
Abstract
The Na+/Ca2+ exchanger (NCX) plays an important role in the maintenance of Na+ and Ca2+ homeostasis in most cells including neurons under physiological and pathological conditions. It exists in three subtypes (NCX1-3) with different tissue distributions but all of them are present in the brain. NCX transports Na+ and Ca2+ in either Ca2+-efflux (forward) or Ca2+-influx (reverse) mode, depending on membrane potential and transmembrane ion gradients. During neuronal ischemia, Na+ and Ca2+ ionic disturbances favor NCX to work in reverse mode, giving rise to increased intracellular Ca2+ levels, while it may regain its forward mode activity on reperfusion. The exact significance of NCX in neuronal ischemic and reperfusion states remains unclear. The differential role of NCX subtypes in ischemic neuronal injury has been extensively investigated using various pharmacological tools as well as genetic models. This review discusses the mode of action of NCX in ischemic and reperfusion states, the differential roles played by NCX subtypes in these states as well as the role of NCX in pre- and postconditioning. NCX subtypes carry variable roles in ischemic injury. Furthermore, the mode of action of each subtype varies in ischemia and reperfusion states. Thus, therapeutic targeting of NCX in stroke should be based on appropriate timing of the administration of NCX subtype-specific strategies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ca2+ signaling is a prerequisite of many cellular physiological activities. Precise control of intracellular Ca2+ (Ca2+ i) is therefore critical for proper regulation of cellular functions. Intracellular organelles, including endoplasmic reticulum, mitochondria, and secretory vesicles have Ca2+ uptake mechanisms to remove Ca2+ from the cytosol and bring Ca2+ i concentration back to the resting level. In the plasma membrane, the Ca2+ pump and the Na+/Ca2+ exchanger (NCX) are the two main mechanisms for exporting Ca2+ out of the cell. Using these mechanisms, Ca2+ concentration in various regions of the cell may be differentially modulated [1–3]. The idea of NCX dates back to the 1960s, when investigators identified a countertransport mechanism between Na+ and Ca2+ across the plasma membrane [4]. Purification and cloning of NCX have resulted in major advances in our understanding of this system [5–8]. NCX plays an important role in the maintenance of Ca2+ i homeostasis and is detected in the plasma membrane of most cells, including neurons and glia [4, 9]. It plays a dominant role in removing Ca2+ from the cytosol in cells that require extracellular Ca2+ for their physiological activities, such as neurons and cardiac muscle cells. NCX is a bidirectional membrane ion transporter. The direction of transport depends on the prevailing Na+ and Ca2+ electrochemical gradients (see below) [10, 11].
NCX Subtypes
Two families of Na+/Ca2+ exchangers were identified, the K+-independent NCX (SLC8) and the K+-dependent NCKX (SSLC8b1). Both exchangers are encoded by multigene families. Three genes, ncx1-3, code for the NCX subtypes NCX1-3 [12, 13], and at least four genes, nckx1-4, code for the NCKX subtypes NCKX1-4 [14, 15]. NCX1 was first cloned from canine cardiac sarcolemma [16], and later the corresponding human gene, SLC8A1, was mapped to chromosome 2p22.1 [17]. The NCX2 gene, SLC8A2, is located on chromosome 19q13.2 [18], while the SLC8A3 gene, encoding NCX3, maps to chromosome 14q24.2 [19]. The recently discovered crystal structure of archaebacterial Methanococcus jannaschii (NCX_Mj) represents a long-awaited breakthrough [20]. Two variants of NCX3 exist in mice: NCX-B, existing in the brain, and NCX-AC, predominant in the skeletal muscles. NCX3-AC has a higher Na+ sensitivity [21]. Although all three members arise from separate genes on different chromosomes, they share high amino acid identity (about 70 %), especially in the hydrophobic regions [5–7, 16]. A specific 20-amino-acid stretch (219–238), known as XIP (endogenous exchange inhibitory peptide), belonging to the so-called f-loop of the exchanger, exerts an autoinhibitory action thus limiting NCX activity. Many splice variants arise from a combination of six small exons (A, B, C, D, E, and F), whereas a mutually exclusive exon (either A or B) appears in each given splice variant. At least 17 NCX1 and 5 NCX3 proteins are produced through alternative splicing, whereas no splice variants of NCX2 have yet been identified.
Although NCX subtypes are found in almost every type of cell, the expression profiles of these isoforms vary among different tissues and change during development [22]. NCX1 is expressed in multiple organs, including the brain, heart, kidney, skeletal muscle, eye, and blood cells. NCX2 is found only in the brain whereas NCX3 is found in both brain and skeletal muscle [23, 24]. In addition to neurons, NCX is also expressed in glial cells, playing many crucial roles, including the regulation in Na and Ca homeostasis in astrocytes, neurotransmitter release, oligodendrocyte maturation, and myelin formation [25–27].
Mode of Action
NCX acts in a reversible and electrogenic way with a stoichiometry of 3 Na+ ions/1 Ca2+ ion [9]; however, more recently, in addition to the major 3:1 transport mode, it has been demonstrated that ion flux ratio can vary from 1:1 to a maximum of 4:1, depending on the intracellular concentration of Na+ (Na+ i ) and Ca2+ ions [28] (for a comprehensive detailed review, see Khananshvili [29]).
The equilibrium potential of the NCX (E NCX) was calculated to be −73 mV. At membrane potentials (E m) more negative than the E NCX, NCX will operate in the direction of Ca2+ efflux (forward mode). Conversely, at E m more positive than the E NCX, NCX will operate in the direction of Ca2+ influx (reverse mode). As the resting potential of the cell is −80 mV (E NCX > E m), NCX will operate in the Ca2+ efflux mode, and it has been demonstrated that Na+/Ca2+ exchange is the major Ca2+-efflux mechanism especially in the heart [4, 30]. When the electrochemical gradient for Na+ is reversed, such as during membrane depolarization or the opening of gated Na+ channels, the exchanger will work in reverse mode, i.e., it will transport Na+ out of the cell and Ca2+ into the cell [9, 31].
The activity of NCX is indirectly dependent on the energy-dependent plasma membrane pumps. Under anoxic and ischemic conditions, the functions of Na+/K+ ATPase and Ca2+ ATPase are impaired, with consequent dysregulation in Na+ i and Ca2+ i homeostasis [32], which is consequently reflected in the mode of activity of NCX (see below). Study of the physiological functions of NCX has been facilitated by the development of pharmacological tools modifying its activity [4]; the most relevant of which are summarized in Table 1. However, the reliability of data has been greatly challenged by the specificity of the pharmacological agents used, as most of them have actions on other ion transport systems.
