
Abstract
The majority of mindfulness intervention studies do not include active control groups. To examine potential unique effects of mindfulness practice and to study the mechanism responsible for beneficial mental health effects associated with mindfulness-based interventions, the present study compared mindfulness meditation with an active control group in a randomised controlled trial. A short-term mindfulness-based intervention (n = 46) was compared with both an active control group—relaxation training (n = 40)—and an inactive wait-list group (n = 40) on self-reported mindfulness and decentering, executive attention, psychological well-being, anxiety, depression, and coping style, in an adult working population with no prior meditation experience. Analyses of covariance showed that the mindfulness group scored higher than the wait-list group on self-reported mindfulness and psychological well-being. However, no differences were found on decentering, anxiety, depression, executive attention, or coping style. Moreover, the study failed to distinguish any unique mindfulness effects since there were no differences between mindfulness and relaxation on any of the variables. Simple mediation analyses, using a bootstrap approach, revealed that decentering acted as a mediator between self-reported mindfulness and psychological well-being. The length of the intervention, the similarities between body scan exercises in MBI and relaxation, and the absence of decentering effects may partly explain the lack of distinct MBI effects, suggesting that MBIs aimed at increasing well-being and problem-focused coping whilst reducing psychological symptoms in a working population should be longer than merely 4 weeks and include more than seven sessions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In Western literature, the original Buddhist term “mindfulness” is usually described as a certain alert, albeit, calm state of consciousness, most closely related to two major consciousness functions: awareness and attention (Brown and Ryan 2003; Brown et al. 2007). There are many different definitions of mindfulness and the majority of them emphasise attention to and awareness of present internal and external stimuli. A definition so commonly used in mindfulness research that it probably can be regarded as the preliminary mindfulness definition of consensus is Kabat-Zinn’s (1994, p. 4) “paying attention in a particular way: on purpose, in the present moment and non-judgementally”.
Mindfulness-based interventions (MBI) have, during the last decade, gained an increased popularity among a wide range of professionals in various fields (Cullen 2011). Treatment programmes, integrating mindfulness meditation techniques, such as mindfulness based stress reduction (MBSR) (Kabat-Zinn 2004), mindfulness based cognitive therapy (MBCT) (Segal et al. 2002), acceptance and commitment therapy (Hayes et al. 1999), and dialectical behavioural therapy (Linehan 1993) have been rapidly established in Western clinical and medical health care settings. Additionally, recent trends show an increasing interest in developing tailored MBI for limited populations, for instance mindfulness-based childbirth and parenting, mindfulness-based eating, mindful leadership, and so on (Cullen 2011).
Correlational studies frequently show that mindfulness meditation as well as self-reported mindfulness are positively related to mental health and well-being and inversely associated with psychological symptoms such as depression and anxiety (Baer et al. 2008; Cash and Whittigham 2010; Keng et al. 2011). Meta-analyses and reviews investigating the effects of MBIs similarly show overall improvements in mental health and psychological well-being (PWB), especially reductions in stress, anxiety, and depression, in clinical as well as in non-clinical populations (Carmody and Baer 2009; Chiesa and Serretti 2009; Fjorback et al. 2011; Grossman et al. 2004; Hofman et al. 2010; Keng et al. 2011). A meta-analysis by Hofman et al. (2010) showed a moderate effect size of improvements in anxiety and depressive symptoms in the overall sample whereas the effect size was large when a sample consisting of patients with anxiety and mood disorders was analysed.
Research on the effect of MBIs on mental health has mostly been carried out on clinical populations and populations with medical diagnoses (e.g. Ramel et al. 2004; Bohlmeijer et al. 2010; Williams et al. 2008). Far less empirical attention has been paid to the potential benefits for a healthy average population. A review by Chiesa and Serretti (2009) revealed that MBSR was effective in reducing stress in healthy subjects compared with inactive controls. In addition, studies published after the Chiesa and Serretti (2009) review showed that MBCT can reduce anxiety and depression in students compared with a wait-list control group (Kaviani et al. 2011), and a mental silence meditation (MSM) intervention significantly reduced stress and depressive symptoms in working adults compared with no-treatment controls (Manocha et al. 2011). Consequently, though not without controversy (Toneatto and Nguyen 2007), the vast majority of reviews and meta-analyses come to the conclusion that MBIs could be recommended for improving mental health and PWB in clinical as well as in non-clinical populations (Chiesa and Serretti 2009; Fjorback et al. 2011; Hofman et al. 2010).
Several researchers have highlighted the lack of active control groups in most of the trials, suggesting that the obtained effects are a result of non-specific unknown variables (Canter 2003; Chiesa and Serretti 2009; Fjorback et al. 2011; Toneatto and Nguyen 2007; Manocha et al. 2011). To be able to detect the unique effects of multi-model MBIs, it is necessary to use a research design with active controls (Canter 2003; Manocha et al. 2011; Toneatto and Nguyen 2007). Of the very few studies that have compared an MBI with an active control group, the initial results are less impressive. MBSR as an adjunct to treatment as usual (TAU) had no additional treatment effect compared with TAU alone in psoriasis patients (Kabat-Zinn et al. 1998). Similarly, no additional effect was found when MBSR combined with psychotherapy was compared with psychotherapy alone in an outpatient sample (Weiss et al. 2005).
It has specifically been stressed that MBI should be compared with relaxation training in order to separate mindfulness effects from mere relaxation or resting (Jain et al. 2007; Manocha et al. 2011), especially since relaxation training also has been associated with reductions in depressive symptoms, anxiety, and distress (Jorm et al. 2008; Manzoni et al. 2008; Murphy et al. 1995; Reynolds and Coats 1986; Stetter and Kupper 2002). In other words, can specific MBI effects be distinguished from simple relaxation effects? To our knowledge, only four studies comparing MBI and relaxation training have thus far been published, and the results have been mixed. Jain et al. (2007) found no significant differences between MBI and relaxation in stress, positive states of mind, and rumination in a student sample. Similarly, no group differences between MBI and progressive relaxation training were found on anxiety and mood states in a sample consisting of community adults (Semple 2010). On the other hand, Tang et al. (2007) showed that just a 1-week MBI significantly decreased stress, anxiety and depressive symptoms in students compared with a relaxation condition. As previously mentioned, Manocha et al. (2011) found that MSM significantly reduced occupational stress and depressive symptoms, but not anxiety, compared with relaxation, thus suggesting some unique effects associated with meditation. The authors hypothesised that “mental silence” (reductions of cognitive activity) may not only be a specific effect, but also a more efficacious ingredient in stress reduction than the relaxation aspect of meditation (Manocha et al. 2011). Investigating specific effects of mindfulness interventions may contribute considerably to the understanding of mindfulness mechanisms.
Mechanisms of Mindfulness
It is often hypothesised that mindfulness meditation enhances mindfulness, and increased mindfulness in turn is believed to have a beneficial effect on mental health and PWB (e.g. Chiesa and Serretti 2009; Josefsson et al. 2011). In other words, the somewhat apparent conclusion is that the mechanism in MBI simply is mindfulness. Whereas the outcomes of numerous MBIs in a wide range of populations have been frequently studied, the mechanism responsible for the mental health benefits associated with these interventions has barely been examined at all.
One regular MBI outcome is indeed increased scores in self-reported mindfulness compared with inactive controls (e.g. Nyklicek and Kuijpers 2008) and regular meditators usually score higher than non-meditators on self-reported mindfulness (e.g. Baer et al. 2008). Moreover, self-reported mindfulness has been shown to mediate the relation between meditation experience and PWB in cross-sectional studies (Baer et al. 2008; Josefsson et al. 2011). In an effort to address the question whether changes in self-reported mindfulness mediate the relation between mindfulness practice (MBSR) and beneficial health effects, Nyklicek and Kuijpers (2008) found that self-reported mindfulness acted as a significant mediator concerning improvements in stress and quality of life, thus giving some preliminary support for the mediating role of mindfulness.
It has also been suggested that the rather broadly (and perhaps vaguely) defined mindfulness construct per se is not the actual mechanism. Shapiro et al. (2006) have developed an ambitious theoretical model where mindfulness is seen as the simultaneous cyclic “moment-to-moment process” (Shapiro et al. 2006, p. 375) consisting of three fundamental components of mindfulness; intention (i.e. the motivational aspect of mindfulness practice), self-regulated attention and attitude (e.g. acceptance, openness, and curiosity). These three components taken together are theorised to lead to a meta-mechanism named reperceiving, which basically means a shift from a self-centred subjective perspective to an objective perspective. Reperceiving is more or less synonymous to the slightly more well-known term decentering, defined as “the ability to observe one’s thoughts and feelings as temporary, objective events in the mind, as opposed to reflections of the self that are necessarily true” (Fresco et al. 2007, p. 234). Reperceiving is in turn hypothesised to lead to four additional mechanisms (self-regulation, values clarification, cognitive, emotional and behavioural flexibility, and exposure) that are believed to be important contributors to the beneficial health effects of mindfulness interventions. In order to empirically examine the mindfulness mechanisms proposed by Shapiro et al. (2006), Carmody et al. (2009) studied the relation between changes in self-reported mindfulness, reperceiving, and the additional mechanisms in MBSR participants. In line with the predictions, significant increases in mindfulness, reperceiving, and the four potential mechanisms were found after the MBSR program, whilst psychological symptoms and stress were, as expected, significantly reduced. However, the study included neither an active nor a non-active control group, thus not controlling for potential placebo effects. Furthermore, mediation analyses did not, however, support a sequential model where increases in mindfulness lead to enhanced repercieving which in turn leads to improved abilities concerning the four additional mechanisms. Carmody et al. (2009) hypothesise that the lack of support is probably due to the fact that the measures used to assess mindfulness and reperceiving were highly correlated. For that reason, the authors conclude that mindfulness and reperceiving, as measured by the Five-Facet Mindfulness Questionnaire (FFMQ) and the Experience Questionnaire (EQ) (Fresco et al. 2007) respectively, are exceedingly overlapping constructs (Carmody et al. 2009).
