
Abstract
Objectives
Over the last years, mindfulness meditation has been claimed to be effective in enhancing several cognitive domains, including executive control. However, these claims have been mostly based on findings pertaining to case-control and cross-sectional studies, which are by nature unable to reveal causal relationships. Aiming to address this issue, we set out to conduct the first quantitative assessment of the literature concerning mindfulness meditation as an enhancer for executive control considering only randomized controlled studies.
Methods
We conducted a systematic review and meta-analysis covering experimental studies testing the effect of mindfulness meditation training on at least one executive control function (working memory, inhibitory control, or cognitive flexibility) in adult samples. Four databases were examined, resulting in the identification of 822 candidate references. After a systematic filtering process, a set of 16 studies was retained for evaluation, of which 13 could be included in a subsequent meta-analysis.
Results
We found an average effect size of g = 0.34 [0.16, 0.51], indicating a small-to-medium effect of mindfulness meditation training in enhancing executive control. Effect sizes for individual functions were g = 0.42 [0.10, 0.74] for working memory, g = 0.42 [0.20, 0.63] for inhibitory control, and g = 0.09 [−0.13, 0.31] for cognitive flexibility. Funnel plot asymmetry analysis revealed no evidence of publication bias.
Conclusions
Taken together, our findings provide preliminary and moderate yet positive evidence supporting the enhancing effects of mindfulness meditation on executive control. Shortcomings of included studies and considerations for future empirical and meta-analytical research are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The scientific interest in mindfulness meditation has grown exponentially over the last decades (Tang 2017; Van Dam et al. 2018). In recent years, studies have reported beneficial effects of mindfulness meditation on outcomes pertaining to a variety of domains, including mental and physical health (Grossman et al. 2004), brain and cognitive function (Tang et al. 2015), and interpersonal functioning (Mcgill et al. 2016). In parallel, several mindfulness-based programs are currently being integrated into a number of institutional settings including the healthcare system (Demarzo et al. 2015), the educational system (Sibinga et al. 2016), the workplace (Good et al. 2016), and the military (Johnson et al. 2014).
It is broadly acknowledged that there are two styles of mindfulness meditation practice: focused attention (FA) and open monitoring (OM) (Lutz et al. 2008; Malinowski 2013; Tang et al. 2015). In FA meditation, the practitioner sustains the attentional focus on a chosen object (most commonly one’s breath) and returns it to this anchor each time the mind wanders. Accordingly, it is theorized that FA develops three attentional control processes, along with their underpinning neural networks: (a) the monitoring faculty that remains vigilant to mind-wandering while attention is sustained to the anchor (alerting network); (b) the ability to detect mind-wandering (salience network) and to disengage from it (executive network); and (c) the ability to redirect the focus to the anchor (orienting network) (Lutz et al. 2008; Malinowski 2013). Some proficiency in FA meditation is required to transition to OM practice, in which the aim is to remain solely in the monitoring state maintaining an open, nonreactive attention to all arising and passing mental events. OM would further develop the practitioner’s meta-awareness of inner mental processes, including mind-wandering (Lutz et al. 2008).
Attentional processes can be enhanced by regular repetition of tasks that involve specific attention networks (Posner et al. 2015). On the other hand, it is well documented that mind-wandering can substantially compromise available attentional and executive control resources, especially when needed to be sustained over prolonged periods of time (Thomson et al. 2015). By systematically strengthening the aforementioned neurocognitive networks (via FA), as well as by increasing one’s capacity to be aware of and disengage from mind-wandering (via FA and OM), mindfulness meditation has been proposed as a potential means for cognitive enhancement (e.g., Lindsay and Creswell 2017; Lutz et al. 2008; Malinowski 2013). Under this proposal, mindfulness meditation training would enhance (executive) attention processes both by increasing available resources and by allowing for more efficient use of them. Even though these explanations remain largely speculative, empirical evidence supporting the cognitive enhancing effect of mindfulness meditation has indeed started to emerge regarding various cognitive functions, which include—yet are not limited to—the executive control domain (Chiesa et al. 2011; Gallant 2016; Lao et al. 2016).
Executive control is a central piece of human cognitive architecture. Also referred to as executive functioning or cognitive control, executive control encompasses a family of top-down cognitive processes that scaffolds human goal-directed behavior and self-regulation. Research has shown that executive control is relevant for mental and physical health (Penadés et al. 2007; Will Crescioni et al. 2011), academic and professional success (Bailey 2007; Borella et al. 2010), or simply to enjoy a better quality of life (Brown and Landgraf 2010). To consider some examples, better executive control has been linked to healthier eating (Calvo et al. 2014), better math and reading competence in school (Checa et al. 2008), better marital satisfaction (Eakin et al. 2004), and more prosocial behavior (Broidy et al. 2003). In turn, dysfunction of this system, either due to aging, stroke, attention-deficit/hyperactivity disorder, or else, may hinder leading an independent life (Chan et al. 2008). As research shows, developing strategies and tools capable to strengthen executive control entails a highly relevant societal challenge to take on.
There have been various formulations of executive control, ranging from views considering it as a unitary multipurpose control system to fractionated models conceiving it as a collection of relatively independent executive functions (for a review, see Morton et al. 2011). Among fractionated perspectives, there is general agreement in differentiating three core executive functions: working memory, inhibitory control, and cognitive flexibility (Diamond 2013; Miyake et al. 2000).
The present study follows the conceptual framework and definitions proposed by Diamond (2013). According to Diamond (2013), working memory involves holding information for processing while simultaneously being able to manipulate it (e.g., maintaining task-relevant information and relating it to long-term memory content in order to solve a particular problem). Examples of tasks tapping into working memory are the Backward Digit Span (that requires to hold in memory a series of numbers while rehearsing them in inverse order) or the N-Back (where the subject is presented with a sequence of stimuli, having to indicate when the current stimulus matches the one shown n presentations earlier in the sequence).
Inhibitory control involves being able to control one’s behavior, attention, thoughts, and/or emotions in order to override a strong internal predisposition or external lure in benefit of longer-term goals. The Stroop test (where the subject is required to respond to the color of the ink of words while inhibiting attending to its meaning in order to avoid the more automatic word naming response) and the Go/No-Go task (that requires the subject to repeatedly respond by pressing a button, but to inhibit that habitual response when certain rare stimuli are presented) are two popular examples of tasks tapping into different aspects of inhibitory control.