Role of NCX in Neuronal Ischemia
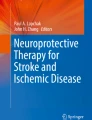
Under normal physiological conditions, it is generally accepted that neuronal NCX is primarily involved in extruding Ca2+ i. Under ischemic conditions, energy-producing machinery fails and production of ATP is low. Anaerobic glycolysis and ATP degradation produce H+, activating the Na+/H+ exchanger and causing Na+ influx [50]. Furthermore, Na+ efflux is attenuated because the Na+/K+ ATPase is inhibited during ischemia. Because the release of glutamate is increased during ischemia [51], overstimulated N-methyl-d-aspartate/α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (NMDA/AMPA) receptors result in Na+ and Ca2+ influx into the neurons, and depending on the duration and severity of the excitotoxic event, acute or delayed neuronal death follows. The process of elevation of Ca2+ i will contribute to neuronal death by activation of calpains, endonucleases, nitric oxide synthase, and phospholipases; free radical production; and mitochondrial dysfunction [52–54]. The rise in Na+ i is also catastrophic, causing cellular swelling and cytoskeletal dysfunction. The rise in Na+ i in the neurons will allow the Na+/glutamate carrier to operate in the opposite direction, allowing excess release of glutamate and increasing excitotoxicity [55]. The net increase in Na+ i, which will increase the E m above the E NCX, causes NCX to work in the reverse or Ca2+-influx mode. On this basis, it is thought that the NCX, working in the reverse mode under ischemic conditions (Figs. 1 and 2), contributes to increase in Ca2+ i in these states.

The alternation in NCX mode of activity before, during, and after ischemic insult

The role of NCX working in reverse mode during an ischemic attack. Does the cell trade removal of excess Na+ i by accepting more Ca2+ i? Dotted arrow indicates slowed ion transport; thick solid line indicates enhanced ion transport. Dashed arrows indicate negative effect; thin solid line indicates positive effect
From this perspective, the NCX while working in its reverse mode may have two opposing roles in ischemic injury: adding to ischemic insult by increasing Ca2+ i and reducing neuronal damage by reducing Na+ i. Various in vivo and in vitro studies (Table 2) have been conducted to address these questions and to delineate the exact role played by NCX in order to evaluate its therapeutic potential. Despite the conflicting results, most in vivo studies using the focal cerebral ischemia model indicate that blocking NCX activity is neurodamaging whereas increasing NCX activity is neuroprotective [63].
The activation of NCX to work in reversal (Ca2+-influx mode) using extracellular Na+ depletion model could prevent neuronal damage and death, and this protective effect was inhibited by amiloride (an NCX inhibitor) [64]. A similar protective effect was shown by stimulation of the Ca2+-influx mode by sodium nitroprusside, which stimulates the NCX owing to its Fe3+ content [62]. Sodium nitroprusside increased Ca2+ following chemical hypoxia, an effect that was blocked by the NCX blockers bepridil and CB-DMB. Amoroso et al. have provided evidence that inhibiting NCX is harmful in rat hippocampal slices exposed to chemical hypoxia and glucopenia [58]. Levels of aspartate (an excitatory amino acid) released were higher when several inhibitors of NCX were present at the beginning of hypoxia, indicating a more severe excitatory insult when NCX reversal mode is inhibited, allowing more Na+ accumulation and release of excitatory neurotransmitters.
The neuroprotective effect of NCX working in the reverse mode (Fig. 2) could be due to a variety of factors. The NCX by promoting Ca2+ influx to the cell will regenerate the Ca2+ stored in the endoplasmic reticulum depleted by the ischemic state [65]. By eliciting a decrease in Na+ i overload, NCX prevents cell swelling and death [66], and by reducing Na+ i it decreases the release of glutamate, reducing the excitotoxic insult exerted by glutamate under ischemic conditions. Li+, which stimulates the reverse mode of NCX, was shown to be protective against glutamate-induced damage; however, this required a dose far higher than that needed to stimulate NCX [47].
Another set of studies yielded different conclusions. KB-R7943, which preferentially inhibits the reversal mode in low doses and the forward mode in high doses, was neuroprotective only in low doses (0.1 μM), whereas high doses (30 μM) exacerbated neuronal damage [59]. The same compound was also found to be neuroprotective by reducing Ca2+ i loads [67]. However, some have suggested that the neuroprotective mechanism of KB-R7943 is unrelated to NCX inhibition, including effects on store-operated Ca2+ channels and NMDA receptors [68] as inhibition of the mitochondrial permeability transition pore [69] and activity on mitochondrial Ca2+ uniporters [70].
S1EA0400, a more potent inhibitor of NCX (IC50 equals 33 nM), also showed a neuroprotective effect both in vivo and in vitro in a series of experiments conducted by Matsudo et al. [39], a finding also confirmed by Iwamoto et al. [44]. However, the matter is complicated by data suggesting that SEA0400 lacks specificity and affects Ca2+ transport through other pathways [71]. Moreover, the mode of action of SEA0400 on NCX seems to be more selective for NCX1 [44, 72], suggesting the need to study the differential roles of individual NCX subtypes, which was facilitated by genetic models (see below). It is worth mentioning that some reports have noted a neutral effect of NCX in neuronal ischemic states, stating that the NCX activity may play no significant role in protecting or damaging ischemic neurons [57].
Role of NCX in Reperfusion States
Following the recovery of ATPase activity, including Na+/K+ ATPase, secondary to replenishment of ATP in reperfusion, NCX operates in a forward mode [59]. Although NCX contributes to Ca2+ i overload by working in reverse mode under ischemic or excitotoxic states, NCX is protective in excitotoxic states when it works in its forward Ca2+ extrusion capacity [73]. Failure of NCX to work in its forward mode contributes to excitotoxic Ca2+ overload. Knockdown of NCX decreased the lethal dose of glutamate and overexpression of NCX decreased glutamate-induced Ca2+ overload and rescued the cells. Bano et al. also proposed that destruction of NCX by calpains contributes to excitotoxic damage [74]. This greatly highlighted the importance of the forward working NCX during reperfusion injury.
