
Abstract
Although the general assumption is that patient navigation helps patients adhere to CRC screening recommendations, concrete evidence for its effectiveness is still currently under investigation. The present literature review was conducted to explore effectiveness of patient navigation and education on colorectal cancer (CRC) screening completion in medically underserved populations. Data collection included PubMed, Google Scholar, and Cochrane reviews searches. Study inclusion criteria included randomized controlled trials and prospective investigations that included an intervention and control group. Case series, brief communications, commentaries, case reports, and uncontrolled studies were excluded. Twenty-seven of the 36 studies screened for relevance were selected for inclusion. Most studies explored the utility of lay and clinic-based patient navigation. Others implemented interventions that included tailored messaging, and culturally and linguistically appropriate outreach and education efforts to meet CRC screening needs of medically underserved individuals. More recent studies have begun to conduct cost-effectiveness analyses of patient navigation programs that impacted CRC screening and completion. Peer-reviewed publications consistently indicate a positive impact of patient navigation programs on CRC screening completion, as well have provided preliminary evidence for their cost-effectiveness.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Burden of Colorectal Cancer
In the USA, colorectal cancer (CRC) is the third most common cancer in both men and women [1]. The overall incidence of CRC in Harris County Texas is 41.8 per 100,000, which is higher compared to the Texas incidence of 40.2 per 100,000 [15]. This is much higher than the goal of 38.6 per 100,000 recommended by the Centers for Disease Control (CDC) and Prevention and the National Institute of Health (NIH) in the Healthy People 2020 objectives [35]. CRC is the second leading cause of cancer-related deaths among male and female residents of Harris County. In 2015, the number of new cases of CRC in Harris County was projected at 1055 (men, 570; women, 485) with 459 deaths [15].
CRC disproportionately affects African Americans; the overall age-adjusted incidence for CRC in African Americans in Harris County is 54.0 per 100,000 (68.2 per 100,000 men and 44.5 per 100,000 women). Furthermore, worse CRC outcomes are observed in African American women, possibly because of more aggressive tumors [33], which result in earlier distant spread, and ultimately death. CRC is the second most common type of new cancer diagnosed in Hispanics (41.8 per 100,000 men and 28.2 per 100,000 women). For Asians, CRC ranks third (42.4 per 100,000 men and 23.5 per 100,000 women). For non-Hispanic whites, CRC also ranks third in new cancers (51.7 per 100,000 men and 34.6 per 100,000 women). The overall mortality rate from CRC in Harris County is 15.6% (based on data from 2008 to 2012) [33]. This is higher than the goal of 14.5% that the CDC and NIH have put forth in the Healthy People 2020 objectives [35]. Other than biological factors, the prevalent view for differences in CRC incidence include delay in diagnosis, lack of insurance, and lack of knowledge and understanding about the benefits of early initiation of CRC screening. Additionally, previous experiences resulting in lack of trust in health care systems, and cultural beliefs about cancer, have been shown to contribute to major gaps in essential CRC screening services [3, 12, 22, 31]. For example, findings from community-based cancer screening interventions indicate a general sense of fatalism among African Americans regarding CRC outcomes [2, 18].
Rationale for the Literature Review
The impact of patient navigation on CRC screening has been evaluated in both community- and hospital-based interventions. The general assumption is that patient navigation is useful in helping patients adhere to CRC screening recommendations; however, concrete evidence for its effectiveness is still currently under investigation. One major limitation in previous studies has been the lack of inclusion of medically underserved patient populations, as well as differences in study design, which makes it difficult to make comparisons between studies. The present literature review was undertaken to explore the effectiveness of patient navigation and education on CRC screening completion in medically underserved populations.