Hence, it is still far from clear whether or not mindfulness and/or reperceiving actually are the active mechanisms explaining the health related benefits of MBIs. In addition, it needs to be clarified if reperceiving really is a separate construct, that is to say, if it is an effect of mindfulness or if it rather should be seen as a part of an overall mindfulness construct.
Mindfulness and Coping
Aside from the proposed mechanism reperceiving and its additional mechanisms (Shapiro et al. 2006), it has also been suggested that the improved health effects of MBI, stress reduction in particular, may be a question of the facilitation of more adaptive coping strategies (Weinstein et al. 2009). Coping is generally defined as “constantly changing cognitive and behavioural efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person” (Lazarus and Folkman 1984, p. 141). Three general types of coping have been identified: problem-focused coping, which is a problem-solving approach aimed at eliminating or altering the source of stress, emotion-focused coping is aimed at reducing distressing emotions associated with a stressful encounter, and avoidant coping—a less adaptive coping style—is associated with denial and disengagement (Carver et al. 1989; Weinstein et al. 2009).
Weinstein et al. (2009) hypothesise that a mindful processing of internal current events may promote more adaptive coping strategies (i.e. actively trying to deal with the problem). This is consistent with the function of reperceiving; instead of being mentally and emotionally caught up in the experience, one can, through the state of mindfulness, shift perspective and relate objectively to the event itself as well as to one’s own cognitive and emotional reactions associated with experiencing the event, potentially leading to more adaptive health-related behaviours as well as improved cognitive flexibility (Shapiro et al. 2006).
To date, the relation between mindfulness and coping has gained very little empirical attention. A pilot study on the effects of MBSR on a high-stress working population revealed that positive coping strategies, but not negative coping strategies, were significantly increased at the post-test (Walach et al. 2007). Furthermore, Weinstein et al. (2009) showed in a series of four studies on student samples (1) that less use of avoidant coping was predicted by trait mindfulness in response to a social threat task, (2) that over a 1-month period, trait mindfulness predicted more use of approach coping and less use of avoidant coping, (3) that on a daily level, trait mindfulness was also associated with less avoidant coping and more approach coping, and (4) that in a real-life stress situation over time, initial trait mindfulness predicted less use of avoidant coping. In contrast, Sears and Kraus (2009) found no significant pre- to post-test changes in approach coping and avoidant coping in a mindfulness meditation group compared with controls.
Hence, results so far point towards a relation where trait mindfulness is positively associated with approach coping and negatively associated with avoidant coping. However, Weinstein et al. (2009) used only the unidimensional Mindful Attention Awareness Scale (MAAS) (Brown and Ryan 2003) to assess trait mindfulness, and the authors recommend future studies to more closely explore how other facets of mindfulness (as measured by the five-dimensional FFMQ) relate to coping styles. Additionally, because of the mixed results concerning the effect of MBI on coping styles, further examination is required.
Mindfulness and Attention
Attention is widely regarded as an essential feature in the mindfulness construct (Bishop et al. 2004; Brown and Ryan 2003; Shapiro et al. 2006). In two proposed theoretical models, self-regulated attention is seen as the core component of mindfulness, including three subcomponents: sustained attention, switching attention, and inhibition of secondary elaborative processing of operations and sensations that arise in the ongoing stream of consciousness (the last subcomponent reflecting an executive attention capacity) (Bishop et al. 2004; Shapiro et al. 2006). Mindfulness meditation is often described as a practice in attentional control, both in Western and Buddhist writings (e.g. Claxton 1987; Thera 1996; Thera 1972). Despite the fact that it is repeatedly claimed that mindfulness training improves self-regulated attention (e.g. Bishop et al. 2004; Shapiro et al. 2006), relatively few studies have in fact investigated the effect of MBIs on objective measures of attentional control. A review by Chiesa et al. (2011) revealed some preliminary evidence for the positive effect of mindfulness meditation on sustained attention. However, the results were far less convincing when executive attention was investigated. Of the nine trials included in the review, only two showed superior performance on executive attention tasks for meditators. Similarly, a study not included in Chiesa et al. (2011) showed no significant differences on the executive attention task; the Stroop Task, between long-term mindfulness meditators and non-meditators (Lykins, Baer and Gottlob 2012). However, it should be noted that study designs, populations, methodological quality, as well as attention measures vary to a great extent among these trials, making it difficult to draw any firm conclusions. For instance, two studies that compared the effect of MBI versus relaxation training on executive attention tasks found different results. Tang et al. (2007) showed that a 1-week MBI, with only five 20-min sessions, significantly improved executive attention on the Attention Network Test (Fan et al. 2002). Semple (2010), on the other hand, found no such differences—neither between mindfulness and relaxation nor between mindfulness and control—on the Stroop Task after a 4-week MBI, (containing two individual mindfulness training sessions, and the participants were also instructed to practice at home twice a day for 20 min).
Although definitions and theoretical models persistently regard self-regulated attention as the essence of the mindfulness construct as well as the main exercise in mindfulness meditation, the evidence so far show little support for any improved performance on executive attention tasks due to MBIs. Furthermore, self-reported mindfulness and performance on an executive attention task—the Stroop Task—were not significantly related at all in Schmertz (2006), and only one mindfulness facet, as measured by the FFMQ (Baer et al. 2006), was related (in the expected direction) to Stroop interference in Josefsson and Broberg (2011).
Hence, the potential effect of mindfulness training on attention regulation, especially executive attention, remains unclear and calls for further research. In the development of theoretical models and operationalisable definitions, it is of major importance to establish the role attention plays in the mindfulness construct.
The Relation Between the Length of the MBI Program and Outcomes
The standard form of the 8-week MBSR programme contains 26 h of class time. The programme also includes a 1-day class of 6 h, thus 32 class hours in all (Carmody and Baer 2009). In addition, the participants are instructed to practice at home for 45 min/day (Carmody and Baer 2008). However, it has been reported that the considerable time commitment required by the MBSR participants is a major reason for declining participation (Carmody and Baer 2009). This has lead some researchers to address the question of how long a mindfulness-based program has to be for positive mental health effects to occur (Carmody and Baer 2009). There is some preliminary evidence that even a short form of MBI could be beneficial, at least for stress and trait mindfulness. Klatt et al. (2009) examined the effects of a low-dose 6-week MBSR—consisting of a 1-h session/week and 20 min home practice on the remaining working days—in a full-time working population. The results showed significant pre- to post-test improvements in self-reported mindfulness (the MAAS) and reductions in stress for the MBSR group but not for the control group. Furthermore, the recently published review by Keng et al. (2011) revealed that several laboratory studies showed that just a single brief mindfulness-induced session can result in immediate positive effects on emotion regulation and anxiety (e.g. Erisman and Roemer 2010; Feldner et al. 2003).
If a short form of MBI can also produce positive health effects, this may be a more realistic and attractive alternative for certain populations who already have a fully occupied and strained schedule, for instance full-time working parents. Clearly, future studies investigating the effects of short MBIs are necessary.
Current Study
Although mindfulness research has advanced significantly during the last decade, several crucial areas still demand further empirical examination. For instance, investigating the unique effects of MBIs, which has almost been neglected in previous research, ought to be highly prioritised. There is also a need to develop and evaluate short-term MBIs in clinical as well as in non-clinical populations. Furthermore, theoretically, attention is widely regarded as the core mindfulness component but studies so far only partly support this notion. Finally, a numerous number of studies provide evidence for the positive health effects gained by MBIs, but proposed mechanisms (i.e. reperceiving/decentering and improved adaptive coping styles) responsible for these beneficial effects have rarely been explored.
Hence, the general aim of the present study was to contribute to the understanding of the mindfulness construct as well as its mechanisms. By employing a randomised controlled trial, the effects of a short MBI was investigated on a battery of tests—executive attention, self-reported mindfulness, decentering, PWB, anxiety, depression, and coping styles—in a working population. Mindfulness meditation was compared with both an active control group (relaxation training) as well as an inactive wait-list group.
A secondary aim was to examine changes in mindfulness in relation to changes in decentering, PWB, executive attention, anxiety, depression, and coping style. In addition, our aim was also to examine whether the proposed decentering mechanism mediates the assumed relation between trait mindfulness and psychological health (PWB, anxiety, and depression).