However, it is known that the Ca2+ extrusion system is critically affected during ischemia by destruction of proteins involved in Ca2+ homeostasis [75], which raises questions about the role of NCX during reperfusion. It seems, however, that not all NCX subtypes are destroyed by Ca2+-dependent proteolysis through ischemia/reperfusion injury. ncx1 messenger RNA (mRNA) level was reduced by 42.1 and 27.8 %, respectively, after 2 and 6 h of reperfusion (after transient middle cerebral artery occlusion (MCAO) for 120 min) and was restored to normal levels after 12 and 24 h of reperfusion. NCX1 protein was decreased after 2 h of reperfusion and regain to normal level at 24 h although other reports show it may remain downregulated for 72 h after reperfusion [76, 77]. The mRNA and protein levels of NCX2 and NCX3 did not change significantly over time [76], but NCX3 protein was reduced indicating that it might be destroyed by proteolytic system during reperfusion [77]. Some have proposed that after the energy state of the cell improves, e.g., during reperfusion, NCX operates in a rectifying Ca2+-efflux (forward) mode, clearing excess Ca2+ i accumulated during the ischemic episode [63]. This has also been supported by the recent work of Cross et al., who showed that neuronal and HEK293 cell survival following oxygen glucose deprivation was dramatically improved following overexpression of NCX2 and NCX3 (but not NCX1) by improving Ca2+ i management, i.e., by working in forward mode [78] (Fig. 1). However, the protective effect of the forward mode is based mainly on excitotoxic models, and further studies are needed to clarify how much NCX contributes in modulating reperfusion injury. This will require conditioned knockdown studies conducted during reperfusion states.
Differential role of the NCX Subtypes in Neuronal Ischemic Injury
NCX1
Using transient MCAO, the cerebral infarcts in NCX1+/− mice were significantly smaller than those in wild-type mice. SN-6, pharmacological blocker for the NCX1, significantly reduced the infarct volume [72]. These findings may explain the protective effect of SEA0400, as a selective NCX1 inhibitor, found in in vivo and in vitro studies (see before). However, these conclusions do not accord with the data reported by Pignataro et al. [79], who showed that intracerebroventricular infusion of oligodeoxynucleotides (ODNs) against NCX1 in rats for 24 and 48 h prior to permanent MCAO caused an increase in the infarction volume. However, the models were different between the two groups. The infarction volume was evaluated 24 h after reperfusion in the former study and 24 h after permanent ischemia in the latter, suggesting that NCX1 may contribute to neuronal damage during ischemia/reperfusion, while having a neuroprotective effect in permanent ischemic states. This also suggests that downregulation of NCX1 during reperfusion [76, 77] might be a physiological protective response of neurons although further investigation is required to test this hypothesis. It is worth mentioning that SN-6 have multiple inhibitory effects on other mechanisms which should be considered while evaluating its effects [80].
The role of NCX1 in mediating cell damage was further evaluated by its role in mediating NMDAR-induced retinal damage. NCX1+/− mice possessed significant protection against retinal damage induced by intravitreal injection of NMDA. SEA0400 significantly reduced NMDA or high intraocular pressure-induced retinal cell damage in mice. It also reduced the expression of phosphorylated mitogen-activated protein kinases (ERK1/2, JNK, p38) induced by NMDA injection [81] and failed to produce its protective effect against Ca2+ overload-mediated factors other than NCX1. This finding may suggest that the Ca2+ overload produced by NCX1 working in its reverse mode may contribute to NMDA-mediated excitotoxicity.
Of the NCX subtypes, NCX1 is the most highly expressed in microglia [82]. Increased NCX1expression and activity, working in reverse mode, has been found in microglial cells inside and surrounding brain infarction core. It has been suggested that these changes carry protective role in the postinfarction period [83].
NCX2
In contrast to NCX1+/−, transient cerebral ischemia in vivo produced a larger infarction and more cell death in the NCX2−/− mouse brain [84] while in wild-type brain, NCX2-expressing neurons were largely spared from cell death after ischemia. NCX2-deficient hippocampal cells showed slower recovery in population spike amplitudes, a sustained elevation of Ca2+ i, and an increased membrane depolarization after in vitro ischemia. This suggests that NCX2 exports Ca2+ (working in forward mode) in ischemia/reperfusion and thus protects neuronal cells from death by reducing Ca2+ i [85]. In addition, overexpression of NCX2 (which is not susceptible to cleavage by calpain) protected neurons against glutamate excitotoxicity, a process that is, at least partially, dependent upon Ca2+-induced injury [74].
In the previously discussed model of Pignataro et al., ODN downregulation of NCX2 protein levels had no effect on infarct size. This suggests that NCX2 does not play a major role in cell death following permanent ischemia [79]. Jeon et al. [85] have demonstrated larger focal injury in rats deficient of the NCX2 protein following transient MCAO. The overexpression of NCX2 in cerebellar granule neurons confers neuroprotection against excitotoxicity in vitro [74]. Taken together, these studies show that NCX2 has a protective effect under the ischemia/reperfusion state, whereas its role in permanent ischemic models may be less important.
NCX3
Similar to NCX2, NCX3 knockout mice display increased brain injury following transient global and transient focal cerebral ischemia [84, 86, 87]. In vitro studies using cortical neuronal cultures subjected to transient oxygen glucose deprivation also revealed increased neuronal injury in NCX3 knockout mouse-derived cultures [87]. Furthermore, the reduced NCX3 activity limits Ca2+-induced neurotoxicity during severe transient but not during severely sustained ischemic insults [78]. Although NCX3 was not shown to be cleaved during ischemia/reperfusion injury (see before) [76], Bano et al. have demonstrated in a rat model of focal ischemia that the NCX3 isoform is cleaved by calpain following permanent ischemia and glutamate-induced excitotoxicity. NCX3 is crucial in extruding the Ca2+ load resulting from glutamate exposure, and the cleavage of the NCX protein contributes to Ca2+ overload [74, 88]. In the permanent ischemia model, ODN downregulation of the NCX3 protein level showed a larger infarction size, rendering NCX3 the only subtype that is protective against reperfusion and permanent injury.