Methods
Overview
We conducted a comprehensive search of the literature for studies that have included patient navigators as key strategy for improving completion and quality of CRC screening. This literature review involved the use of several search engines including PubMed, Google Scholar, and Cochrane reviews. The following terms were used to identify articles: patient navigation, colonoscopy, fecal occult blood test (FOBT), fecal immunochemical test (FIT), CRC screening and outreach, CRC screening and prevention education, racial/ethnic disparities in CRC, and patient-centered approaches to CRC care. In addition, manual searches were conducted of studies referenced in these publications. We included randomized controlled trials and prospective investigations that had an intervention and control group. Case series, brief communications, commentaries, case reports, and uncontrolled studies were excluded. In instances where authors had multiple publications that presented data on the same population, the most recent publication was considered. Literature reviews and studies that presented design of CRC patient education protocols without including findings were excluded from the review as well. The review is subdivided into several major themes: (1) racial/ethnic disparities in CRC screening, (2) CRC prevention and education strategies, (3) impact of patient navigation on CRC screening, (4) tailored CRC education, and (5) cost-effectiveness of patient navigation programs to improve CRC screening completion.
In order to conduct a comprehensive review of the methodology followed in each research study, the Consolidated Standards of Reporting Trials (CONSORT) guidelines was used [34]. The CONSORT checklist was used to review how studies were designed, analyzed, and interpreted. This checklist aided in the decision of which studies to include in the literature review.
Results
Overview
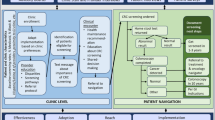
As can be seen in Fig. 1, 79 articles were initially identified. Of these articles, 43 did not mention CRC screening as main study outcome, did not specifically explore effectiveness of patient navigation on CRC screening, were concept papers, or presented policy statements. Another nine articles were excluded from the review because they presented literature reviews of studies conducted within the same time period evaluated in the present review, or were of poor methodological quality. In the end, 27 articles published in peer-reviewed journals between 2003 and 2016, were included in this review. Of these studies, 18 were RCTs [3–6, 8–14, 16, 20, 24, 25, 28–32, 38], five were descriptive or cross-sectional [7, 13, 17, 19, 23], and four were prospective studies [21, 27, 28, 38].

Study Flow Diagram
No. of articles identified through literature search (N = 79)
Review of Studies Included in the Literature Review
Characteristics of the studies are outlined in Table 1. The main topics in the majority of publications were interventions that explored ways to change CRC screening behaviors in medically underserved populations. Some explored the utility of traditional provider-patient interactions as motivation to obtain CRC screening [9, 10, 14, 28]. Other studies implemented interventions that included tailored messaging [6, 10, 18, 21, 25, 32], lay and clinic-based patient navigation programs [5, 8, 11, 13, 14, 17, 26, 29, 30, 37, 38], and culturally and linguistically appropriate outreach and education efforts to meet the CRC screening needs of medically underserved individuals [3, 9, 16, 18, 26]. A total of four studies conducted cost-effectiveness analyses of their patient navigation program to improve CRC screening [7, 17, 20, 38].
With the exception of studies conducted by Braschi CD, et al., Fiscella K, et al., Green BB, et al., Jandorf L, et al., Hendren S, et al., and Wells KJ, et al. in 2012 and 2016 [3, 8, 10, 17, 11, 37, 38], the majority of studies that had a patient navigation component demonstrated a positive impact on timely CRC screening [6, 9, 10, 13, 14, 26, 28–30, 33]. The patient navigation component in these studies included a number of barrier resolution services including help with transportation, health insurance, traditional patient reminder systems, and attention was given to implementing culturally and linguistically appropriate CRC education. For example, Pelto DJ, et al. [27], in a secondary analysis using data from two prospective PN cohorts, determined whether a patient navigation program targeted at African American and Latino participants helped increase CRC awareness and subsequently led to colonoscopy completion. In this study, a total of 742 African American and Latino patients were randomized to either a patient navigation or non-navigation arm. Patient navigation consisted of a health education intervention delivered in a culturally and linguistically appropriate manner. Patients in the navigation arm were significantly more likely to complete a colonoscopy compared to the non-navigation arm. In addition, language of health education instruction provided by patient navigators and patient income were significant predictors of colonoscopy completion. Similarly, Braschi CD et al. [3] explored the effect of a culturally appropriate patient navigation program targeted at a Latino patient population. Study groups consisted of patients randomized to a patient navigation group including tailored CRC education and a standard PN group (non-tailored). Key independent variables were socio-demographic and personal information. Main results revealed no significant differences in colonoscopy screening rates between the study groups. However, language acculturation and annual income above $10,000 were significantly associated with colonoscopy completion.