Based on theory and previous results, it was hypothesised that (1) the mindfulness group would increase significantly in mindfulness and decentering from pre-to post-test compared with the other two groups and (2) that both the mindfulness group and the relaxation group would show significantly greater improvements than the wait-list group in depression, anxiety, and PWB. Considering the previously described mixed results on attention and coping styles in relation to mindfulness, we decided to study these potential intervention effects in an exploratory fashion, without making any specific predictions. Furthermore, in the mindfulness group, we hypothesised that (3) mindfulness changes would correlate positively with decentering change, and that both mindfulness changes as well as decentering change would be positively related to PWB change. We also expected (4) mindfulness changes as well as decentering change in the mindfulness group to be negatively related to anxiety and depression changes. Furthermore, we predicted that (5) decentering would act as a mediator between mindfulness and all three psychological health outcome variables: PWB, anxiety, and depression.
Method
Participants
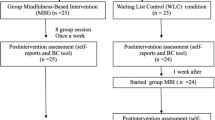
Ninety-eight employees with no prior meditation experience were voluntarily recruited from several local workplaces in Halmstad municipality, county of Halland. Initially, it was planned that the sample would be randomised in three groups (one experiment group, one active control group, and one non-active control group) but despite a great interest at the outset, the number of individuals who finally volunteered were fewer than expected, and the concern for potential drop-outs during the intervention made us decide to randomise the participants in only two groups: a mindfulness meditation group and a relaxation training group. After the randomisation was done (May 2009), and before the pre-test (September 2009), three people in the mindfulness group and nine in the relaxation group dropped out (the most common reason given for dropping out was changes in working schedules) which consequently resulted in a total sample of 86 participants: the mindfulness meditation group (6 men and 40 women, mean age = 48.9 years (SD = 10.2)), and the relaxation training group (2 men and 38 women, mean age = 50.4 years (SD = 10.4)).
In addition, a new recruitment campaign was made a year and a half later from the same workplaces and organisations, resulting in 47 new volunteers. However, seven volunteers later announced that they would be indisposed for the pre-test for various reasons (e.g. sickness) and thus dropped out. Hence, 40 participants subsequently constituted a wait-list group (3 men and 37 women, mean age = 45.1 years (SD = 8.9)). This group was offered to participate in a mindfulness course for beginners (five sessions, 1 h/session, and one session/week) after the post-test had been completed. In all, 126 (employees) individuals participated in the present study.
The mindfulness meditation group and the relaxation training group were divided in four different class groups, thus each class consisted of approximately 20 participants.
Drop-out rates—22 participants were lost to the post-test assessment: eight participants in the mindfulness group (n = 38), five in the relaxation group (n = 35), and nine in the control group (n = 31). Thus, 104 participants completed both the pre- and the post-test.
Means and standard deviations for attendance rates (seven sessions between pre-and post-test) were 6.45 (0.6) for the mindfulness group and 6.23 (0.8) for the relaxation group.
Materials
Education (highest level of education) was assessed in terms of five response alternatives: 9-year compulsory school, upper secondary school, community college, specialist training, and university education (see Table 1).
Josefsson and Broberg (2011) recommended that computer skills should be assessed when computerised attention tests are used. Consequently, computer skills were measured by computer usage and computer game habit on a 7-point Likert type scale (never—several times/day), and with an open question on hours of computer usage/week.
Prior experience in meditation-related practices such as yoga, Tai-chi, and Qi-gong was assessed on a nominal scale (Yes–No), and an open follow-up question where the participants were asked to specify type of practice (see Table 1).
Measures
The Stroop Task (Stroop 1935) is a widely used measure of executive attentional capacity. The test requires that participants ignore their habitual process of word reading and instead concentrate on the colour the word is printed in. The Stroop effect means that the response time for incongruent colour-words (e.g. the word red printed in blue) is slower and less accurate than for congruent colour words (e.g. the word red printed in red) as well as for a neutral control condition (e.g. XXX printed in red). This effect is usually referred to as Stroop interference (MacLeod 2005). Low interference scores could thus be interpreted as reflecting a high level of executive attention.
A computerised version of the The Stroop Task (SuperLabpro, version 4.0) was used. In short, participants were presented oral as well as written instructions to press the key in the same colour as the colour words and letters (XXX) shown at the centre of the screen. Four colours were used: green, yellow, blue, and red. Participants were instructed to respond as quickly and as accurately as possible. The letters were in bold print, 150 mm, Arial Baltic. The first round consisted of a practice trial showing 22 colour words and letters in different colours. The stimuli remained on the screen until responses were made. The actual test consisted of 82 quasi-randomised stimuli including ten XXXs, 36 congruent colour words, and 36 incongruent colour words.
Stroop interference (incongruent–neutral) was calculated by subtracting the average reaction time (RT; in milliseconds) for the incongruent condition from the average RT for the neutral condition. Stroop interference (incongruent–congruent) was calculated by subtracting the average RT for the incongruent condition from the average RT for the congruent condition.
Stroop errors are the errors made in the incongruent condition only. Stroop RT is the average RT for correct responses in the incongruent condition.
The Stroop Task was administered via eight Dell computers (Dell Optiflex GX620) with a 17-in. screen.
The Five-Facet Mindfulness Questionnaire
To measure self-reported mindfulness, the Swedish short-form 29-item version of the FFMQ was used (Lilja et al. 2011). The Swedish FFMQ has shown good psychometric properties, similar to the ones found in the original version (Baer et al. 2006). Cronbach’s alpha for the Swedish FFMQ subscales ranged from 0.75 to 0.85 (Lilja et al. 2011). The FFMQ is designed to measure five distinct mindfulness skills in daily life (non-reactivity to inner experience, observing, acting with awareness, describing, and non-judging of experience) using a 1–5 Likert scale ranging from never or very rarely true to very often or always true. High scores indicate a high level of mindfulness.
Psychological Well-being
A Swedish version (Lindfors 2002; Lindfors et al. 2006) of the short form of Ryff’s PWB scale (Ryff 1989; Ryff 1995) was used in this study. This short version of PWB consists of 18 items with a 1–6 Likert scale (completely disagree–completely agree), where higher scores indicate higher levels of PWB. The items cover six dimensions of PWB (with three items each): self-acceptance, positive relations with others, autonomy, environmental mastery, purpose in, and personal growth. The present study used only the total PWB scale. Cronbach’s alpha for the Swedish short version of the PWB total scale was 0.77 in Josefsson et al. (2011).
The COPE Inventory
The widely used COPE inventory was developed by Carver et al. (1989). The instrument measures 14 different coping strategies on a 1–4 scale (I did not do this at all–I did this a lot) and consists of 13 scales and one single-item question. Five scales assess problem-focused coping (active coping, planning, suppression of competing activities, restraint coping, and seeking social support for instrumental reasons). Five other scales measure emotion-focused coping (seeking social support for emotional reasons, positive reinterpretation and growth, acceptance, turning to religion, focus on and venting of emotions). The remaining three scales and the single item question measure avoidant coping, reflecting less adaptive coping strategies (denial, behavioural disengagement, mental disengagement, and alcohol–drug disengagement).
The Swedish version has shown similar psychometric properties as the original scale; Cronbach’s alpha ranged from 0.60 to 0.95 (Muhonen and Torkelson 2001).
The Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HAD) (Zigmond and Snaith 1983) was primarily designed to assess anxiety and depression in non-psychiatric medical patients. The measure consists of the two subscales: anxiety (HAD-A) and depression (HAD-D). The subscales contain seven items each on a 0–3 scale. A total sum score is calculated for anxiety and depression respectively, ranging from 0 to 21. Each subscale has three cut-off points. Anxiety: 0–6 = no anxiety problems, 7–10 = mild to moderate anxiety, and >10 = potential anxiety disorder. Depression: 0–6 = no depression, 7–10 = depressed mood/gloominess, and >10 = potential risk for depression that may require professional treatment. The psychometric properties of the HAD is generally considered to be good and the scale is widely used for detecting depression and anxiety disorders in psychiatric as well as in general populations (Bjelland et al. 2002; Herrmann 1997).
The Experience Questionnaire
The decentering subscale of the EQ (Fresco et al. 2007) was used to assess decentering. The scale consists of 12 items on a five-point Likert scale (never–always). Higher scores indicate higher levels of decentering. Item examples: “I can separate myself from my thoughts and feelings”, and “I have the sense that I am fully aware of what is going on around me and inside me”. The recently developed EQ has shown preliminary good validity and reliability with an internal consistency of 0.83 (Fresco et al. 2007). The Swedish translation of the original decentering scale was made by one of the authors of the present study. Three independent translators, blind to the original measure, performed back translations which resulted in only minor changes on a few items. In the present study, the internal consistency of the Swedish version was similar to the original scale: 0.82 for the pre-test and 0.87 for the post-test.