Pre- and Postconditioning
Preconditioning is a phenomenon whereby a subliminal injurious stimulus is applied before a longer, harmful ischemia, whereas postconditioning refers to a short sublethal brain ischemia subsequent to a prolonged harmful ischemic episode, which may confer ischemic neuroprotection [89]. NCX, NCX3 in particular, seems to also play a role in such protective phenomena. Interestingly, NCX3 was upregulated when the brain was exposed to a transient ischemic episode for 30 min (but not 120 min, see before) [77]. Although 120 min of transient MCAO reduced the expression of NCX1 (see before), the 30-min episode did not change its expression. More surprising, the matter was changed when tMCAO for 120 min was preceded by a transient ischemic episode (for 30 min) 72 h previously; both NCX1 and NCX3 were then upregulated. Moreover, small interfering RNA (siRNA) against NCX1 and NCX3 before preconditioning significantly reduced the protective effect of preconditioning [77]. Of the NCX subtypes, NCX3 protein and ncx3 mRNA were the ones that were upregulated in those brain regions protected by postconditioning. NCX3 silencing, induced by intracerebroventricular infusion of siRNA, partially reverted the postconditioning-induced neuroprotection [90]. Further studies are needed to clarify the mode of action of NCX3 under these conditions.
Mitochondrial NCX
The mitochondrial Na+/Ca2+ exchanger (NCXmito), located in the inner mitochondrial membrane, extrudes Ca2+ ions from its matrix in exchange with cytosolic Na+ ions. The stoichiometry of NCXmito-operated Na+/Ca2+exchange has long been the subject of controversy, but evidence of an electrogenic 3:1 Na+/Ca2+ exchange is increasing. NCXmito has a role in controlling neuronal Ca2+ homeostasis and neuronal bioenergetics. The three isoforms of plasma membrane NCX can contribute to NCXmito in neurons and astrocytes [91]. Based on its role in regulating both mitochondrial and potentially cytoplasmic Ca2+, NCXmito seems to be an interesting candidate to study under ischemic conditions. Experimental evidence suggests that supraphysiological activation of NCXmito contributes to neuronal cell death in the ischemic brain, and its activity is related to reduction in the ability to reestablish normal ionic homeostasis. These data suggest that NCXmito could represent an important target for the development of new neurological drugs [92].
NCKX
Despite its importance in maintaining Na+, Ca2+, and K+ homeostases in the CNS, the role of NCKX under ischemic conditions, at least relative to NCX, has not generated enough interest. The role of this protein in the development of ischemic damage was assessed by knocking down its expression with ODNs intracerebroventricularly, infused by an osmotic minipump for 48 h, starting from 24 h before permanent MCAO. NCKX2 knockdown increased the extent of the ischemic lesion [93]. Further studies conducted by the same group showed that after MCAO, NCKX2 mRNA and protein expression were downregulated in the ischemic core and peri-infarctional areas. NCKX2−/− primary cortical neurons displayed a higher vulnerability and a greater Ca2+ i increase under hypoxic conditions, compared with NCKX2+/+ neurons. These results indicate that NCKX2 may be involved in brain ischemia, and it may represent a new potential target to be investigated in the study of the molecular mechanisms involved in cerebral ischemia [94]. However, other reports have shown that under conditions in which NCX is inhibited, NCKX can provide a way by which Ca2+ can get access and contribute to ischemic damage [95], suggesting that the protective role of NCKX is evident only when NCX is functioning.
Conclusions and Unanswered Questions
It is clear that different NCX subtypes exert variable roles in neuronal ischemic injury. The lack of pharmacological tools or agents that specifically modify the function of particular NCX subtypes has greatly limited our understanding of the differential roles of each subtype in neuronal ischemic injury. Genetic models and knockdown of the NCX subtypes have helped to some extent in exploring their roles. The availability of Cre/loxp system to generate conditional NCX1−/− (NCX1−/− mice are embryonic lethal at 11 days postcoitum due to absence of spontaneous heart beats [96]) may help in further exploring the function of this particular subtype [97]. The potential lack of temporal and spatial selectivity of some antisense knockdown strategies limits their usefulness as experimental tools in studying NCX.
NCX subtypes carry variable roles in ischemic injury; furthermore, the mode of action of each subtype varies in ischemia and reperfusion states, which necessitates time-sensitive and subtype-specific therapeutic targeting. The role of other Na+ /Ca2+ exchanger systems, NCKX and NCXmito in neuronal injury is still unclear and further investigations are highly required to understand their role.
References
Rizzuto R, Pozzan T. Microdomains of intracellular Ca2+: molecular determinants and functional consequences. Physiol Rev. 2006;86(1):369–408. doi:10.1152/physrev.00004.2005.
Schneggenburger R, Neher E. Presynaptic calcium and control of vesicle fusion. Curr Opin Neurobiol. 2005;15(3):266–74. doi:10.1016/j.conb.2005.05.006.
Verkhratsky A. Physiology and pathophysiology of the calcium store in the endoplasmic reticulum of neurons. Physiol Rev. 2005;85(1):201–79. doi:10.1152/physrev.00004.2004.
Annunziato L, Pignataro G, Di Renzo GF. Pharmacology of brain Na+/Ca2+ exchanger: from molecular biology to therapeutic perspectives. Pharmacol Rev. 2004;56(4):633–54. doi:10.1124/pr.56.4.5.
Li Z, Matsuoka S, Hryshko LV, Nicoll DA, Bersohn MM, Burke EP, et al. Cloning of the NCX2 isoform of the plasma membrane Na(+)-Ca2+ exchanger. J Biol Chem. 1994;269(26):17434–9.
Nicoll DA, Quednau BD, Qui Z, Xia YR, Lusis AJ, Philipson KD. Cloning of a third mammalian Na+-Ca2+ exchanger, NCX3. J Biol Chem. 1996;271(40):24914–21.
Nicoll DA, Ottolia M, Lu L, Lu Y, Philipson KD. A new topological model of the cardiac sarcolemmal Na+-Ca2+ exchanger. J Biol Chem. 1999;274(2):910–7.
Philipson KD, Longoni S, Ward R. Purification of the cardiac Na+-Ca2+ exchange protein. Biochim Biophys Acta. 1988;945(2):298–306.
Blaustein MP, Lederer WJ. Sodium/calcium exchange: its physiological implications. Physiol Rev. 1999;79(3):763–854.
Philipson KD, Nicoll DA. Sodium-calcium exchange: a molecular perspective. Annu Rev Physiol. 2000;62:111–33. doi:10.1146/annurev.physiol.62.1.111.