Cognitive flexibility is defined as the ability to change our mental set to efficiently adapt to the demands of the environment. It is typically measured by means of tasks such as the Trail Making Test (where the subject is required to continuously switch between responding to numbers and letters) or the Wisconsin Card Sorting Task (that requires the subject to flexibly switch response strategies based on experimenter’s feedback on participants’ performance). Other higher-order executive-related processes such as planning, reasoning, or problem solving would be built upon the three core executive functions (Diamond 2013).
To date, three systematic reviews have assessed the effect of mindfulness meditation over executive control in adult population (Chiesa et al. 2011; Gallant 2016; Lao et al. 2016). Chiesa et al. (2011) evaluated the effects of several mindfulness-related practices (including Zen meditation, Vipassana retreats, or Mindfulness-Based Stress Reduction programs, among others) on a wide range of cognitive functions. Regarding executive control, the authors concluded that mindfulness training may be effective in enhancing executive attention and response inhibition (aspects of inhibitory control), verbal fluency (an aspect of cognitive flexibility), and working memory at different stages of training. Lao et al. (2016) conducted a similar review but focused on standardized Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT) programs, and found preliminary evidence for working memory and cognitive flexibility (but found no evidence for executive attention, while the evidence for response inhibition was mixed). Lastly, Gallant (2016) included mainly standardized mindfulness-based programs (such as MBSR or MBCT) but also other meditation practices (such as Vipassana or Shambala meditations) and narrowed the focus of the systematic review to just executive functioning. Gallant, in contrast, found inhibitory control to be the most consistently executive function improved by mindfulness meditation training, with more variable outcomes for working memory and cognitive flexibility.
Even though these findings may seem somewhat inconsistent, the discrepancies can arguably be attributed to two reasons. First, the reviews operationalized mindfulness meditation differently. Consequently, to an extent, each of them included studies evaluating different types of programs and meditations. This conceptual divergence likely affected their results and conclusions. Second, each review followed different taxonomies of cognition and executive control, thus seeming discrepancies may be partly just a terminological issue. To bring one example, Lao et al. (2016) concluded that “studies did not support […] executive function improvements. We found preliminary evidence for improvements in working memory and […] cognitive flexibility” (p. 109). These authors conceptualized working memory as a memory sub-function, while cognitive flexibility was not subsumed by any broader cognitive category. Such cognitive classification differs from the one followed by Gallant (2016), for whom executive functioning comprises inhibition (inhibitory control), updating (working memory), and shifting (cognitive flexibility). When taking into account these divergences, previous research appears to provide initial evidence for an enhancing effect of mindfulness meditation over executive control―even if such effect is still to be characterized in terms of both the particularities of the practices that bring it about and the specific cognitive sub-domains involved.
These preliminary findings of the positive effects of mindfulness meditation training in executive control outcomes (as well as in other cognitive and non-cognitive domains) are nonetheless paralleled by significant concerns that scholars from within and outside the field have raised about the methodological rigor behind much of extant evidence (e.g., Coronado-Montoya et al. 2016; Isbel and Summers 2017; Van Dam et al. 2018). One of the main limitations in the mindfulness literature refers to an overabundance of research methodologies that are unable to reveal causal relationships, such as the use of case-control and cross-sectional designs. High-standard methodologies such as randomized controlled trials (RCTs) have been rather scarce in the literature until recently (Creswell 2017). Accordingly, the above mentioned systematic reviews were largely based on non-experimental (i.e., non-RCT) studies. Moreover, none of them conducted a meta-analysis, likely because the inclusion of different study designs hindered the quantitative synthesis of the results. This circumstance underscores the need for a systematic and meta-analytic assessment of the literature circumscribed to only experimental studies, so as to validate―or otherwise update―our current understanding of the field.
On the basis of the above considerations, the aim of the present systematic review and meta-analysis was to evaluate and quantify the efficacy of mindfulness meditation (i.e., FA and OM practices) in enhancing executive control (i.e., working memory, inhibitory control, and cognitive flexibility) in adult population by―importantly―assessing RCTs exclusively. In addition, we also set out to assess whether findings in our review were likely to be overestimated by methodological biases in included studies (Higgins et al. 2011) and/or by publication bias (Sterne et al. 2011).
Methods
Search Procedure
The systematic review was conducted by following the PRISMA statement (Moher et al. 2009; see Supplementary Materials for a PRISMA checklist). We examined the databases Web of Science, PsycINFO, PubMed, and Cochrane Library in search of eligible studies, entering the following syntax: “(mindfulness OR “integrative body-mind training” OR meditat* OR MBSR OR MBCT OR IBMT OR MBRP OR MBRE OR “focused attention” OR “open monitoring” OR “body scan” OR zazen OR zen OR vipassana OR samatha OR “acceptance and commitment”) AND ((executive OR cognition OR “cognitive function” OR prefrontal) OR (inhibition OR inhibitory OR “self-control” OR (“selective attention” OR “focused attention” OR cingulate)) OR (“working memory” OR updating OR monitoring) OR (flexibility OR shifting OR switching)))”. The search was conducted on September 2017. It was limited to articles in English, Spanish, or French, published any time.
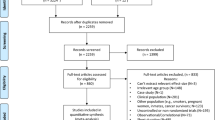
A set of 822 registers was obtained, from which we conducted a systematic filtering process (see Fig. 1). First, we removed 342 duplicates. Thereafter, inclusion criteria C1 to C5 (see “Selection Criteria”) were applied while screening the title and abstract of the remaining papers. Papers not clearly violating at least one criterion were retained for full-text examination. On a later stage, the first author (LC) and the second author (VP) independently examined the remaining set of 57 papers while applying the inclusion criteria. When necessary, we contacted the authors of the studies for paper retrieval and/or further clarification of its content. Inter-rater disagreements regarding the inclusion of studies were solved through discussion. In case of persistent disagreement, the fourth author (JL) was brought into the discussion until consensus was achieved. A set of 16 studies was retained after full search procedure (Ainsworth et al. 2013; Allen et al. 2012; Greenberg et al. 2013; Josefsson et al. 2014; Mallya and Fiocco 2016; Mitchell et al. 2017; Moynihan et al. 2013; Mrazek et al. 2013; Prätzlich et al. 2016; Sahdra et al. 2011; Schoenberg et al. 2014; Tang et al. 2007; Tsai and Chou 2016; Valls-Serrano et al. 2016; Wetherell et al. 2017; Zeidan et al. 2010).

