
Abstract
Genetics and genomics are increasingly relevant to primary healthcare but training is unavailable to many practitioners. Education that can be accessed by practitioners without cost or travel is essential. The Gen-Equip project was formed to provide effective education in genetics for primary healthcare in Europe and so improve patient care. Partners include patient representatives and specialists in genetics and primary care from six countries. Here, we report the progress and challenges involved in creating a European online educational program in genetics.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Primary care can be provided by a range of health professionals and is defined by the World Health Organization as health care that is directly accessible by patients as the first point of contact, as well as being comprehensive and ongoing (WHO 2016). In addition to managing symptomatic patients, primary care involves prevention, pre-symptomatic detection of disease, and early diagnosis, all of which are relevant to patients at risk of genetic disease.
With expansion of genetics and genomics in mainstream healthcare, primary care professionals are increasingly expected to provide appropriate services to their patients who have or may be at risk of a genetic condition. At least 10% of patients have a condition with a genetic component (Global Genes 2017) and these will be seen in primary care. It is important that primary care professionals can recognize whether a patient might be affected by, or carry, a genetic condition; and secondly are aware of situations where genetic/genomic investigation may help inform management and treatment. This requires appropriate skills and genetics knowledge to deliver care that addresses patient needs and maximises the use of health resources.
Primary care providers are currently challenged to identify patients whose symptoms, physical findings, or family history indicates the need for genetic diagnosis and/or testing, to determine how to use genetic information most effectively to improve disease prevention and to target different options for disease management (Carroll et al., 2016; Christensen et al., 2016; Lopes-Júnior et al., 2016). Primary healthcare professionals face substantial challenges in utilizing genetic information, namely translating genetic risk into clinical action (Christensen et al., 2016). It is unsurprising therefore that full integration of genomic medicine in primary care settings has been slow to materialise (Rahimzadeh & Bartlett, 2014).
Previous studies indicate that primary care practitioners lack practical knowledge of genetics and confidence in providing services related to genetic conditions (Carroll et al., 2016; Houwink et al., 2011, 2012). There is therefore strong potential for professionals to fail to recognize patients who are at risk of genetic disease, resulting in them not being referred to specialist services or being managed inappropriately.
The intervention
The majority of other educational projects to enhance understanding of genetics in primary care have been based in a single country, as was evidenced by the studies included in a systematic review (Paneque et al., 2016). For this and reasons of funding and travel and time commitment needed, access to genetics education by primary care practitioners was limited. Therefore, to maximize efforts and enable primary care practitioners in multiple countries and settings to access education, we formed a project team comprising partners from six countries with representatives from primary care, clinical genetics and patient organisations. The aim was to improve care of patients with genetic conditions in Europe by maximizing access to genetics education in primary care professionals.
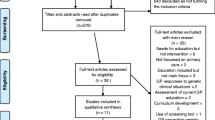
As a foundation for the project, we undertook a systematic review of genetic education for primary care (Paneque et al., 2016). Using the results of that review and two workshops attended by partners of the project and key stakeholders (from primary care and public health), a genetics education curriculum for European professionals was prepared (www.primarycaregenetics.org).
The Gen-Equip project has proceeded on the basis of providing case-based modules built around a typical clinical consultation with a primary care professional. The learning objectives of the educational activities are to enable primary care practitioners:
-
to recognize a patient who may be at risk of or affected by a genetic condition;
-
to assess and refer patients for specialist genetic services appropriately;
-
to enhance the ability of primary care practitioners to support patients with a genetic condition or risk and encourage communication within families.
Initially, a website (www.primarycaregenetics.org), in six different languages, was built as a tool for dissemination. At the initial stakeholder meeting, primary care professionals who were present strongly advised that, due to lack of foundational knowledge of genetics, the education should be focused on the recognition and family-management of constitutional-genome based genetic conditions, rather than attempting to cover the more diverse and rapidly advancing field of the application of somatic genomic alteration for informing targeted treatment. Nine case-based modules set in primary care were prepared, with two-three partners leading on each module. The text for each was prepared and circulated for comments among all partners until consensus was reached on the content: this ensured that the content was acceptable to primary care practitioners, genetics experts and patient representatives in the project team. Additional videos and other resources were prepared and the modules were launched in English. Each one was then translated into languages of the partner countries, with additional modification to ensure that healthcare guidance and cultural norms were respected. This also required recording videos of simulated patients around which module was based in the local language and setting, translating all pre and post-module quizzes and all instructions for using the modules. To ensure consistency, one partner (based in UK) has managed the uploading of the materials onto the educational software and this in itself has been challenging as errors in spelling etc. in the different languages cannot be easily detected and all materials must be re-checked by the relevant partner in each country multiple times.
The modules are now available online and are accessible free of charge. As continuing professional development points are available when the modules are completed, learners are required to register using their name and email address. Module topics include familial cancer, familial hypercholesterolemia, inherited cardiac conditions, the child with a genetic condition, and pregnancy or reproduction-related scenarios (www.primarycaregenetics.org ). All have been accredited for Continuing Professional Education by the Royal College of General Practitioners and the European Specialist Nurses Organization. In addition, using the “Care Bundle” approach that has proven successful in other educational interventions, we have provided a set of accessible clinical tools for practice on the website.
A series of short online webinars are also available on the following core topics:
-
Taking and recording a family history
-
Genetic testing results and what they mean for your patient
-
Common inheritance patterns
-
Prenatal testing options
-
Referring your patient to genetic services.