Procedure
E-mails were sent to the personnel manager of several working organisations in Halmstad (Halmstad municipality, County of Halland, Region Halland, Halmstad Insurance Company, and Lokaldelen i Sverige AB) asking if they had a preliminary interest in letting their staff participate in the present study. Thereafter, an information letter introducing the study was sent to the staff by the personnel manager of each organisation respectively who then forwarded the information letter to the staff. In addition, an advertisement of the study was also placed on the Region Halland website. In the information letter, the purpose of the study was presented, inclusion criteria (e.g. no prior meditation experience) and a careful description of the content and procedure of the data collections. Employees interested in participating in the present study were encouraged to contact one of the authors by e-mail or phone. Thereafter, all individuals who expressed interest in participating were invited to a brief presentation of the study, held at Halmstad University. At the presentation, written informed consent forms were collected. A restricted randomisation procedure was employed, using a shuffled approach to the random allocation rule (Schultz and Grimes 2002).
As previously mentioned, a second recruitment was made one and a half year after the first one. The same working organisations were addressed and the procedure was similar to the first recruitment, but there was no invitation to the University for a presentation of the study. Thus, all information was sent by e-mail to the volunteers. Informed consent was completed prior to the first data collection.
The Stroop Task was administered at the Behavioural and Cognitive Laboratory at Halmstad University. Instructions for the Stroop Task were given orally as well as written (on the computer screen). The self-report scales were administered on the same occasion in a classroom at Halmstad University. It took the participants approximately 30 min to complete the questionnaire and 5 min to perform the attention test.
Previous researchers (Josefsson and Broberg 2011; Rani and Rao 2000) suggest that attention regulation may be temporarily improved right after meditation. Therefore, it was decided that the pre-tests would be administered prior to the first intervention session, and similarly, the post-tests were also administered right before the last (the eighth) intervention session. Thus, the post-test was administered approximately 4 weeks after the pre-test.
All participants were given written and oral information about the study and were informed that the data were confidential, as well as their right to quit the study at any time. Participants did not receive any compensation for taking part in the study.
Mindfulness Meditation Condition
The MBI in the present study was not a manualised programme, and it is therefore not comparable to standardised MBIs such as MBSR (see Kabat-Zinn 2004) and MBCT (see Segal et al. 2002). The MBI in the present study consisted mainly of standard sitting mindfulness practices; attention to the breath, awareness of and attention to internal objects (e.g. thoughts, images, and emotions), bodily sensations (e.g. body scan exercises where attention is paid on each body part), sensory perceptions (e.g. taste and smell), and external objects (e.g. sounds and sights). The subjects were taught to notice all these inner and outer objects with a so called non-judgemental awareness and a general attitude of acceptance, thus not deliberately trying to affect or change whatever it is that arises in the field of consciousness. The major difference in content between this MBI and the MBSR programme is that the MBI used in this study did not include any yoga exercises. The mindfulness instructor was a psychologist, specialised in integrating mindfulness exercises in clinical settings. The instructor had also been teaching mindfulness meditation for (non-clinical) beginners as well as for advanced practitioners for 10 years.
Relaxation Training Condition
A relaxation training programme based on the holistic psychohygiene concept originally developed by Lindemann (1986), and introduced in Sweden by Ryberg (1986), was used. The programme aims at increasing body awareness and includes relaxation of major muscle groups and body parts, one by one, finally covering the whole body.
The relaxation training instructor has an experience of over 25 years in teaching relaxation training for various groups (e.g. elite athletes and health care staff).
The duration of both interventions was 4 weeks, consisting of two 45-min sessions/week. Since the eight and last session took place after the data collection, the total number of intervention sessions between the pre- and post-test was seven.
Classes for the mindfulness meditation groups and the relaxation training groups were held in an aerobic/dance-class room in the gym at Halmstad University.
Analyses
Initially, one-way ANOVAs were performed to examine if demographic characteristics and background variables differed between the groups.
One-way analyses of covariance (ANCOVAs), controlling for the pre-test and education, were conducted to explore post-test differences between the three conditions on the Stroop variables, the FFMQ scales, decentering, the PWB total scale, the HAD scales, and the cope scales (problem-focused coping, emotion-focused coping, and avoidant coping).
The Bonferroni test was employed in all post-hoc analyses. Pearson’s r was used to examine pre- and post-test relations between FFMQ scales and decentering.
Change score variables were computed for all above mentioned scales. Pearson’s r was used to study relations in changes from pre- to post-test (in the total sample as well as separate analyses for the three conditions) between FFMQ change scales and decentering change as well as these scales’ relations with coping style changes, HAD changes, PWB total change scale, and Stroop changes.
Mediation analyses were performed in accordance with the recommendations in Preacher and Hayes (2004). The SPSS macro-script (Preacher and Hayes 2008) was used for all analyses. A bootstrapping procedure was used to test indirect effects (bootstrapped sample, 5,000). Since the ANCOVAs showed no significant post-test group differences on anxiety and depression, we only tested if decentering mediated the relation between mindfulness (FFMQ total) (IV) and PWB (DV). Furthermore, results from the correlational analyses showed that decentering and the theoretically similar mindfulness facet non-react were strongly related to one another, indicating a substantial overlapping between the constructs. Therefore, we computed a total FFMQ variable where Non-React was excluded. Thus, the FFMQ total scale used in the mediation analyses consisted of the remaining four facets: describe, non-judge, observe, and act aware. Cronbach’s alpha for the revised FFMQ total scale was 0.86. Four simple mediation analyses were performed for each dependent variable, respectively. First, a cross-sectional model was tested on the total sample including pre-test scores on mindfulness (IV), decentering (M), and PWB (DV). The following three models were tested using a sample consisting of the two active intervention groups (mindfulness and relaxation). The second model consisted of pre-test mindfulness, post-test decentering, and post-test PWB. The third model included pre-test mindfulness, decentering pre–post change, and post-test PWB. The fourth model included only pre–post change scores: mindfulness change, decentering change, and PWB change.
Results
Outliers on the Stroop error variable (incongruent condition) were detected and removed from the analyses. Consequently, we had to exclude not only the Stroop error variable on these outliers but also Stroop RT as well as the two Stroop interference variables. At the pre-test, 21 outliers were removed from the mindfulness group, 12 from the relaxation group, and two from the wait-list group. At the post-test seven outliers were removed from the mindfulness group, four from the relaxation group, and one from the wait-list group.
Demographic Characteristics and Group Differences
There were no significant baseline differences between the mindfulness group, the relaxation group and the control group in the following variables: age, gender, prior experience of meditation-related practice, computer usage, and computer game habit. However, the results showed a significant effect of education (F(2, 122) = 8.87, p < 0.01, η 2 = 0.13). The post hoc test showed that the relaxation group demonstrated significantly lower education compared with the mindfulness group (p < 0.05) as well as the control group (p < 0.001), probably due to the fact that fewer participants in the relaxation group, compared with the other two conditions, had a university education (see Table 1). With regard to prior experience of meditation related practice the far most commonly mentioned practice was yoga. Tai-chi and Qi-gong were also frequently reported.
Pre-Test Scores on Anxiety and Depression
The HAD cut-off points showed that around a third to a quarter of the participants’ individual scores indicated a potential anxiety disorder whereas a third of the participants scored on the mild to moderate anxiety level. About 40 % of the participants scored on the level indicating no anxiety problems (see Table 2).
The vast majority of all three groups (80 % and above) scored on the level indicating no signs of depression. The rest of the participants’ scores (except one participant in the mindfulness group) indicated depressed mood/gloominess (see Table 2).
Comparisons Between Mindfulness, Relaxation, and Wait-list on Post-tests
ANCOVAs, controlling for the pre-test and education, showed significant effects on two FFMQ scales: describe and the FFMQ total scale. The post hoc analysis revealed that the mindfulness group (p < 0.01) as well as the relaxation group (p < 0.001) rated themselves significantly higher than the wait-list group on describe. Furthermore, the mindfulness group scored significantly higher than the wait-list group on the FFMQ total scale (p < 0.01). Additionally, a trend was found indicating a significant effect on observe (see Table 4). The post hoc test also revealed a trend for observe where the mindfulness group scored higher than the wait-list group (p = 0.053). Thus, no significant effects were found on non-react, act aware, and non-judge. Furthermore, a significant effect was found on the PWB total scale. The post hoc test indicated that the mindfulness group scored higher than the wait-list group (p < 0.01). Furthermore, no significant group differences were found on any Cope style scales, Stroop variables, HAD scales, or decentering (see Table 3).
Correlations Between Mindfulness and Decentering
Analysing the total sample, at the pre-test, decentering was positively correlated with the FFMQ total scale (r (104) = 0.72, p < 0.001) as well as all mindfulness facets, ranging from r = 0.35 (observe) to r = 0.72 (non-react). Similarly, at the post-test, decentering was positively correlated with the FFMQ total scale (r (104) = 0.81, p < 0.001) and all mindfulness facets, ranging from r = 0.44 (non-judge) to r = 0.72 (non-react).
Correlations Between Change Scores
The Mindfulness Group
Decentering change showed significant positive relations with two FFMQ change variables: non-react (r (38) = 0.53, p < 0.01), observe change (r (38) = 0.32, p = 0.05), and FFMQ total scale (r (38) = 0.50, p < 0.01) (see Table 4). Furthermore, decentering change was also positively related to PWB change (r (38) = 0.42, p < 0.01). Decentering change showed a significant and negative relation with both anxiety change (r (38) = −0.36, p < 0.05) and depression change (r (38) = −0.32, p = 0.05). Decentering change was not significantly related to coping style changes or Stroop changes.