PRISMA flowchart of study selection process
Selection Criteria
Studies needed to satisfy the five following criteria to be included in this review. (C1) The article is a peer-reviewed research report. Narrative and systematic reviews, doctoral dissertations, posters, registered study protocols, commentaries, books and book chapters, essays, and other theoretical accounts were therefore excluded. (C2) The study includes mindfulness mediation training as part of the intervention and assesses executive control as outcome according to the definitions provided in section below (see “Operational Definitions”). (C3) The study is a controlled trial with randomization of participants to experimental (receiving meditation training) and control group (not receiving meditation training). (C4) Study participants are adults (i.e., aged ≥ 18 years). (C5) Descriptions of experimental design, statistical analyses, and results of the study are complete and clearly described. Statistical analyses assess pre- to post-intervention differences in the experimental as compared with the control group (i.e., analysis of interaction between time of assessment [pre- and post-intervention] and group [experimental and control group] is addressed). Studies analyzing solely post-intervention differences were therefore excluded. In case of incompleteness or ambiguity, we contacted the first author of the study for further clarification. Studies for which clarification was not provided were excluded.
Operational Definitions
Mindfulness Meditation Training
We defined mindfulness meditation training as any training regime in which participants are taught one or both formal practices broadly recognized as mindfulness meditation (i.e., FA and/or OM meditation). Given that we aimed, to the extent possible, at evaluating the effects of mindfulness meditation free from ancillary factors (see Isbel and Summers 2017), at least one of the included mindfulness practices should be purely cognitive and, thus, not involve physical exercise or vocalization (interventions exclusively based on yoga or mantra repetition were therefore excluded). Lastly, the training regime should be sustained in time for more than one session (1-day brief laboratory inductions were therefore excluded).
Executive Control Assessment
Executive control assessments must include at least one neuropsychological test or computerized cognitive task involving reaction time or response accuracy measurement (studies using solely self- or other-report measures or only physiological, neurophysiological, or neuroimaging assessments were therefore excluded). Moreover, they must assess specifically either working memory or inhibitory control or cognitive flexibility as defined by Diamond (2013). General measures that conflate several sub-processes (e.g., the Symbol Digit Modalities Test, where participants presumably deploy working memory and set switching as well as other cognitive processes such as fine motor skills) were therefore excluded.
Data Extraction
We extracted the following information from each of the included studies: mean age of the sample being tested, sample size, duration of the intervention provided, total approximate dosage of the intervention (in minutes), population assessed (healthy or clinical), name of the intervention (when provided), control group used, and categorization of control group as active or passive (see Table 1). The first author extracted the data, and any queries were clarified with the second and fourth authors. Subsequently, we extracted from each study the data needed to calculate an effect size estimate (see “Data Analyses” for details). In three studies, data of interest were only depicted graphically (i.e., were not reported numerically). In those instances, we used the online software WebPlotDigitizer (Version 4.1; Rohatgi 2018) to extract the underlying numerical data from bar plots. WebPlotDigitizer has been shown as a valid and reliable tool (Drevon et al. 2017). When data were not available (either numerically or graphically), we contacted the corresponding authors of the study via e-mail for data retrieval. When no reply was obtained, we contacted all other authors. Unfortunately, for three of the included studies, either requested data were not available or a reply was not obtained from any of its authors. Therefore, only 13 of the 16 studies included in the systematic review could also be included in subsequent meta-analyses.
Risk of Bias Assessment
Methodological quality of included studies was assessed by means of the Cochrane Collaboration’s tool for assessing risk of bias (Higgins et al. 2011). The tool evaluates six potential sources of bias: (a) selection bias (whether randomization was adequately performed and allocation of participants to experimental/control group adequately concealed); (b) performance bias (whether participants and personnel providing the intervention were blind to study hypothesis); (c) detection bias (whether outcome assessors where blinded to study hypothesis); (d) attrition bias (whether amount, nature, or handling of incomplete outcome data was adequately addressed); (e) reporting bias (whether selective outcome reporting was found); and (f) other bias (whether the study appears to be at risk of other biases not previously evaluated). The Cochrane Collaboration’s tool diagnoses studies at high or low risk of bias for each of the aforementioned domains. Alternatively, if studies fail to provide enough information to assess their quality, they are evaluated as unclear risk of bias. We used RevMan (Version 5.3, The Cochrane Collaboration 2014) software to code information of each of the studies included and to generate graphical summaries of their individual and combined risk of bias (see Figs. 2 and 3).

Risk of bias summary

Risk of bias graph
Data Analyses
Effect Size and Variance
We conducted a meta-analysis in order to estimate the weighted averaged effect size found in our pool of included studies. To this end, Hedges’ g was chosen as effect size estimate for each individual study. Hedges’s g is a weighted version of Cohen’s d that allows for unbiased estimation when sample sizes are small (Borenstein et al. 2009). Given that all included studies used a pretest-posttest control group experimental design, we followed the procedure for effect size estimation recommended by Morris (2008). Thus, Hedges’ g is defined as follows:
where Mpost, T, Mpre, T, Mpost, C and Mpre, C are the post-intervention and pre-intervention mean scores for the treatment group and control group, respectively. In turn, SDpre is the pooled standard deviation of the pre-intervention scores defined as follows:
where nT, nC, SDpre, T and SDpre, C are the number of participants and the standard deviations of the scores at pre-intervention for treatment and control group, respectively. Lastly, CP is a correction for bias defined as follows:
In turn, the variance of Hedges’ g is defined as follows:
where r is the correlation between pre-test and post-test scores. As this statistic was not reported in any of the studies under consideration, we conducted our analyses assuming r = 0.5 in all cases. However, to ascertain the robustness of the results under this assumption, we conducted sensitivity analyses also imputing r = 0.25 and r = 0.75 in the calculations. In both cases, we obtained virtually identical results than those for r = 0.5. For the sake of simplicity, we only report the results of the latter.