Quednau BD, Nicoll DA, Philipson KD. The sodium/calcium exchanger family-SLC8. Arch Eur J Physiol. 2004;447(5):543–8. doi:10.1007/s00424-003-1065-4.
Canitano A, Papa M, Boscia F, Castaldo P, Sellitti S, Taglialatela M, et al. Brain distribution of the Na+/Ca2+ exchanger-encoding genes NCX1, NCX2, and NCX3 and their related proteins in the central nervous system. Ann N Y Acad Sci. 2002;976:394–404.
Linck B, Qiu Z, He Z, Tong Q, Hilgemann DW, Philipson KD. Functional comparison of the three isoforms of the Na+/Ca2+ exchanger (NCX1, NCX2, NCX3). Am J Physiol. 1998;274(2 Pt 1):C415–23.
Kiedrowski L, Czyz A, Li XF, Lytton J. Preferential expression of plasmalemmal K-dependent Na+/Ca2+ exchangers in neurons versus astrocytes. Neuroreport. 2002;13(12):1529–32.
Kimura J, Watanabe Y, Li L, Watano T. Pharmacology of Na+/Ca2+ exchanger. Ann N Y Acad Sci. 2002;976:513–9.
Nicoll DA, Longoni S, Philipson KD. Molecular cloning and functional expression of the cardiac sarcolemmal Na(+)-Ca2+ exchanger. Science. 1990;250(4980):562–5.
Kraev A, Chumakov I, Carafoli E. The organization of the human gene NCX1 encoding the sodium-calcium exchanger. Genomics. 1996;37(1):105–12. doi:10.1006/geno.1996.0526.
Kikuno R, Nagase T, Ishikawa K, Hirosawa M, Miyajima N, Tanaka A, et al. Prediction of the coding sequences of unidentified human genes. XIV. The complete sequences of 100 new cDNA clones from brain which code for large proteins in vitro. DNA Res: Int J Rapid Publ Rep Genes Genomes. 1999;6(3):197–205.
Gabellini N, Bortoluzzi S, Danieli GA, Carafoli E. The human SLC8A3 gene and the tissue-specific Na+/Ca2+ exchanger 3 isoforms. Gene. 2002;298(1):1–7.
Liao J, Li H, Zeng W, Sauer DB, Belmares R, Jiang Y. Structural insight into the ion-exchange mechanism of the sodium/calcium exchanger. Science. 2012;335(6069):686–90. doi:10.1126/science.1215759.
Michel LY, Verkaart S, Koopman WJ, Willems PH, Hoenderop JG, Bindels RJ. Function and regulation of the Na+-Ca2+ exchanger NCX3 splice variants in brain and skeletal muscle. J Biol Chem. 2014;289(16):11293–303. doi:10.1074/jbc.M113.529388.
Papa M, Canitano A, Boscia F, Castaldo P, Sellitti S, Porzig H, et al. Differential expression of the Na+-Ca2+ exchanger transcripts and proteins in rat brain regions. J Comp Neurol. 2003;461(1):31–48. doi:10.1002/cne.10665.
Lee SL, Yu AS, Lytton J. Tissue-specific expression of Na(+)-Ca2+ exchanger isoforms. J Biol Chem. 1994;269(21):14849–52.
Philipson KD, Nicoll DA, Matsuoka S, Hryshko LV, Levitsky DO, Weiss JN. Molecular regulation of the Na(+)-Ca2+ exchanger. Ann N Y Acad Sci. 1996;779:20–8.
Paluzzi S, Alloisio S, Zappettini S, Milanese M, Raiteri L, Nobile M, et al. Adult astroglia is competent for Na+/Ca2+ exchanger-operated exocytotic glutamate release triggered by mild depolarization. J Neurochem. 2007;103(3):1196–207. doi:10.1111/j.1471-4159.2007.04826.x.
Reyes RC, Verkhratsky A, Parpura V. Plasmalemmal Na+/Ca2+ exchanger modulates Ca2+-dependent exocytotic release of glutamate from rat cortical astrocytes. ASN neuro. 2012;4(1). doi:10.1042/AN20110059.
Boscia F, D’Avanzo C, Pannaccione A, Secondo A, Casamassa A, Formisano L, et al. Silencing or knocking out the Na(+)/Ca(2+) exchanger-3 (NCX3) impairs oligodendrocyte differentiation. Cell Death Differ. 2012;19(4):562–72. doi:10.1038/cdd.2011.125.
Kang TM, Hilgemann DW. Multiple transport modes of the cardiac Na+/Ca2+ exchanger. Nature. 2004;427(6974):544–8. doi:10.1038/nature02271.
Khananshvili D. Sodium-calcium exchangers (NCX): molecular hallmarks underlying the tissue-specific and systemic functions. Arch Eur J Physiol. 2014;466(1):43–60. doi:10.1007/s00424-013-1405-y.
Philipson KD, Nicoll DA, Ottolia M, Quednau BD, Reuter H, John S, et al. The Na+/Ca2+ exchange molecule: an overview. Ann N Y Acad Sci. 2002;976:1–10.
Schnetkamp PP. The SLC24 Na+/Ca2+-K+ exchanger family: vision and beyond. Arch Eur J Physiol. 2004;447(5):683–8. doi:10.1007/s00424-003-1069-0.
Meyer FB. Calcium, neuronal hyperexcitability and ischemic injury. Brain Res Brain Res Rev. 1989;14(3):227–43.
Taglialatela M, Canzoniero LM, Cragoe Jr EJ, Di Renzo G, Annunziato L. Na(+)-Ca2+ exchange activity in central nerve endings. II. Relationship between pharmacological blockade by amiloride analogues and dopamine release from tuberoinfundibular hypothalamic neurons. Mol Pharmacol. 1990;38(3):393–400.
Sharikabad MN, Cragoe Jr EJ, Brors O. Inhibition by 5-N-(4-chlorobenzyl)-2′,4′-dimethylbenzamil of Na+/Ca2+ exchange and l-type Ca2+ channels in isolated cardiomyocytes. Pharmacol Toxicol. 1997;80(2):57–61.
Watanabe Y, Kimura J. Inhibitory effect of amiodarone on Na(+)/Ca(2+) exchange current in guinea-pig cardiac myocytes. Br J Pharmacol. 2000;131(1):80–4. doi:10.1038/sj.bjp.0703527.
Watano T, Kimura J, Morita T, Nakanishi H. A novel antagonist, No. 7943, of the Na+/Ca2+ exchange current in guinea-pig cardiac ventricular cells. Br J Pharmacol. 1996;119(3):555–63.
