
Abstract
p16 is overexpressed in oral squamous cell carcinoma patients who are positive for human papilloma virus. The p53 tumor suppressor gene is commonly mutated in human cancer. The aim is to correlate clinical and pathological features with p16 and p53 expression. This is a prospective, observational study of 50 consecutive cases (43 males and 7 females) who underwent surgery for oral cancer. p16 and p53 were determined by immunohistological staining. The results were obtained and analyzed using chi-square test (Statistical Software SPSS 21.0 version); p value ≤ 0.05 was considered significant. Of the 50 cases, p16 and p53 were overexpressed in 30% and 54% of patients, respectively. Overexpression of p16 was not significantly associated with age, subsites of oral cavity, or degree of differentiation. However, smokeless tobacco was significantly associated with p16 expression (p = 0.012). Similarly, overexpression of p53 was not correlated with age, subsites of oral cavity, or degree of differentiation. Seventy-five percent of poorly differentiated cancers had overexpression of p53 though this did not reach statistical significance (p = 0.279). p53 was overexpressed in smokers (80.95%) and those consuming alcohol (60%).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Oral squamous cell carcinoma (OSCC) is characterized by mortality and morbidity rates that have changed little despite advances in the field of oncology.
Human papilloma virus (HPV) is now identified as a risk factor for oral cancer and is associated with overexpression of p16. These tumors have better survival following surgery and radiotherapy. Globally, the incidence of HPV varies across head and neck cancers, fluctuating from 3% in oral cavity to 12% in oropharyngeal cancers [1]. This site-based variance is attributable to sexual practices and addictions. In India, the incidence of HPV ranges from 0 to 74% in oral cancers and 26 to 70% in oropharyngeal cancers [2]. The p16 marker may mediate its effects by contributing to reduced proliferative capacity, leading to smaller tumor size and lower invasive potential [3].
TP53 is a tumor suppressor gene located on chromosome 17p. One of the most common events in human carcinogenesis is mutation in p53. The defective, mutated protein accumulates inside cancer cells and can be detected by immunohistochemical methods. Overexpression of p53 in oral cancer portends poor prognosis and resistance to chemotherapy. p53 overexpression in oral cancer varies in different parts of the world, owing to divergent risk factors and pathogenesis of the disease. Studies conducted in India [4] report 85.6% p53 overexpression in locally advanced oral cancers.
Material and Methods
The study was conducted at the Department of Surgical Oncology, Army Hospital (Research & Referral), New Delhi. This center provides comprehensive cancer care along with the Departments of Medical Oncology, Radiation Oncology, Oncopathology, and others.
Fifty consecutive cases with oral cancer who underwent primary surgical treatment between April 2017 and April 2019 were selected. We had 43 men and 7 women in our study group. Specimens were fixed in 10% formalin for grossing and further processing as per the College of American Pathologists (CAP) protocol. Slides were stained with routine H&E and other special methods when required. Immunohistochemistry (IHC) was carried out on poly-l-lysine-coated slides. A p16 antibody 584A4 clone was used which identified p16 of human origin. The p53 antibody used was DO-7 clone which recognized 1–45 amino acids of p53 human origin.
Evaluation of Immunohistochemistry
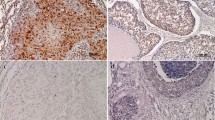
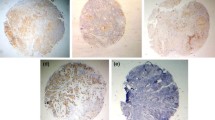
Immunohistochemical staining was examined by light microscopy for confirmation. IHC positivity was assessed by visualization of cytoplasmic and/or nuclear staining by the distinct brown color of oxidized DAB (3,3′-diaminobenzidine). The intensity was analyzed subsequently along with the tumor grade. The respective positive controls were evaluated for the correctness of the procedure.
Immunohistochemistry Studies
The proportion of malignant cell staining positively for the IHC markers was quantified using Detre’s quickscore method [5], from 1 through 6. This score was termed category A. The whole section was then scanned at low power in order to gauge the general level of intensity throughout. The average intensity was termed as category B and graded from 0 through 3 based on no staining to weak, moderate, or strong staining. An addition of scores in categories A and B yielded the additive quickscore. The product of A and B yielded a multiplicative quickscore. A positive cutoff quick score is ≥ 3.
Statistical Methods
Descriptive and inferential statistics with chi-square test for categorical data and Pearson correlation were used to see relationship between variables. Statistical Software SPSS 21.0 version was used in analysis. Statistical significance was considered when p value ≤ 0.05.