The intercorrelation between FFMQ change facets showed only two significant associations: observe change was positively related to describe change (r (38) = 0.37, p < 0.05), and act aware change was positively related to non-judge change (r (38) = 0.38, p < 0.05). Furthermore, two FFMQ change scales were significantly and positively associated with PWB change: FFMQ total scale (r (38) = 0.56, p < 0.001) and act aware (r (38) = 0.44, p < 0.01). The following FFMQ change scales were negatively associated with anxiety change: act aware (r (38) = −0.36, p < 0.05), describe (r (38) = −0.32, p < 0.05), non-judge (r (38) = −0.32, p < 0.05), and FFMQ total scale (r (38) = 0.46, p < 0.01). The only FFMQ change scale that was significantly (and negatively) related to depression change was act aware (r (38) = −0.32, p = 0.05). Two FFMQ change scales were significantly related to coping style changes: FFMQ total scale (r (38) = 0.35, p < 0.05) as well as non-judge (r (38) = 0.35, p < 0.05) were positively related to emotion-focused coping. There were no significant relations between FFMQ changes and Stroop changes.
The Relaxation Group
Decentering change was significantly and positively related to three FFMQ change variables: non-react (r (35) = 0.38, p < 0.05), act aware (r (35) = 0.46, p < 0.01), and FFMQ total scale (r (35) = 0.41, p < 0.05). Furthermore, decentering change was negatively related to anxiety change (r (35) = −0.48, p < 0.05) but not to depression change. Decentering change was not significantly related to either PWB change, coping style changes, or Stroop changes.
Two FFMQ change variables were significantly and positively associated with PWB change: act aware (r (35) = 0.54, p < 0.01) and FFMQ total scale (r (35) = 0.34, p < 0.05). Only one FFMQ change scale, act aware, was significantly and negatively related to anxiety change (r (35) = −0.42, p < 0.05). One FFMQ change scale, FFMQ total change scale, was significantly related with depression change (r (35) = −0.34, p < 0.05). Furthermore, the only significant association between FFMQ changes and coping style changes was the negative relation between observe and problem-focused coping (r (35) = −0.38, p < 0.05). FFMQ change scales were not significantly related to Stroop changes.
The Wait-List Group
Decentering change was not significantly related to FFMQ changes, PWB change, HAD changes, coping style changes, or Stroop changes.
Of the FFMQ change scales, only describe change was significantly and negatively related to depression change (r (31) = −0.55, p < 0.01). No significant associations were found between FFMQ change and anxiety change. One FFMQ change variable was significantly associated with coping style change: non-judge was negatively related to avoidant coping (r (31) = −0.36, p < 0.05). FFMQ changes were not related to PWB change or Stroop changes.
Simple Mediation Analyses
Psychological Well-being
The overall results from the simple mediation analyses (see Table 5) showed that decentering, in three (of the four) models that were tested significantly mediated the relation between mindfulness and PWB. Moreover, all direct effects of mindfulness on decentering were significant and positive except in one model (PWB 3) where the effect was non-significant. The direct effect of mindfulness on PWB was significant and positive in all four models. The total effect of mindfulness (when decentering was controlled for) was significant and positive in three models (PWB 1, PWB 3, and PWB 4), and non-significant in PWB 2. The total effect of decentering on PWB (when mindfulness was controlled for) was significant and positive in two models (PWB 1 and PWB 2), and non-significant in the remaining two models. The bootstrap analyses revealed that decentering significantly mediated the effect of mindfulness on PWB in three models (PWB 1, PWB 2, and PWB 4).
Discussion
The purpose of the present study was to investigate the effects of a short-term MBI, compared with relaxation training and a wait-list group, on a number of tests: executive attention, mindfulness facets, decentering, PWB, anxiety, depression, and coping style.
The first hypothesis was partly confirmed. The mindfulness group scored significantly higher on the post-test than the wait-list group on the FFMQ total scale and describe, and nearly significantly higher on observe. On the other hand, there were no differences at all in FFMQ scales between the mindfulness group and the relaxation group. Unexpectedly, the relaxation group also rated themselves significantly higher than the wait-list group on describe. In contrast to our predictions, no group differences were found on decentering.
Although we expected the mindfulness group to score higher than the wait-list group on more mindfulness facets, these results are still consistent with earlier studies (e.g. Nyklicek and Kuijpers 2008), and seem to indicate that even a short-term mindfulness program can produce increases in overall trait mindfulness, suggesting that mindfulness skills in daily life—especially describe and observe—are rather quickly improved. However, we did not find any evidence for any unique MBI effects on trait mindfulness and decentering that are distinct from relaxation. We can think of three potential reasons for this absence of unique effects. First, the length of the intervention may have been too short and the number of sessions too few for mindfulness skills to be sufficiently developed and manifested. Thus, a longer intervention may show further advances in mindfulness skills which in turn may facilitate the decentered perspective, characterised by its unidentification of self-centred thoughts and feelings.
Second, mindfulness training and relaxation training include similar exercises, for instance, the body scan exercise in Western mindfulness practice is similar to standard relaxation training. Both of these exercises involve paying attention to sensations in each body part until the whole body is covered and then feeling the body as a whole. This means that a mindful awareness of the body may be a side effect of relaxation training. Likewise, relaxation ought to be a side effect of body scan exercises in mindfulness practice. Although relaxation may produce increases in mindfulness and decentering, one should bear in mind that the relaxation group only scored higher on one facet (describe), compared with the wait-list group. Moreover, similar body exercises in mindfulness and relaxation may not fully explain why the relaxation group also improved their describing skills compared with the wait-list group. Thus, relaxation training appears to be associated with a better capacity to verbalise thoughts, opinions and feelings. The relation between relaxation and improved verbalising capacity could be an interesting topic for future research.
Third, in line with the above reasoning, the lack of decentering effects may also be a question of what type of meditation exercises that are actually practiced in MBIs. Mikulas (2011) makes a convincing case arguing that Western conceptualisations of mindfulness as well as certain mindfulness exercises are more related to concentration-based meditation than mindfulness meditation. In Buddhist meditation, concentration (Samatha) is mainly a practice of attention-regulation whereas mindfulness meditation (Vipassanna) is more of an insight-oriented practice. However, Western as well as Buddhist mindfulness meditation practices usually contain a combination of the two meditation traditions (Grabovac et al. 2011). Nevertheless, this distinction proposes that common standard MBI exercises such as focused attention to the breath, attention to sensory processes and perceptions (sounds, sights, smell, and taste) as well as body-oriented exercises such as the aforementioned body scan and yoga, could be seen as training in concentration. Moreover, concentration is a skill that is especially important to develop for beginners, because improved concentration capacity calms the mind and helps the practitioner to establish a focused attention on the meditation object, i.e. the breath. Therefore, concentration exercises are often integrated early in mindfulness meditation practice (Goldstein and Kornfield 2001; Grabovac et al. 2011; Mikulas 2011). As a result, a short MBI may be more concentration-based than the regular 8-week MBI. A plausible hypothesis is that insight-oriented exercises (e.g. awareness of mental and emotional processes) activate the decentering mechanism to a greater extent than concentration-related meditation. Hence, if we assume that it is insight-oriented practice (mindfulness) that principally leads to enhanced decentering, then the lack of decentering effects may be due to the fact that the meditation exercises in this short-term MBI are more concentration based than insight based.
Similarly, the second hypothesis was also only partly confirmed. As expected, the mindfulness group scored significantly higher than the wait-list group on the PWB total scale. On the other hand, the relaxation group did not differ from the wait-list group on PWB. Inconsistent with our hypothesis and in contrast to previous studies indicating reductions in anxiety and depression in non-clinical populations (e.g. Kaviani et al. 2011; Manocha et al. 2011); no significant group differences were found in either depression or anxiety. However, previous research also indicates that the MBI effect on anxiety and depression symptoms is larger in clinical populations (e.g. Hofman et al. 2010). Overall, the results from this study suggest that a 4-week mindfulness intervention improves PWB but the length of this intervention appears to be too short for significant reductions in anxiety and depression symptoms to occur. Thus, PWB seems to develop more quickly and before symptom reductions in anxiety and depression take place. Furthermore, if decentering is the actual mindfulness mechanism responsible for beneficial mental health effects, then the absence of decentering effects may be the main reason why the mindfulness group did not significantly reduce anxiety and depression symptoms compared with the other two groups.