He Z, Petesch N, Voges K, Roben W, Philipson KD. Identification of important amino acid residues of the Na+-Ca2+ exchanger inhibitory peptide, XIP. Jo Membr Biol. 1997;156(2):149–56.
Iwamoto T, Shigekawa M. Differential inhibition of Na+/Ca2+ exchanger isoforms by divalent cations and isothiourea derivative. Am J Physiol. 1998;275(2 Pt 1):C423–30.
Matsuda T, Arakawa N, Takuma K, Kishida Y, Kawasaki Y, Sakaue M, et al. SEA0400, a novel and selective inhibitor of the Na+-Ca2+ exchanger, attenuates reperfusion injury in the in vitro and in vivo cerebral ischemic models. J Pharmacol Exp Ther. 2001;298(1):249–56.
Pignataro G, Tortiglione A, Scorziello A, Giaccio L, Secondo A, Severino B, et al. Evidence for a protective role played by the Na+/Ca2+ exchanger in cerebral ischemia induced by middle cerebral artery occlusion in male rats. Neuropharmacology. 2004;46(3):439–48. doi:10.1016/j.neuropharm.2003.09.015.
Trosper TL, Philipson KD. Effects of divalent and trivalent cations on Na+-Ca2+ exchange in cardiac sarcolemmal vesicles. Biochim Biophys Acta. 1983;731(1):63–8.
Watanabe Y, Iwamoto T, Matsuoka I, Ohkubo S, Ono T, Watano T, et al. Inhibitory effect of 2,3-butanedione monoxime (BDM) on Na(+)/Ca(2+) exchange current in guinea-pig cardiac ventricular myocytes. Br J Pharmacol. 2001;132(6):1317–25. doi:10.1038/sj.bjp.0703926.
de la Pena P, Reeves JP. Inhibition and activation of Na+-Ca2+ exchange activity by quinacrine. Am J Physiol. 1987;252(1 Pt 1):C24–9.
Iwamoto T, Kita S, Uehara A, Imanaga I, Matsuda T, Baba A, et al. Molecular determinants of Na+/Ca2+ exchange (NCX1) inhibition by SEA0400. J Biol Chem. 2004;279(9):7544–53. doi:10.1074/jbc.M310491200.
Hasegawa H, Muraoka M, Matsui K, Kojima A. Discovery of a novel potent Na+/Ca2+ exchanger inhibitor: design, synthesis and structure-activity relationships of 3,4-dihydro-2(1H)-quinazolinone derivatives. Bioorg Med Chem Lett. 2003;13(20):3471–5.
Erdreich A, Rahamimoff H. The inhibition of Ca uptake in cardiac membrane vesicles by verapamil. Biochem Pharmacol. 1984;33(14):2315–23.
Iwamoto T, Uehara A, Nakamura TY, Imanaga I, Shigekawa M. Chimeric analysis of Na(+)/Ca(2+) exchangers NCX1 and NCX3 reveals structural domains important for differential sensitivity to external Ni(2+) or Li(+). J Biol Chem. 1999;274(33):23094–102.
Reeves JP, Bailey CA, Hale CC. Redox modification of sodium-calcium exchange activity in cardiac sarcolemmal vesicles. J Biol Chem. 1986;261(11):4948–55.
Amoroso S, Tortiglione A, Secondo A, Catalano A, Montagnani S, Di Renzo G, et al. Sodium nitroprusside prevents chemical hypoxia-induced cell death through iron ions stimulating the activity of the Na+-Ca2+ exchanger in C6 glioma cells. J Neurochem. 2000;74(4):1505–13.
Cengiz P, Kleman N, Uluc K, Kendigelen P, Hagemann T, Akture E, et al. Inhibition of Na+/H+ exchanger isoform 1 is neuroprotective in neonatal hypoxic ischemic brain injury. Antioxid Redox Signal. 2011;14(10):1803–13. doi:10.1089/ars.2010.3468.
Kostandy BB. The role of glutamate in neuronal ischemic injury: the role of spark in fire. Neurol Sci: Off J Italian Neurol Soc Italian Soc Clin Neurophysiol. 2012;33(2):223–37. doi:10.1007/s10072-011-0828-5.
Szydlowska K, Tymianski M. Calcium, ischemia and excitotoxicity. Cell Calcium. 2010;47(2):122–9. doi:10.1016/j.ceca.2010.01.003.
Robertson CL, Scafidi S, McKenna MC, Fiskum G. Mitochondrial mechanisms of cell death and neuroprotection in pediatric ischemic and traumatic brain injury. Exp Neurol. 2009;218(2):371–80. doi:10.1016/j.expneurol.2009.04.030.
Celsi F, Pizzo P, Brini M, Leo S, Fotino C, Pinton P, et al. Mitochondria, calcium and cell death: a deadly triad in neurodegeneration. Biochim Biophys Acta. 2009;1787(5):335–44. doi:10.1016/j.bbabio.2009.02.021.
Rossi DJ, Oshima T, Attwell D. Glutamate release in severe brain ischaemia is mainly by reversed uptake. Nature. 2000;403(6767):316–21. doi:10.1038/35002090.
Stys PK, Waxman SG, Ransom BR. Ionic mechanisms of anoxic injury in mammalian CNS white matter: role of Na+ channels and Na(+)-Ca2+ exchanger. J Neurosci: Off J Soc Neurosci. 1992;12(2):430–9.
Aarts M, Iihara K, Wei WL, Xiong ZG, Arundine M, Cerwinski W, et al. A key role for TRPM7 channels in anoxic neuronal death. Cell. 2003;115(7):863–77.
Amoroso S, Sensi S, di Renzo G, Annunziato L. Inhibition of the Na(+)-Ca++ exchanger enhances anoxia and glucopenia-induced [3H] aspartate release in hippocampal slices. J Pharmacol Exp Ther. 1993;264(2):515–20.
Breder J, Sabelhaus CF, Opitz T, Reymann KG, Schroder UH. Inhibition of different pathways influencing Na(+) homeostasis protects organotypic hippocampal slice cultures from hypoxic/hypoglycemic injury. Neuropharmacology. 2000;39(10):1779–87.
Czyz A, Baranauskas G, Kiedrowski L. Instrumental role of Na+ in NMDA excitotoxicity in glucose-deprived and depolarized cerebellar granule cells. J Neurochem. 2002;81(2):379–89.