Aggregates
Some of the included studies contributed effect sizes for more than one outcome of interest. In those instances, we calculated aggregated effect sizes so that each study ultimately had one overall effect size to contribute to subsequent meta-analyses. The rationale for this approach is described in detail in Borenstein et al. (2009). In short, calculation of aggregates deals with the problematic practice of treating outcomes coming from the same study as if they were independent, therefore assigning more relative weight to these studies and improperly estimating the precision of its effect. The procedure followed to compute a single aggregated effect size, \( \overline{g,} \) from two individual outcomes is defined as follows:
where g1 and g2 are the individual effect sizes. In turn, the variance of the aggregated effect size is defined as follows:
where \( {V}_{g_1} \)and \( {V}_{g_2} \)are the variances of g1 and g2, respectively, and r is the correlation between the two outcomes. In absence of the value of this correlation, it was set as 0.5 as proposed by Wampold et al. (1997). Some studies contributed three or four outcomes to our meta-analyses. Equations used to calculate aggregates in those instances are detailed in Borenstein et al. (2009).
To confirm the robustness of the results, we also conducted a multi-level meta-analysis including all the individual effect sizes, adding a random intercept at the study level to account for dependencies among effect sizes. The results of this analysis were virtually identical to those of the overall univariate meta-analysis with aggregate effect sizes (see “Meta-Analysis”). For the sake of simplicity, we only report the results of the latter.
Meta-Analysis
Four univariate meta-analyses were conducted: one to obtain the overall summary effect for all included studies and one per each individual executive function (i.e., working memory, inhibitory control, and cognitive flexibility). Random-effect models were fitted in all cases (Cumming 2013). Additionally, we conducted an Egger’s regression test for funnel plot asymmetry to evaluate the potential presence of publication bias within the literature reviewed. Funnel plots depict effect estimates against their standard error. Given that precision in estimating an effect will increase as the sample size increases (and thus the standard error decreases), results from small studies will spread largely whereas those from large studies will collapse closer to the mean effect estimate. In the absence of bias, results should distribute symmetrically around the mean effect estimate. However, publication bias will usually induce asymmetry in the distribution of effect sizes, as small studies with negative results will be more likely to be missing. Egger’s regression test statistically evaluates the degree of asymmetry of the distribution (Egger et al. 1997).
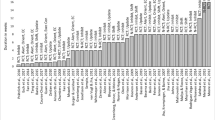
We used the metaphor package for R (Viechtbauer 2010) to conduct all meta-analytic procedures and to generate corresponding figures (forest plot and funnel plot, see Figs. 4 and 5). As proposed by Cohen (1992), we interpreted effect sizes of 0.2, 0.5, and 0.8 as small, medium, and large, respectively.

Forest plot of studies included in overall meta-analysis

Funnel plot of studies included in overall meta-analysis
Results
Qualitative Results
The present systematic review included 16 studies sampling a total of 1112 participants. In most cases, participants were novices to the practice of mindfulness meditation, when not completely meditation-naive. In one study, though, a certain level of experience was required for participation (i.e., having completed prior to recruitment at least three 5- to 10-day meditation retreats; Sahdra et al. 2011), and four studies did not provide information regarding previous experience with meditation (Moynihan et al. 2013; Mrazek et al. 2013; Schoenberg et al. 2014; Valls-Serrano et al. 2016). The studies assessed participants from the entire adult life-span (mean ages ranging from 20.3 to 73.4 years) and primarily evaluated the effect of mindfulness meditation in healthy participants (only four studies addressed clinical populations). The use of active/passive control group was evenly distributed among studies (eight studies used the former, seven used the latter, and one used both). A summary of these and other main characteristics of included studies is provided in Table 1. In total, 32 outcomes were assessed throughout the studies. Of them, 15 reported a statistically significant effect favoring the mindfulness meditation training program over the control intervention. No significant effects were reported for the remaining 17 outcomes. A summary of the assessments used as well as the main findings across the studies can be found in Table 2.
The Cochrane Collaboration tool suggested that included studies are, overall, at low risk in regard to attrition and reporting bias. However, risk regarding selection, performance, and detection bias remains largely unknown, given that most studies failed to report sufficient information to evaluate them. Summaries of individual and combined risk of bias are provided in Figs. 2 and 3.
Quantitative Results
Meta-Analysis
As mentioned above, we were able to obtain enough information to estimate an effect size for 13 of the 16 studies, which were therefore included in subsequent meta-analyses. The overall weighted mean effect size reported in these studies was g = 0.34, 95% CI [0.16, 0.51], z = 3.76, p < .001, indicating a small-to-medium effect favoring mindfulness training over control interventions in enhancing executive control. A forest plot with individual effect sizes as well as the weighted mean is depicted in Fig. 4. The test for heterogeneity failed to reach statistical significance Q(12) = 17.18, p = .143, I2 = 33.27%, 95% CI [0, 72.31]. A funnel plot representing individual effects against their standard error is depicted in Fig. 5. Egger’s regression test for funnel plot asymmetry was far from statistical significance, z = 0.40, p = .686, indicating that the result of the meta-analysis is unlikely to be overestimated by publication bias.
Effect size estimates for each individual executive function were as follows: g = 0.42, 95% CI [0.10, 0.74], z = 2.60, p = .009 for working memory; g = 0.42, 95% CI [0.20, 0.63], z = 3.83, p < .001 for inhibitory control; and g = 0.09, 95% CI [−0.13, 0.31], z = 0.80, p = .423 for cognitive flexibility. These results indicate small-to-medium effect sizes for working memory and inhibitory control and no significant effect for cognitive flexibility. Respectively, the results for heterogeneity tests were Q(3) = 2.66, p = .446, I2 = 0%, 95% CI [0, 94.70]; Q(8) = 9, p = .342, I2 = 18.33%, 95% CI [0, 74.74]; and Q(4) = 4.28, p = .369, I2 = 0%, 95% CI [0, 92.46].
Discussion
The aim of the present systematic review and meta-analysis was to assess the efficacy of mindfulness meditation as a cognitive enhancer for executive control. Our literature-search strategy allowed us to identify 16 randomized controlled studies conducted in adults, of which 13 could be included in a subsequent meta-analysis. Across these studies, the efficacy of mindfulness meditation (i.e., FA and OM meditation practices) in enhancing working memory, inhibitory control, and/or cognitive flexibility was assessed by means of neuropsychological tests and/or computerized cognitive tasks. Additionally, we assessed the methodological quality of the included studies and examined the possibility of publication bias in the literature reviewed.