Green BB and colleagues [10] in a 4-group parallel-design RCT, examined whether the use of nurse navigation, EHR-linked mailings (automated), and combined automated with telephone assistance improved CRC screening over 2 years. Results showed that in comparison with usual care, EHR-linked mailings, and nurse navigation led to twice as many patients being current with CRC screening (usual care, 26.3%; EHR-linked, 50.8%; navigated, 64.7%).
In another study that explored the effectiveness of mailed CRC outreach education on completion of CRC screening, Singal AG, et al. [32] found that CRC screening was significantly increased among the mailed outreach group. In particular, FIT-based outreach was found to be more effective than colonoscopy-based outreach.
In another RCT, Meade CD, et al. [23] reported on experiences and lessons learned from implementing a lay patient navigator program to improve CRC screening completion among primary care medically underserved patients. Patient navigation was conducted by lay patient navigators and navigation services provided in six hospital-affiliated outpatient clinics and included barrier resolution services and helping to coordinate CRC care. Study population consisted of 588 Hispanic patients who predominantly spoke Spanish. The lay patient navigation program was effective in helping patients through a complex health care system. However, authors recommended a combination of lay and professional patient navigation to enhance coordination of CRC care, including completion recommended CRC screening. In an RCT conducted by Goldman S, et al. [9], 420 patients were randomized to either a PN outreach group or usual care. The goal of this study was to determine whether FOBT screening increased as a result of participating in the PN-led outreach intervention. Authors reported that intervention patients were significantly more likely to complete a fecal occult blood test compared to usual care (36.6 vs. 14.8%, p < 0.001, respectively). In addition, participants who visited the clinic often were more likely to complete the CRC screening test.
All cost-effectiveness studies included in this review have concluded that the use of patient navigation services as part of routine patient care are not only cost-effective, but can also generate revenue due to CRC screening completion. For example, Jandorf L, et al. [17] in a cost-effectiveness analysis of a colonoscopy patient navigation program included data from 503 multi-ethnic primary care patients 50 years and older, randomized to either a professional health education group or a community-based peer navigation group. Patient navigator salaries, supply costs, and navigation time were included in the cost-effectiveness analysis. Patient navigation resulted in 78.5% of patients completing a colonoscopy. Cost-effective analysis revealed that the patient navigation program resulted in a profit for the institution over a two-year period.
Conclusions
Peer-reviewed publications consistently indicate a positive impact of patient navigation programs on CRC screening completion as well have provided preliminary evidence for their cost-effectiveness. More well-conducted studies are needed that explore the use of EHRs in promotion of timely CRC screening and outreach.