Pilitsis JG, Diaz FG, O’Regan MH, Phillis JW. Inhibition of Na(+)/Ca(2+) exchange by KB-R7943, a novel selective antagonist, attenuates phosphoethanolamine and free fatty acid efflux in rat cerebral cortex during ischemia-reperfusion injury. Brain Res. 2001;916(1–2):192–8.
Tortiglione A, Pignataro G, Minale M, Secondo A, Scorziello A, Di Renzo GF, et al. Na+/Ca2+ exchanger in Na+ efflux-Ca2+ influx mode of operation exerts a neuroprotective role in cellular models of in vitro anoxia and in vivo cerebral ischemia. Ann N Y Acad Sci. 2002;976:408–12.
Jeffs GJ, Meloni BP, Bakker AJ, Knuckey NW. The role of the Na(+)/Ca(2+) exchanger (NCX) in neurons following ischaemia. J Clin Neurosci: Off J Neurosurg Soc Austral. 2007;14(6):507–14. doi:10.1016/j.jocn.2006.07.013.
Amoroso S, De Maio M, Russo GM, Catalano A, Bassi A, Montagnani S, et al. Pharmacological evidence that the activation of the Na(+)-Ca2+ exchanger protects C6 glioma cells during chemical hypoxia. Br J Pharmacol. 1997;121(2):303–9. doi:10.1038/sj.bjp.0701092.
Sirabella R, Secondo A, Pannaccione A, Scorziello A, Valsecchi V, Adornetto A, et al. Anoxia-induced NF-kappaB-dependent upregulation of NCX1 contributes to Ca2+ refilling into endoplasmic reticulum in cortical neurons. Stroke: J Cerebral Circ. 2009;40(3):922–9. doi:10.1161/STROKEAHA.108.531962.
Annunziato L, Cataldi M, Pignataro G, Secondo A, Molinaro P. Glutamate-independent calcium toxicity: introduction. Stroke: J Cerebral Circ. 2007;38(2 Suppl):661–4. doi:10.1161/01.STR.0000247942.42349.37.
Floyd CL, Gorin FA, Lyeth BG. Mechanical strain injury increases intracellular sodium and reverses Na+/Ca2+ exchange in cortical astrocytes. Glia. 2005;51(1):35–46. doi:10.1002/glia.20183.
Amran MS, Homma N, Hashimoto K. Pharmacology of KB-R7943: a Na+-Ca2+ exchange inhibitor. Cardiovasc Drug Rev. 2003;21(4):255–76.
Wiczer BM, Marcu R, Hawkins BJ. KB-R7943, a plasma membrane Na(+)/Ca(2+) exchanger inhibitor, blocks opening of the mitochondrial permeability transition pore. Biochem Biophys Res Commun. 2014;444(1):44–9. doi:10.1016/j.bbrc.2014.01.009.
Santo-Domingo J, Vay L, Hernandez-Sanmiguel E, Lobaton CD, Moreno A, Montero M, et al. The plasma membrane Na+/Ca2+ exchange inhibitor KB-R7943 is also a potent inhibitor of the mitochondrial Ca2+ uniporter. Br J Pharmacol. 2007;151(5):647–54. doi:10.1038/sj.bjp.0707260.
Reuter H, Henderson SA, Han T, Matsuda T, Baba A, Ross RS, et al. Knockout mice for pharmacological screening: testing the specificity of Na+-Ca2+ exchange inhibitors. Circ Res. 2002;91(2):90–2.
Morimoto N, Kita S, Shimazawa M, Namimatsu H, Tsuruma K, Hayakawa K, et al. Preferential involvement of Na(+)/Ca(2)(+) exchanger type-1 in the brain damage caused by transient focal cerebral ischemia in mice. Biochem Biophys Res Commun. 2012;429(3–4):186–90. doi:10.1016/j.bbrc.2012.10.114.
Ranciat-McComb NS, Bland KS, Huschenbett J, Ramonda L, Bechtel M, Zaidi A, et al. Antisense oligonucleotide suppression of Na(+)/Ca(2+) exchanger activity in primary neurons from rat brain. Neurosci Lett. 2000;294(1):13–6.
Bano D, Young KW, Guerin CJ, Lefeuvre R, Rothwell NJ, Naldini L, et al. Cleavage of the plasma membrane Na+/Ca2+ exchanger in excitotoxicity. Cell. 2005;120(2):275–85. doi:10.1016/j.cell.2004.11.049.
Schwab BL, Guerini D, Didszun C, Bano D, Ferrando-May E, Fava E, et al. Cleavage of plasma membrane calcium pumps by caspases: a link between apoptosis and necrosis. Cell Death Differ. 2002;9(8):818–31. doi:10.1038/sj.cdd.4401042.
Li LL, Sun LN, Zhou HY, Li ZB, Wang XL. Selective alteration of expression of Na+/Ca2+ exchanger isoforms after transient focal cerebral ischemia in rats. Neurosci Lett. 2006;404(3):249–53. doi:10.1016/j.neulet.2006.06.003.
Pignataro G, Boscia F, Esposito E, Sirabella R, Cuomo O, Vinciguerra A, et al. NCX1 and NCX3: two new effectors of delayed preconditioning in brain ischemia. Neurobiol Dis. 2012;45(1):616–23. doi:10.1016/j.nbd.2011.10.007.
Cross JL, Boulos S, Shepherd KL, Craig AJ, Lee S, Bakker AJ, et al. High level over-expression of different NCX isoforms in HEK293 cell lines and primary neuronal cultures is protective following oxygen glucose deprivation. Neurosci Res. 2012;73(3):191–8. doi:10.1016/j.neures.2012.04.007.
Pignataro G, Gala R, Cuomo O, Tortiglione A, Giaccio L, Castaldo P, et al. Two sodium/calcium exchanger gene products, NCX1 and NCX3, play a major role in the development of permanent focal cerebral ischemia. Stroke: J Cerebral Circ. 2004;35(11):2566–70. doi:10.1161/01.STR.0000143730.29964.93.
Gandhi A, Siedlecka U, Shah AP, Navaratnarajah M, Yacoub MH, Terracciano CM. The effect of SN-6, a novel sodium-calcium exchange inhibitor, on contractility and calcium handling in isolated failing rat ventricular myocytes. Cardiovasc Ther. 2013;31(6):e115–24. doi:10.1111/1755-5922.12045.