Ethical Consideration
All patients received standard of care as per international NCCN guidelines. No patient was treated with any non-standard or experimental therapy. Approval from institutional ethical and scientific committee has been obtained.
Results
We studied 50 consecutive patients. The mean age was 56 years, with a range of 31 to 83 years. Most patients were in the age group of 40–70 years (78%). Male-to-female ratio was 6.1:1. All our patients had a non-healing ulcer at presentation and 80% complained of pain in the ulcer.
Oral tongue was the most common site of primary tumor (48%) followed by buccal mucosa (16%), gingivobuccal sulcus (14%), lower alveolus (8%), retromolar trigone (8%), gingivolabial sulcus (4%), and floor of mouth (2%).
Eighty-six percent of our patients had used tobacco in one form or another (smoking 30% and smokeless tobacco 36%). Alcohol was an additive risk factor in 20% of tobacco users.
Only 6% of patients presented with early T1 tumors. Forty-six percent had ulcers ranging from 2 to 4 cm (T2), while another 46% had locally advanced T4 tumors. On clinical examination and imaging, 46% of patients were of N0 status.
All patients underwent wide local excision of lesion with nodal dissection either in the form of SOHND or MRND. Surgery was performed in all cases by a qualified and experienced oncosurgeon with proper oncological margins. Defect was closed primarily in 56% cases, mainly in oral tongue. Reconstruction was individualized to PMMC (18%), free fibular graft reconstruction (20%), anterolateral thigh flap (4%), and radial artery based forearm flap (2%). MRND (levels I–V) was done in 59.65%, SOHND (levels I–III) in 38.60%. The mean harvest of lymph nodes was 29.32 ± 9.95 in MRND and 18.64 ± 8.69 in SOHND.
p16 and p53 were overexpressed in 30% and 54% of patients, respectively.
There was no significant association between p16 expression and age; 82.33% of patients who were p16-negative were of age < 40 years (p = 0.654). Similarly, subsites of oral cavity and degree of differentiation of tumor were also not related to p16 expression. Fifty percent of alcohol users and 80.95% of smokers were p16-negative; hence, both risk factors were not significantly associated with p16. However, smokeless tobacco was significantly associated with p16 expression (p = 0.012). The correlation of p16 expression with various clinical and pathological factors is depicted in Table 1.
There was no significant association between p53 expression and age; 24 out of 44 patients aged ≥ 40 years were p53-positive (p = 1.000). Subsites of oral cavity and degree of differentiation of tumor were also not related to p53 expression. However, 75% of poorly differentiated tumors overexpressed p53.
p53 expression was high in smokers (80.95%) and those consuming alcohol (60%). Smoking was significantly associated with p53 (p = 0.002); however, association with alcohol did not reach statistical significance (p = 0.736). Smokeless tobacco was also significantly associated with p53 expression (p = 0.005). Correlation of p53 expression with various clinical and pathological factors is depicted in Table 2.
Discussion
p53 Expression
The p53 gene, located on chromosome 17p13.1 encodes a 53-kDa 393 amino acid nuclear phosphoprotein known to regulate cell growth and proliferation. Alteration or inactivation of the wild type of gene product is thought to play an important role in multistep carcinogenesis. The p53 tumor suppressor gene is commonly mutated in human cancers and is in the forefront of oral cancer research.
In the present series of primary oral squamous cell carcinomas, p53 phosphoprotein was detectable by immunohistochemistry (IHC) in 54% of cases. The prevalence of p53 positivity in our study was compared with findings of other Indian investigators. A wide variation is noticeable in the percentage of p53 overexpression in oral carcinomas. Ghanghoria S et al. [6] and Dave KV [7] found p53 in 64% and 65% of Indian population, respectively.
Seventy-five percent of poorly differentiated carcinomas in our study were p53-positive. However, p53 mutation and degree of differentiation were not significantly associated (p = 0.279). p53 is significantly associated with both smoking and smokeless tobacco (p = 0.002 and p = 0.005, respectively). Similar observations were made by Gatoo MA el al. [8] in their study in north Indian population. They observed that p53 expression was associated with smoking and smokeless tobacco (p = 0.029). Importantly, p53 was related neither to alcohol nor to advancing age in our study.
p16 Expression
Human papillomavirus (HPV)–associated head and neck squamous cell cancers (HNSCC) have become increasingly common in the West, but the same cannot be said about India. These cancers have a different biology and confer a better prognosis. The current role of HPV testing in the management of patients in India is not clearly defined. HPV integration and transcription of viral oncoprotein induce overexpression of p16. Immunohistochemically, expression of p16 can be used as a surrogate marker of HPV.
