Reinhart KK, Rowan K, Seymour CW, Watson RS, West TE, Marinho F, Hay SI, Lozano R, Lopez AD, Angus DC, Murray CJL, Naghavi M. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395:200–11. https://doi.org/10.1016/S0140-6736(19)32989-7.
Lin T, Qin T, Jiang S, Zhang C, Wang L. Anti-inflammatory and anti-biotic drug metronidazole loaded ZIF-90 nanoparticles as a pH responsive drug delivery system for improved pediatric sepsis management. Microb Pathog. 2023;176: 105941. https://doi.org/10.1016/j.micpath.2022.105941.
Alter SJ, Bennett JS, Koranyi K, Kreppel A, Simon R. Common childhood viral infections. Curr Probl Pediatr Adolesc Health Care. 2015;45:21–53. https://doi.org/10.1016/j.cppeds.2014.12.001.
Auriti C, De Rose DU, Santisi A, Martini L, Piersigilli F, Bersani I, Ronchetti MP, Caforio L. Pregnancy and viral infections: mechanisms of fetal damage, diagnosis and prevention of neonatal adverse outcomes from cytomegalovirus to SARS-CoV-2 and Zika virus. Biochim Biophys Acta Mol Basis Dis. 2021;1867: 166198. https://doi.org/10.1016/j.bbadis.2021.166198.
Justiz Vaillant AA, Gulick PG. HIV disease current practice in: StatPearls, StatPearls Publishing. Treasure Island (FL). 2023. http://www.ncbi.nlm.nih.gov/books/NBK534860/ (accessed July 27, 2023).
WHO. HIV data and statistics. WHO 2023. https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics (accessed July 27, 2023).
Chiappetta DA, Hocht C, Taira C, Sosnik A. Efavirenz-loaded polymeric micelles for pediatric anti-HIV pharmacotherapy with significantly higher oral bioavailability. Nanomedicine. 2010;5:11–23. https://doi.org/10.2217/nnm.09.90.
Zidan AS, Rahman Z, Khan MA. Product and process understanding of a novel pediatric anti-HIV tenofovir niosomes with a high-pressure homogenizer. Eur J Pharm Sci. 2011;44:93–102. https://doi.org/10.1016/j.ejps.2011.06.012.
Moretton MA, Taira C, Flor S, Bernabeu E, Lucangioli S, Höcht C, Chiappetta DA. Novel nelfinavir mesylate loaded d-α-tocopheryl polyethylene glycol 1000 succinate micelles for enhanced pediatric anti HIV therapy: in vitro characterization and in vivo evaluation. Colloids Surf, B. 2014;123:302–10. https://doi.org/10.1016/j.colsurfb.2014.09.031.
Dharshini KP, Devi RD, Banudevi S, Narayanan VHB. In-vivo pharmacokinetic studies of dolutegravir loaded spray dried chitosan nanoparticles as milk admixture for paediatrics infected with HIV. Sci Rep. 2022;12:13907. https://doi.org/10.1038/s41598-022-18009-x.
Guedes MDV, Marques MS, Berlitz SJ, Facure MHM, Correa DS, Steffens C, Contri RV, Külkamp-Guerreiro IC. Lamivudine and zidovudine-loaded nanostructures: green chemistry preparation for pediatric oral administration. Nanomaterials. 2023;13:770. https://doi.org/10.3390/nano13040770.
Lizzo JM, Cortes S. Pediatric asthma in: StatPearls StatPearls Publishing Treasure Island (FL). 2023. http://www.ncbi.nlm.nih.gov/books/NBK551631/ (accessed July 24, 2023).
Chen Y-D, Liang Z-Y, Cen Y-Y, Zhang H, Han M-G, Tian Y-Q, Zhang J, Li S-J, Yang D-S. Development of oral dispersible tablets containing prednisolone nanoparticles for the management of pediatric asthma. Drug Des Devel Ther. 2015;9:5815–25. https://doi.org/10.2147/DDDT.S86075.
Li H, Yao Y, Fu H. Novel pediatric suspension of nanoparticulate zafirlukast for the treatment of asthma: assessment and evaluation in animal model. Micro & Nano Letters. 2021;16:485–91. https://doi.org/10.1049/mna2.12078.
Funding
This work was supported through Research Establishment Grants awarded by the Faculty of Health and College of Pharmacy, Dalhousie University (Grant ID: R34000).
Author information
Authors and Affiliations
Contributions
Saba Abedin: writing — original draft; writing — review and editing; investigation; methodology; visualization. Oluwatoyin A. Adeleke: conceptualization; methodology; visualization; writing — original draft; writing — review and editing; funding acquisition; project administration; supervision.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders. The authors approved the submitted version of the manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Abedin, S., Adeleke, O.A. State of the art in pediatric nanomedicines. Drug Deliv. and Transl. Res. 14, 2299–2324 (2024). https://doi.org/10.1007/s13346-024-01532-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13346-024-01532-x