Another possibility is that decentering is not the main mechanism responsible for reductions in psychological symptoms. Recently, a new theoretical mindfulness model—a Buddhist Psychological Model (BPM)—was introduced, proposing that the major mechanism for psychological symptom reduction and increased well-being is decreased mental proliferation (Grabovac et al. 2011). Mental proliferation is described as the “habitual reactions of attachment and aversion to the pleasant, unpleasant, and neutral feelings of prior sense impressions and mental events” (Grabovac et al. 2011, p. 157). Strong reactions may result in increased mental proliferation which in turn may lead to rumination. Furthermore, the theory states that fundamental insights about three characterististics lead to reductions in attachment and aversion to mental and emotional contents, which in turn result in decreased mental proliferation. The three characteristsics are: (1) the impermanence of mental events and sense impressions, (2) attachment and aversion to mental events and sense impression lead to suffering, and (3) the self is not constituted by mental events and sense impressions: “not-self”. In addition, three aspects of meditation practice (acceptance, concentration/attention regulation, and ethical practices) also contribute to the attainment of reduced mental proliferation. According to this theory, decentering is only related to two components in the BPM: acceptance and concentration/attention regulation (Grabovac et al. 2011). Although decentering may influence the reduction of mental proliferation by its association with acceptance and concentration, and thereby improving psychological symptoms, this theory suggests that merely decentering may not be enough to significantly reduce anxiety and depression symptoms.
Similar to the majority of studies investigating the relation between mindfulness meditation and executive attention (e.g. Lykins et al. 2012; Semple 2010), our exploratory analyses revealed no group effects at all, suggesting that executive attention capacity is not improved by short-term mindfulness training in an average population. The lack of attention effects may be influenced by the fact that several exercises in MBIs are less a practice of executive attention; it is rather a training of focusing attention on one particular object whilst ignoring other sensations. If unwanted sensory objects interfere (i.e. thoughts), attention is immediately redirected to the current meditation object (i.e. the breath). In other words, it is a practice of sustained attention. Furthermore, as Josefsson and Broberg (2011) point out, in mindfulness meditation many practices involve directing attention towards internal objects (e.g. thoughts and feelings) whilst the purpose of the Stroop Task is to quickly respond to external targets (words and colours). Thus, the mindfulness meditator may develop a refined attentional ability to be aware of current internal objects and sensations, but this improved ability does not seem to be related to performance on attention tasks requiring quick responses to external targets. It remains for future research to develop alternative methods to assess attention regulation that are more in resemblance with the internally directed attention practiced in mindfulness meditation (Josefsson and Broberg 2011).
We also agree with Lykins et al. (2012) who state that there is no reason to assume that mindfulness practice should lead to a heightened capacity to respond quickly to stimuli, considering the absence of time pressure in the calm and serene nature of mindfulness meditation. In line with Lykins et al. (2012), it may be concluded that effects on attention regulation may be of less importance compared with other beneficial psychological and physiological health outcomes due to mindfulness meditation.
In line with Sears and Kraus (2009), no group effects were found on coping style. Walach et al. (2007) did find significant MBSR post-test increases in positive coping strategies compared with the control group but no differences were found on negative coping. Our results confirm that mindfulness training for a non-clinical healthy population does not seem to affect the use of avoidant coping (negative coping). Furthermore, these results also suggest that neither problem-focused coping nor emotion-focused coping are altered due to mindfulness practice. Unless the population is very stressed, it may be concluded that short-term mindfulness training does not increase problem-focused coping and decrease avoidant coping in an average working population.
The overall pattern of the change score correlations in the different conditions showed that there were more significant relations in the mindfulness group compared with the other groups. It should be noted though that the mindfulness group and the relaxation group had quite a similar correlational pattern with only some minor differences. As would be expected, the wait-list sample had very few significant change correlations.
For the most part, our third and fourth hypotheses concerning correlational changes in the mindfulness group were confirmed. In line with our predictions, decentering change was positively related to the FFMQ total scale change, non-react change, and PWB change. Furthermore, decentering change was negatively related to anxiety change and depression change.
The FFMQ total change scale as well as act aware change were positively correlated with PWB change. Several FFMQ change scales were, as expected, negatively correlated with anxiety change (FFMQ total scale, act aware, non-judge, and describe). On the other hand, only one FFMQ change scale, act aware, was negatively associated with depression change.
The strong correlations at the pre- and the post-tests between decentering and non-react (in the total sample) as well as the strong correlation between decentering change and non-react change in the mindfulness group may reflect the theoretical similarities between these two constructs, and it is highly possible that they, to a substantial extent, assess the same phenomena. Furthermore, the pre- and post-test correlations between the FFMQ total scale and decentering in the overall sample are similar to what Carmody et al. (2009) found, and confirm their conclusion that mindfulness (as measured by the FFMQ) and decentering (as measured by the EQ) should be seen as overlapping rather than separate constructs, and therefore probably reflect an underlying measurement problem. A question that arises is whether mindfulness is better operationalised as a one- or perhaps a two-dimensional construct—as in the MAAS (Brown and Ryan 2003) or the Toronto Mindfulness scale (Lau et al. 2006) for instance—as opposed to the multidimensional FFMQ?
Surprisingly, the only single mindfulness change facet that was related to PWB change was act aware change. A result that may reflect that mindful acting in every day life—being aware of and attending to current behaviours—is an aspect of trait mindfulness that appears to play a more important role in the facilitation of PWB than has previously been recognised.
In line with our predictions and previous research (e.g. Hofman et al. 2010), the results further indicate that increases in mindfulness and decentering are associated with reductions in anxiety symptoms. Whereas increases in decentering are associated with depression reductions, increases in mindfulness are only weakly related to depression decreases. An improved ability to act with awareness is associated with depressive symptom reductions, once again reflecting the seemingly important role this facet plays in mental health.
Additional correlational change analyses in the mindfulness group showed that neither decentering change nor FFMQ changes were significantly related to Stroop changes. In line with our previous conclusions concerning the relation between mindfulness, decentering, and executive attention, the correlational analyses also indicate that increases in mindfulness and decentering do not improve executive attention capacities. Similarly, changes in decentering were not related at all to coping style changes. On the other hand, the results indicate that increases in overall trait mindfulness, particularly the capacity not to judge, evaluate or criticise experiences and mental events, are associated with a more frequent use of emotion-focused coping strategies. Perhaps a harsh and critical attitude towards one’s thoughts and feelings inhibits an individual from seeking emotional support from others? If I, for instance, am ashamed of my unwanted and unaccepted thoughts and feelings or feel guilty about them, then I might not expect other people to be more tolerant or forgiving. Consequently, I choose not to turn to others for emotional support. In contrast, a self-accepting and less self-critical attitude may make me more open and less afraid to ask for other people’s help. Nevertheless, the present study failed to support previous correlational results on mindfulness and coping style (Weinstein et al. 2009) where trait mindfulness was positively associated with approach coping (similar to this study’s problem-focused coping) and negatively associated with avoidant coping.
The findings from the simple mediation analyses generally supported our fifth hypothesis. Significant mediating effects of decentering were found in three models for PWB. In contrast to the lack of support Carmody et al. (2009) found when they examined decentering as a mediator between mindfulness and psychological outcomes, our results indicate that decentering acts as a mediator between mindfulness and PWB. The difference between our results compared with Carmody et al. (2009) may, to some extent, be influenced by the fact that we excluded non-react from the mindfulness variable (and kept the other four facets) while Carmody et al. (2009) composed their mindfulness variable by the three FFMQ facets; non-react, observe, and non-judge. Although we found rather strong support for the mediating effect of decentering, it is highly possible that other mechanisms, aside from decentering, contribute to increased well-being and reduced anxiety. In the BPM (Grabovac et al. 2011), several components are believed to lead to the proposed mechanism, decreased mental proliferation, and decentering is associated with only two of those components (as described earlier in this paper). Thus, decentering contributes significantly to decreased mental proliferation, but decentering is not viewed as the major sole mechanism in the BPM. Other aspects, such as insight about the three characteristics appear to play an even more important role than decentering in the enhancement of decreased mental proliferation, which is hypothesised to lead to improved mental health and well-being.
In order to properly examine decentering as a mechanism enhanced by mindfulness practice, it is necessary to include variables that clearly separate the construct of mindfulness from its major mechanism. As an alternative to FFMQ, the unidimensional MAAS could be used as the mindfulness variable and EQ–decentering as the mechanism in future mediation analyses, investigating decentering as a mechanism responsible for mental health effects due to MBIs. In future mediation analyses, we also recommend to use a systematic approach, similar to ours, where several models are tested: cross-sectional models to pre–post change score models.
Limitations, Methodological Issues, and Directions for Future Research
The generalisability to the average working population may be limited because of several reasons. Firstly, the participants who announced interest to take part in the study were probably specifically attracted to meditation and mindfulness. Secondly, the pre-test anxiety mean scores were higher than expected; almost a third of the participants’ pre-test anxiety scores indicated a potential anxiety disorder. A result that may suggest that people with anxiety symptoms are more motivated to seek and take part in complementary and alternative treatments, such as mindfulness meditation and relaxation training, for their problems. Finally, the majority of participants had prior experiences in other meditation-related Eastern practices, such as yoga, Qi-gong, and Tai-chi.