In our study, 30% of the patients were HPV-positive based on p16 expression. This is in line with other studies in Indians from different regions. Prevalence of HPV in squamous cell carcinomas (SCC) of the oral cavity in India has been reported to be 33.6% in the Eastern region [9], 48% in South India [10], 15% in West India [11], and 27.5% in Central India [12].
In our study, 83.3% of the patients under 40 years were p16-negative which contradicts western literature where p16 expression is more common in younger patients. However, we found no significant association between p16 expression and age (p = 0.654), and site of tumor (p = 0.980). We found that p16 expression was significantly associated with smokeless tobacco (p = 0.012); however, it was not related to smoking or alcohol. Similar results were found in a study done by Ralli M et al. [13]. They observed that smokeless tobacco was statically associated with p16 expression (p = 0.03) and was not associated with alcohol intake (p = 0.308). No statistically significant association of p16 expression and nodal metastasis was found in our study.
Hence, overexpression of p53 is more likely to be found in tobacco users and poorly differentiated tumors, signifying a poorer outcome. Overexpression of p16, as a marker of HPV, is associated with use of smokeless tobacco. Neither is affected by the site of tumor or involvement of nodes.
References
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55:74–108
Patel KR, Vajaria BN, Begum R, Desai A, Patel JB, Shah FD et al (2014) Prevalence of high-risk human papillomavirus type 16 and 18 in oral and cervical cancers in population from Gujarat, West India. J Oral Pathol Med 43:293–297
Capote A, Escorial V, Muñoz-Guerra MF, Rodríguez-Campo FJ, Gamallo C et al (2007) Elective neck dissection in early-stage oral squamous cell carcinoma- -does it influence recurrence and survival? Head Neck 29:3–11
Khan H, Gupta S, Husain N, Misra S, Mps N, Jamal N, Ghatak A (2014) Correlation between expressions of cyclin-D1, EGFR and p53 with chemoradiation response in patients of locally advanced oral squamous cell carcinoma. BBA Clin 21(3):11–17
Detre S, Saclani Jotti G, Dowsett M (1995) A “quickscore” method for immunohistochemical semiquantitation: validation for oestrogen receptor in breast carcinomas. J Clin Pathol 48(9):876–878
Ghanghoria S, Ghanghoria A, Shukla A (2015) p53 expression in oral cancer: a study of 50 cases. J Pathol Nepal 5(9):747–751
Dave KV, Chalishazar M, Dave VR, Panja P, Singh M, Modi TG (2016) Immunohistochemical expression of p53 and its clinicopathological correlation with modified Anneroth’s histological grading system. J Oral Maxillofac Pathol 20(1):29
Gatoo MA, Dar AM, Siddiqui M (2018) Correlation of p53 expression with different histological grades in oral squamous cell carcinoma patients from northern India. Am J Cancer Sci 6(1):1–4
Nagpal JK, Patnaik S, Das BR (2002) Prevalence of high-risk human papilloma virus types and its association with P53 codon 72 polymorphism in tobacco addicted oral squamous cell carcinoma (OSCC) patients of Eastern India. Int J Cancer 97:649–653
Elango KJ, Suresh A, Erode EM, Subhadradevi L, Ravindran HK, Iyer SK et al (2011) Role of human papilloma virus in oral tongue squamous cell carcinoma. Asian Pac J Cancer Prev 12:889–896
D’Costa J, Saranath D, Dedhia P, Sanghvi V, Mehta AR (1998) Detection of HPV-16 genome in human oral cancers and potentially malignant lesions from India. Oral Oncol 34:413–420
Gheit T, Vaccarella S, Schmitt M, Pawlita M, Franceschi S, Sankaranarayanan R et al (2009) Prevalence of human papillomavirus types in cervical and oral cancers in central India. Vaccine. 27:636–639
Ralli M, Singh S, Yadav SP, Sharma N, Verma R, Sen R (2016) Assessment and clinicopathological correlation of p16 expression in head and neck squamous cell carcinoma. J Cancer Res Ther 12(1):232
Acknowledgments
The authors acknowledge the support of the Dept’s of Pathology, Radiation Oncology, Medical Oncology, Anaesthesiology and the Administration in carrying out this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Approval from institutional ethical and scientific committee has been obtained.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Agarwal, V.K., Sharma, R., Gahlot, G. et al. Clinical and Histopathological Correlation of p16 and p53 Expression in Oral Cancer. Indian J Surg Oncol 12 (Suppl 1), 164–168 (2021). https://doi.org/10.1007/s13193-020-01145-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-020-01145-z