Our findings indicate that mindfulness meditation exerts a small-to-medium effect in enhancing executive control (g = 0.34), with small-to-medium effect sizes for working memory (g = 0.42) and inhibitory control (g = 0.42) and no significant effect for cognitive flexibility (g = 0.09). Moreover, these effects seem to be consistent given the relatively small, non-significant heterogeneity found for each of them (especially in regard to each individual executive function). Furthermore, in light of the results of the funnel plot asymmetry analysis, the effects are not likely to be overestimated by publication biases. This pattern of findings, alongside the fact that they are obtained based on randomized controlled studies, suggests that mindfulness meditation training might indeed be effective in enhancing executive control.
The findings partially align with those from previous systematic reviews (Chiesa et al. 2011; Gallant 2016; Lao et al. 2016). Our results indicate that mindfulness meditation may be effective in enhancing working memory, as suggested by Chiesa et al. (2011) and Lao et al. (2016). Gallant (2016), in contrast, concluded that mindfulness meditation does not improve working memory in itself. In this author’s view, working memory improvements would be driven by an indirect effect, namely, by reductions in mind-wandering. As previously discussed, this is indeed a plausible mechanism underlying improvements in working memory following mindfulness meditation training. However, in our view, the “indirect” nature of the effect does not deny its existence. In fact, the three studies reviewed by Gallant reported working memory to be improved as a consequence of mindfulness meditation training (Jha et al. 2010; Mrazek et al. 2013; Zeidan et al. 2010).
A similar picture is found for inhibitory control, for which two previous reviews seem to align with ours (Chiesa et al. 2011; Gallant 2016) while one differs (Lao et al. 2016). The opposite pattern is seen regarding cognitive flexibility, with conclusions by Gallant (2016) more in line with ours, in contrast to those by Chiesa et al. (2011) and Lao et al. (2016). In these cases, differences in results seem to be based on conceptual discrepancies. As anticipated in the introduction, different conceptualizations of mindfulness meditation may lead to different search algorithms and study selection criteria and therefore to different sets of studies included. For instance, one researcher may define mindfulness training as comprised by only standardized mindfulness-based programs such as MBSR or MBCT, while another might also include Vipassana and other types of traditional meditation practice. The same applies to executive control. Following different cognitive taxonomies may render different sets of studies included. As an example, one researcher may consider executive attention to be part of inhibitory control, while another might consider it a separate attentional function. Ultimately, conceptual divergences―which are, to an extent, inherent to the study of psychological and cognitive constructs―may lead to different results and conclusions.
There is also a methodological reason potentially explaining differences between our results and those from previous reviews. In contrast to previous research, our study includes a meta-analysis. Findings obtained by meta-analyzing a set of studies can substantially differ from those rendered by simply “vote-counting” positive and null results in the same set of studies (Siddaway et al. 2019). For instance, a meta-analysis may find a significant positive effect when combining a set of non-significant findings coming from underpowered studies. One strength of our approach is to more accurately provide evidence in terms of the existence (or lack thereof) of an effect of mindfulness meditation in enhancing executive control, while additionally estimating the magnitude of such effect.
With all that being said, the results of our meta-analysis must be interpreted with caution due to at least two reasons. First, the risk of selection, performance, and detection bias in included studies is largely unknown. This is due to the fact that most studies failed to report sufficient information as for us to make informed judgments in this regard. In particular, details on how randomization and participants’ allocation to groups were performed (selection bias) and regarding the blinding of participants, instructors, and outcome assessors (performance and detection biases) were largely underreported. Empirical research has shown that bias in randomized controlled trials is associated with overestimated intervention effects (Higgins and Green 2011). For instance, interventions not reporting to use double-blinding have been shown to be associated with overestimated intervention effects by 18%, on average, as compared with those reporting it (Pildal et al. 2007). This circumstance, added to the fact that a small proportion of items per study were at high risk of bias, calls for prudence when interpreting the size of the effects found in the meta-analysis. Moreover, it underscores the value of thorough reporting practices in future empirical research, especially when also considering that three of our 16 studies (i.e., more than 18%) could not be meta-analyzed due to the scarcity of reported statistical information.
The second reason for caution interpreting our findings relates to the small set of studies that we were able to include, which may not afford sufficient statistical power for our tests to detect existing heterogeneity, both overall and, especially, within each executive function. This limitation may also affect the test for funnel plot asymmetry and, therefore, the inferred unlikelihood of publication bias in the literature reviewed. The small number of included studies also prevented us from conducting moderator analyses to investigate whether effect sizes were related to any study-level independent variable. In fact, it is recommended to have no less than 30 studies to conduct such analysis, and, in some cases, even 60 studies would not be adequate to perform them (Lau 2006). Given the value of revealing distinctive patterns of effectiveness depending on variations in the interventions provided (e.g., duration) or in populations assessed (e.g., young versus older adults), future meta-analyses must consider this approach once more studies are available.
Importantly, readers must also be careful when interpreting the seeming different effect found for cognitive flexibility as compared with working memory and inhibitory control. Two aspects are worth discussing in this regard. First, even though these meta-analyses suggest that such differences may exist in the population, we cannot be certain that these divergences are not reflecting just sampling variation. This is especially true considering the limited number of studies contributing to the meta-analyses for working memory and cognitive flexibility (four and five, respectively). Although the estimate for cognitive flexibility did not reach statistical significance, the upper bound of its confidence interval falls at g = 0.31, indicating that the true population effect might actually be closer to the estimates for working memory and inhibitory control than it seems prima facie. Second, a closer look at the tests used to assess each executive function reveals that cognitive flexibility was measured by means of paper-based neuropsychological tests in all but one case. In contrast, working memory and inhibitory control were more consistently assessed by means of computerized cognitive tasks. As has been previously discussed (Mak et al. 2018), it is possible that paper-based neuropsychological tests and computerized cognitive tasks are not equally sensitive. Computerized tasks allow measuring reaction times down to the millisecond, likely being more sensitive than paper-based assessments, which are usually based on accuracy scores. If this is true, the smaller effect found for cognitive flexibility as compared with working memory and inhibitory control could be partially driven by an artifact. Once again, as the number of experimental studies on the topic grows, larger meta-analyses will be needed to evaluate the presence of this differential effect, ideally conducting moderator analysis to reveal potential confounds derived from the type of assessments used (computerized vs. paper-based tasks).