The modified short-term MBI used in the present study has not been previously tested. This MBI is similar to the content in MBSR but, as mentioned earlier in the method section, no yoga exercises were included in this programme. Carmody and Baer (2008) found that the yoga exercises in MBSR were significantly related to more outcome variables that indicate reductions in psychological symptoms than any other technique practiced in the programme. Moreover, yoga was also significantly associated with four FFMQ facets as well as improved well-being. In comparison, sitting meditation was only significantly related to increased well-being, two FFMQ facets, and two indicators of symptom reduction. Thus, yoga appears to be a very important feature in MBSR. Maybe this is not so surprising, considering that previous research indicate that yoga reduces depression (Pilkington et al. 2005; Uebelacker et al. 2010) as well as anxiety symptoms (Javnbakht et al. 2009). Hence, the lack of significant anxiety and depression reductions may partially be influenced by the absence of yoga in our MBI.
It should be recognised that the increasing number of self-report questionnaires designed to assess mindfulness have been vastly criticised for suffering of several problems (e.g. interpretation and understanding of items may depend on meditation experience, substantial differences in content, and a large variety in number of subscales among different measures) (Grossman 2008; Grossman and Van Dam 2011). In general, Grossman and Van Dam (2011) think that mindfulness has lost some of its original Buddhist meaning in Western conceptualisations and definitions. In fact, Grossman and Van Dam (2011) argue that the Western mindfulness concept may be at risk of being oversimplified and even banalised. Consequently, the majority of self-report questionnaires may not sufficiently reflect the Buddhist mindfulness construct. For instance, describe and acting with awareness (FFMQ) appear, according to Grossman and Van Dam (2011), to have very little to do with mindfulness as it is described in Buddhist literature. Josefsson (2010) has also questioned the relevance of “describing skills” to the mindfulness construct as well as to the practice of mindfulness. In sum, the validity of the FFMQ (as well as other mindfulness scales) may not be as strong as previous validation studies (e.g. Baer et al. 2008) have indicated. Thus, it is far from clear to what extent the FFMQ actually assesses the fundamental original characteristics of mindfulness.
It is still necessary to investigate the potential unique effects of mindfulness practice. We recommend future trials to try a longer MBI than 4 weeks and compare the health effects with relaxation training, in clinical as well as in non-clinical populations. Furthermore, we find the BPM theory very appealing and promising and an important challenge for future research is to operationalise the mechanisms and empirically test this model.
Conclusions
The results from this study indicate that a short-term MBI improves trait mindfulness and PWB in a non-clinical working population compared with a wait-list group. However, no group differences were found on any of the other variables: decentering depression, anxiety, executive attention, and coping style. Furthermore, the results failed to distinguish any unique MBI effects. The length of the intervention, the similarities between body exercises in MBI and relaxation, and the absence of decentering effects may partly explain the lack of distinct MBI effects, suggesting that MBIs aimed at increasing well-being and problem-focused coping whilst reducing psychological symptoms in a working population should be longer than merely 4 weeks and include more than seven sessions. Furthermore, the lack of decentering effects may, according to the previously described BPM theory (Grabovac et al. 2011), suggest that decentering is not the main mechanism responsible for improved mental health. On the other hand, the mediation analyses supported the hypothesis that increases in mindfulness lead to increased decentering abilities which in turn leads to improved PWB. In line with the BPM theory, decentering may be seen as a crucial additional secondary mechanism.
The results of the present study clearly give further support to previous studies (Lykins et al. 2012) that indicate that executive attention is not improved by mindfulness training. Consequently, proposed theoretical mindfulness models (e.g. Bishop et al. 2004; Shapiro et al. 2006) where self-regulated attention is the core component in the mindfulness construct may be revised to exclude executive attention. Considering that the concentration-based exercises in MBIs could be regarded as training in sustained attention, it may not be surprising that executive functioning is usually not improved due to mindfulness practice. However, it is possible that the attention instruments are not sensitive enough to detect potential MBI effects on attention, such as the refined and improved capacity to attend to internal stimuli (thoughts and emotions). A real challenge for future research is to design instruments that have the capacity to assess internally directed attention.
References
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45.
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., et al. (2008). Construct validity of the Five Facet Mindfulness Questionnaire in meditating and nonmeditating samples. Assessment, 15, 329–342.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., et al. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practise, 11, 230–241.
Bjelland, I., Dahl, A. A., Tangen Haug, T., & Neckelman, D. (2002). The validity of the hospital anxiety and depression scale. An updated literature review. Journal of Psychosomatic Research, 52, 69–77.
Bohlmeijer, E., Prenger, R., Taal, E., & Cuijpers, P. (2010). The effects of mindfulness-based stress reduction therapy on mental health of adults with a chronic medical disease: a meta-analysis. Journal of Psychosomatic Research, 68, 539–544.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 4, 822–848.
Brown, K. W., Ryan, R. M., & Creswell, D. J. (2007). Mindfulness: theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18, 211–237.
Canter, P. H. (2003). The therapeutic effects of meditation. The conditions treated are stress related, and the evidence is weak. BMJ, 326, 1049–1050.
Carmody, J., & Baer, R. A. (2008). Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31, 23–33.
Carmody, J., & Baer, R. A. (2009). How long does a mindfulness-based stress reduction program need to be? A review of class contact hours and effect sizes for psychological distress. Journal of Clinical Psychology, 65, 627–638.
Carmody, J., Baer, R. A., Lykins, E. B., & Olendzki, N. (2009). An empirical study of the mechanisms of mindfulness in a mindfulness-based stress reduction program. Journal of Clinical Psychology, 65, 613–626.
Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: a theoretically based approach. Journal of Personality and Social Psychology, 56, 267–283.
Cash, M., & Whittigham, K. (2010). What facets of mindfulness contribute to psychological well-being, and depressive, anxious, and stress-related symptomatology? Mindfulness, 1, 177–182.
Chiesa, A., & Serretti, A. (2009). Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. Journal of Alternative and Complementary Medicine, 15, 593–600.
Chiesa, A., Calati, R., & Serretti, A. (2011). Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clinical Psychology Review, 31, 449–464.
Claxton, G. (1987). Meditation in Buddhist psychology. In M. A. West (Ed.), The psychology of meditation (pp. 23–38). Oxford: Clarendon.
Cullen, M. (2011). Mindfulness-based interventions: an emerging phenomenon. Mindfulness, 2, 186–193.
Erisman, S. M., & Roemer, L. (2010). A preliminary investigation of the effects of experimentally induced mindfulness on emotional responding to film clips. Emotion, 10, 72–82.
Fan, J., McCandliss, B. D., Sommer, T., Raz, A., & Posner, M. I. (2002). Testing the efficiency and independence of attentional networks. Journal of Cognitive Neuroscience, 14, 340–347.
Feldner, M. T., Zvolensky, M. J., Eifert, G. H., & Spira, A. P. (2003). Emotional avoidance: an experimental test of individual differences and response suppression using biological challenge. Behaviour Research and Therapy, 41, 403–411.
Fjorback, L. O., Arendt, M., Örnböl, E., Fink, P., & Walach, H. (2011). Mindfulness-based stress reduction and mindfulness-based cognitive therapy – a systematic review of randomized controlled trials. Acta Psychiatrica Scandinavica, 124, 102–119.
Fresco, D., Moore, M. T., van Dulmen, M. H. M., Segal, Z. V., Ma, H. S., Teasdale, J. D., et al. (2007). Initial psychometric properties of the experience questionnaire: validation of a self-report measure of decentering. Behaviour Therapy, 38, 234–246.
Goldstein, J., & Kornfield, J. (2001). Seeking the heart of wisdom: the path of insight meditation. Boston: Shambala.
Grabovac, A. D., Lau, M. A., & Willett, B. R. (2011). Mechanisms of mindfulness: a Buddhist psychological model. Mindfulness, 2, 154–166.
Grossman, P. (2008). On measuring mindfulness. Journal of Psychosomatic Research, 64, 405–408.
Grossman, P., & Van Dam, N. T. (2011). Mindfulness, by any other name…: trials and tribulations of Sati in Western psychology and science. Contemporary Buddhism, 12, 219–239.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits. A meta-analysis. Journal of Psychosomatic Research, 57, 35–43.
Hayes, S. C., Stroshal, K. D., & Wilson, K. G. (1999). Acceptance and commitment therapy: an experiential approach to behaviour change. New York: Guildford.
Herrmann, C. (1997). International experience with the Hospital Anxiety and Depression scale—a review of validation data and clinical results. Journal of Psychosomatic Research, 42, 17–41.
Hofman, S. G., Sawyer, A. T., Witt, A. A., & Oh, D. (2010). The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. Journal of Consulting and Clinical Psychology, 78, 169–183.
Jain, S., Shapiro, S. L., Swanick, S., Roesch, S. C., Mills, P. J., Bell, I., et al. (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: effects on distress, positive states of mind, rumination, and distraction. Annals of Behavioral Medicine, 33, 11–21.
Javnbakht, M., Hejazi Kenari, R., & Ghazemi, M. (2009). Effects of yoga on depression and anxiety of women. Complementary Therapies in Clinical Practice, 15, 102–104.
Jorm, A. F., Morgan, A. J, & Hetrick, S. E. (2008). Relaxation for depression. Cochrane database for systematic reviews, 4. Art. No.: CD007142. doi:10.1002/14651858.CD007142.pub2
Josefsson, T. (2010) Mindfulness and meditation experience in relation to attentional performance and psychological well-being among meditators and non-meditators. Unpublished licentiate dissertation, University of Gothenburg, Sweden.