Reference
American Cancer Society (2015) Cancer Facts & Figures. Atlanta: American Cancer Society 2015
Advani A, Atkeson B, Brown C, Peterson B, Fish L, Johnson J et al (2003) Barriers to the participation of African American patients with cancer in clinical trials. Cancer 97(6):1499–1506
Balogh EP, Ganz PA, Murphy SB, Nass SJ, Ferrell BR, Stovall E et al (2011) Patient centered cancer treatment planning: improving the quality of oncology care. Summary of an Institute of Medicine workshop. Oncologist 16(12):1800–1805
Braschi CD, Sly JR, Singh S, Villagra C, Jandorf L (2014) Increasing colonoscopy screening for Latino Americans through a patient navigation model: a randomized clinical trial. Journal of Immigrant and Minority Health/Center for Minority Public Health 16(5):934–940
Braun KL, Thomas WL, Domingo J-LB, Allison AL, Ponce A, Haunani KP et al (2015) Reducing cancer screening disparities in medicare beneficiaries through cancer patient navigation. J Am Geriatr Soc 63(2):365–370
Daskalakis C, Vernon SW, Sifri R, DiCarlo M, Cocroft SJA et al (2014) The effects of test preference, test access, and navigation on colorectal cancer screening. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 23(8):1521–1528
Donaldson EA, Holtgrave DR, Duffin RA, Feltner F, Funderburk W, Freeman HP (2012) Patient navigation for breast and colorectal cancer in 3 community hospital settings: an economic evaluation. Cancer 118(19):4851–4859
Fiscella K, Whitley E, Hendren S, Raich P, Humiston S, Winters P et al (2012) Patient navigation for breast and colorectal cancer treatment: a randomized trial. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 21(10):1673–1681
Goldman SN, Liss DT, Brown T, Lee JY, Buchanan DR, Balsley K, et al (2015) Comparative effectiveness of multifaceted outreach to initiate colorectal cancer screening in Community Health Centers: a randomized controlled trial. J Gen Intern Med 30(8):1178–1184
Green BB, Anderson ML, Wang C-Y, Vernon SW, Chubak J, Meenan RT et al (2014) Results of nurse navigator follow-up after positive colorectal cancer screening test: a randomized trial. Journal of the American Board of Family Medicine: JABFM 27(6):789–795
Hendren S, Griggs JJ, Epstein R, Humiston S, Jean-Pierre P, Winters P et al (2012) Randomized controlled trial of patient navigation for newly diagnosed cancer patients: effects on quality of life. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 21(10):1682–1690
Holmes-Rovner M, Williams GA, Hoppough S, Quillan L, Butler R, Given CW (2002) Colorectal cancer screening barriers in persons with low income. Cancer Pract 10(5):240–247
Honeycutt S, Green R, Ballard D, Hermstad A, Brueder A, Haardörfer R et al (2013) Evaluation of a patient navigation program to promote colorectal cancer screening in rural Georgia, USA. Cancer 119(16):3059–3066
Horne HN, Phelan-EHRick DF, Pollack CE, Markakis D, Wenzel J, Ahmed S et al (2015) Effect of patient navigation on colorectal cancer screening in a community-based randomized controlled trial of urban African American adults. Cancer Causes Control 26(2):239–246
Houston Department of Health and Human Services (2013). The City of Houston health disparities data report, 2013. Retrieved from http://www.houstontx.gov/health/disparity.pdf
Jandorf L, Braschi C, Ernstoff E, Wong CR, Thelemaque L, Winkel G et al (2013) Culturally targeted patient navigation for increasing African Americans’ adherence to screening colonoscopy: a randomized clinical trial. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 22(9):1577–1587
Jandorf L, Tassel LM, Cooperman JL, Graff Zivin J, Ladabaum U, Hall D et al (2013) Cost analysis of a patient navigation system to increase screening colonoscopy adherence among urban minorities. Cancer 119(3):612–620
Klabunde CN, Vernon SW, Nadel MR, Breen N, Seeff LC, Brown ML (2005) Barriers to colorectal cancer screening: a comparison of reports from primary care physicians and average-risk adults. Med Care 43(9):939–944
Ladabaum U, Mannalithara A, Jandorf L, Itzkowitz SH (2015) Cost-effectiveness of patient navigation to increase adherence with screening colonoscopy among minority individuals. Cancer 121(7):1088–1097
Lairson DR, Dicarlo M, Deshmuk AA, Fagan HB, Sifri R, Katurakes N et al (2014) Cost-effectiveness of a standard intervention versus a navigated intervention on colorectal cancer screening use in primary care. Cancer 120(7):1042–1049
Liu G, Perkins A. Using a lay cancer screening navigator to increase colorectal cancer screening rates. JABFM 28(2):280–282
Mandelblatt J, Andrews H, Kao R, Wallace R, Kerner J (1996) The late-stage diagnosis of colorectal cancer: demographic and socioeconomic factors. Am J Public Health 86(12):1794–1797
Meade CD, Wells KJ, Arevalo M, Calcano ER, Rivera M, Sarmiento Y et al (2014) Lay navigator model for impacting cancer health disparities. J Cancer Educ 29(3):449–457
Myers RE, Bittner-Fagan H, Daskalakis C, Sifri R, Vernon SW, Cocroft J, Andrel J et al (2013) A randomized controlled trial of a tailored navigation and a standard intervention in colorectal cancer screening. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 22(1):109–117
Myers RE, Sifri R, Daskalakis C, DiCarlo M, Geethakumari PR, Cocroft J et al (2014) Increasing colon cancer screening in primary care among African Americans. J Natl Cancer Inst 106(12)
Paskett ED, Rushing J, D’Agostino R, Tatum C, and Velez R. 1997. Cancer screening behaviors of low-income women: the impact of race. Women’s Health (Hillsdale, N.J.) 3(3–4), 203–226.