It is worth mentioning that only two of the studies under consideration in the systematic review reported being registered trials, none of which could be included in the meta-analysis. Several meta-research studies show that effect sizes tend to be substantially smaller in registered trials (Kaplan and Irvin 2015; Papageorgiou et al. 2018), possibly due to selective reporting and other biases in unregistered research that artificially inflate effect sizes (Kerr 1998; Simmons et al. 2011). Ideally, future RCTs conducted in this topic should adhere to preregistered protocols and analysis plans, to ensure that their results are free from these sources of bias.
Another aspect that may inform future directions in the field stems from the small number of clinical studies that we were able to include. Four studies conducted in clinical populations were included in the systematic review, of which only three could be meta-analyzed. As a consequence, we were not able to investigate the differential effects of mindfulness meditation in clinical as compared with healthy populations, let alone to compare different clinical populations with each other. This is unfortunate, especially given that executive control is compromised in a wide range of psychological and psychiatric disorders from attention-deficit/hyperactivity disorder or addiction to depression or schizophrenia (for reviews, see Diamond 2013; Royall et al. 2002). More experimental studies in this area are needed. In turn, ascertaining to what extent mindfulness meditation is effective in enhancing executive control in such populations as well as investigating whether or not and how much this improvement translates into symptom amelioration or remission entails a highly relevant research challenge that we encourage future meta-analytical studies to take on.
In summary, this systematic and meta-analytic review provides preliminary and moderate yet positive evidence supporting the enhancing effects of mindfulness meditation in executive control. We hope that the current meta-analysis will pave the way to future experimental studies further evaluating this subject. Importantly, these studies must consider upgrading current reporting standards regarding methods used and results obtained, so as to facilitate cumulative science. As in any other scientific field, only a cooperative endeavor will render the most valuable outcomes. In turn, as the field continues to grow, we hope that future meta-analytic research will be able to afford a more comprehensive account of the effectiveness of mindfulness meditation by revealing not only to what extent it enhances executive control but also under what specific circumstances and for which particular populations it does so.
References
Ainsworth, B., Eddershaw, R., Meron, D., Baldwin, D. S., & Garner, M. (2013). The effect of focused attention and open monitoring meditation on attention network function in healthy volunteers. Psychiatry Research, 210(3), 1226–1231.
Allen, M., Dietz, M., Blair, K. S., van Beek, M., Rees, G., Vestergaard-Poulsen, P., … Roepstorff, A. (2012). Cognitive-affective neural plasticity following active-controlled mindfulness intervention. Journal of Neuroscience, 32(44), 15601–15610.
Bailey, C. E. (2007). Cognitive accuracy and intelligent executive function in the brain and in business. Annals of the New York Academy of Sciences, 1118(1), 122–141.
Borella, E., Carretti, B., & Pelegrina, S. (2010). The specific role of inhibition in reading comprehension in good and poor comprehenders. Journal of Learning Disabilities, 43(6), 541–552.
Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to meta-analysis. Chichester: John Wiley & Sons.
Broidy, L. M., Nagin, D. S., Tremblay, R. E., Bates, J. E., Brame, B., Dodge, K. A., … Vitaro, F. (2003). Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: a six-site, cross-national study. Developmental Psychology, 39(2), 222.
Brown, T. E., & Landgraf, J. M. (2010). Improvements in executive function correlate with enhanced performance and functioning and health-related quality of life: evidence from two large, double-blind, randomized, placebo-controlled trials in ADHD. Postgraduate Medicine, 122(5), 42–51.
Calvo, D., Galioto, R., Gunstad, J., & Spitznagel, M. B. (2014). Uncontrolled eating is associated with reduced executive functioning. Clinical Obesity, 4(3), 172–179.
Chan, R. C. K., Shum, D., Toulopoulou, T., & Chen, E. Y. H. (2008). Assessment of executive functions: review of instruments and identification of critical issues. Archives of Clinical Neuropsychology: The Official Journal of the National Academy of Neuropsychologists, 23(2), 201–216.
Checa, P., Rodríguez-Bailón, R., & Rueda, M. R. (2008). Neurocognitive and temperamental systems of self-regulation and early adolescents’ social and academic outcomes. Mind, Brain, and Education, 2(4), 177–187.
Chiesa, A., Calati, R., & Serretti, A. (2011). Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clinical Psychology Review, 31(3), 449–464.
Cochrane Collaboration. (2014). Review manager (RevMan) [computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155.
Coronado-Montoya, S., Levis, A. W., Kwakkenbos, L., Steele, R. J., Turner, E. H., & Thombs, B. D. (2016). Reporting of positive results in randomized controlled trials of mindfulness-based mental health interventions. PLoS One, 11(4), e0153220.
Creswell, J. D. (2017). Mindfulness interventions. Annual Review of Psychology, 68(1), 491–516.
Cumming, G. (2013). Understanding the new statistics: effect sizes, confidence intervals, and meta-analysis. London: Routledge.
Demarzo, M. M. P., Cebolla, A., & Garcia-Campayo, J. (2015). The implementation of mindfulness in healthcare systems: a theoretical analysis. General Hospital Psychiatry, 37(2), 166–171.
Diamond, A. (2013). Executive functions. Annual Review of Psychology, 64(1), 135–168.
Drevon, D., Fursa, S. R., & Malcolm, A. L. (2017). Intercoder reliability and validity of webplotdigitizer in extracting graphed data. Behavior Modification, 41(2), 323–339.
Eakin, L., Minde, K., Hechtman, L., Ochs, E., Krane, E., Bouffard, R., et al. (2004). The marital and family functioning of adults with ADHD and their spouses. Journal of Attention Disorders, 8(1), 1–10.
Egger, M., Davey Smith, G., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. British Medical Journal, 315(7109), 629–634.
Gallant, S. N. (2016). Mindfulness meditation practice and executive functioning: breaking down the benefit. Consciousness and Cognition, 40, 116–130.