Josefsson, T., & Broberg, A. G. (2011). Meditators and non-meditators on sustained and executive attentional performance. Mental Health, Religion and Culture, 14, 291–309.
Josefsson, T., Larsman, P., Broberg, A. G., & Lundh, L.-G. (2011). Self-reported mindfulness mediates the relation between meditation experience and psychological well-being. Mindfulness, 2, 49–58.
Kabat-Zinn, J. (1994). Wherever you go, there you are. Mindfulness meditation in every day life. New York: Hyperion.
Kabat-Zinn, J. (2004). Full catastrophe living: using the wisdom of your body and mind to face stress, pain and illness. London: Piatkus Books Ltd.
Kabat-Zinn, J., Wheeler, E., Light, T., Skillings, A., Scharf, M. J., Cropley, T. G., et al. (1998). Influence of a mindfulness meditation-based stress reduction intervention on rates of skin clearing in patients with moderate to severe psoriasis undergoing phototherapy (UVB) and photochemotherapy (PUVA). Psychosomatic Medicine, 60, 625–630.
Kaviani, H., Javaheri, F., & Hatami, N. (2011). Mindfulness-based cognitive therapy (MBCT) reduces depression and anxiety induced by real stressful setting in non-clinical population. International Journal of Psychology and Psychological Therapy, 11, 285–296.
Keng, S.-L., Smoski, M. J., & Robins, C. J. (2011). Effects of mindfulness on psychological health: a review of empirical studies. Clinical Psychology Review, 31, 1041–1056.
Klatt, M., Buckworth, J., & Malarkey, W. B. (2009). Effects of low-dose mindfulness-based stress reduction (MBSR-ld) on working adults. Health Education & Behavior, 36, 601–614.
Lau, M. A., Bishop, S. R., Segal, Z. V., Buis, T., Anderson, N. D., Carlson, L., et al. (2006). The Toronto mindfulness scale: development and validation. Journal of Clinical Psychology, 62, 1445–1467.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer.
Lilja, J. L., Frodi-Lundgren, A., Johansson Hanse, J., Josefsson, T., Lundh, L.-G., Sköld, C., et al. (2011). Five facet mindfulness questionnaire—reliability and factor structure: a Swedish version. Cognitive Behaviour Therapy, 40, 291–303.
Lindemann, H. (1986). Avspänning på ett enkelt sätt. Stockholm: Forum.
Lindfors, P. (2002). Positive health in a group of Swedish white-collar workers. Psychological Reports, 91, 839–845.
Lindfors, P., Berntsson, L., & Lundberg, U. (2006). Factor structure of Ryff’s psychological well-being scales in Swedish female and male white-collar workers. Personality and Individual Differences, 40, 1213–1222.
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. New York: Guildford.
Lykins, E. L. B., Baer, R. A., & Gottlob, L. (2012). Performance-based tests on attention and memory in long term mindfulness meditators and demographically matched nonmeditators. Cognitive Therapy and Research, 36, 103–114.
MacLeod, C. M. (2005). The Stroop Task in cognitive research. In A. Wenzel & D. C. Rubin (Eds.), Cognitive methods and their application to clinical research (pp. 17–40). Washington: American Psychological Association.
Manocha, R., Black, D., & Stough, C. (2011). A randomized, controlled trial of meditation for work stress, anxiety and depressed mood in full time workers. Evidence-Based Complementary and Alternative Medicine, 8. doi:10.1155/2011/960583.
Manzoni, G. M., Pagnini, F., Castelnuovo, G., & Molinari, E. (2008). Relaxation training for anxiety: a ten years systematic review with meta-analysis. BMC Psychiatry, 8, 41. doi:10.1186/1471-244X-8-41.
Mikulas, W. L. (2011). Mindfulness: significant common confusions. Mindfulness, 2, 1–7.
Muhonen, T., & Torkelson, E. (2001). A Swedish version of the Cope inventory. Psychological Reports 1(2), Department of Psychology, Lund University.
Murphy, G. E., Carney, R. M., Knesevich, M. A., Wetzel, R. D., & Whitworth, P. (1995). Cognitive behavior therapy, relaxation training, and tricyclic antidepressant medication in the treatment of depression. Psychological Reports, 77, 403–420.
Nyklicek, I., & Kuijpers, K. F. (2008). Effects of mindfulness-based stress reduction intervention on psychological well-being and quality of life: is increased mindfulness indeed the mechanism? Annals of Behavioral Medicine, 35, 331–340.
Pilkington, K., Kirkwood, G., Rampes, H., & Richardson, J. (2005). Yoga for depression: the research evidence. Journal of Affective Disorders, 89, 13–24.
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, & Computers, 36, 717–731.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Ramel, W., Goldin, P. R., Carmona, P. E., & McQuaid, J. R. (2004). The effects of mindfulness meditation on cognitive processes and affect in patients with past depression. Cognitive Therapy and Research, 28, 433–455.
Rani, J. N., & Rao, K. P. (2000). Effects of meditation on attention processes. Journal of Indian Psychology, 18, 53–60.
Reynolds, W. M., & Coats, K. I. (1986). A comparison of cognitive-behavioral therapy and relaxation training for the treatment of depression in adolescents. Journal of Consulting and Clinical Psychology, 54, 653–660.
Ryberg, L. (1986). Lugn och harmonisk med psykisk träning. Västerås: ICA Förlaget.
Ryff, C. D. (1989). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology, 57, 1069–1081.
Ryff, C. D. (1995). Psychological well-being in adult life. Current Directions in Psychological Science, 4, 99–104.
Schmertz, S. K. (2006). The relation between self-report mindfulness and performance on tasks of attention. Master’s thesis, Georgia State University.
Schultz, K. F., & Grimes, D. A. (2002). Generation of allocation sequences in randomised trials: chance, not choice. The Lancet, 359, 515–519.
Sears, S., & Kraus, S. (2009). I think therefore I am: cognitive distortions and coping style as mediators for the effects of mindfulness meditation on anxiety, positive and negative affect, and hope. Journal of Clinical Psychology, 65, 561–573.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002). Mindfulness-based cognitive therapy for depression: a new approach to preventing relapse. New York: Guildford.
Semple, R. J. (2010). Does mindfulness meditation enhance attention? A randomized controlled trial. Mindfulness, 1, 121–130.
Shapiro, S. L., Carlson, L. E., Astin, J. A., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 3, 378–386.
Stetter, F., & Kupper, S. (2002). Autogenic training: a meta-analysis of clinical outcome studies. Applied Psychophysiology and Biofeedback, 27, 45–98.
Stroop, J. R. (1935). Studies of interference in serial verbal reactions. Journal of Experimental Psychology, 18, 643–662.
Tang, Y.-Y., Ma, Y., Wang, J., Fan, Y., Feng, S., Lu, Q., et al. (2007). Short-term meditation training improves attention and self-regulation. PNAS, 104, 17152–17156.
Thera, N. (1972). The power of mindfulness. San Francisco: Unity.
Thera, N. (1996). The heart of Buddhist meditation. San Francisco: Weiser Books.
Toneatto, T., & Nguyen, L. (2007). Does mindfulness meditation improve anxiety and mood symptoms? A review of the controlled research. La Revue canadienne de psychiatrie, 52, 260–260.
Uebelacker, L., Epstein-Lubow, G., Gaudiano, B., Tremont, G., Battle, C. L., & Miller, I. W. (2010). Hatha yoga for depression: critical review of the evidence for efficacy, plausible mechanisms of action, and directions for future research. Journal of Psychiatric Practice, 16, 22–23.
Walach, H., Nord, E., Zier, C., Dietz-Waschkowski, B., Kersig, S., & Schupbach, H. (2007). Mindfulness-based stress reduction as a method for personnel development: a pilot evaluation. International Journal of Stress Management, 14, 188–198.
Weinstein, N., Brown, K. W., & Ryan, R. M. (2009). A multi-method examination of the effects of mindfulness on stress attribution, coping, and emotional well-being. Journal of Research in Personality, 43, 374–385.
Weiss, M., Nordlie, J. W., & Siegel, E. P. (2005). Mindfulness-based stress reduction as an adjunct to outpatient psychotherapy. Psychotherapy and Psychosomatics, 74, 108–112.
Williams, J. M. G., Alatiq, Y., Crane, C., Fennell, M. J. V., Duggan, D. S., Hepburn, S., et al. (2008). Mindfulness-based cognitive therapy (MBCT) in bipolar disorder: preliminary evaluation of immediate effects on between-episode functioning. Journal of Affective Disorders, 107, 275–279.
Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67, 361–370.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Josefsson, T., Lindwall, M. & Broberg, A.G. The Effects of a Short-term Mindfulness Based Intervention on Self-reported Mindfulness, Decentering, Executive Attention, Psychological Health, and Coping Style: Examining Unique Mindfulness Effects and Mediators. Mindfulness 5, 18–35 (2014). https://doi.org/10.1007/s12671-012-0142-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-012-0142-1