Pelto DJ, Sly JR, Winkel G, Redd WH, Thompson HS, Itzkowitz SH et al (2015) Predicting colonoscopy completion among African American and Latino/a participants in a patient navigation program. J Racial Ethn Health Disparities 2(1):101–111
Percac-Lima S, López L, Ashburner JM, Green AR, Atlas SJ (2014) The longitudinal impact of patient navigation on equity in colorectal cancer screening in a large primary care network. Cancer 120(13):2025–2031
Raich PC, Whitley EM, Thorland W, Valverde P, Fairclough D, Denver Patient Navigation Research Program (2012) Patient navigation improves cancer diagnostic resolution: an individually randomized clinical trial in an underserved population. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 21(10):1629–1638
Ritvo PG, Myers RE, Paszat LF, Tinmouth JM, McColeman J, Mitchell B, Serenity M, Rabeneck L. Personal navigation increases colorectal cancer screening uptake. Cancer Epidemiol Biomarkers Prev 24(3):506–511
Robbins AS, Siegel RL, Jemal A (2012) Racial disparities in stage-specific colorectal cancer mortality rates from 1985 to 2008. J Clin Oncol 30:401–405
Singal AG, Gupta S, Tiro JA, Skinner CS, McCallister K, Sanders JM et al (2016) Outreach invitations for FIT and colonoscopy improve colorectal cancer screening rates: a randomized controlled trial in a safety-net health system. Cancer 122(3):456–463
Texas Department of State Health Services, Texas Cancer Registry. Expected New Cancer Cases and Deaths by Primary Site, Harris County, Texas, 2013. Retrieved from http://www.dshs.state.tx.us
The CONSORT group http://www.consort-statement.org (Accessed April 10, 2016).
U.S. Department of Health and Human Services, Healthy people 2020 objectives. Retrieved from http://healthypeople.gov/2020/topicsobjectives2020/objectives
Wells KJ, Lee J-H, Calcano ER, Meade CD, Rivera M, Fulp WJ et al (2012) A cluster randomized trial evaluating the efficacy of patient navigation in improving quality of diagnostic care for patients with breast or colorectal cancer abnormalities. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 21(10):1664–1672
Wells KJ, Winters PC, Jean-Pierre P, Warren-Mears V, Post D, Van Duyn MAS, et al. 2016. Patient Navigation Research Program Investigators. Effect of patient navigation on satisfaction with cancer-related care. Supportive Care in Cancer: Official Journal of the Multinational Association of Supportive Care in Cancer 24(4), 1729–1753.
Wilson FA, Villarreal R, Stimpson JP, Pagán JA (2015) Cost-effectiveness analysis of a colonoscopy screening navigator program designed for Hispanic men. Journal of Cancer Education: The Official Journal of the American Association for Cancer Education 30(2):260–267
Author information
Authors and Affiliations
Corresponding author
Additional information
All work was conducted at Baylor College of Medicine
Rights and permissions
About this article

Cite this article
Sunny, A., Rustveld, L. The Role of Patient Navigation on Colorectal Cancer Screening Completion and Education: a Review of the Literature. J Canc Educ 33, 251–259 (2018). https://doi.org/10.1007/s13187-016-1140-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13187-016-1140-0