Inokuchi Y, Shimazawa M, Nakajima Y, Komuro I, Matsuda T, Baba A, et al. A Na+/Ca2+ exchanger isoform, NCX1, is involved in retinal cell death after N-methyl-D-aspartate injection and ischemia-reperfusion. J Neurosci Res. 2009;87(4):906–17. doi:10.1002/jnr.21906.
Newell EW, Stanley EF, Schlichter LC. Reversed Na+/Ca2+ exchange contributes to Ca2+ influx and respiratory burst in microglia. Channels. 2007;1(5):366–76.
Boscia F, Gala R, Pannaccione A, Secondo A, Scorziello A, Di Renzo G, et al. NCX1 expression and functional activity increase in microglia invading the infarct core. Stroke: J Cerebral Circ. 2009;40(11):3608–17. doi:10.1161/STROKEAHA.109.557439.
Molinaro P, Cataldi M, Cuomo O, Viggiano D, Pignataro G, Sirabella R, et al. Genetically modified mice as a strategy to unravel the role played by the Na(+)/Ca (2+) exchanger in brain ischemia and in spatial learning and memory deficits. Adv Exp Med Biol. 2013;961:213–22. doi:10.1007/978-1-4614-4756-6_18.
Jeon D, Chu K, Jung KH, Kim M, Yoon BW, Lee CJ, et al. Na(+)/Ca(2+) exchanger 2 is neuroprotective by exporting Ca(2+) during a transient focal cerebral ischemia in the mouse. Cell Calcium. 2008;43(5):482–91. doi:10.1016/j.ceca.2007.08.003.
Jeffs GJ, Meloni BP, Sokolow S, Herchuelz A, Schurmans S, Knuckey NW. NCX3 knockout mice exhibit increased hippocampal CA1 and CA2 neuronal damage compared to wild-type mice following global cerebral ischemia. Exp Neurol. 2008;210(1):268–73. doi:10.1016/j.expneurol.2007.10.013.
Molinaro P, Cuomo O, Pignataro G, Boscia F, Sirabella R, Pannaccione A, et al. Targeted disruption of Na+/Ca2+ exchanger 3 (NCX3) gene leads to a worsening of ischemic brain damage. J Neurosci: Off J Soc Neurosci. 2008;28(5):1179–84. doi:10.1523/JNEUROSCI. 4671-07.2008.
Bano D, Munarriz E, Chen HL, Ziviani E, Lippi G, Young KW, et al. The plasma membrane Na+/Ca2+ exchanger is cleaved by distinct protease families in neuronal cell death. Ann N Y Acad Sci. 2007;1099:451–5. doi:10.1196/annals.1387.006.
Gidday JM. Cerebral preconditioning and ischaemic tolerance. Nat Rev Neurosci. 2006;7(6):437–48. doi:10.1038/nrn1927.
Pignataro G, Esposito E, Cuomo O, Sirabella R, Boscia F, Guida N, et al. The NCX3 isoform of the Na+/Ca2+ exchanger contributes to neuroprotection elicited by ischemic postconditioning. J Cerebral Blood Flow Metab: Off J Int Soc Cerebral Blood Flow Metab. 2011;31(1):362–70. doi:10.1038/jcbfm.2010.100.
Gobbi P, Castaldo P, Minelli A, Salucci S, Magi S, Corcione E, et al. Mitochondrial localization of Na+/Ca2+ exchangers NCX1-3 in neurons and astrocytes of adult rat brain in situ. Pharmacol Res: Off J Italian Pharmacol Soc. 2007;56(6):556–65. doi:10.1016/j.phrs.2007.10.005.
Castaldo P, Cataldi M, Magi S, Lariccia V, Arcangeli S, Amoroso S. Role of the mitochondrial sodium/calcium exchanger in neuronal physiology and in the pathogenesis of neurological diseases. Prog Neurobiol. 2009;87(1):58–79. doi:10.1016/j.pneurobio.2008.09.017.
Cuomo O, Pignataro G, Gala R, Boscia F, Tortiglione A, Molinaro P, et al. Involvement of the potassium-dependent sodium/calcium exchanger gene product NCKX2 in the brain insult induced by permanent focal cerebral ischemia. Ann N Y Acad Sci. 2007;1099:486–9. doi:10.1196/annals.1387.051.
Cuomo O, Gala R, Pignataro G, Boscia F, Secondo A, Scorziello A, et al. A critical role for the potassium-dependent sodium-calcium exchanger NCKX2 in protection against focal ischemic brain damage. J Neurosci: Off J Soc Neurosci. 2008;28(9):2053–63. doi:10.1523/JNEUROSCI. 4912-07.2008.
Kiedrowski L. NCX and NCKX operation in ischemic neurons. Ann N Y Acad Sci. 2007;1099:383–95. doi:10.1196/annals.1387.035.
Wakimoto K, Kobayashi K, Kuro OM, Yao A, Iwamoto T, Yanaka N, et al. Targeted disruption of Na+/Ca2+ exchanger gene leads to cardiomyocyte apoptosis and defects in heartbeat. J Biol Chem. 2000;275(47):36991–8. doi:10.1074/jbc.M004035200.
Henderson SA, Goldhaber JI, So JM, Han T, Motter C, Ngo A, et al. Functional adult myocardium in the absence of Na+-Ca2+ exchange: cardiac-specific knockout of NCX1. Circ Res. 2004;95(6):604–11. doi:10.1161/01.RES.0000142316.08250.68.
Acknowledgments
I would like to express my sincere thanks and appreciation to Dr. Seena Ajit, Drexel University College of Medicine for her continuous support and encouragement. I also want to extend my thanks to Dr. Ole Mortensen and Dr. James Barrett. I acknowledge the help of Diana Winters in editing the review. The author is a recipient of a Fulbright grant funded by the US Department of State Bureau of Educational and Cultural Affairs.
Compliance with Ethical Standards
ᅟ
Conflicts of Interest
The author declares no conflict of interest.
Research Involving Human Participants and/or Animals
This article does not contain any studies with human participants or animals performed by the author.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Shenoda, B. The Role of Na+/Ca2+ Exchanger Subtypes in Neuronal Ischemic Injury. Transl. Stroke Res. 6, 181–190 (2015). https://doi.org/10.1007/s12975-015-0395-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12975-015-0395-9