Good, D. J., Lyddy, C. J., Glomb, T. M., Bono, J. E., Brown, K. W., Duffy, M. K., … Lazar, S. W. (2016). Contemplating mindfulness at work. Journal of Management, 42(1), 114–142.
Greenberg, J., Reiner, K., & Meiran, N. (2013). “Off with the old”: mindfulness practice improves backward inhibition. Frontiers in Psychology, 3, 618.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: a meta-analysis. Journal of Psychosomatic Research, 57(1), 35–43.
Higgins, J., & Green, S. (2011). Cochrane handbook for systematic reviews of interventions (version 5.1.0). The Cochrane collaboration. Retrieved from http://handbook-5-1.cochrane.org/.
Higgins, J. P. T., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., … Sterne, J. A. C. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. British Medical Journal, 343(7829), 1–9.
Isbel, B., & Summers, M. J. (2017). Distinguishing the cognitive processes of mindfulness: developing a standardised mindfulness technique for use in longitudinal randomised control trials. Consciousness and Cognition, 52, 75–92.
Jha, A. P., Stanley, E. A., Kiyonaga, A., Wong, L., & Gelfand, L. (2010). Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion, 10(1), 54–64.
Johnson, D. C., Thom, N. J., Stanley, E. A., Haase, L., Simmons, A. N., Shih, P.-A. B., … Paulus, M. P. (2014). Modifying resilience mechanisms in at-risk individuals: a controlled study of mindfulness training in marines preparing for deployment. The American Journal of Psychiatry, 171(8), 844–53.
Josefsson, T., Lindwall, M., & Broberg, A. G. (2014). The effects of a short-term mindfulness based intervention on self-reported mindfulness, decentering, executive attention, psychological health, and coping style: examining unique mindfulness effects and mediators. Mindfulness, 5(1), 18–35.
Kaplan, R. M., & Irvin, V. L. (2015). Likelihood of null effects of large NHLBI clinical trials has increased over time. PLoS One, 10(8), e0132382.
Kerr, N. L. (1998). HARKing: hypothesizing after the results are known. Personality and Social Psychology Review, 2(3), 196–217.
Lao, S. A., Kissane, D., & Meadows, G. (2016). Cognitive effects of MBSR/MBCT: a systematic review of neuropsychological outcomes. Consciousness and Cognition, 45, 109–123.
Lau, J. (2006). The case of the misleading funnel plot. British Medical Journal, 333(7568), 597.
Lindsay, E. K., & Creswell, J. D. (2017). Mechanisms of mindfulness training: monitor and acceptance theory (MAT). Clinical Psychology Review, 51, 48–59.
Lutz, A., Slagter, H. A., Dunne, J. D., & Davidson, R. J. (2008). Attention regulation and monitoring in meditation. Trends in Cognitive Sciences, 12(4), 163–169.
Mak, C., Whittingham, K., Cunnington, R., & Boyd, R. N. (2018). Efficacy of mindfulness-based interventions for attention and executive function in children and adolescents—A systematic review. Mindfulness, 9(1), 59–78.
Malinowski, P. (2013). Neural mechanisms of attentional control in mindfulness meditation. Frontiers in Neuroscience, 7, 8.
Mallya, S., & Fiocco, A. J. (2016). Effects of mindfulness training on cognition and well-being in healthy older adults. Mindfulness, 7(2), 453–465.
Mcgill, J., Adler-Baeder, F., & Rodriguez, P. (2016). Mindfully in love: a meta-analysis of the association between mindfulness and relationship satisfaction. Journal of Human Sciences and Extension, 4(1), 89–101.
Mitchell, J. T., McIntyre, E. M., English, J. S., Dennis, M. F., Beckham, J. C., & Kollins, S. H. (2017). A pilot trial of mindfulness meditation training for ADHD in adulthood: impact on core symptoms, executive functioning, and emotion dysregulation. Journal of Attention Disorders, 21(13), 1105–1120.
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cognitive Psychology, 41(1), 49–100.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine, 6(7), e1000097.
Morris, S. B. (2008). Estimating effect sizes from pretest-posttest-control group designs. Organizational Research Methods, 11(2), 364–386.
Morton, J. B., Ezekiel, F., & Wilk, H. A. (2011). Cognitive control: easy to identify but hard to define. Topics in Cognitive Science, 3(2), 212–216.
Moynihan, J. A., Chapman, B. P., Klorman, R., Krasner, M. S., Duberstein, P. R., Brown, K. W., & Talbot, N. L. (2013). Mindfulness-based stress reduction for older adults: effects on executive function, frontal alpha asymmetry and immune function. Neuropsychobiology, 68(1), 34–43.
Mrazek, M. D., Franklin, M. S., Phillips, D. T., Baird, B., & Schooler, J. W. (2013). Mindfulness training improves working memory capacity and GRE performance while reducing mind wandering. Psychological Science, 24(5), 776–781.
Papageorgiou, S. N., Xavier, G. M., Cobourne, M. T., & Eliades, T. (2018). Registered trials report less beneficial treatment effects than unregistered ones: a meta-epidemiological study in orthodontics. Journal of Clinical Epidemiology, 100, 44–52.
Penadés, R., Catalán, R., Rubia, K., Andrés, S., Salamero, M., & Gastó, C. (2007). Impaired response inhibition in obsessive compulsive disorder. European Psychiatry, 22(6), 404–410.
Pildal, J., Hróbjartsson, A., Jörgensen, K. J., Hilden, J., Altman, D. G., & Gøtzsche, P. C. (2007). Impact of allocation concealment on conclusions drawn from meta-analyses of randomized trials. International Journal of Epidemiology, 36(4), 847–857.
Posner, M. I., Rothbart, M. K., & Tang, Y. Y. (2015). Enhancing attention through training. Current Opinion in Behavioral Sciences, 4, 1–5.
Prätzlich, M., Kossowsky, J., Gaab, J., & Krummenacher, P. (2016). Impact of short-term meditation and expectation on executive brain functions. Behavioural Brain Research, 297, 268–276.
Rohatgi, A. (2018). WebPlotDigitizer (version 4.1) [computer software]. Retrieved from https://automeris.io/WebPlotDigitizer/
Royall, D. R., Lauterbach, E. C., Cummings, J. L., Reeve, A., Rummans, T. A., Kaufer, D. I., … Coffey, C. E. (2002). Executive control function: a review of its promise and challenges for clinical research. The Journal of Neuropsychiatry and Clinical Neurosciences, 14(4), 377–405.