Assessment
The success of the project is being assessed by the level of usage and uptake of the educational materials and the evidence that use of the educational materials are being effective in improving knowledge, skills and practice. We are investigating short- and long-term changes through the comparison of pre- and post-module test scores, a cross-sectional survey to assess usefulness to practice and user satisfaction as well as qualitative thematic analysis study to explore usefulness in daily practice.
To assess changes in knowledge, we aim to collect pre and post-module data from at least 350 individuals. We aim to achieve at least 30% increase in knowledge when pre and post course scores are compared. While the differences in scores vary markedly according to the topic of the module, initial evaluation indicates the model is effective. For example, based on 200 pre- and post-test scores, mean pre-test score for the breast/ovarian cancer module (where pre-test scores are among the highest for the modules) was 77.6% (standard error = 2.97), compared with the post-test score of 90.4% (standard error = 2.69) and this represented a highly significant difference in the means (t(33) = −5.87, p = 0.000). This type of assessment will be repeated for each partner country.
All professionals completing the modules have been asked to complete a survey giving feedback and again, initial feedback has been positive regarding the style of educational delivery and appropriateness for practice. A proportion of these will be interviewed in each partner country to assess how the educational content has influenced practice, for example to identify if there are barriers to using the knowledge in practice and if there are any changes in attitudes and experiences while discussing genetic risk and testing information. Factors such as concern about patient anxiety, not having access to specialist genetic services, and time constraints have been shown to be barriers to provision of appropriate genetic healthcare in primary care professionals (Mikat-Stevens et al., 2015), and the use of qualitative interviews to collect data will enable us to explore these issues. Initial user feedback has been very positive, with the majority of respondents indicating they would recommend the modules to colleagues.
Conclusion
Collaboration across different European countries has enabled efforts to develop quality resources to be maximized. The process of implementing this project has been enriched by the multidisciplinary nature of the partners involved, as well as the different experiences they provided according to their different healthcare settings and countries. It can be seen as a relevant model for designing and implementing appropriate educational programs for health professionals with varied professional backgrounds and taking into consideration the diversity of contexts for providing healthcare services. In addition, sustainability of the educational project is assured not only through individual partners, but the inclusion of the European Society for Human Genetics (ESHG) as an associate in the project to support promotion and dissemination and to provide a long-term repository for the materials.
The results of the final evaluation will indicate whether the efforts have been effective and will provide further guidance on effective training interventions for the future. All practitioners are invited to use the educational materials and to disseminate then to students or colleagues who may benefit from using them. Feedback on any aspect of the learning materials is welcomed (www.primarycaregenetics.org).
References
Carroll JC, Makuwaza T, Manca DP, Sopcak N, Permaul JA, O'Brien MA, Heisey R, Eisenhauer EA, Easley J, Krzyzanowska MK, Miedema B, Pruthi S, Sawka C, Schneider N, Sussman J, Urquhart R, Versaevel C, Grunfeld E (2016) Primary care providers' experiences with and perceptions of personalized genomic medicine. Canadian Family Physician Medecin De Famille Canadien 62:e626–e635
Christensen KD, Vassy JL, Jamal L, Lehmann LS, Slashinski MJ, Perry DL, Robinson JO, Blumenthal-Barby J, Feuerman LZ, Murray MF, Green RC, McGuire AL (2016) Are physicians prepared for whole genome sequencing? A qualitative analysis. Clin Genet 89:228–234
Global Genes ™ (2017) Rare Diseases: Facts and Statistics. https://globalgenes.org/rare-diseases-facts-statistics. Accessed 15 February 2017
Houwink EJ, Henneman L, Westerneng M, van Luijk SJ, Cornel MC, Jan Dinant G, van der Vleuten C (2012) Prioritization of future genetics education for general practitioners: a Delphi study. Genetics in Medicine 14:323–329
Houwink EJ, van Luijk SJ, Henneman L, van der Vleuten C, Jan Dinant G, Cornel MC (2011) Genetic educational needs and the role of genetics in primary care: a focus group study with multiple perspectives. BMC Fam Pract 12:5
Lopes-Júnior LC, Carvalho Júnior PM, De Faria Ferraz VE, Nascimento LC, van Riper M, Flória-Santos M (2016) Genetic education, knowledge and experiences between nurses and physicians in primary care in Brazil: a cross-sectional study. Nursing & Health Sciences . doi:10.1111/nhs.1230411 August 2016
Mikat-Stevens NA, Larson IA, Tarini BA (2015) Primary-care providers' perceived barriers to integration of genetics services: a systematic review of the literature. Genetics In Medicine: Official Journal Of The American College Of Medical Genetics 17:169–176
Paneque M, Turchetti D, Jackson L, Lunt P, Houwink E, Skirton H (2016) A systematic review of interventions to provide genetics education for primary care. BMC Fam Pract 17:89
Rahimzadeh V, Bartlett G (2014) Genetics and primary care: where are we headed? J Transl Med 12:238–238
World Health Organisation. Primary Health Care: Main terminology (2016) http://www.euro.who.int/en/health-topics/Health-systems/primary-health-care/main-terminology. Accessed 15 February 2017
Acknowledgements
This project was co-funded by the European Union, Project Number 2014-1-UK01-KA204-000065 under the Erasmus + programme.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This project was co-funded by the European Union, Project Number 2014–1-UK01-KA204–000065 under the Erasmus + programme. Note: The material in this paper reflects only the author’s views and the European Commission and Ecorys UK are not responsible for any use that may be made of the information it contains.
Conflict of interest
The authors declare they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Paneque, M., Cornel, M.C., Curtisova, V. et al. Implementing genetic education in primary care: the Gen-Equip programme. J Community Genet 8, 147–150 (2017). https://doi.org/10.1007/s12687-017-0296-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12687-017-0296-6