Sahdra, B. K., MacLean, K. A., Ferrer, E., Shaver, P. R., Rosenberg, E. L., Jacobs, T. L., … Saron, C. D. (2011). Enhanced response inhibition during intensive meditation training predicts improvements in self-reported adaptive socioemotional functioning. Emotion, 11(2), 299–312.
Schoenberg, P. L. A., Hepark, S., Kan, C. C., Barendregt, H. P., Buitelaar, J. K., & Speckens, A. E. M. (2014). Effects of mindfulness-based cognitive therapy on neurophysiological correlates of performance monitoring in adult attention-deficit/hyperactivity disorder. Clinical Neurophysiology, 125(7), 1407–1416.
Sibinga, E. M. S., Webb, L., Ghazarian, S. R., & Ellen, J. M. (2016). School-based mindfulness instruction: a RCT. Pediatrics, 137(1), e20152532.
Siddaway, A. P., Wood, A. M., & Hedges, L. V. (2019). How to do a systematic review: a best practice guide for conducting and reporting narrative reviews, meta-analyses, and meta-syntheses. Annual Review of Psychology, 70(1), 747–770.
Simmons, J. P., Nelson, L. D., & Simonsohn, U. (2011). False-positive psychology: undisclosed flexibility in data collection and analysis allows presenting anything as significant. Psychological Science, 22(11), 1359–1366.
Sterne, J. A. C., Sutton, A. J., Ioannidis, J. P. A., Terrin, N., Jones, D. R., Lau, J., … Higgins, J. P. T. (2011). Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. British Medical Journal, 343(7818), 1–8.
Tang, Y. Y. (2017). The neuroscience of mindfulness meditation: how body and mind work together to change our behavior. London: Springer Nature.
Tang, Y. Y., Ma, Y., Wang, J., Fan, Y., Feng, S., Lu, Q., … Posner, M. I. (2007). Short-term meditation training improves attention and self-regulation. Proceedings of the National Academy of Sciences, 104(43), 17152–17156.
Tang, Y. Y., Hölzel, B. K., & Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nature Reviews Neuroscience., 16(4), 213.
Thomson, D. R., Besner, D., & Smilek, D. (2015). A resource-control account of sustained attention: evidence from mind-wandering and vigilance paradigms. Perspectives on Psychological Science, 10(1), 82–96.
Tsai, M.-H., & Chou, W.-L. (2016). Attentional orienting and executive control are affected by different types of meditation practice. Consciousness and Cognition, 46, 110–126.
Valls-Serrano, C., Caracuel, A., & Verdejo-Garcia, A. (2016). Goal management training and mindfulness meditation improve executive functions and transfer to ecological tasks of daily life in polysubstance users enrolled in therapeutic community treatment. Drug and Alcohol Dependence, 165, 9–14.
Van Dam, N. T., van Vugt, M. K., Vago, D. R., Schmalzl, L., Saron, C. D., Olendzki, A., et al. (2018). Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science, 13(1), 36–61.
Viechtbauer, W. (2010). Conducting meta-analysis in R. Journal of Statistical Software, 36(3).
Wampold, B. E., Mondin, G. W., Moody, M., Stich, F., Benson, K., & Ahn, H. (1997). A meta-analysis of outcome studies comparing bona fide psychotherapies: empirically, “all must have prizes”. Psychological Bulletin, 122(3), 203–215.
Wetherell, J. L., Hershey, T., Hickman, S., Tate, S. R., Dixon, D., Bower, E. S., & Lenze, A. E. J. (2017). Mindfulness-based stress reduction for older adults with stress disorders and neurocognitive difficulties: a randomized controlled trial. Journal of Clinical Psychiatry, 78(7), 736–743.
Will Crescioni, A., Ehrlinger, J., Alquist, J. L., Conlon, K. E., Baumeister, R. F., Schatschneider, C., & Dutton, G. R. (2011). High trait self-control predicts positive health behaviors and success in weight loss. Journal of Health Psychology, 16(5), 750–759.
Zeidan, F., Johnson, S. K., Diamond, B. J., David, Z., & Goolkasian, P. (2010). Mindfulness meditation improves cognition: evidence of brief mental training. Consciousness and Cognition, 19(2), 597–605.
Acknowledgments
We wish to thank the anonymous reviewers whose valuable comments helped improving earlier versions of this article. This research project was partly conducted during the first author’s master studies (MSc Neuroscience and Cognition, Utrecht University). The paper is part of the doctoral dissertation of the first author under the supervision of the last author.
Data Availability Statement
Data and scripts used for the conduction of the meta-analyses are publicly available at Open Science Framework (https://osf.io/pdtwv/).
Funding
LC was supported by a doctoral fellowship from “la Caixa” Foundation (ID 100010434). The fellowship code is LCF/BQ/ES18/11670002. MAV was supported by grants 2016-T1/SOC-1395 from Comunidad de Madrid (Programa de Atracción de Talento Investigador) and PSI2017-85159-P from the Spanish Agencia Estatal de Investigación, Ministerio de Economía y Competitividad. JL was supported by a research project grant PSI2017-84926-P from the Spanish Agencia Estatal de Investigación, Ministerio de Economía y Competitividad.
Author information
Authors and Affiliations
Contributions
LC: conceptualized and conducted the systematic review, conducted the meta-analysis and wrote the manuscript. VP: participated as second reviewer of the literature. MAV: conducted the meta-analysis and provided critical review and feedback during the writing of the previous versions of this manuscript. JL: assisted conceptualizing and conducting the systematic review and provided critical review and feedback during the writing of previous versions of this manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human Participants and Animal Studies
There was no research involving human participants and/or animals.
Informed Consent
There was no informed consent.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOC 63 kb)
Rights and permissions
About this article

Cite this article
Cásedas, L., Pirruccio, V., Vadillo, M.A. et al. Does Mindfulness Meditation Training Enhance Executive Control? A Systematic Review and Meta-Analysis of Randomized Controlled Trials in Adults. Mindfulness 11, 411–424 (2020). https://doi.org/10.1007/s12671-019-01279-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-019-01279-4